
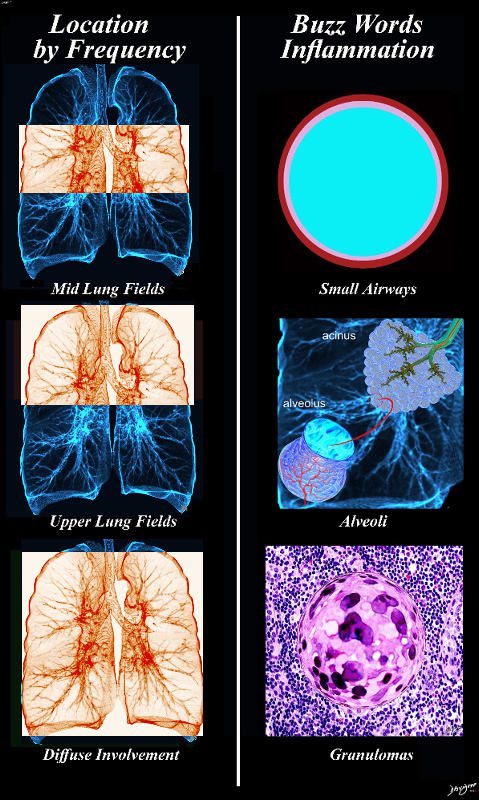
Hypersensitivity – aka (extrinsic allergic alveolitis)
Ashley Davidoff MD TheCommonvein.net lungs-0732b01
-
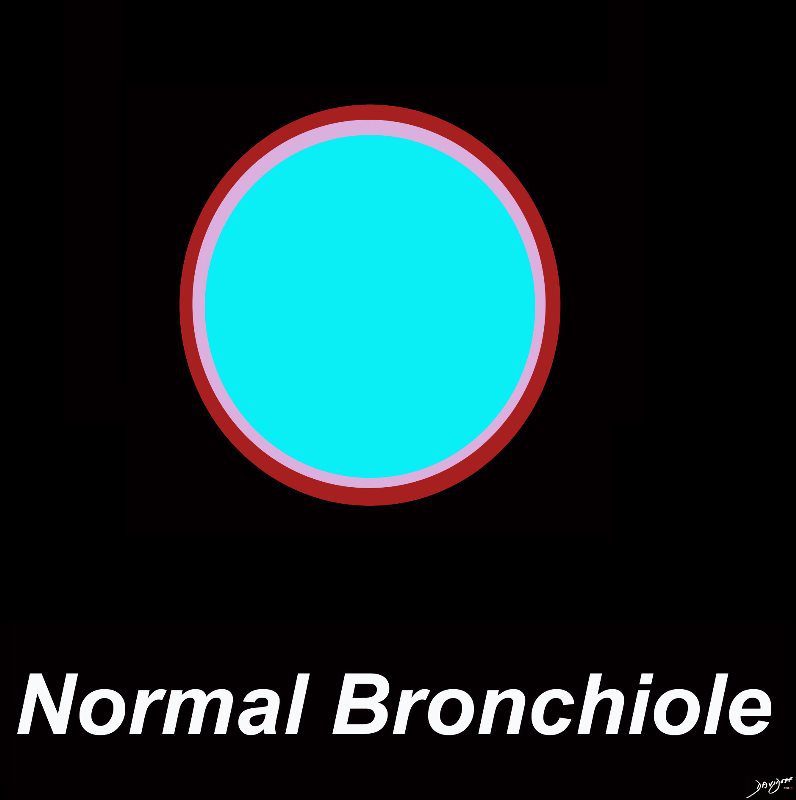
A normal bronchiole usually 1mm or less in diameter. The wall consists of ciliated cuboidal epithelium and a layer of smooth muscle. Bronchioles divide into even smaller bronchioles, called terminal bronchioles, which are 0.5 mm or less in diameter and are primarily lined by club cells, and accompanied by a small number of ciliated cuboidal cells.. Respiratory bronchioles are the final division of the bronchioles within the lung and they are .5mm or less in diameter and contain a simple non ciliated cuboidal epithelium and a thin layer of smooth muscle
Ashley Davidoff MD TheCommonVein.net lungs-0721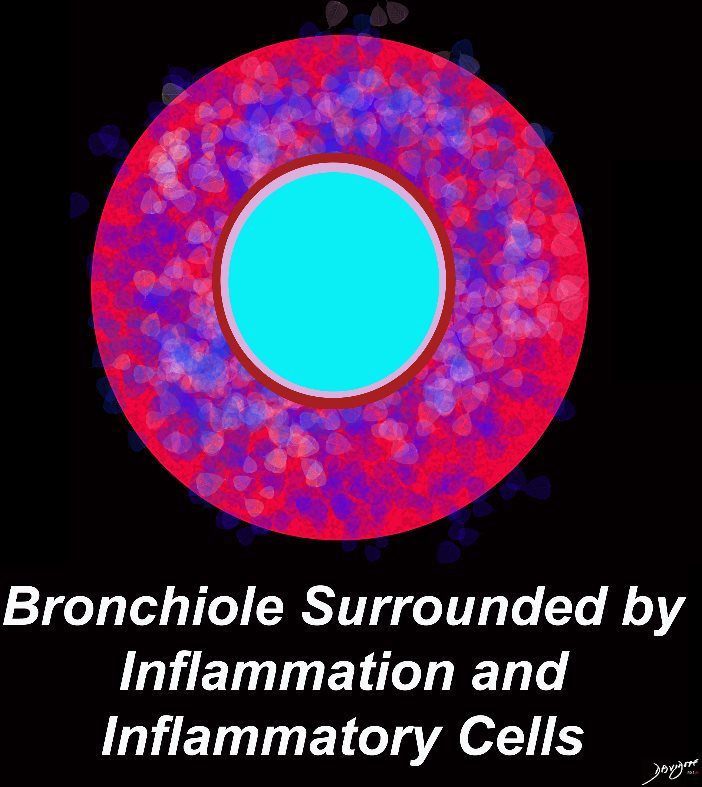
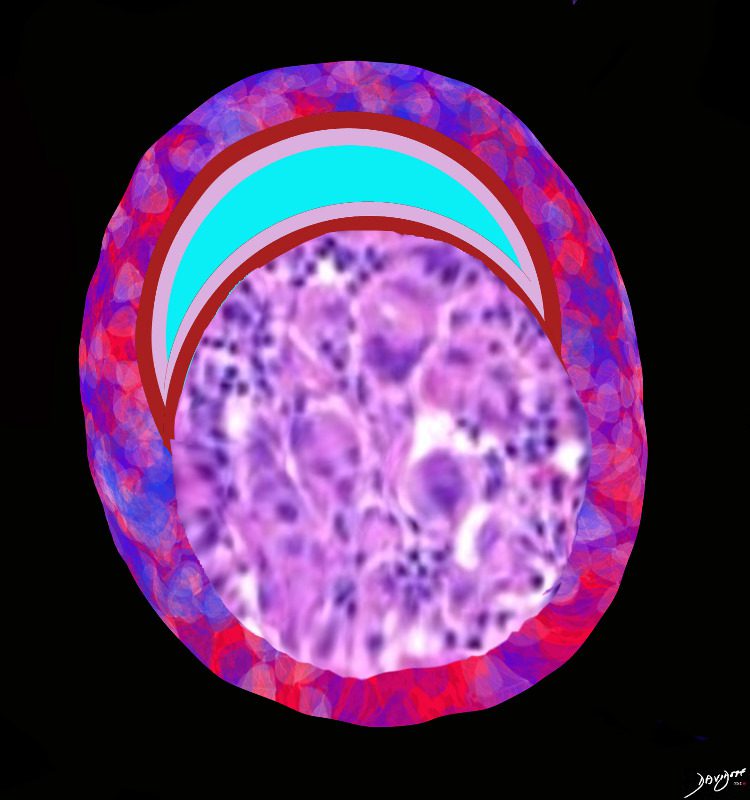
Smoking excites the Langerhans cell which in turn induces and attracts early cellular interstitial infiltrates which surround the bronchiole. The diagram shows a bronchiole surrounded by an acute cellular inflammatory response
Ashley Davidoff MD TheCommonVein.net lungs-0722=
- Alveolitis
- Cellular Bronchiolitis
- Granulomas
- acute, subacute, and chronic/fibrotic
- Immune reaction – inflammation to an
- allergen
- protein
- microbe
- animal protein
- plant protein
- hapten = low molecular wt protein combining with host protein becomes immunogenic
- Smoking
- 95% of pts with HP are non smokers
- 5% smokers with HP have a high mortality
- protein
- Pneumonitis –
- Terminal bronchiole and alveoli
- Nutshell Buzz
- Airway Thickening
- Alveolitis
- Acute stage
-
-
- Diffuse Alveolar Damage
- Increased permeability
- Neutrophils
- neutrophillic exudate
- air space opacity
- GGO
- consolidation
- air space opacity
- Exudate
- Fill Alveoli
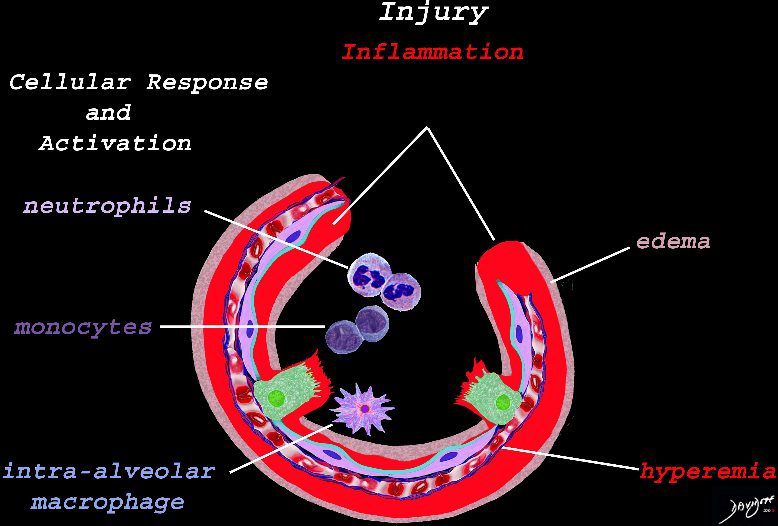
Early Events in the Pathophysiology of the ARDS
The initial injury results in an acute severe inflammatory response consisting hyperemia , edema with migration initially of neutrophils in the first 6-24 hours followed by monocytes (24-48hours). The intra -alveolar macrophages are activated.
Ashley Davidoff
TheCommonVein.net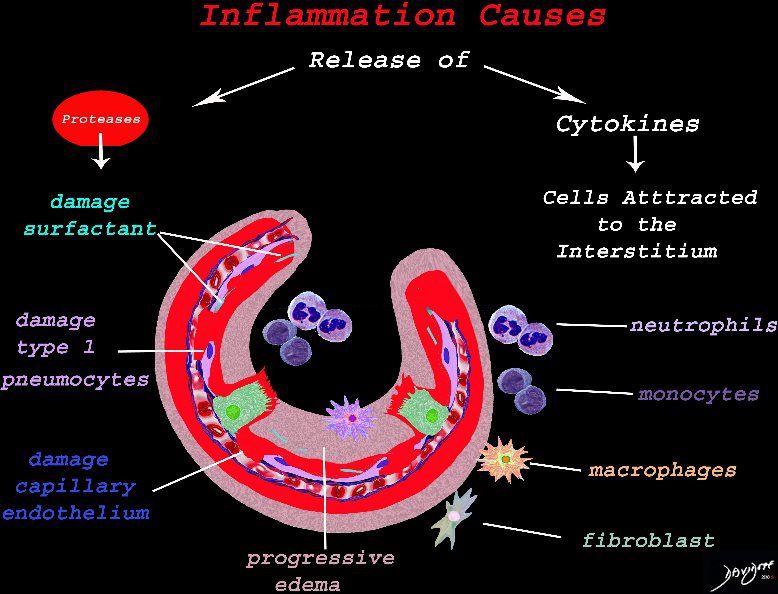
Result of Cellular Response
The cells of the immune system release cytokines, chemotactic agents and proteases. Immune cells , macrophages and fibroblasts are attracted to the interstitium. Some of proinflammatory agents are toxic to the cell lining causing damage to the surfactant, type 1 pneumocytes and the capillary endothelium. There is progressive edema.
Ashley Davidoff
TheCommonVein.net
Result of Cellular Response and Associated Tissue Injury
The damage to the endothelium of the capillary results in bleeding into the alveoli. The severe tissue damage and fluid exudation results in protein rich intra-alveolar fluid . The fibroblasts start to lay down collagen as part of the early repair process
Ashley Davidoff
TheCommonVein.net
Hyaline Membrane
A hyaline membrane evolves covering the damaged surface of the alveolus. This impedes gas exchange
Ashley Davidoff
TheCommonVein.net web-lungs-473.webp
Exudative Diffuse Alveolar Damage (DAD) in early ARDS. Comparison between ARDS and normal lung tissue demonstrates the presence of alveolar collapse, neutrophil infiltration, areas of microscopic hemorrhage, hyaline membrane formation and alveolar edema in ARDS. Histopathology images were adapted and reproduced under Creative Commons licenses: ARDS histopathology component by Nephron (Own work) [CC BY-SA 3.0 (http://creativecommons.org/licenses/by-sa/3.0) or GFDL (http://www.gnu.org/copyleft/fdl.html)], via Wikimedia Commons; and Normal lung alveoli component By Jpogi ?Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=46568489.
Acute exudative phase of diffuse alveolar damage with prominent hyaline membranes (DAD)
Courtesy Dr Yale RosenThe Fluid in the Alveoli Can Result in
- Fill Alveoli
- Diffuse Alveolar Damage
-
- Radiology
- GGO’s
- Consolidation
- Position
- bilateral
- midlung >upper lung >diffuse
- only lower lungs does not happen
- bilateral
- Shape
- Ill defined
- Patchy and or
- Nodular Infiltrates
- Position
-
Bird Fanciers Disease
Acute Hypersensitivity Pneumonitis
Upper and Mid Lung Field
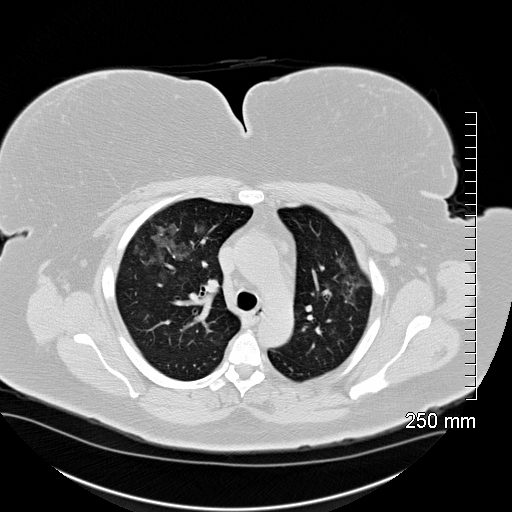
Acute Hypersensitivity Pneumonitis
54-year-old female who keeps parakeets present with mild dyspnea
Chest CT shows mild ground glass changes in the mid and upper lung fields consistent with acute hypersensitivity pneumonitis (HP)
Ashley Davidoff TheCommonVein.net 136571

Acute Hypersensitivity Pneumonitis
54-year-old female who keeps parakeets present with mild dyspnea
Chest CT shows mild ground glass changes in the mid and upper lung fields consistent with acute hypersensitivity pneumonitis (HP)
Ashley Davidoff TheCommonVein.net 136573
-
-
-
-
- Nodular
-

Aspiration Pneumonia Pulmonary Edema and DAD
54 year old male alcoholic with seizures presents with diffuse alveolar disease consistent with pulmonary edema (a). CT scan (b) shows bibasilar infiltrates consistent with aspiration.
Follow up CXR 6 months later (c) shows resolution
Ashley Davidoff MD TheCommonVein.net
-
-
-
-
Non Fibrotic = Subacute Phase
-
Structurally
- Small Airways
- Poorly Defined Ground Glass Nodules
- Alveoli – Alveolitis =
- Mosaic Attenuation
- Combined Small Airway and Alveoli
- 3 density sign = head cheese sign
- Small Airways
-
Disease
- Inflammation
- Cellular Infiltrate and Edema
- Around Bronchioles
- Bronchiolitis = Cellular Bronchiolitis
-
Smoking excites the Langerhans cell which in turn induces and attracts early cellular interstitial infiltrates which surround the bronchiole. The diagram shows a bronchiole surrounded by an acute cellular inflammatory response
Ashley Davidoff MD TheCommonVein.net lungs-0722
- Around Alveoli =
- Alveolitis –
-
lungs-0021catalogue-signed-smallb.jpg
Inflamed Alveoli
Ashley Davidoff MD TheCommonvein.net lungs-0021Inflammation in the Wall of the Alveoli = Interstitial Infiltrate

High magnification photomicrograph of a lung biopsy taken showing chronic hypersensitivity pneumonitis (H&E), showing mild expansion of the alveolar septa (interstitium) by lymphocytes.[clarification needed] A multinucleated giant cell, seen within the interstitium to the right of the picture halfway down, is an important clue to the correct diagnosis.
Courtesy Wikiwand web lungs 435
- Around Bronchioles
- Granulomas around the bronchiole or arteriole
- Impinging on the Lumen of a Centrilobular Bronchiole
-
Granuloma Impinges on the lumen of the centrilobular bronchiole The peri- bronchiole inflammation has receded in this subacute to chronic phase
Ashley Davidoff MD TheCommonVein.net lungs-0729- Granulomas around the bronchiole or arteriole
- Occluding the Lumen of a Centrilobular Bronchiole

Granuloma occludes the lumen of the centrilobular bronchiole and the peri-bronchiole inflammation has receded in this subacute to chronic phase
Ashley Davidoff MD TheCommonVein.net lungs-0731
- Cellular Infiltrate and Edema
- Inflammation
-
-
Diagnosis
- Mid Lung Fields> Upper Lung Fields > Diffuse
- Bronchiolitis
- Alveolitis
- GGO
- Patchy
- GGO
- Granulomas
- Nodules
- GGO
- reticlonodular
- Reticulation
- Ground Glass
- Heterogeneous
- Lobular sparing air trapping mosaic attenuation
- Head Cheese Sign
-

{kind=link}
{kind=link}
{kind=link}

Courtesy Rainer Zenz source Wiki
Structural focus
Ashley Davidoff MD TheCommonVein.net lungs-0721
Normal Small Airways
The Duct, and the Artery
The pulmonary arteriole accompanies the airway as it carries oxygen from the trachea to the alveoli. They part ways at the alveoli where the pulmonary venule then takes the oxygenated blood from capillary network around the alveoli back to the left atrium.
The intimate relationship of the airways and the pulmonary artery and their close approximation in size, is helpful in radiology, firstly to identify theese structures and secondly to define disease such as heart failure and bronchiectasis.
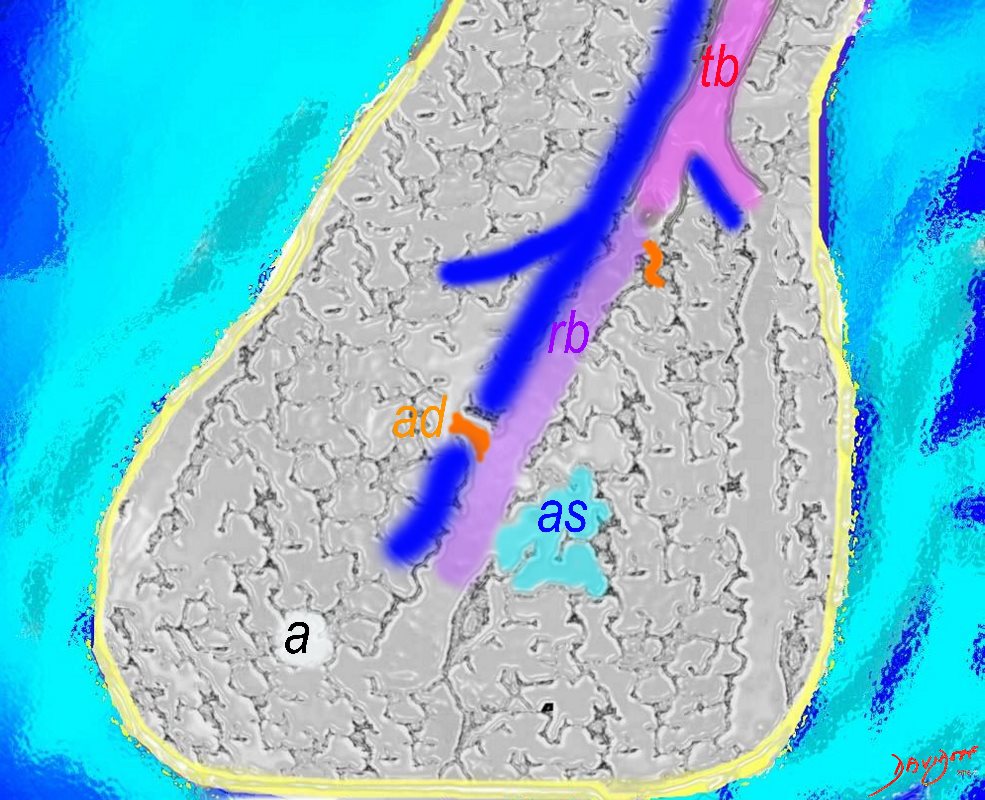
The acinus as shown in this image is defined as a unit of lung consisting of a single first order respiratory bronchiole that subtending a cluster of alveoli reminiscent of a bunch of grapes or berries (acinus in Latin means berry) . The lobular bronchiole (lb) branches into the terminal bronchiole (tb), which then branches into the first order respiratory bronchiole (rb). Subsequent branching after the respiratory bronchiole, includes in order, the alveolar duct (ad), alveolar sac (as), and then finally the berry like alveoli.
Courtesy Ashley Davidoff 2019
lungs-0033-low res
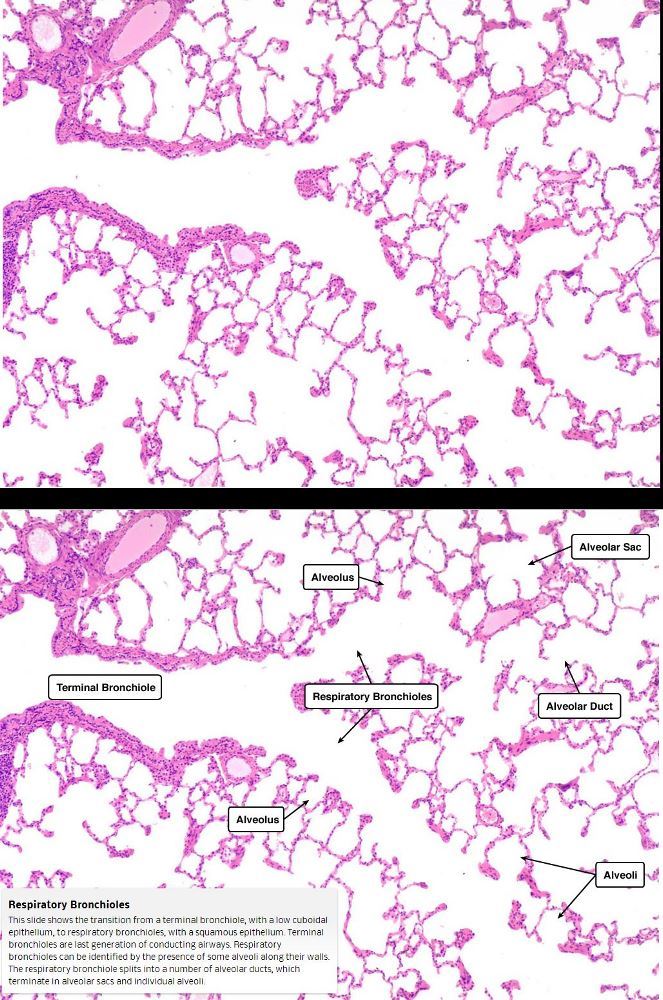
This slide shows the transition from a terminal bronchiole, with a low cuboidal epithelium, to respiratory bronchioles, with a squamous epithelium. Terminal bronchioles are last generation of conducting airways.
Respiratory bronchioles can be identified by the presence of some alveoli along their walls. The respiratory bronchiole splits into a number of alveolar ducts, which terminate in alveolar sacs and individual alveoli
Courtesy medcell.med.Yale.edu

Courtesy Dr Yale Rosen

The Buck Ends Here
The alveolus is lined by a simple epithelium ? one cell layer thick. There are two types of lining cells; Type 1 pneumocytes are squamous cells that cover 90% of the surface of the inner lining of the lung , and type II cuboidal pneumocytes that are in fact much more numerous than Type I. They are involved in the production of surfactant . In the lumen there are resident macrophages which play a crucial role in the immune system. The mucosa is grounded by a basement membrane and a lamina propria, and connected to the lamina propria and basement membrane of the surrounding capillary. The alveolus is lined by a thin layer of surfactant. (teal blue)
Ashley Davidoff
TheCommonVein.net
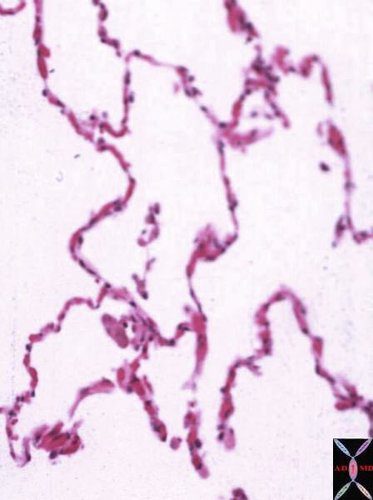
Lower magnification of the lung with H and E stain shows cup-shaped alveolar spaces outlined by delicate thin alveolar capillary membrane.
key words
lung, pulmonary, normal alveolus, alveoli, histology, interstitium, interstitial
Courtesy Armando Fraire MD. 32819
Courtesy Wikiwand
web lungs 435
Abrupt onset
Flu like symptoms
malaise
Note
patients with fibrotic HP often overlap with those described in patients with idiopathic interstitial pneumonias – UIP and NSIP
- distinction between
- IPF and an inflammation-driven disorder such as fibrotic HP
- is crucial, because
- immunosuppressive therapy is considered to be harmful in IPF
- appropriate in fibrotic HP.
- On the other hand
- anti-fibrotic treatment licensed for IPF,
- not for fibrotic HP.
/www.youtube.com/watch?v=CPwRi6DO5VY

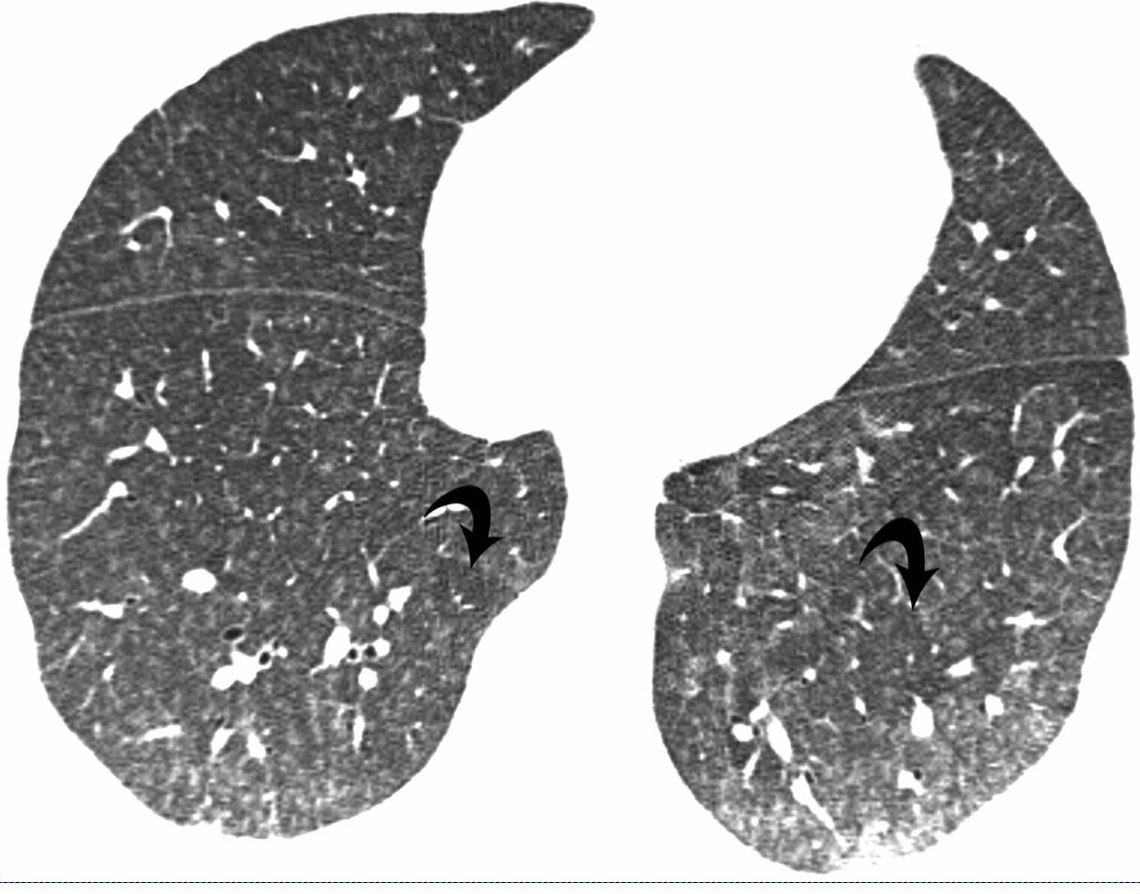
High-resolution CT: increase in density in areas of ground glass and air trapping in lower lobes in a patient with hypersensitivity pneumonitis
Courtesy Mluisamtz11


Parekh, M et al Review of the Chest CT Differential Diagnosis of Ground-Glass Opacities in the COVID Era Radiology Vol. 297, No. 3 July 2020



GGO Non fibrotic

Air trapping
Fibrotic HP
Upper lobe predominance

Small Airway Disease Terminal Bronchiole
Small Airway Disease Giant Cell Around the Terminal Bronchiole

Multinucleate giant cells within a terminal bronchiole.
Courtesy Dr Yale Rosen
Small Airway Disease – Organizing Pneumonia – Terminal Bronchiole

Areas of organizing pneumonia are frequently seen in hypersensitivity pneumonitis.
Courtesy Dr Yale Rosen
Interstitial Infiltrates

Mild interstital inflammation and multiple granulomas.
Courtesy Dr Yale Rosen

Interstitial chronic inflammation and a granuloma composed of multinucleate giant cells.
Courtesy Dr Yale Rosen
Mild interstital inflammation and multiple granulomas.
Courtesy Dr Yale Rosen

An interstitial granuloma composed of multinucleate giant cells.
Courtesy Dr Yale Rosen

Patchy chronic interstitial inflammation and a granuloma composed of multinucleate giant cells.
Courtesy Dr Yale Rosen
Courtesy Wikiwand
web lungs 435
Nutshell Buzz

Courtesy Mutleysmith Wikipedia

Courtesy Nephron
7 Years Prior
CT Hypersensitivity Pneumonitis
Mild Thickening of the Interlobular Septa and prominence of Some Centrilobular Nodules

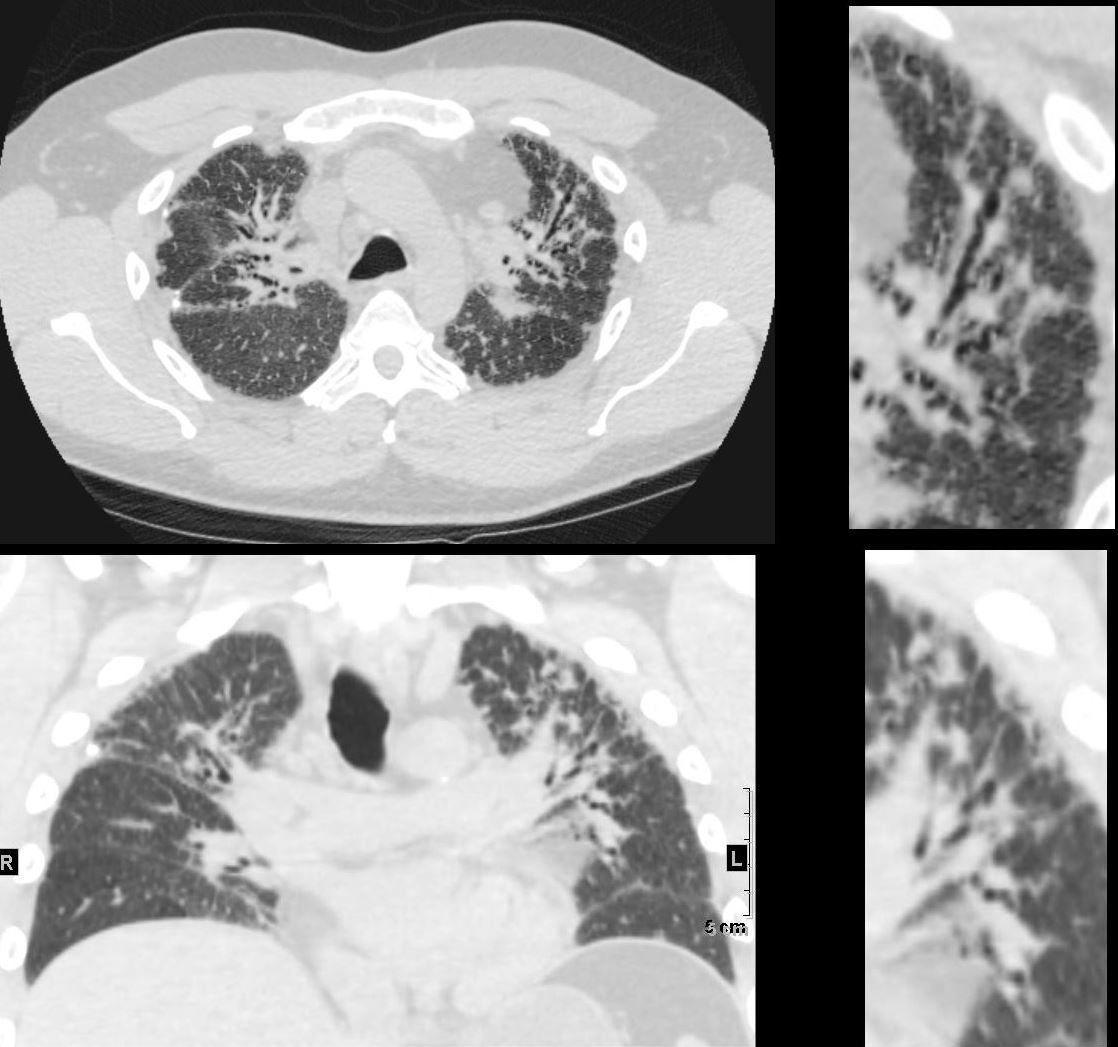
CT Hypersensitivity Pneumonitis
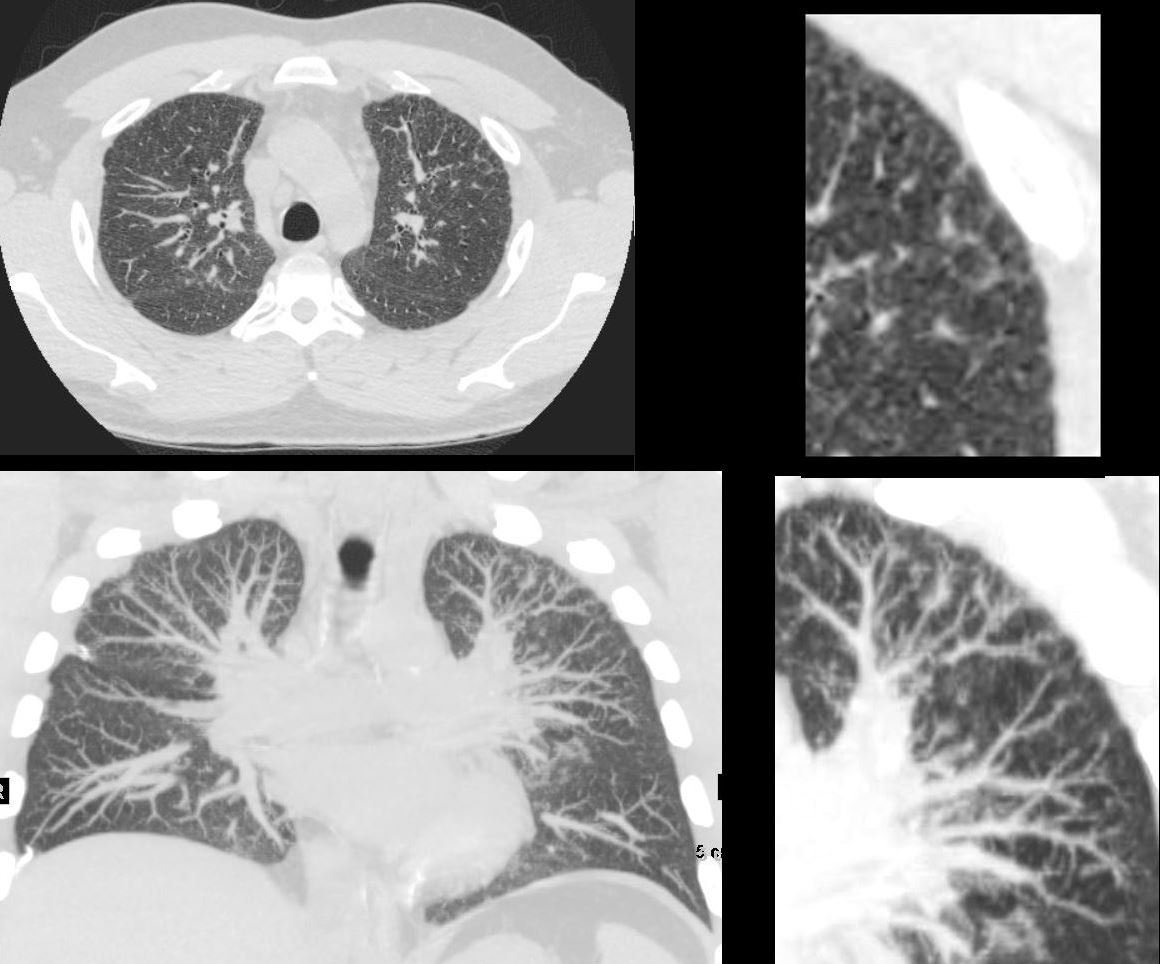
CT in the axial plain (upper panels) and coronal plane (lower panels) show most prominent changes in the anterior segment of the upper lobes
The findings are characterized by evidence of thickening of the interlobular septa, nodular bronchovascular bundle and centrilobular nodules. indicating small airway disease
Ashley Davidoff MD TheCommonVein.net 135836
6 Years Prior
Mild Progression of Thickening of the Interlobular Septa and Prominence of Some Centrilobular Nodules
CT Hypersensitivity Pneumonitis
CT in the axial plain (upper panels) and coronal plane (lower panels) show most prominent persistent changes in the anterior segment of the upper lobes
The findings are characterized by evidence of thickening of the interlobular septa, nodular bronchovascular bundle and centrilobular nodules. indicating small airway disease
Ashley Davidoff MD TheCommonVein.net 135837
5 Years Prior
Minimal Change

CT Hypersensitivity Pneumonitis CT in the axial (upper)and coronal plane (lower panels) show most prominent progressive changes in the anterior segment of the left upper lobe
The findings are characterized by evidence of thickening of the bronchovascular bundle and centrilobular nodules upper right panel) indicating small airway disease
Ashley Davidoff MD TheCommonVein.net 135838
Current
Progressive Nodular Thickening Along the Bronchovascular Bundle and Enlarging Centrilobular Nodules
CT in the axial (upper)and coronal plane (lower panels) show most prominent and progressive changes in the anterior segment of the left upper lobe
The findings are characterized and by evidence of thickening of the bronchovascular bundle (upper right panel) and centrilobular nodules (lower right panel) indicating small airway disease
Ashley Davidoff MD TheCommonVein.net 135839

CT in the axial (upper)and coronal plane (lower panels) show most prominent changes in the anterior segment of the left upper lobe
The findings are characterized and best appreciated in the upper right panel by evidence of small airway disease including tree in bud and centrilobular nodules most prominent in the periphery
Ashley Davidoff MD TheCommonVein.net 135835
Hypersensitivity Pneumonitis Pattern
{kind=link}

a- PD-1 inhibitor pneumonitis: Hypersensitivity pneumonitis pattern in a 68-year-old man with metastatic renal cell carcinoma who was treated with nivolumab and presented with a new cough at 6 months of therapy. (a) Axial chest CT image shows new multifocal GGOs in a centrilobular distribution throughout both lungs and mosaic attenuation, findings that represent pneumonitis with a hypersensitivity pneumonitis pattern. Nivolumab therapy was withheld, and the patient underwent corticosteroid therapy.
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care RadioGraphicsVol. 37, No. 5
{kind=link}

b
Axial follow-up CT image obtained after 1 month of corticosteroid therapy shows marked improvement of pneumonitis and resolution of GGOs. Nivolumab continued to be withheld, and corticosteroid therapy was tapered. At 1.5 months after completing the corticosteroid taper, without restarting nivolumab or any other systemic therapy, the patient experienced a worsening cough.
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care RadioGraphicsVol. 37, No. 5
{kind=link}

c
Axial chest CT image shows development of diffuse GGOs with areas of air trapping, findings indicative of pneumonitis with a hypersensitivity pneumonitis pattern. The radiographic pattern of this second episode is similar to that noted in the initial episode and represents pneumonitis flare.
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care RadioGraphicsVol. 37, No. 5
{kind=link}
Pneumonitis in a 62-year-old woman with advanced pancreatic neuroendocrine tumor treated with everolimus and temozolomide. Axial CT image obtained at 10.3 months of therapy shows diffuse bilateral GGOs and reticular opacities that are indicative of a hypersensitivity pneumonitis pattern. The patient had mild shortness of breath and was treated with prednisone.
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care RadioGraphicsVol. 37, No. 5
{kind=link}
Pneumonitis in a 42-year-old man with an EGFR exon 19 deletion mutation who was treated with erlotinib in the United States. Axial chest CT images (b obtained at a lower level than a) obtained at 8 weeks of therapy show multifocal areas of GGOs in both lungs, findings that represent pneumonitis. Note the absence of traction bronchiectasis or volume loss.
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care RadioGraphicsVol. 37, No. 5
{kind=link}

Pneumonitis in a 42-year-old man with an EGFR exon 19 deletion mutation who was treated with erlotinib in the United States. Axial chest CT images (b obtained at a lower level than a) obtained at 8 weeks of therapy show multifocal areas of GGOs in both lungs, findings that represent pneumonitis. Note the absence of traction bronchietasis or volume loss.
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care RadioGraphicsVol. 37, No. 5
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care RadioGraphicsVol. 37, No. 5
References and LINKS
- Videos
- AUR
Title web link Hypersensitivity Pneumonitis AUR Cardiothoracic Imaging
- AUR