
68 yo male with tobacco use and chronic dyspnea presumed to be due to COPD who presents for follow-up in pulmonary clinic. He has had multiple admissions in the past year for respiratory failure in the setting of recurrent COPD exacerbations and pneumonia. He presents today with worsening cough and dyspnea consistent with COPD exacerbation. Overall, his COPD continues to be severe.
CT shows evidence of medium and small airway disease extending into the secondary lobules with tree in bud changes

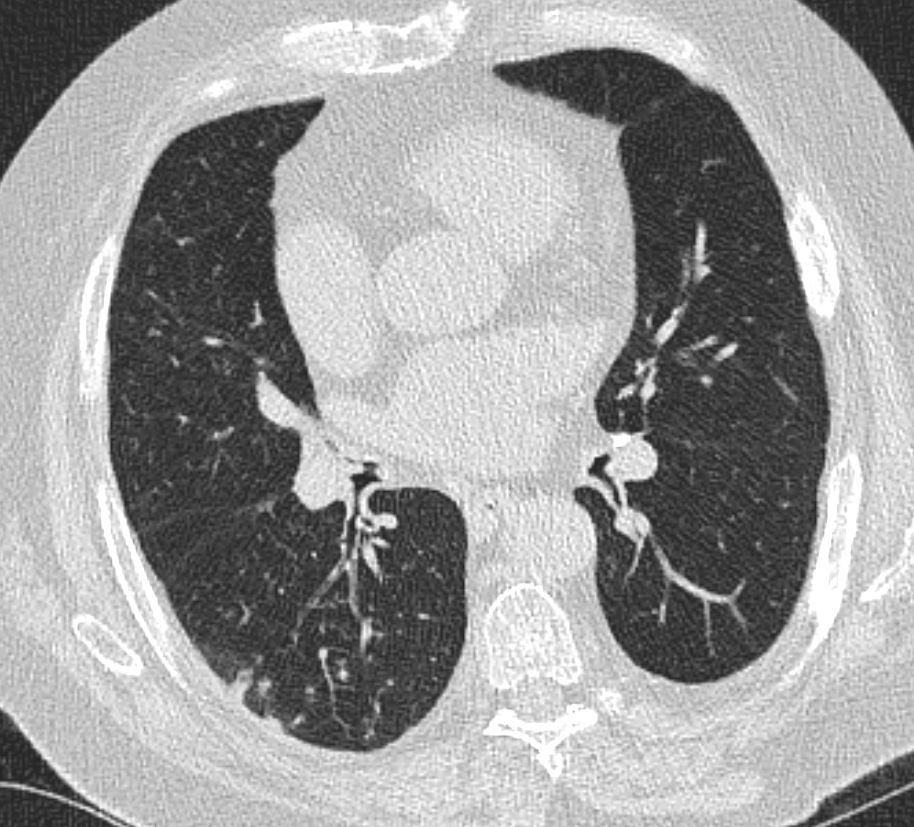

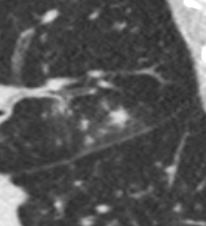
Note a centrilobular nodule likely reflecting an inpacted bronchiole

Thick medium size airway
68M-tree-in-bud-002-medium-small-airway-disease.jpg
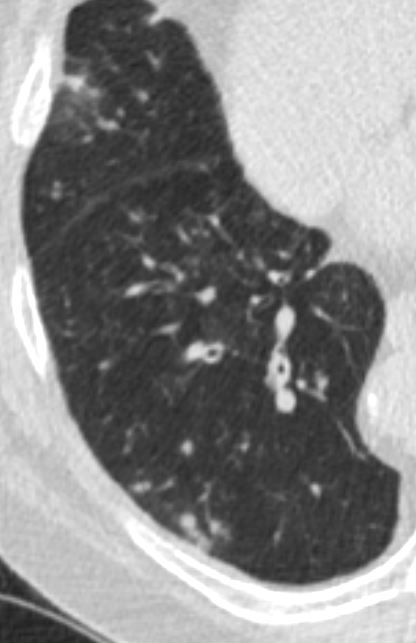
Vein outlining the secondary lobule with multiple intralobular nodules
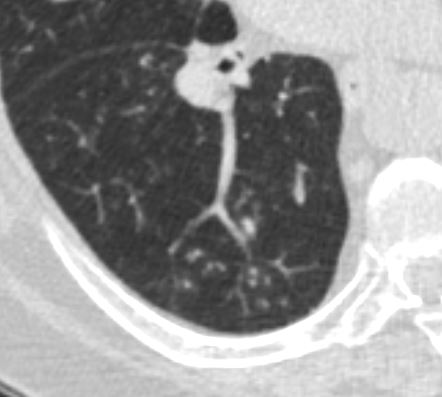

Thick Medium Sized Airways becoming Impacted



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
This patient had most of these findings in the right lung and has a large hiatus hernia Hypothesis was that the patient who has sleep apnea may have aspirated while sleeping on his right side left lung was relatively devoid of similar changes
# Acute COPD exacerbation
diagnosis of presumed COPD in the setting of tobacco use and multiple admissions with wheezing along with imaging findings consistent with chronic bronchitis. He has never had PFTs. He is currently on therapy with symbicort and spiriva and reports adherence to these inhalers, though technique was not reviewed today. He has been using his nebulizer frequently and has had a subacute worsening of symptoms including dyspnea and cough. He feels like he “is always in an exacerbation”. He is on azithromycin three times weekly in the setting of his frequent exacerbations. His ongoing worsening of his COPD is likely multifactorial in the setting of ongoing tobacco use and known high aspiration risk. Ambulatory saturation today >90%.
#Obstructive sleep apnea
Patient has severe sleep apnea based on last sleep study. We will continue to encourage and discuss use of CPAP.
#Tobacco use disorder
Patient with ongoing tobacco use, 5-6 cigarettes daily. Patient appreciates contribution to lung health but is not confident in ability to abstain. He has been referred for smoking cessation in the past. At this time, he declined nicotine replacement or other smoking cessation therapy.