
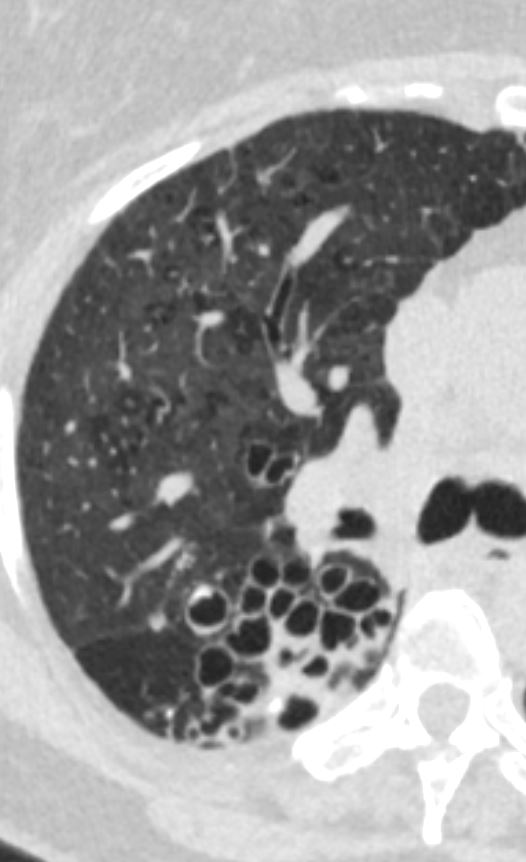
This is a case of a 68 year patient with both severe bronchiectasis in the upper lobes and mid lung regions and evidence of centrilobular emphysema and the the question raised is if the emphysema and bronchitis led to the bronchiectasis?
There are also feautures of prior TB with calcifications in the right upper lobe
- different radiological COPD phenotypes based on the
- presence and severity of emphysema,
- bronchial wall thickening, and
- bronchiectasis.
- Bronchiectasis caused by
- chronic airway inflammation and/or infection.
- prevalence in h COPD is high,
- especially advanced stages. T
- it is
- a different clinical COPD phenotype
- more frequent chronic bronchial infection
- more severe
- and more exacerbations,
- poor prognosis. A
Diffuse Disease with Bronchiectasis noted in the Upper Lobes

Ashley Davidoff MD TheCommonVein.net 68-bronchiectasis 001a

Ashley Davidoff MD TheCommonVein.net 68-bronchiectasis 001b

Ashley Davidoff MD TheCommonVein.net bronchiectasis 008
Diffuse Disease, Upper Lobe and Mid Lung Predominance, Centrilobular Nodules Mosaic Attenuation and Suggestion of Centrilobular Emphysema

Ashley Davidoff MD TheCommonVein.net 68-bronchiectasis 004

Ashley Davidoff MD TheCommonVein.net 68-bronchiectasis 005

Ashley Davidoff MD TheCommonVein.net 68-bronchiectasis 002

Ashley Davidoff MD TheCommonVein.net 68-bronchiectasis 003

Ashley Davidoff MD TheCommonVein.net 68-bronchiectasis 006

Ashley Davidoff MD TheCommonVein.net 68-bronchiectasis 007
{kind=link}

Ashley Davidoff MD TheCommonVein.net bronchiectasis 006b
Ashley Davidoff MD TheCommonVein.net bronchiectasis 006c
{kind=link}
68-bronchiectasis-006d.jpg
Segmental and Subsegmental Bronchiectasis with extension of the disease process into the small airways characterised by centrilobular nodulesAshley Davidoff MD TheCommonVein.net bronchiectasis 006d

Ashley Davidoff MD TheCommonVein.net bronchiectasis 009