

Infection
TB
{kind=link}
ABPA

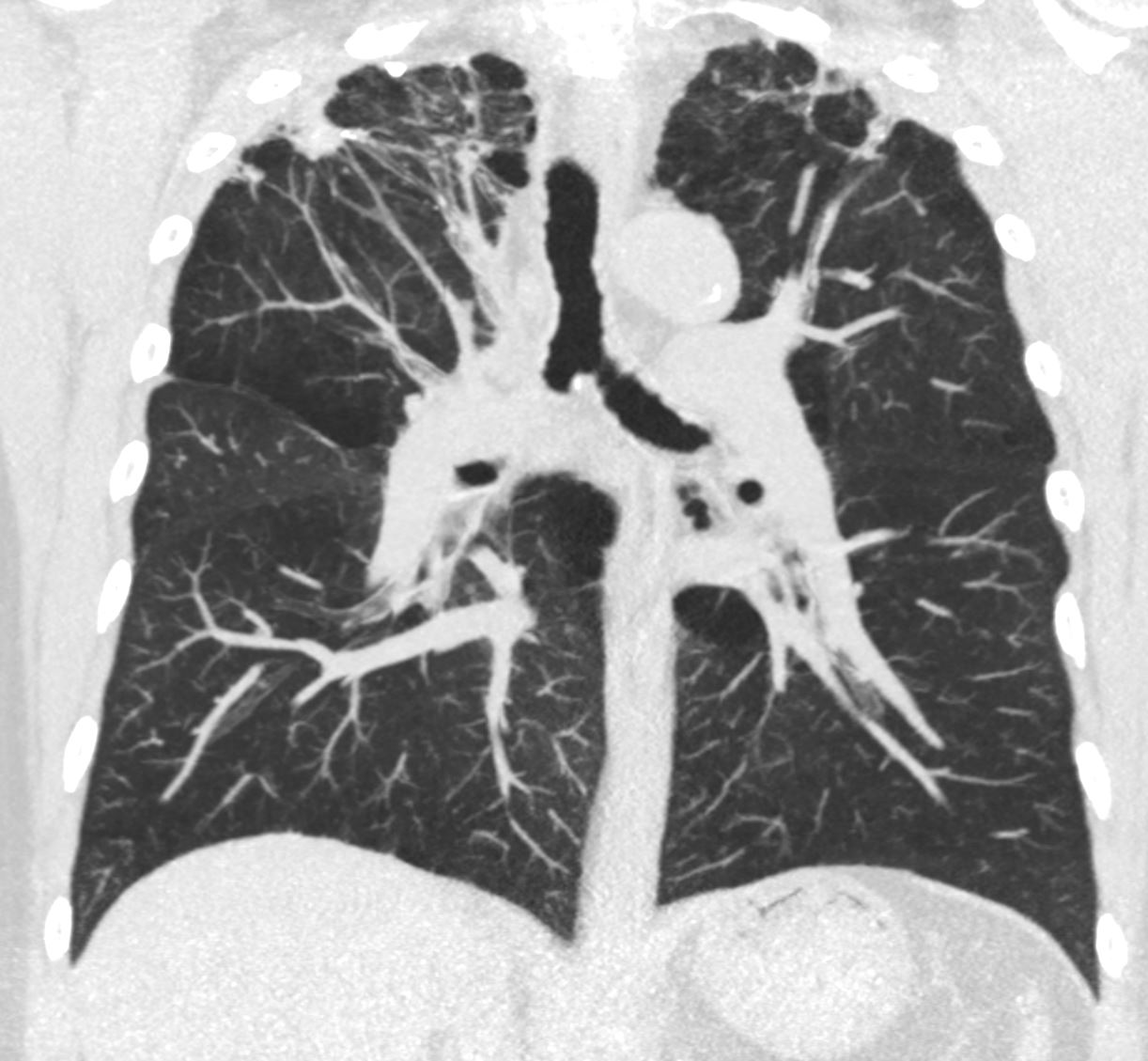
CT scan through the chest shows medium sized bronchi, bronchioles and small airways impacted with fluid. This collage is presented to reveal tree in bud changes resulting from impaction in the smaller terminal bronchioles and respiratory units. The tree-in-bud pattern also results in small centrilobular nodules connected to multiple branching linear structures of similar caliber from a single stalk. Originally it was felt to result from endobronchial spread of Mycobacterium tuberculosis, but is is now recognized in diverse entities including peripheral airway diseases caused by infection (bacterial, fungal, viral, or parasitic), congenital disorders, idiopathic disorders (obliterative bronchiolitis, pan bronchiolitis), aspiration or inhalation of foreign substances, immunologic disorders, connective tissue disorders and peripheral pulmonary vascular diseases such as neoplastic pulmonary emboli.
In this case there are also dilated medium sized airways, impacted with soft tissue characteristic of the finger in glove sign and most likely due to allergic bronchopulmonary aspergillosis (ABPA)
Ashley Davidoff MD Ashley Davidoff MD TheCommonVein.net
47113c01
Inflammation
Emphysema

Sarcoidosis
lung-sarcoid-64M-stagee-5-018-2years-ago-CT.jpg
{kind=link}
Silicosis

Courtesy Maegan Lu, Jonathan Scalera, MD
Courtesy Maegan Lu, Jonathan Scalera, MD
Hypersensitivity Pneumonitis
Langerhans Cell Histiocytosis
Ashley Davidoff MD TheCommonVein.net 50F 01a
Crack Lung

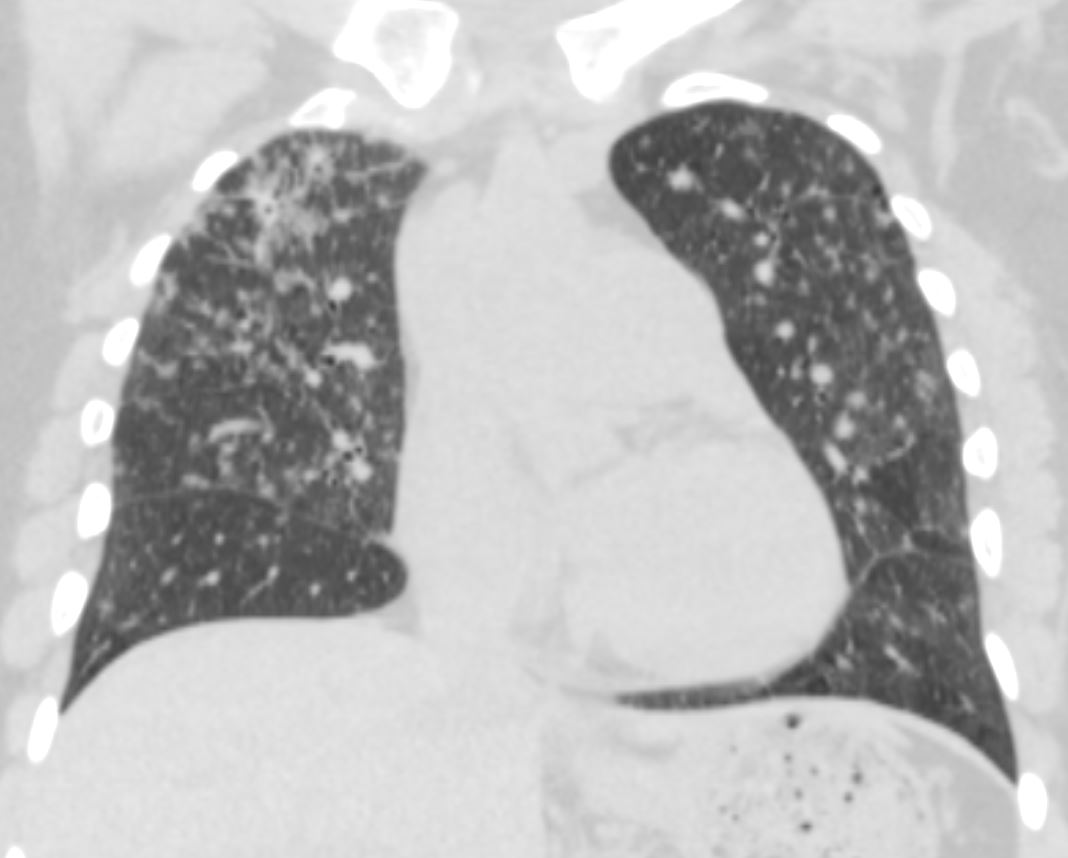
55 year old male with substance use disorder presents with progressive and now more severe dyspnea. Frontal CXR shows extensive upper lobe ground glass changes in the upper lobes. Inhalational pneumonitis was suspected with multifocal regions of consolidation.
Progressive inhalational pneumonitis from smoking or cocaine inhalation was suspected
Ashley Davidoff MD TheCommonVein.net 251Lu 135918

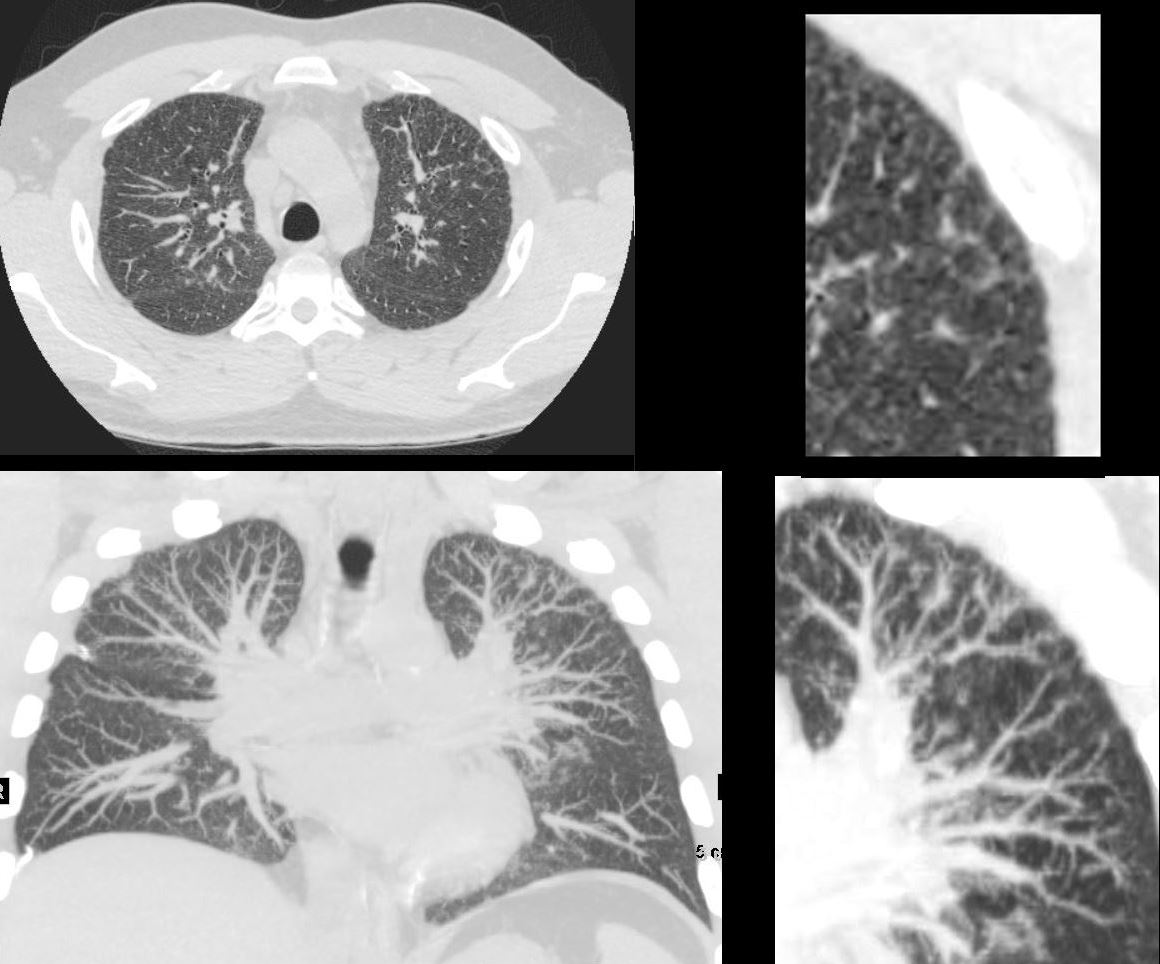
55-year-old male with substance use disorder presents with progressive and now more severe dyspnea. Coronal CT through the mid lung fields shows upper lobe predominant ground glass changes with thickening of the interlobular septa and a ?crazy paving? appearance is suggested. The superior segments of the lower lobes are also involved. Subpleural sparing is suggested. Thickening and irregularity of the right and left major fissures and the transverse fissure are noted.
Progressive inhalational pneumonitis from smoking or cocaine inhalation was suspected. DIP and hypersensitivity pneumonitis remained in the differential diagnosis
Ashley Davidoff MD TheCommonVein.net 251Lu 135935

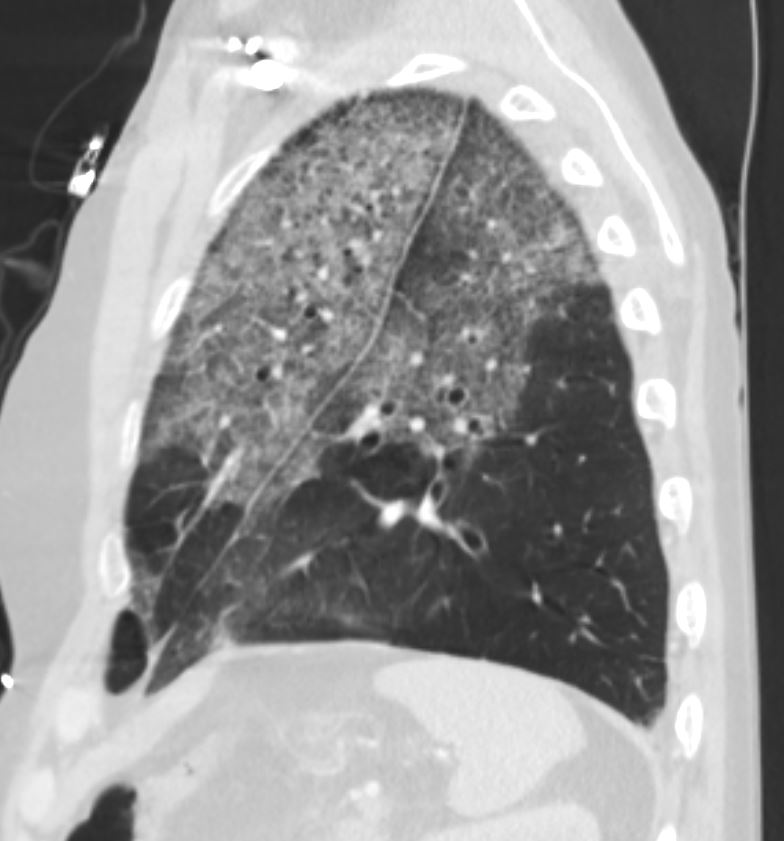
55-year-old male with substance use disorder presents with progressive and now more severe dyspnea. Sagittal CT through the right lung field shows ground glass changes in the upper mid and superior segment of the lower lobe. The fissures of the areas of involved lung are focally thickened. There is subpleural sparing
Progressive inhalational pneumonitis from smoking or cocaine inhalation was suspected. DIP and hypersensitivity pneumonitis remained in the differential diagnosis
Ashley Davidoff MD TheCommonVein.net 251Lu 135940
55-year-old male with substance use disorder presents with progressive and now more severe dyspnea. Sagittal CT through the left lung field shows ground glass changes in the upper mid and superior segment of the lower lobe. The fissures of the areas of involved lung are focally thickened. There is subpleural sparing and ?crazy paving? pattern suggested with thickened interlobular septa.
Progressive inhalational pneumonitis from smoking or cocaine inhalation was suspected. DIP and hypersensitivity pneumonitis remained in the differential diagnosis
Ashley Davidoff MD TheCommonVein.net 251Lu 135943
Chronic Eosinophilic Pneumonia

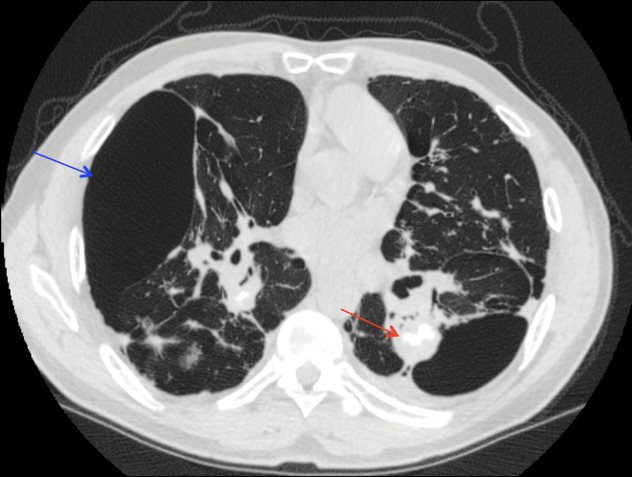
CT scan in the coronal performed 6 months ago at the time of clinical presentation shows upper lobe predominant peripheral infiltrates more prominent in the left upper lobe. Subsequent diagnosis by BAL of chronic eosinophilic pneumonia (CEP) was made
Ashley Davidoff TheCommonVein.net
DIP
Malignancy Mechanical/Atelectasis Trauma Metabolic Circulatory- Hemorrhage Immune Infiltrative Idiopathic Iatrogenic Idiopathic