
From Small to Large
Discoid
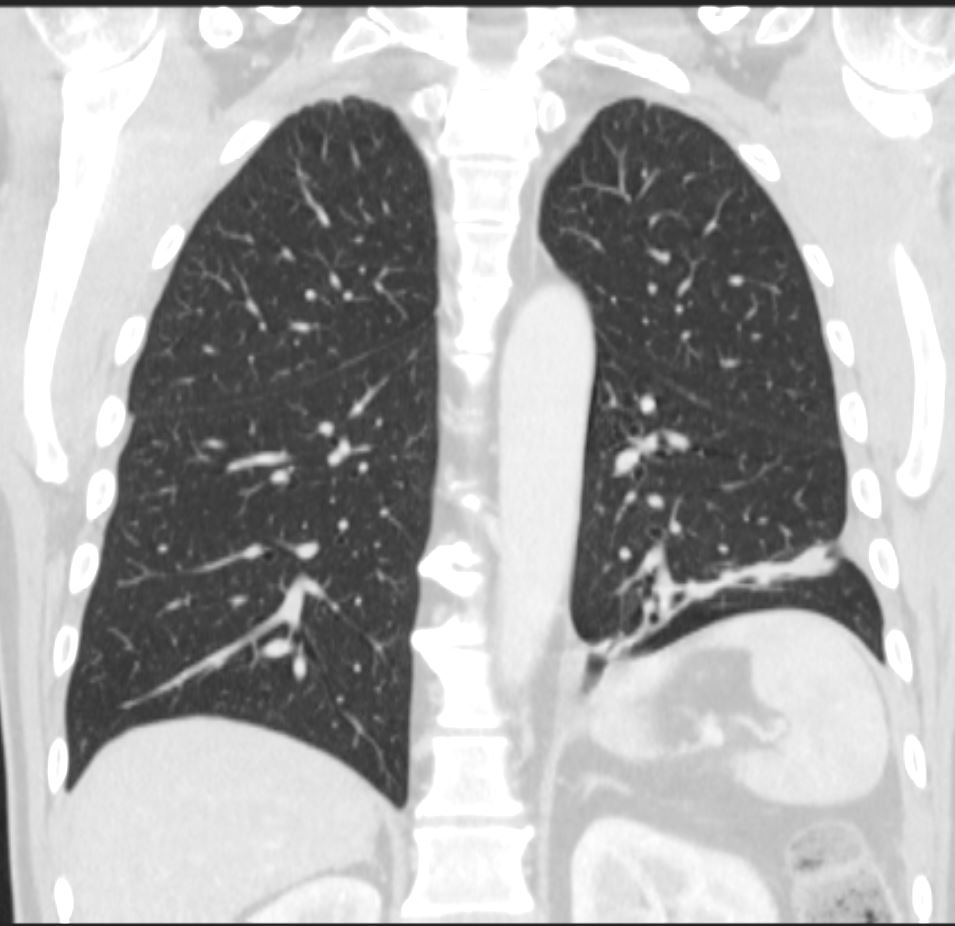
CT scan in the coronal plane 3 months later shows significant improvement of the atelectasis involving a basal segment of the left lower lobe associated with persistent elevation of the left hemidiaphragm indicating volume loss. The atelectasis now has a discoid, linear, or plate-like appearance
Ashley Davidoff MD TheCommonVein.net 276Lu 136238
aka discoid atelectasis aka plate-like atelectasis
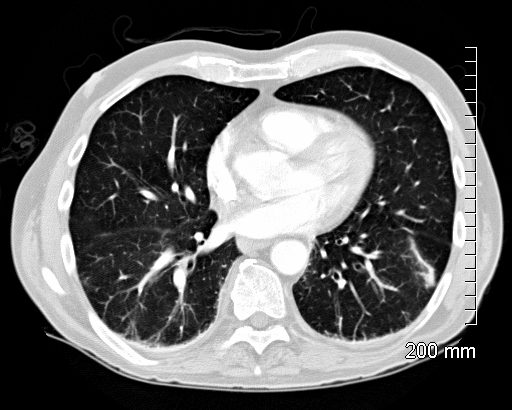
66 year old male with linear (discoid) atelectasis in the left lower lobe on CT
Ashley Davidoff MD TheCommonVein.net

60 year old male with linear (discoid) atelectasis in the middle lobe and the left upper lobe on CT. Note moderate sized bilateral pleural effusion. Minor compressive atelectasis caused by the left effusion.
Ashley Davidoff MD TheCommonVein.net
66 year old male with linear (discoid) atelectasis in the left lower lobe on CT
Ashley Davidoff MD TheCommonVein.net
Segmental Subsegmental
Subsegmental Obstruction of the
Apical Segment of the Right Upper Lobe
Carcinoid Tumor Causing Obstruction
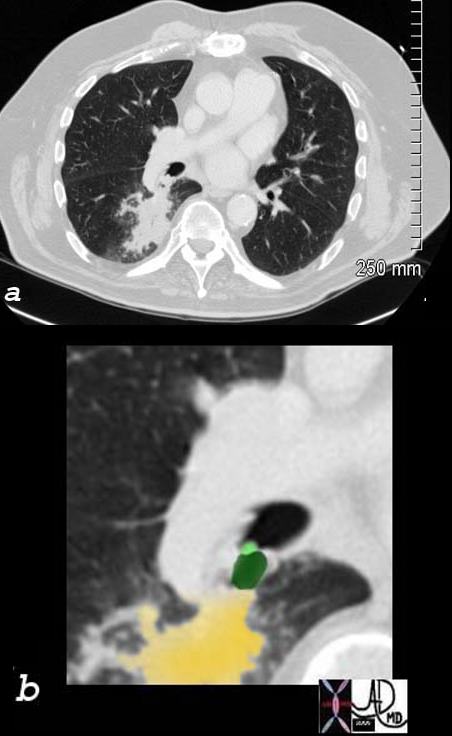
65 year old female presents with a cough. CT shows a mass (green) in proximal portion of the right lower lobe bronchus with post obstructive atelectasis in the superior segment of the right lower lobe (yellow) pathology revealed carcinoid tumor
Ashley Davidoff MD TheCommonVein.net
75679c02
Right Middle Lobe Lateral Segment
Sub Segmental Atelectasis

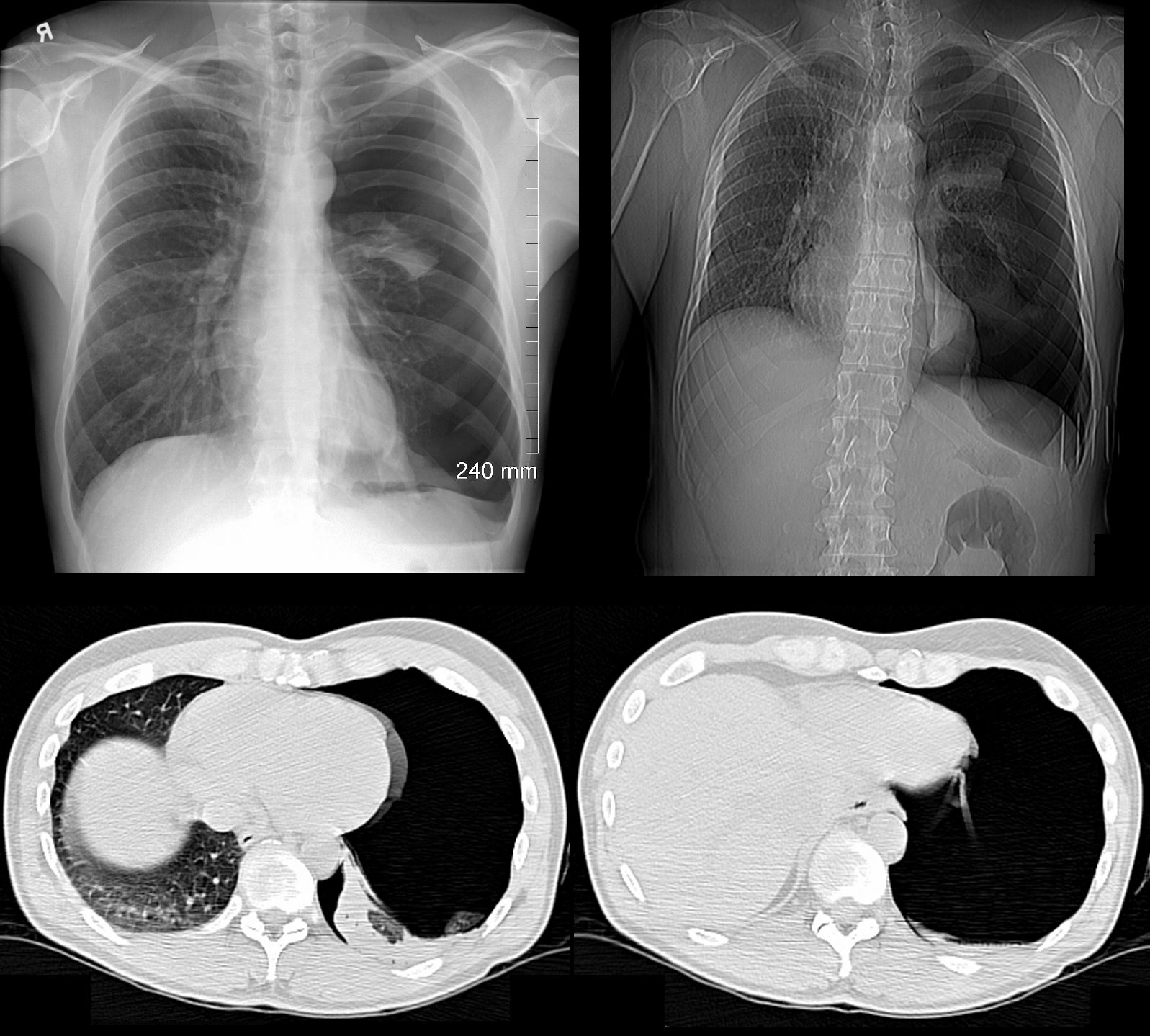
CT Allergic Bronchopulmonary Aspergillosis (ABPA)
48 year old female with a history of asthma presents with productive cough. CT scan 18 months prior confirms atelectasis in the middle lobe (upper panel and right lower panel) . There is diffuse mild multicentric foci of bronchial wall thickening in the segmental and subsegmental airways of the middle lobe, lingula and the lower lobes bilaterally (upper panel magnified in lower 3 panels).
Ashley Davidoff MD TheCommonVein.net
Compressive Normal Structures

68 year old male with a cough.
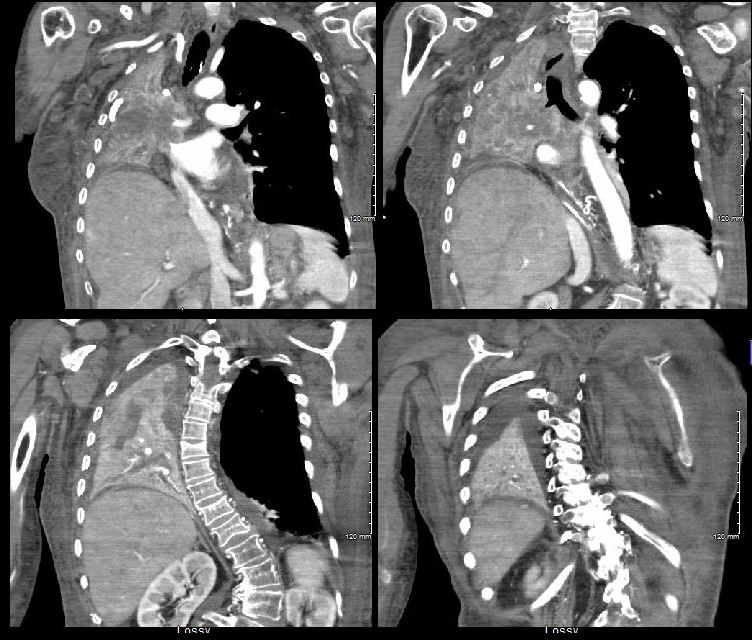
CT shows Compressive Atelectasis alongside the pulsating aorta
Ashley Davidoff MD TheCommonVein.net
37493
Lobar Collapse
Right Upper Lobe Collapse
Squamous Cell Causing
Obstruction but Airways Filled with
Tumor or Infection or Mucus

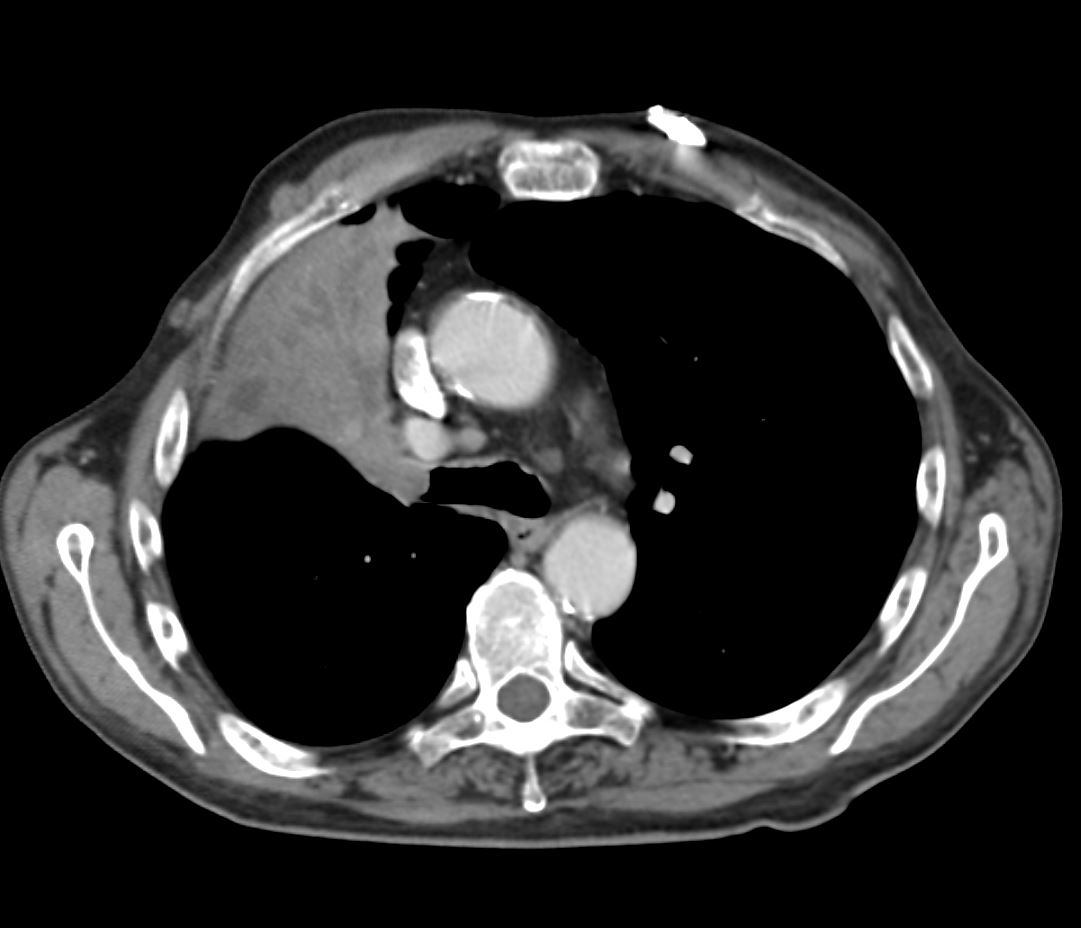
55-year-old male presenting with dyspnea
Axial CT at the level of the carina shows atelectasis of the RUL caused by a central obstructing lesion in the right upper lobe bronchus (b, white arrowhead) resulting in atelectasis of the RUL characterized by a wedge-shaped consolidation of the anteriorly positioned right upper lobe. The major fissure is displaced anteriorly (a, pink arrowhead). There is extensive filling of the distal bronchiectatic segmental and subsegmental airways of the RUL (b, yellow arrowheads). Final diagnosis was a central RUL proximal squamous cell carcinoma.
Ashley Davidoff TheCommonVein.net 212Lu 136432cL

55-year-old male presenting with dyspnea
Coronal CT at the level of the trachea and mainstem bronchi, shows atelectasis of the RUL caused by a central obstructing lesion in the right upper lobe bronchus resulting in atelectasis of the RUL characterized by a wedge-shaped consolidation of the right upper lobe with superiorly displaced major fissure. There is extensive filling of the distal bronchiectatic segmental and subsegmental airways of the RUL. Final diagnosis was a central RUL proximal squamous cell carcinoma.
Ashley Davidoff TheCommonVein.net 212Lu 136433

Endoscopic image of a central squamous cell carcinoma (SCC) with extensive
Ashley Davidoff TheCommonVein.net 212Lu 136434
{kind=link}

CXR shows right upper lobe (RUL) atelectasis. Final diagnosis was a central RUL proximal squamous cell carcinoma with extensive filling of the distal bronchi-ectatic segmental and subsegmental airways
Ashley Davidoff TheCommonVein.net

CXR shows right upper lobe (RUL) atelectasis. Final diagnosis was a central RUL proximal squamous cell carcinoma with extensive filling of the distal bronchi-ectatic segmental and subsegmental airways
Ashley Davidoff TheCommonVein.net
Ashley Davidoff TheCommonVein.net
Ashley Davidoff TheCommonVein.net

Ashley Davidoff TheCommonVein.net
Lobar Collapse
Right Upper Lobe Collapse
Occluded Right Main Stem Bronchus by Carcinoma with Pathology Correlation
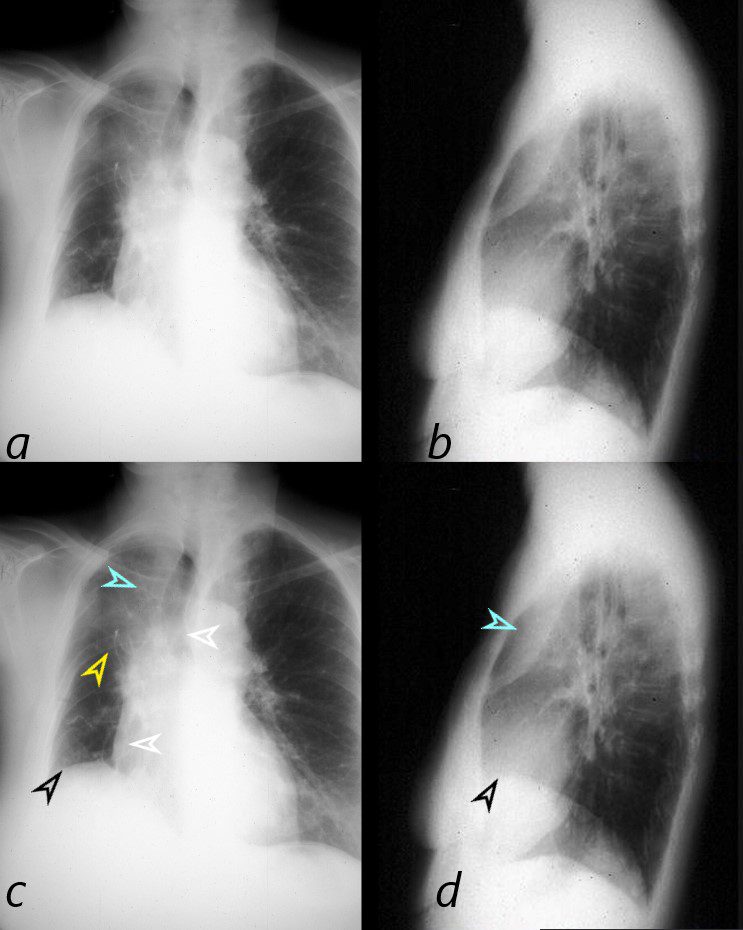
This combination of images shows the manifestations of a malignant mass in the hilum causing compression of the right mainstem bronchus. The PA CXR shows signs of volume loss (atelectasis characterized by elevation of the right hemidiaphragm (black arrowhead), rightward tracheal and mediastinal shift (white arrowheads) and elevation of the minor fissure contributing to the reverse S sign of Golden. There is a vague infiltrate in the right upper lobe correlating with an anterior pie shaped density of the lateral (blue arrowheads), consistent with collapse of the anterior segment of the RUL
32292cL01
Ashley Davidoff MD TheCommonVein.net
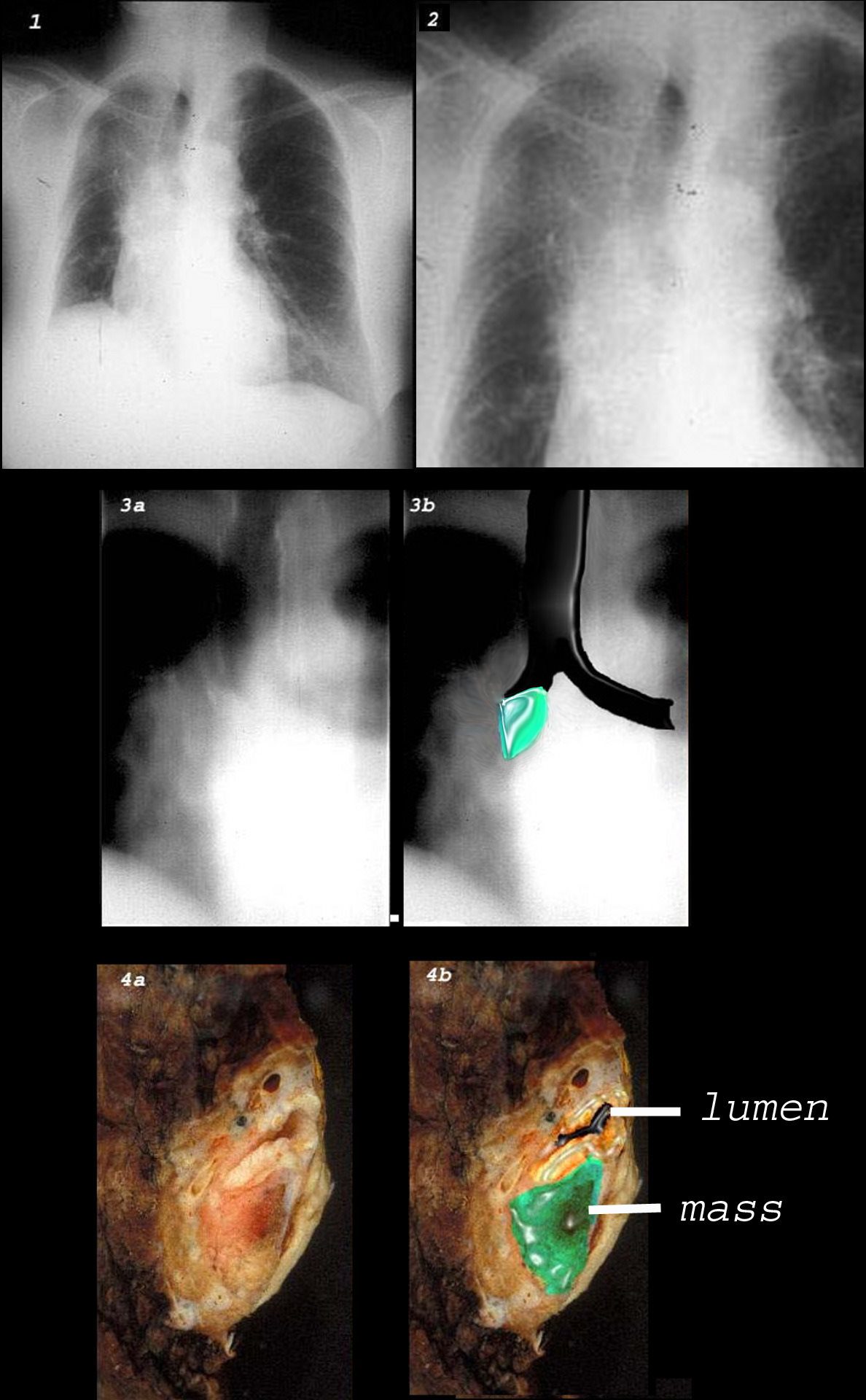
This combination of images shows the manifestations of a malignant mass in the hilum causing compression of the right mainstem bronchus. There is elevation of the right hilum on the CXR, associated with collapse of the anterior segment of the RUL seen as a vague density in the P-A . The tomogram (3a) shows an abrupt cut off of the right mainstem bronchus while the overlay in 3b shows the occlusion of the right mainstem bronchus, the implied tumor overlaid in green. Images 4a and 4b are the correlative gross pathology images showing the tumor in green pushing and occluding the right mainstem
Ashley Davidoff MD TheCommonVein.net
Tracheal Deviation and Soft Tissue Density at the Right Apex
TB with Chronic Right Upper Lobe Atelectasis
{kind=link}
Ashley Davidoff MD TheCommonVein.net
{kind=link}
 TB with Chronic Right Upper Lobe Atelectasis
TB with Chronic Right Upper Lobe AtelectasisAshley Davidoff MD TheCommonVein.net
{kind=link}
 TB with Chronic Right Upper Lobe Atelectasis
TB with Chronic Right Upper Lobe AtelectasisAshley Davidoff MD TheCommonVein.net
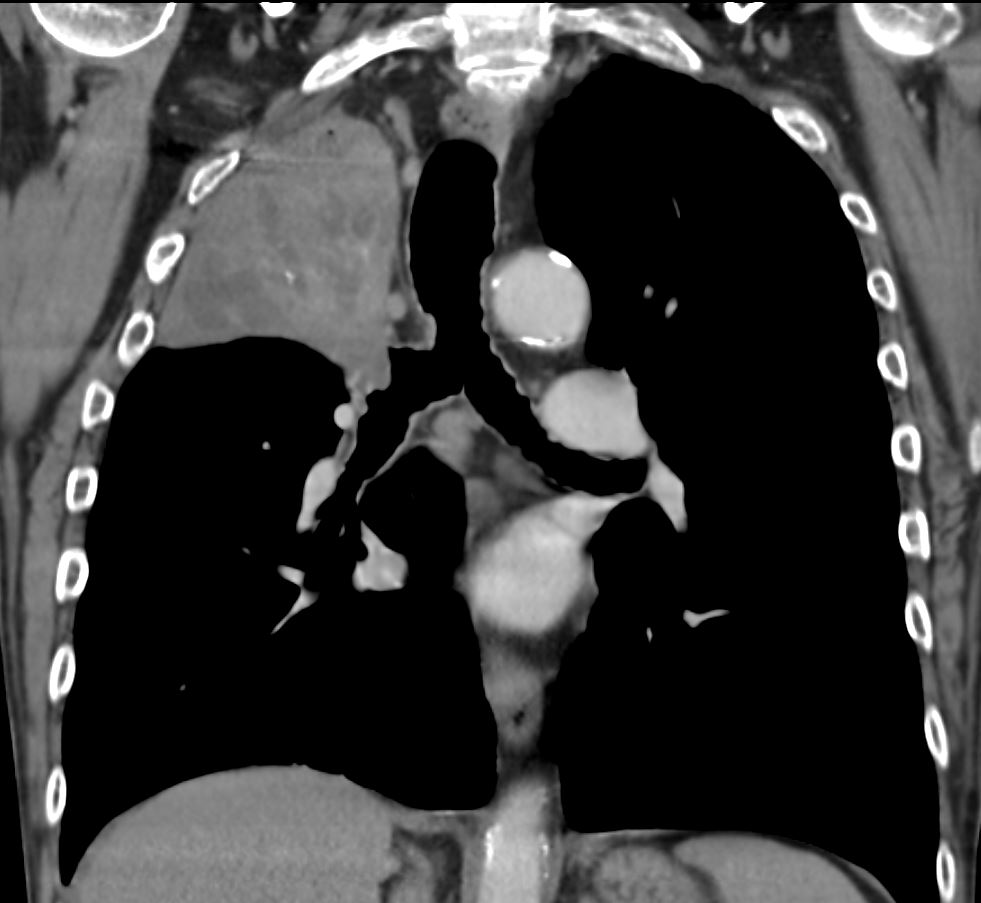
Left Upper Lobe Collapse and Luftsichel Sign

Left Upper Lobe Atelectasis
Female patient with central squamous cell carcinoma of the lung with left upper lobe collapse and hyperinflation of the left lower lobe resulting in a Luftsichel sign
Ashley Davidoff MD TheCommonVein.net 152Lu

Left Upper Lobe Atelectasis
Female patient with central squamous cell carcinoma of the lung with left upper lobe collapse and hyperinflation of the left lower lobe resulting in a Luftsichel sign
Ashley Davidoff MD TheCommonVein.net 152Lu
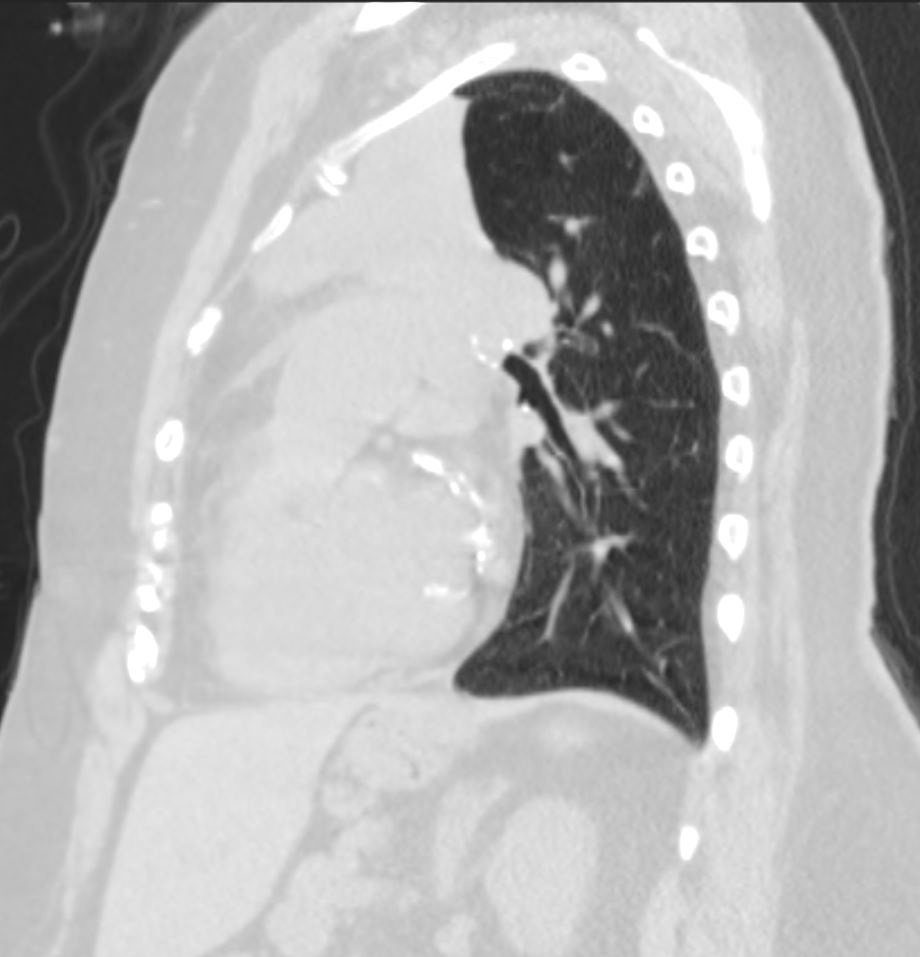
Left Upper Lobe Atelectasis
Female patient with central squamous cell carcinoma of the lung with left upper lobe collapse with atelectatic lung collapsed anteriorly
Ashley Davidoff MD TheCommonVein.net 152Lu

Left Upper Lobe Atelectasis
Female patient with central squamous cell carcinoma of the lung with left upper lobe collapse and hyperinflation of the left lower lobe resulting in a Luftsichel sign.
The left lung is relatively lucent as a result of hyperinflation . The atelectatic left upper lobe manifests as an anterior soft tissue density along the anterior mediastinum.
Ashley Davidoff MD TheCommonVein.net 152Lu
Ashley Davidoff MD TheCommonVein.net

Ashley Davidoff MD TheCommonVein.net

Ashley Davidoff MD TheCommonVein.net
Central Cancer Causing Left Upper Lobe Collapse
{kind=link}

69year old male presents with a cough and weight loss
A PA CXR left upper lobe atelectasis and a Luftsichel sign characterised by a consolidation along the left superior mediastinum with sigmoid shaped interposed air from the hyperinflated left lower lobe. There is elevation of the left hemidiaphragm secondary to the volume loss
Ashley Davidoff MD TheCommonVein.net
69M cancer LUL collapse Luftsischel sign 001
{kind=link}
69M-cancer-LUL-collapse-Luftsischel-sign-003.jpg
69year old male presents with a cough and weight loss
The axial CT scan shows a central low density mass causing collapse of the left upper lobe positioned anteriorly with the major fissure also displaced anteriorly by the hyperinflated lower lobe
Ashley Davidoff MD TheCommonVein.net
69M cancer LUL collapse Luftsischel sign 003
Bilateral Lower Lobar Atelectasis with
Occlusion of the Right Main Stem Bronchus

74 year old male alcoholic with bilateral basilar lobar atelectasis caused by bilateral aspiration
CT scan shows airless lower lobes with small bilateral effusions. 3D reconstruction shows total obstruction of the right mainstem bronchus, and patent proximal mainstem bronchus
Ashley Davidoff MD TheCommonVein.net
Left Lower Lobe Collapse ,
Partial Left Upper and Right Lower Collapse

88 year old male with bilateral effusions shown on the CXR. Axial CT shows thickened pleura on the left with compressive atelectasis of the lower lobe and a smaller region of crescentic compressive atelectasis on the right. 3D reconstruction shows atelectasis of the left lower lobe and portion of the lingula. The left effusion is complex.
Ashley Davidoff MD TheCommonVein.net
Normal vs Lobar Atelectasis

3D reconstruction of a normal patient (above) and of a patient with compressive atelectasis (below) The image below is from an 88 year old male with bilateral complex effusions with compressive atelectasis of the lower lobe and portion of the lingula
Ashley Davidoff MD TheCommonVein.net
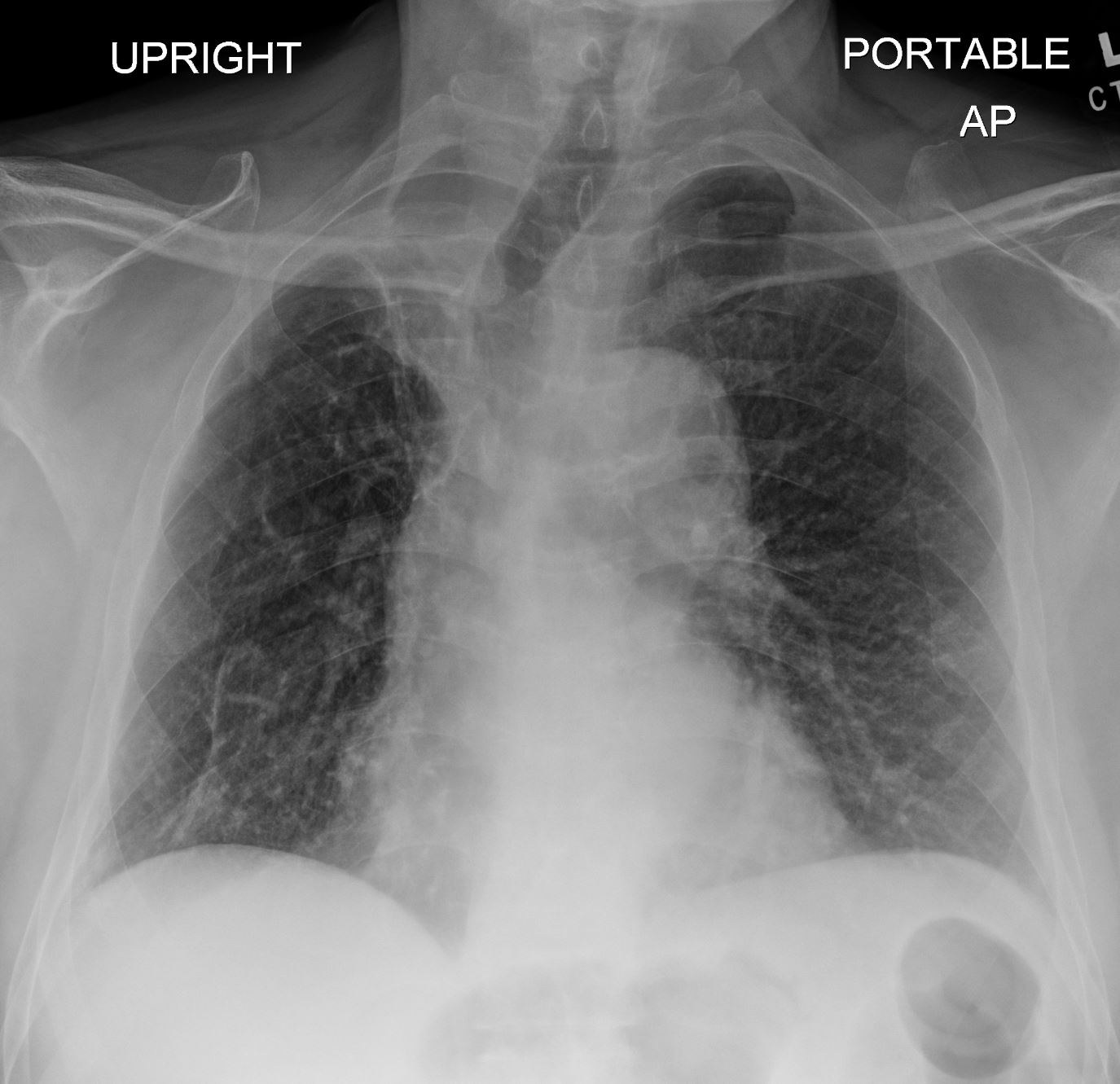
Total Lung Collapse
Total Left Lung Collapse
Tension Pneumothorax

Ashley Davidoff MD TheCommonVein.net
77949
49 year old male with a cough presents for a Chest Xray which showed a tension pneumothorax. Chest tube was placed emergently in the radiology department.
Ashley Davidoff MD TheCommonVein.net
117300c
Total Right Lung Collapse
Tension Hydrothorax

from large pleural effusion and probable hemothorax under tension with atelectasis of the right lung
85-year-old female with a history of lung cancer, presents with dyspnea and hypotension. CXR shows white out of the right hemithorax with pressure effect characterised by narrowing of the distal trachea cardio-mediastinal shift to the left and atelectasis in the left lower lobe.
Ashley Davidoff MD TheCommonVein.netSee 106Lu 118468
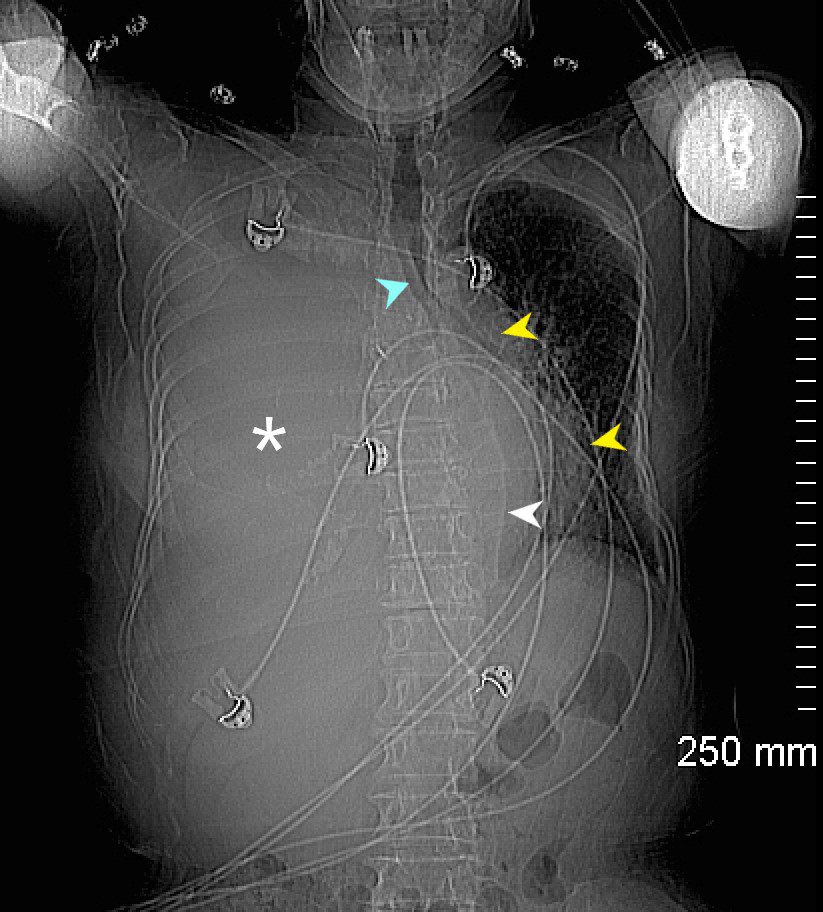
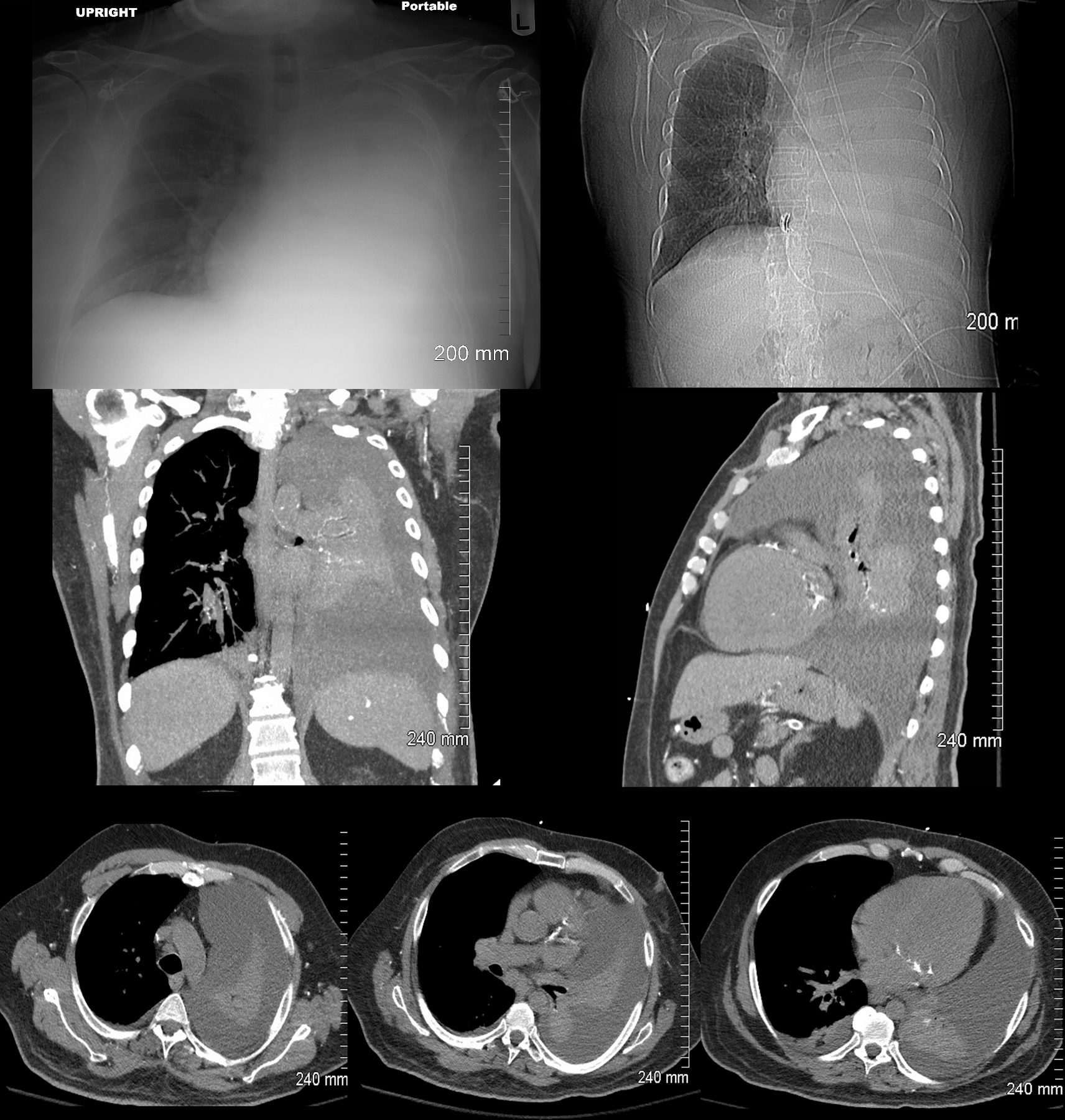
85-year-old female with a history of lung cancer, presents with a dyspnea and hypotension. Scout film prior to the CT scan shows ?white out? of the right hemithorax (white asterisk) with pressure effect characterised by narrowing of the trachea (blue arrow) mediastinal shift yellow arrows) and herniation into the left chest characterised by a leftward shift of the azygo-esophageal junction line (white arrow).
Ashley Davidoff MD TheCommonVein.ne 106Lu 118463L
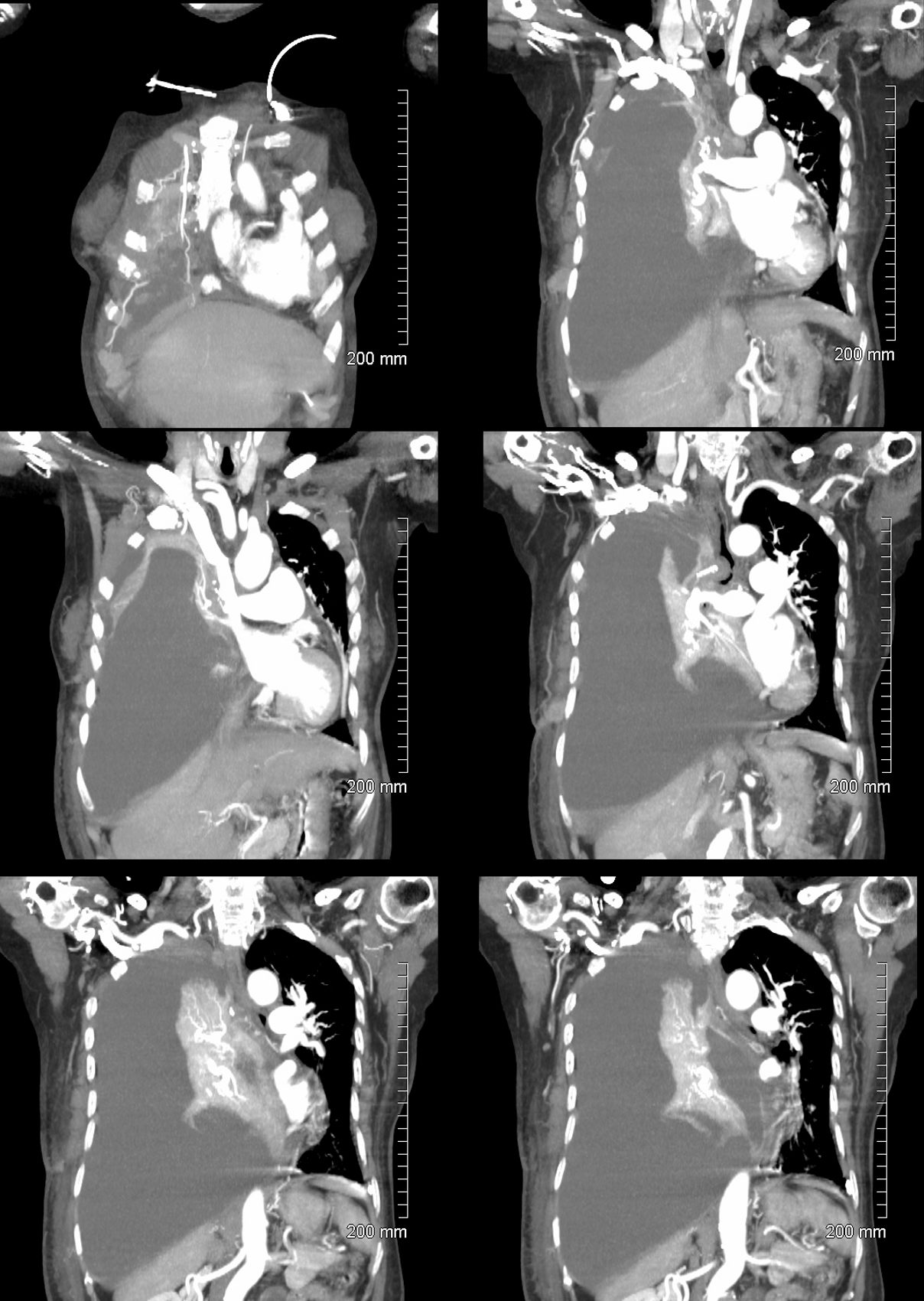
85-year-old female with a history of lung cancer, presents with a dyspnea and hypotension. CT scan shows a large right pleural effusion under pressure, with mediastinal shift to the right. In addition, there is compression of the heart with back up of venous return due the pressure effect on the heart and vascular structures. Among the structures showing venous distension are the SVC (blue arrowhead,a) right sided upper limb veins (blue arrowhead b) and the left upper pulmonary veins (red arrowhead, b. The effusion in the right pleural cavity with atelectatic lung herniates into the left hemithorax, (white arrowhead, c). There is a dense sediment in the pleural fluid (red arrowhead, d) suggesting blood in the pleural cavity. The left atrium is compressed (maroon arrowhead, d)
Ashley Davidoff MD TheCommonVein.net106Lu 118467c
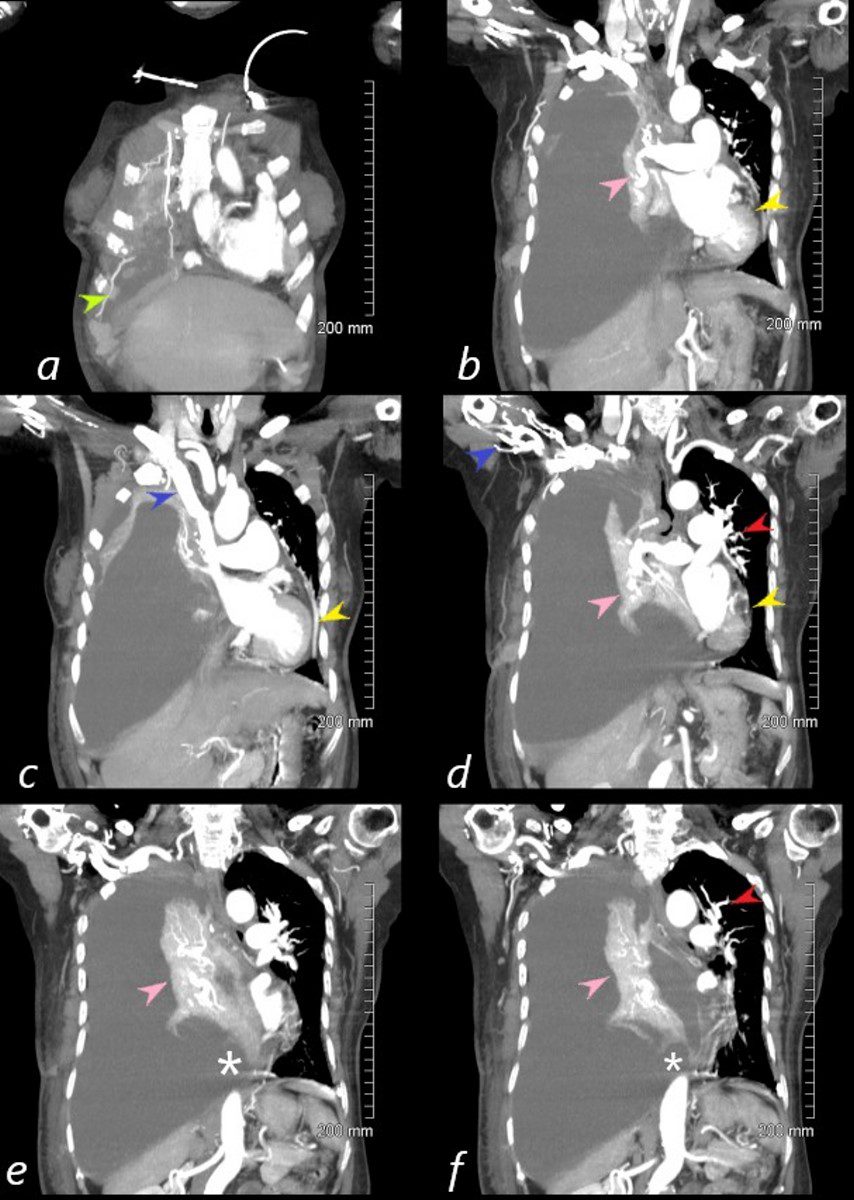
85-year-old female with a history of lung cancer, presents with a dyspnea and hypotension. Reconstruction of the CT scan in the coronal plane, shows a large right pleural effusion under pressure with herniation into the left chest (white asterisk e,and f) , with mediastinal shift to the left (yellow arrowhead b, c, d). In addition, there is compression of the heart with back up of venous return due the pressure effect on the heart and vascular structures. Among the structures showing venous distension are the SVC (blue arrowhead, c) right sided upper limb veins (blue arrowhead d) and the left upper pulmonary veins (red arrowhead, d and f). The density of the systemic venous abd arterial systems is similar, but vascular structures as noted by the green arrowhead in a could represent venous collaterals.
Ashley Davidoff MD TheCommonVein.ne 106Lu 118467cL
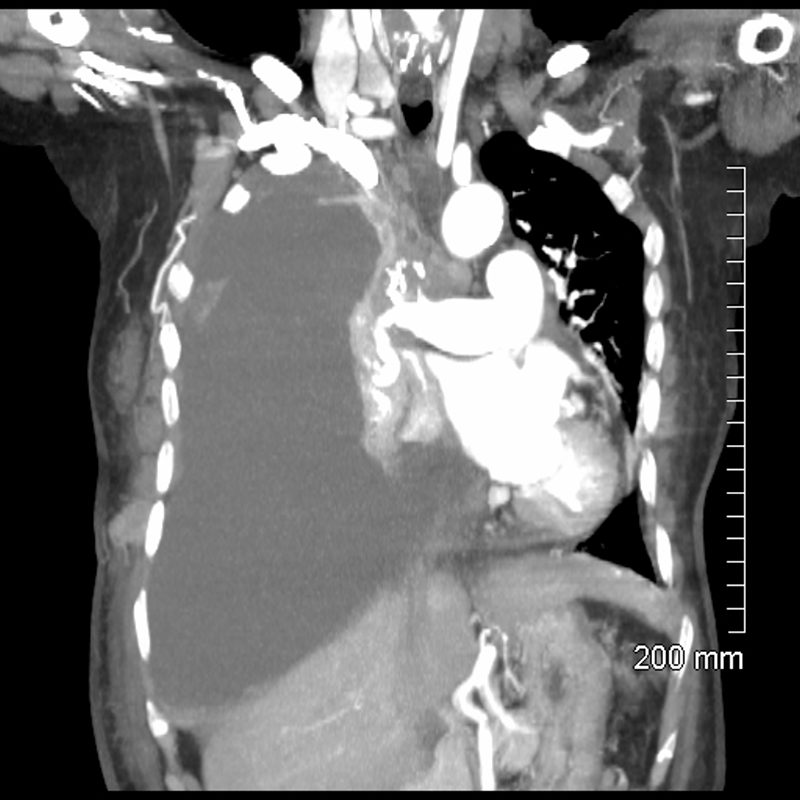
85-year-old female with a history of lung cancer, presents with a dyspnea and hypotension. CT scan shows a large right pleural effusion under pressure, with mediastinal shift to the left. In addition, there is compression of the heart with back up of venous return due the pressure effect on the heart and vascular structures. The effusion in the right pleural cavity with atelectatic lung herniates into the left hemithorax.
Ashley Davidoff MD TheCommonVein.net 106Lu 118467
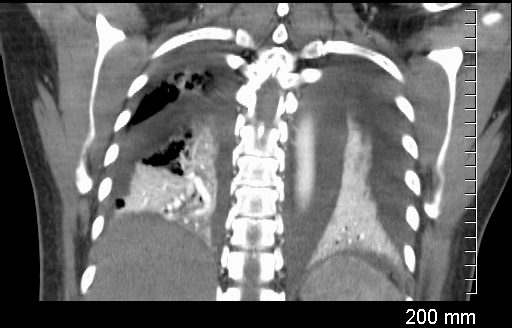
Coronal CT through the lungs show bilateral pleural effusions with compressive atelectasis
Ashley Davidoff MD TheCommonvein.net
238Lu

Compressive Atelectasis and Complex Pleural Effusions
Sagittal CT through the left lung shows undulations of the posterior surface of the left lung, and the suggesting differing pressures on the lung parenchyma by the effusions and indicating complexity and loculation.
Ashley Davidoff MD TheCommonVein.net
238Lu
Whole Lung Atelectasis Due to Obstruction
{kind=link}
59-F-total-atelectasis-001-1.jpg
Occluded Main Stem Bronchus, Atelectasis of the Right Lung, and Pleural Effusion59F shows total white out caused by collapse of right lung with an
occluded right main step bronchus associated with a
large right sided effusion. The occlusion is likely due to proximal cancer. A pigtail drain has been placed to drain the effusion
Ashley Davidoff MD TheCommonVein.net 104 Lu
59F shows total collapse of left lung with an
occluded right main step bronchus(top right image)associated with a
right sided effusion. The occlusion is likely due to proximal cancer
Ashley Davidoff MD TheCommonVein.net 104 Lu
Total Lung Compressive Atelectasis
Effusion
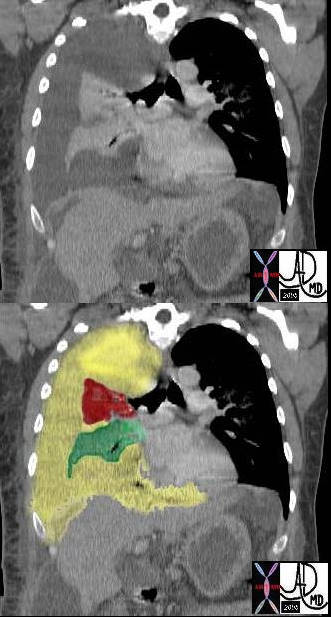
In this case there a large right sided pleural effusion (yellow) with secondary atelectasis of the right lung. (red and green) This coronal CT of the chest at the level of the left ventricle shows a large right pleural effusion which lies between the visceral and parietal pleura. Once the effusion is large enough to weaken the capillary forces that hold the parietal and visceral pleura together, it fail, and the lung collapses which is what is noted on this image ? ie total lung collapse because of loss of cohesive adhesive forces.
Courtesy of: Ashley Davidoff, M.D. TheCommonvein.net 42558c
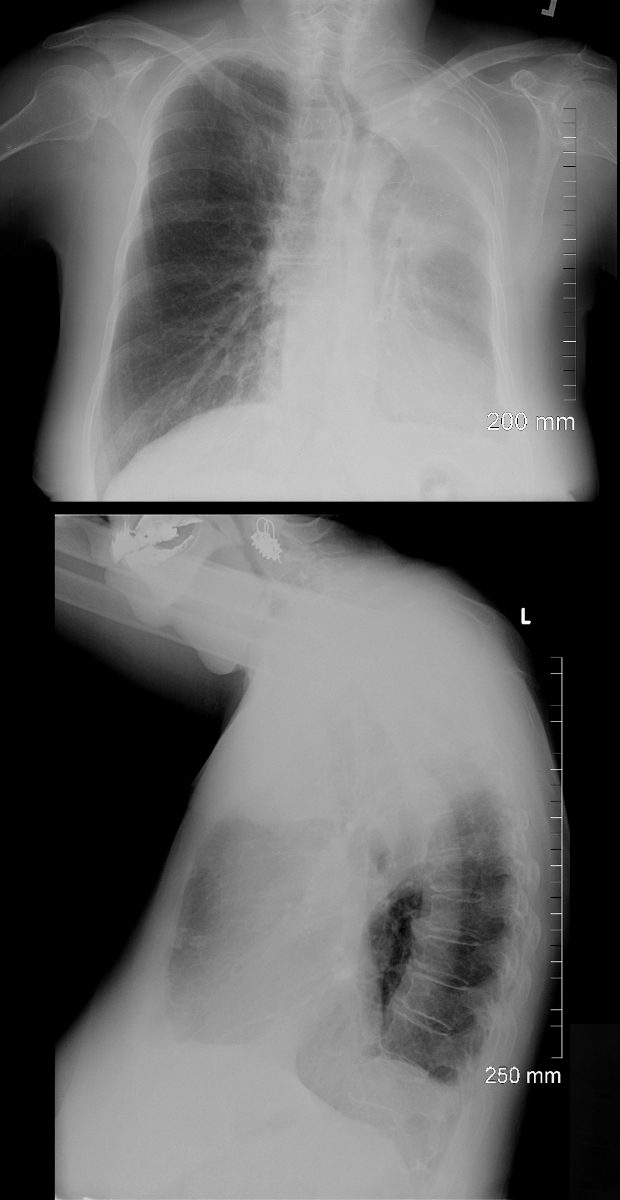
White Out of the CXR with Passive Compressive Atelectasis of the Left Lung
48 year-old male presents with a dyspnea. CXR shows a total white out of the left chest with pulmonary congestion. CT scan shows a large left pleural effusion with total atelectasis of the left lung. Incidental note is made of premature calcific coronary artery disease.
Ashley Davidoff MD TheCommonVein.net
Small Cell Lung Carcinoma p/w with a “White Out”

62-year-old female presents with acute dyspnea and chest pain
Frontal CXR shows a “white out” of the left hemithorax. The left hemidiaphragm is elevated and there is leftward mediastinal shift indicating volume loss
She was subsequently diagnosed with a small cell lung carcinoma that was obstructing the left main stem bronchus
Ashley Davidoff MD TheCommonVein.net 298Lu 136700
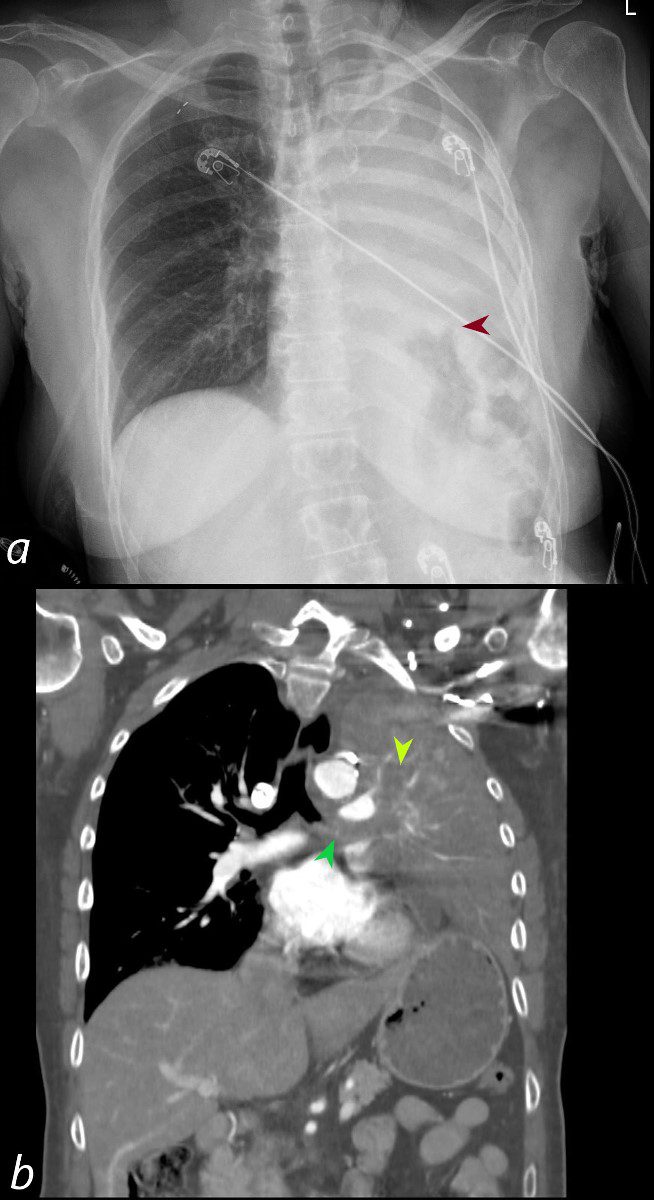
62-year-old female presents with acute dyspnea and chest pain
Frontal CXR shows a “white out” of the left hemithorax. The left hemidiaphragm is elevated (maroon arrowhead) and there is leftward mediastinal shift indicating volume loss.
Coronal CT confirms the presence of an obstructing lesion in the left mainstem bronchus,(b, dark green arrowhead), with extension of the soft tissue into an upper lobe bronchus (b light green arrowhead). There is total collapse of the left lung and an elevated left hemidiaphragm
Subsequent pathological diagnosis of small cell lung carcinoma was established
Ashley Davidoff MD TheCommonVein.net 298Lu 136702

62-year-old female presents with acute dyspnea and chest pain
Coronal CT confirms the presence of an obstructing lesion in the left mainstem bronchus, (dark green arrowhead, a), with extension of the soft tissue into bronchiectatic upper lobe bronchi (light green arrowheads b, c, d) There is total collapse of the left lung.
Subsequent pathological diagnosis of small cell lung carcinoma was established
Ashley Davidoff MD TheCommonVein.net 298Lu 136704