
- The reticular pattern,
- characterized by a network of linear opacities
- reflects the presence of fibrotic changes in connective tissue structures including
- the interlobular septa
- intralobular tissues
- bronchovascular bundle
- interalveolar septa
- . The specific combination of involvement in these structures can provide additional clues to the underlying cause of the fibrotic lung disease.
The secondary pulmonary lobule is a functional unit of the lung that is typically defined by the structures supplied by a single small bronchiole. In fibrotic lung diseases with a reticular pattern on imaging, the involvement is often related to changes in specific structures within the secondary lobule. The primary structures affected include:
- Interlobular Septa:
- Involvement in Reticular Disease:
- Fibrosis or scarring of the interlobular septa can lead to
- thickening which can be irregular and incomplete
- increased opacity,
- Peribronchovascular Interstitium
- Fibrosis in the peribronchovascular interstitium can lead to a reticular pattern,
- especially if it affects the connective tissue around small bronchioles.
- Involvement in Reticular Disease:
- Subpleural Connective Tissue:
- Involvement in Reticular Disease: Fibrosis in the subpleural connective tissue
- Intralobular Septa:
- Involvement in Reticular Disease: Fibrosis of the intralobular septa can also contribute to the reticular pattern.
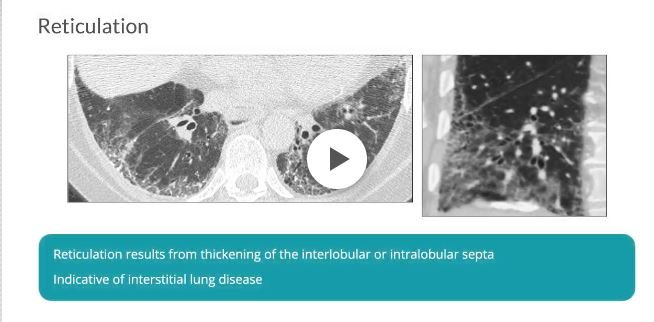
Reticulation results from thickening of the interlobular or intralobular septa and appears as several linear opacities that resemble a mesh or a net on HRCT scans.7 The presence of reticulation is indicative of interstitial lung disease.7 (Hansell DM, Bankier AA, MacMahon H, et al. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008;246:697-722.)
Radiology Rounds
- Subpleural reticulation
- typically in a peripheral subpleural distribution
- located ?1 cm from the pleura
- normal aging
- can be accompanied by subpleural cysts,
- independent of smoking history
- UIP
- bilateral basilar subpleural reticulation,
- traction bronchiectasis,
- architectural distortion and
- honeycombing
- normal aging
- UIP reticulation
UIP 05
reticulation subpleural
Case courtesy of Royal Melbourne Hospital Respiratory, Radiopaedia.orgUIP and Reticular Pattern
70 year old male with UIP and CHF showing extensive dominantly bibasilar and peripheral reticulation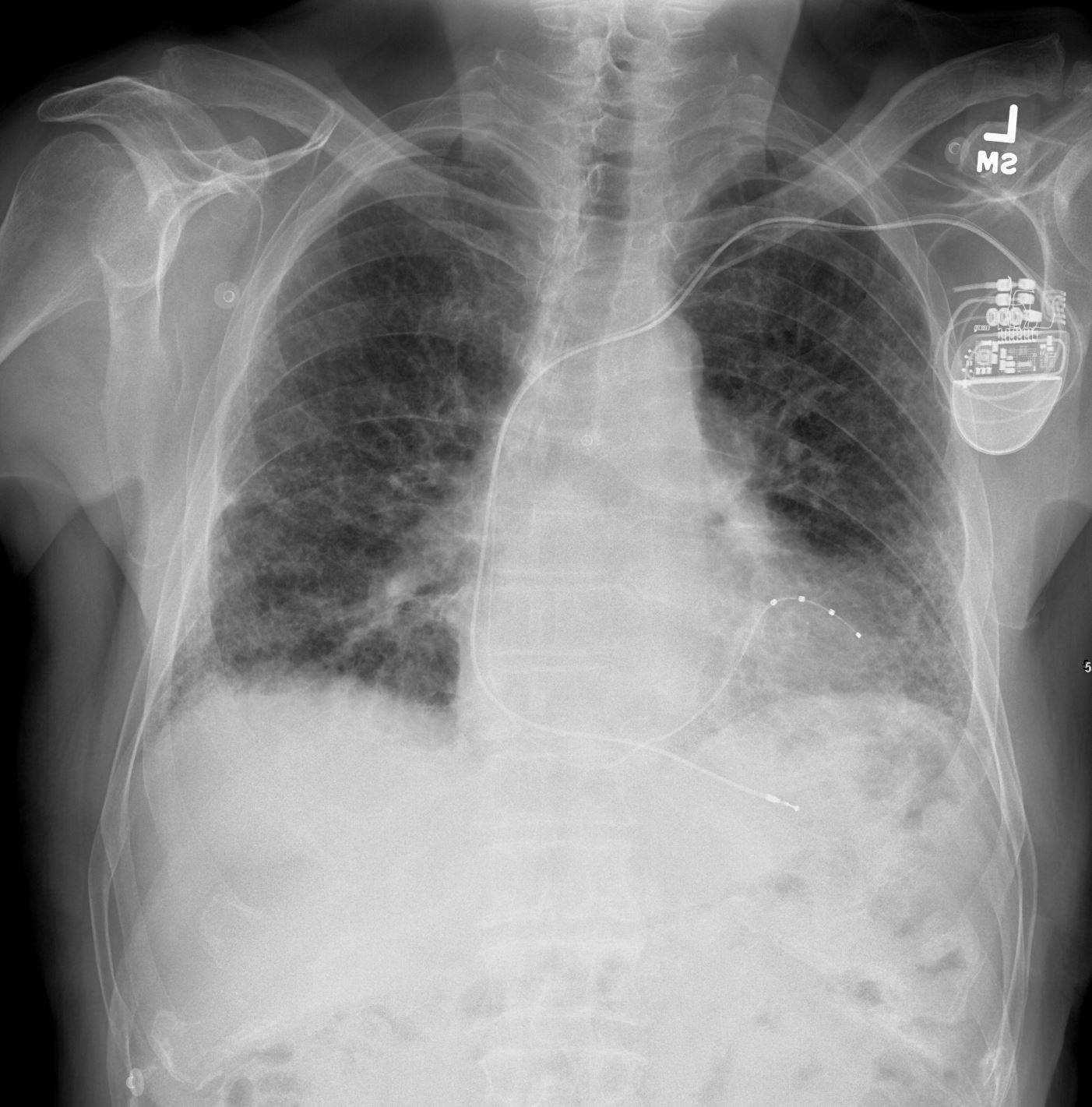
CXR UIP and Reticular Pattern
70 year old male with UIP showing extensive dominantly bibasilar and peripheral reticulation
Ashley Davidoff MD TheCommonVein.net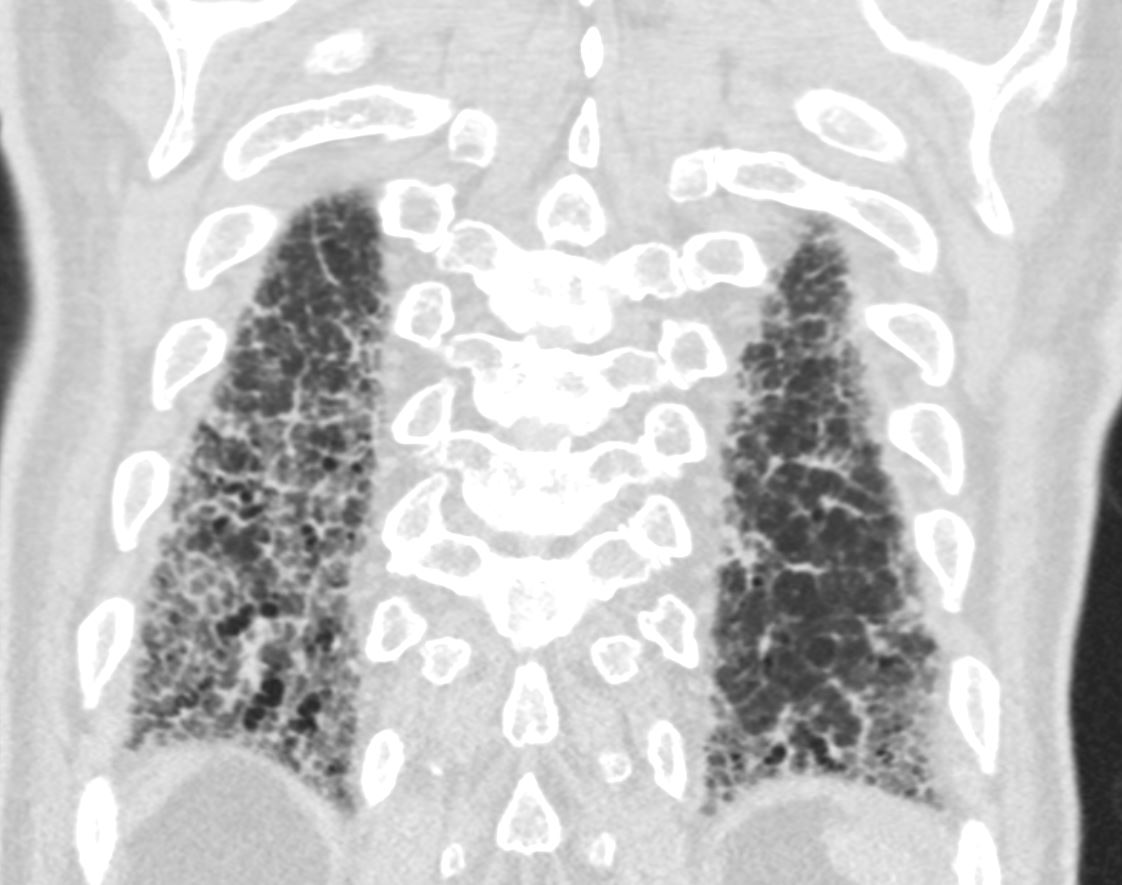
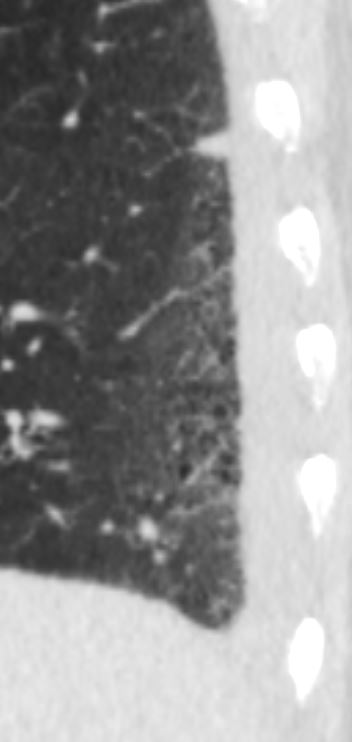
CT UIP and Reticular Pattern Thickened Interlobular Septa
70 year old male with UIP showing extensive dominantly bibasilar and peripheral reticulation
Ashley Davidoff MD TheCommonVein.net uip-004
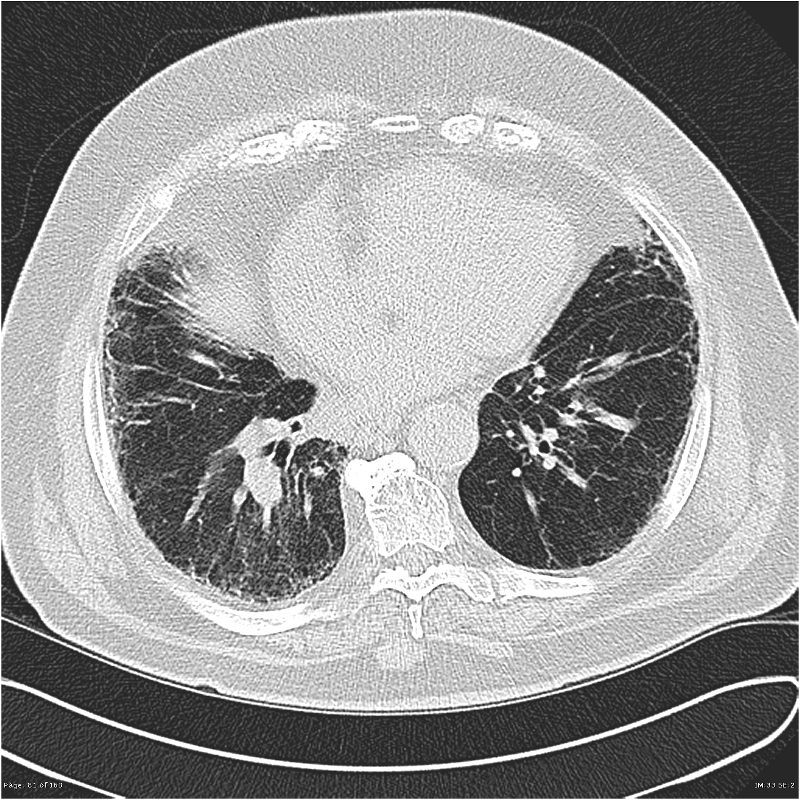
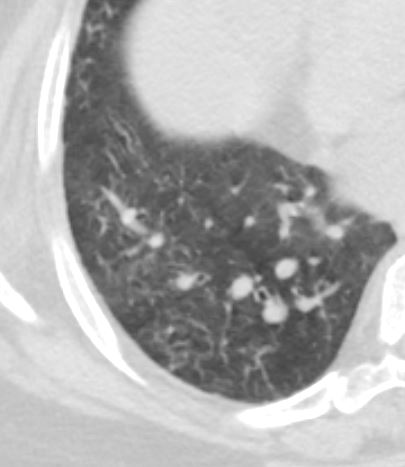
CT UIP and Reticular Pattern
70 year old male with UIP showing extensive dominantly bibasilar and peripheral reticulation
Ashley Davidoff MD TheCommonVein.net uip-003
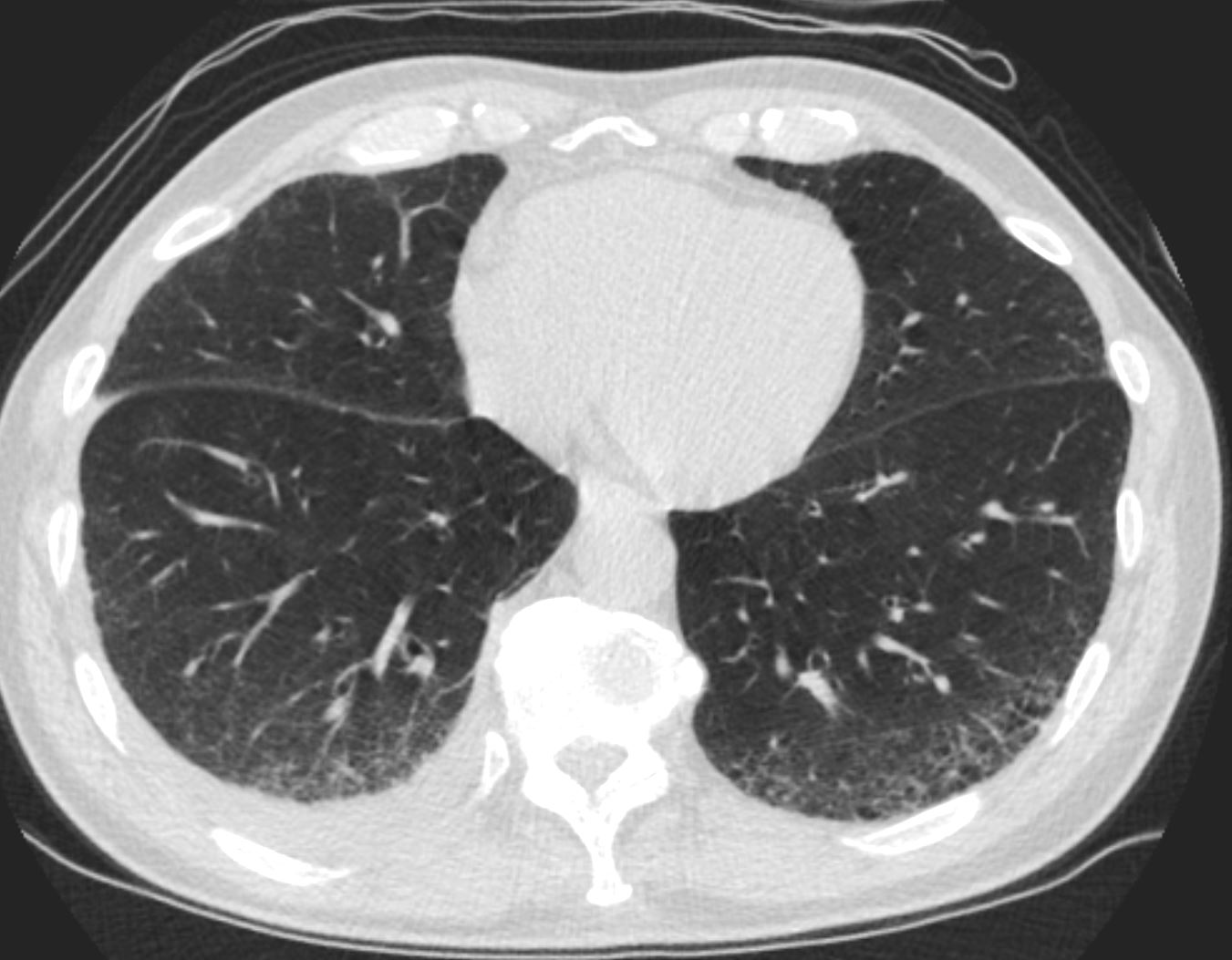
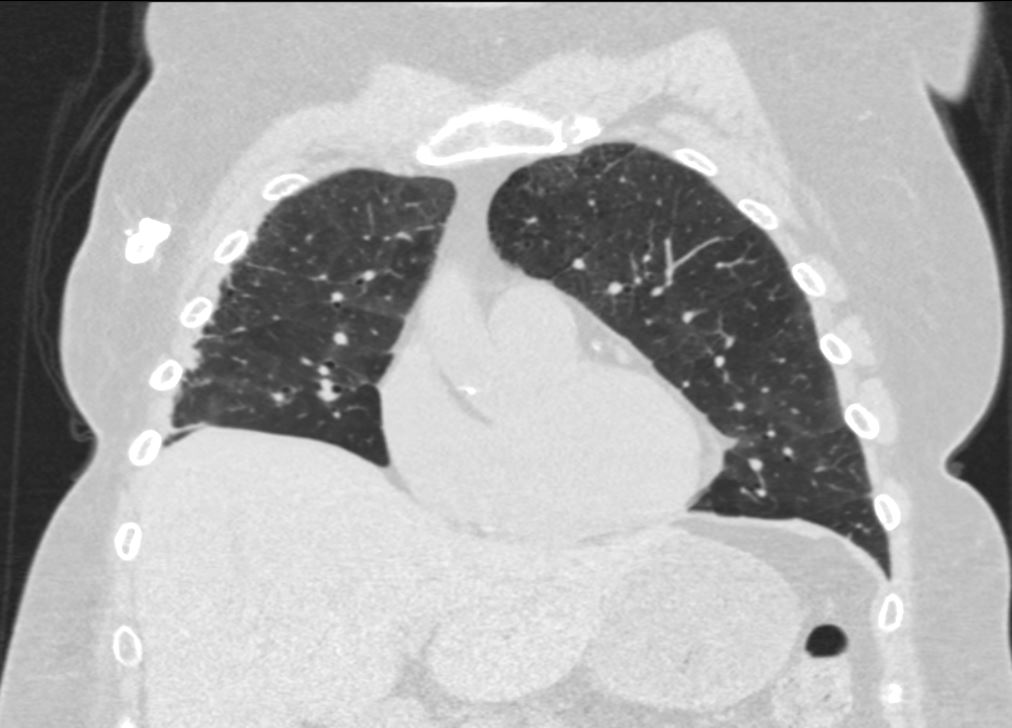
CT UIP and Reticular Pattern
70 year old male with UIP showing extensive dominantly bibasilar and peripheral reticulation
Ashley Davidoff MD TheCommonVein.net uip-002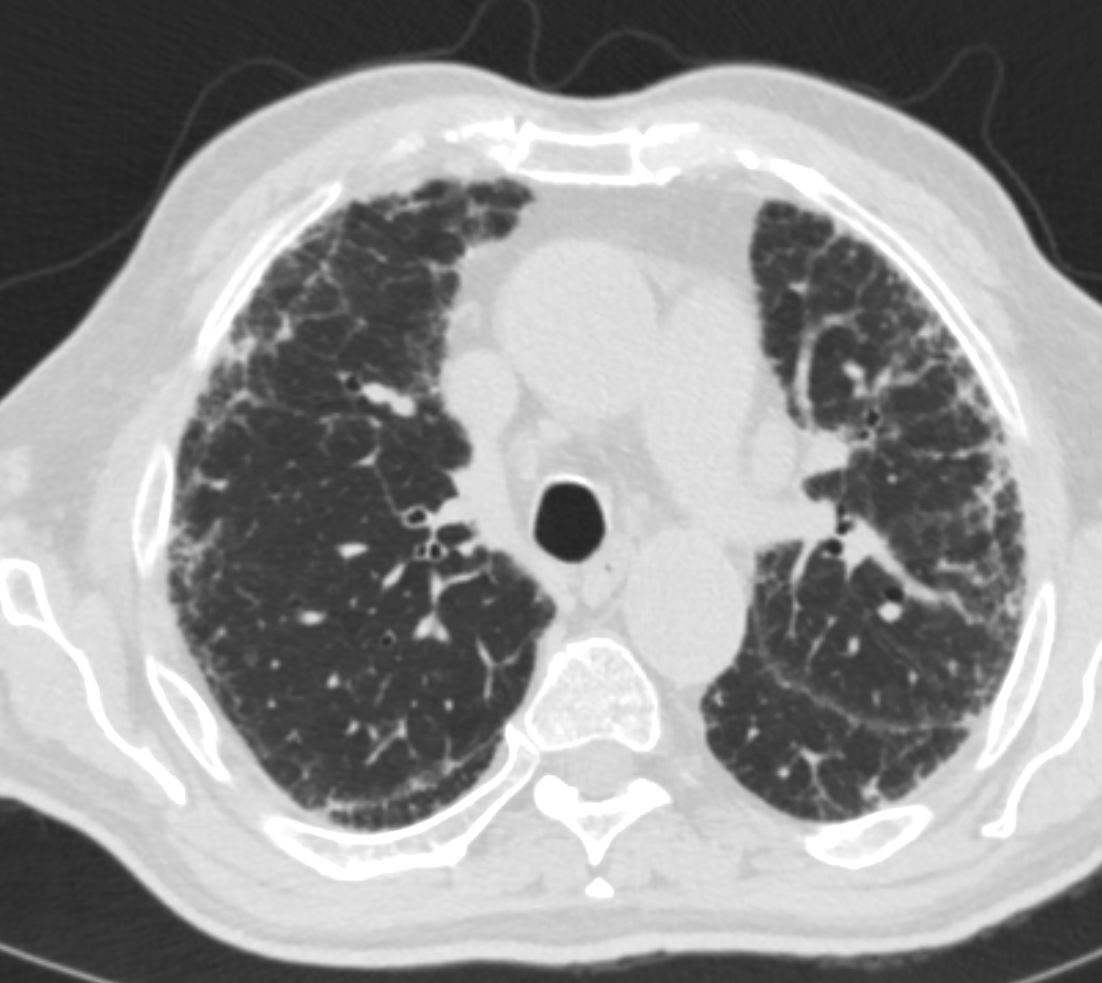
CT UIP and Reticular Pattern
70 year old male with UIP showing extensive dominantly bibasilar and peripheral reticulation
Ashley Davidoff MD TheCommonVein.net uip-005
CT UIP and Reticular Pattern
70 year old male with UIP showing extensive dominantly bibasilar and peripheral reticulation
Ashley Davidoff MD TheCommonVein.net uip-006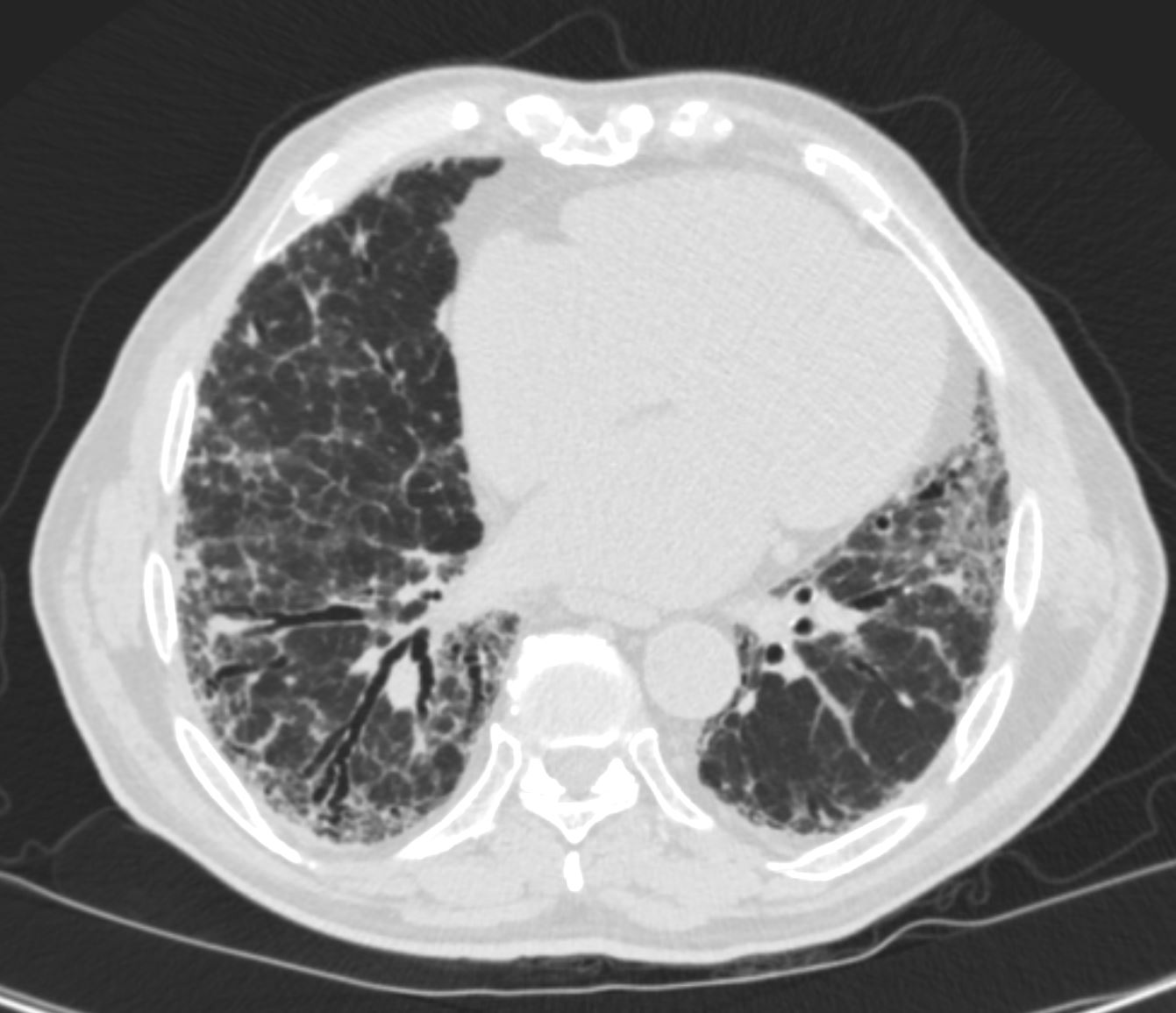
CT UIP and Reticular Pattern
70 year old male with UIP showing extensive dominantly bibasilar and peripheral reticulation
Ashley Davidoff MD TheCommonVein.net uip-007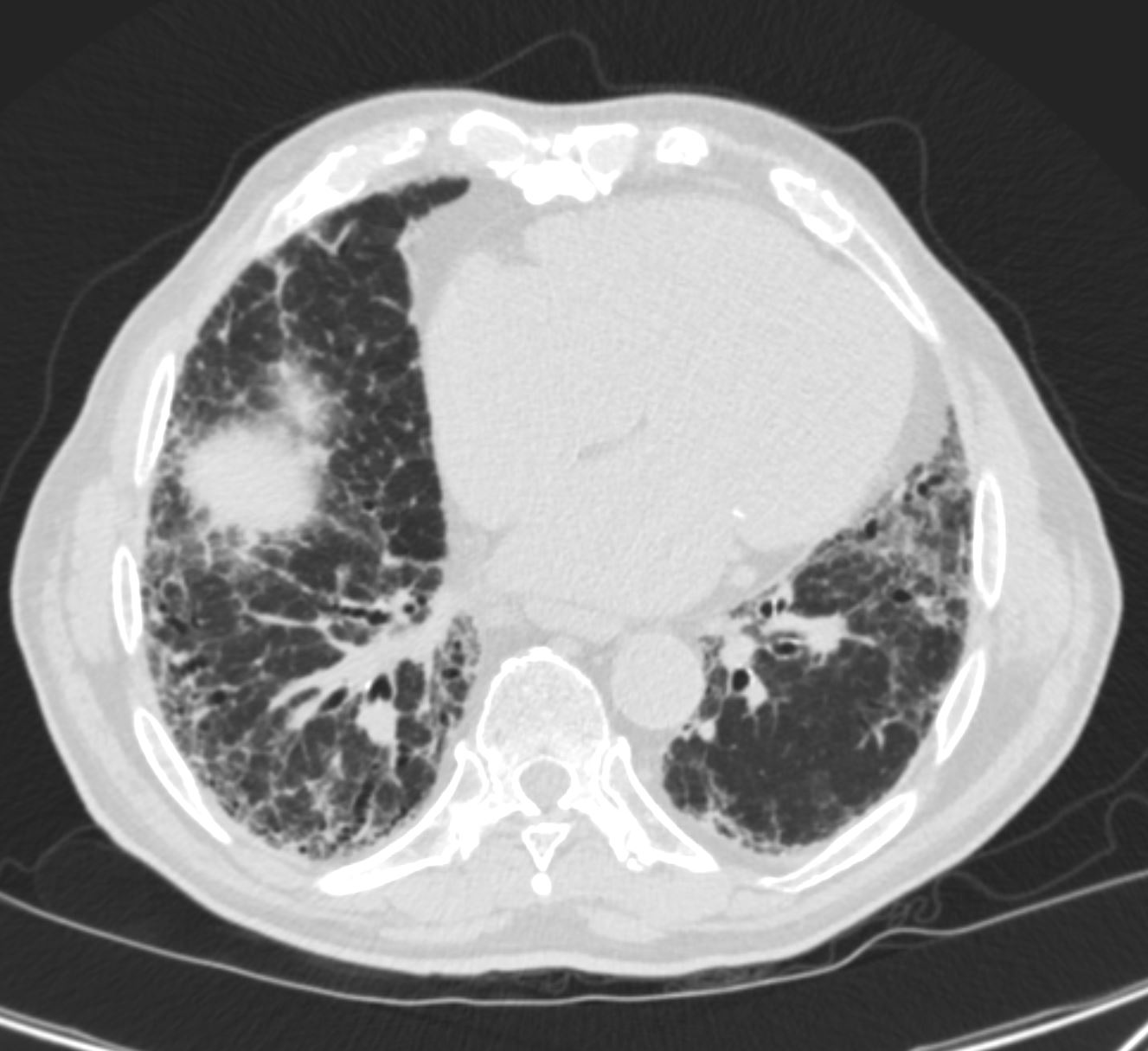
CT UIP and Reticular Pattern
70 year old male with UIP showing extensive dominantly bibasilar and peripheral reticulation
Ashley Davidoff MD TheCommonVein.net uip-008Reticular Changes Caused by Fibrosis of the Interlobular Septa
Combined Pulmonary Fibrosis and Emphysema

Ashley DavidoffMD TheCommonVein.net combined pulmonary fibrosis and emphysema 002
Ashley DavidoffMD TheCommonVein.net combined pulmonary fibrosis and emphysema 000b

Ashley DavidoffMD TheCommonVein.net combined pulmonary fibrosis and emphysema 000c

Ashley DavidoffMD TheCommonVein.net combined pulmonary fibrosis and emphysema 003
Ashley DavidoffMD TheCommonVein.net combined pulmonary fibrosis and emphysema 004
-
Post COVID 19
-
Reticular fibrosis post COVID
Ashley Davidoff MD TheCommonVein.net - Diffuse Reticular Lung Disease
- PCP HIV
-

PCP Pneumonia
46 year old female with HIV presents with dyspnea. CXR scan shows a diffuse reticular pattern with suggestion of upper lobe predominance
Ashley Davidoff MD TheCommonVein.net 30755c
PCP Pneumonia
48 year old male with HIV presents with dyspnea. CT scan shows a reticular pattern within ground glass background, dominantly in the lower lobes, and affecting the right lower lobe more than the left
Ashley Davidoff MD TheCommonVein.net 30755cReticular Changes Post XRT

Reticular Changes Post XRT
Ashley Davidoff MD
TheCommonVein.net
Reticular Changes Post XRT
Ashley Davidoff MD
TheCommonVein.net
{kind=link}