
Infection
Inflammation
Aspiration
{kind=link}

Ashley Davidoff MD TheCommonVein.net crazy paving ICU 003

Ashley Davidoff MD TheCommonVein.net crazy paving ICU 002

Ashley Davidoff MD TheCommonVein.net

Ashley Davidoff
TheCommonVein.net ARDS-crazy-paving
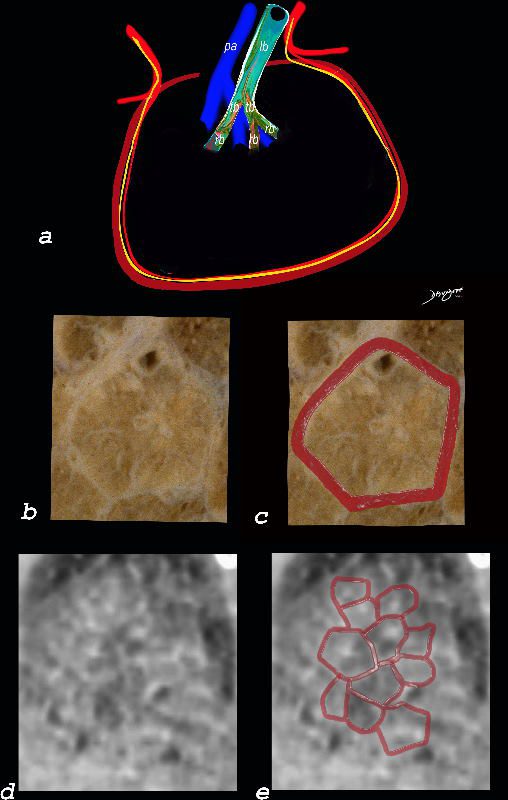
Interlobular Septal Infiltration with Eosinophils and Inflammatory Exudate – Thickening of the Interlobular Septa – Crazy Paving Kerley B lines
The diagram shows the thickened septum surrounding the secondary lobule due to an inflammatory process, cellular infiltrate and congestion of the venules and lymphatics in the septum (a) . An anatomic specimen of a secondary lobule from a patient with thickened interlobular septa is shown in c and overlaid in d. CT of the lungs in a patient with acute eosinophillic pneumonia shows thickened interlobular septa and centrilobular nodules and the thickened septa are overlaid in red (e).
Ashley Davidoff MD The CommonVein.net
lungs-0761
Neoplasm Malignant

shows a bilateral crazy-paving pattern and centrilobular nodules. (b) Photomicrograph (original magnification,
400; hematoxylin-eosin stain) of a specimen from open lung biopsy shows replacement of the alveolar epithelium
by epithelial neoplastic cells with abundant intracytoplasmic mucin (arrows).
Rossi, S.E et al ?Crazy-Paving? Pattern at Thin-Section CT of
the Lungs: RadiologicPathologic Overview Radiographics Volume 23 – Number 6, 2003

Excellent example of crazy paving
Ashley Davidoff TheCommonVein.net 117625
{kind=link}
32469cd.jpg
CT scan through the chest shows diffuse ground glass changes with crazy paving, cardiomegaly with LV dilatation, and bilateral pleural effusions. the differential diagnosis includes amiodarone toxicityAshley Davidoff MD

57-year-old female with progressive dyspnea.
CXR shows bilateral, diffuse alveolar opacities having a perihilar and basal distribution with sparing of the apices
CT shows diffuse ground glass change with crazy paving morphology characterized by bilateral diffuse ground-glass opacities (GGO) with interlobular and intralobular septal thickening. There is a geographical distribution .
Differential diagnosis
ARDS
PCP pneumonia
CHF
Alveolar Hemorrhage
UIP
Hypersensitivity Pneumonitis
XRT pneumonitis
COP
Chronic Eosinophilic
Lymphangitis
Veno-Occlusive Disease
Ashley Davidoff MD

57-year-old female with progressive dyspnea.
CXR shows bilateral, diffuse alveolar opacities having a perihilar and basal distribution with sparing of the apices
CT shows diffuse ground glass change with crazy paving morphology characterized by bilateral diffuse ground-glass opacities (GGO) with interlobular and intralobular septal thickening. There is a geographical distribution .
Differential diagnosis
ARDS
PCP pneumonia
CHF
Alveolar Hemorrhage
UIP
Hypersensitivity Pneumonitis
XRT pneumonitis
COP
Chronic Eosinophilic
Lymphangitis
Veno-Occlusive Disease
Ashley Davidoff MD
TheCommonVein.net

57-year-old female with progressive dyspnea.
CXR shows bilateral, diffuse alveolar opacities having a perihilar and basal distribution with sparing of the apices
CT shows diffuse ground glass change with crazy paving morphology characterized by bilateral diffuse ground-glass opacities (GGO) with interlobular and intralobular septal thickening. There is a geographical distribution .
Differential diagnosis
ARDS
PCP pneumonia
CHF
Alveolar Hemorrhage
UIP
Hypersensitivity Pneumonitis
XRT pneumonitis
COP
Chronic Eosinophilic
Lymphangitis
Veno-Occlusive Disease
Ashley Davidoff MD

57-year-old female with progressive dyspnea.
CXR shows bilateral, diffuse alveolar opacities having a perihilar and basal distribution with sparing of the apices
CT shows diffuse ground glass change with crazy paving morphology characterized by bilateral diffuse ground-glass opacities (GGO) with interlobular and intralobular septal thickening. There is a geographical distribution .
Differential diagnosis
ARDS
PCP pneumonia
CHF
Alveolar Hemorrhage
UIP
Hypersensitivity Pneumonitis
XRT pneumonitis
COP
Chronic Eosinophilic
Lymphangitis
Veno-Occlusive Disease
Ashley Davidoff MD

Source
Signs in Thoracic Imaging
Journal of Thoracic Imaging 21(1):76-90, March 2006.

Crazy paving in ILD is a CT feature of interstitial lung disease and is characterised by diffuse ground glass caused by a combination of interlobular septal and intralobular septal thickening resulting well demarcated patchy densities in the lungs.
Infection
Inflammation
Desquamative Interstitial Pneumonia (DIP)
Diffuse Ground Glass Changes Lower Lung Fields and
Interlobular Septal Thickening (Crazy Paving)

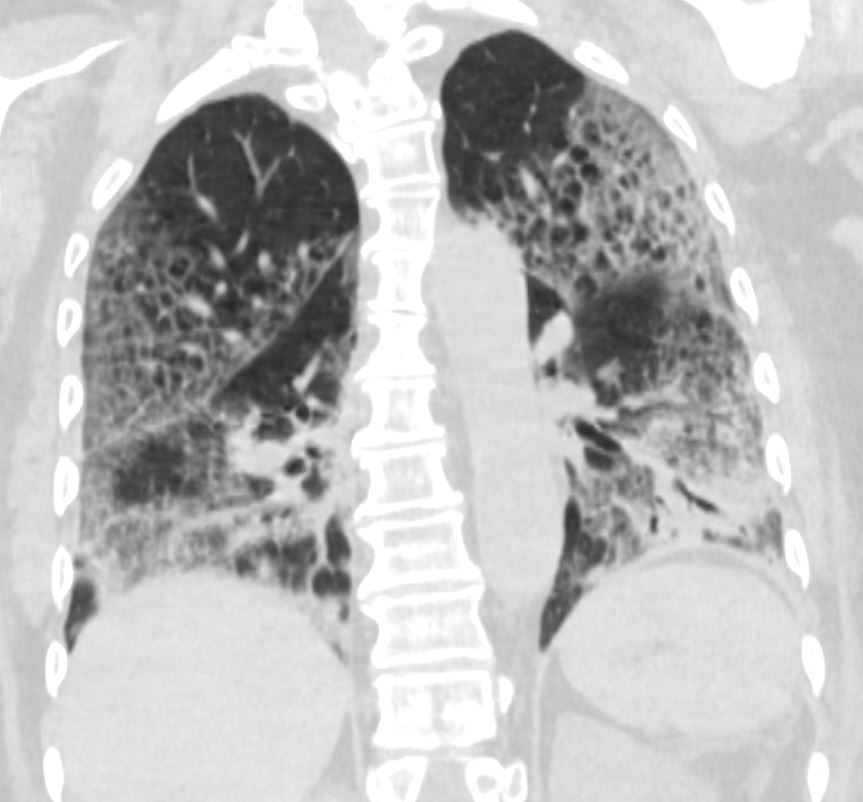
51-year-old female smoker with a history of COPD asthma and pulmonary hypertension presents with progressive dyspnea. Coronal CT through the posterior lungs shows diffuse ground glass changes in the lower lobes with interlobular septal thickening
Pathology confirmed a diagnosis of DIP
Ashley Davidoff MD TheCommonVein.net 252Lu 135997
Crack Lung

55 year old male with substance use disorder presents with progressive and now more severe dyspnea. CT through the mid lung fields shows extensive upper lobe and superior segmental lower lobe ground glass changes with thickening of the interlobular septa giving the appearance of ?crazy paving?. Thickening and irregularity of the major and middle fissures are also noted. There is bilateral peripheral sparing with a batwing distribution
Progressive inhalational pneumonitis from smoking or cocaine inhalation was suspected. DIP and hypersensitivity pneumonitis remained in the differential diagnosis. (Crack Lung)
Ashley Davidoff MD TheCommonVein.net 251Lu 135928

55-year-old male with substance use disorder presents with progressive and now more severe dyspnea. Sagittal CT through the left lung field shows ground glass changes in the upper mid and superior segment of the lower lobe. The fissures of the areas of involved lung are focally thickened. There is subpleural sparing.
Progressive inhalational pneumonitis from smoking or cocaine inhalation was suspected. DIP and hypersensitivity pneumonitis remained in the differential diagnosis (Crack Lung)
Ashley Davidoff MD TheCommonVein.net 251Lu 135942
Malignancy Mechanical/Atelectasis Trauma Metabolic Circulatory- Hemorrhage
Immune
Amiodarone Toxicity

75-year-old male with cardiomyopathy atrial fibrillation and treatment with amiodarone and a RUL infiltrate thought to be related to amiodarone therapy. There was no clinical evidence nor radiological evidence of heart failure.
CT scan shows ground glass changes with multicentric crazy paving appearance that was thought to be related to amiodarone toxicity. bilateral small effusions are present, right greater than left. Following withdrawal of amiodarone and steroids administration he improved clinically and radiologically 3 months later confirming the probability of amiodarone toxicity
Ashley Davidoff MD TheCommonVein.278 Lu 32471
Infiltrative Idiopathic Iatrogenic Idiopathic