
Infection
Inflammation
Malignancy
Adenocarcinoma of Left Lung with Bilateral Lymphangitic Spread CXR

CXR of 50-year-old female with primary adenocarcinoma of the left lung shows extensive consolidation of the left lower lung field with diffuse bilateral reticulonodular changes reminiscent of lymphangitic spread of disease bilaterally
Ashley Davidoff MD TheCommonVein.net 158Lu 131022
Adenocarcinoma of Left Lung with Bilateral Lymphangitic Spread

50 year old female with primary adenocarcinoma of the left lung presenting with pneumonic consolidation of the left lung, and diffuse reticulonodular changes bilaterally
CT in a coronal plane shows intralobular nodules, nodular changes along the fissures, interlobular septa, and diffuse nodular thickening of the interlobular septa. These findings represent lymphatic spread along the lymphovascular bundles and are consistent with the diagnosis of lymphangitis carcinomatosa
Ashley Davidoff MD TheCommonVein.net 158Lu 131024
Mechanical/Atelectasis Trauma Metabolic Circulatory- Hemorrhage Immune Infiltrative Idiopathic Iatrogenic Idiopathic
Aspiration Pneumonia in a Background of Interstitial Lung Disease

55-year-old female with shortness of breath. CT (above) is from 4 years prior and shows an interstitial process characterized by ground glass and reticular change. The patient presents 4 years later with fever and white count and the CT (below) shows a pneumonic process in a background of ac chronic interstitial process with cystic air spaces and architectural distortion. Aspiration pneumonia was considered most likely
Ashley Davidoff MD TheCommonVein.net 135535
Chronic Eosinophilic Pneumonia (CEP)

CT scan in the coronal performed 6 months ago at the time of clinical presentation shows upper lobe predominant peripheral infiltrates more prominent in the left upper lobe. Subsequent diagnosis by BAL of chronic eosinophilic pneumonia (CEP) was made
Ashley Davidoff TheCommonVein.net

CT scan in the coronal performed 6 months ago at the time of clinical presentation shows upper lobe predominant peripheral infiltrates more prominent in the left upper lobe. Subsequent diagnosis by BAL of chronic eosinophilic pneumonia (CEP) was made
Ashley Davidoff TheCommonVein.net
Wedge Shaped Infarction
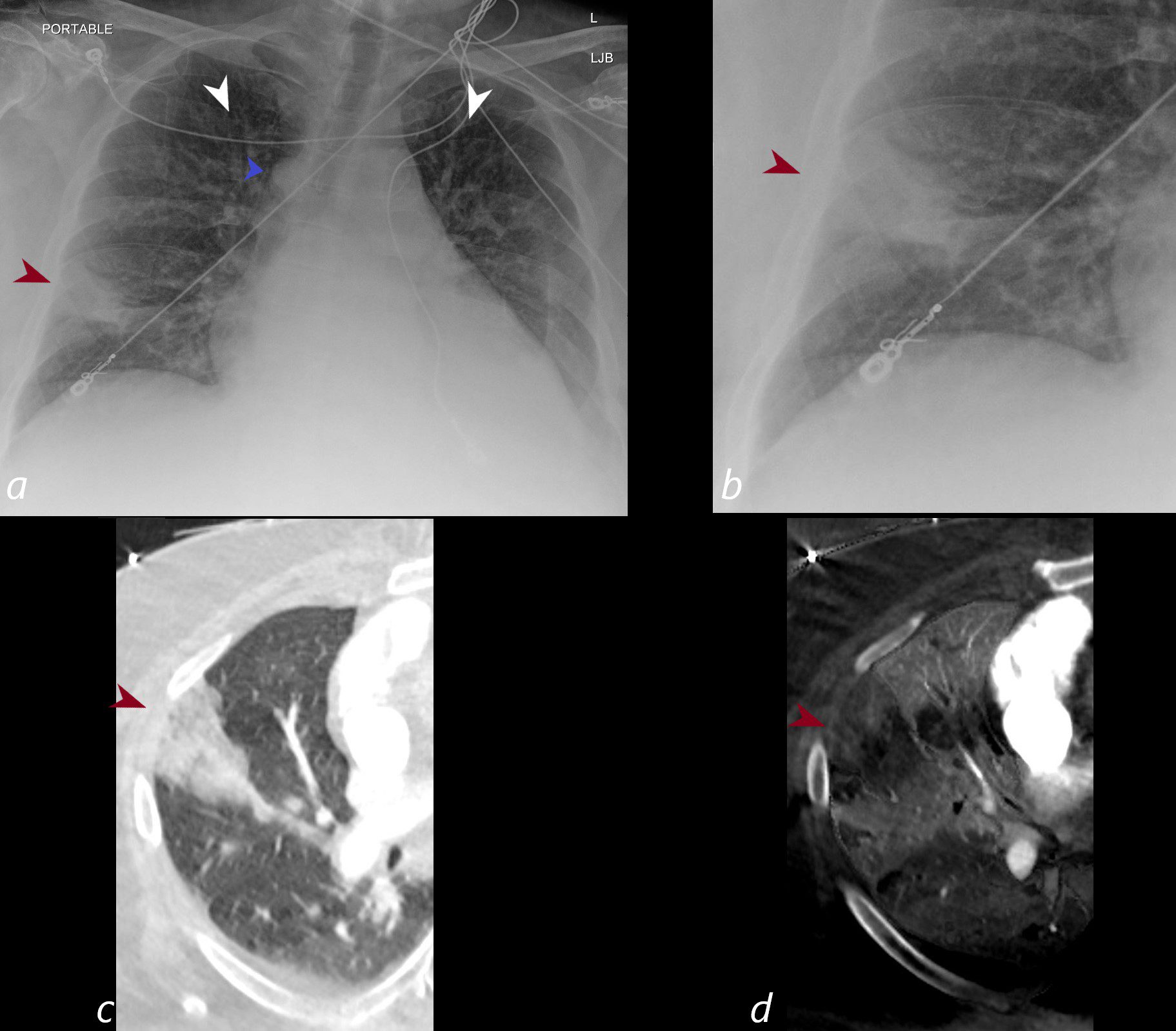
CXR shows a wedge shaped infiltrate in the middle lobe of the lung secondary to a pulmonary embolus (PE) characteristic of a Hampton’s hump (maroon arrowheads a,b) The infarction is confirmed on the CT with contrast (maroon arrowhead c) as well as the region of a perfusion defect (d- maroon arrowhead) In addition there is evidence of CHF on the CXR with cephalization of the vessels (white arrowheads c) cardiomegaly with left atrial enlargement, and enlargement of the azygous vein (blue arrowhead a)
Ashley Davidoff MD TheCommonVein.net)