
The lungs are two huffing and puffing sponge-like organs that dominate the chest cavity, essential in their function as the principle structures of respiration. An understanding of their unique anatomy and physiology brings understanding of how diseases will affect the lungs, and how these changes will manifest on X-ray and CT evaluation. In this first part of the series on the lung we emphasize principles, and outline how structure is integrated with function, disease, and imaging. The unique structural characteristics of the lungs include:
Dominance in the chest cavity
Ability to accommodate the entire cardiac output with every heartbeat
Asymmetric nature
Irregular and dichotomous branch pattern of the bronchovascular bundle
Tubular transport system, with a single system functioning for both delivery and removal
Spongy air-filled character
Pyramidal or cone shape
Dual blood supply
The unique functional aspects include:
The ability to move air efficiently
The ability to exchange gases efficiently
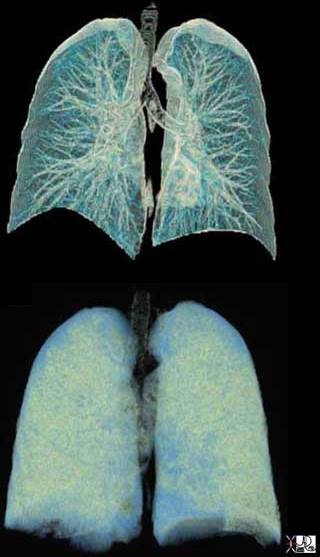
Anatomic Range of the Respiratory System
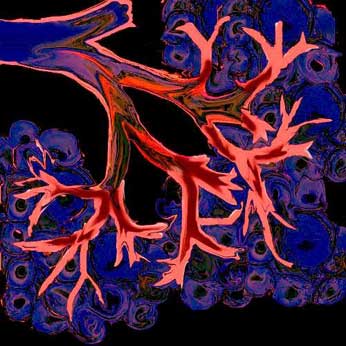
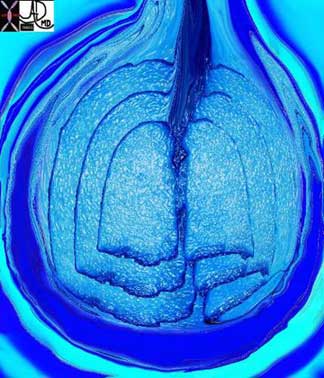
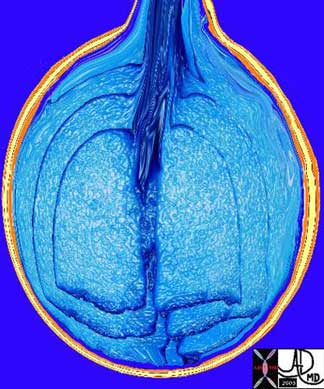
This collage reflects the anatomic range of the respiratory system from the macroscopic to the microscopic ? a continuum of structure.

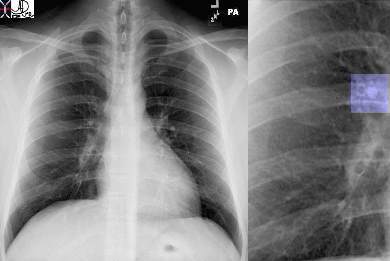
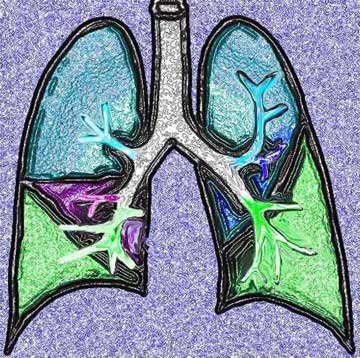
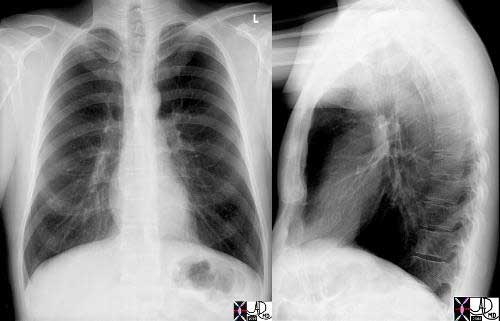
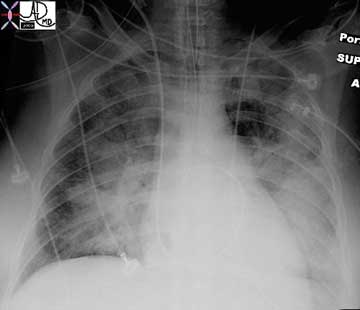
Image 3: The chest X-ray, shows the lucent lungs within the thoracic cavity.
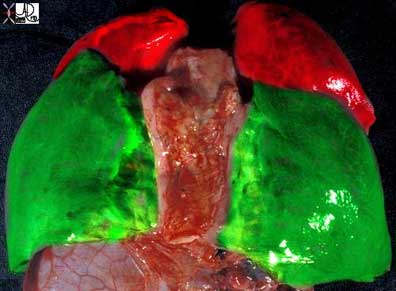
Image 4: A diagram of the trilobed right lung and the bilobed left lung.
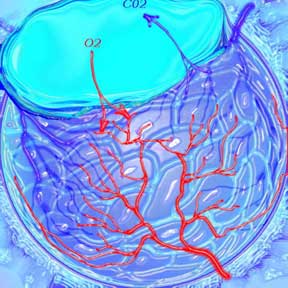
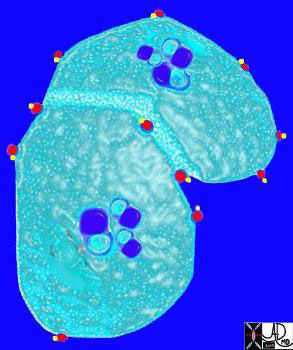
Image 5: Two respiratory units of the lung are shown in the next image, each called a pulmonary lobule. The lobule consists of a central bronchiole (light blue) and pulmonary arteriole (dark blue), surrounded by the air filled acinus (teal) with its peripheral venules. (red)
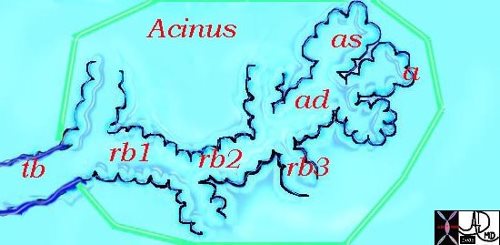
Image 6: The acinus is magnified in image 6, showing first the tubular terminal bronchiole branching into the respiratory bronchioles, alveolar sacs, and finally the grape like alveoli.
Image 7: The organization of the connective tissues of the lung.
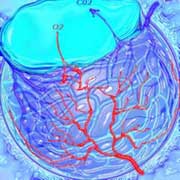
Image 8: Finally we get down to the grapes or alveoli of the lung with surrounding vessels (8),
Image 9: A single alveolus is shown.
Courtesy of: Ashley Davidoff, M.D.
It seems a long way for the air to travel but the system can deliver the air to and from the outside in a single breath, and exchange the gases at the capillary level even more rapidly. It is a remarkable system.
Overview
As we progress through the module there is a recurring pattern of the dual function of the respiratory apparatus ? an airway system that transports the air, and an exchange system that enables transfer of the gases across the alveolar membrane.
The lungs are part of a larger system called the respiratory system. The role of the lungs is to deliver ambient air (ventilation) to the alveoli and to act as the agent for gas exchange by contributing one layer of epithelium to the bilayered membrane, a double layer that serves as the ultimate interface for gas exchange. The primary role of the pulmonary arterial circulation is to transport blood to the alveolar interface (perfusion) and to also play a part in the exchange of carbon dioxide and oxygen by providing the second layer of the bilayered filter. It is the homeostatic aim of the body to match the ventilation with the perfusion, in order to maintain uniform ventilation (V) to perfusion (Q) ratio (V/Q).
The lungs are exposed directly to the air in the atmosphere and to the blood within the circulatory system. Through the lungs the blood is therefore exposed to the atmosphere, which on the one hand contains life-sustaining oxygen but on the other can present a hostile environment filled with microorganisms, industrial chemicals, and toxic fumes.
Courtesy of: Ashley Davidoff, M.D.
The lungs are made of expandable, sponge-like tissues. Their close proximity to the heart and circulatory system allows for rapid exchange of gases between the air and the circulatory system as noted above. This function is easily accomplished during rest, where resting respiratory rate in an adult is about 12 breaths per minute and heart rate 72 beats per minute. During exercise the respiratory rate can increase to 40-50 breaths per minute and the heart rate, increasing in concert, can reach 180-200 per minute. The interface of circulation with the respiratory system has to be sufficiently equipped to allow delivery, uptake, and exchange of gases at this accelerated pace. The key soldier in the exchange of oxygen is a complex protein called hemoglobin, which lies in the red cell.
I imagine the hemoglobin molecule scurried by the forces of the right ventricle into the pulmonary circulation. As it enters the chambers of exchange, the open windows of the lungs herald the fresh air. Under basal conditions, the hemoglobin gnome can work at a leisurely pace filling his baskets with oxygen. Under exercise conditions he has to start working like crazy, grabbing molecules of oxygen and stacking these into his storage baskets, surrounded by an accelerated pace with gale-like air forces and flood-like blood conditions. Hemoglobin is a remarkable molecule and can adapt its function to these extremes in physiology.
Carbon dioxide is a by product of body metabolism and is dissolved in the blood. Exchanges between the circulation and alveoli occur rapidly and efficiently across the alveolar membrane due to differences in the partial pressure of gas between the blood and the alveoli.
Courtesy of: Ashley Davidoff, M.D.
Examination of the lungs with a stethoscope
The presence of a structure in the body that is almost totally filled with air makes it a unique, challenging, and rewarding organ to examine clinically and radiologically. Examination of the lungs with a stethoscope enables the clinician to evaluate inspiratory and expiratory movement of air. Some pathologic conditions, including aspiration of a foreign body, collapsed lung, or inadvertent intubation of the bronchus, result in airway obstruction. In these conditions there is no air entry into the affected bronchus and subtended lung. The clinical finding of the lack of air entry, based simply on the lack of air sound, can be a life saving diagnostic maneuver.
Unusual but interesting words are used to describe the sounds of air character and movement on clinical examination. These include percussion, tactile fremitus, bronchophony, whispering pectoriloquy, and egophony and relate to the way air moves through the airways, and how the transmission may change when there is fluid in the pleural space or in the lungs. When the air mixes with the fluid, characteristic sounds such as rales and crepitus will result.

Courtesy of: Ashley Davidoff, M.D.
Imaging the Chest
From the radiological point of view, x-rays used in plain chest x-ray (CXR) or CT scan move almost unimpeded through the lungs, and present as a radiolucency or blackness on the image. On the other hand, the mediastinum serves as a moderate barrier to x-rays, and the ribs and spinal column present an even greater barrier. The tissues of the chest vary significantly in the degree to which they absorb or reflect x-rays. This difference presented a challenging problem to radiologists and physicists over the years, particularly related to technical factors that would optimize imaging of the mediastinum and heart on the one hand, and the lungs on the other. The advent of CT scanning with a superior gray scale, and with digital technology, has helped solve this problem, so that we are able to window in to the gray scale of the specific part being imaged. We can, for example, look specifically at the lungs using the gray scale and window level appropriate for the lung, (lung windows) for the mediastinum (mediastinal windows) or for the bones (bone windows).

Courtesy of: Ashley Davidoff, M.D.
What structures do we see on x-ray?
Why do we see structures on x-ray? We are able to define two side-by-side structures if they have contrasting x-ray absorption characteristics and hence densities. On a plain film of the chest for example, the trachea and main bronchi are usually visualized because the air filled trachea is surrounded by relatively thick soft tissue walls and other soft tissues of the mediastinum creating the necessary density differential to enable distinction. The air in the visible mainstem bronchi is surrounded and separated from the surrounding air filled parenchyma and by relatively thick walls of soft tissue density and this contrasting density allows the mainstem bronchi to be seen. As we progress to the smaller bronchi, usually after the fourth order of branching, the soft tissue walls become too thin to create an air-soft tissue interface and hence we cannot resolve nor see them.
Almost 90% of the lung is air and only about 10% is soft tissue, interstitium and blood. The dominant density of the lungs is therefore black or lucent. The soft tissues of the lung, including the blood vessels and the connective tissue (also called the interstitium), impede the x-ray, resulting in a gray or soft tissue density. The interface of lucent air (black) against a soft tissue background of the interstitium (gray) provides a sharp and contrasting interface of density, allowing an almost microscopic view of the lungs. If the pressure in the capillaries becomes abnormally high, for example more than 25 mmHg, fluid starts to leak into the interstitium. The clarity of the interstitial markings becomes reduced and blurry. The radiologist is able to imply pathophysiological changes based on the fuzziness of the blood vessels and can approximate the pressure in the capillaries. This change is best appreciated on a plain film of the chest. The plain chest film has stood the test of time, proving its value since Roentgen?s discovery in the late 19th century.
Courtesy of: Ashley Davidoff, M.D.
42464c02
Most disease states replace the air of the lungs with fluid or soft tissue, and appear as increasing densities on the CXR. In pneumonia the alveoli become filled with pus or fluid. The air in the lung parenchyma is replaced by soft tissue elements. If there is persistence of air in the smaller airways, they will now be visualized, since the air in the airways is now in contrast to the surrounding density of the fluid filled parenchyma. This sign is called an ?air bronchogram? and is characteristic of consolidated lung with a patent airway.
CT with a wider gray scale enables us to visualize subsegmental bronchi and bronchioles both in normal conditions and under various pathological situations.
Courtesy of: Ashley Davidoff, M.D.

Courtesy of: Ashley Davidoff, M.D.
42480F
42480b02F
Flow: Basic Principles
The function of air transport is the domain of the tracheobronchial tree, which as a tubular system has to obey the universal principles of flow within a tube. At the terminal end of these tubes are epithelial-layered grape-like clusters where gas exchange takes place. The principles of exchange of gases across a membrane are also universal in the body. If you understand flow in tubes, and exchange of gases, chemicals, and molecules across a membrane, you can apply the understanding to many aspects of body function.
Flow will only occur when a pressure difference exists between the two sides of the tubes. When we breathe in, the intercostal muscles contract and expand the chest laterally and the diaphragm moves down, increasing the volume of the chest cavity in a craniocaudal dimension. As a result, the alveoli expand, causing a negative pressure in the alveolar side of the tubes. The pressure in the atmosphere is higher and thus air will flow from a high-pressure system to a low-pressure system ? i.e. from the atmosphere to the lungs. During expiration, the elastic nature of the chest, with the relaxation of intercostal muscles and diaphragm, result in a return of the chest to its pre inspiratory position. The chest therefore is in a contracted size, causing a relative increase of pressure in the alveoli when compared to the atmosphere, and air will flow from the alveoli to the atmosphere. Inspiration is therefore an active process requiring energy and muscle contraction, and expiration is a passive process of elastic recoil.
Courtesy of: Ashley Davidoff, M.D.
32645b04b04
Flow: Basic Principles: Velocity of Flow
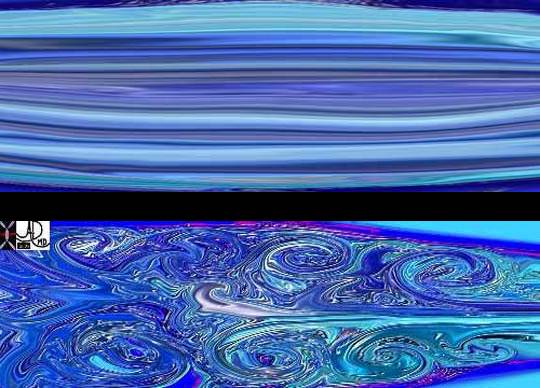
Velocity of flow relates to factors such as tubular diameter, resistance, friction, and pressure differences, as well as the nature of the medium being transported. Velocity of flow will also depend on whether the flow is laminar or turbulent. If it is laminar, it will be governed by Poiseuille?s law, which states that velocity of flow is directly proportional to the driving pressure.
As velocity increases, flow becomes turbulent and Poiseuille?s law does not apply. Flow in the larger parts of the airways tends to be turbulent and in the smaller tubes it is laminar. Under resting conditions, laminar flow exists from the medium-sized bronchi onward down to the bronchioles. During exercise, the airflow is accelerated, and laminar flow may be confined only to the very small airways. Laminar flow is quiet while turbulent flow is noisy. Thus when your doctor or nurse places a stethoscope on your chest and asks you to breath in and out, they are listening to the turbulent flow in your larger airways. The audible ?huffing and puffing? that occurs with exercise results from greater forcefulness of the muscles in an attempt to get more air in and out, and the turbulence becomes audible even without the stethoscope.
Courtesy of Ashley Davidoff M.D.
42433b04
42434b07
Quiz Me
If flow is turbulent, it will be governed by Poiseuille?s law.
True False
Resistance to flow depends on sympathetic tone of the smooth muscle, which governs the radius. Radius has a very powerful effect on the velocity of laminar flow. Very small changes in radius result in large changes in velocity. In health, the sympathetic tone is well balanced with the needs of a person?s physiology. However, if the tone is increased due to environmental allergens or exercise induced spasm, then tone may increase to the extent that it limits air movement and the patient becomes short of breath. Wheezing is the resulting sound of turbulent air through constricted bronchioles, which can be heard and felt by the clinician and the patient.
The tracheobronchial system is beautifully designed to enable rapid and efficient delivery of relatively clean air to the alveoli. Not only is the delivery rapid, but also it is uniform throughout the lung. The design is such that with a single inspiration, the fresh air reaches all alveoli (whether they are at the base or apex of the lungs), simultaneously. What a system! If we, in the world at large, could deliver an equal and adequate amount of supplies efficiently and simultaneously to all, at the precise time when needed, we would have a much happier world. Not only is it a system that delivers efficiently to the alveoli, but also its second function is to return with waste for delivery to the atmosphere. No other tube in the body performs this dual function of back and forth movement through the same piece of tubing. The gastrointestinal system will deliver via the esophagus, stomach and small bowel but excretion is via the large bowel. In the cardiovascular system the arteries deliver and the veins remove. They are one-way streets whereas the airways are a two-way system.
Flow: Airways and Blood Vessels
The lungs are divided into lobes, segments, subsegments, lobules, acini, and alveoli. An appropriate conduit group, meaning an artery, vein and lymphatic, accompanies each of these parts. The tracheobronchial tree is composed successively of the trachea, mainstem bronchi, lobar bronchi, segmental bronchi, terminal bronchioles, respiratory bronchioles, and alveolar ducts. The respiratory tree divides into paired branches of unequal length and diameter. This arborizing format is called an irregular dichotomy. Gas exchange starts at the respiratory bronchiole and becomes progressively more efficient and effective as the respiratory bronchiole progresses to the alveolar ducts, then alveolar sacs and finally the alveoli. The preliminary exchange of gases at the pre alveolar level enhances the delivery and exchange to the alveoli.
Courtesy of: Ashley Davidoff, M.D.
32686b05
Flow: Airways and Blood Vessels: The Arteries
The accompanying arteries include the main pulmonary artery (MPA), the right pulmonary artery (RPA), and the left pulmonary artery (LPA). The lobar arteries, segmental and subsegmental arteries follow, which finally become the arterioles, which are the smallest arteries. When the arteriolar wall becomes one cell layer thick it is called a capillary.

32687b01
Courtesy of: Ashley Davidoff, M.D.
Flow: Airways and Blood Vessels: The Bronchovascular Bundle
The bronchovascular bundle, as the name implies, consists of a combination of bronchi and vessels (in this case arteries), and it is positioned in the middle of the pulmonary lobule. The lobule (a.k.a. secondary lobule) is the unit of lung parenchyma consisting of three to five respiratory bronchioles and arteries with their progeny. The progeny of the respiratory bronchioles are given specific names starting with the alveolar ducts, and progressing through the alveolar sacs and finally the alveoli. The lobule is surrounded by a membrane of connective tissue that contains lymphatics and venules. We will describe this unit extensively in a coming section. The position of bronchovascular bundle is centrilobular, meaning that it is in the center of the lobule, while the venous and lymphatic conduits are distributed around the periphery of the lobules. Lymphatics sometimes accompany the bronchovascular bundle as well.
Courtesy of: Ashley Davidoff, M.D.
42440b08
Flow: Airways and Blood Vessels: Venous Drainage
Venous drainage is usually via one major upper lobe and one major lower lobe pulmonary vein to each lung, but clinically significant variations do exist. Segmental and subsegmental veins and venules are the equivalent subdivisions of the veins. The capillaries surround the alveoli.

Courtesy of: Ashley Davidoff, M.D.
37756b01
Flow: Applied
In the clinical world the sounds of air movement are caused by turbulent airflow and these sounds are evaluated by the stethoscope. The stethoscope is also a simple tubular structure with a membrane on its far end. There is normal airway turbulence in the larger airways and so it is normal to hear air movement in the lungs during inspiration and expiration. Inspiration is noisier and shorter in duration than expiration. The larger the diameter of the airway, the higher the pitch of the sound, while the smaller the diameter, the lower the pitch.
With anaphylaxis or foreign body inhalation, there are varying degrees of obstruction of the upper airways and an audible high-pitched sound on inspiration can be heard. This sound is called stridor. Anaphylaxis could affect the larger and / or the smaller airways. If the proximal larger airways are affected then stridor results, and if the smaller airways are affected then wheezing is heard.
If the stridor is caused by anaphylaxis then epinephrine may be required, whereas if it is caused by aspiration of a piece of poorly chewed steak then the Heimlich maneuver is required. If you are in a restaurant when a patron clutches his throat and stridorous noises are heard, the question to ask would be ?meat or shrimp?? If the person were eating steak then the Heimlich maneuver would be indicated, and if it were shrimp and accompanying signs of hives and facial swelling were present and severe enough, epinephrine would be necessary. Either way, acute stridor is a serious and life threatening situation.

Courtesy of: Ashley Davidoff, M.D.
32467b05
In an acute asthmatic attack the problem lies in the smaller airways. As stated above, in the normal patient, flow at this level is usually inaudible because of its laminar nature. The narrowing caused by muscle spasm and secretions occurs at the level of the smaller bronchi and the turbulence that results is heard as a wheezing sound on expiration. Why expiration and not inspiration? Good question. On inspiration the chest cavity expands and so do the alveoli and bronchioles. The change in size of the bronchioles with inspiration is often sufficient to allow laminar flow to persist, and hence no sound will result. On expiration the diminishing size of the chest cavity causes the bronchioles to recoil, resulting in a smaller diameter, and together with the spasm will result in air trapping, turbulence and wheezing. If the spasm is severe, there may be wheezing both on inspiration as well as expiration. Emphysema and chronic bronchitis are also causes of wheezing during exhalation. In all these conditions the overall intake of air exceeds the volume exhaled, and so the net result is air trapping and increase in the lung volume.
If there is a large amount of air trapping, the radiologist will see the larger air volumes as hyperexpanded or hyperinflated lungs. In such cases, if one counts the posterior ribs on the CXR, more than 10 posterior ribs will be visualized above the diaphragm. Flattening of the diaphragms also will occur and is best seen on the lateral CXR. Since a large portion of the air seen in the large lungs is static air, it will contain a higher level of carbon dioxide and relatively lower levels of oxygen. In severe asthma, poor oxygenation of the blood results and oxygen saturation falls. The air trapping seen in emphysema is caused by a loss of elasticity of the alveoli and abnormal overexpansion of the alveoli. With larger surface areas and hence volumes, there is an increase ventilation (V) without an overall appropriate increase in perfusion (Q), resulting in a V/Q mismatch, and thus inadequate gas exchange.
Courtesy of: Ashley Davidoff, M.D.
41987c
In an acute asthmatic attack, wheezing can be heard on inspiration.
True False
Lung Movement: Basic Principles
The lung is often compared to a bellows system, meaning that with alternate expansion and contraction, air travels one way through a tube during expansion and is expelled the other way when the mechanism recoils.
Inspiration is an active process requiring muscle contraction and therefore energy, while expiration is a passive process of elastic recoil requiring no energy. As noted, one of the unique features of the lung is its ability to act as a two-way transport system. No other tube in the body is asked to perform this dual function. At first this seems like a simple demand on the system, but as you will see it is more complicated than a simple bellows system, and a fine balance exists between the complex forces of inspiration and the complex forces of expiration. Biology has had to make some considerable adaptations in order for the dual function of the airways to coexist.
Courtesy of: Ashley Davidoff, M.D.
Lung Movement: 5 Layers
There are five general functional layers to the bellows system. They include the bony cage, the muscle layer, the pleural layer, the lung and the layer of surfactant. The combination of bony, muscular, membranous, spongy, elastic, and chemical properties of the complex described, keeps the air moving in and out efficiently.

Courtesy of: Ashley Davidoff, M.D.
42530b05b09b01a08
First Layer ? Bone
The bony cage of ribs, sternum and spine create an outer protective layer with the sternum and spine being the relatively rigid components and the ribs acting as the pliable component. The ribs have been compared to bucket handles as they move up and out during inspiration pivoting on the sternum and spine which act as two fixed points.

Courtesy of: Ashley Davidoff, M.D.
42530b08
Second Layer ? Muscle
The second layer includes the diaphragm inferiorly, the intercostal muscles circumferentially, the serratus anterior anterolaterally, scapular elevators posteriorly, and erector spinae muscles posteriorly. Superiorly the scalene and sternocleidomastoid muscles assist when necessary. The abdominal muscles also play a role as accessory muscles of respiration since movement of the chest cavity has effect on the abdomen, and vice versa. In fact, a principle to always keep in mind is that no cavity, system, organ, or cell is an isolated island ? they all in the end work in concert for the greater health of the whole. John Donne, an English poet of the 17th century, proposed that ?no man is an island,? promoting the same concept of the interconnectedness of all.
During inspiration the diaphragm moves down and intercostal muscle contraction causes outward chest vectors, resulting in chest cavity expansion. As a result there is a decrease in intrathoracic pressure and airflow into the lungs. When the muscles relax, the diaphragm flattens, the intercostals return to baseline position by passive and elastic recoil, and the chest moves inward, causing the chest volume to decrease. The intrathoracic pressure rises and becomes higher than the atmospheric pressure and therefore air will move outward from a position of high pressure to one of low pressure.

Courtesy of: Ashley Davidoff, M.D.
42530b05b09b14
Third Layer ? Pleura
The third layer is the double-layered pleura, with one component intimately attached to the chest wall, and the other layer intimately attached to the lung. Between them there is a thin layer of fluid that binds the two layers together by capillary action. The pleural surface constantly absorbs the fluid or gas that enters the space and a negative pressure of about 10mm Hg is maintained. We have all experienced the power of the thin fluid layer of water between two clean smooth surfaces of glass, which cannot be pulled apart because of the adhesive and cohesive capillary action. Capillary action is the interaction between contacting surfaces of a liquid and a solid. The cohesion and adhesion that result keep the outer chest cage of bone and muscle in intimate contact with the lungs, being pulled and pushed together in the harmonious dance of respiratory movement.
The adhesion and cohesion of the lung to the chest wall is a lifelong relationship of intimate contact, characterized by 10-15 in and out movements per minute at rest, and sometimes up to 20 ? 40 breaths per minute during exercise. The harmony and intimacy continue despite the rigorous jolts of life including violent sneezes, cough whoops, jumps to the basketball hoops and the likes of usual rough and tumble. It is a simple but marvelous mechanism that keeps two structures bound together by such a simple but powerful physical principle. When there is a large effusion or pneumothorax then the cohesive and adhesive mechanisms fail, and collapse of the lung ensues.
Ashley Davidoff, M.D.
42540b06
Fourth Layer ? Lung
The lung as a whole provides the next functional layer, but within the lung there is a combination of structures, each with different properties and needs. For the sake of understanding we will consider it a single layer. The relatively rigid upstream airways do not change much with the ins and outs of respiration, while the smaller airways and to greater extent the alveoli undergo significant change in size, expanding with inspiration and getting smaller with expiration.
The alveoli exhibit a surface tension which creates an environment for recoil during expiration and if held unchecked would undergo complete collapse. The tendency for recoil is necessary and healthy, while the collapse is of course harmful. The total collapse of the alveoli is prevented by the automatic rhythm of involuntary inspiration, which reverses the process, as well as the presence of surfactant (our fifth layer) that prevents the collapse. In the absence of surfactant the pressure required to keep the alveoli open is 20-30mmHg. Surfactant reduces this to about 3-5 mmHg.
Fifth Layer ? Surfactant
Surfactant, the fifth and last layer, is a lipoprotein solution secreted by specialized cells of the alveolus. It serves to reduce the surface tension and ease the force necessary to open the alveoli during inspiration. In blowing up a balloon, we find that the most difficult part is when the radius of the balloon is small. Thus the surface tension on the balloon is high when the radius is small. As the radius increases the surface tension decreases and it becomes easier to blow up the balloon. Surfactant if it were present in the balloon would decrease the wall tension by an order of 15, to ease the energy and pressure necessary to inflate it.

Courtesy of: Ashley Davidoff, M.D.
42530b05b09b01a12
Applied: First Layer ? Bone
We will now review the 5 layers and apply our knowledge of the physiology and anatomy to the diagnostic and therapeutic world.
Courtesy of: Ashley Davidoff, M.D.
42554
42554ab03
First Layer ? Bone: Fractured Ribs
The fracture of two to three ribs in one place does not result in respiratory difficulty. The pain that ensues can cause decreased respiratory excursion and consequent mild atelectasis. Pain limiting respiratory motion is a very common clinical and radiological scenario, often seen in patients who have had abdominal or chest surgery.
Flail chest, on the other hand, is fortunately not common, but is an urgent clinical problem following extensive blunt traumatic chest injury. Flail chest arises when three or more ribs are fractured both anteriorly and posteriorly, resulting in a loss of chest support. Paradoxical chest movement results so that during inspiration the fractured ribs follow the movement of the lung rather than the chest wall from which they have become detached. Thus during inspiration the isolated ribs and associated chest wall move inward instead of out, and during expiration they move out instead of inward. This injury is usually seen as a consequence of severe trauma, and associated lung parenchymal injury is common. Clinical consequences are a combination of the loss mechanical efficiency and loss of parenchymal function.
The following case represents a controlled situation of paradoxical motion of the chest. The patient was asked to take a deep breath in. Can you work out what the problem is?
The CT was taken at end expiration. During expiration the chest cage normally recoils moving inward. Because of the lack of support of the chest the affected segment is moving out ward. This is also paradoxical.
Courtesy of: Ashley Davidoff, M.D.
42575 42573
First Layer ? Bone: Scoliosis
The effects of scoliosis on respiratory function both before and after surgical correction have revealed that the degree of scoliosis did not correlate with the severity of respiratory difficulty, though there was improvement by about 10% of lung function following surgical correction.

The CT scan (right) shows the proximal thoracic spine running at right angles to its normal axis, indicating a severe scoliosis. The anatomy of the lung is severely distorted.
Courtesy of: Ashley Davidoff, M.D.
29470 29476
Second Layer ? Muscle
The ring of muscle is the next layer.
42554ab06

42557b01b

Ashley Davidoff MD
42557b01b01
Ashley DAvidoff MD 42557b04
Second Layer ? Muscle: Paralysis
It is not uncommon to see paralysis of one hemidiaphragm without untoward (has no functional consequence) effect. However, when both components of the diaphragm fail, therapeutic intervention is urgent. Diseases that affect the neural signal (polio, Guillain Barre, quadriplegic syndromes), transmission of the neural signal (myasthenia gravis), or disease of the muscle itself (tetanus, myopathy), can result in respiratory failure. In the acute situation when respiratory compromise is severe the patient will require a ventilator. The iron lung was developed to treat polio in 1927. It was the first respirator and was developed by a Harvard researcher Philip Drinker. He used an iron box and two vacuum cleaners to create a push and pull motion on the chest.
Third Layer ? Pleura
The next layer is the pleura, which acts as the intermediary between the chest wall and the lungs.
The pleural adhesion/cohesion mechanism is quite a robust system, but like all mechanical systems under duress it can fail. Pneumothorax is a well-known failure of this system and is caused by air leaking from the lung, which intervenes in the bonding mechanism and separates the two pleural components. Pleural effusions increase the distance between the lungs and the chest wall and when large can cause collapse or atelectasis of the lungs
Quiz Me
A pneumothorax is a collection of air in the pleural cavity.
True False
Third Layer ? Pleura: Pneumothorax
When a patient has a small pneumothorax we ask that the patient lie in bed with the affected lung on the down side (ipsilateral decubitus position) so that we limit the chest wall movement on that side and hence air movement into the lung. If the pneumothorax is large the patient can become symptomatic and a life-threatening event called tension pneumothorax can ensue. In tension pneumothorax, air leaks into the pleural space on inspiration and is trapped on expiration. The air subsequently accumulates until the pressure is sufficiently high in the pleural space to cause compression of the venous structures in the chest. The elevated venous pressure prevents venous return to the heart and cardiac output falls. Quick recognition of this entity and immediate decompression by a needle or a tube is life saving.

Courtesy of: Ashley Davidoff, M.D.
42525
Third Layer ? Pleura: Pleural Effusion
The following is also a problem with the pleural space ? Can you solve the problem?
42558

Courtesy of: Ashley Davidoff, M.D.
42558b03
Fourth and Fifth Layer
Restrictive Lung Disease
The next layer is the lung. Restrictive lung disease occurs when the interstitial tissue of the lung lose elasticity and is replaced by fibrotic tissue. The patient has greater difficulty in expanding the lung and the recoil mechanism is also affected.
Hyaline Membrane Disease
The next layer is the surfactant.
Premature babies do not produce surfactant and therefore their tendency to collapse the alveoli during inspiration is increased. Also, greater forces are necessary to inflate the alveoli. Extensive atelectasis or lung collapse results in this condition and the baby may require a respirator to help keep the lungs open. This disease is called hyaline membrane disease, or respiratory distress syndrome.
ARDS
A parallel disease in older patients is called ARDS, or adult respiratory distress syndrome. It is characterized by diffuse alveolar damage (DAD), resulting in a relative lack of surfactant and consequent microatelectasis. There are many causes of DAD including sepsis, multisystem trauma, smoke inhalation, near drowning, and narcotic overdose. The absence of production of surfactant, in combination with the fluid accumulation in the alveoli, causes an increase in surface tension and more patient muscular effort is required to expand the alveoli. When this effort fails there is atelectasis and reduced oxygen delivery and carbon dioxide excretion. The failing respiratory system requires a respirator to help keep the alveoli patent.
Breathing Instructions ? The CXR
In general we intuitively know that when we take a deep breath we are using our muscles to actively inspire. When we breathe out it is a relaxation of that mechanism caused by actual muscle relaxation and the elastic recoil of the layers of the chest. We can of course breath out all the way until we have expired right to what we think is the last drop of air, and this takes effort and muscle contraction as well. When you as a technologist have a patient for a routine CXR you ask your patient to ?take a deep breath in, blow it all the way out and hold it?.? And you click your exposure. You can readily see that there is still quite a lot of air left in the lung. This is called the dead space of the lung, found in patients who are well and alive! Read on and learn all about what happens to the lung volumes and capacities during that process.
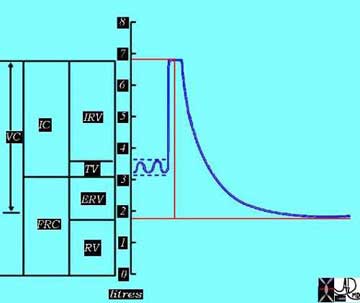
Lung Function Tests ? Lung Volumes
In order to explain the process we will pretend that you are a lung function technologist for a moment. You are going to test your patient?s lung volumes, capacities, and velocities. We want you to think and apply what you see on these graphs to your own situation when you are doing a CXR, and to imagine the differences between an inspiration CXR and expiration CXR. We particularly want you to see the difference in volume of air between the inspiration film and the expiration film.
So we go back to our theoretical patient undergoing lung function tests and we place a mouthpiece over her mouth and attach the tubing on the other end to a recording device called a spirometer. As our patient lies on the table breathing quietly under resting conditions we notice a simple rhythmic pattern on the spirogram. This pattern is entirely involuntary caused by the production of a signal from the center of respiration located in the brain that causes the diaphragm and other muscles to contract and to expand the chest, and then as it switches off, the muscular relaxation and elastic recoil cause the chest to contract.
Courtesy of: Ashley Davidoff, M.D.
42529b06b01b
Lung Function Tests ? Lung Volumes: Breath-hold Deep Inspiration
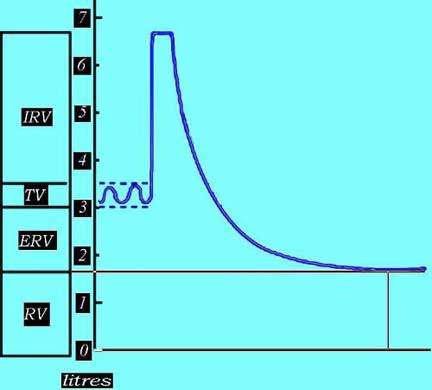
We reset our spirometer to get our basal conditions set between the 3 and 4 liter mark so that we have room on the graph to see what happens with forced inspiratory effort and forced expiratory effort.
For those of you who require your patient to ?breath hold? for MRI and CT, we are in fact asking them to stop this involuntary breathing pattern in order to prevent chest wall and lung movement that would otherwise cause motion artifact on our images.
For our CXR we now ask our patient to take as deep a breath in as possible and we see a dramatic change on the graph.

Courtesy of: Ashley Davidoff, M.D.
42529b06b02
When you ask your patient to take a deep breath in for a CXR, the chest volume will increase by more than 3 liters. The patient will muster all their diaphragmatic forces to contract the intercostal muscles to enlarge the chest cavity and pull in air. The lung in the healthy patient will now contain about 6.7 liters of air. When our patients can take a deep breath and hold it in, the radiologists are better able to identify disease processes since the interface of air and the soft tissue of the disease are larger and therefore the disease is more easily seen.
For those of you who are ultrasound technologists you use the consequences ?deep breath in? to bring the diaphragm and upper abdominal organs down, beyond the rib cage, in order to optimize your window to the upper abdomen.
Lung Function Tests ? Lung Volumes: Expiration
Now as the patient reaches peak inspiration we tell her to breath out as completely and rapidly as possible, and our spirometer reading does the following:

Courtesy of: Ashley Davidoff, M.D.
42529b06aa02
The difference between the end of basal expiration and complete expiration is called the expiratory reserve volume (ERV).
For the lung function technologist the speed with which the expiration is performed is a key issue in lung function, but for you the degree to which the patient can empty their lungs is key for a good expiration film.
Lung Function Tests ? Lung Volumes: Residual Volume
At the end of this complete expiration, there is still a volume of air left in the lungs and airways, and this is called the residual volume (RV), which is the air filled space that keeps everything open after a full expiration. When we perform a CXR in expiration, we ask our patients to breathe in and then all the way out, and to hold it out, and we then expose our film. The air you see in the lungs at the end of expiration is called the residual volume. The lungs are at their smallest volume in end expiration and at this point contain about 1.5-1.7 liters in our patient. In the normal adult the RV ranges between 1.0 and 2.4 liters.
Courtesy of: Ashley Davidoff, M.D.
42529b06aa03
Lung Capacities
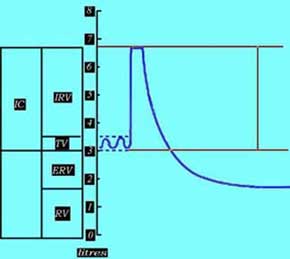
We now move on to our patient?s lung capacities, which represent a combination of the volumes we have spoken about. What do you think inspiratory capacity is? It is of course the combination of the basal inspiration, which is our tidal volume of 500mls combined with the inspiratory reserve volume (3.2liters) giving us a total of a 3.7 liters capacity for inspiration.
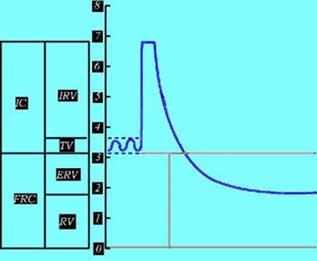
The amount of air left in the lungs after a resting expiration includes the expiratory reserve volume and the residual volume is called the functional reserve capacity (FRC).
Courtesy of: Ashley Davidoff, M.D.
42529b06aa04
Courtesy of: Ashley Davidoff, M.D.
42529b06aa05d
Lung Capacities: Vital Capacity
The vital capacity (VC) is defined, as is the maximum volume of air expelled after a maximum inspiration. For you, this is the difference in amount of air in the lungs between a CXR with maximum inspiration and a CXR with maximum expiration. In this patient it is about 5 liters ? a large difference in volume and a large difference in the appearance of the chest, sometimes making the difference as to whether a pneumothorax is seen or not seen. Why is this so important? A small pneumothorax itself may not have any functional significance meaning the patient has no untoward effect. It does however reflect a leak, and a leak can get better or worse. In the situation in which it gets bigger it can cause a life-threatening situation and so it is essential to make the diagnosis of even a small pneumothorax. Using expiration technique for the clinical question of pneumothorax is essential.
Courtesy of: Ashley Davidoff, M.D.
42529b06aa06bd
Lung Capacities: Total Lung Capacity
The total lung capacity is a combination of the vital capacity and the residual volume. Thus it is a combination of the maximum volume of air that the patient can move in and out of his lungs and the air that remains in the lungs after a forced expiration.

Ashley Davidoff, M.D.
42529b06aa

Courtesy of: Ashley Davidoff, M.D.
42529b06aa07
The names and details of the volumes and capacities are not meant to confound you with impractical minutiae, which are not important to you in your day-to-day work. It is more meant to give you a sense of the volume changes that occur during quiet and forced breathing and the impact that these movements have on your work, whether it is taking a CXR where you want to optimize inspiration or expiration, during an MRI or CT examination where you want to minimize respiratory artifact, or during an ultrasound examination where you want to optimize your window to the upper abdomen.
Gas Exchange: Basic Principles
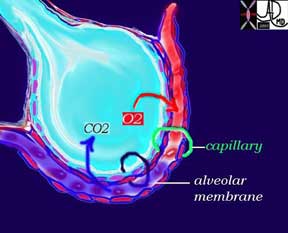
While the function of air transport is the domain of the tracheobronchial tree, it is the function of the alveoli to act as a membrane for gas exchange to and from the atmosphere and the blood. The principles of gas exchange across a membrane are also universal in the body. The movement of both oxygen and carbon dioxide is by diffusion. Diffusion is the movement of the gases, fluids, or chemicals from a higher level of concentration to a lower level. The partial pressure of the two gases is a measure of their concentrations. The greater the difference in partial pressure the greater the rate of diffusion. Oxygen is carried mostly by a macromolecule of protein called hemoglobin while carbon dioxide is mostly carried in the form of bicarbonate in the serum.
The membrane across which the gases have to move is between 0.3 ? 1.0 micron thick and consists of two cell layers. One layer is the epithelium of the alveolus and the second layer is the epithelium (called endothelium) of the capillary.
Courtesy of: Ashley Davidoff, M.D.
42445b03b12
Fick?s law governs the movement of air across a membrane. The net movement or diffusion rate of a gas across a fluid membrane is proportional to the difference in partial pressure, proportional to the area of the membrane, and inversely proportional to the thickness of the membrane. The total membrane surface area of the alveoli is about 80-100 square meters and the thickness is less than a millionth of a meter, so it is a very effective gas exchange interface.
At rest about 6-10 liters of air is moved through the tracheobronchial tree per minute. In this same minute about 600ccs of oxygen moves from the alveoli into the blood, while 600 ccs of carbon dioxide moves across the membrane into the alveoli. During exercise up to 100 liters of air can be moved through the airways per minute and about 3 liters of oxygen and 3 liters of carbon dioxide is moved across the membrane.
Gas Exchange: Applied Physiology
The alveolar membrane can get affected by disease processes that may accumulate fluid or pus within the alveoli causing a thickened membrane. Interstitial fibrosis is a second cause of thickening of the respiratory membrane that will affect the efficiency and speed of gas exchange.
Courtesy of:Ashley Davidoff, M.D.
42073b01
Components of the Lung
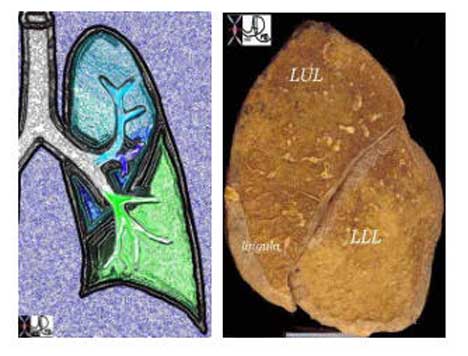
The right and left lungs are asymmetric with the right having three lobes and the left two lobes. The lingula is part of the left upper lobe (LUL).

Courtesy of: Ashley Davidoff, M.D.
32558b02
Courtesy of: Ashley Davidoff, M.D.
32557b01
Right Lung Parts: Basic Anatomy
The right lung has three lobes: upper, middle, and lower. The lobes are subdivided into segments that are determined by the branching of the main bronchi. The right lung usually has the segments subtended by ten segmental bronchi. The right upper lobe (RUL) has three segments called the apical, posterior, and anterior segments. The right middle lobe (RML) has two segments named the lateral and the medial segments. The right lower lobe (RLL) has five segments also named according to position: superior, anterior basal, lateral basal, posterior basal, and medial basal segments. The superior segmental bronchus is the first branch of the RLL system and it is directed posteriorly. The superior segment is vulnerable in the supine patient who aspirates because of its posterior position.

Courtesy of: Ashley Davidoff, M.D.
32686b03
Right Lung Anatomy Continued
The superior segment occupies the entire upper portion of the lower lobe. It sits atop the remaining four segments of the right lung: the anterior basal, lateral basal, posterior basal, and medial basal segments. These basal segments form the base of the almost pyramidal-shaped lower lobe, as well as the base of the lung. The basal segments and base of the lung rest upon the diaphragm.

Courtesy of: Ashley Davidoff, M.D.
32159B03b
Right Lung Parts: Applied Anatomy
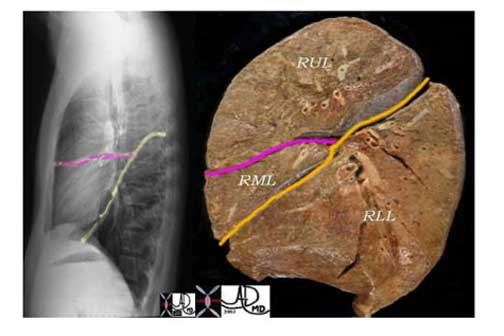
It is essential to know and understand the distribution of the lobes for accurate assessment of the CXR. For example, a disease process in the upper lung field on the right does not necessarily mean that the disease is in the RUL. Since the RLL is so large and extends almost the entire thoracic distance (see image 3a), it is difficult to localize on the P-A exam of the chest. However, if one reviews the lateral exam, the distinction between right upper and right lower lobe is much easier, since the lower lobe is mostly posterior and below the fissure, and the upper lobe mostly anterior and above the fissure.
The major fissure is the dividing line between the RLL on the one hand and the RUL and RML on the other. The minor fissure, also known as the transverse fissure, divides the RUL from the RML and is easily perceived on the lateral examination.

Courtesy of: Ashley Davidoff, M.D.
Courtesy of: Ashley Davidoff, M.D.
Right Lung Applied Continued
Sometimes there is an extra lobe in the right upper lung field called the azygous lobe and the azygous vein runs in the accessory fissure. The azygous lobe is an accessory lobe in the apex of the right lung that is found in approximately 0.5% of routine chest x-rays. It is recognized by a fissure in the apex that has an inverted comma shape.
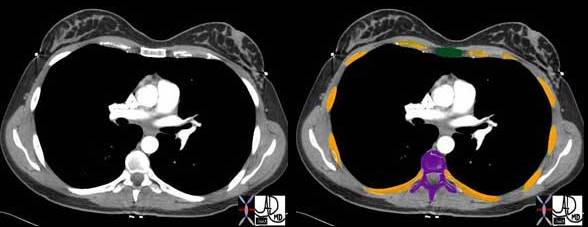
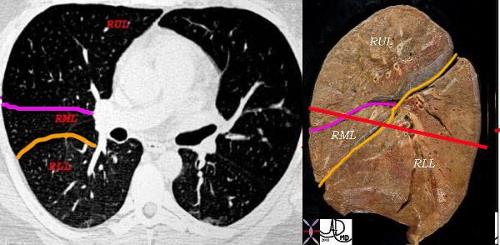
The following diagram demonstrates the cross sectional appearance of the right lung at the level where both the major and minor fissures are seen. It correlates the CT scan with the anatomical specimen.
Courtesy of: Ashley Davidoff, M.D
32160c2lb_6
Courtesy of: Ashley Davidoff, M.D.
Left Lung Parts: Basic Anatomy
The left and right lungs are very different. We have already noted that the mainstem bronchi are different, with the left mainstem bronchus being long and thin, while the right mainstem bronchus is short and fat. The left lung has only two lobes. There is a left upper lobe (LUL) and a left lower lobe (LLL). The left lung does not have a middle lobe. Instead, the middle lobe equivalent is the lingula, which is in fact part of the LUL and not a separate lobe.
The two lobes of the left lung are separated by the major or oblique fissure, which is the only fissure on the left side. The left lung is smaller than the right and has eight segments compared to the ten segments on the right.
The upper lobe of the left lung has superior and lingula divisions. Both of these divisions have two segments each. The segments of the superior division are the apical-posterior and the anterior segments. The lingula is divided into superior and inferior segments. As noted there is no fissure between the upper segments of the LUL and the lingula ? they are both part of the LUL.
The division of the lower lobe closely resembles that of the right except that there is consolidation of two of the left lower lobe segments. Thus, while the RLL has five segments, the LLL has only four. Again, as is characteristic, the left lung consolidates its component parts.
The superior segment of the LLL forms the top of the pyramid of the LLL. Inferiorly and at the base of this pyramid, the anterior and medial segments combine to form the anteromedial basal segment, followed by the lateral basal, and posterior basal segments.
Courtesy of: Ashley Davidoff, M.D.
Quiz Me
The left lower lung has _________ segments.
(Note: You will be given 2 tries to answer this question, then the answer will be provided.)
two
three
four
five
Left Lung Parts: Applied Anatomy
The overall volume of the left lung is smaller than the right, but the distribution of volume between LUL and LLL is more equalized and balanced. Again, in the P-A projection the two lobes overlap each other. A nodule in the upper lung field or lower lung field as seen on the P-A projection can be located either in the upper or lower lobe. The lateral examination is essential to accurately locate the disease. The LUL is anterior and above the fissure (see Fig 1b), while the LLL is posterior and below the fissure (see Fig 2b).

Courtesy of:Ashley Davidoff, M.D.
Quiz Me
A nodule in the lower lung field is always located in the lower lobe of the lung.
True False
When we read plain films of the chest we use the position and relations of the lungs to the heart and the fissures to locate disease processes, including infiltrates, nodules, and regions of atelectasis. We use two principles to locate disease. The first is the described relations of structures to each other, and the second is the concept of ?silhouetting.? The important facts that pertain are that the RML abuts the right heart border, the lingula the left heart border, and the lower lobes on both sides abut the diaphragm. The principle of ?silhouetting? is commonly used to define the nature and location of a soft tissue process in the lung. We have described the fact that we are able to see and distinguish two different structures because their densities are different. Thus we are able to see the heart border or the diaphragm, for example, because they abut air- filled lung tissue that has a completely different density to their soft tissue nature. If, however, the air-filled lung is replaced by pus or exudates (pneumonia) or become airless (atelectasis), then the abutting structures both have soft tissue density and cannot be distinguished from one another. If there is a process that silhouettes the right heart border in the P-A projection then we know that this process is in the RML. Similarly, if the left heart border cannot be distinguished from the disease process, we know that it is in the lingula.
It is important to identify accurately the location of disease, particularly nodules and masses that may have to be surgically removed, since the surgeon has to know which part of the lung has to be removed.

Courtesy of: Ashley Davidoff, M.D.

Courtesy of: Ashley Davidoff, M.D.
Smaller Parts ? The Acinus
The bronchi proceed from the mainstem bronchus via 16 to 23 divisions into the terminal bronchioles. Thereafter sac-like protrusions develop in the system, which allow gas exchange to start taking place. The first branch that is able to perform this gas exchange is called the respiratory bronchiole. After three divisions the respiratory bronchioles become alveolar ducts and after further division become alveolar sacs. Finally, at the terminal end of this pathway, are the alveoli. The system that starts at the respiratory bronchiole and terminates at the alveoli is called an acinus, and it is functionally characterized by having the ability to both conduct air as well as enable gas exchange. The acinus averages about 6-7mm in diameter. When it is filled with fluid, it can be visualized on a CXR as a 6-7mm density called an ?acinar shadow.? As a structural entity it has little diagnostic utility. We will expand on the pulmonary lobule in the next section, which has greater implications for the imaging of the lung. Functionally however, the acinus can be considered as the unit of gas exchange in the lung.
Courtesy of: Ashley Davidoff, M.D.
42446b12

Courtesy of: Ashley Davidoff, M.D.
42650
The Secondary Lobule (a.k.a pulmonary lobule)
We will now move upstream toward the terminal bronchiole to gain an understanding of the secondary lobule. From a radiological point of view, it is structurally a more important unit than the acinus. It is a conglomerate of 3 to 5 acini enclosed in a membrane with a polyhedral (having many surfaces) shape. From a structural and radiological point of view it is important to understand this entity, since it has implications in the understanding of the CXR, conventional CT, high-resolution CT and in the structural changes that occur in some of the lung diseases.
We have already described the ?buddy system? that exists in the lung, with the branches of arterioles and bronchi traveling together, and the venules and lymphatics going together. Lymphatics sometimes also accompany the bronchovascular bundle.
The Secondary Lobule (a.k.a. pulmonary lobule): Grapes of Exchange ? A Romantic Story

Story and illustrations by: Ashley Davidoff, M.D.
42440b05
From the minute I saw him I loved him and I knew that no matter what evolved, we would spend our lives together? little did I know what the working relationship would be.
Here follows a true story about me, the bronchiole, and my lifelong buddy the pulmonary arteriole.
He and I were on a mission. I had my origins in the atmosphere and he from the heart. We came from very different backgrounds and had come a long way on this trip on the highways and byways of the airways and circulation. My mission was to take products from the air in the atmosphere and deliver them to the grapes of exchange and his was to deliver blue blood to the same grapes. In this communication we will speak mostly of the journey to the grapes in the house of the pulmonary lobule. The grapes of exchange in my imagination had something to do with bonding and marriage ? perhaps the exchange of vows. The story turns out quite differently. We had great travels together and took a lot of pictures!!
I think by this time you know what we had already been through. He had started out as a large elastic vessel off the right heart called the main pulmonary artery (nickname ?MPA?) and I had started out as the trachea. (nickname ?trach?). We met at the doorway of the lung called the hilum, and took a fancy to each other right away and so we decided to travel together. We had traveled a long way by the time our story begins both experiencing many divisions and were right in the middle of an inspiration. We both looked quite different at this point having given birth to many offspring. In the new language ? we had both ?morphed? quite a bit but this was a necessary part of the mission. Of course we were much smaller than we had been. He had lost some of his elasticity and developed a bit of muscle. I had lost my entire cartilaginous skeleton and had developed some muscle as well. We were told that from now on we were both going to lose muscle and I in particular was going to change drastically. I could not wait! I secretly hoped that this change would make me more attractive and bring me closer to a happy union since I was promised a happy union in the end. My name at this stage was ?terminal bronchiole?. A foreboding and deathly chill rattled down my muscularis as I said the word ?terminal? knowing that I was going to lose the small amount of muscle that I had.
We reached the doorway surrounding the secondary lobule and faced the polyhedral entrance. It was quite beautiful I thought in my teal blue outfit.
Ashley Davidoff MD
42448b03
We took a quick walk around the polyhedral structure.

Ashley Davidoff MD
42449b02
We returned to the entrance and took a closer look at the goings on inside through the large front entrance windows of the pulmonary lobule. Below is a picture of what we saw.

Ashley DAvidoff MD
42440b08
As we were ushered into the lobule, we were faced by a refreshing atmosphere of comforting air and a hub of activity. In addition to the swishing sounds of air movement we heard a hubbub of clinking and clanking. We were told that the sounds were coming from the grapes of exchange (wedding bells?). We also noticed that there were at least three other couples that looked like the people of our tribe ? three other bronchovascular bundles. We called our tribe the ?bronchovascular bundle? with the one part of the bundle being the progeny of the bronchus and the other, the progeny of the pulmonary artery.A group picture inside the lobule is shown below. Fortunately the flash was working because it was a little dark inside.
Ashley Davidoff MD
42447b03b01
We noted there were other pairs of people they called the pulmonary venules (red) and lymphatics (yellow). A joyous union with these pairs was also promised. I could not imagine how. They looked so different to each other ? the lymphatic, tiny and dressed in a bright yellow suit and the vein in passionate red. They seemed so foreign, almost from another space, time zone and culture. At this vantage point we got a vague sense of what was to come, but in our wildest dreams we could not have imagined how our bodies were going to change and what was to happen as we moved inward into the chambers of gas exchange.
I did not realize that my body had already started to morph at the time of the picture ? little sac-like love handles spreading all along my formerly sleek and beautiful body. Yech! I did not look good at all. My buddy the arteriole on the other hand as well as members of the other tribe maintained their sleek tubular looks. ?Why me?? I shouted. ?All for the good of the nation and good gas exchange!!? they shouted above the swishing of air and clanging of the factories. ?Easy for you to say,? I replied. ?Some of us have to suffer some bad morphs for the good of the whole? they said, ?but those love handles kind of suit you,? they exclaimed with a wry smile. I was so sad.
Well the divisions started coming rapidly and so we all became smaller very quickly. I was getting rounder and rounder while they were getting thinner and sleeker. Things seemed to be rushing at an accelerated pace and I must say that there was some excitement in the air as we all got closer and closer to each other. In the big picture we seemed to be coming together as a team, and the whole landscape seemed more colorful and more promising. We reached out to the other tribe and they too us.

42447b05b02
I remained on the plump side as my love handles grew more pronounced and rounder while the clanging noises grew louder and louder. I was dividing into alveolar ducts and alveolar sacs and finally into alveolus which of course is a complete transformation from my former tube like shape to the spherical shape of the grape. In the mean time my buddy the artery grew as small as an 8-micron red cell and remained true to his tubular form. He started to surround me completely but was more in concert with that beastly red vein as he ran headstrong in blind passion to join her in capillary union. For a moment they each lost their identity becoming the tiniest of tubes neither arteriole nor venule. I on the other hand became at one with the fruit of the vine and in stuporous state I think I became the grape itself. Through my waist I felt the pleasant freshness of gusts of air going back and forth through my skin. My delivery of fresh air moved very quickly into the capillary. Little did I know that it was the oxygen that I carried which gave my competition the beautiful red glow of health. The odious carbon dioxide moved the other way. This toxic waste came directly from the man I had known and trusted for so long. Thanks for nothing.
I do not like to show the next picture much since for me it is a sad one. There I am a ditched lover, fat as a grape, in the middle of the capillary union between my blue ?ex? and his new partner in crime, the red beast. Yes of course it was for the better ? they all say that ? but what about me?
As you have learned already, the blood circulation needs two types of vessels: one to carry the blood to the lungs and a second to carry it from the lungs. I on the other hand do it all by myself. On inspiration I take air to the lungs and on expiration I take it away through the same vessel to the atmosphere. This is the lot of all women. We do double the amount of work schlepping here and there and everywhere and get no respect for it.
So at this junction we are in the middle of an inspiration (for me ? what kind of inspiration could I feel in my morphed format) and we were just about to start the expiration. While I was traveling to the exit of the lobule during this phase of my life, my ?ex? was going in the same direction ? now transformed into a beautiful vessel with that healthy glow. Despite my odious load and my downtrodden feeling I moved with a sense of optimism.
What do you know? As I left the chamber of the lobule I shed my love handles one by one and my saccular form started to take on the sleek and tubular look again. I looked and felt brand new. ?Hmm? I thought ? perhaps he will fall in love with me again. I was hoping for another inspiration, just to show him once again how beautiful I was both on the outside and the inside. And that my friends was my nightmare in the Grapes of Exchange.
The Secondary Lobule: Applied Anatomy
The secondary lobule contains all the structural elements of the lung compacted into a small space and it is a recognizable structural entity that measures about 1 ? 2.5cms. There are 3-5 bronchovascular bundles per secondary lobule. Prior to entering the secondary lobule the bronchovascular bundles branch at approximately 1cm intervals. However, once they enter the confines of the lobule the branching becomes fast furious and a new branch originates every 1 ? 3mms. A lot of structure subsequently is packed into a small space. The lobules are well formed in the apices and the peripheral aspects of the lungs and poorly formed posteriorly.
Courtesy of: Ashley Davidoff, M.D. and Armando Fraire, M.D.
32699b
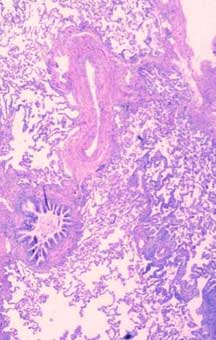
The Secondary Lobule: Applied: Disease of the Secondary Lobule
The interlobular septa and the secondary lobules are not normally visualized. However, any disease of the lung, particularly if the lymphatics are involved, will expose the lobules mostly by providing better visualization of the interlobular septa. If more than three contiguous secondary lobules are visualized then the lung is abnormal.

Courtesy of: Ashley Davidoff, M.D.
32291
Quiz Me
If more than _____ contiguous secondary lobules are visualized then the lung is abnormal.
One
Two
Three
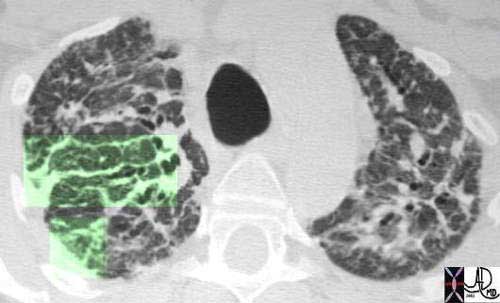
The Secondary Lobule: Applied: CT Example
At the level of the terminal bronchiole the arteriole and bronchiole measure about 0.2 mms each and it is the challenge of our CT technology to resolve these structures. At this level we are starting to push the limits of resolution. Thin collimation allows us to optimally visualize the lobule. We are thus better able to visualize the septa and the lobules with 1.5mm collimation than with 3mm collimation and our chances diminish, as collimation gets thicker. The evolution of high resolution CT scan has allowed us insight into the lobule and provides a better understanding of the diseases that affect the lobule.

Courtesy of: Ashley Davidoff, M.D.
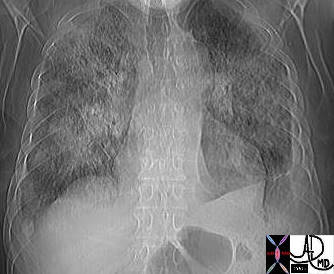
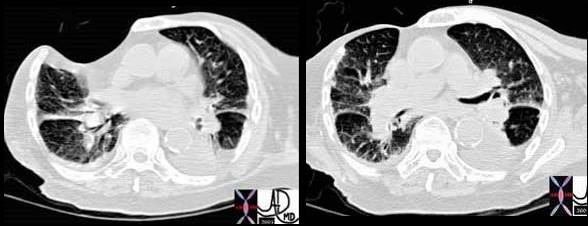
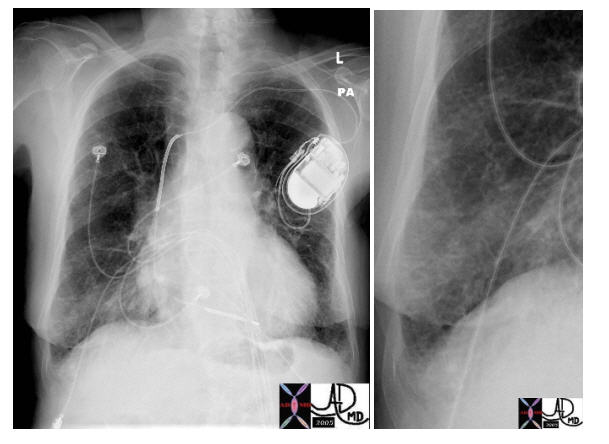
The Secondary Lobule: Applied: Congestive Heart Failure
We are never able to visualize the normal lobule on a plain film, but in diseases such as congestive cardiac failure when the lymphatics become overwhelmed they distend and become visible. In congestive cardiac failure the heart fails as a pump. In left ventricular failure the resulting congestion is reflected in the left ventricle (LV), left atrium (LA), pulmonary veins, and capillaries as increased pressure. It is reflected structurally as dilatation of the chambers and vessels. The increased fluid and pressure not only cause dilatation but also cause the fluid to leak out into the interstitium. The lymphatics are able to remove and mop up some of the excess fluid, but there is a point when the volume overwhelms the lymphatics and the excess fluid remains in the interstitium. On a CXR the findings include dilatation and cephalization of the arterioles, peribronchial cuffing, Kerley B lines (thickening of the interlobular septa), pleural effusion, and subpleural edema.
Kerley B lines are interesting manifestations of the thickened interlobular septa. After the discussion on the polygonal shape of the secondary lobule one might think that on the CXR we would identify a polygonal shape. However, the interlobular septa take on a linear shape, at the periphery and base of the lungs. It just so happens that the septa between the lobules run at right angles to the pleural surface at the costophrenic angles and so Kerley B lines are defined as linear, non-tapering, horizontal lines measuring 1-2cms., positioned at right angles to, and in contact with the pleural surface. Kerley B lines are best seen on a CXR.
Courtesy of: Ashley Davidoff, M.D.
The Secondary Lobule: Applied: Carcinoma Sarcoidosis
Courtesy of: Priscilla Slanetz, M.D. and Ashley Davidoff, M.D.
31867b03

Courtesy of: Ashley Davidoff, M.D.
32199cw
Conclusion
In this first part of the series on the lung we have emphasized the structure of the lung, and outlined how structure is integrated with function, disease, and imaging. We have focused on the principles describing a tubular system involved with transport, and a membranous system involved with gas exchange. The manner in which the lungs in concert with the muscles, bones, and membranes of the chest accomplish movement of air is remarkable. The principles of physics is an important aspect of understanding flow and exchange, but as you will see again and again, biological systems have changing needs under changing physiological conditions, and therefore we cannot treat the system as a simple tube or a simple filtering mechanism. The physics can only guide our understanding of a biological system. Diseases of the lungs are common and varied, and the chest x-ray is still the most common radiological examination that is performed. Imaging of the chest and lungs has been significantly advanced by the advent of multidetector CT and tailored examinations are required depending on the part of the lung that is deemed suspect. Thus a CT for pulmonary embolism will have little need for high-resolution technique for interstitial lung structure, and similarly a study for the evaluation for interstitial disease in sarcoidosis has little need for conventional CT technique. The technique applied is going to be guided by the clinical question.