
Pooja Sikka MD Ashley Davidoff MD
Problem Posed
Solution

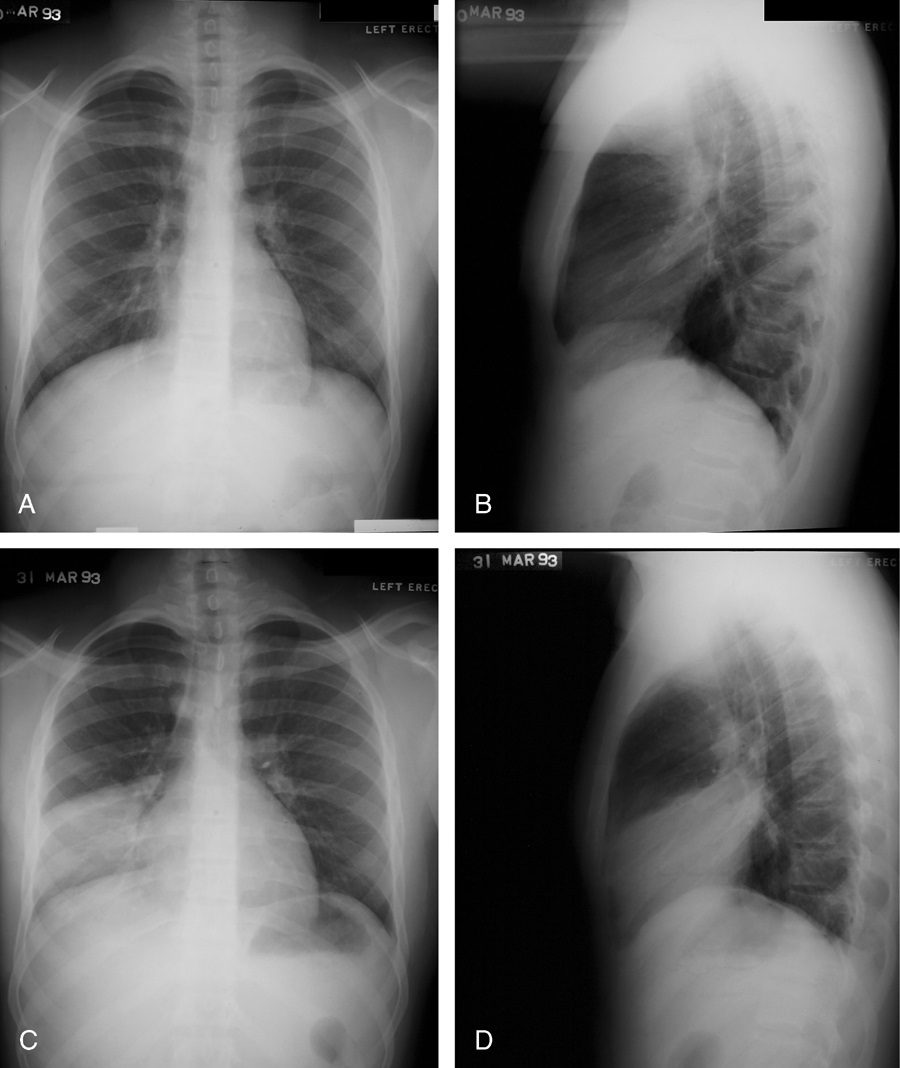
77 year old female with history of asthma, allergic bronchopulmonary aspergillosis (ABPA) and COPD
CXR shows hyperinflation, and consolidation in the left lower lobe silhouetting the left hemidiaphragm, with prominent bronchovascular bundles in the upper lung fields seen both on the PA and the lateral Diagnosis: Asthma Allergic Bronchopulmonary Aspergillosis (ABPA) COPD
Ashley Davidoff TheCommonVein.net

46 year old immunocompromised male presents with a fever. Axial CT shows a subsegmental lingula infiltrate, abutting and silhouetting the left heart border
Ashley Davidoff TheCommonVein.net

46 year old immunocompromised male presents with a fever. Scout for the CT scan shows a cavitating nodule in the left apex and a lingula infiltrate partially silhouetting the left heart border.
Ashley Davidoff TheCommonVein.net
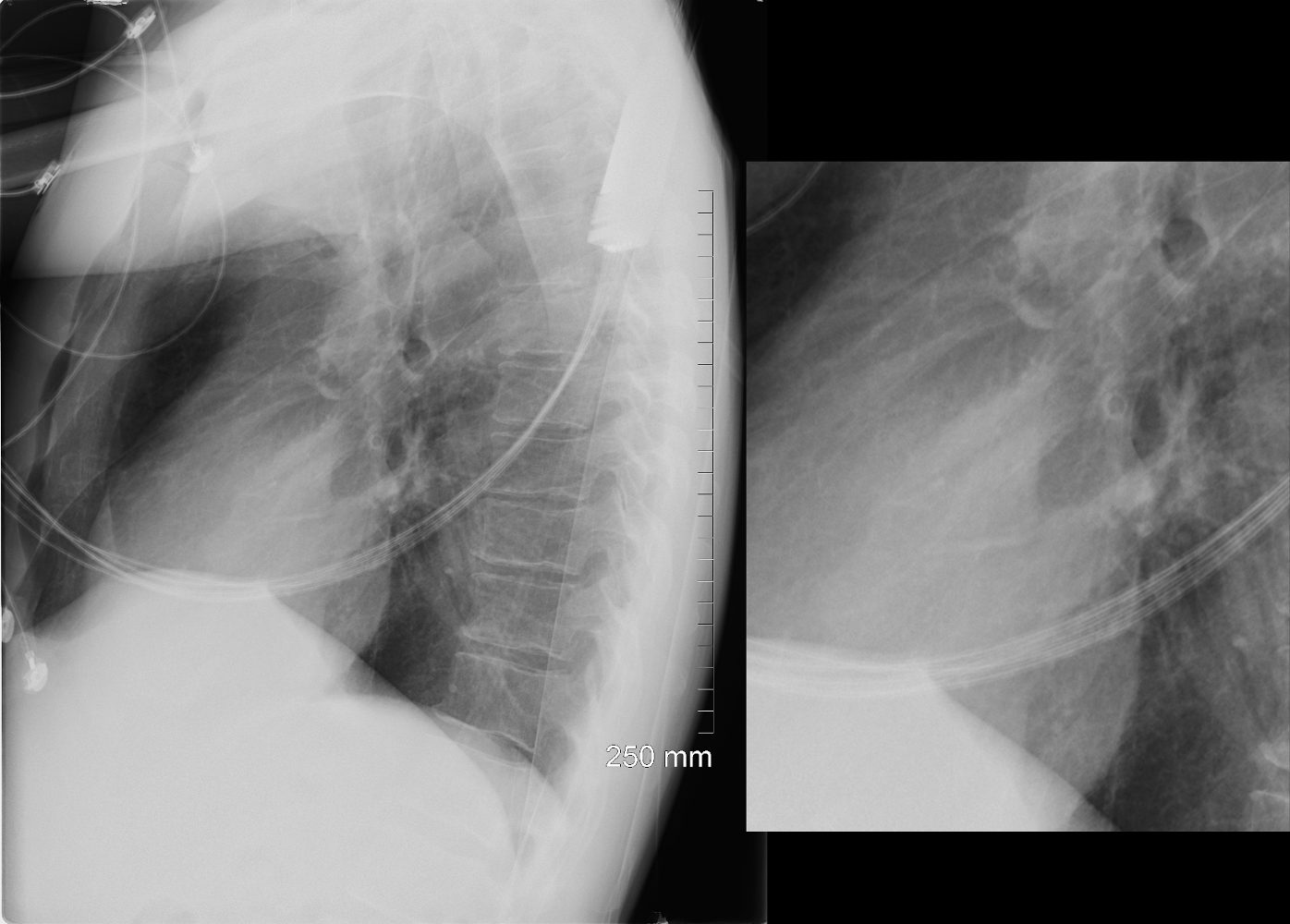
46 year old immunocompromised male presents with a fever. Lateral CXR shows a lingula infiltrate, partially silhouetting the left heart border better seen in the magnified view.
Ashley Davidoff TheCommonVein.net

46 year old immunocompromised male presents with a fever. CXR shows a cavitating nodule in the left apex and a lingula infiltrate partially silhouetting the left heart border.
Ashley Davidoff TheCommonVein.net

77 year old male presents chest discomfort
CT scan without contrast shows atelectasis of the right lower lobe )asterisk c and r) and also seen axial projection (a) magnified in (b) and in (c) magnified in {d) Red arrowheads in b and d show airways filled with material. Aspergillus was isolated at bronchoscopy. Coronal imaging (e magnified in f) show silhouetting of the right hemidiaphragm by the atelectatic lung (white arrowheads
Ashley Davidoff TheCommonVein.net 117786cL
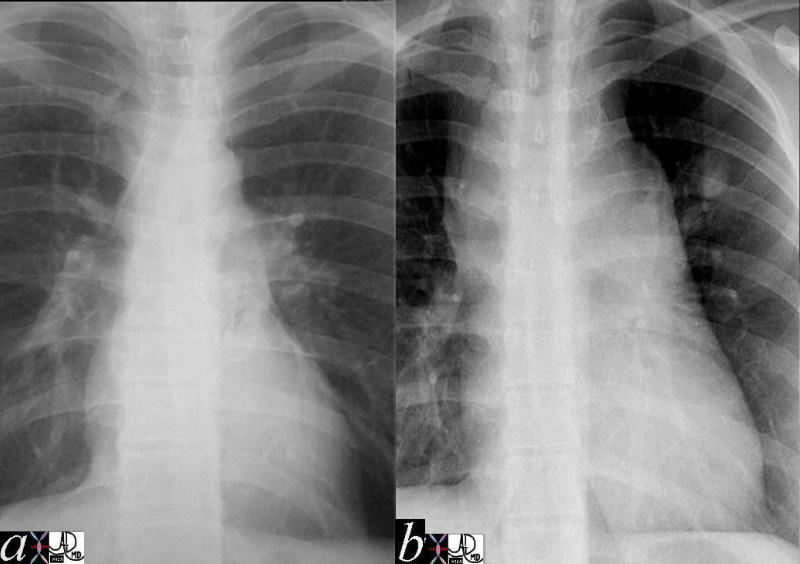
The first image represents the normal and the second a mediastinal silhouette that is very abnormal. There are multiple ?mogul? enlargements, including the region of the aortic knob, the pulmonary segment and the SVC. The following CT explains the appearance.
Ashley Davidoff MD TheCommonVein.net 2056c02
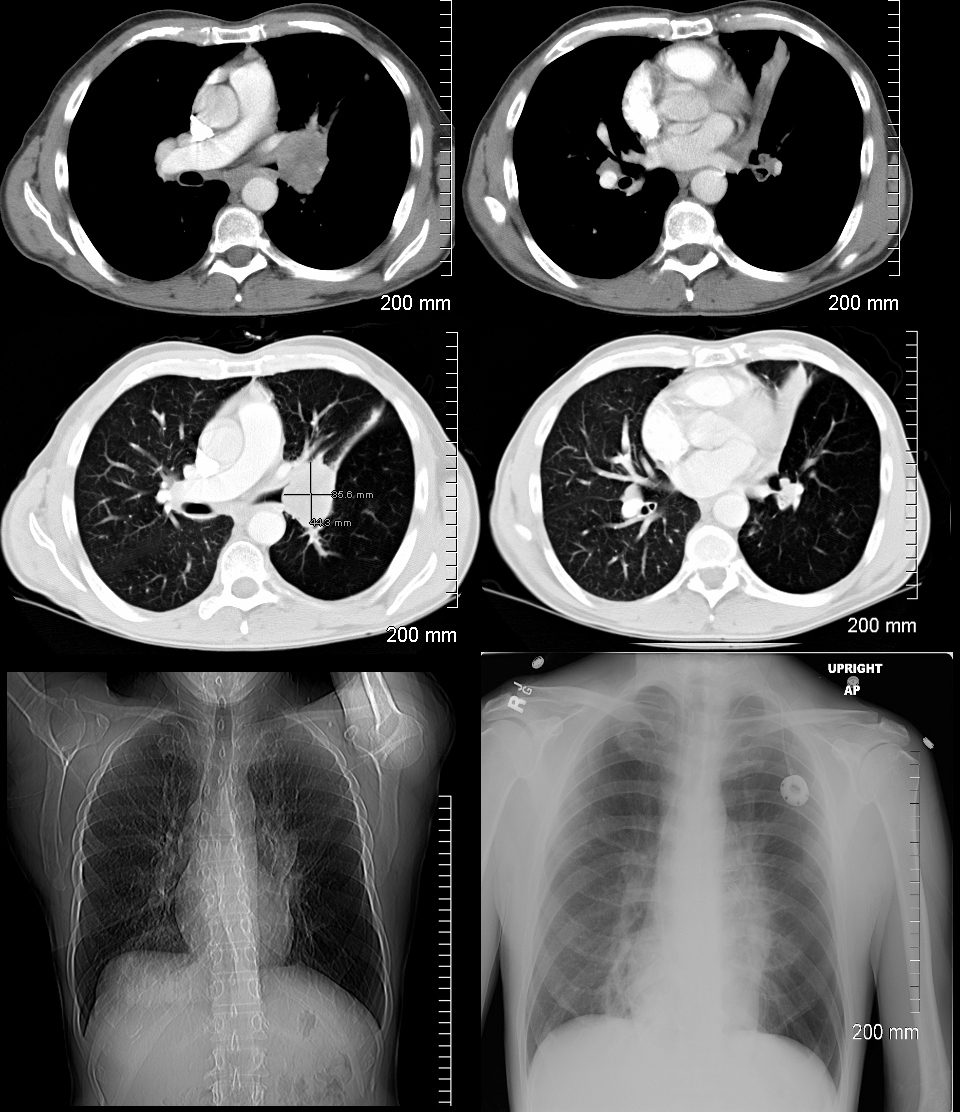
Axial CT images show a central mass with lingula atelectasis. The scout film shows silhouetting of the left heart border. The CXR shows similar finding following stent placement in the lingula
Ashley Davidoff MD TheCommonVein.net
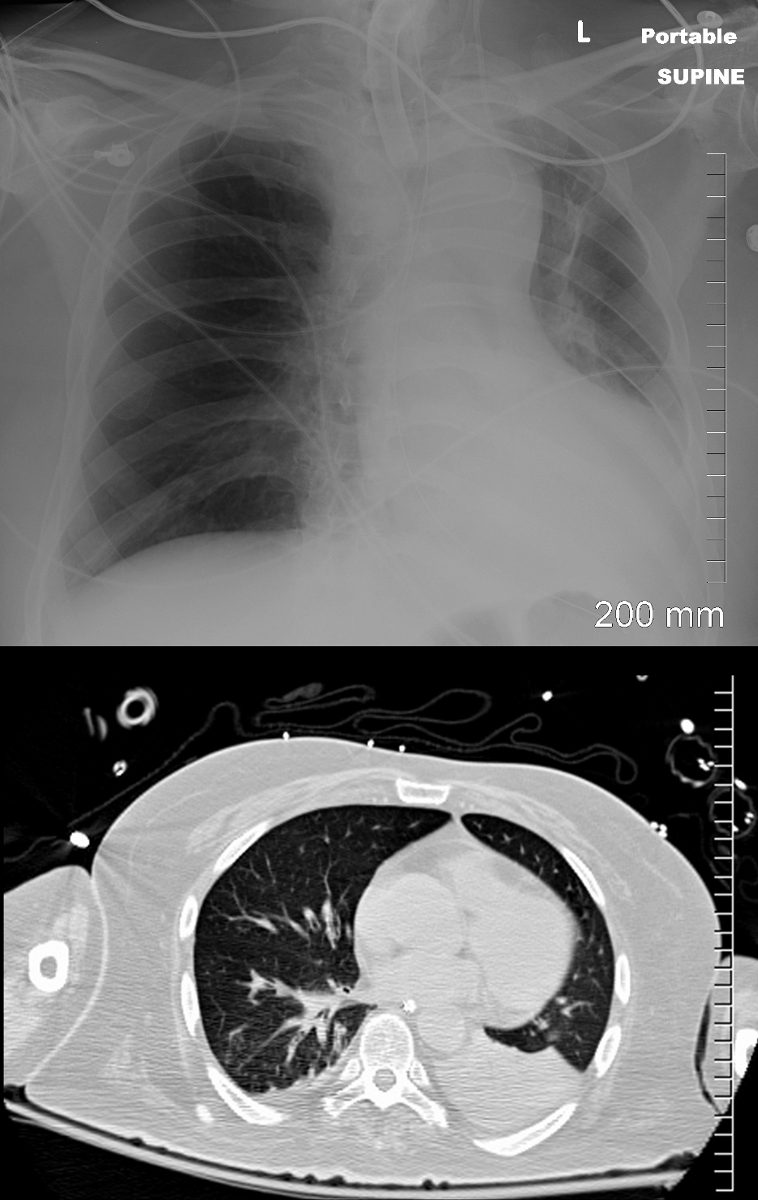
57-year old male presents with a cough. CXR shows silhouetting of the left hemidiaphragm and leftward mediastinal shift. CT scan shows an airless consolidation with leftward shift consistent with atelectasis.
Ashley Davidoff MD TheCommonVein.net

Ashley Davidoff MD TheCommonVein.net

Ashley Davidoff MD TheCommonVein.net 130896c

Source
Signs in Thoracic Imaging
Journal of Thoracic Imaging 21(1):76-90, March 2006.
Source
Signs in Thoracic Imaging
Journal of Thoracic Imaging 21(1):76-90, March 2006.
Previous problem Next problem