

Fun Lung

found Roaming Near the Hilum of the Lung on Sagittal CT Reconstruction
Ashley Davidoff MD TheCommonVein.net lungs-0706-lo resb

Ashley Davidoff MD TheCommonVein.net lungs-0706-lo res

From the series “Art of the The X-ray”
Ashley Davidoff MD TheCommonVein.net 01 Christmas lo resb

Ashley Davidoff MD The CommonVein.net lungs-0718

Ashley Davidoff MD The CommonVein.net lungs-0717

Ashley Davidoff MD The CommonVein.net lungs-0716

Ashley Davidoff MD The CommonVein.net lungs-0715

Ashley Davidoff MD The CommonVein.net lungs-0714

Ashley Davidoff MD The CommonVein.net lungs-0713

Ashley Davidoff MD The CommonVein.net lungs-0710
Trees in the Body
Showing derivation of the art piece
Ashley Davidoff MD TheCommonvein.net trees-0010

Ashley Davidoff MD TheCommonVein.net trees-0001

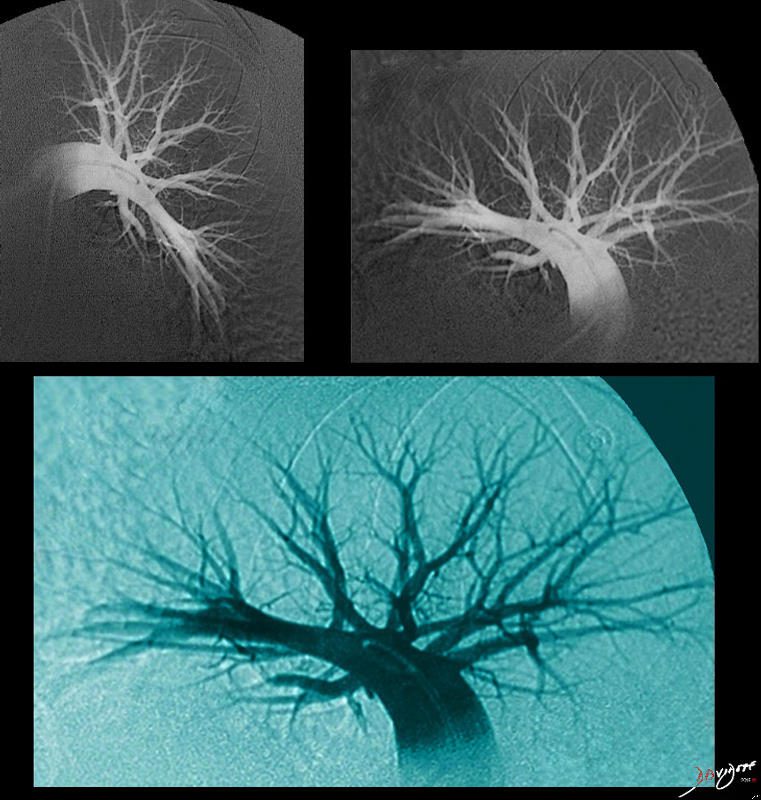
Art image derived from a parasagittal view of a reconstructed CT scan – CTA of the chest
Ashley Davidoff MD TheCommonvein.net 46649c01.800

Top left image is sagittal oblique CT scan of the chest and shows a prominent sternum and heavily calcified costochondral junctions. When turned upside down (middle top , a cedar tree is created, then multiplied (middle image) and placed along a river in a mountain under a beautiful summer sun.
Ashley Davidoff MD TheCommonVein.net lungs-0708
Racing Car in the Chest

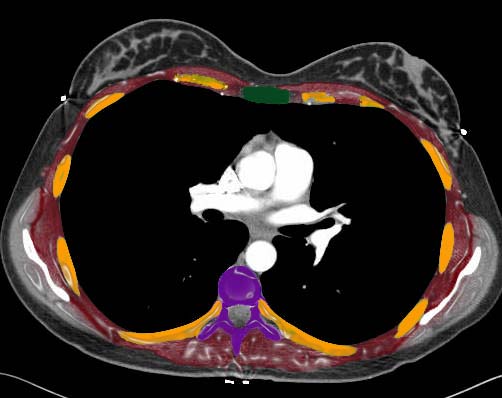
Created from the hardware anterior to the chest on a CT scan
Ashley Davidoff MD
TheCommonVein.net chest-0004
Sunrise in the Chest
Ashley Davidoff MD
TheCommonVein.net chest-0003
Overview and Collages

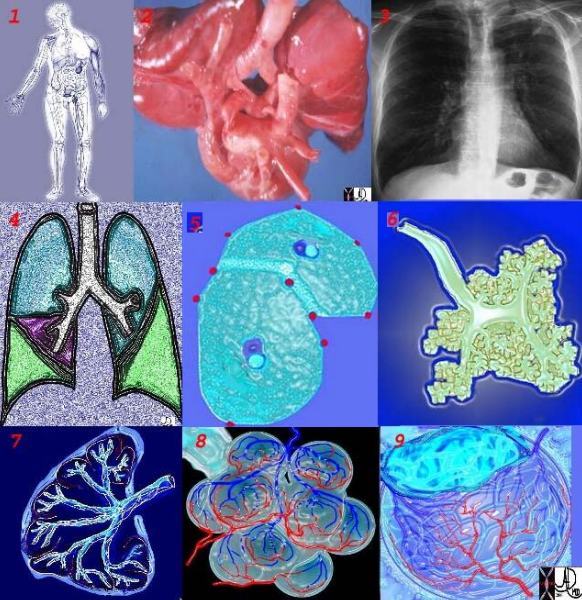
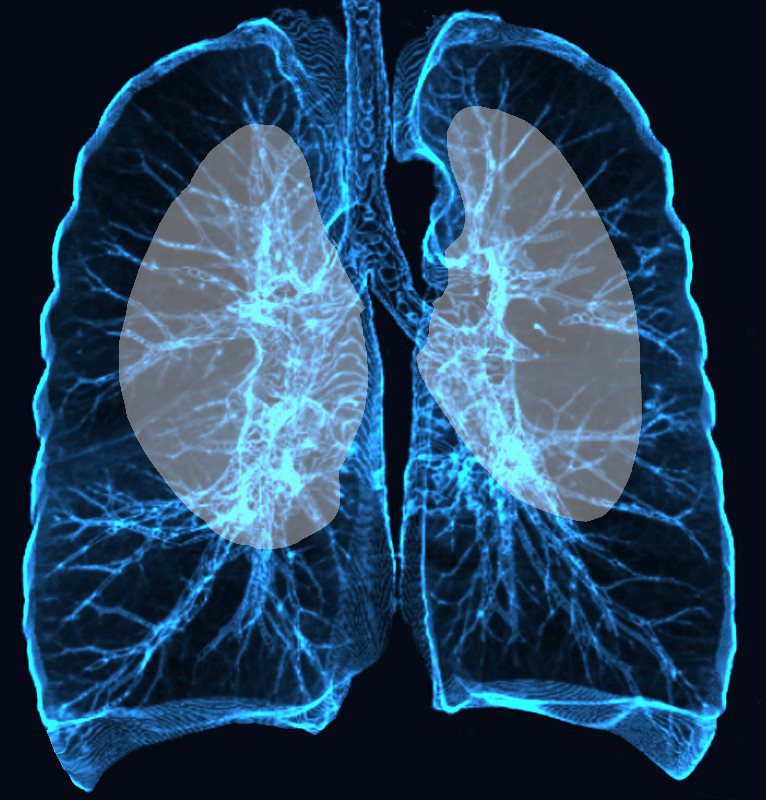
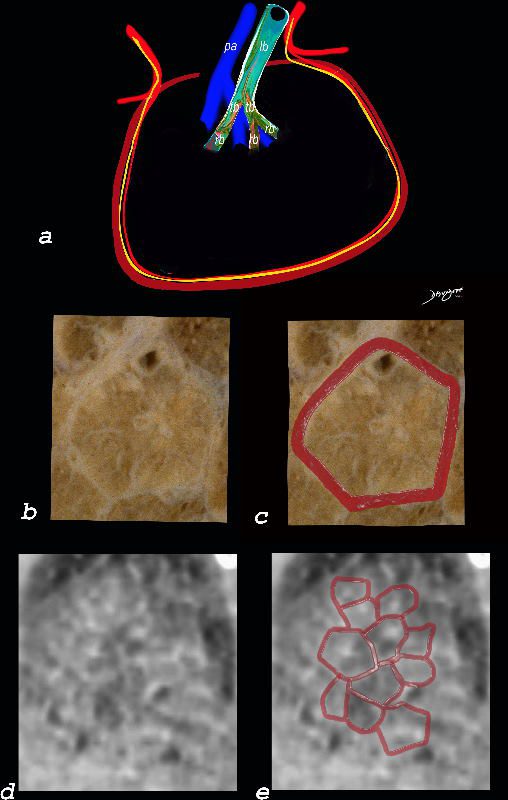
This is a collage illustrating the axial fiber system starting at the hilum, (1,2) coursing along the pulmonary artery (3) and bronchovascular system, (3,4,6) surrounded by a basket of connective tissue (4,5) extending into the polygonal secondary lobule (7,8) and ending in the alveolar ducts and sacs. (9) .
Ashley Davidoff MD TheCommonVein.net
01collageaxialfiber
Anatomy
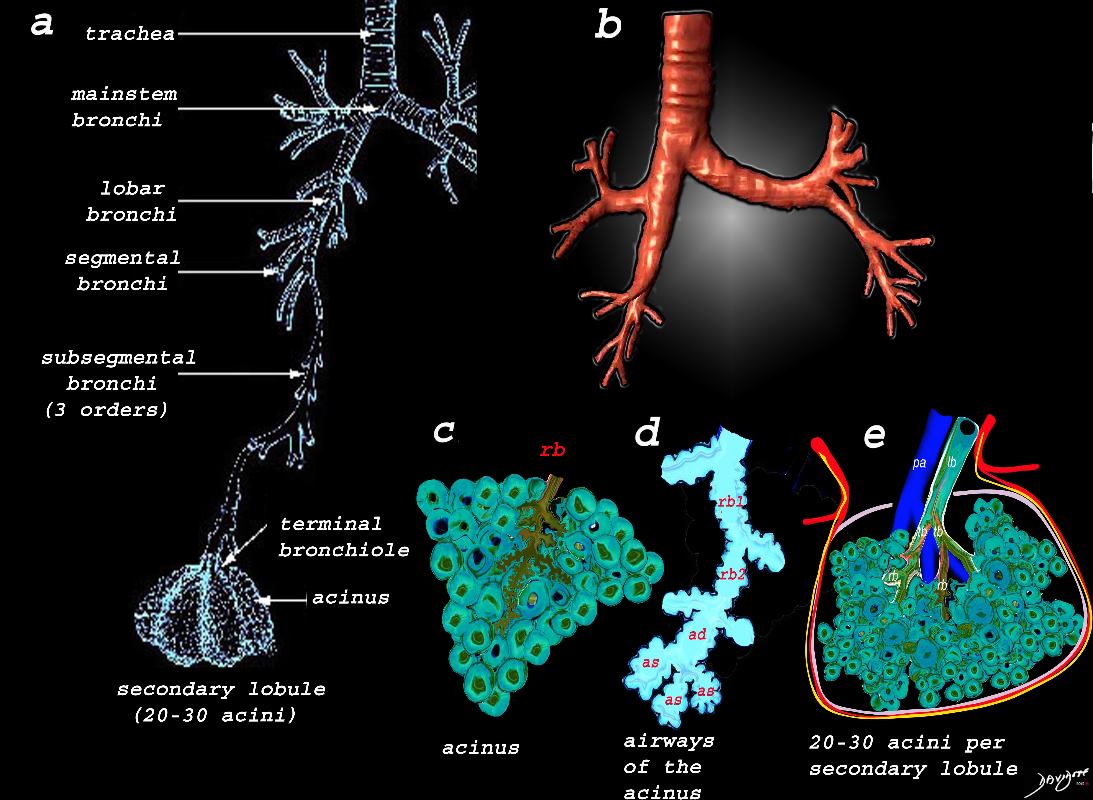
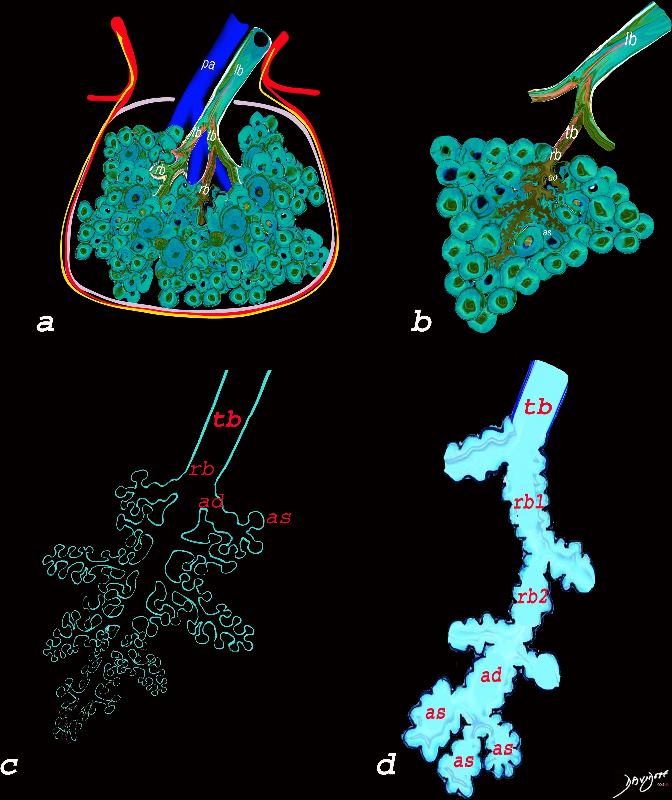
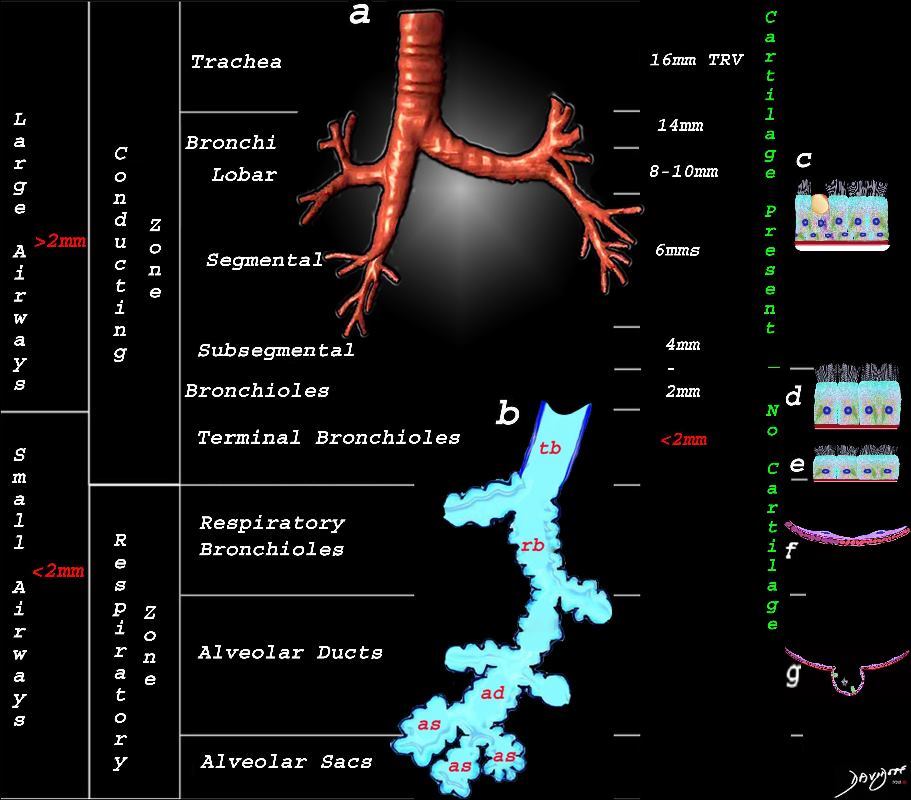
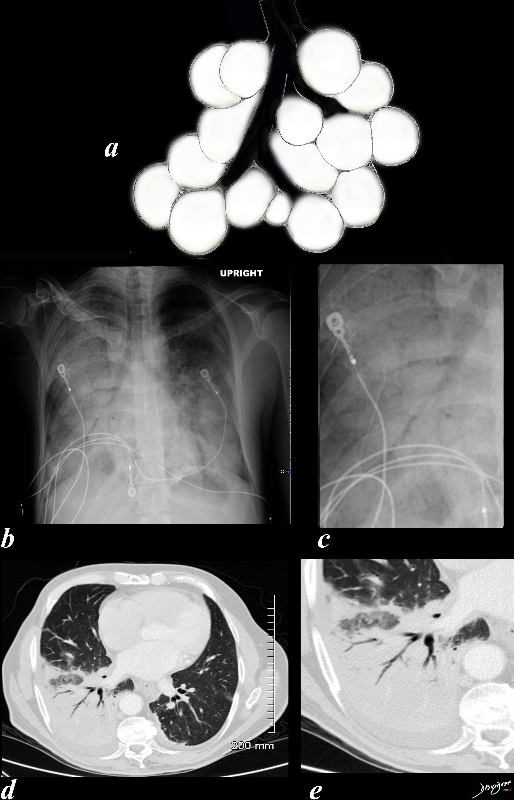
Image a shows the airways starting in the trachea and continuing to the mainstem bronchi, lobar bronchi, segmental bronchi, and subsegmental bronchi,. The subsegmental bronchi have 3 subsequent generations until the bronchiole is reached. The terminal bronchiole is the last of the transporting airways and is considered the most proximal small airway with a diameter of 2mm or less, and it gives rise to the respiratory bronchiole which is the feeding airway for the acinus . The acinus is the functional unit of the lung.
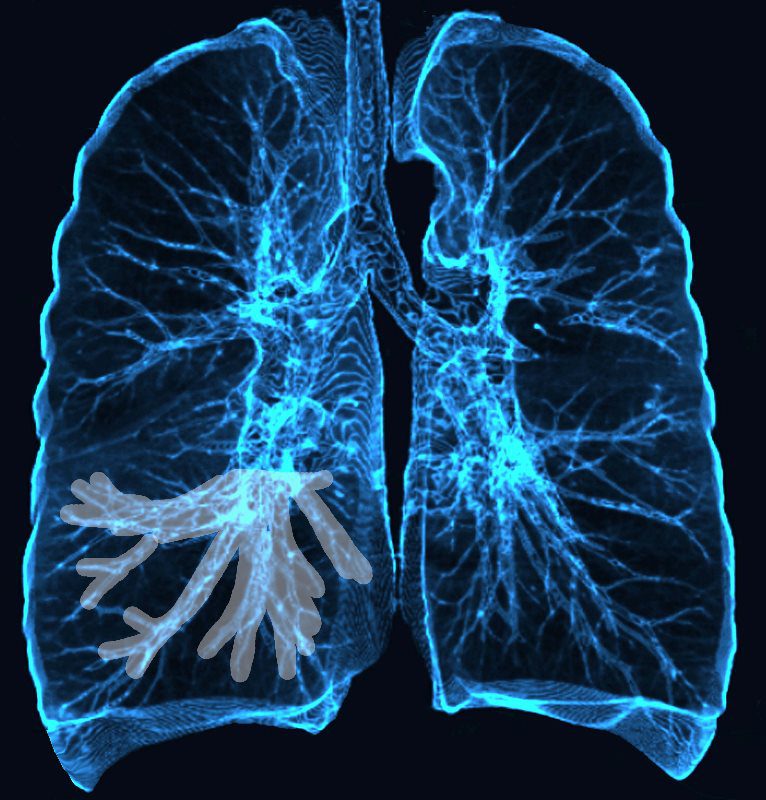
Image b is a 3D reconstruction of a CT scan showing the proximal airways from the trachea to the segmental airways.
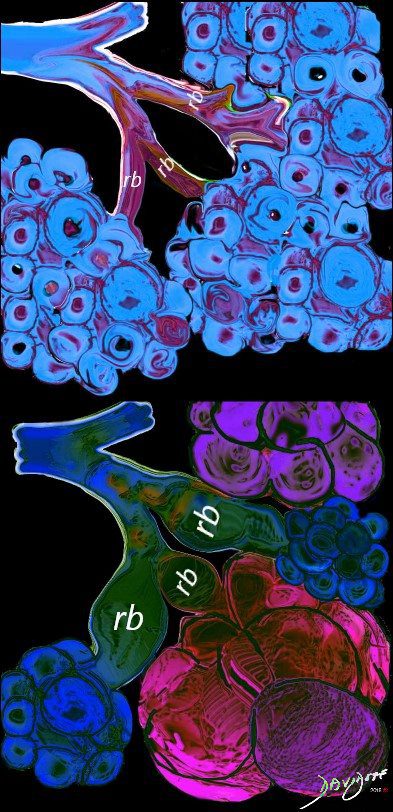
Image c shows the structures that make up the acinus and the other parts of the small airways, starting with the respiratory bronchiole (rb) . The diagram in d, shows the detail of the small airways that participate in gas exchange, including the respiratory bronchiole, (rb) alveolar duct, (ad) and alveolar sac (as)
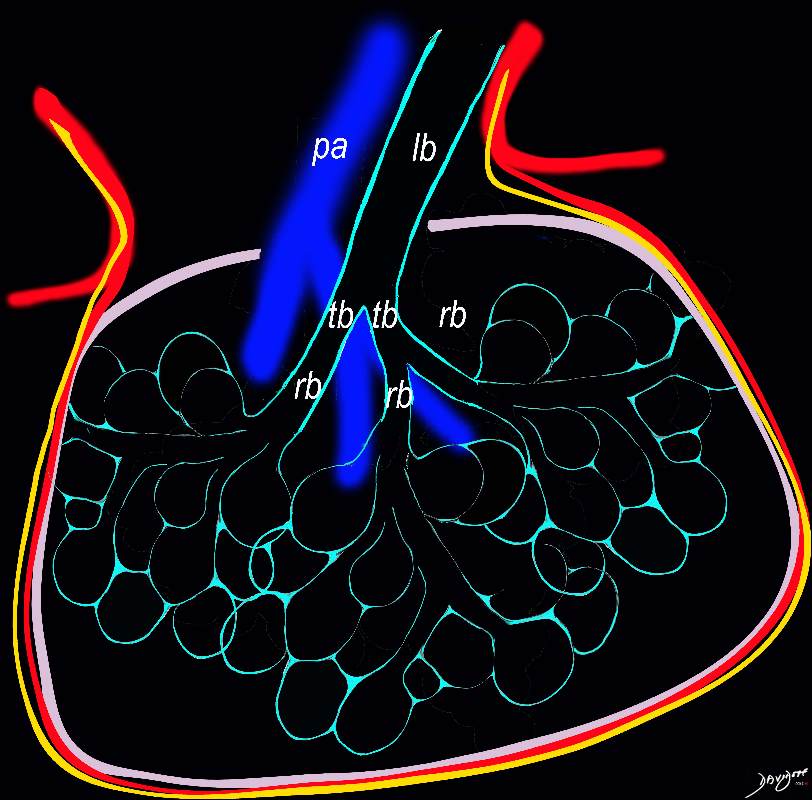
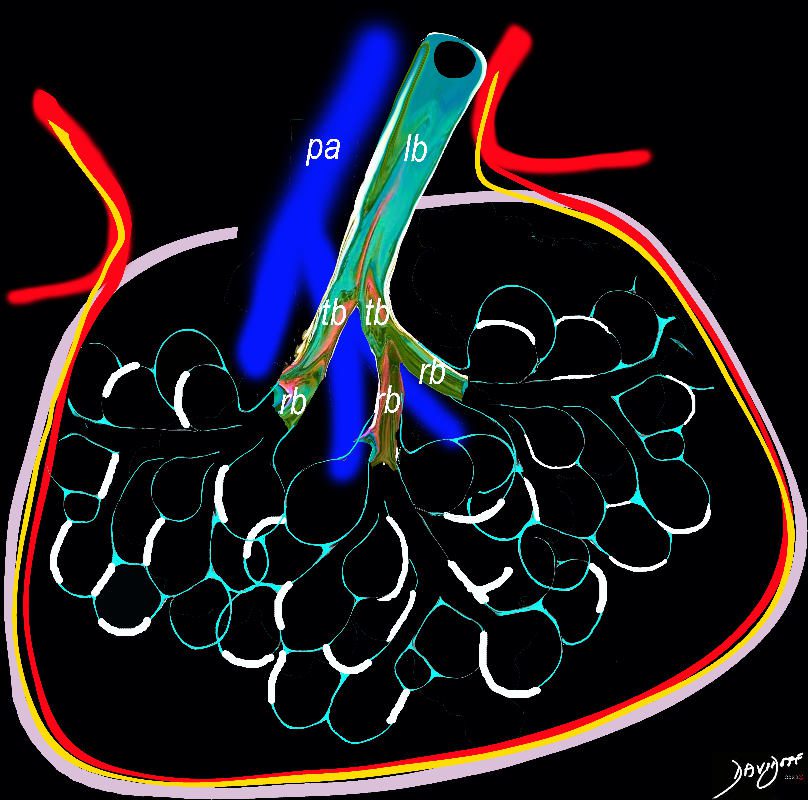
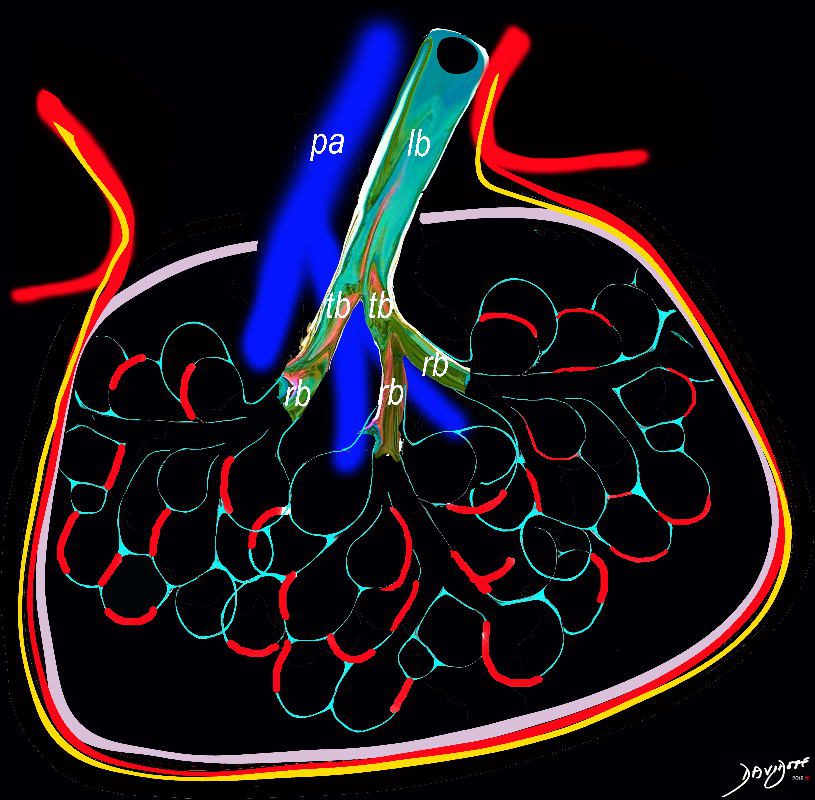
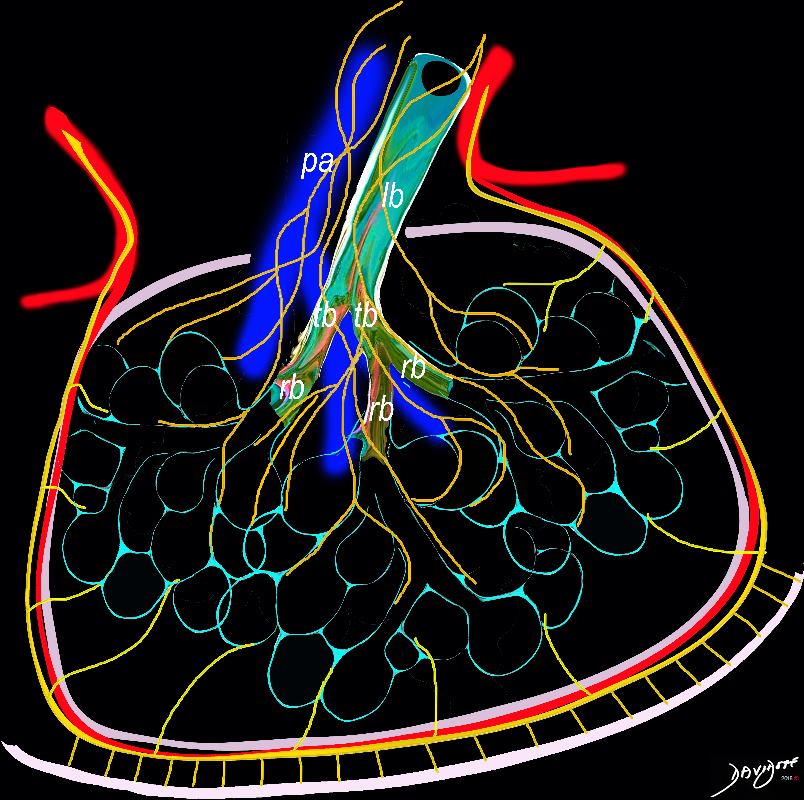
Image e shows the secondary lobule made from about 20-30 acini, arising from a single lobular bronchiole accompanied by a single pulmonary arteriole (pa).. Structure that surround and enclose the secondary lobule include the pulmonary venule, (red) lymphatics,(yellow) and a fibrous septum (pink).
Ashley Davidoff MD TheCommonVein.net
lungs-0739
Trachea Bronchi
The classical branching pattern of many trees
Ashley Davidoff MD TheCommonVein.net lungs-0037
To remember the difference in the sizes of the mainstem bronchi think of 2 very different men in the airways. The right – short, stout and cute, and the left – tall thin and gracile
The carinal angle is about 85 degrees
Ashley Davidoff MD TheCommonVein.net 42474b14b
Muscles
Ashley Davidoff, M.D. TheCommonVein.net 42554ab07c
000 Skeleton

Courtesy of: Ashley Davidoff, M.D. TheCommonVein.net
42530b08
000 Physiology Breathing

Ashley Davidoff, M.D. TheCommonVein.net 42540b06
Segmental Airways Subsegmental Airways Small Airways
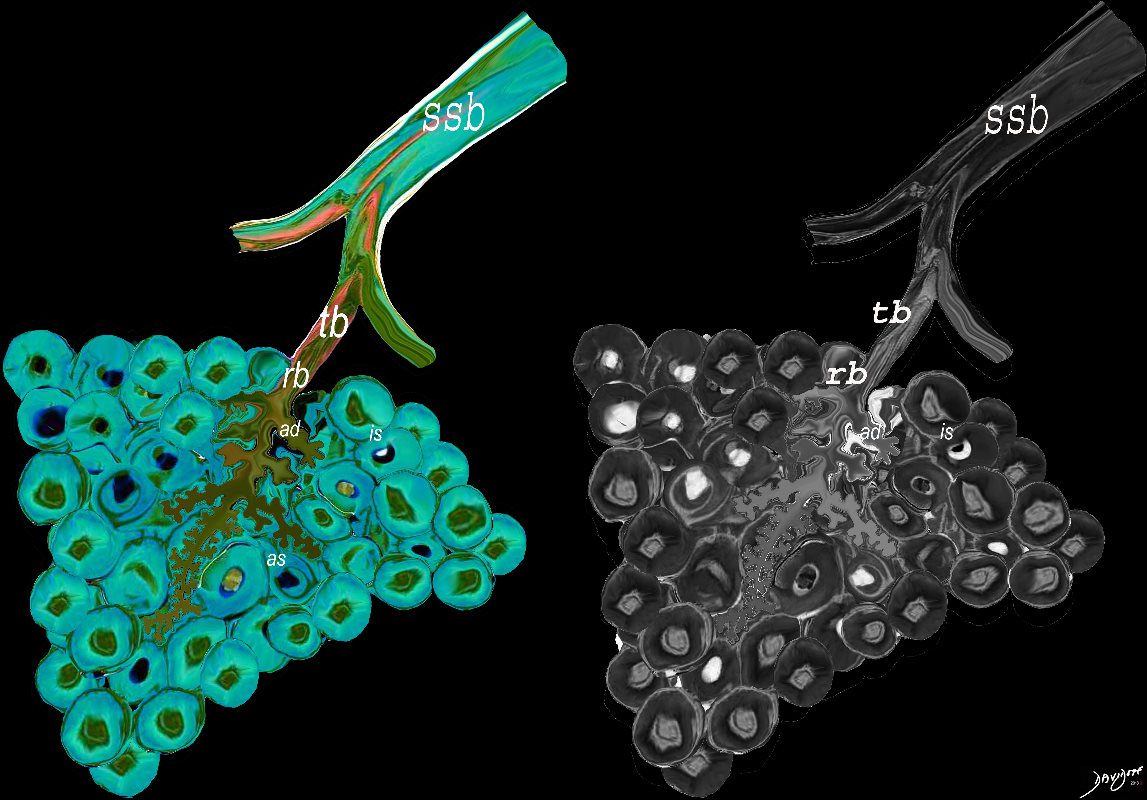
The diagram allows us to understand the the components and the position of the small airways starting in (a) which is a secondary lobule that is fed by a lobular bronchiole(lb) which enters into the secondary lobule and divides into terminal bronchioles (tb) which is the distal part of the conducting airways, and at a diameter of Ashley Davidoff MD TheCommonVein.net lungs-0744

The diagram allows us to understand the the components and the position of the small airways starting in (a) which is a secondary lobule that is fed by a lobular bronchiole(lb) which enters into the secondary lobule and divides into terminal bronchioles (tb) which is the distal part of the conducting airways, and at a diameter of 2mm or less . It divides into the respiratory bronchiole (rb) a transitional airway which then advances into the alveolar ducts(ad) and alveolar sacs (as) Diseases isolated to the small airways do not affect the alveoli and hence there is peripheral sparing Ashley Davidoff MD TheCommonVein.net lungs-0749

Ashley Davidoff MD TheCommonVein.net lungs-0747
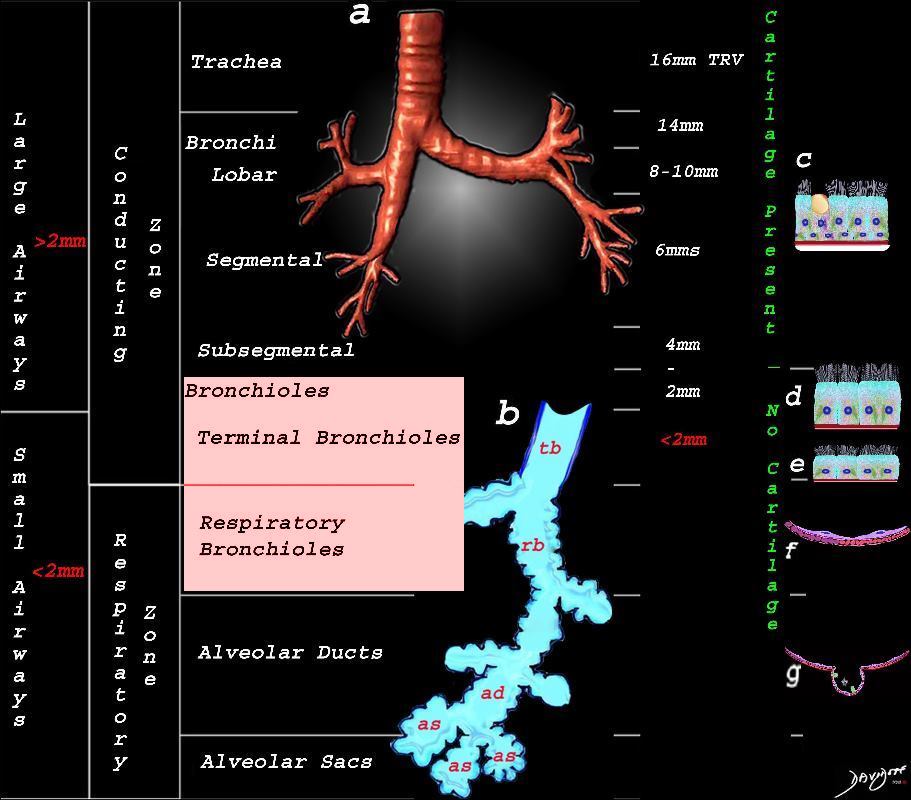
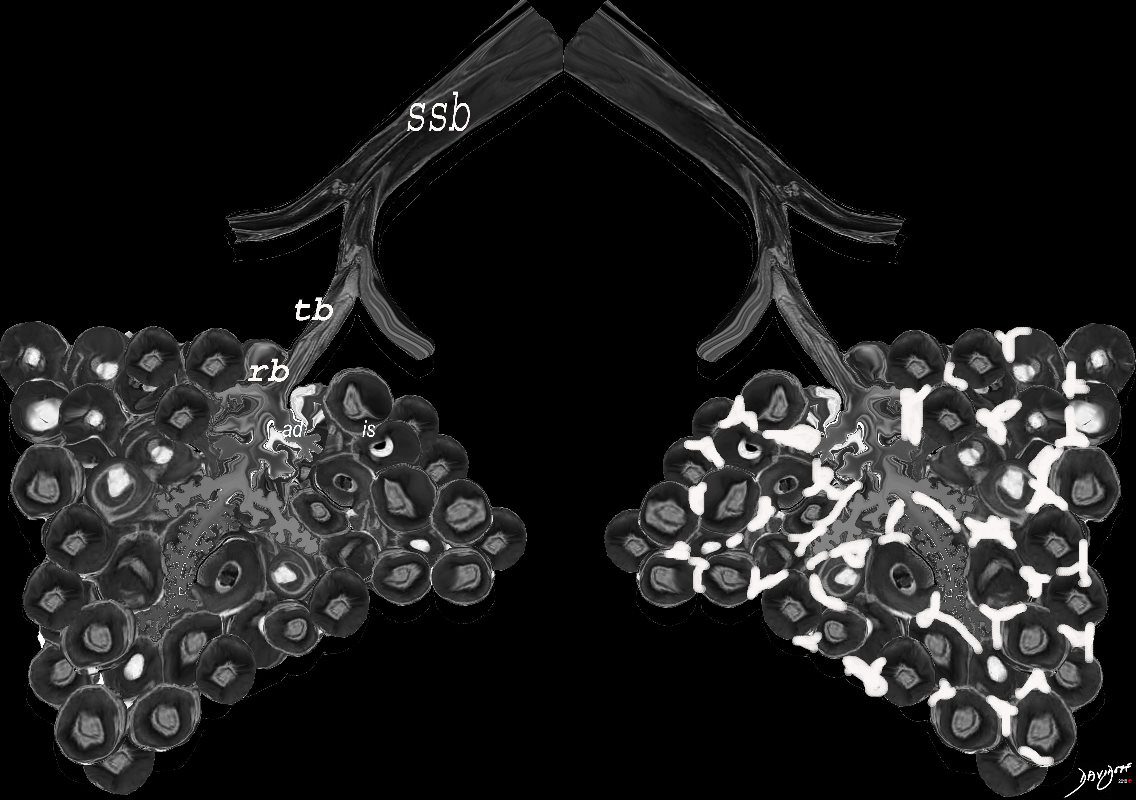
This image shows the division of the airways in the lungs classified as large airways and small airways.
A large airway is considered any airway larger than 2mm, and therefore includes all the airways involved with transport of air except for the terminal bronchiole. Included as seen in image a, are the trachea, mainstem bronchi, lobar bronchi segmental and subsegmental airways and the 3 subsequent divisions of subsegmental bronchi and bronchioles till the last transporting airway ? the respiratory bronchiole which is usually about 2mm and is considered a small airway Image (a) shows the airways starting in the trachea and continuing to the mainstem bronchi, lobar bronchi, segmental bronchi, and subsegmental bronchi.
Image b shows the structures that make up the small airways starting with the terminal bronchiole (tb) followed by the respiratory bronchiole (rb) alveolar duct, (ad) and alveolar sacs (as)
Image (c) shows the histologic makeup of the large airways that include a pseudostratified ciliated columnar epithelium with mucus secreting goblet cells a muscular layer (red) and a prominent cartilage layer (white) In the larger bronchioles (d) the epithelium remains as a pseudostratified, ciliated, columnar epithelium with prominent muscular layer (red). The columnar epithelium transitions to a stratified ciliated cuboidal epithelium by the terminal bronchiole s (f) both still with a muscular layer. The respiratory epithelium transitions from a cuboidal epithelium to a squamous epithelium (f) with alveoli and type I and II pneumocytes starting to branch (g)
Ashley Davidoff MD TheCommonVein.net lungs-0740nL01bronchioloes
This image shows the division of the airways in the lungs classified as large airways and small airways.
A large airway is considered any airway larger than 2mm, and therefore includes all the airways involved with transport of air except for the terminal bronchiole. Included as seen in image a, are the trachea, mainstem bronchi, lobar bronchi segmental and subsegmental airways and the 3 subsequent divisions of subsegmental bronchi and bronchioles till the last transporting airway ? the respiratory bronchiole which is usually about 2mm and is considered a small airway Image (a) shows the airways starting in the trachea and continuing to the mainstem bronchi, lobar bronchi, segmental bronchi, and subsegmental bronchi.
Image b shows the structures that make up the small airways starting with the terminal bronchiole (tb) followed by the respiratory bronchiole (rb) alveolar duct, (ad) and alveolar sacs (as)
Image (c) shows the histologic makeup of the large airways that include a pseudostratified ciliated columnar epithelium with mucus secreting goblet cells a muscular layer (red) and a prominent cartilage layer (white) In the larger bronchioles (d) the epithelium remains as a pseudostratified, ciliated, columnar epithelium with prominent muscular layer (red). The columnar epithelium transitions to a stratified ciliated cuboidal epithelium by the terminal bronchiole s (f) both still with a muscular layer. The respiratory epithelium transitions from a cuboidal epithelium to a squamous epithelium (f) with alveoli and type I and II pneumocytes starting to branch (g)
Ashley Davidoff MD TheCommonVein.net lungs-0740nL
Ashley Davidoff MD TheCommonVein.net lungs-0721

Ashley Davidoff MD TheCommonVein.net lungs-0746
Acinus

The pulmonary arteriole (pa) accompanies the lobular bronchiole (lb). The arteriole transports deoxygenated blood and the bronchiole carries oxygen from the trachea to the alveoli.
They part ways at the alveoli
Ashley Davidoff MD TheCommonVein.net lungs-0034
Secondary Lobule
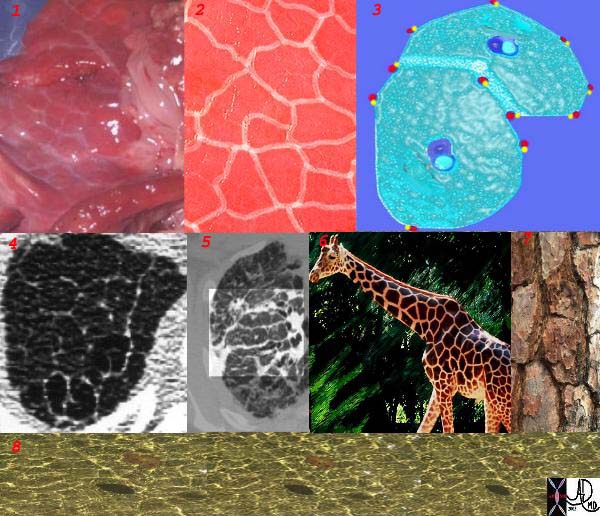
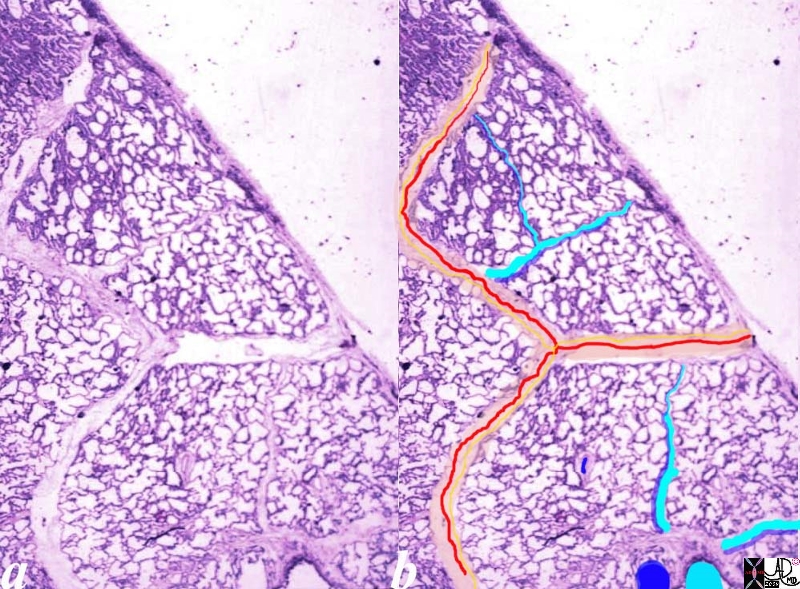
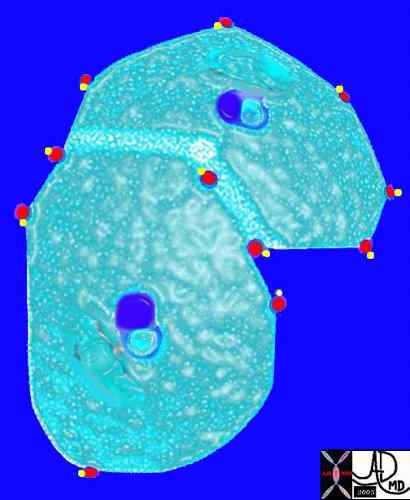
This is a series of images demonstrating the shape of the secondary lobule. The first image (1) is a post mortem specimen with congested lungs showing the interlobular septa, while the next (2), is an overlay of the septa in white showing their polygonal shape. The next drawing reveals side-by-side secondary lobules with central bronchovascular bundles and peripheral lympho-vascular bundles. Image 4 is a CT image through the apex of the lung showing thickened secondary lobules in a patient with mild emphysema, and 5 shows marked thickening of the interlobular septa in a patient with end stage sarcoidosis. 6,7,8 show the shape of the secondary lobules in the skin of a giraffe, the bark of a pine, and the ripples of the water respectively.
Ashley Davidoff MD TheCommonVein.net 31866collage

The secondary lobule is subtended by the lobular arteriole (a) and the lobular bronchiole (b) which which in turn branches into the respiratory bronchioles, alveolar ducts, and nd alveolar sacs (c) The acinus (d) consists of a respiratory bronchiole and its associated alveolar ducts, sacs, and alveoli and represents the functional unit of the lung.
The secondary lobule is drained by the pulmonary venule (e) which runs in the interlobular septum also containing the lymphatics (f). The whole unit is housed and surrounded by a connective tissue framework (g) . The latter 3 structures form the interlobular septum.
Ashley Davidoff MD TheCommonVein.net lungs-0751
Ashley Davidoff MD TheCommonVein.net lungs-0008
Normal lung histology
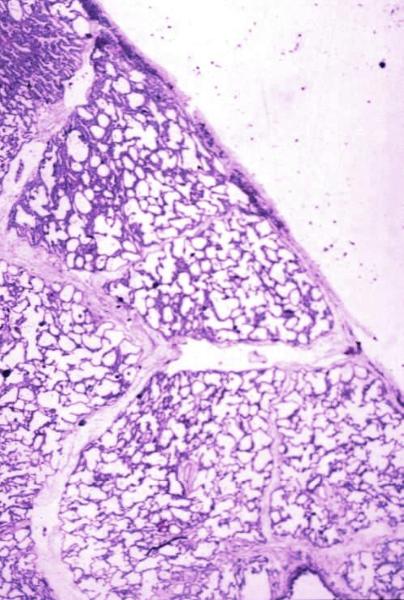
This image is a panoramic view of the lung showing secondary lobules and interlobular septa. Within the interalveolar septae, one sees small venules and lymphatics.Courtesy Armando Fraire MD. 32649b
code lung pulmonary alveoli alveolus secondary lobule interlobular septa vein lymphatic histology
interstitium interstitial
Courtesy of: Armando Fraire, M.D. Ashley Davidoff TheCommonVein.net
32649b
Keywords:
lung pulmonary alveoli alveolus secondary lobule interlobular septa vein lymphatic histology interstitium interstitial normal copyright 2009 all rights reserved
The segments form the secondary lobules.
Normal lung histology. This image of the lung periphery shows secondary lobules and interlobular septa. Within the interlobular septae, one sees small venules and lymphatics. The matrix of the lobule contains alveoli.
Courtesy of: Armando Fraire, M.D. Ashley Davidoff TheCommonVein.net
The arteries and airways pair up and travel together from the interlobular septa to the hilum. The pulmonary lobule, also called the secondary lobule is a structural unit surrounded by a membrane of connective tissue, and it is smaller than a subsegment of lung but larger than an acinus. This diagram shows two secondary lobules lying side by side. The pulmonary arteriole (royal blue) and bronchiole (pink) are shown together in the centre of the lobule (“centrilobular”), while the oxygenated pulmonary venules (red) and lymphatics (yellow) are peripheral and also form a formidable and almost inseparable pair.
42440b03
Ashley Davidoff MD
TheCommonVein.net
Ashley Davidoff MD TheCommonVein.net

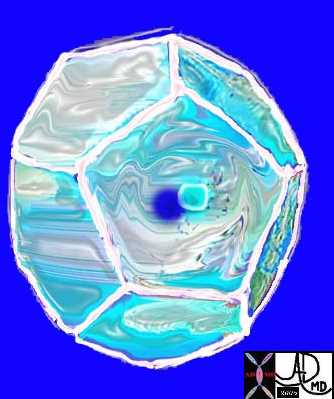
Here is a picture of the outside of the polyhedral pulmonary lobule from the side. It looked quite futuristic. Through the transparent side window we saw a couple similar to ourselves. From this vantage point the morphing did not look too different from what we had already been through – division after division – leaner and meaner. Ashley Davidoff MD. The Common Vein.net 42449b02
The secondary lobule is housed in a connective tissue framework in which run the lymphatic and venular tributaries . Together these 3 structures form the interlobular septum.
The lobar arteriole enters the framework, accompanied by the lobar bronchiole, and they all run together and form the interlobular septa. This structure measures between .5cms and 2cms and is visible on CT scan.
It is important in clinical radiology since many of the structures can be identified in health, and more particularly in disease, enabling the identification and characterization of many pathological processes.
Courtesy Ashley Davidoff MD The CommonVein.net lungs-0735
This picture was taken just before the real drama started. The image gives a sense of what was to come. You can see here in the house of the lobule that we were all dividing into smaller parts and were getting smaller and the picture was quite colorful and rosy. I fully expected to have intimate contact with the arteriole? but it did not happen as I expected…… Ashley Davidoff MD. The Common Vein.net 42447b05b02
This picture shows us on the left with a white ring around us (we were the tallest) and the other couples who looked so much like us (also ringed). We called our tribe the “bronchovascular bundle” with the one part of the bundle being the progeny of the bronchus and the other the progeny of the pulmonary artery. In the distance at the periphery we could see the pairs from the other friendly tribe – the red pulmonary vein with its smaller yellow buddy the lymphatic. Behind them we could see the transparent window membrane through which we had peaked earlier. Oh my goodness!!! Look what has happened to my body!!!!!!!…… Ashley Davidoff MD. The Common Vein.net 42447b03b01
Alveoli

This diagram shows the PCO2 of the arterial blood at 45mmHg with red cell again showing telling signs of blue deoxygenation while the inspired air has a PCO2 of 40mmHg. There is therefore diffusion from the high to the low pressure and a net movement of carbon dioxide into the alveolus to equilibrate the pressure of 40mmHg. The venous blood is thus relatively depleted of CO2 with a PCO2 of 40mmHg. |
Ashley Davidoff MD TheCommonVein.net 42445b11
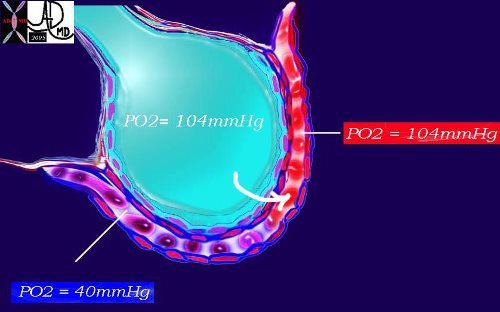
This diagram again shows the alveolus in teal, the arteriolar component of the capillary with red cells in blue and venular component replenished by oxygen in red. As noted above, the PO2 of the arterial blood is 40mmHg while the inspired air is 104mmHg. A pressure gradient thus exists and diffusion from the high to the low pressure occurs with a net movement of oxygen into the blood to equilibrate the pressure. Venous blood is now rich in oxygen with a PO2 of 104mmHg.
Ashley Davidoff MD TheCommonVein.net 42445b08b

The alveolus is lined by a complex detergent type solution called surfactant (pink) which reduces the surface tension in the alveolus, making it easier for the alveolus to expand during inspiration and preventing alveolar collapse on expiration.
Ashley Davidoff TheCommonVein.net 42530b05b09b01a12
The diagram shows an alveolus, lined by a single layer of squamous cells,
Ashley Davidoff MD TheCommonVein.net lungs-0705-lo res
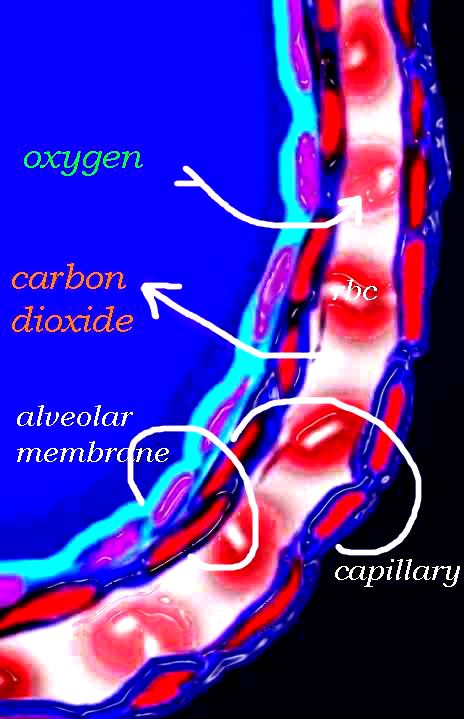
The diagram shows an alveolus, lined by a single layer of squamous cells, surrounded by a capillary with red cells which is also lined by a single layer of squamous endothelial cells . The images show exchanges of oxygen and carbon dioxide through the alveolar membrane .
Ashley Davidoff MD TheCommonVein.net lungs-0028b-low res
Cells of the Bronchi Cells of the Small Airways
Cells of the Alveoli

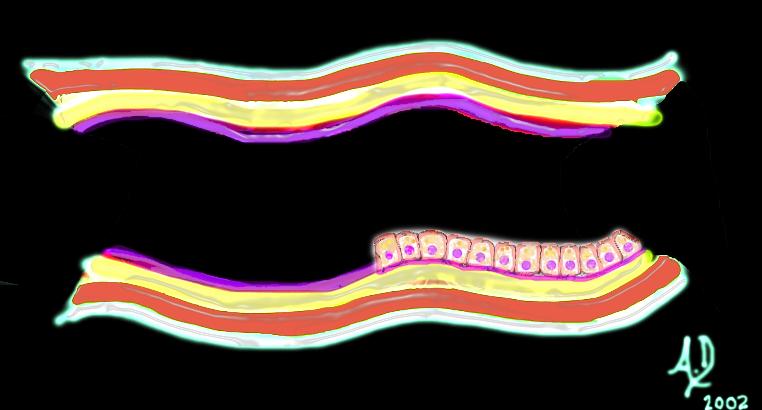
This upper diagram shows the ciliated columnar epithelium present throughout the 20- 25 generations of branching, until the airways start to transition their function from a transport system to a gas exchange system at the respiratory bronchiole level The ciliated columnar epithelium becomes a ciliated cuboidal epithelium. There are no goblet cells in the bronchioles In addition to the ciliated cells there are 2 other types of cells including the club cell (purple) and the neuroendocrine cell. The club cells Purple with dome shaped superior aspects – formerly Clara Cell) have many functions. The neuroendocrine cell (NE) (dark pink and round ) can be seen as a single cell (NE) and sometimes seen in a cluster, known as a neuroendocrine body (NEB) . The cells rest on a basement membrane, with prominent muscle layer (maroon) as well as elastic tissue (pink). There is no cartilage
Ashley Davidoff MD TheCommonVein.net
lungs-0741n

The club cell aka bronchiolar exocrine cells formerly known as the Clara cell is a low columnar cell with short microvilli and are most abundant in the bronchioles
Ashley Davidoff MD TheCommonVein.net lungs-0743
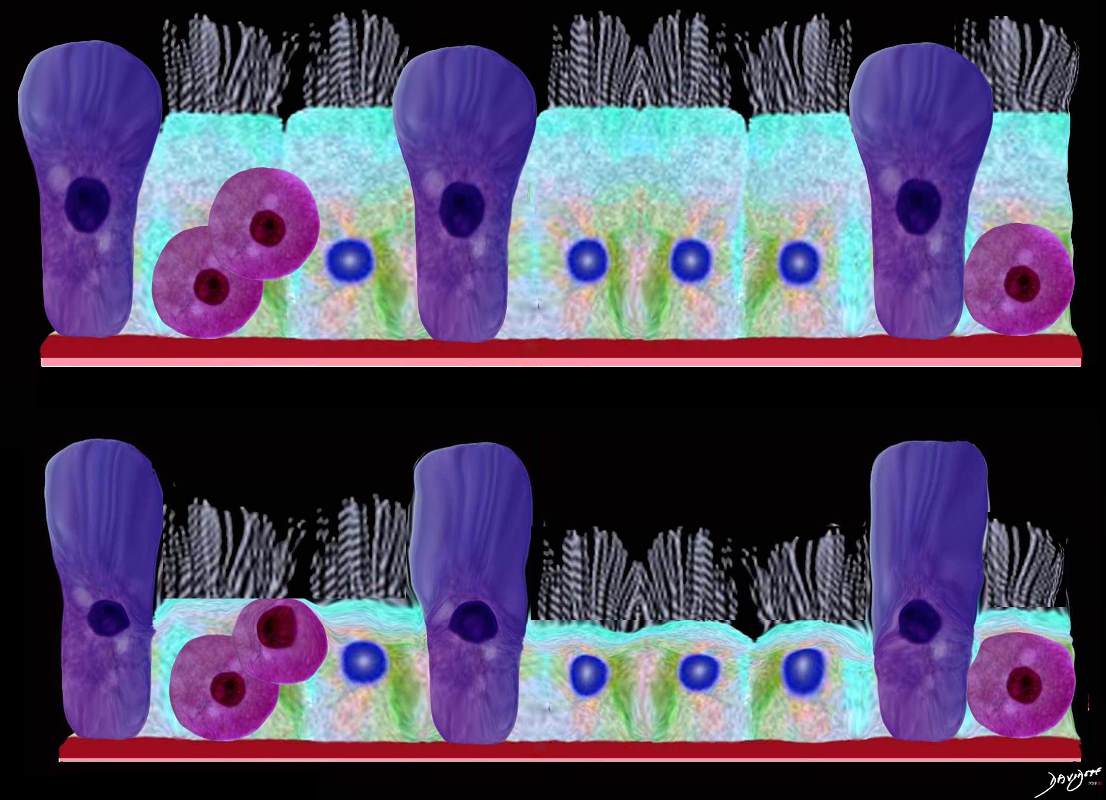
This upper diagram shows the ciliated columnar epithelium present throughout the 20- 25 generations of branching, until the airways start to transition their function from a transport system to a gas exchange system at the respiratory bronchiole level The ciliated columnar epithelium becomes a ciliated cuboidal epithelium. There are no goblet cells in the bronchioles In addition to the ciliated cells there are 2 other types of cells including the club cell (purple) and the neuroendocrine cell. The club cells Purple with dome shaped superior aspects – formerly Clara Cell) have many functions. The neuroendocrine cell (NE) (dark pink and round ) can be seen as a single cell (NE) and sometimes seen in a cluster, known as a neuroendocrine body (NEB) . The cells rest on a basement membrane, with prominent muscle layer (maroon) as well as elastic tissue (pink). There is no cartilage
Ashley Davidoff MD TheCommonVein.net
lungs-0741

Ashley Davidoff MD TheCommonVein.net lungs-0752

Photograph of the Heart and Lungs created with a red pepper (the heart, grapes (alveoli) carrots (pulmonary arteries), dandelion(mediastinum) and banana peels (ribs)
Ashley Davidoff MD TheCommonVein.net
lungs-00677-lo-res.jpg
At the level of the mebranous airways (respiratory bronchiole, alveolar duct, alveolar sac and alveoli, the mucosa becomes mostly a simple squamous epitheliumAshley Davidoff
TheCommonVein.net lungs-00677
Ashley Davidoff
TheCommonVein.net lungs-00676

Ashley Davidoff
TheCommonVein.net
lungs-00675-lo-res
CXR
Basilar and peripheral distribution
Ashley Davidoff MD TheCommonvein.net lungs-0769b

Chronic eosinophilia is characterised by alveolar filling with eosinophils and inflammatory exudates(a) and interalveolar interstitial thickening, (overlaid in red in b). The infiltrates are classically peripherally positioned, usually upper lobes, more commonly bilateral but can be unilateral, and manifest as consolidation and or ground glass opacities. The CT shows bilateral peripheral consolidations in the upper lobes
Ashley Davidoff MD The CommonVein.net lungs-0775-e

Chronic eosinophilia is characterised by alveolar filling with eosinophils and inflammatory exudates(a) and interalveolar interstitial thickening, (overlaid in red in b). The infiltrates are classically peripherally positioned, usually upper lobes, more commonly bilateral but can be unilateral, and manifest as consolidation and or ground glass opacities. The CT shows bilateral peripheral consolidations in the upper lobes
Ashley Davidoff MD The CommonVein.net lungs-0775e

Subpleural Sparing
Ashley Davidoff MD TheCommonvein.net lungs-0775 0775-lo res subpleural sparing

As the disease progresses the lower disease becomes more extensive and the disease progresses into the periphery of the upper lobes as well
Ashley Davidoff MD TheCommonvein.net lungs-0769c
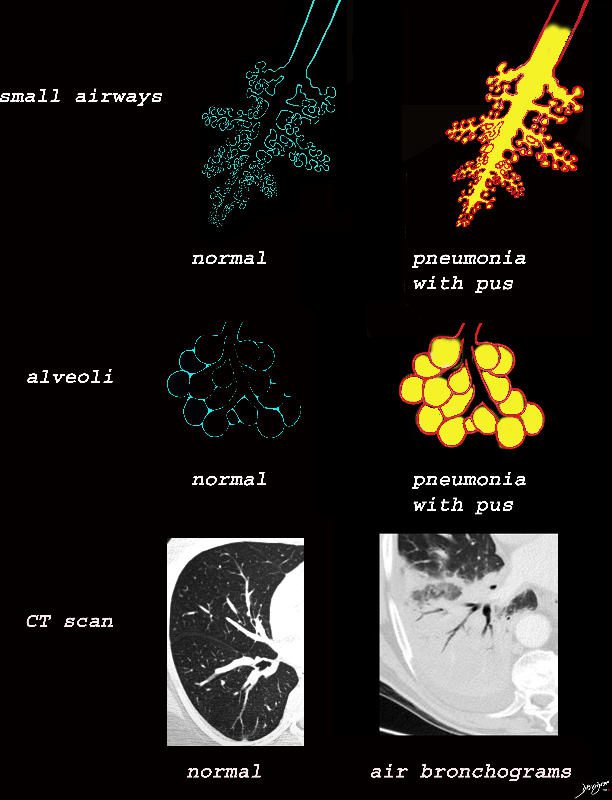
The collage provides a perspective of purulent accumulation in the small airways and the alveoli that results in consolidation. A process that increases the density of the lungs to a net “white” regional density will result in a consolidation and in this case when the fluid is infected it is labelled “pneumonia” The net result on CT is air bronchograms within the non aerated dense lung tissue.
Ashley Davidoff MD TheCommonVein.net lungs-0734
Ashley Davidoff MD TheCommonVein.net lungs-0733
Ashley Davidoff TheCommonVein.net lungs-0755
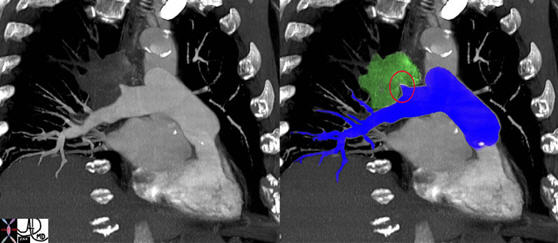
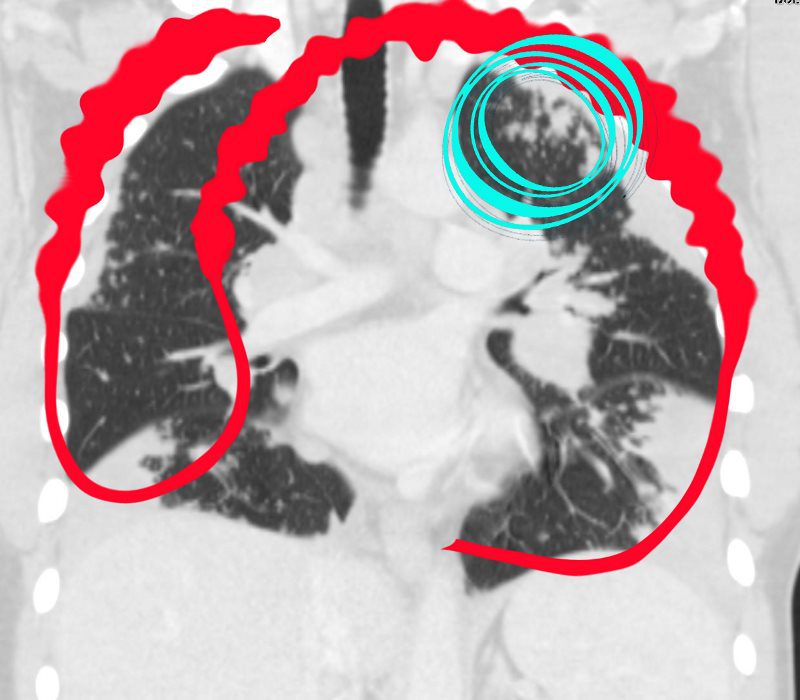
The coronal image shows a centrally placed small cell carcinoma (green mass in right image) occluding the right upper lobe pulmonary artery (red ring).
Images courtesy: Ashley Davidoff, M.D. TheCommonVein.net Lung cancer P 025
000 HP
Ashley Davidoff MD TheCommonvein.net lungs-0732b01

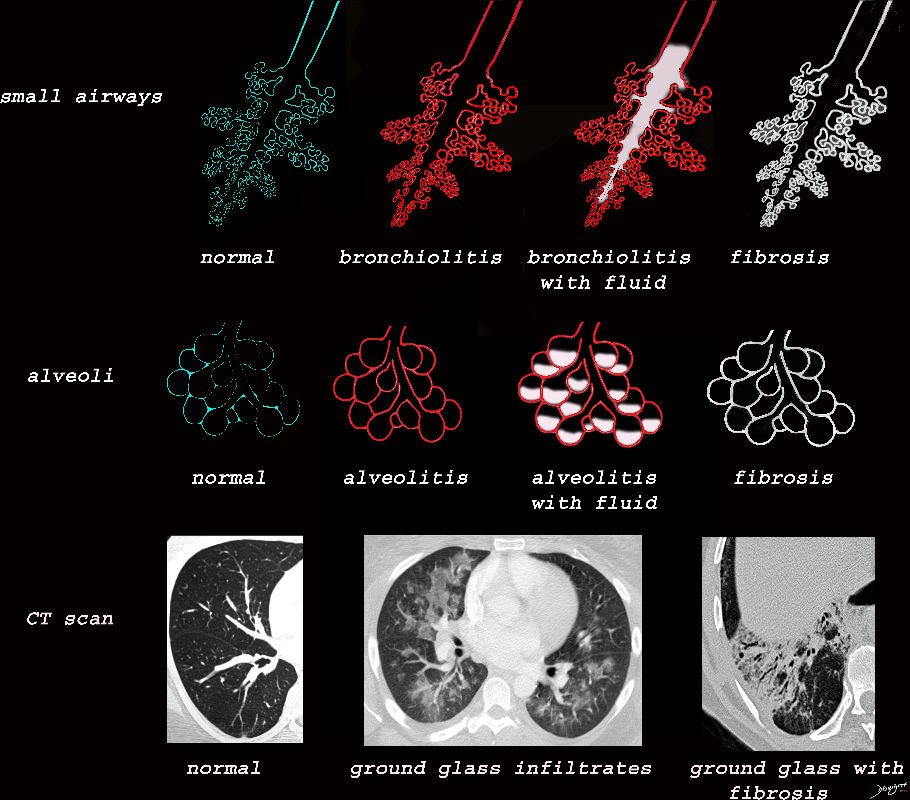
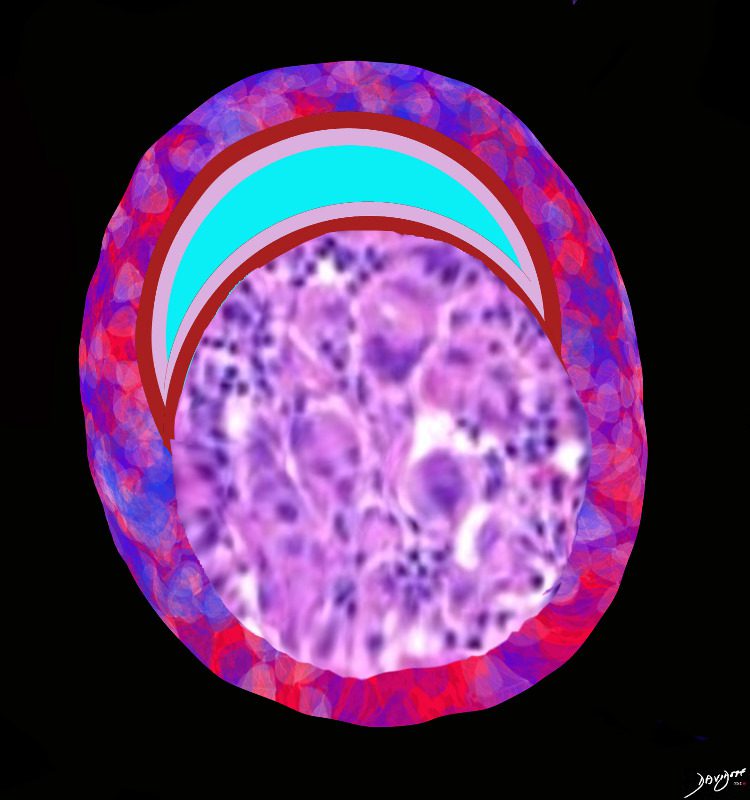
Ground glass opacification may be caused by partial filling of the alveolus with cellular material with partial replacement of air with solid material with the net density being gray rather than white if the alveolus were fully filled. The black of the airway nor the white of the vessels may blend with the gray density and hence they are not visualised in ground glass opacities. The replacement may be due to cellular infiltration including inflammatory ,benign or malignant cells without or with fluid.
Ashley Davidoff MD TheCommonVein.net lungs-0707ad

Ashley Davidoff MD TheCommonVein.net lungs-0702d- lo res
Black White and Gray Densities
The filling of alveoli with fluids or cells results in a density that is ?white? on X-ray and CT scan and is in distinct contrast to the black of the air filled airways. This contrast results in an air bronchogram. The smaller airways in a normal patient are not usually visualized because the ?black? of the of the airways and the black of the air filled alveoli does not create a contrast.
Ashley Davidoff MD TheCommonvein.net
lungs-0708d

Consolidation is the replacement of air with solid material resulting in obscuration of blood vessels and airway walls The replacement may be due to cellular infiltration including inflammatory ,benign or malignant cells without or with fluid.
Ashley Davidoff MD TheCommonVein.net
lungs-0707d- lo res

Ashley Davidoff MD TheCommonVein.net
lungs-0704d

Ashley Davidoff MD TheCommonVein.net
lungs-0705d- lo res

Inflammatory fluids half fill the alveolus and will therefore result in ground Glass Infiltrates
Ashley Davidoff MD TheCommonVein.net
lungs-0703d

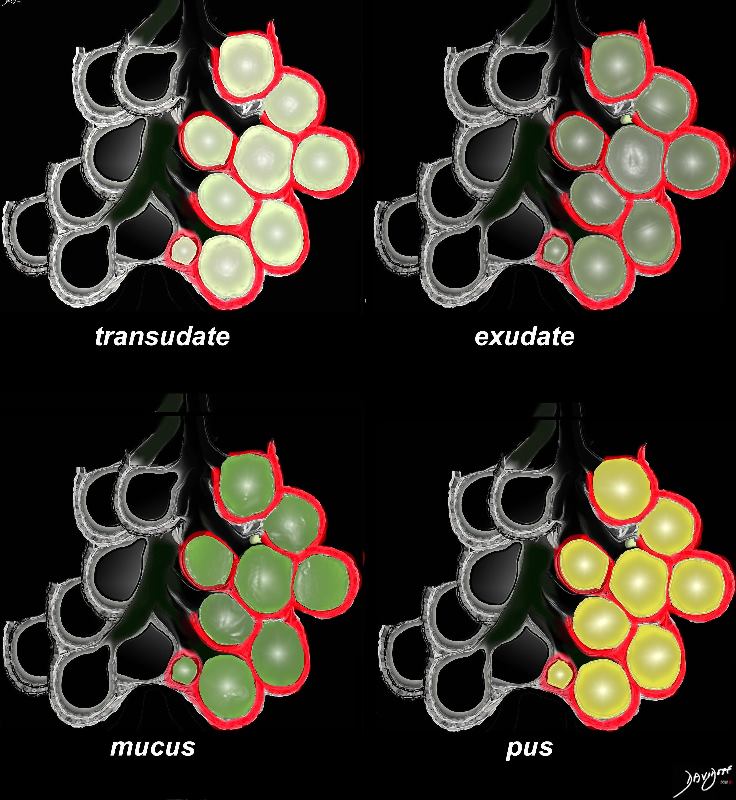
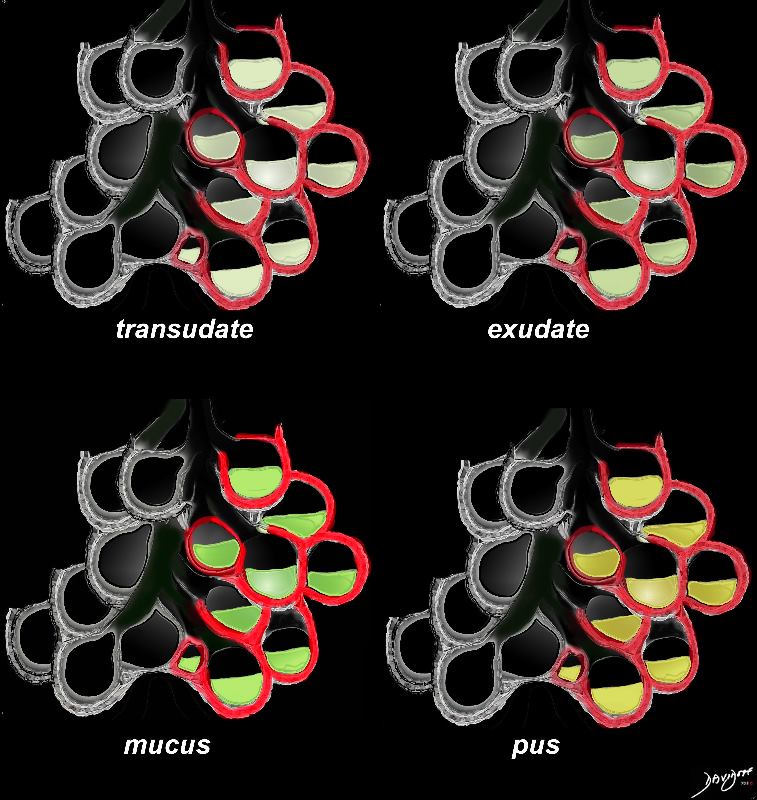
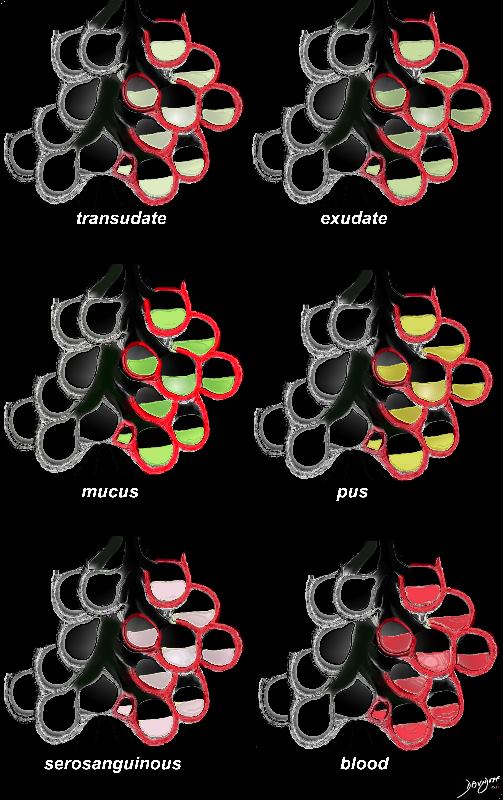
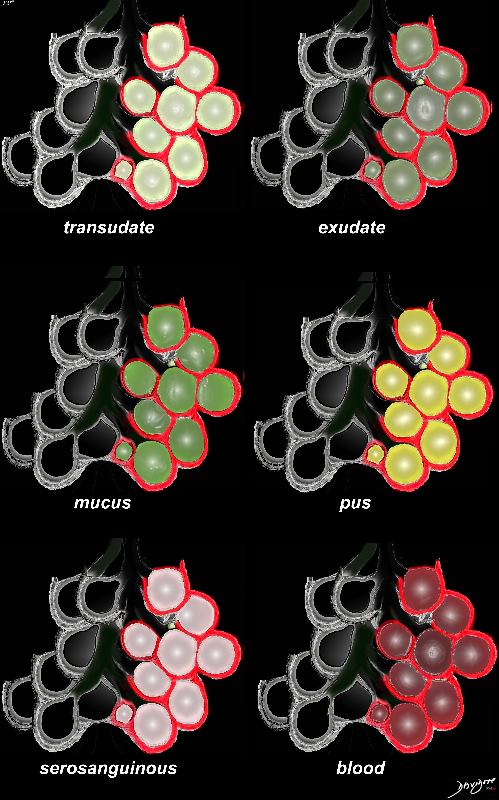
The acute inflammatory process results in fluid exudation into the alveoli which can take the form of a serous transudate, and exudate or in the form of mucus, and when severe (eg ARDS) can result in tissue and vessel destruction and could be be blood tinged. Infected fluid could be mucoid or purulent. The extent of filling the alveoli results either in a ground glass appearance when partially filled or a consolidation when filled.
Ashley DAvidoff MD TheCommonVein.net
lungs-0701d- lo res
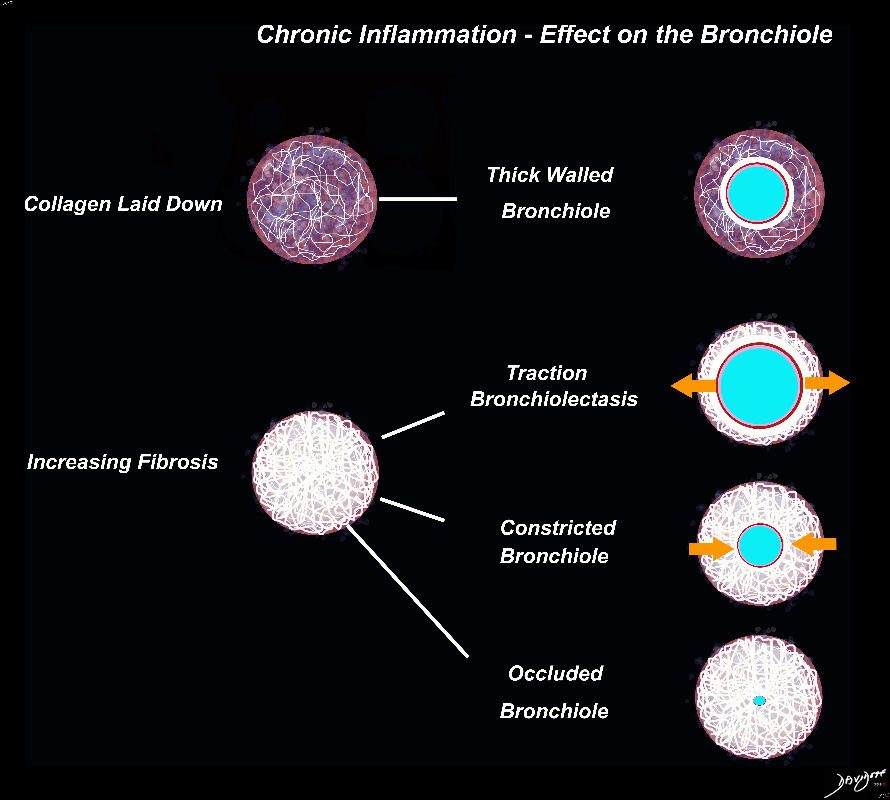
I the early phases collagen starts to get laid down resulting in a thick walled bronchiole surrounded by a subacute inflammatory response of cells and resolving fluid. As the fibrotic process advances it gets denser resulting in traction bronchiectasis and bronchiolectasis. The ongoing may eventually constrict the airway and subsequently occlude occlude the airway
Ashley Davidoff MD TheCommonVein.net lungs-0700d
Acute Inflammation

Ashley Davidoff MD TheCommonVein.net lungs-0698d

Ashley Davidoff MD TheCommonVein.net lungs-0698
000 Fibrotic Disease

Ashley Davidoff MD TheCommonVein.net Chronic Inflammation ? The Basics
Ashley Davidoff MD TheCommonVein.net lungs-0699d

Ashley Davidoff MD TheCommonVein.net lungs-0700
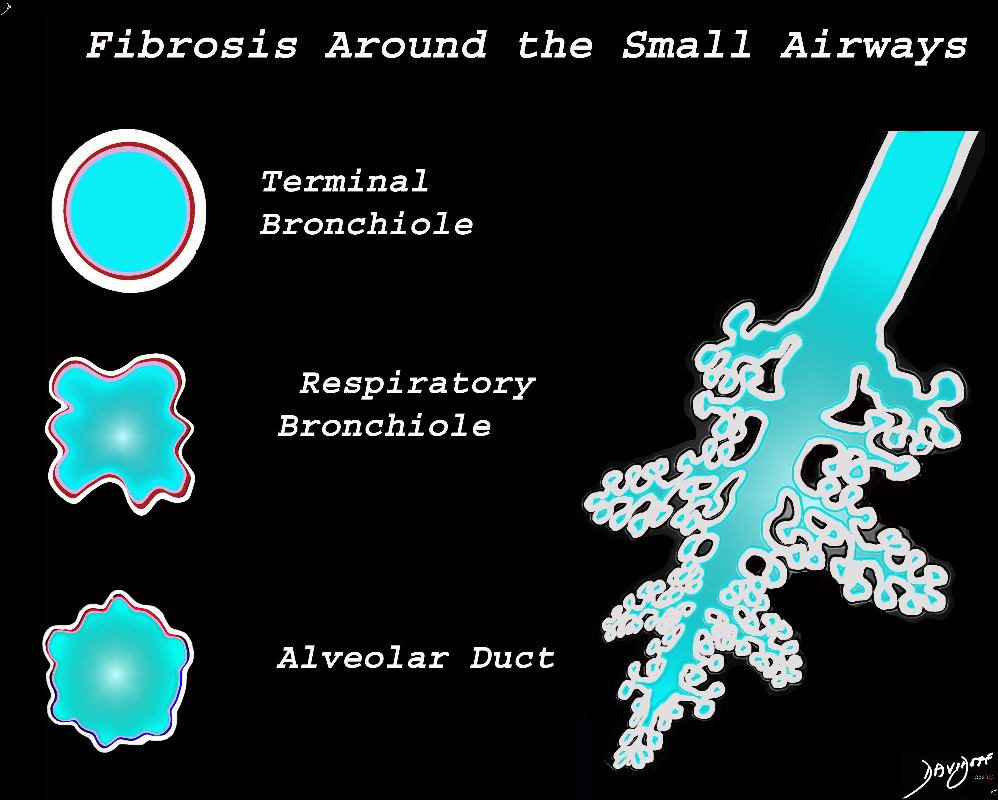
The diagram shows fibrotic changes around the small airways including the terminal bronchiole, respiratory bronchiole and the alveolar duct. In this instance the increase density from the fibrotic tissue would result in ground glass changes in the parenchyma and ground glass centrilobular nodules. Since the airways are patent there would be no air trapping.
Ashley Davidoff MD TheCommonVein.net lungs-0777
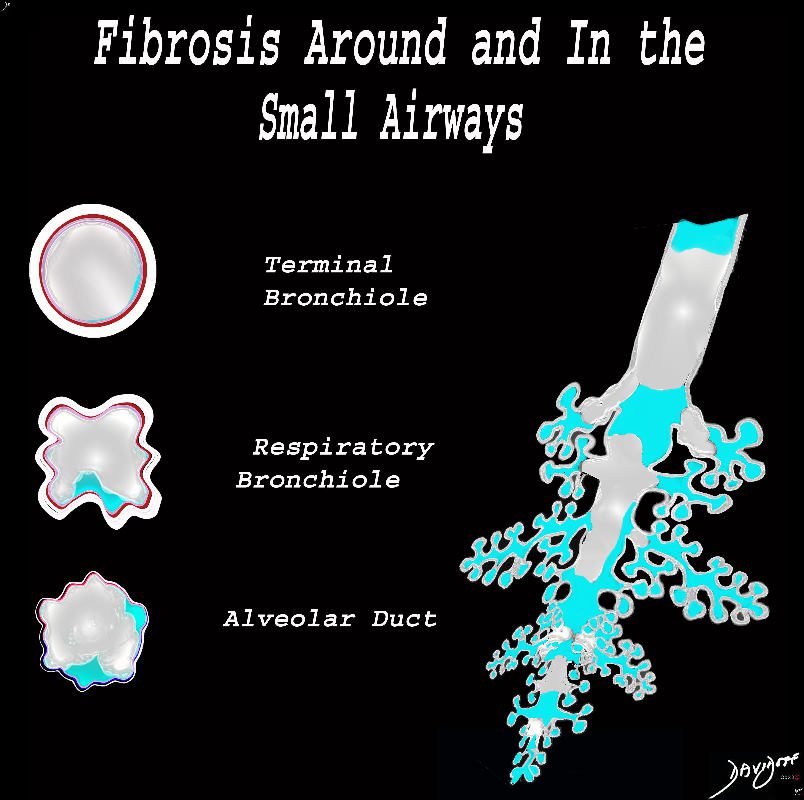
The diagram shows fibrotic changes around and within the small airways including the terminal bronchiole, respiratory bronchiole and the alveolar duct. In this instance the increase density from the fibrotic tissue would result in ground glass changes in the parenchyma and solid centrilobular nodules. Obstruction of the small airways would result in air trapping.
Ashley Davidoff MD TheCommonVein.net lungs-0778
Ashley Davidoff TheCommonVein.net
lungs-0738b
000 Granulomatous Diseases
Ashley Davidoff MD
TheCommonvein.net

Ashley Davidoff The Common Vein.net

Ashley Davidoff MD TheCommonVein.net lungs-0731
Ashley Davidoff MD TheCommonVein.net lungs-0729
000 Cancer
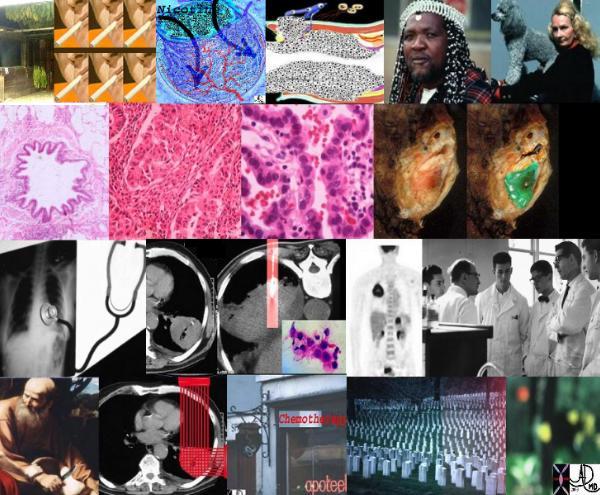
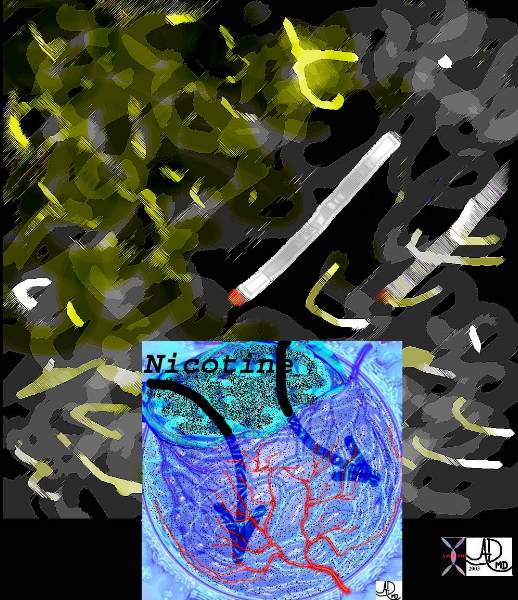
This is the story of lung cancer, (left top) from the tobacco leaves of Virginia, to the cigarette, a nicotine filled alveolus, repeated contact with epithelium, and malignant proliferation with compromise of the lumen. People of all types affected by the curse of smoke. The histology may be of the non small cell or the small cell type, but in either case malignant and space occupying. A cough is common with the clinical presentation and a mass frequent on CT. Biopsy follows with staging by PET scan, multidisciplinary conference, and therapeutic choices ? surgery, radiation and or chemotherapy. Mortality is usually inevitable with this devastating disease, but there is always hope for a cure in early stages.
Ashley Davidoff
TheCommonVein.net
10296cc
keywords lung pulmonary disease introduction collage people grosspathology smoking
Ground Glass Opacity (GGO) Caused by Cellular Accumulation with Partial Filling of the Alveolus Ground glass opacification may be caused by partial filling of the alveolus with cellular material with partial replacement of air with solid material with the net density being gray rather than white if the alveolus were fully filled. The black of the airway nor the white of the vessels may blend with the gray density and hence they are not visualized in ground glass opacities.
Ashley Davidoff MD TheCommonVein.net lungs-0707a
The Ground Glass Opacity (GGO) in this case is caused by partial filling of the alveolus with malignant cells Ground glass opacification may be caused by partial filling of the alveolus with cellular material resulting in partial replacement of air with solid material. The net density is gray rather than white in the situation where the alveolus is fully replaced with cells or fluid. There is blending of the black of the subtending airways and the white of the vessels with the gray density of the cellular infiltrate and hence the normal vessels are not visualized in ground glass opacities.
Ashley Davidoff MD TheCommonVein.net 134375b01

Ashley Davidoff MD TheCommonVein.net lungs-0707

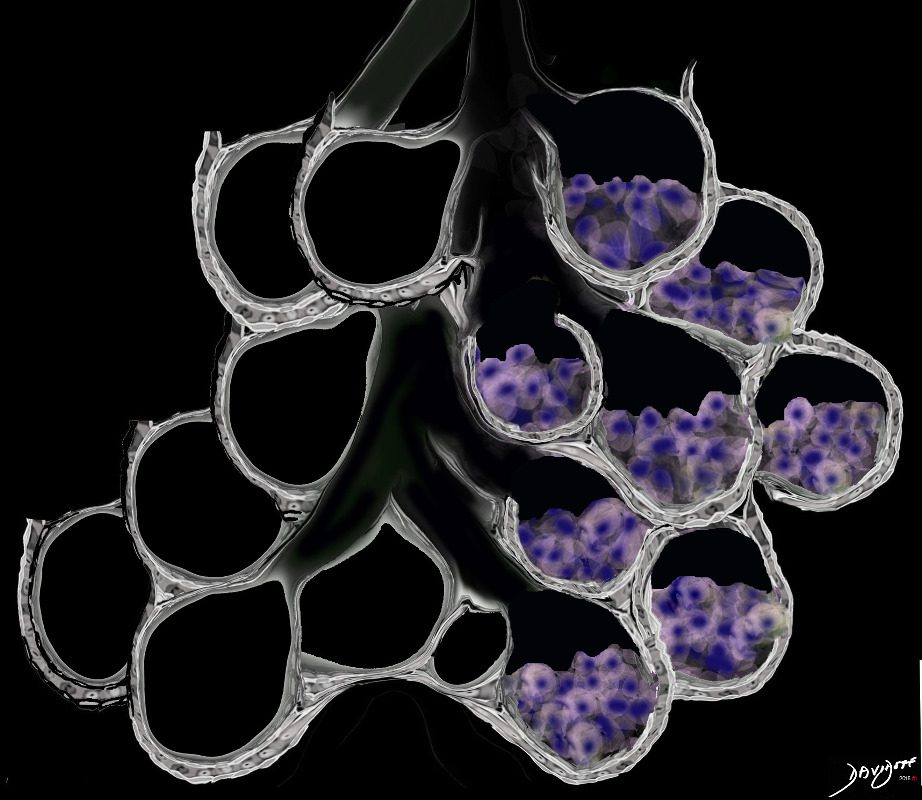
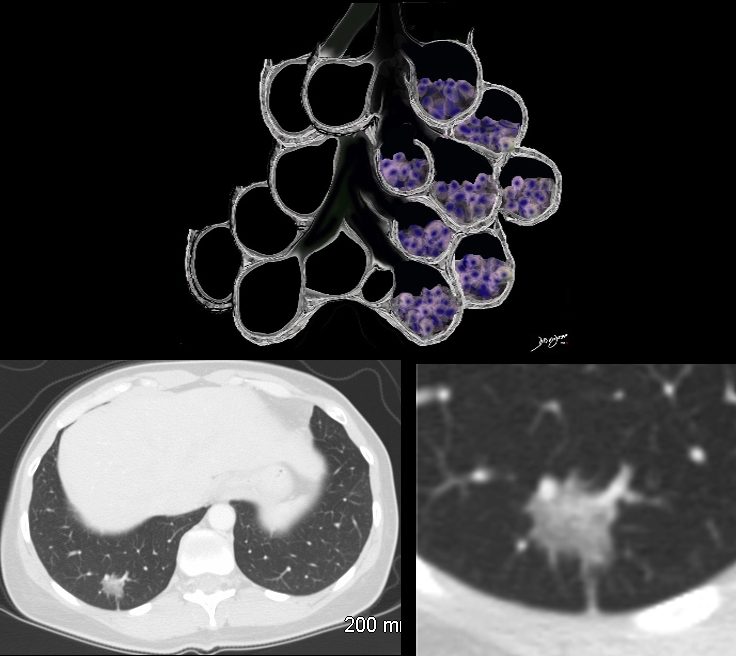
The focal nodules (middle row) and segmental consolidation in the right upper lobe (lower row) in this case is caused by total filling of the alveoli with malignant cells. This results in opacification of the alveoli and the “white” density in contrast to the “black” airways, enable the airways to be visualised as air bronchograms
Ashley Davidoff MD TheCommonVein.net 87770c01
000 Inflammation Infection
Ashley Davidoff MD TheCommonVein.net
Inflammatory fluids half fill the alveolus and will therefore result in ground Glass Infiltrates
Ashley Davidoff MD TheCommonVein.net
Ashley Davidoff MD TheCommonVein.net
Types of Fluid Accumulation in the Alveoli
The acute inflammatory process results in fluid exudation into the alveoli which can take the form of a serous transudate, and exudate or in the form of mucus, and when severe (eg ARDS) can result in tissue and vessel destruction and could be be blood tinged. Infected fluid could be mucoid or purulent. The extent of filling the alveoli results either in a ground glass appearance when partially filled or a consolidation when filled.
Ashley Davidoff MD TheCommonVein.net
lungs-0701
transudate-exudate-mucus-blood-tinged-pus-fluids-in-the-alveoli-L-scaled.jpg
Ashley Davidoff MD TheCommonVein.net
Ashley Davidoff MD TheCommonVein.net lungs-0704
000 Radiology
000 Consolidation
Black White and Gray Densities
The filling of alveoli with fluids or cells results in a density that is ?white? on X-ray and CT scan and is in distinct contrast to the black of the air filled airways. This contrast results in an air bronchogram. The smaller airways in a normal patient are not usually visualized because the ?black? of the of the airways and the black of the air filled alveoli does not create a contrast.
Ashley Davidoff MD TheCommonvein.net
lungs-0708

Ashley Davidoff MD TheCommonVein.net lungs-0699

Ashley Davidoff MD TheCommonVein.net lungs-0728b

Ashley Davidoff MD TheCommonVein.net lungs-0728b -hi res

Ashley Davidoff MD TheCommonVein.net lungs-0726

Ashley Davidoff MD TheCommonVein.net lungs-0725

Ashley Davidoff MD TheCommonVein.net lungs-0724

Ashley Davidoff MD TheCommonVein.net lungs-0724b

Ashley Davidoff MD TheCommonVein.net lungs-0723b

Ashley Davidoff MD TheCommonVein.net lungs-0723
Ashley Davidoff MD TheCommonVein.net lungs-0722

Ashley Davidoff MD TheCommonVein.net

Ashley Davidoff MD TheCommonVein.net lungs-0707
Ashley Davidoff MD TheCommonVein.net lungs-0702

Ashley Davidoff MD TheCommonVein.net lungs-0701
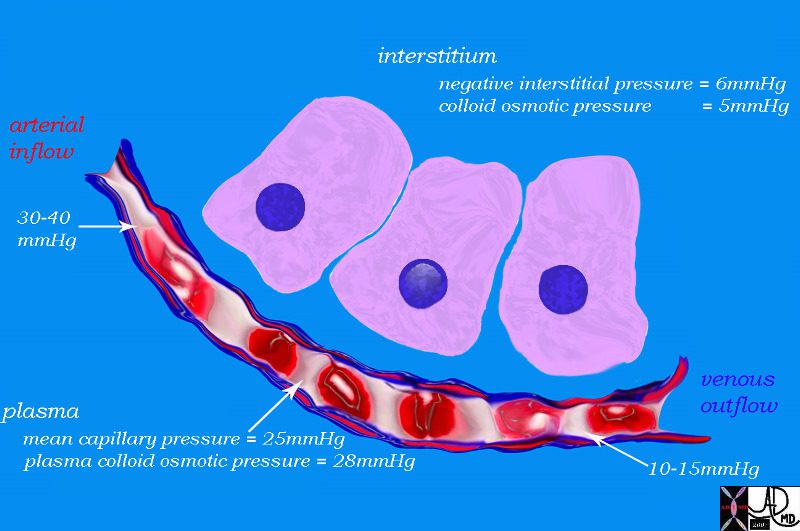
The fluid thus will move from the capillaries into the interstitium
Ashley Davidoff MD The CommonVein.net 42445b03d06

Ashley Davidoff MD TheCommonvein.net lungs-0056

Ashley Davidoff MD TheCommonVein.net lungs-0057
Ashley Davidoff MD TheCommonVein.net
lungs-0700
42530b05b08.jpg
Art of the Sternum and Costochondral Junctions and Soft Tissues and Upper LimbsAshley Davidoff MD TheCommonVein.net
42530b08

Ashley Davidoff MD TheCommonVein.net
42530b04

Ashley Davidoff MD TheCommonVein.net
42530b02

This artistic rendition of the small parts of the lung shows the beginning of the peripheral system just before it enters the acinus. This duct is called the terminal duct and it is the last part of the ductal system that has no ability for gas exchange. After its first division, the bronchioles become the respiratory bronchioles, and they are the first in the system to have an ability to both transport the gases as well as enable gas exchange.
Ashley Davidoff TheCommonVein.net
lungs- lo res 0002

Ashley Davidoff MD TheCommonVein.net lungs-0059

Ashley Davidoff MD TheCommonVein.net lungs-0058
Ashley Davidoff MD TheCommonVein.net lungs-0699
Ashley Davidoff MD TheCommonVein.net lungs-0698
lungs-0021catalogue-signed-smallb.jpg
Inflamed AlveoliAshley Davidoff MD TheCommonvein.net lungs-0021

This cupola or dome was photographed in the church of the Villa Melzi gardens in Bellagio, Italy. If you imagine yourself in the chest cavity and you look up towards the neck, this is what you will see ? the dome shaped structure of the apex of the lung and pleura.
Ashley Davidoff TheCommonVein.net 78115pb01

Ashley Davidoff TheCommonVein.net . 22071b01.800

Two leaves of the coleus plant, with a pyramidal or conical shape that reminded the photographer of a set of lungs. The branching system originates from the hilum of the leaf almost at its center, but unlike the tracheobronchial tree it is not irregularly dichotomous.
Ashley Davidoff TheCommonVein.net . 42643
The chest quietly expands and contracts under basal conditions in order to serve the alveoli. At first glance it seems like a simple bellows-like process, but as one delves into the layers of detail, the complexity of the structural design unfolds as a combination of physical and chemical forces.
Ashley Davidoff MD TheCommonVein.net 42530b05b09b28
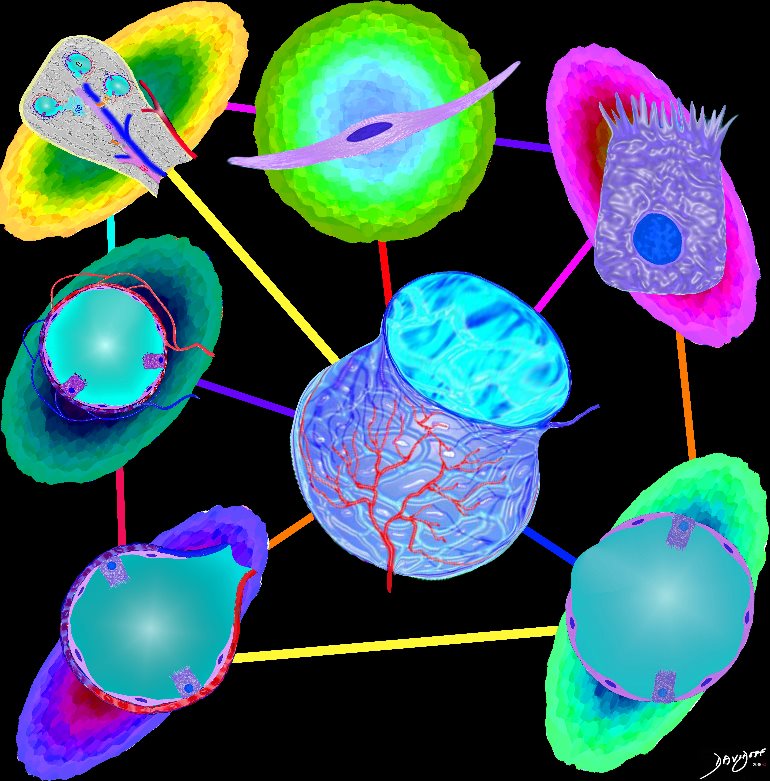
The image shows some of the major components of the lung that when bonded create a new and powerful unit – a vital organ. In the center is an example of the airways and parenchyma making up the 2 lungs. At 12 oclock the tracheo-bronchial tree with segmental and subsegmental airways. At 1 o?cloclock, is a cross section of the lungs showing some of the segments of the lung. At 5o?clock a cross section shows the arteries and veins of the lungs. At 7o?clock the drawing shows the pleura and pleural space of the lungs. At 9o?clock, a coronal reformat of the tracheobronchial tree shows the lymph node stations of the lungs. At 11 o?clock is the golden alveolus, the epicentral unit where gas exchange takes place
Ashley Davidoff MD TheCommonVein.net lungs-0696

The axial CT through the level of the heart shows a few of the right and left pulmonary segments including parts of the middle lobe, lingula and of the lung bases
Ashley Davidoff MD TheCommonVein.net 32557bb03.8s
Normal 3D reconstruction of a CT scan of the Heart Showing the Left Atrium and Pulmonary Veins
Ashley Davidoff MD TheCommonVein.net
77612b.3kb07.8s

The white arrow points to the potential path of a needle to a lesion in the liver. To the observer it would seem low and out of range of the pleura and lung. Since the costophrenic sulcus would not be visible to ultrasound nor CT interrogation it is difficult to know exactly where it lies. One just has to knowthat it may lie quite low, and that on inspiration the lung may in fact fill that space as well. Hence the potential complications include a pneumothorax from this approach, and if long term catheter drainage is contemplated transgression of the pleural space may cause an effusion or an infection resulting in an empyema.
Ashley Davidoff MD TheCommonVein.net 32634b15

The inferior aspect of the left lung base is magnified in this image s. It shows the costophrenic sulcus where the visceral pleura is absent and two layers of parietal pleura face each other. Ashley Davidoff MD TheCommonVein.net 32634b11b04b
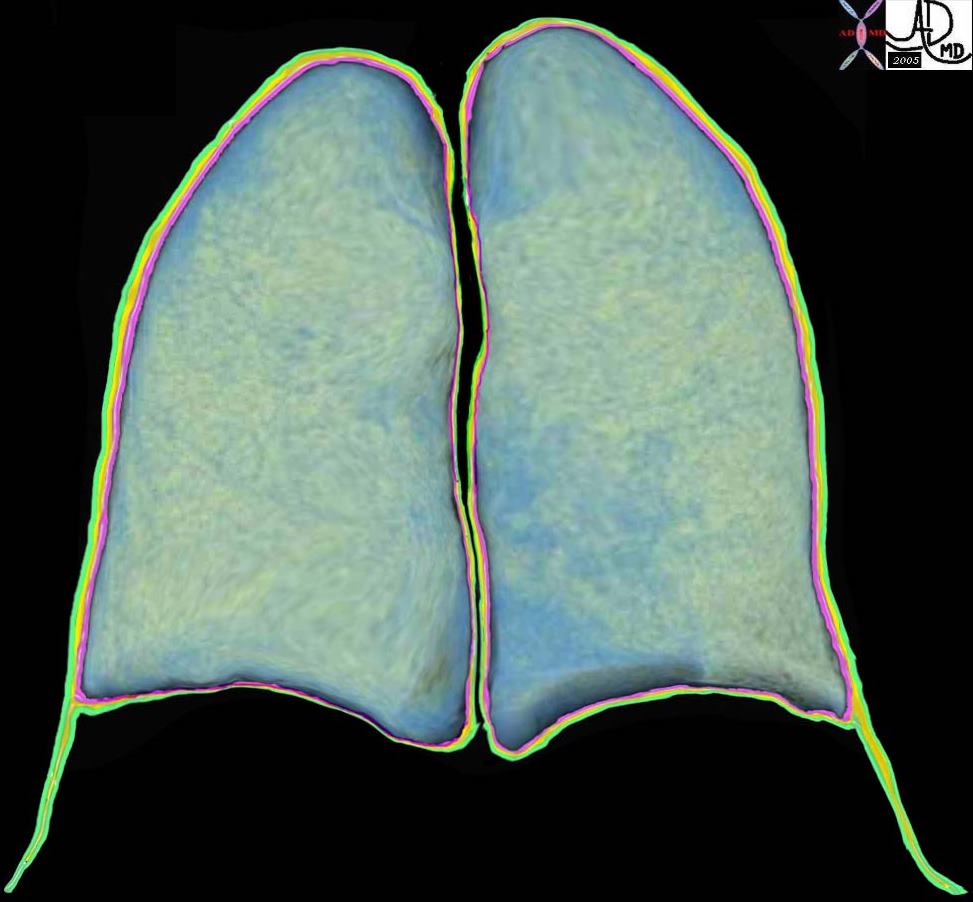
The coronally reformatted image of the lung parenchyma has been outlined with the visceral pleura, (pink) the pleural fluid in the pleural space, (orange) and the parietal pleura. (green) Note how at end expiration the parietal pleura in the costophrenic sulcus extends beyond the lung margin so that the visceral pleura is absent in the costophrenic sulcus and there are two layers of parietal pleura facing each other. During inspiration the lung expands into this space. 32634b10
Key Words lung pleura pulmonary
Ashley Davidoff MD TheCommonVein.net

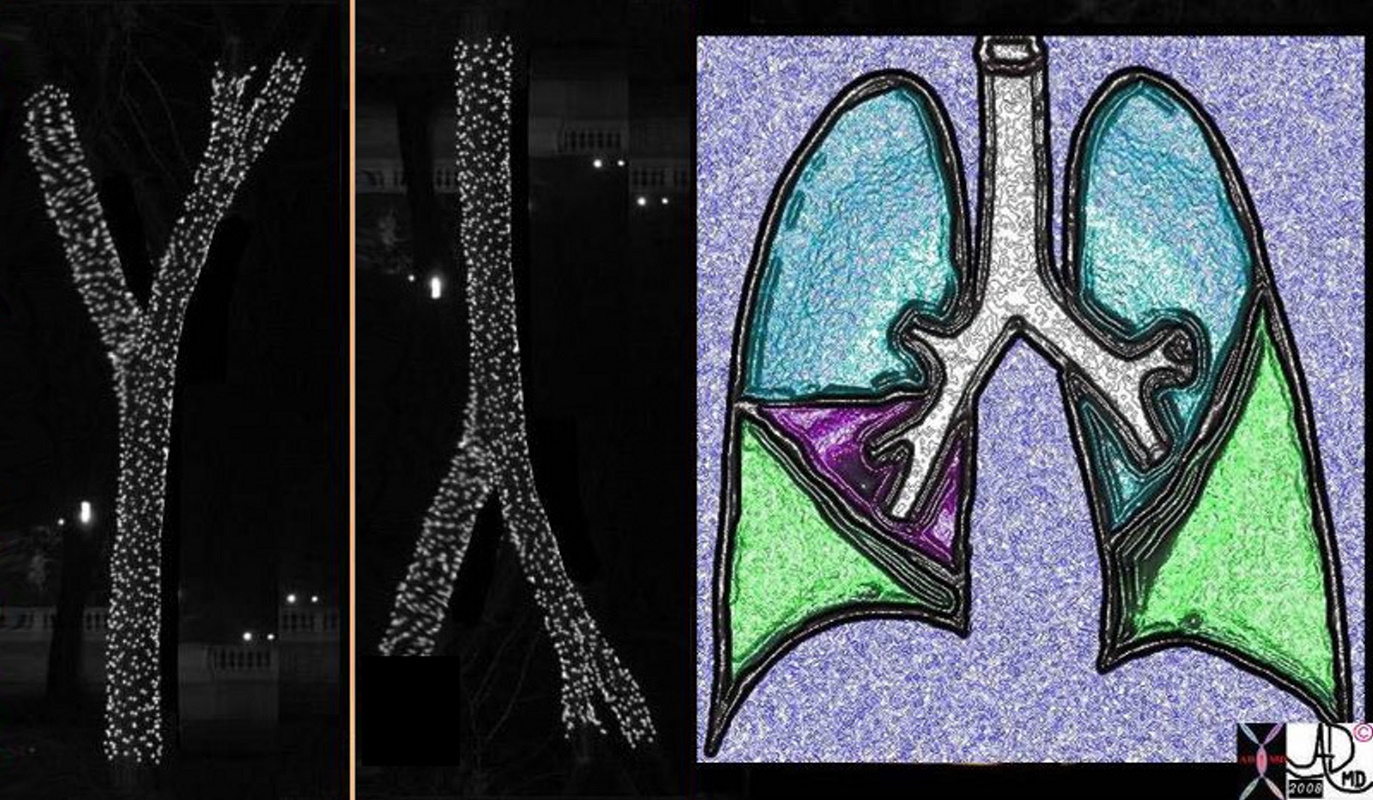
This is a drawing is of a left lung in coronal section. Note there are only two lobes separated by the major fissure
Courtesy Ashley Davidoff MD The CommonVein.net 32686b05L01
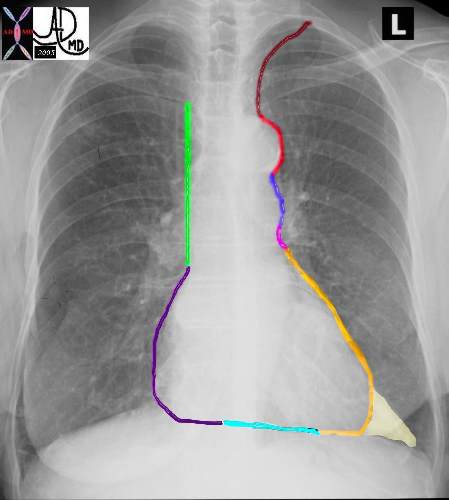
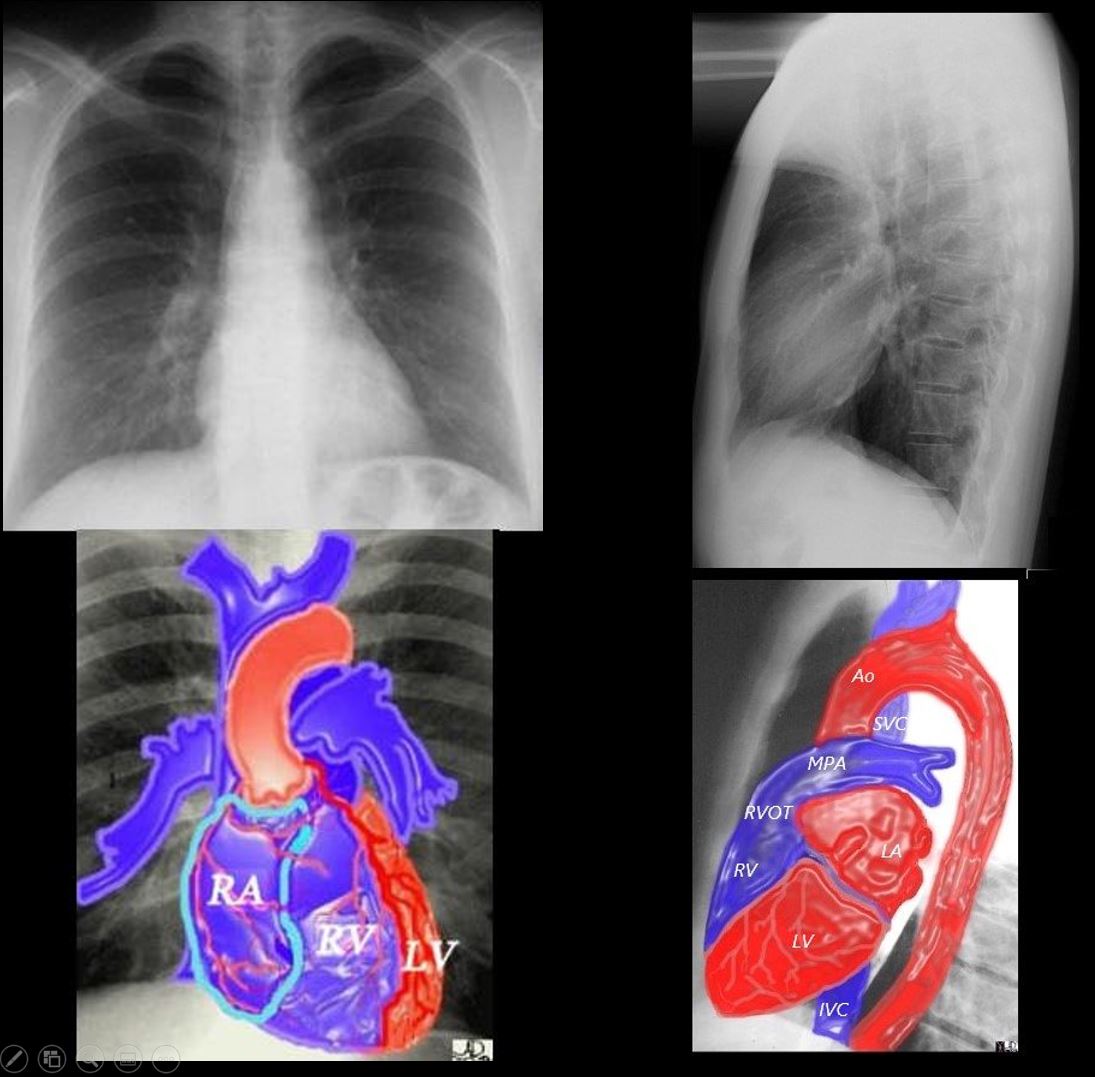
Start with the left slope at the apex of the left lung. After you get off the ski-lift, follow the signs to the ?Subclavian Steel? which is painted in dark maroon ? just like blood. You will gain speed very quickly off this slope which starts with the subclavian artery. This is the most dangerous of the slopes since you are almost upside down as you start. As you gather speed come across the bump of the aorta. This trail is called the ?Aortic Notch? and its sign is colored in bright red. ? This trail holds the biggest mogul. A shallow mogul of the MPA (?Lung Artree? dark blue) comes next, and then a concave in pink for the left atrial appendage. ?Pretty Pendage? (short lived) After that it is a great mild and long slope of the orange LV (?Smooth Elvee?) until you pass alongside the triangular fat pad of the LV.
The second slope on the right starts near the apex of the right lung and is marked with a bright green sign called ?vein cave? As you step off the lift ? there is a ninety degree drop, and if you look to your left you will see the red cells in the superior vena cava traveling much slower than you. After the ?vein cave? route, the gentle curve around the right atrium (purple) takes over and you are brought to an almost negligible slope of the right ventricle. (teal) The right and left slope meet at the bottom by the ski house.
Ashley Davidoff MD TheCommonVein.net 42260bb01

This diagram shows the segmental branches of the right bronchial system. The RUL has three branches, the apical, posterior and anterior segments. (teal overlay) The middle lobe has two segmental branches called lateral and medial segments. (pink) The right lower lobe has five: the superior, anterior basal, lateral basal, posterior basal and medial basal segments. Ashley Davidoff MD. TheCommonVein.net 32686b03
Ashley Davidoff TheCommonVein.net 42438b03
key words mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage neoplasm malignancy benign obtuse angles with the lumen circumferential narrowing constriction obstruction histopathology imaging diagnosis
Ashley Davidoff TheCommonVein.net 32347d06
32347d04 key words mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage neoplasm malignancy benign obtuse angles with the lumen histopathology imaging diagnosis
Ashley Davidoff TheCommonVein.net 32347d04
32347d03 key words mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage obtuse angles or right with the lumen histopathology imaging diagnosis Ashley Davidoff TheCommonVein.net 32347d03

Normal chest CT of the upper lobes of both lungs. The trachea is horse shoe shaped.
Ashley Davidoff TheCommonVein.net 32158 42636c01
32347d02 key words mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage obtuse angles or right angle 90 degree ninety degree angle with the lumen histopathology imaging diagnosis
Ashley Davidoff TheCommonVein.net 32347d02

32347d01 key words mucosa submucosa muscularis adventitia serosa mucosal mass polyp neoplasm carcinoma acute angles with the lumen histopathology imaging diagnosis Ashley Davidoff TheCommonVein.net 32347d01

This image shows the arteriole (royal blue) and the bronchiole (teal) travelling side by side bith of equal size. Ashley Davidoff MD TheCommonVein.net 42440b05
This cross sectional drawing shows the pulmonary artery in royal blue, pulmonary veins in red and the bronchi in teal. At the most central portion of each hilum there are usually 2 veins, one artery and one bronchus. This is because the length of the bronchus and artery prior to division is relatively long, while the confluence of the veins is close to the entrance into the left atrium. Thus the superior veins from the upper lobes are anterior and the veins to the inferior lobes are posterior. Courtesy Ashley Davidoff MD TheCommonVein.net 31592

Ashley Davidoff thecommonvein.net
Ashley Davidoff thecommonvein.net

Ashley Davidoff
TheCommonVein.net

Ashley Davidoff
TheCommonVein.net

Ashley Davidoff
TheCommonVein.net lungs-0695



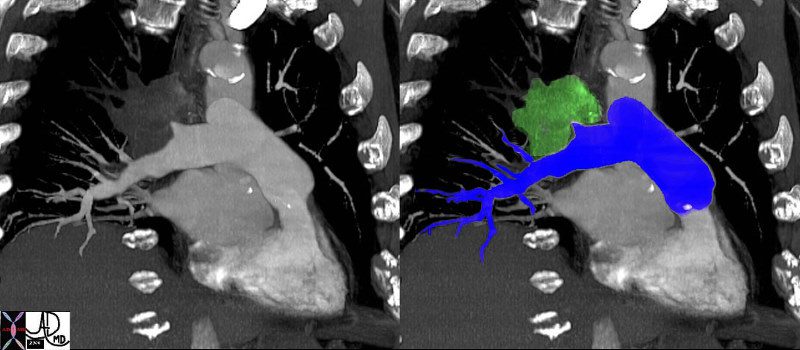
The coronal image shows a centrally placed small cell carcinoma (green mass in right image) occluding the right upper lobe pulmonary artery. (red ring)
Courtesy Ashley Davidoff MD.
TheCommonVein.net
46645c04.

A collage of food from the farming to the picking packaging and the eating ? Who knows what is finally in the final multifaceted complex product that has so much effect on our health ? ?We are what we eat!?
Ashley Davidoff
TheCommonVein.net
10376c

This is a collage of people in London, Johannesburg, New York and Boston. Did you notice the similarity of the poodle and the blonde lady?
Ashley Davidoff
TheCommonVein.net
10369c

This is a collage showing the evolution of a malignant cell (1) into a nodule restricted to the epithelium (2) which with time penetrates the basement membrane and progressively extends into the submucosa and muscularis (3). Subsequent extension into local lymph nodes and blood vessels occurs (4) as well as growth into the lumen. As it grows circumferentially, narrowing and eventually obstruction of the lumen complicates the process (5) Space in tubular systems is limited and malignant growth has no respect for this space nor for boundaries. By definition malignant disease is space occupying.
Ashley Davidoff
TheCommonVein.net
32336c

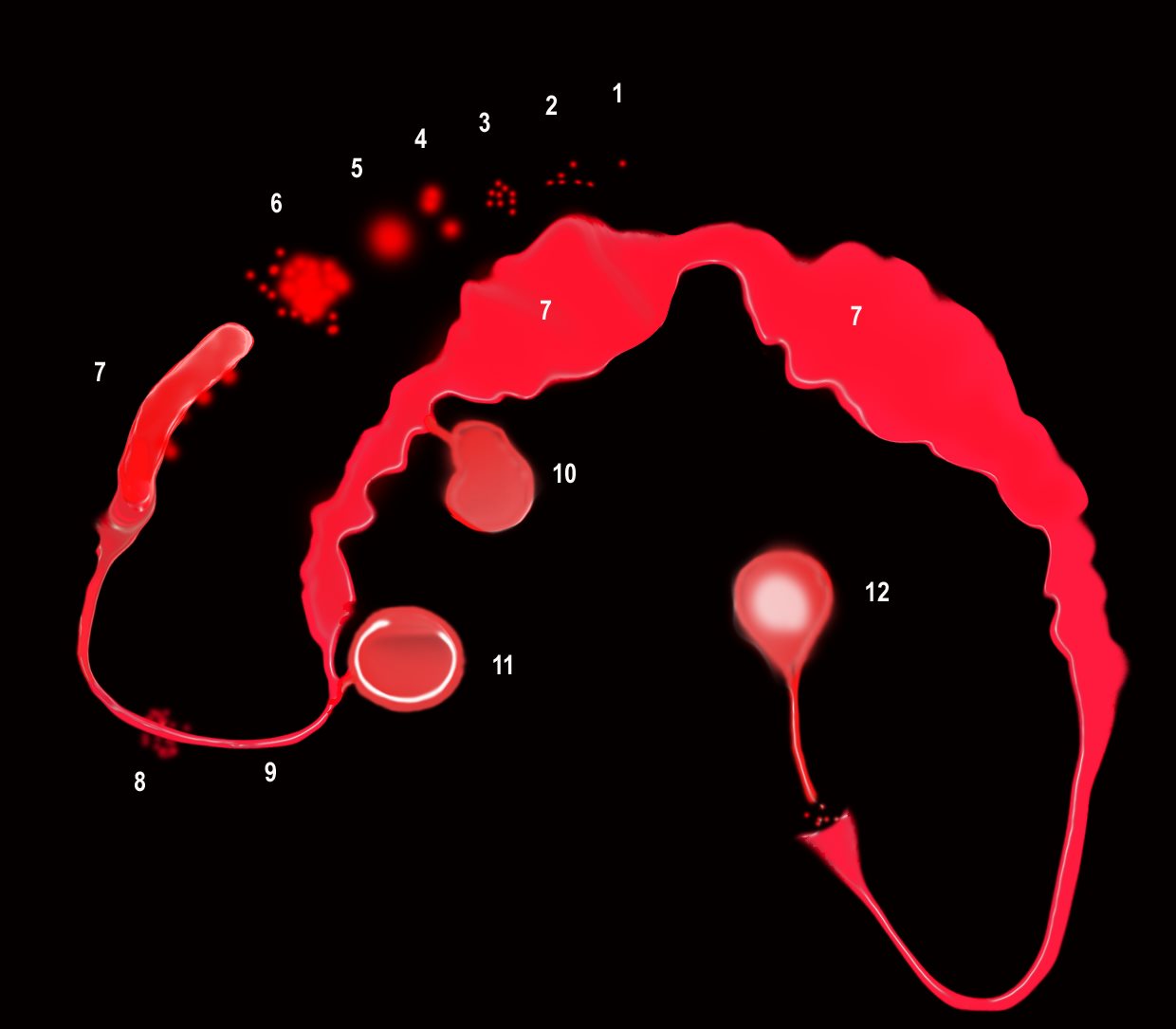
There are Aortic Nodes 5 Subaortic Nodes (A-P window) 6 Paraaortic Nodes (Ascending Aorta or Phrenic) Inferior Mediastinal Nodes 7= subcarinal nodes 8=Paraesophageal Nodes 9 = Pulmonary Ligament Nodes 10 Hilar Nodes 11 Interlobar Nodes 12 Lobar Nodes
Ashley Davidoff
TheCommonVein.net
32682n04.801

This artistic rendition of the small parts of the lung shows the beginning of the peripheral system just before it enters the acinus. This duct is called the terminal duct and it is the last part of the ductal system that has no ability for gas exchange. After its first division, the bronchioles become the respiratory bronchioles, and they are the first in the system to have an ability to both transport the gases as well as enable gas exchange.
Ashley Davidoff
TheCommonVein.net
32645b04b05.8s

This diagram shows the basic division of the tracheobronchial tree into lobes. The right lung is divided into right upper (RUL) (teal) right middle, (RML pink) and right lower lobe (RLL green). The left lung is divided into left upper (LUL teal), which includes the lingula(dark blue), and left lower lobe (LLL= green). Note that the two mainstem bronchi are of unequal length and size. The right mainstem is short and fat while the left is long and thin. This irregular dichotomous branching pattern is characteristic of the branching pattern of all the conducting systems within the lungs.
Ashley Davidoff
TheCommonVein.net 32686b05

A hyaline membrane evolves covering the damaged surface of the alveolus. This impedes gas exchange
Ashley Davidoff
TheCommonVein.net lungs-0694

The damage to the endothelium of the capillary results in bleeding into the alveoli. The severe tissue damage and fluid exudation results in protein rich intra-alveolar fluid . The fibroblasts start to lay down collagen as part of the early repair process
Ashley Davidoff
TheCommonVein.net lungs-0693
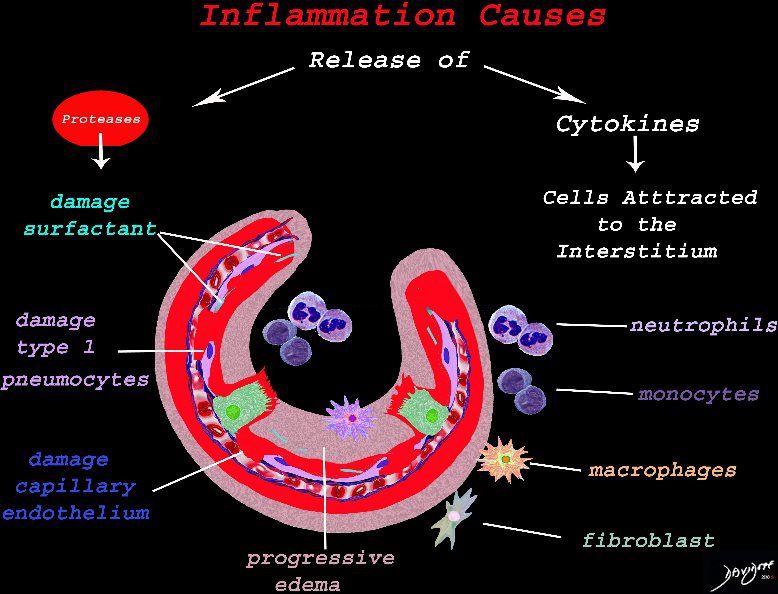
The cells of the immune system release cytokines, chemotactic agents and proteases. Immune cells , macrophages and fibroblasts are attracted to the interstitium. Some of proinflammatory agents are toxic to the cell lining causing damage to the surfactant, type 1 pneumocytes and the capillary endothelium. There is progressive edema.
Ashley Davidoff
TheCommonVein.net lungs-0692
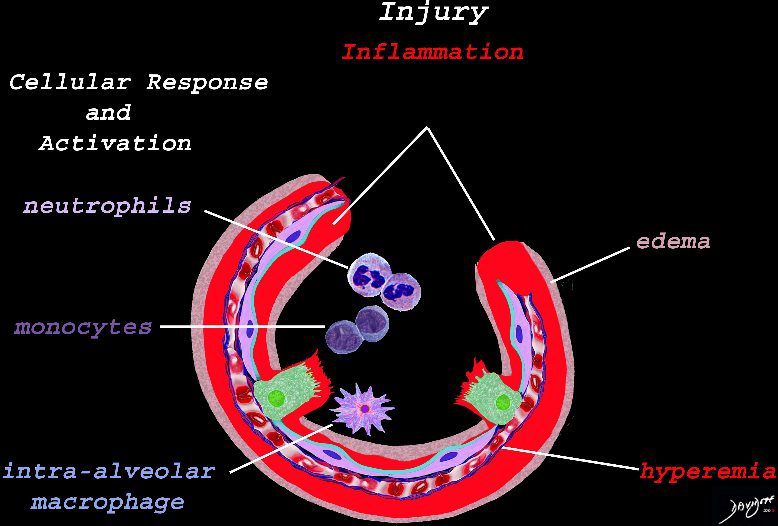
The initial injury results in an acute severe inflammatory response consisting hyperemia , edema with migration initially of neutrophils in the first 6-24 hours followed by monocytes (24-48hours). The intra -alveolar macrophages are activated.
Ashley Davidoff
TheCommonVein.net lungs-0691
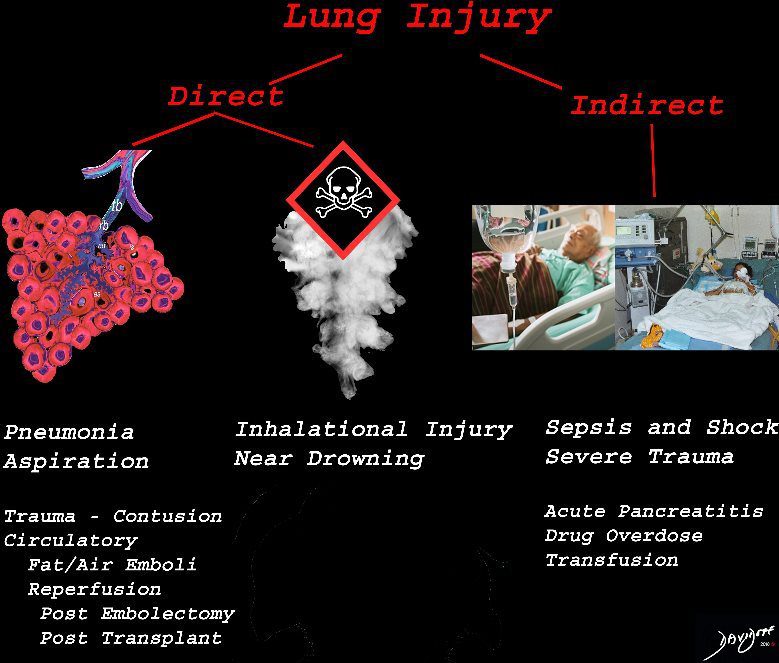
The lung is injured either by direst causes most commonly pneumonia, aspiration or from inhalation of toxic substances. Severe systemic illnesses, most commonly sepsis with shock, and severe trauma are considered indirect causes.
Ashley Davidoff
TheCommonVein.net lungs-0690

The diagram shows the lining of the normal alveolus composed of type 1 pneumocyte squamous in nature and the cuboidal cell (type pneumocyte) which rest on a lamina propria, and basement membrane (not shown) shared with the inner endothelial layer of the capillary. Intra-alveolar macrophage lies within the alveolar lumen
Ashley Davidoff TheCommonVein.net lungs-0689
42474b18.800 lung trachea bronchi tracheobronchial tree
Ashley Davidoff MD
TheCommonVein.net 42474b18.800

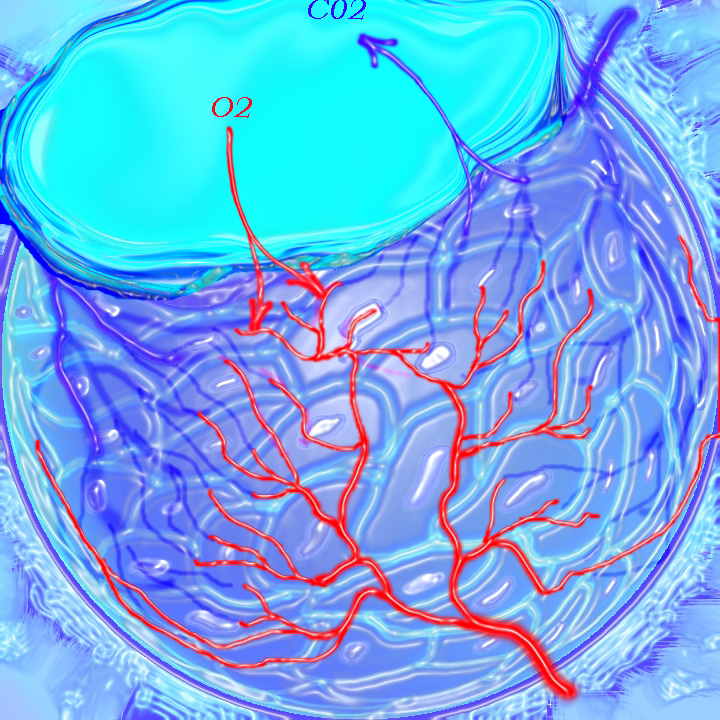
This is a drawing of a cluster of alveoli surrounded by the capillary network, fed by an arteriole in blue, and drained by a venule in red. The second image shows the exchange of life giving oxygen for the by product of metabolic activity ? carbon dioxide
Ashley Davidoff MD
TheCommonVein.net
32165c

Snow covered red berries ? the contrast between the cherry red and the snow white make them look delicious.
Ashley Davidoff MD
TheCommonVein.net
02160p

Tree in bud nociceptors free nerve endings trees in the body
Ashley Davidoff MD
TheCommonVein.net87559pb04b07b.8s
Ashley Davidoff MD
TheCommonVein.net.
32697

A drawing showing the normal acinus in teal and the abnormal emphysematous acinus in green characterised by destruction of the septal walls, enlargement of the alveoli, and loss of elasticity. The absence of involvement of the respiratory bronchiole makes the pathological diagnosis of centrilobular emphysema. Ashley Davidoff MD
TheCommonVein.net 32645

This diagram illustrates the branching pattern of the tracheobronchial tree that extends from the bronchi to the terminal bronchioles transitioning into the alveoli via the alveolar sacs.
32645b04b04 lung D
Ashley Davidoff MD
TheCommonVein.net 32645a10.800
32647 Davidoff
Ashley Davidoff MD
TheCommonVein.net
42444b18.8 lungs anatomy X-ray
Ashley Davidoff MD TheCommonVein.net 42444b18.8

The left pulmonary artery seen in the left upper image is turned 90 degrees anticlockwise to reflect it upright shape of a tree (top left)) then flipped 90degrees and colored over to reveal its tree like morphology. keywords lung pulmonary artery pulmonary trunk
Ashley Davidoff MD TheCommonVein.net 46649c01.800

32368 Ashley Davidoff MD
TheCommonVein.net

Ashley Davidoff MD
TheCommonVein.net 46649b04b.800

The tracheobronchial tree turned upside down shows it?s similarity to the branching pattern of a tree.
keywords lung bronchus tracheobronchial tree airway tree the common vein applied biology
Ashley Davidoff MD TheCommonVein.net
32620c02.800
Tracheobronchial Tree
Tree, flower, tracheobronchial tree, trachea bronchi lung
Ashley Davidoff TheCommonVein.net 32620b14.800b02p

The chest is surrounded by a ring of muscle (maroon) made up of a various groups which work in concert. The diaphragm is the workhorse of the respiratory muscles and is shown as a thick maroon band inferiorly.
Ashley Davidoff MD
TheCommonVein.net 42530b05b09b14

The five major layers that keep the air moving include the outer bony cage, the muscular layer represented in maroon, the pleural complex (orange yellow orange) the lung (blue) and surfactant within the alveolus. (pink)
42530b05b09b01a08
Ashley Davidoff MD
TheCommonVein.net

This artistic rendition of the heart and lungs uses the shape of fruit and vegetables to create an image of the chest. The lungs are made of grapes, the pulmonary arteries are made of carrots, the ribs are made of banana peel and the heat is made of a red pepper. 02032p Ashley Davidoff MD
TheCommonVein.net
lungs-00687-lo-res.jpg
Smoking and the Alveolus –The effect of the proteases and and elastases cause destruction of the alveoli and loss of elasticity, and therefore overall function. The destruction leads to bullous disease
The accumulation of smokers macrophage, and in the case of Langerhans cell histiocytosis leads to space occupation of the alveoli also reducing function
Ashley Davidoff
TheCommonVein.net
lungs-00687

Light brown granules in the macrophage is characteristic of the smokers macrophage
Ashley Davidoff
TheCommonVein.net lungs-00686

At the level of the membranous airways the effect is predominantly related to the loss of elasticity, and aberrant accumulation of smoking related macrophages.
The weakening and destruction results in emphysema and the abnormal accumulation of smoking related macrophages relates to DIP
Ashley Davidoff
TheCommonVein.net lungs-00685
Ashley Davidoff
TheCommonVein.net lungs-00683

The Buck Ends Here
The alveolus is lined by a simple epithelium ? one cell layer thick. There are two types of lining cells; Type 1 pneumocytes are squamous cells that cover 90% of the surface of the inner lining of the lung , and type II cuboidal pneumocytes that are in fact much more numerous than Type I. They are involved in the production of surfactant . In the lumen there are resident macrophages which play a crucial role in the immune system. The mucosa is grounded by a basement membrane and a lamina propria, and connected to the lamina propria and basement membrane of the surrounding capillary. The alveolus is lined by a thin layer of surfactant. (teal blue)
Ashley Davidoff TheCommonVein.net lungs-00679

Ashley Davidoff MD TheCommonvein.net lungs-0009

The lobular (most distal of the subsegmental airways give rise to the terminal bronchiole which give rise to the membranous airways. These include in order, the respiratory bronchiole, alveolar ducts and alveolar sacs
Ashley Davidoff TheCommonvein.net lungs-0007
When there are extensive interstitial fibrotic changes in the interstitial compartments of the lung which include the and the interalveolar septa, and the supporting interstitium of the lung between the acini and small airways, the overall net density of the region of involvement will be gray, and when adjacent to the black air filled airways, a ground glass appearance will be apparent
Ashley Davidoff
TheCommonVein.net
ssb = subsegmental bronchiole
tb = terminal bronchiole
rb = respiratory bronchiole
as = alveolar duct
as = alvelar sac
is = anteralveolar septum
Ashley Davidoff
TheCommonVein.net lungs-00682
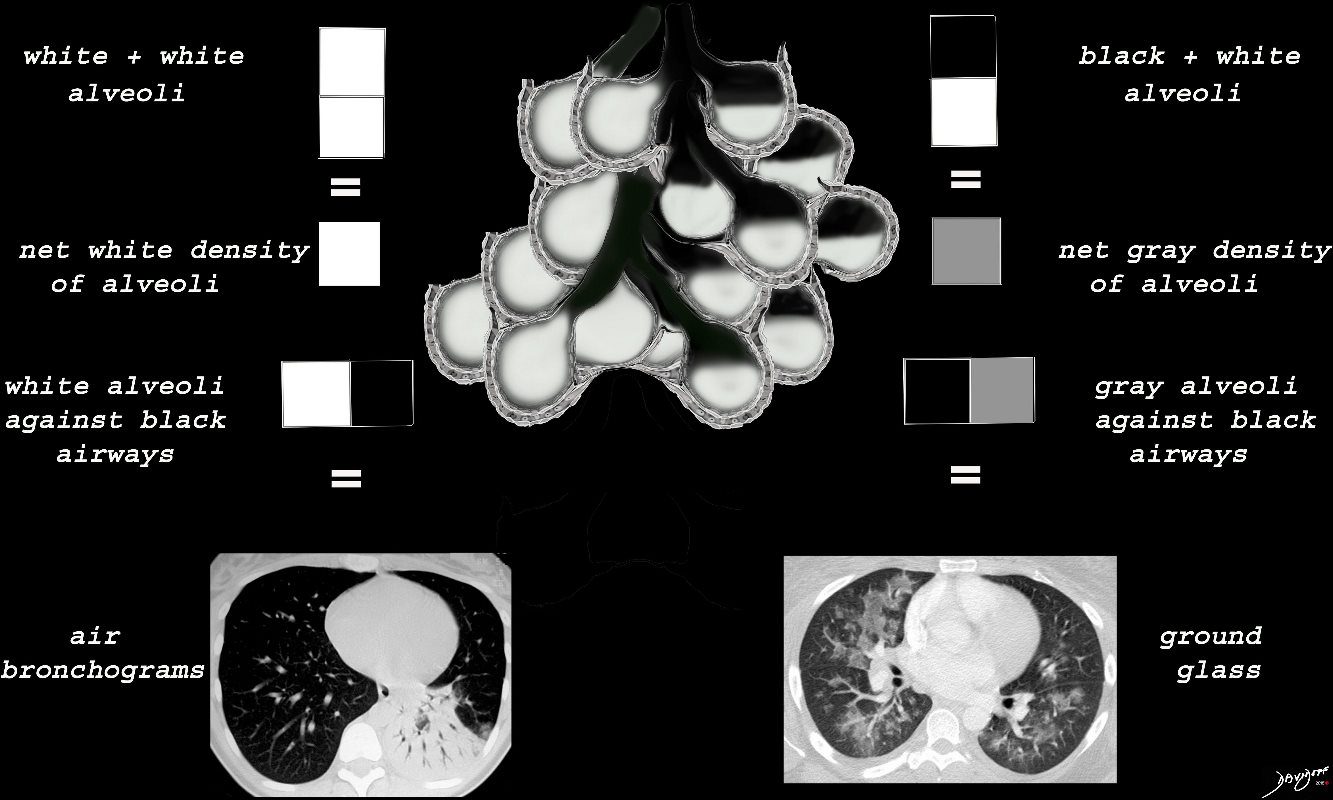
When the alveoli are fully filled with fluid, tumor, or pus for example, the overall net density will be white, and when adjacent to air filled airways, air bronchograms are visible (left side of image)
When the alveoli are only partially filled, the density of the fluid added to the density of the air results in an overall gray density, and when positioned next to air filled bronchi, there is insufficient contrast to create an air bronchogram and sufficient to enable visualization of the blood vessels. This is called ground glass opacification
Ashley Davidoff
TheCommonVein.net lungs-00681
The subsegmental medium sized airways give rise to the terminal bronchiole (tb) which gives rise to the membranous airways. These include in order, the respiratory bronchiole (rb), alveolar duct (ad) and alveolar sac (as)
Ashley Davidoff
TheCommonvein.net lungs-00680

Airways are lined by a pseudostratified ciliated columnar epithelium interspersed with mucus secreting goblet cells
Ashley Davidoff
TheCommonVein.net lungs-00674b01-lo res
42651c-1.jpg
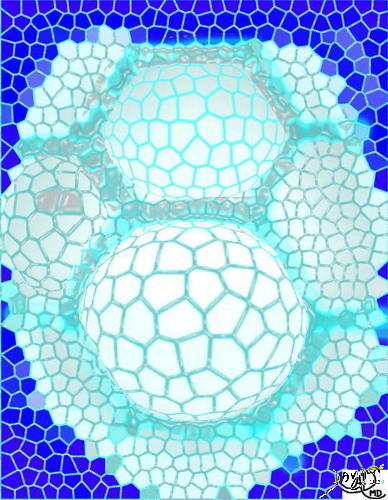
This collage reflects the range of the respiratory system from the macroscopic and anatomic to the microscopic – a continuum of structure. Image 2 is a post-mortem specimen taken from the front and slightly above. It shows the trachea and bronchi supplying the two lungs above, with the aortic arch and cardiac structures in the middle and below. Note how pink the lungs are in this specimen from an unfortunate baby with congenital heart disease. Image 3, the chest X-ray, shows the lucent lungs within the thoracic cavity while image 4 is a diagram of the trilobed right lung and the bilobed left lung. Two respiratory units of the lung are shown in the next image each called a pulmonary lobule (5). The lobule consists of a central bronchiole (light blue) and pulmonary arteriole (dark blue), surrounded by the air filled acinus (teal) with its peripheral venules. (red) The acinus is magnified in the next image (6), showing first the tubular terminal bronchiole branching into the respiratory bronchioles, alveolar sacs, and finally the grape like alveoli. The organization of the connective tissues of the lung is shown in image 7. Finally we get down to the grapes or alveoli of the lung with surrounding vessels (8), and a single alveolus is seen in 9. It seems a long way for the air to travel but the system can deliver the air to and from the outside in a single breath, and exchange the gases at the capillary level even more rapidly. It is a remarkable system.42651c
keywords lung chest
Ashley Davidoff TheCommonVein.net
keywordslung chest
Ashley Davidoff TheCommonVein.net

This diagram illustrates the acinus which consists of the respiratory bronchioles (rb 1, 2, 3) the alveolar duct (ad) the alveolar sac (as) and the alveoli. (a)
Courtesy Ashley Davidoff MD 42446b12
Ashley Davidoff
TheCommonVein.net
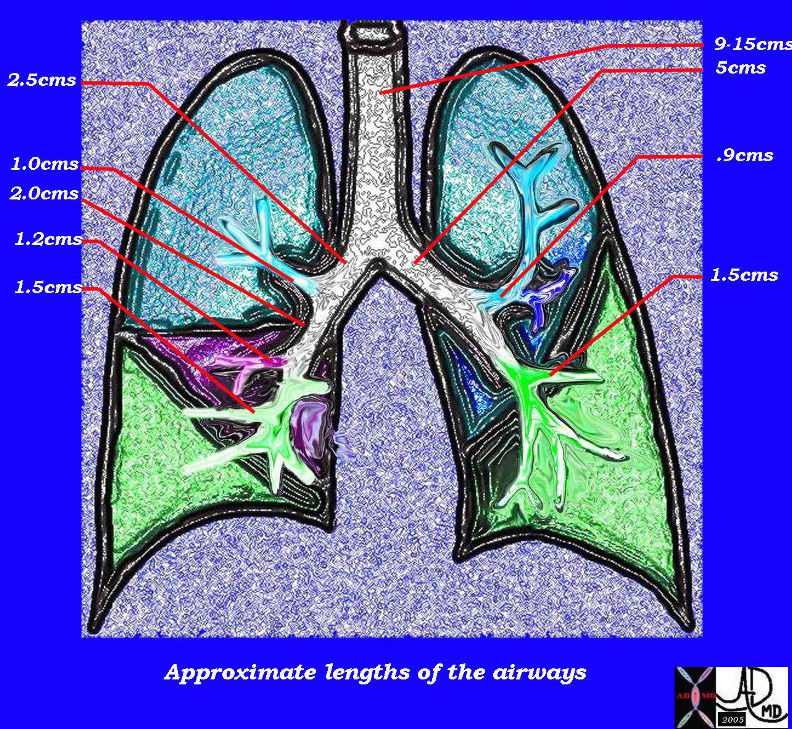
This diagram of the airways reveals the approximate lengths of the airways. Note that the left main stem bronchus is about twice the length of the right whose length is truncated by the take off of the right upper lobe bronchus.
Courtesy Ashley Davidoff MD
TheCommonVein.net
32686b05L04b
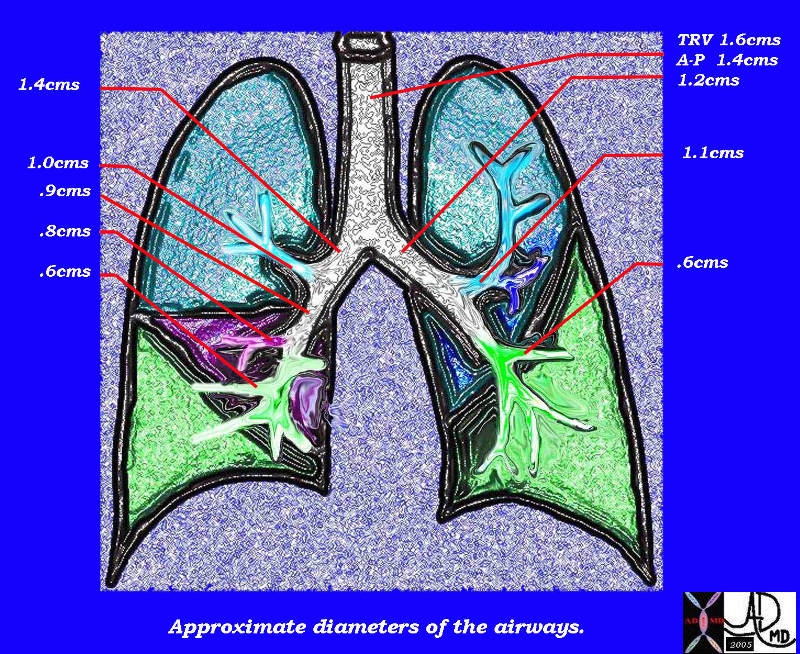
This diagram of the airways reveals the approximate diameters of the airways. Note that the left main stem bronchus is thinner than right whose length is truncated by the take off of the right upper lobe bronchus.
Ashley Davidoff MDTheCommonVein.net
32686b05L05b

Image on the left shows normal size and appearance of terminal bronchioles and alveoli. On the right the image shows the effects on the respiratory bronchioles and when severe, on the alveoli as well
Ashley Davidoff MD
TheCommonVein.net
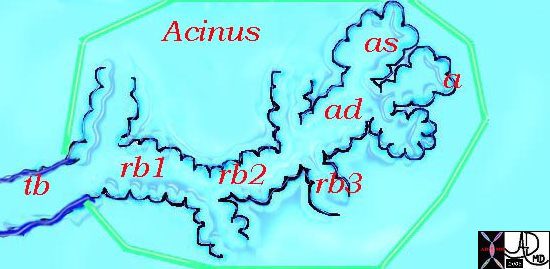
This diagram illustrates the acinus which consists of the respiratory bronchioles (rb 1, 2, 3) the alveolar duct (ad) the alveolar sac (as) and the alveoli. (a)
Courtesy Ashley Davidoff MD 42446b12
TheCommonVein.net
key words art mucosa submucosa muscularis adventitia serosa histology tube colon small bowel lung bronchus bronchi esophagus stomach large bowel bile duct ureter tube principles
Ashley Davidoff TheCommonVein.net 32347

The acinus with its arborizations is shaped more like a bunch of grapes.
Courtesy of: Ashley Davidoff, M.D 42650
TheCommonVein.net

An alveolus subjected day and night for 20 years to black smog from a human chimney. It had no choice but to react.
Courtesy Ashley Davidoff MD. 32166f
The CommonVein.net

Polycyclic Aromatic Hydrocarbons (PAH’s) are by products of nicotine and are flat compounds that are similar to benzene in structure. Liver enzymes oxidize the PAH’s making their incorporation into DNA possible. The change in DNA structure leads to interference in function and a predisposition to carcinogenesis.
Image modified by Ashley Davidoff MD. 54460 The CommonVein.net
These diseases are all about cigarettes and the garbage that they deposit in our lungs.
Courtesy Ashley Davidoff MD. 32646d The CommonVein.net
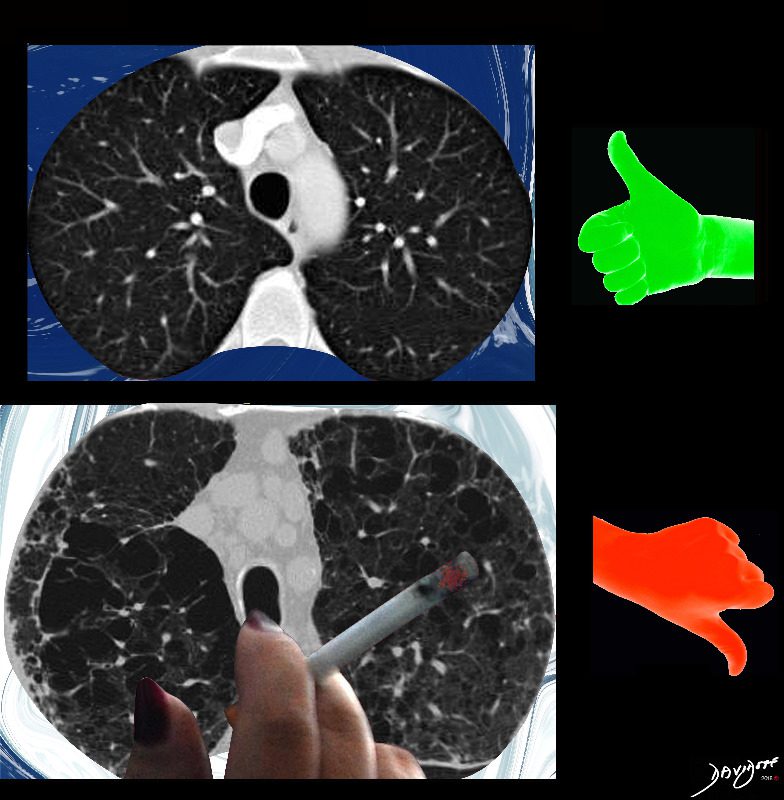
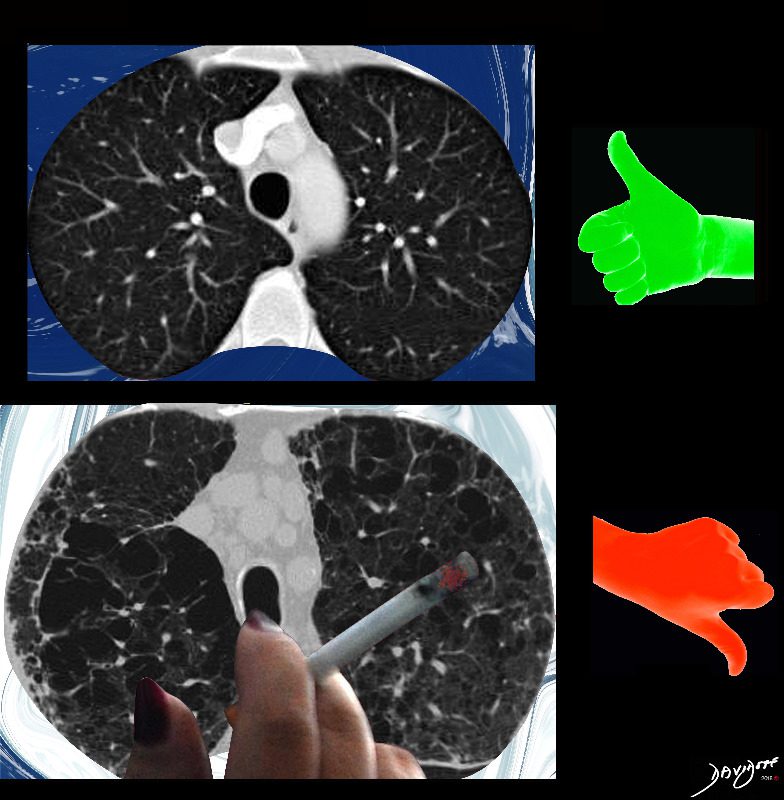
The imaging difference between healthy lungs (thumbs up) and emphysematous lungs (thumbs down)
Ashley Davidoff MD
TheCommonVeein.net lungs-0071
Cigars are not as carcinogenic as cigarettes probably due to the fact that cigar smoke is not usually inhaled. In the early 1900?s cigar smoking was associated with elegance and currently portrays a sense of bravado as demonstrated in this image.
Courtesy Ashley Davidoff MD 13021g
TheCommonVein.net

From the series “People of Israel”
Ashley Davidoff MD
TheCommonVein.net

From the series “People of Israel”
Ashley Davidoff MD
TheCommonVein.net

Ashley Davidoff MD
TheCommonVein.net
Ashley Davidoff TheCommonVein.net lungs-0055
Ashley Davidoff TheCommonVein.net lungs-0055b
Ashley Davidoff MD The4CommonVein.net cells-0072
First line of defense against infections of the lung.
Reside in alveolar walls, lymphatic channels and lymph node.
Originate in the bone marrow and are part of the Mononuclear Phagocytic System.
Ashley Davidoff
TheCommonVein.net lungs-0063

It produces the phospholipid – part of the surfactant that reduces surface tension and allows the alveoli to remain open
#cells
Ashley Davidoff
TheCommonVein.net lungs-0062
– flattened for gas exchange, forms a part of the Blood-Gas Barrier
nd sometimes vacuolated cytoplasm
It produces the phospholipid – part of the surfactant that reduces surface tension and allows the alveoli to remain open
#cells
Ashley Davidoff
TheCommonVein.net lungs-0061
Parts and Bonds
Ashley Davidoff MD TheCommonVein.net lungs-0060
“S” of SARCOIDOSIS
The granulomas start as micronodules in close association with the lymphatics (1) spread in the intralobular septa and centrilobular bronchioles ((2) cluster and conglomerate to form macro nodules (4,5) sometimes manifesting as the galaxy sign (6). As they cluster and conglomerate they can cause conglomerate masses along the pathway (7) most commonly centrally as the lymphatics become confluent in the hila (7)
The lymphovascular bundles may be accompanied by nodularity (8) or just by thickening (9).
The lymph nodes in the mediastinum become significantly enlarged and fleshy (10). They often calcify (12) sometimes on the calcify on the rim of the node (eggshell calcification (11)
Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The ?S? drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD TheCommonVein.net 132082-S06L

Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The ?S? drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD TheCommonVein.net 132082 S01.8

“S” of SARCOIDOSIS
In this diagram the arrows show the direction of flow of the lymphatics. Pleural lymphatics (yellow arrows), Fissural lymphatics, green arrows), flow from the interlobular septa (purple arrows) and along the bronchovascular bundles (blue arrows) all flow toward the lymph nodes in the hila and mediastinum (pink arrows).
Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The ?S? drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD TheCommonVein.net 132082 000 b01.8
132082-000.8.jpg
NODULES IN THE SECONDARY LOBULES“S” of SARCOIDOSIS
Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The ?S? drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD TheCommonVein.net 132082 000.8

“S” of SARCOIDOSIS
Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The ?S? drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD TheCommonVein.net 132082 009 summary.8

“S” of SARCOIDOSIS
Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The ?S? drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD TheCommonVein.net
132082 008 bronchovascular.8
“S” of SARCOIDOSIS
Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The ?S? drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD TheCommonVein.net
132082 006 galaxy 02.8

“S” of SARCOIDOSIS
Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The ?S? drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD TheCommonVein.net
132082 005b nodules.8

“S” of SARCOIDOSIS
Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The ?S? drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD TheCommonVein.net
132082 005 pawnbroker medici.8

“S” of SARCOIDOSIS
Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The ?S? drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD TheCommonVein.net
132082 004 fissures.8

“S” of SARCOIDOSIS
Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The ?S? drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD TheCommonVein.net
132082 003 subpleural.8
132082-002-secondary-lobule.8.jpg
NODULES IN THE SECONDARY LOBULES“S” of SARCOIDOSIS
Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The ?S? drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD TheCommonVein.net
132082 002 secondary lobule.8
000 Smoking and Lung Disease
Ashley Davidoff MD
TheCommonVein.net lungs-0038


A dancer demonstrates a normal carinal angle (upper image) and as she continues to extend her left leg, (lower images) the angle becomes greater than 80 degrees and in terms of the carinal angle becomes abnormal.
Ashley Davidoff MD

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

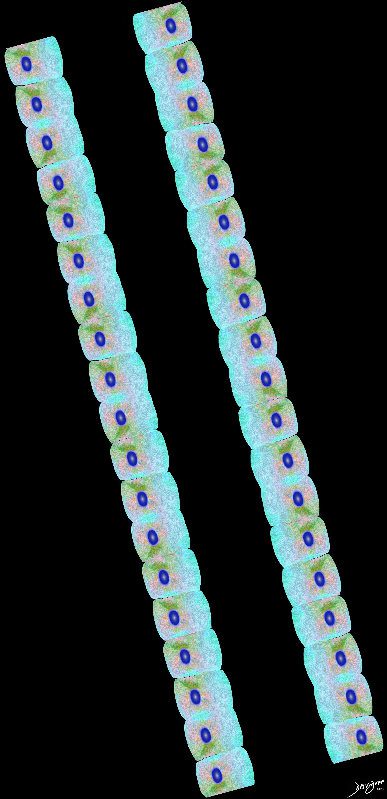
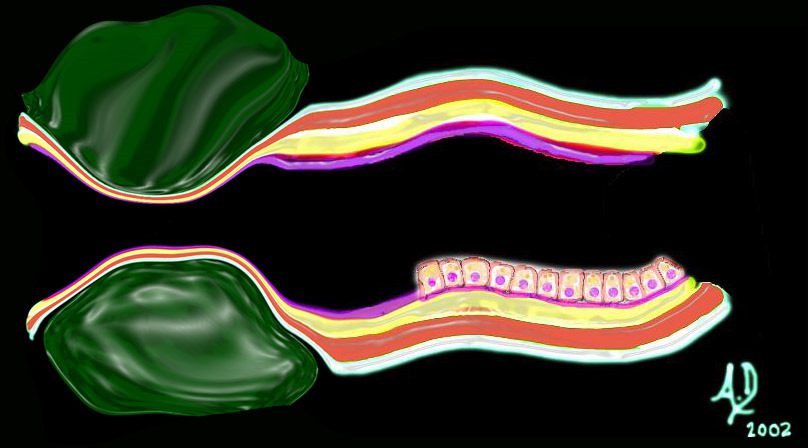
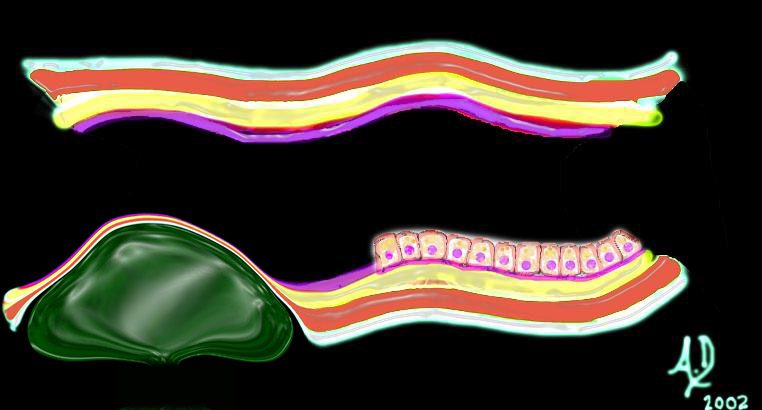
Cross section diagrams of the small airways. The top diagram shows a normal terminal bronchiole with columnar epithelium (pink), and muscularis (maroon). The respiratory bronchiole starts to have features of evolving respiratory airways, and he mucosa becomes cuboidal with persistence of the muscularis.
The alveolar duct has a squamous epithelium (pink), and is surrounded by a capillary network (blue – arteriolar component, and red venular component)
Ashley Davidoff MD thecommonvein.net lungs-0776b

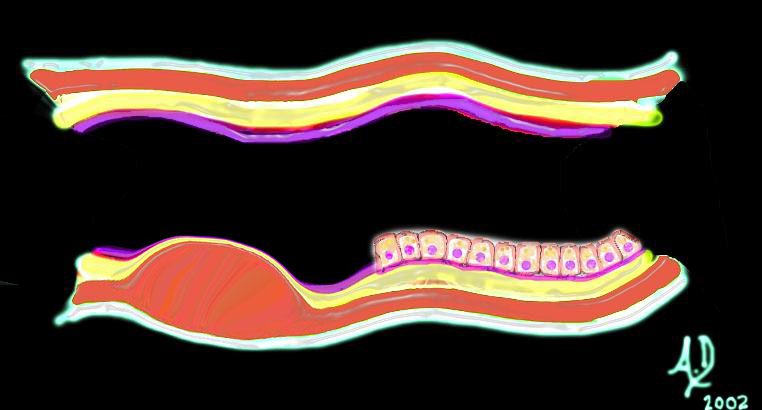
Cross secrtion diagrams of the small airways. The top diagramof a normal terminal bronchiolewith cuboidal epithelium (pink), and muscularis (maroon)
below is the alveolar duct. the mucosa has become a flattened squamous epithelium (pink), and surrounded by a capillary network (blue – arteriolar component, and red venular component)
Ashley Davidoff MD thecommonvein.net lungs-0776
Ashley Davidoff TheCommonVein.net lungs-0736a01
Diffuse Lung Disease
Ashley Davidoff MD TheCommonvein.net lungs-0775

Upper lung field distribution
Ashley Davidoff MD TheCommonvein.net lungs-0774
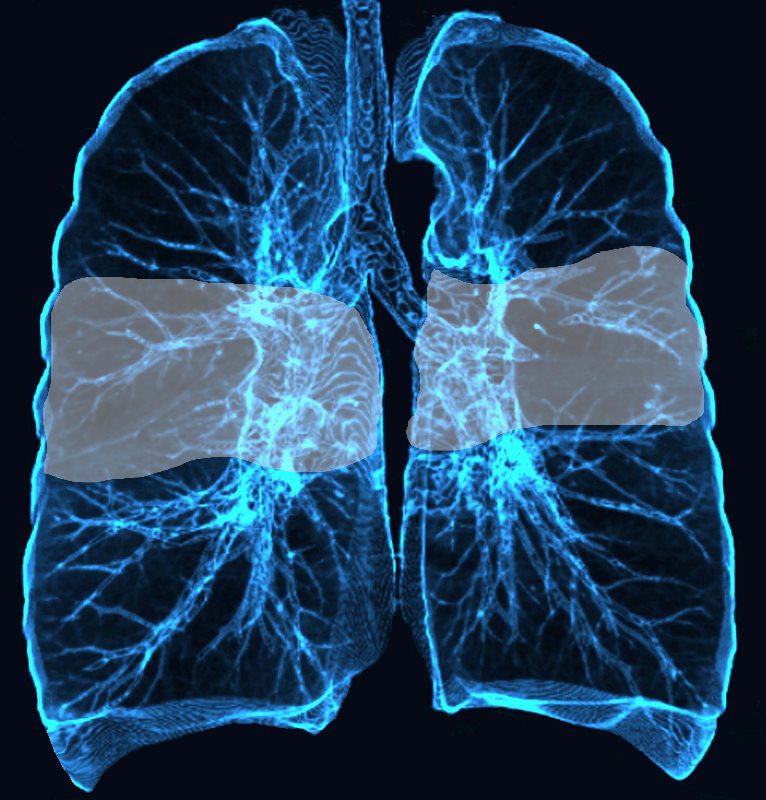
Mid lung field distribution
Ashley Davidoff MD TheCommonvein.net lungs-0773

Upper and mid lung field distribution
Ashley Davidoff MD TheCommonvein.net lungs-0772

Lower Lobe distribution
Ashley Davidoff MD TheCommonvein.net lungs-0771
Perihilar distribution
Ashley Davidoff MD TheCommonvein.net lungs-0770
Broncho vascular distribution
Ashley Davidoff MD TheCommonvein.net lungs-0769

Diagram shows inflammation (red ) in the walls of the alveoli with thickening of the interlobular septa (maroon) . The increased density in the interalveolar septa and interlobular septa results in a ground glass opacity with and crazy paving appearance on CT scan
Ashley Davidoff TheCommonVein.net
lungs-0736a
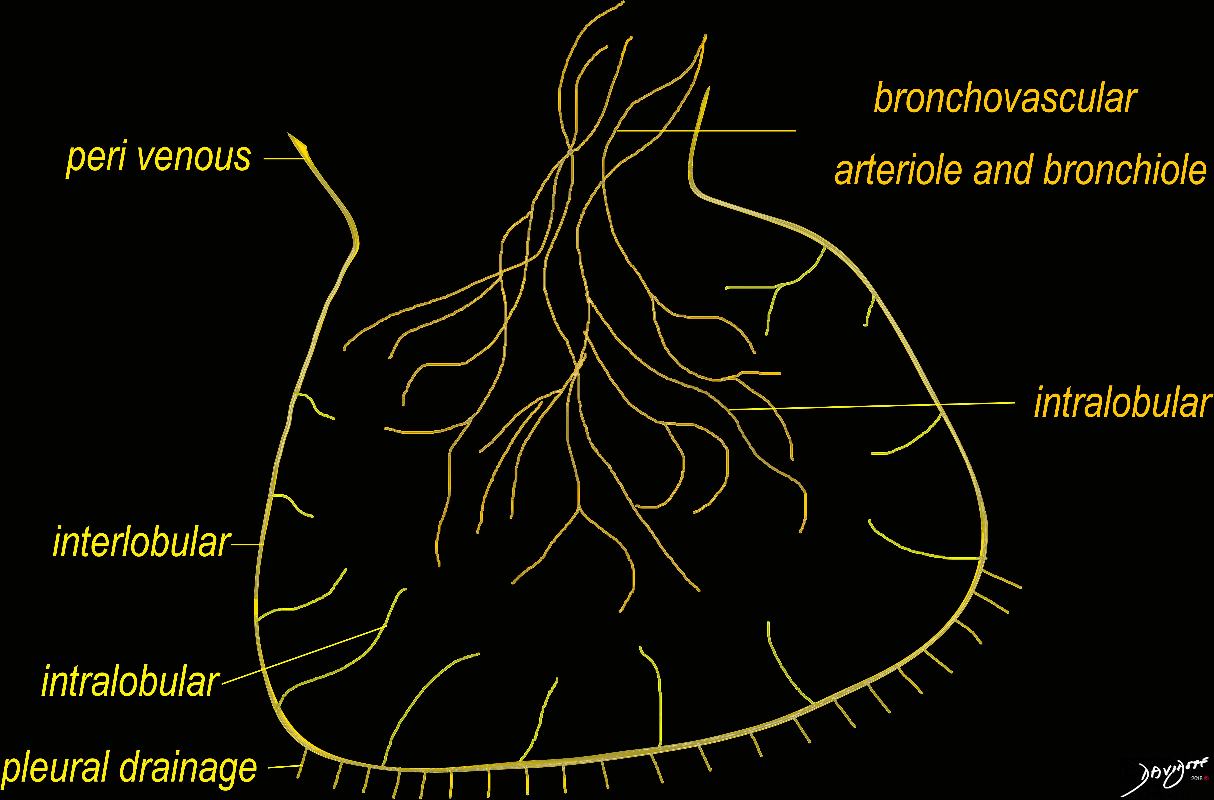
The diagram shows the 2 systems of lymphatic drainage at the level of the secondary lobule. The superficial system drains some of the interstitium of the secondary lobule, runs in the interlobular septa and drains all the pleura. Thee pathway to the lymph nodes in the mediastinum is via the pulmonary veins. The deeper system drains the interstitium in the interalveolar septa, and then they travel along the bronchovascular bundle accompanying the bronchi and pulmonary artery and into the lymph nodes of the hila and mediastinum
Ashley Davidoff MD TheCommonVein.net lungs-0768
The diagram shows the 2 systems of lymphatic drainage at the level of the secondary lobule. The superficial system drains some of the interstitium of the secondary lobule, runs in the interlobular septa and drains all the pleura. Thee pathway to the lymph nodes in the mediastinum is via the pulmonary veins. The deeper system drains the interstitium in the interalveolar septa, and then they travel along the bronchovascular bundle accompanying the bronchi and pulmonary artery and into the lymph nodes of the hila and mediastinum
Ashley Davidoff MD TheCommonVein.net lungs-0767

Ashley Davidoff MD The CommonVein.net lungs-0766
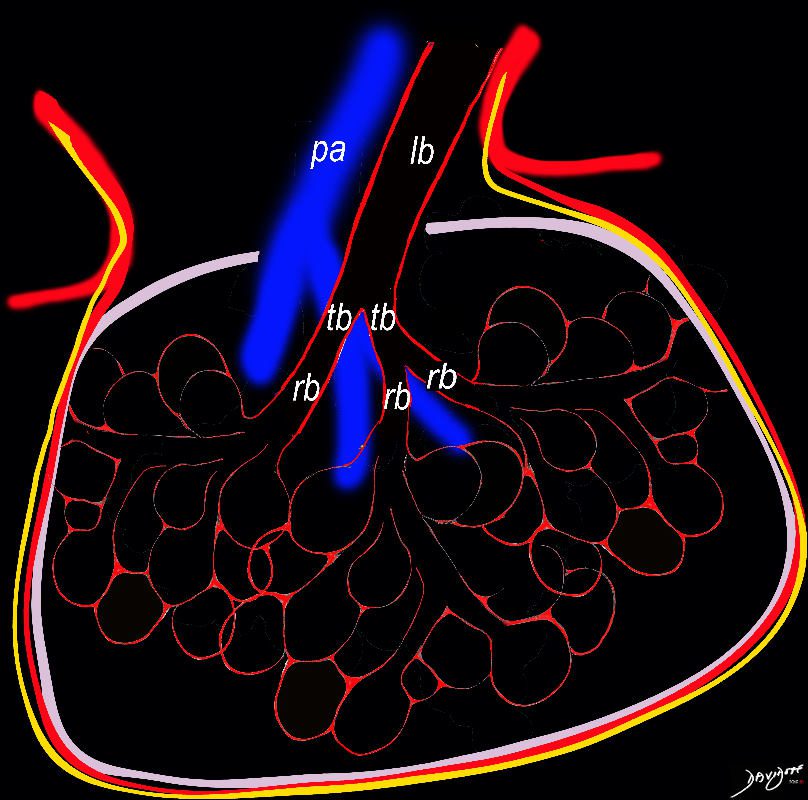
Diagram shows inflammation (red ) in the walls of the alveoli. The increased density in the interalveolar septa results in a ground glass opacity on T scan
Ashley Davidoff TheCommonVein.net
lungs-0736
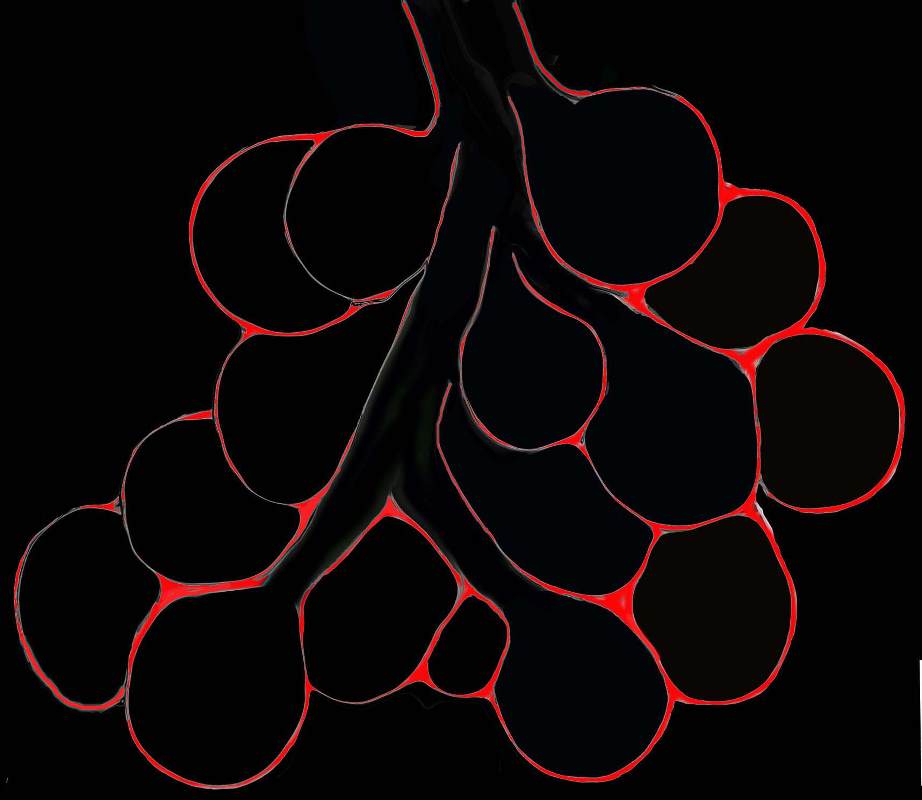
Diagram shows inflammation (red ) in the walls of the alveoli. The increased density in the interalveolar septa results in a ground glass opacity on T scan
Ashley Davidoff TheCommonVein.net
lungs-0736b
{kind=link}
Interlobular Septal Infiltration with Eosinophils and Inflammatory Exudate – Thickening of the Interlobular Septa – Crazy Paving Kerley B lines
The diagram shows the thickened septum surrounding the secondary lobule due to an inflammatory process, cellular infiltrate and congestion of the venules and lymphatics in the septum (a) . An anatomic specimen of a secondary lobule from a patient with thickened interlobular septa is shown in c and overlaid in d. CT of the lungs in a patient with acute eosinophillic pneumonia shows thickened interlobular septa and centrilobular nodules and the thickened septa are overlaid in red (e).
Ashley Davidoff MD The CommonVein.net
lungs-0761
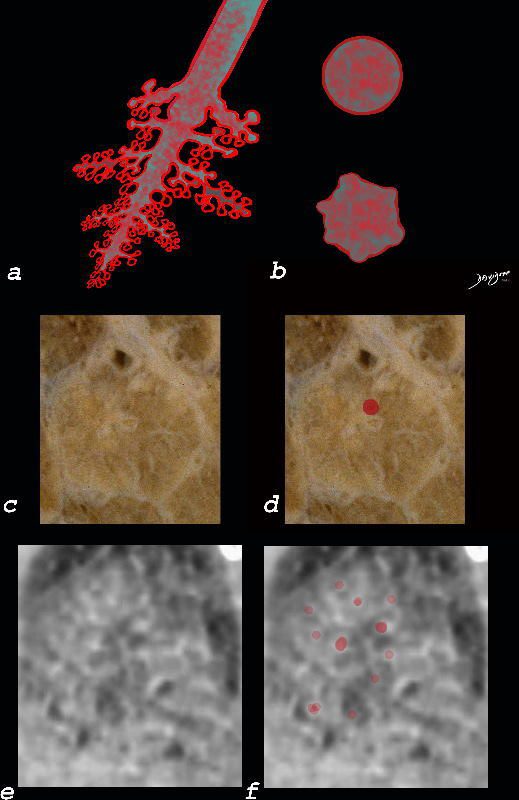
The diagram shows the small airways of the lung including the respiratory bronchiole, alveolar ducts and alveolar sacs in coronal (a) and in cross section (b) and correlated with an anatomic specimen of a secondary lobule that contains a thickened interlobular septum . The respiratory bronchiole is overlaid in maroon (d), next to the arteriole. Images e and f are magnified views of a CT of the lungs in a patient with acute eosinophillic pneumonia and the centrilobular nodules reflecting small airway disease are highlighted in f.
Ashley Davidoff MD The CommonVein.net lungs-0760b

Ashley Davidoff MD TheCommonVein.net lungs-0759
Amyloidosis

Ashley Davidoff TheCommonVein.net lungs-0754
Ashley Davidoff TheCommonVein.net lungs-0753
Ashley Davidoff MD TheCommonVein.net lungs-0752
The secondary lobule is subtended by the lobular arteriole (a) and the lobular bronchiole (b) which which in turn branches into the respiratory bronchioles, alveolar ducts, and nd alveolar sacs (c) The acinus (d) consists of a respiratory bronchiole and its associated alveolar ducts, sacs, and alveoli and represents the functional unit of the lung.
The secondary lobule is drained by the pulmonary venule (e) which runs in the interlobular septum also containing the lymphatics (f). The whole unit is housed and surrounded by a connective tissue framework (g) . The latter 3 structures form the interlobular septum.
Ashley Davidoff MD TheCommonVein.net lungs-0751

The secondary lobule is housed in a connective tissue framework in which run the lymphatic and venular tributaries . Together these 3 structures form the interlobular septum.
The lobular arteriole enters the framework, accompanied by the lobular bronchiole, and they all run together and form the interlobular septa. This structure measures between .5cms and 2cms and is visible on CT scan.
It is important in clinical radiology since many of the structures can be identified in health, and more particularly in disease, enabling the identification and characterization of many pathological processes.
Courtesy Ashley Davidoff MD The CommonVein.net lungs-0751
Normal Histology

Ashley Davidoff MD TheCommonVein.net lungs-0742
Histology of the Small Airways

Ashley Davidoff MD TheCommonVein.net lungs-0742
CHF
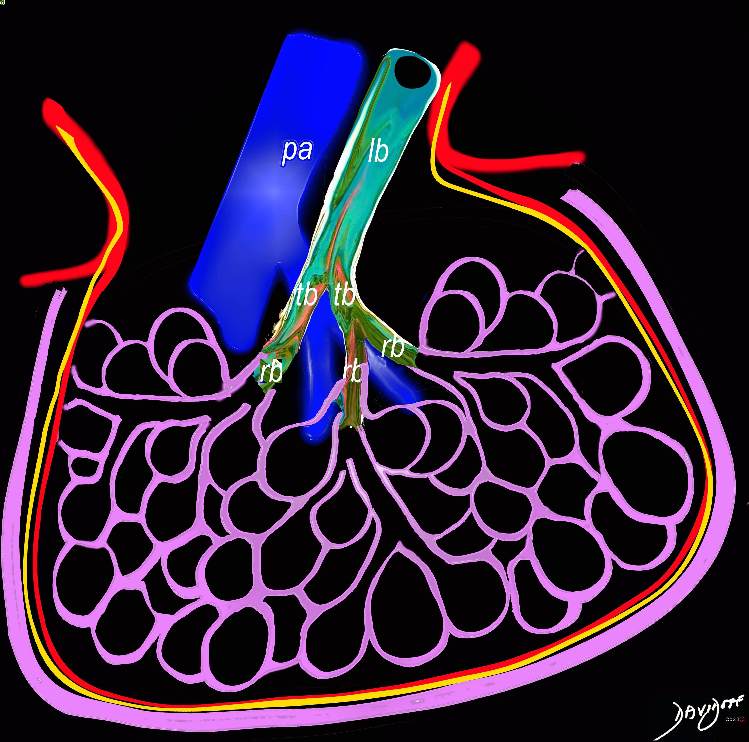
When the end diastolic pressure is between 20 and 30 the intravascular pressure exceeds the intravascular oncotic pressure and fluid starts to leak into the interstitium. The interalveolar septa thicken with fluid (pink) and the interlobular septa also thicken (pink) . The elevation of the end diastolic pressure raises the pressure in the pulmonary veins which is transmitted to the pulmonary artery, and the pulmonary arteriole thus enlarges and becomes larger than its companion airway
The end diastolic pressure is about between 20 and 30 and fluid has started to leak out into the interstitium and results in thickening of the septa
Ashley Davidoff MD TheCommonVein.net lungs-0738 chf01
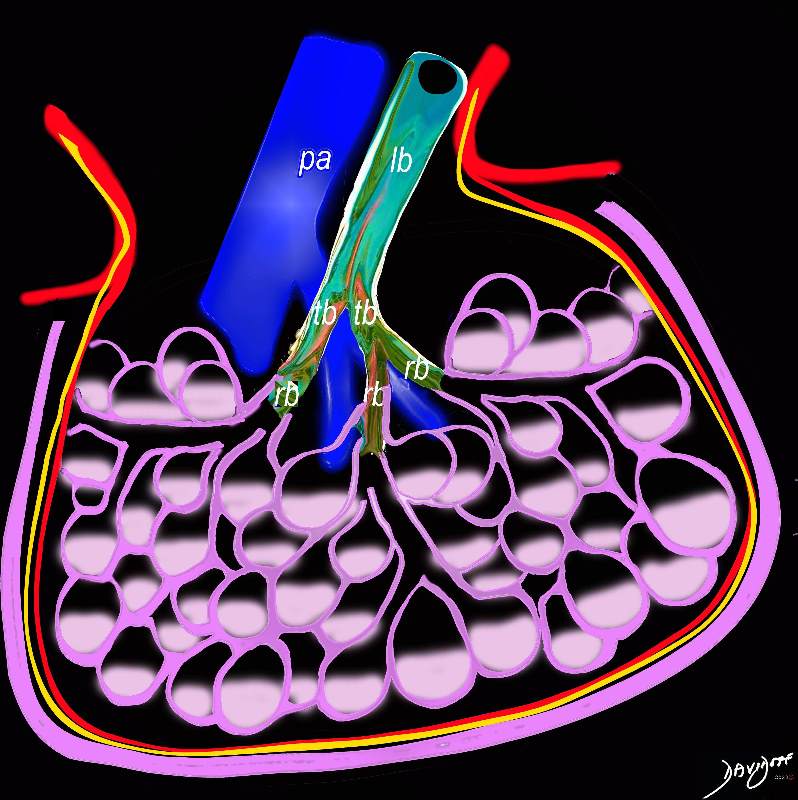
When the end diastolic pressure is between 30 and 40 the intravascular pressure exceeds the intravascular oncotic pressure and fluid continues to leak into the interstitium but now also starts to fill the alveoli. The interalveolar septa and interlobular septa remain thickened with fluid (pink) and the pulmonary arteriole remains enlarged.
Ashley Davidoff MD TheCommonVein.net lungs-0738 chf02
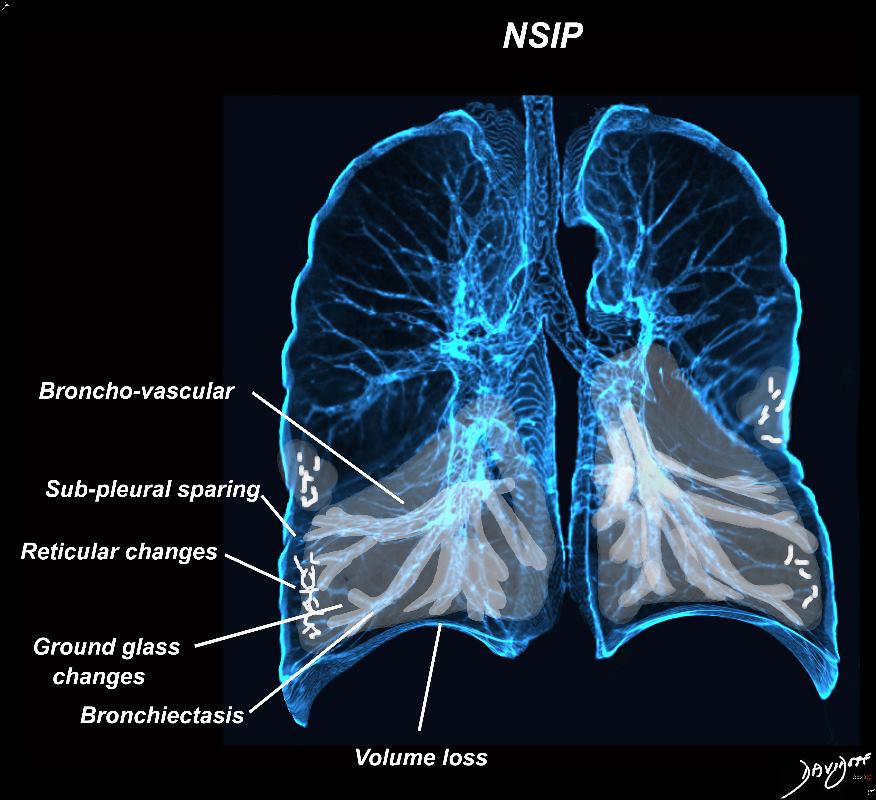
Broncho vascular distribution associated with peripheral sparing, ground glass changes, reticulations, and volume loss, dominantly in the lower lobes but to some extent in the middle lobe and upper lobes
Ashley Davidoff MD TheCommonvein.net lungs-0771b

In moderate CHF, when the intravascular pressure is between 30 and 40 mmHg, it exceeds the intravascular oncotic pressure, and fluid starts to leak out of the capillaries into the interstitium. There is distension of the pulmonary arterioles, the lymphatics and thus into the interlobular septa.
The thickening of the interlobular septa (white arrows a,b,c, and d) result in the appearance of Kerley B lines on CXR (red arrows e, and red arrowheads f) . The overall increase in density caused by the fluid accumulations in the inter, and intralobular septa may result in ground glass opacity seen on the CT in images g and h.
Ashley Davidoff MD TheCommonVein.net lungs-0738 chf01b
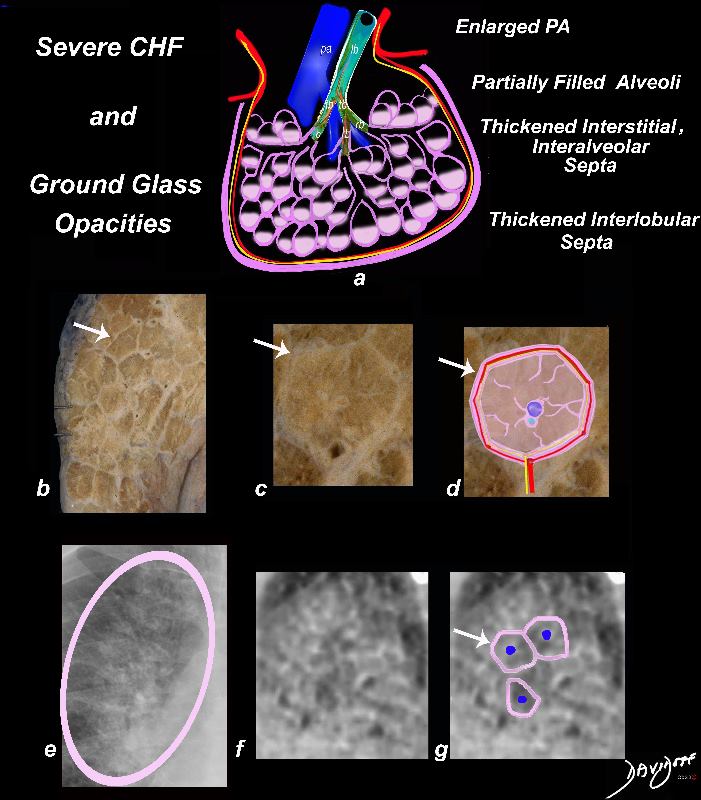
In severe heart failure the end diastolic pressure is between 30 and 40mmHg and fluid continues to leak into the interstitium but now also starts to fill the alveoli. The interalveolar septa and interlobular septa remain thickened (white arrows, b,c,d, and e) and the fluid in the alveoli result in the appearance of ground glass on CXR (circled in pink in e, and noted in the appearance on CT (f,g)) . The pulmonary arteriole remains enlarged ( blue sphere a,d,g).
Ashley Davidoff MD TheCommonVein.net lungs-0738 chf02b
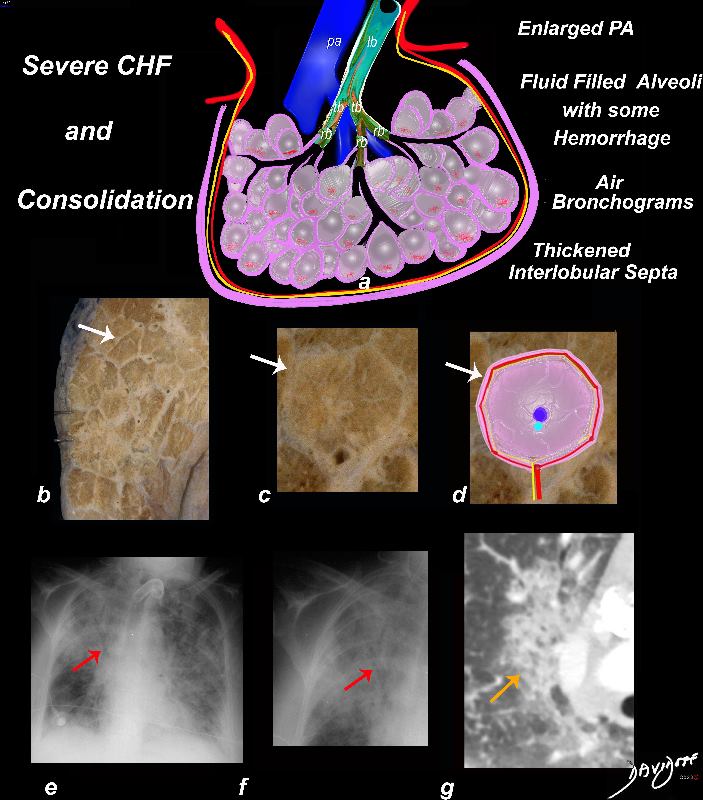
When the end diastolic pressure is between 30 and 40 the intravascular pressure exceeds the intravascular oncotic pressure and fluid continues to leak into the interstitium but now also starts to completely fill the alveoli. Red cells may also leak into the alveoli caused by capillary rupture. The interalveolar septa and interlobular septa remain thickened with fluid (a, and white arrows in b, c, and d). The filling of the alveoli, results in a consolidation seen on the CT, (orange arrow g) and a net ?white density? of the parenchyma which results in air bronchograms against the air filled ?black airways? (a, and CXR – red arrows in e and f). The pulmonary arteriole remains enlarged (blue vessel in a and sphere in d).
Ashley Davidoff MD TheCommonVein.net lungs-0738 chf04b
NSIP and Bronchiectasis

Broncho vascular distribution associated with peripheral sparing, ground glass changes, reticulations, and volume loss, dominantly in the lower lobes but to some extent in the middle lobe and upper lobes
Ashley Davidoff MD TheCommonvein.net lungs-0771b
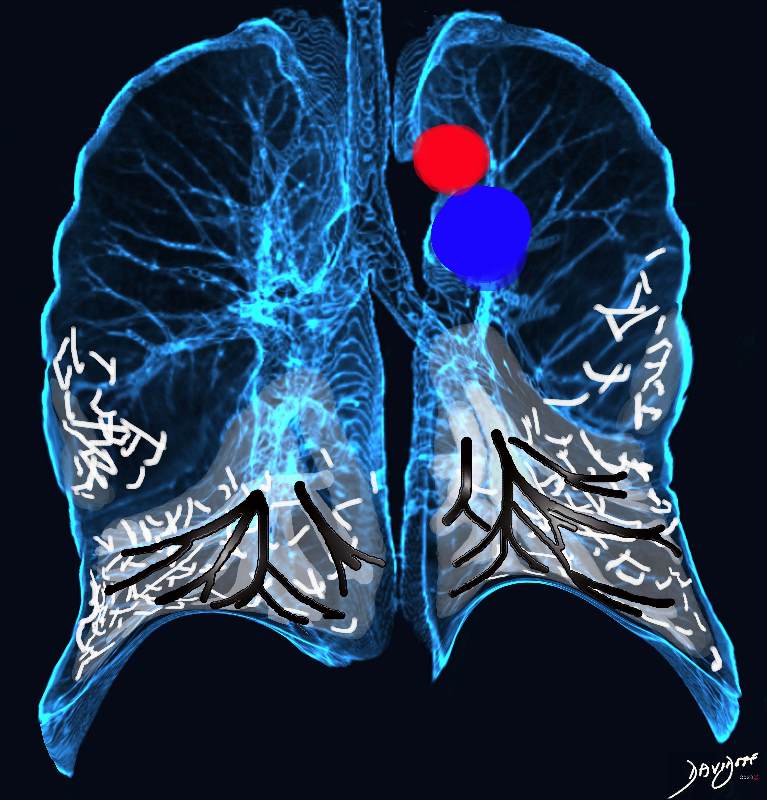
Broncho vascular distribution associated with increased reticular changes, more prominent traction bronchiectasis, decreased lung volumes , and decreased lung volumes, dominantly in the lower lobes but to some extent in the middle lobe and upper lobes. Pulmonary hypertension becomes more common.
Ashley Davidoff MD TheCommonvein.net lungs-0771d

Broncho vascular and inter- alveolar interstitial fibrosis dominantly in the lower lobes but affecting the middle and upper lobes to lesser extent resulting in bronchiectasis and reticulations. The overall increase in density results in ground glass changes
Ashley Davidoff MD TheCommonvein.net lungs-0738 NSIP
Interalveolar Fibrosis
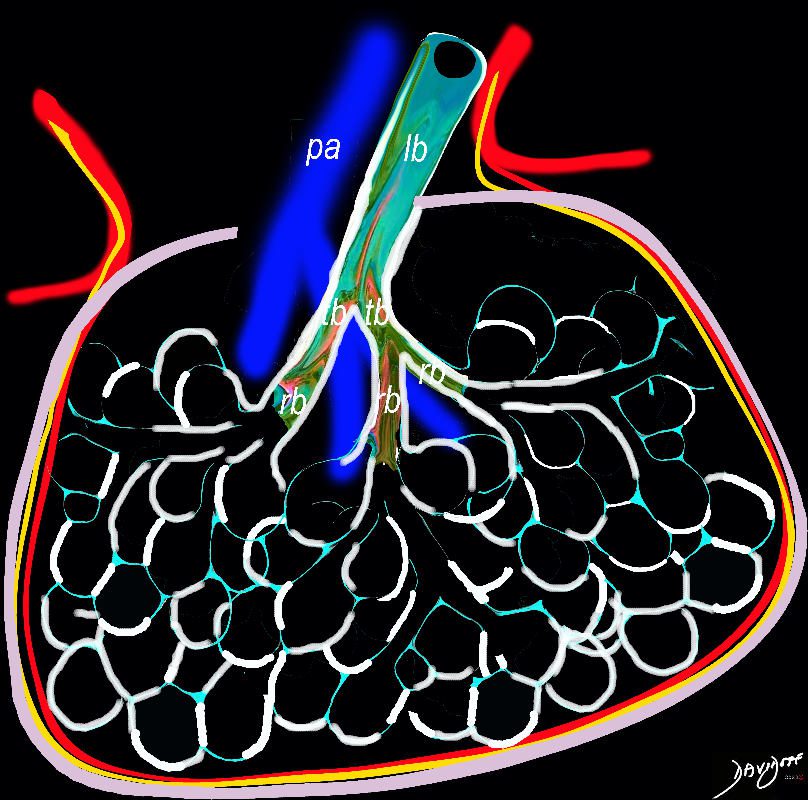
Ashley Davidoff TheCommonVein.net lungs-0738b01
Acute Eosinophillic Pneumonia
Acute Eosinophilic pneumonia is characterised by ground glass opacities (100%) and sometimes consolidation (55%) most commonly with a random distribution 60%. Septal lines (90%) and thickening of the bronchovascular bundles (66%) and bilateral pleural effusions (75%) were common.
Ashley Davidoff MD TheCommonvein.net lungs-0775-b (Reference De Giacomi F et al)

Acute Eosinophilic pneumonia is characterised by ground glass opacities (100%) and sometimes consolidation (55%) most commonly with a random distribution 60%. Septal lines (90%) and thickening of the bronchovascular bundles (66%) and bilateral pleural effusions (75%) were common.
Ashley Davidoff MD TheCommonvein.net lungs-0775-bL (Reference De Giacomi F et al)
Ashley Davidoff TheCommonVein.net lungs-0755
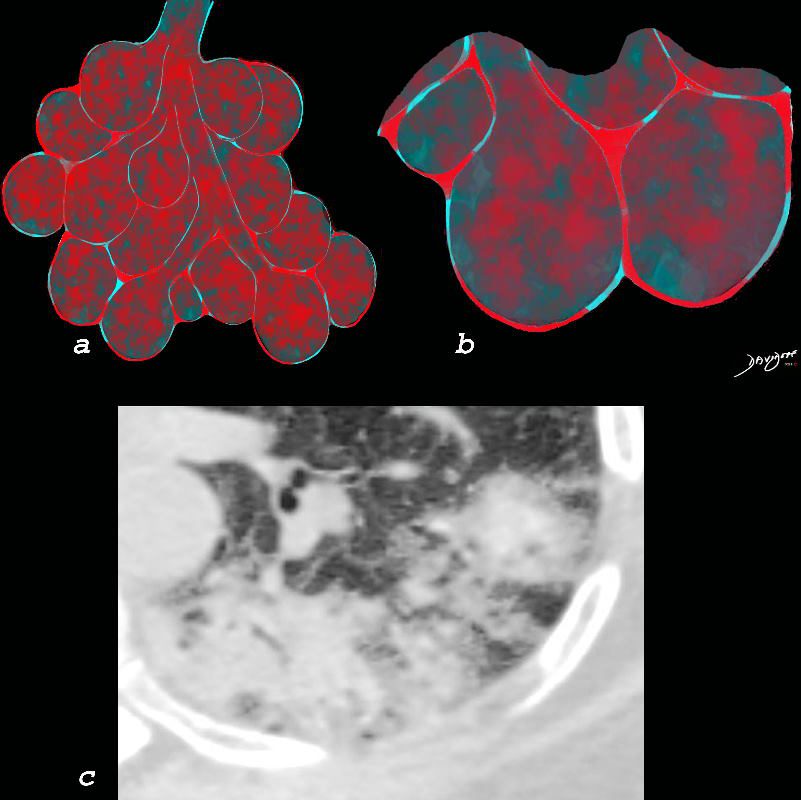
Chronic eosinophilia is characterised by alveolar filling with eosinophils and inflammatory exudates(a) and interalveolar interstitial thickening, (overlaid in red in b). The infiltrates are classically peripherally positioned, usually upper lobes, more commonly bilateral but can be unilateral, and manifest as consolidation and or ground glass opacities. The CT shows a peripheral consolidation in the left upper lobe
Ashley Davidoff MD The CommonVein.net lungs-0764
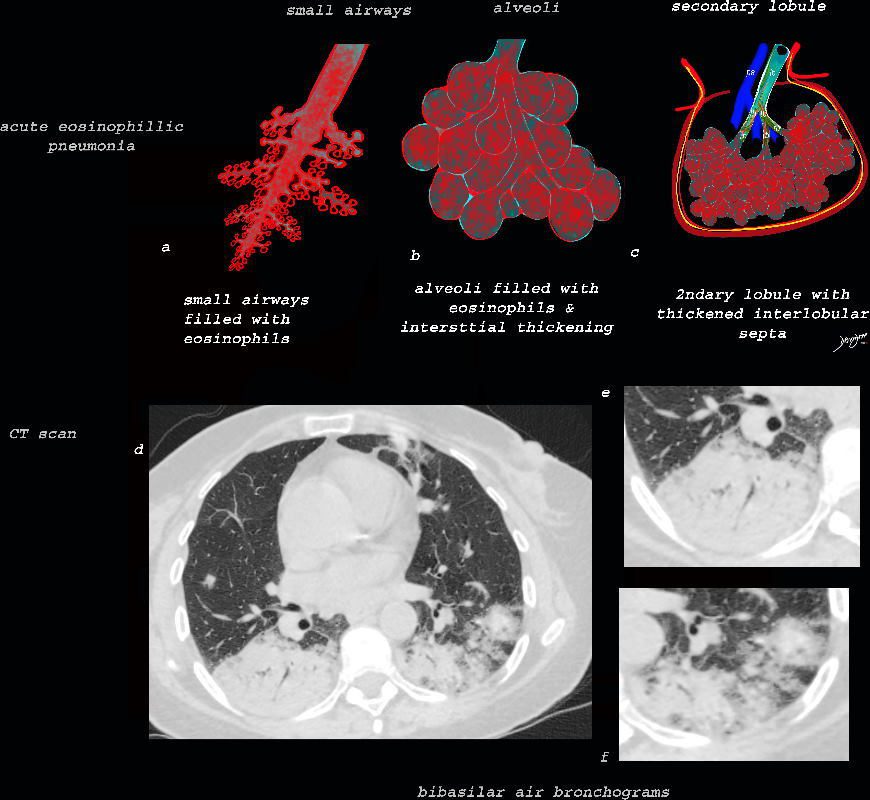
As the disease advances the small airways, and alveoli, get progressively filled with eosinophils, inflammatory cells and fluids resulting in consolidation. This image reveals progressive filling of the small airways, (a) alveoli, (b) and secondary lobules (c) with eosinophils and products of inflammation resulting in multi-segmental consolidations (d), in the lung bases, with air bronchograms at the right base (e), and less dense consolidation at the left base (f)
Ashley Davidoff MD The CommonVein.net lungs-0763
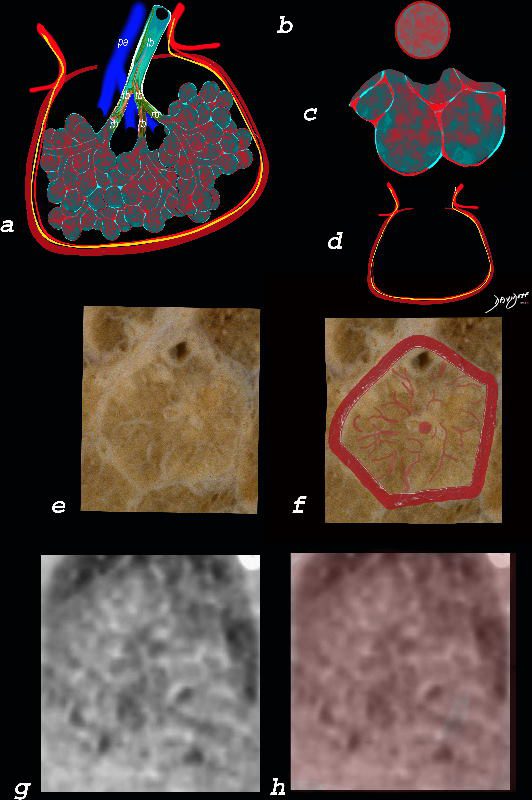
The ground glass changes are a combination of the cellular and exudative inflammatory response in the small airways, alveoli, interalveolar septa and interstitium, and thickened alveolar septum
The diagram shows the abnormal secondary lobule (a) The involved components include the small airways(b) alveoli and interalveolar interstitium (c) and the thickened interlobular septum (d) surrounding the secondary lobule due to an inflammatory process, cellular infiltrate and congestion of the venules and lymphatics in the septum. An anatomic specimen of a secondary lobule from a patient with thickened interlobular septa and interstitial thickening is shown in image e, and is overlaid in red (f) . A magnified view of an axial CT of the lungs in a patient with acute eosinophillic pneumonia shows thickened interlobular septa and centrilobular nodules (g) The inflammatory changes in the aforementioned structures result in an overall increase in density of the lung manifesting as ground glass changes (g) and overlaid in red (h)
Ashley Davidoff MD The CommonVein.net lungs-0762

This diagram reveals the important structural changes in the secondary lobule that includes filling of the alveoli with eosinophils and proteinaceous and fibrinous exudate as well as infiltration into the alveoar septa and interstitium (redwalls) . An important component of the disease is the thickening of the interlobular septa (maroon) which results in Kerley B lines and an interstitial pattern reminiscent of cardiogenic interstitial edema.
Ashley Davidoff TheCommonVein.net lungs-0758

Ashley Davidoff TheCommonVein.net
lungs-0756b01
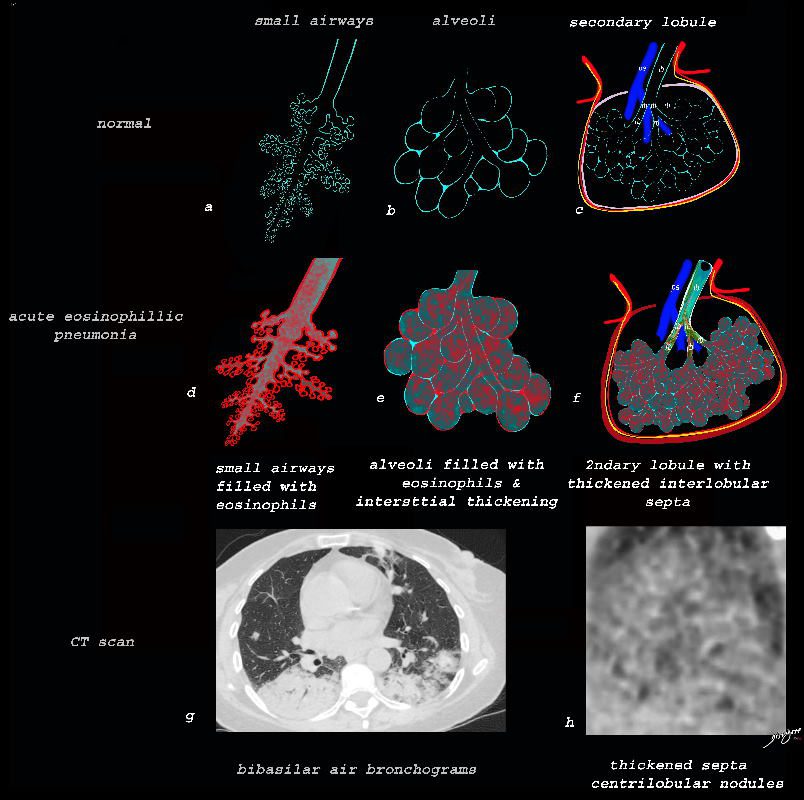
Ashley Davidoff TheCommonVein.net lungs-0757b

Ashley Davidoff TheCommonVein.net lungs-0757
Alveolar Proteinosis
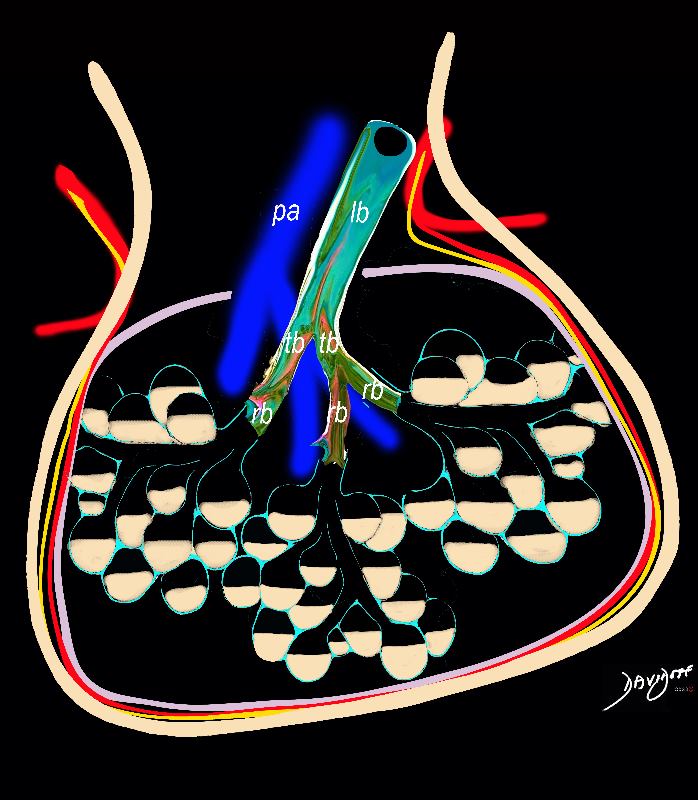
Accumulation of proteinaceous material in the alveoli, impairing gas exchange and leading to respiratory failure. Extensive thickening of interlobular septa leading to crazy paving appearance. Half filled alveoli lead to ground glass appearance
Ashley Davidoff TheCommonVein.net lungs-0738b
COVID

Actually a photograph of the Buttonbush reminiscent of the shape of the virus
Ashley Davidoff MD TheCommonVein.net lungs-0066

Ashley Davidoff MD TheCommonvein.net lungs-0069

Source of Contamination and then Transmission in Conversation
Ashley Davidoff MD TheCommonvein.net lungs-0052

A mere scratching of your chin could be fatal.
One of the best reasons to wear a mask is to remind you: hands off.
Please keep your hands off your face!
Ashley Davidoff MD TheCommonvein.net lungs-0051

Man buys meat at the wet market and corona virus spreads to his hands during the purchase or during food preparation.

The virus enters the lungs and travels to the smallest parts of the lungs, tiny lung sacs called the alveoli where oxygen exchange takes place
{kind=link}
008a.jpg
CELLULAR INVASIONCorona virus invades the cells of the alveoli by using its spike glycoproteins. These spike proteins attach to the cell membrane and the virus can then enter the cell.
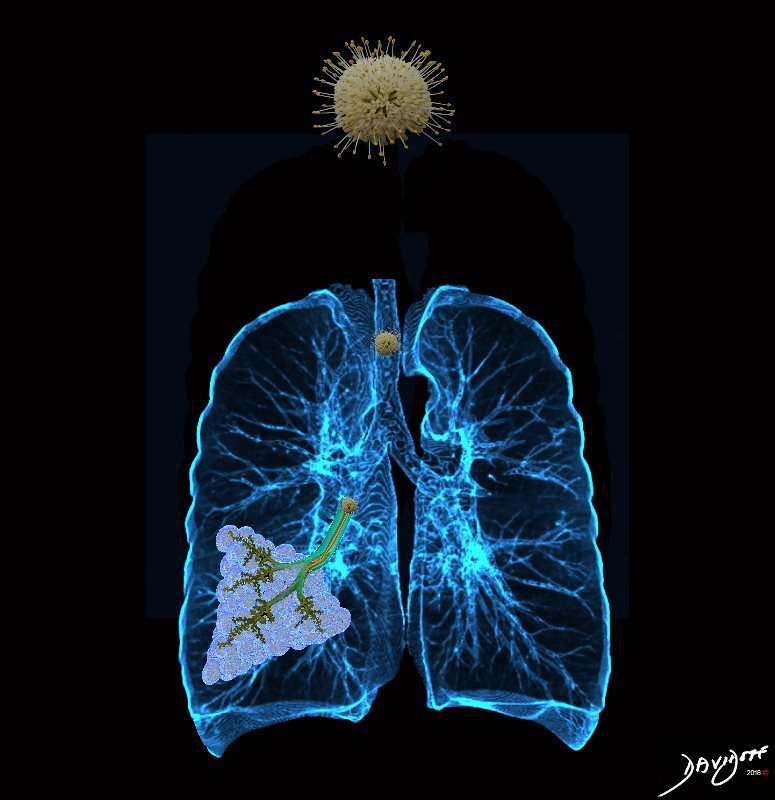
The virus enters the lungs and travels to the smallest parts of the lungs, tiny lung sacs called the alveoli where oxygen exchange takes place
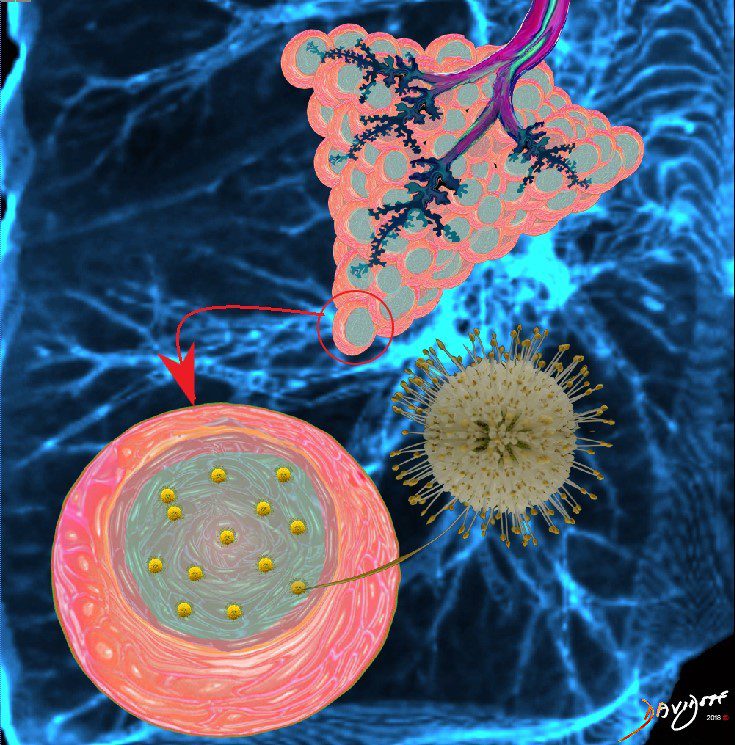
The virus replicates and invades more cells of the alveoli
As COVID-19 causes inflammation of the the lungs, infected fluid fills the lungs thus disrupting gas exchange.

The infection starts in small basal segments

and progresses to involve more and more lung
o his mouth and he inhales the virus. The virus does not proliferate if it is ingested, only if inhaled.