Subpleural Sparing
idiopathic, inflammatory, infectious, inhalational, cardiac, traumatic, and bleeding disorders. Specific disorders that can cause subpleural sparing patterns include nonspecific interstitial pneumonia (NSIP), organizing pneumonia (OP), pulmonary alveolar proteinosis (PAP), diffuse alveolar hemorrhage (DAH), vaping-associated lung injury (VALI), cracked lung, pulmonary edema, pneumocystis jirovecii pneumonia (PJP), pulmonary contusion, and more recently, Coronavirus disease 2019 (COVID-19) p
the density and distribution of lymphatics could explain preferential clearing of the subpleural regions during acute injury. T
Infection
PCP PJP COVID
Inflammation
Inhalational Crack Lung Vaping
Scleroderma NSIP and OP
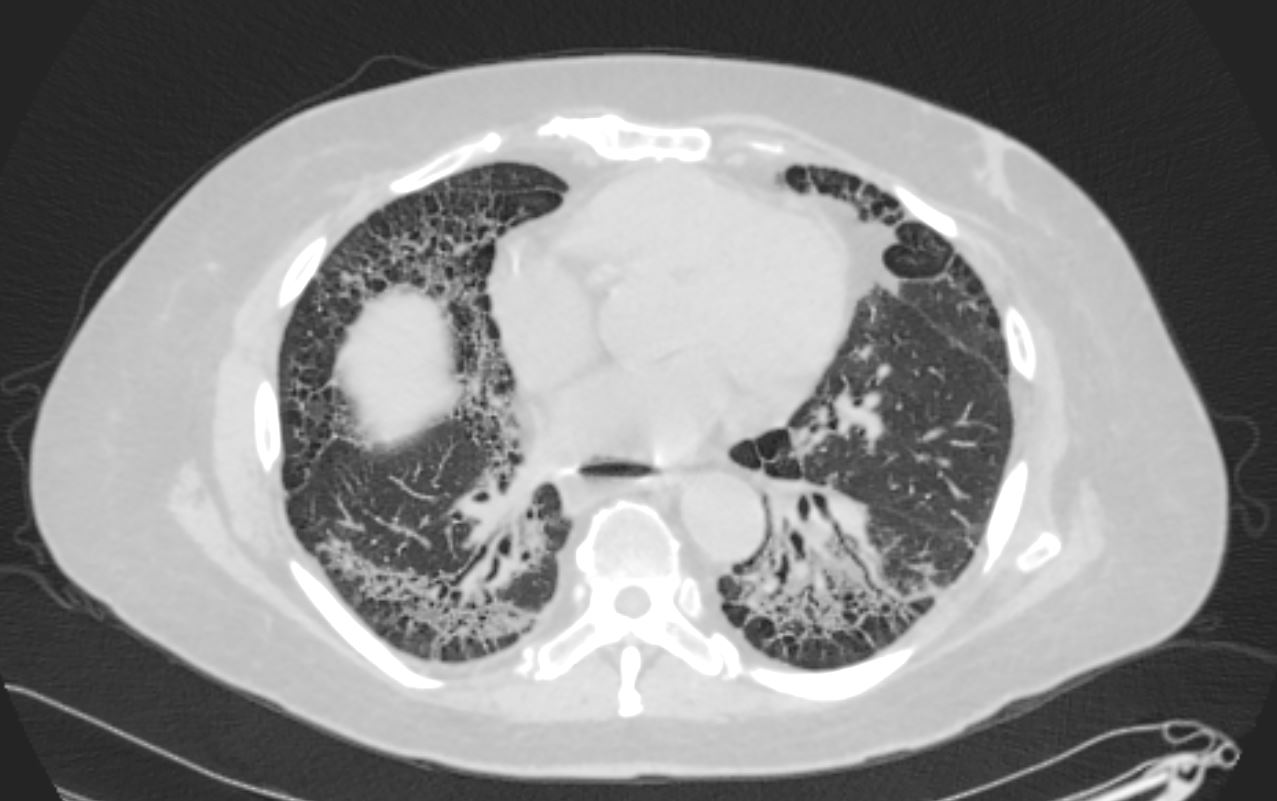
Axial CT shows peripheral reticular changes, ground glass, bronchiolectasis at both lung bases, volume loss with crowding of the bronchovascular bundles posteriorly and subpleural sparing posteriorly. Note air-fluid level in the distended esophagus.
Ashley Davidoff MD TheCommonVein.net 110Lu 136598

59-year-old male presents with history of scleroderma, Raynaud’s disease, and ILD
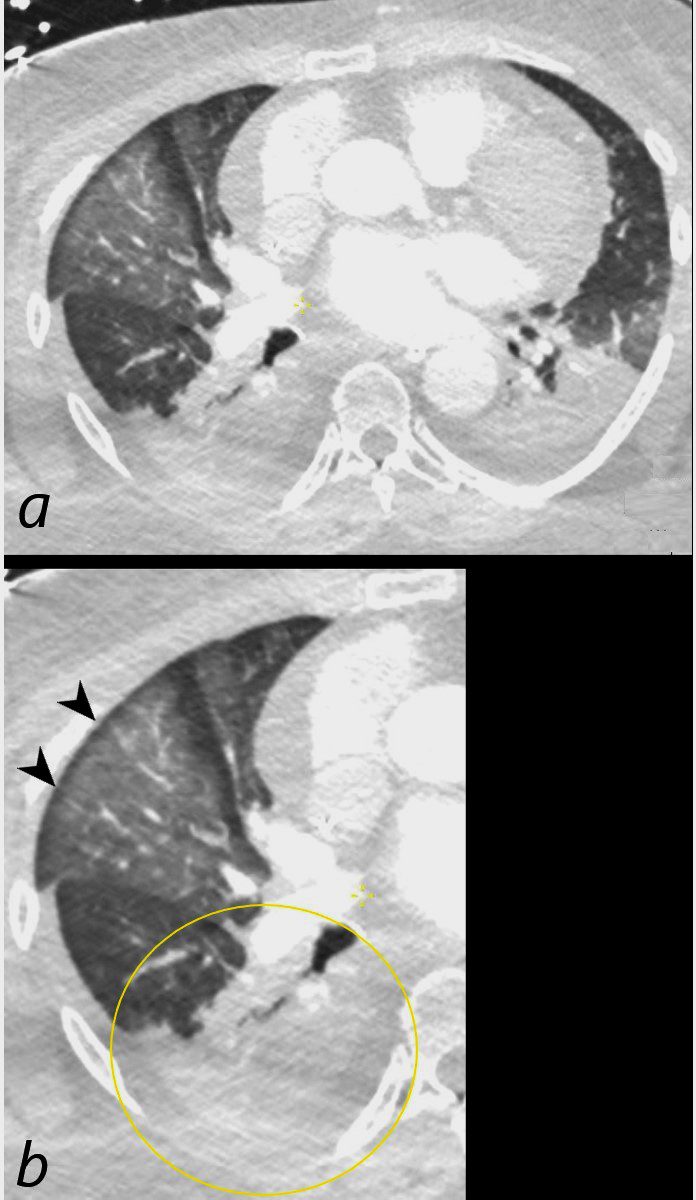
Coronal CT shows bibasilar volume loss, reticular change, ground glass changes, bronchovascular thickening , bronchiectasis, and subpleural sparing, all features characteristic of NSIP
.
The lower image highlights the bronchovascular thickening volume loss bronchiectasis and subpleural sparing. The fibrotic process has resulted in traction of the secondary lobules in the region of subpleural sparing
Ashley Davidoff MD TheCommonVein.net 110Lu 136592c01