
Shape of the Lungs
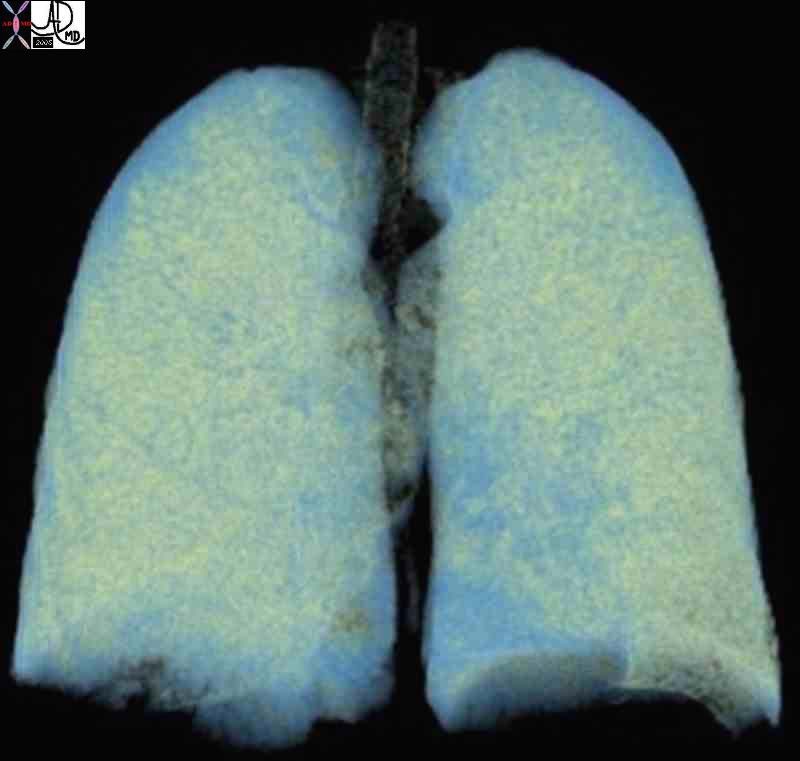
The lungs are funnel, conical, or even pyramidal in shape, with a narrow apex and a broad, concave base.
Ashley Davidoff TheCommonVein.net 32634d02 32634b02

Ashley Davidoff TheCommonVein.net 32634d02 32634b02

Two leaves of the coleus plant, with a pyramidal or conical shape that reminded the photographer of a set of lungs. The branching system originates from the hilum of the leaf almost at its center, but unlike the tracheobronchial tree it is not irregularly dichotomous.
Ashley Davidoff TheCommonVein.net . 42643
Together within the thoracic cage, the lungs may be viewed as an inverted wine glass with the stem of the cup representing the neck and the glass itself the chest. It is the shoulders that are added to the chest that give the sense of the breadth of the chest and the term “broad-chested” is in fact more accurately broad shouldered.

Ashley Davidoff TheCommonVein.net . 22071b01.800
The apex, also called the cupola is dome shaped, fitting snuggly into the space created by the soft tissue confluence of the mediastinal parietal pleura with the costal parietal pleura and the bony frame formed by the clavicle and first rib. It is positioned 2-3cm superior to the medial third of the clavicle where it projects through the superior thoracic inlet.

This cupola or dome was photographed in the church of the Villa Melzi gardens in Bellagio, Italy. If you imagine yourself in the chest cavity and you look up towards the neck, this is what you will see ? the dome shaped structure of the apex of the lung and pleura.
Ashley Davidoff TheCommonVein.net 78115pb01
Lung parenchyma is relatively exposed at the apex making it vulnerable to penetrating injuries of the neck.
The base of the lung is concave so that there is a snug fit with the hemi diaphragms bilaterally. An intimate and parallel contact is maintained during all phases of respiration. This contact is necessary since the function of these two structures is intimately linked. The shape of the base will of course change with respiration and, like two dancers doing the tango, the diaphragm and lung move gracefully, intimately, and sometimes dramatically together with each phase of respiration – even with the sharp turn of events of a hiccup or a cough (or the tango equivalents – the gancho or the giro!).
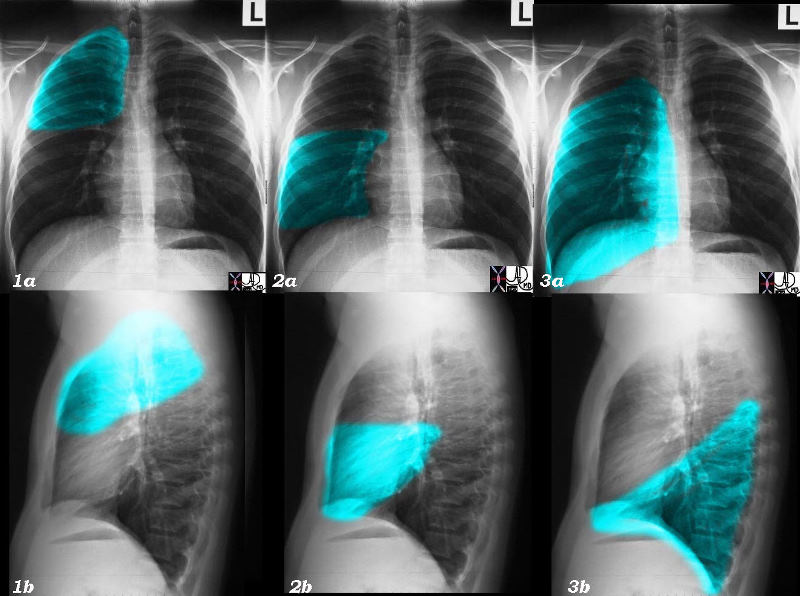
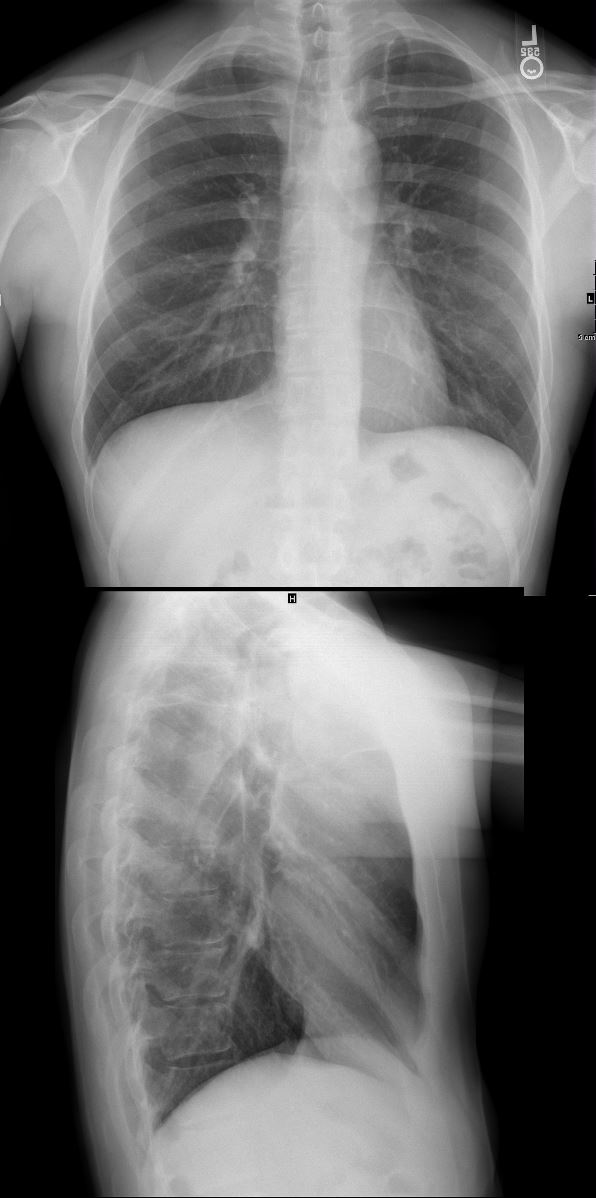
Each lobe of the lungs has a characteristic shape, and may look very different in the A-P projection and lateral projection.. The RUL is roughly triangular in shape but with blunted or rounded angles. It?s A-P shape is very similar to its lateral shape. The RML and the RLL are both rectangular in the A-P projection but triangular in the lateral view, (apex at hilum and base anteriorly), though the RML is comparatively smaller.
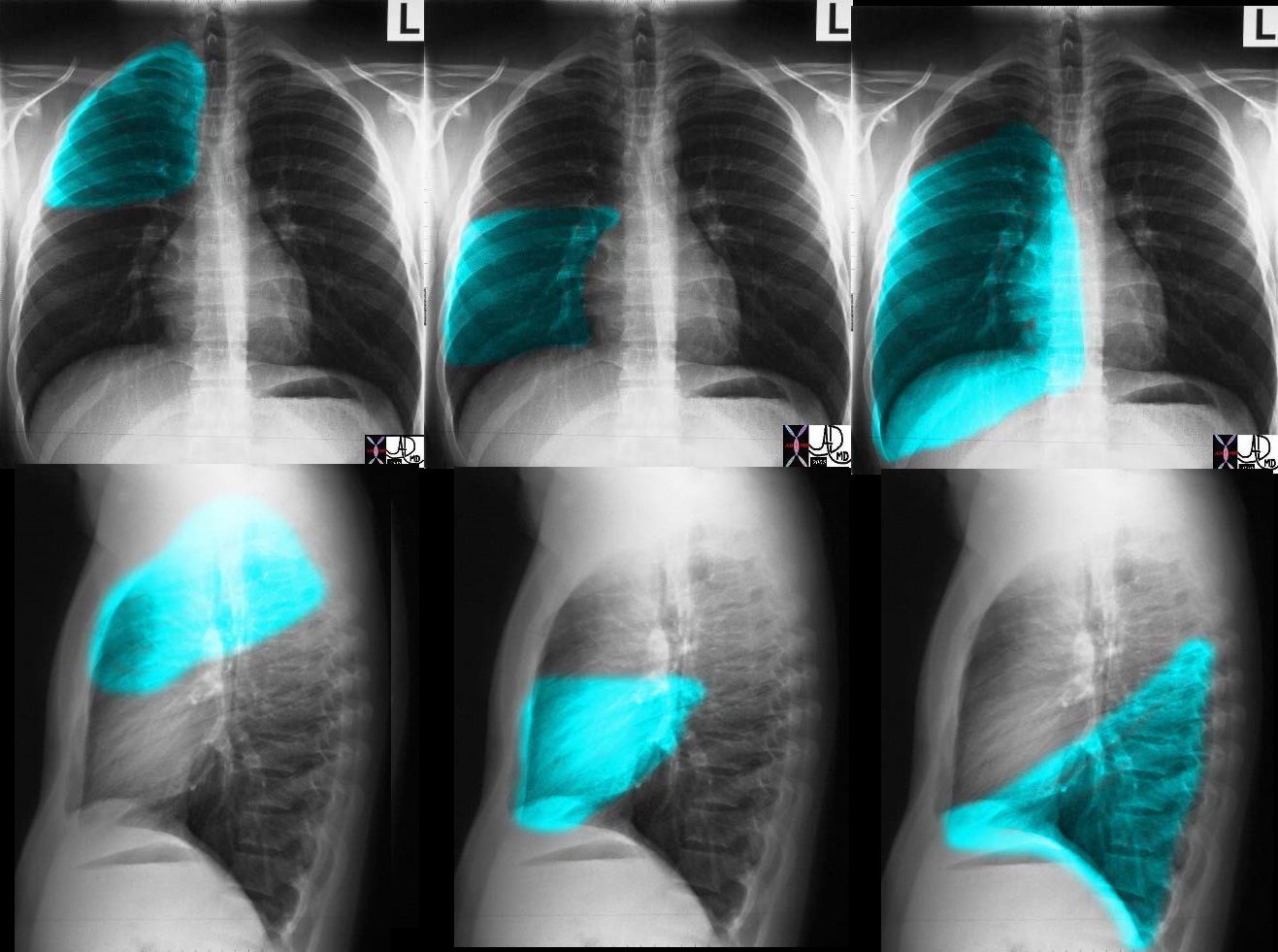
These images (left to right) show the shapes of the RUL, RML and RLL. In Fig 1a and 1b the overlay represents the upper lobe. Image 2a and 2b represent the middle lobe while in 3a and 3b the lower lobe is represented. Note how the middle lobe hugs the right heart border and how much larger the RLL is compared to the RML and the RUL.
Ashley Davidoff TheCommonVein.net 30398c01
Ashley Davidoff MD
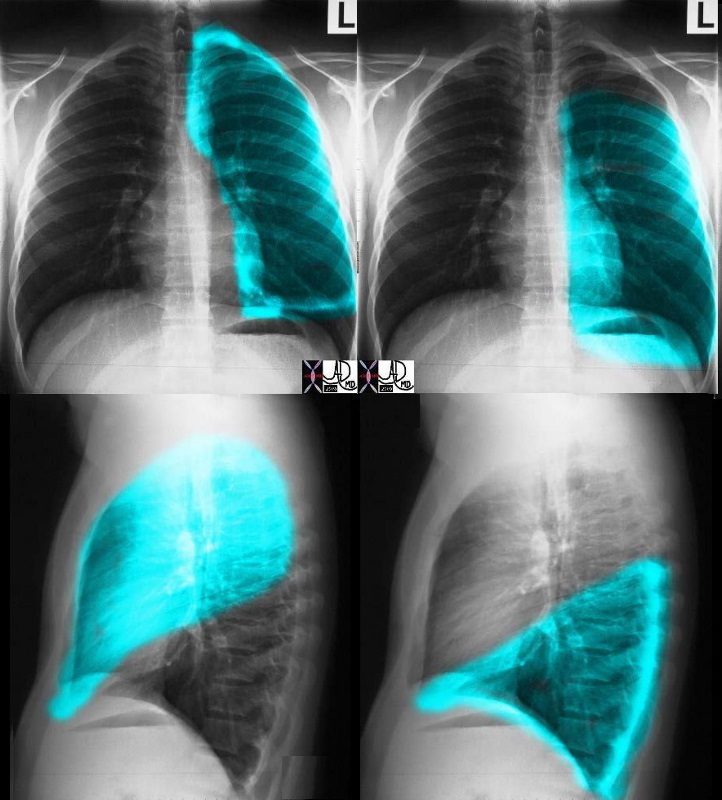
In left sided images (top and bottom on the left), the overlay represents the upper lobe and lingula. Note how the lingula hugs the left heart border. The top and bottom on the right represent the left lower lobe. The volume of the LUL and LLL is about equal. Courtesy Ashley Davidoff MD. 30398c02.8
The LUL from the A-P projection resembles a rectangle with the upper edge being rounded, while from the lateral view it is shaped like half an oval, the bottom part being pointed. The LLL, from the A-P projection, is almost a perfect rectangle, and from the lateral view is almost a perfect triangle.
Applied Anatomy
In a hyperinflated state such as exists in emphysema, the lungs are full, bulging with air, and less pliant, causing the diaphragm to flatten. Clinically, the patient is described as having a barrel shaped chest, a pigeon shaped chest, or in Latin pectus carinatum. The CXR in this circumstance will show flattened hemi diaphragms, reflecting the almost fixed shape of the lungs, and an increase in the air space behind the sternum, (the retrosternal air space) which causes the barrel shape described above.

Keywords:
lungs pulmonary enlarged hyperinflated diaphragm flattened emphysema COPD imaging plain film CXR
Ashley Davidoff MD
TheCommonVein.net
30672c

#signs in medicine
Ashley Davidoff MD TheCommonVein.net
Narrow A-P diameter and an Asthenic build
Predisposes to Pneumothorax
28-year-old male presents for follow up post bullectomy after having a spontaneous pneumothorax. He has a narrow A-P diameter and an asthenic build and the surgical sutures are noted in the left apex of the lung
Ashley Davidoff MD TheCommonVein.net 136231c

28-year-old male presents for follow up post bullectomy after having a spontaneous pneumothorax. He has a narrow A-P diameter and an asthenic build and the surgical sutures are noted in the left apex of the lung (b, arrowhead)
Ashley Davidoff MD TheCommonVein.net 136231c
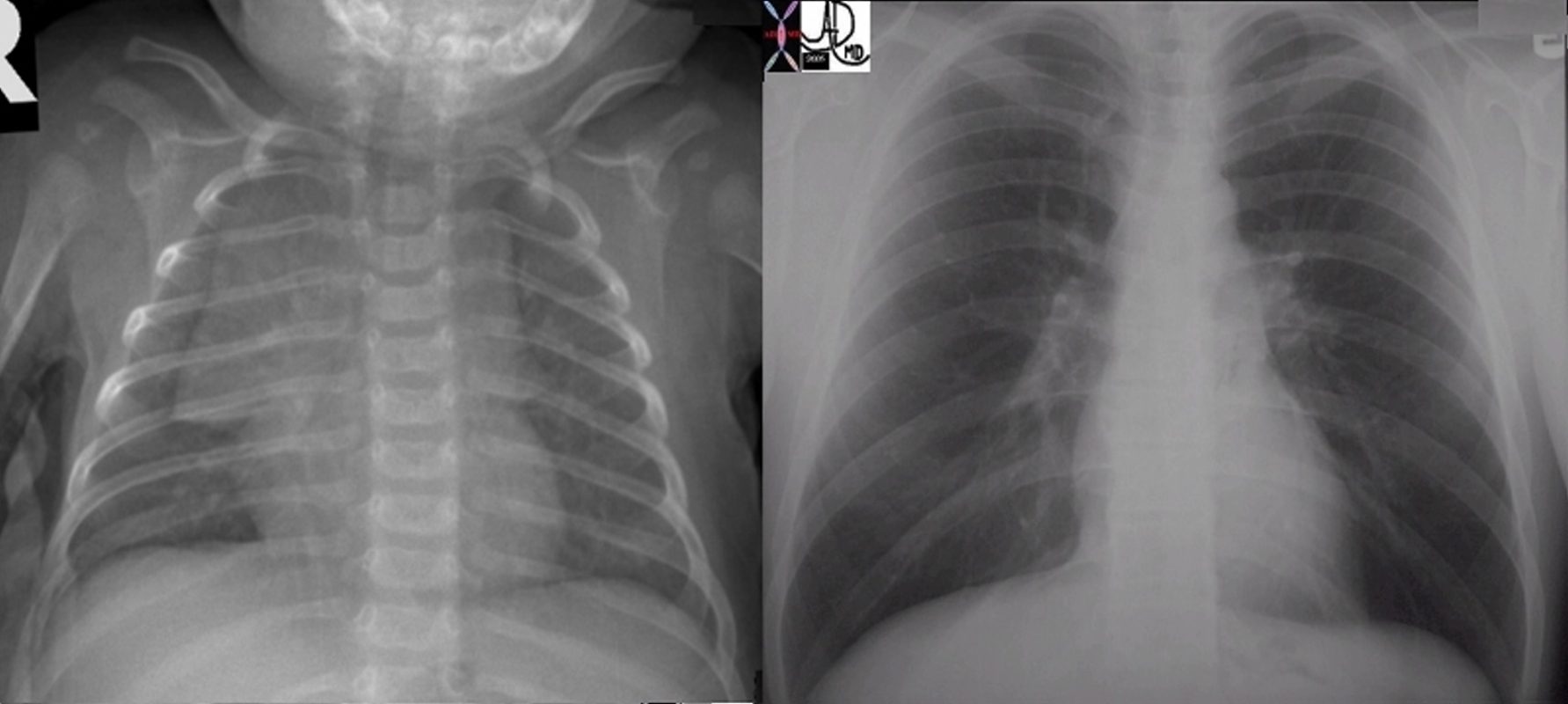
keywords lung chest thymus baby adult mediastinum normal anatomy applied biology CXR chest X-ray plain film time
Ashley Davidoff MD TheCommonVein.net 6663c01

82 year old man s/p thoracoplasty for treatment of right upper lobe TB. Associated finding is left ventricular enlargement
Ashley Davidoff MD TheCommonVein.net
Shapes of Disease
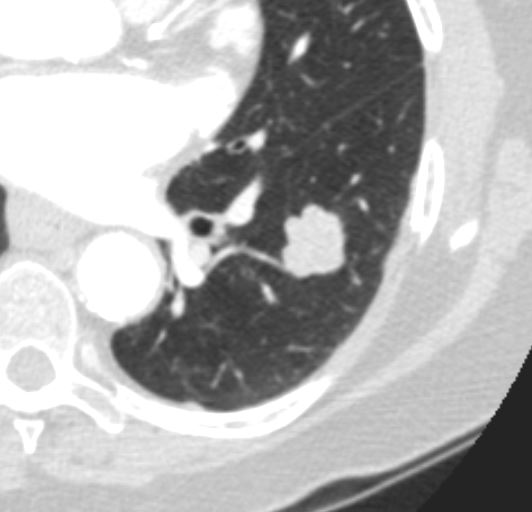
Lobulated Nodule
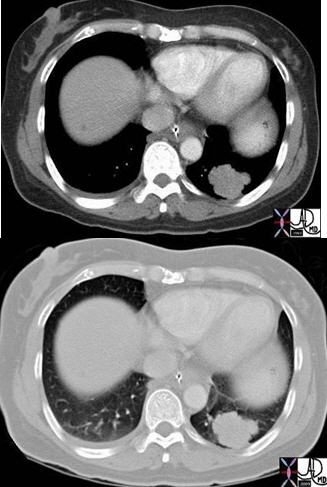
Axial images of the case shown above through the lung mass in a 51-year-old female who presents with nausea vomiting and abdominal distension and who was shown to have a small bowel obstruction. The mass is situated in the left lower lobe and was an incidental asymptomatic finding. It measures in the 3cm range, is lobulated and peripherally located. Pathology showed an adenocarcinoma.
Courtesy: Ashley Davidoff, M.D.TheCommonVein.net Lung cancer P 020
Adenocarcinoma Poorly Differentiated
Ashley Davidoff MD TheCommonVein.net
Effusions Simple vs Loculated
Simple Effusion Obeying the Laws of Gravity
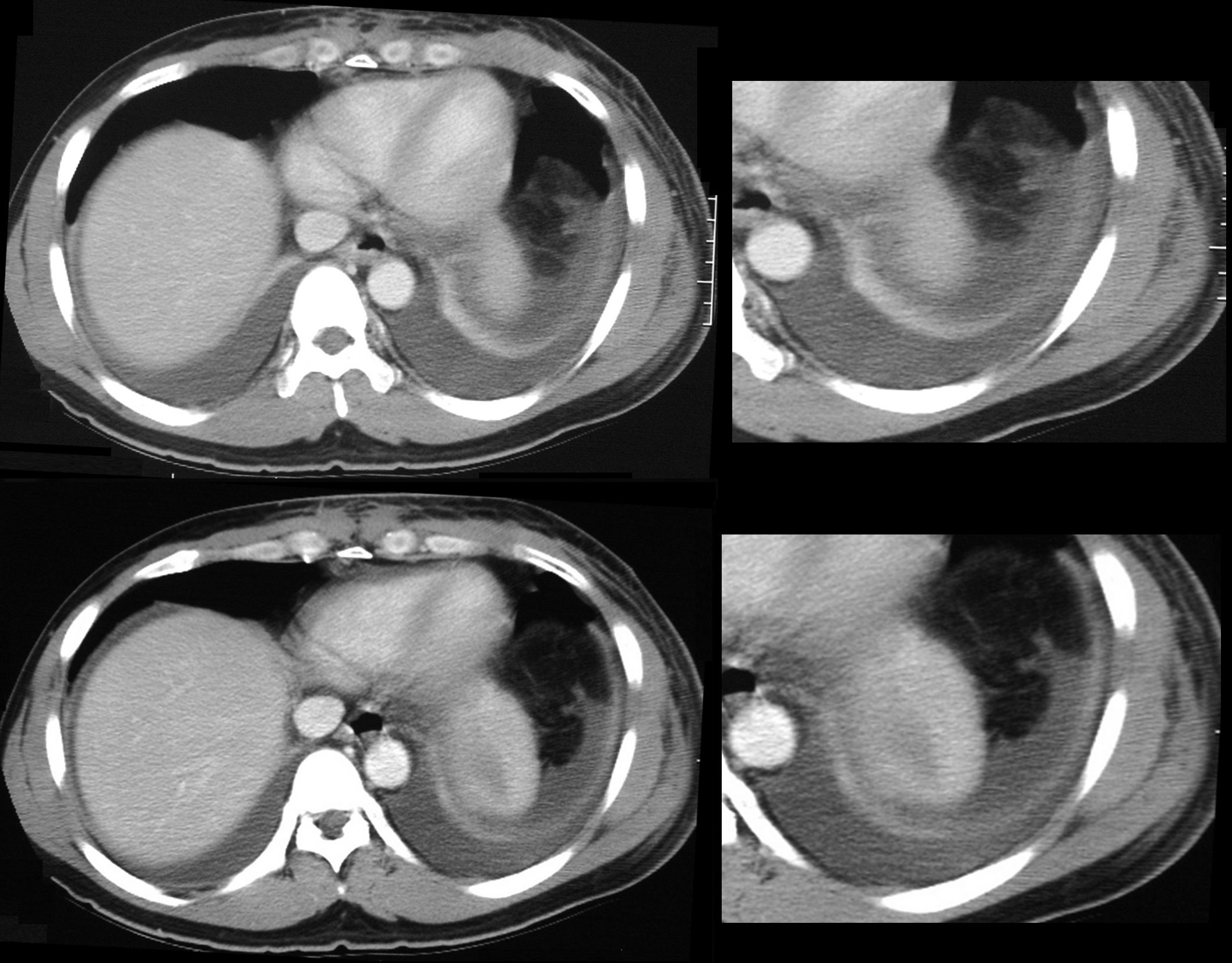
58year old male presents with dyspnea. CT scan shows bilateral pleural effusions with crescentic region of compressive atelectasis in the left lower lobe
Ashley Davidoff MD TheCommonVein.net
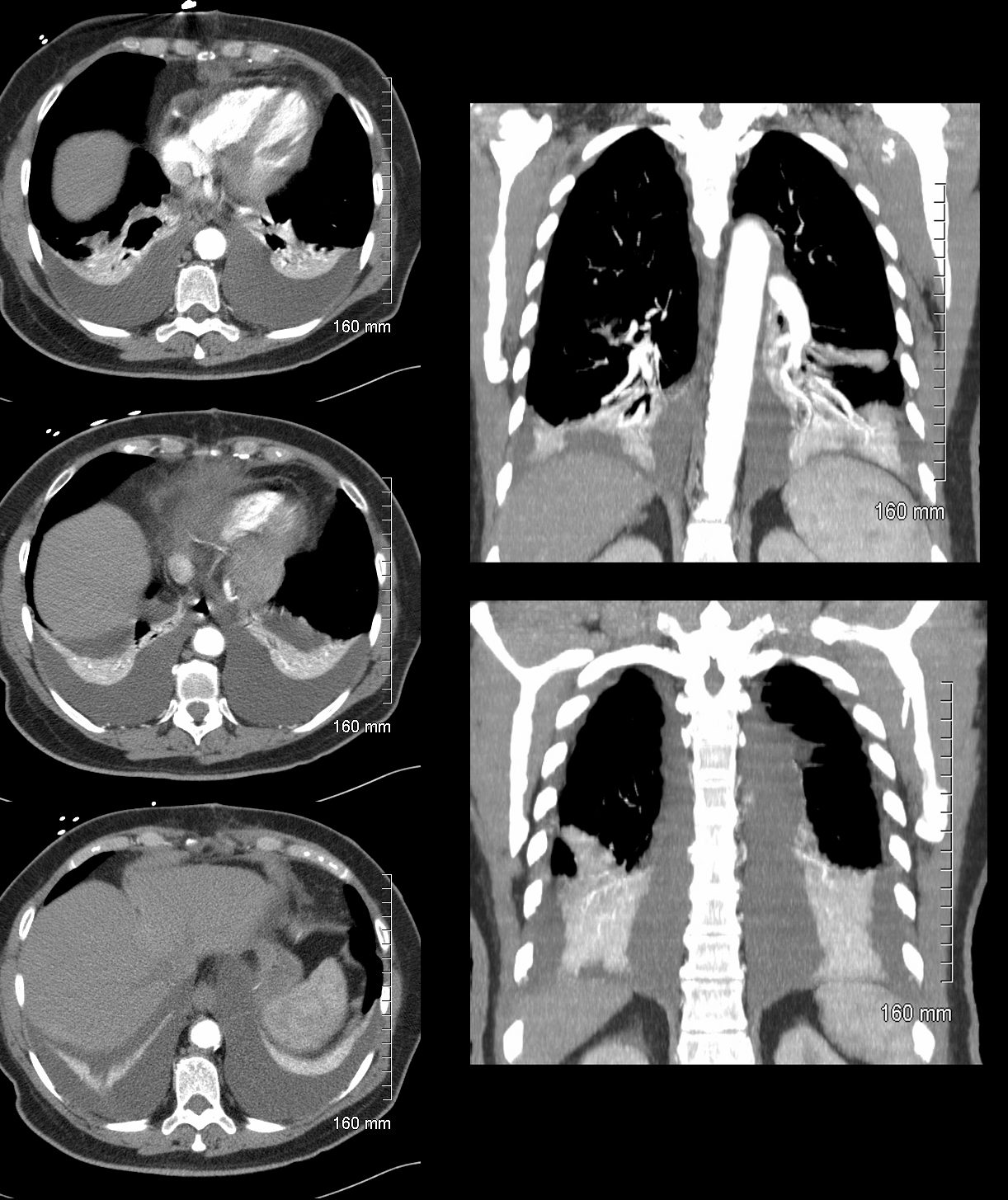
66 year-old female with bilateral simple pleural effusions and compressive atelectasis
Ashley Davidoff MD TheCommonVein.net
Complex Effusion Not Obeying the Laws of Gravity
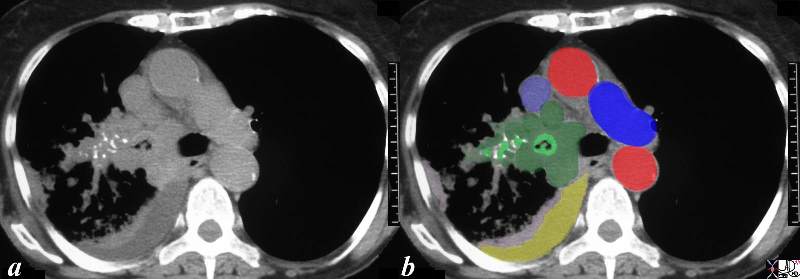
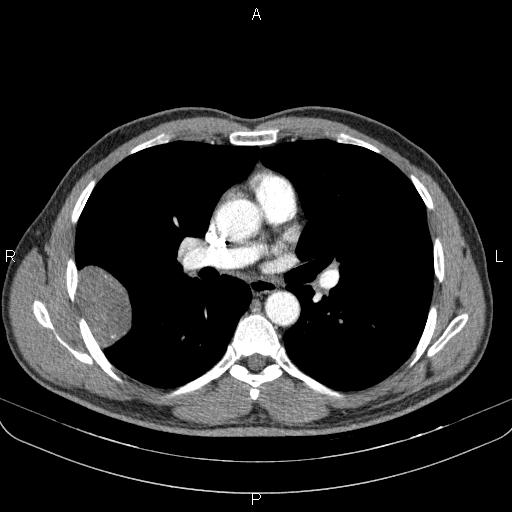
This CT scan is from a middle aged female with poorly differentiated small cell carcinoma, with extensive mediastinal and hilar involvement (dark green in b) extending into and almost occluding the right main stem bronchus light green with black air in the centre) and occluding the smaller airways (light green surrounded by white bronchial cartilage). A complex right effusion (yellow) and atelectasis is seen (light pink). The relationship to the SVC (light blue ) is noted without mass effect at this time, with aorta in red and left pulmonary artery (royal blue). Parenchymal disease is suspected based on the increased soft tissue noted in the mediastinal windows in the right lower lobe.
Courtesy Ashley Davidoff MD TheCommonVein.net 32429bc03.8s
Ashley Davidoff MD TheCommonVein.net
Pleural Based Nodules
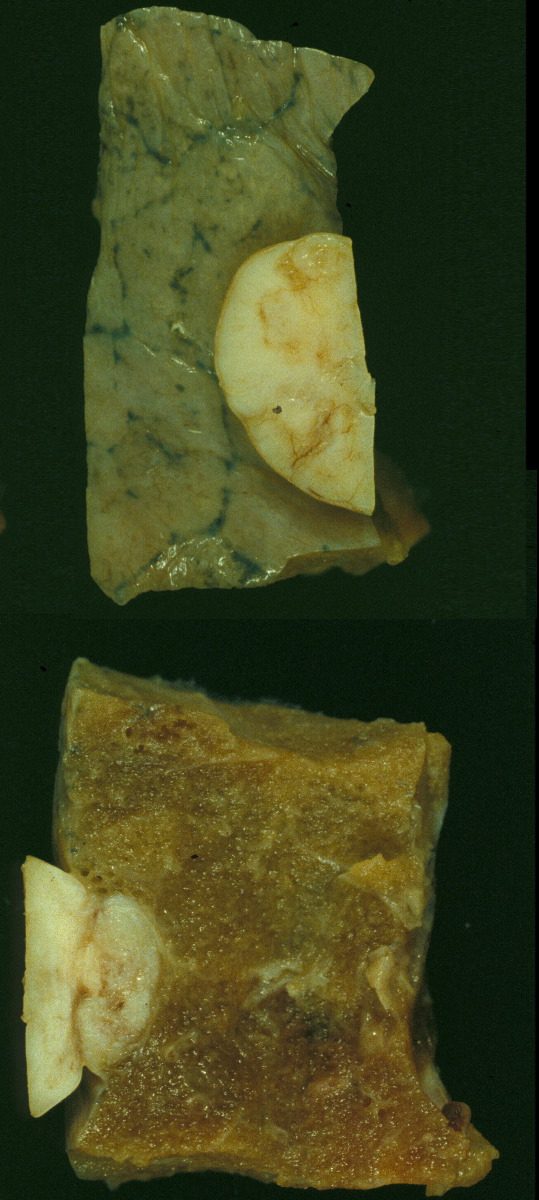
This is a post mortem specimen of a lung in a patient who had primary lung carcinoma with metastatic disease, in whom an incidental benign fibrous mesothelioma was found. The upper image reflects the external surface and the lower image the internal aspect of the lung. Note in the extrinsic mass effect on the lung in both images. Also note the accumulation of carbon in the interlobular septa in the upper image 32198c
Keywords:
lungs pulmonary pleura nodule neoplasm benign fibrous mesothelioma gross pathology
Ashley Davidoff MD TheCommonvein.net 32198c
Note Case courtesy of Mohammadtaghi Niknejad, Radiopaedia.org, rID: 85784
web lungs 687
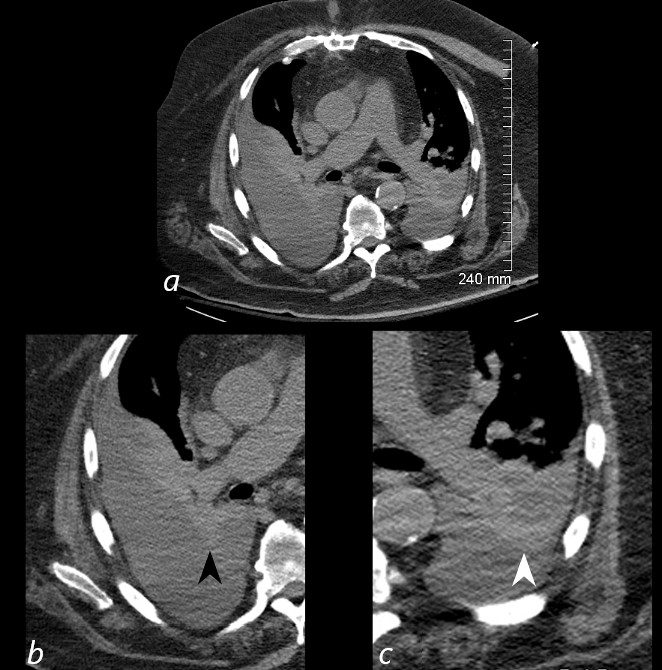
Wedge Shaped Lesions
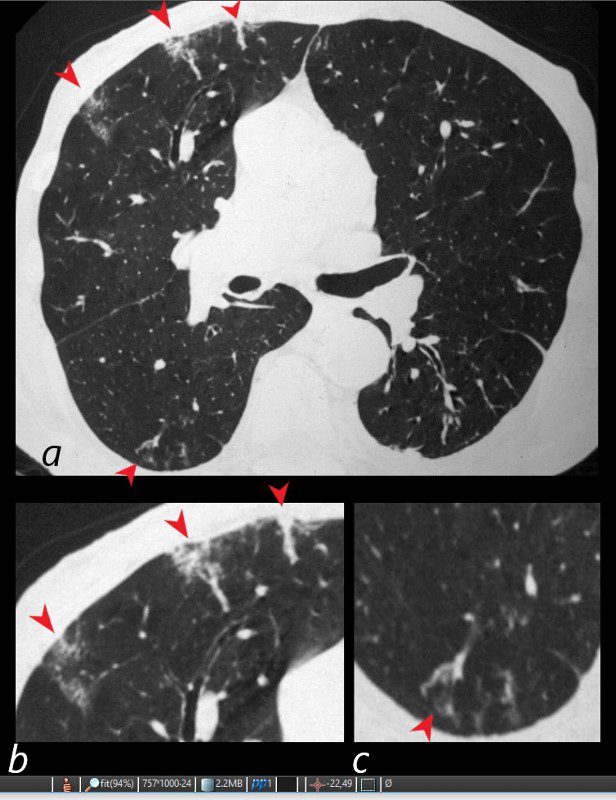
81-year-old male with weight loss, renal failure, and hemoptysis
CT axial view (a) shows multiple peripheral wedge shaped ground glass densities subtended by distended feeding vessels (a,b,c, red arrowheads) reflecting areas of microinfarction due to vasculitis that affects both the arterioles and venules.
Priscilla Slanetz MPH MD TheCommonVein.net

Source
Signs in Thoracic Imaging
Journal of Thoracic Imaging 21(1):76-90, March 2006.