- 35yo gentleman
- profoundly immunocompromised
- HIV,
- history of AIDS
- hepatitis C,
- opiate use disorder
- active IVDU
- cirrhosis
- presents with
- cough, rhinorrhea, and shortness of breath, hypoxemic
- varicella meningitis
- acute renal failure
- covid PNA superimposed w/ klebsiella oxytoca cavitary infection
- in respiratory failure
- septic shock
- s/p intubation,
- Profound immunosuppression
- CD4 <50
- strep pneumo bacteremia and PNA.
- influenza A,
- bacteremia
- pneumococcal disease
- Other considerations
- PJP,(Pneumocystis Jirovecii ) fungal pneumonia including endemic mycosis, nocardia, TB. ,,
- multiple infections pneumo pneumonia and bacteremia at this time.
- PJP,(Pneumocystis Jirovecii ) fungal pneumonia including endemic mycosis, nocardia, TB. ,,
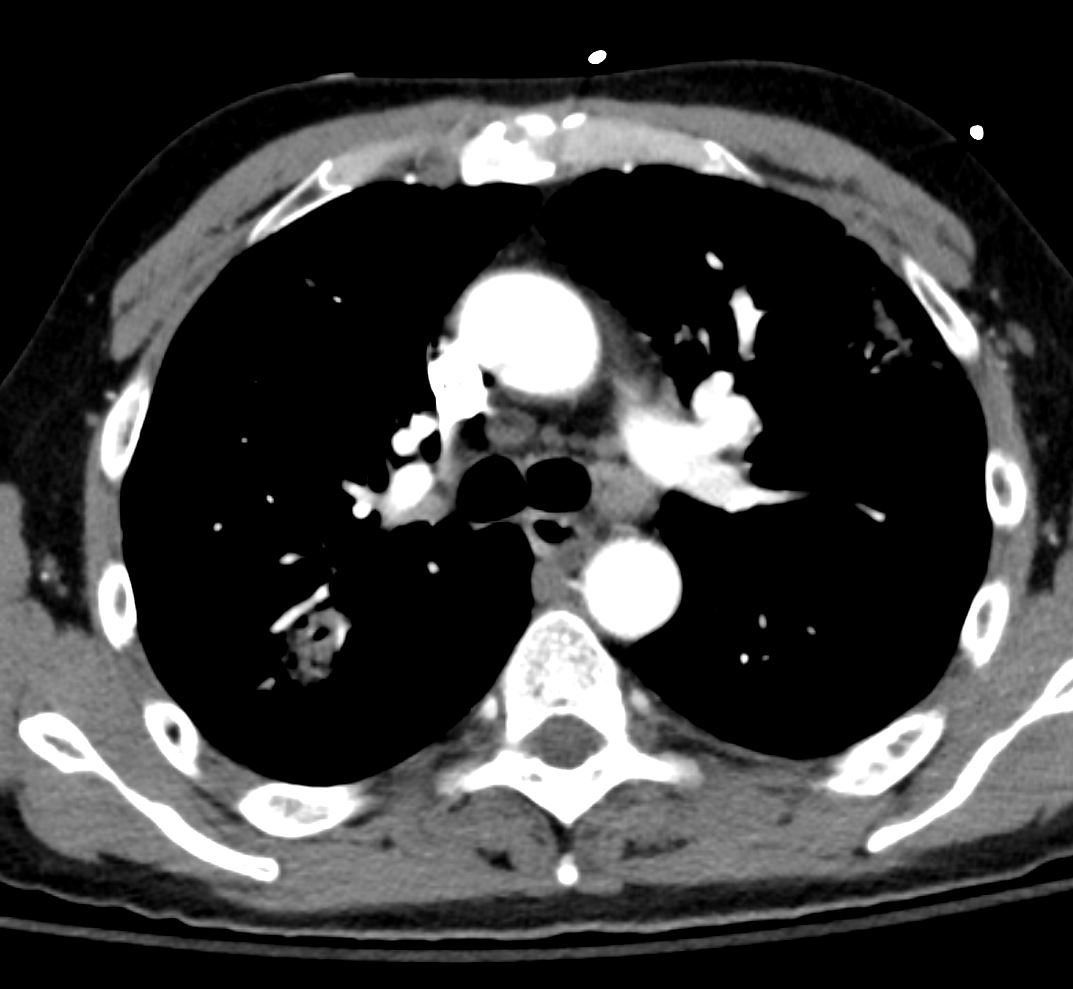
- 8months ago CavitatingInfections
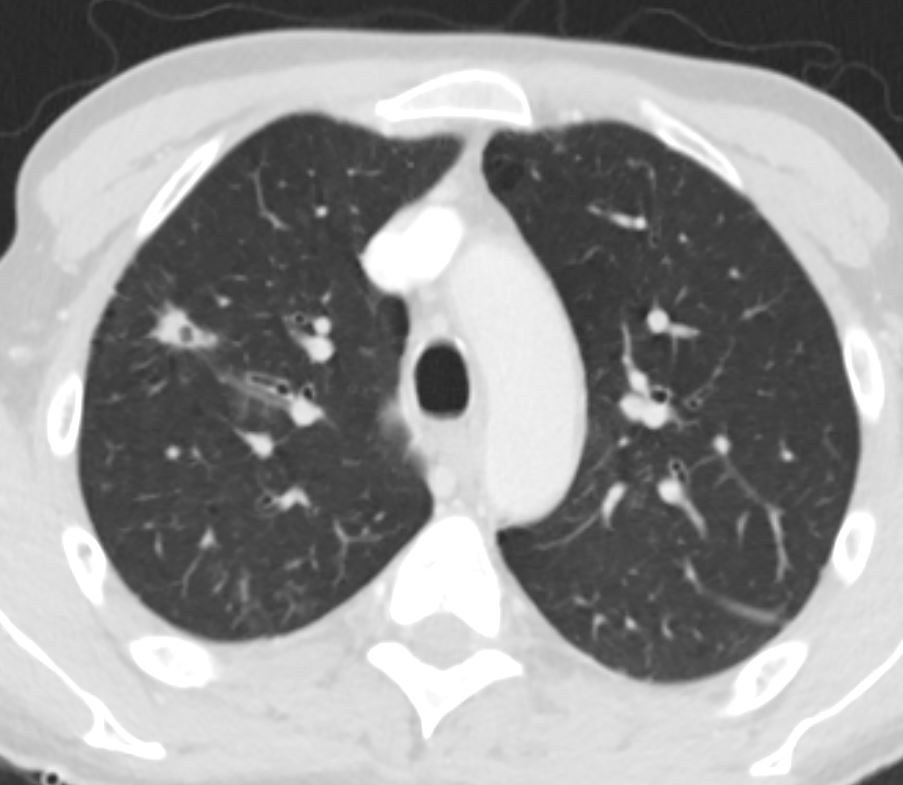
Lungs-HIV-AIDS-possible-PCP-39M-002c-CT-8-mths-ago.jpg
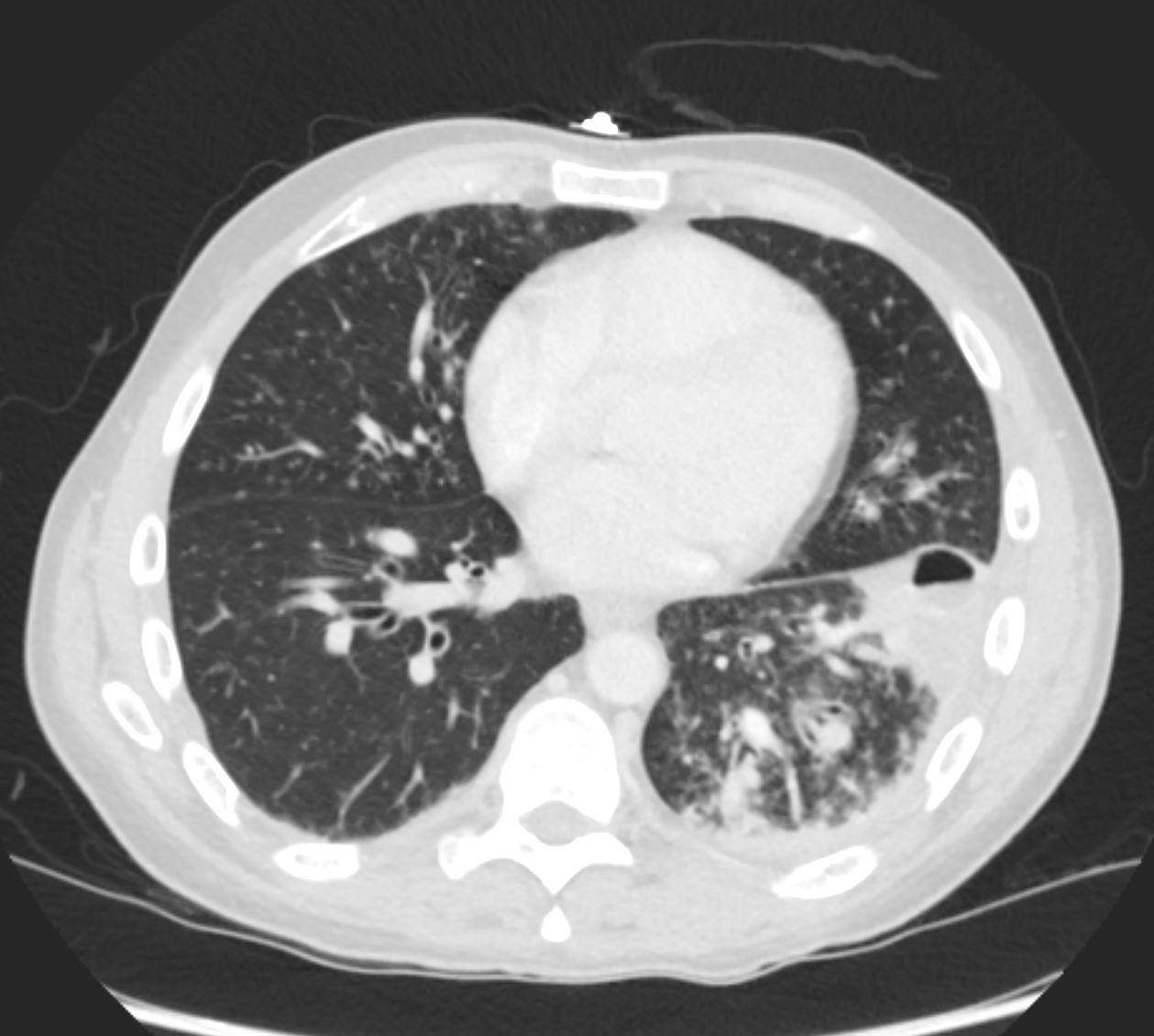

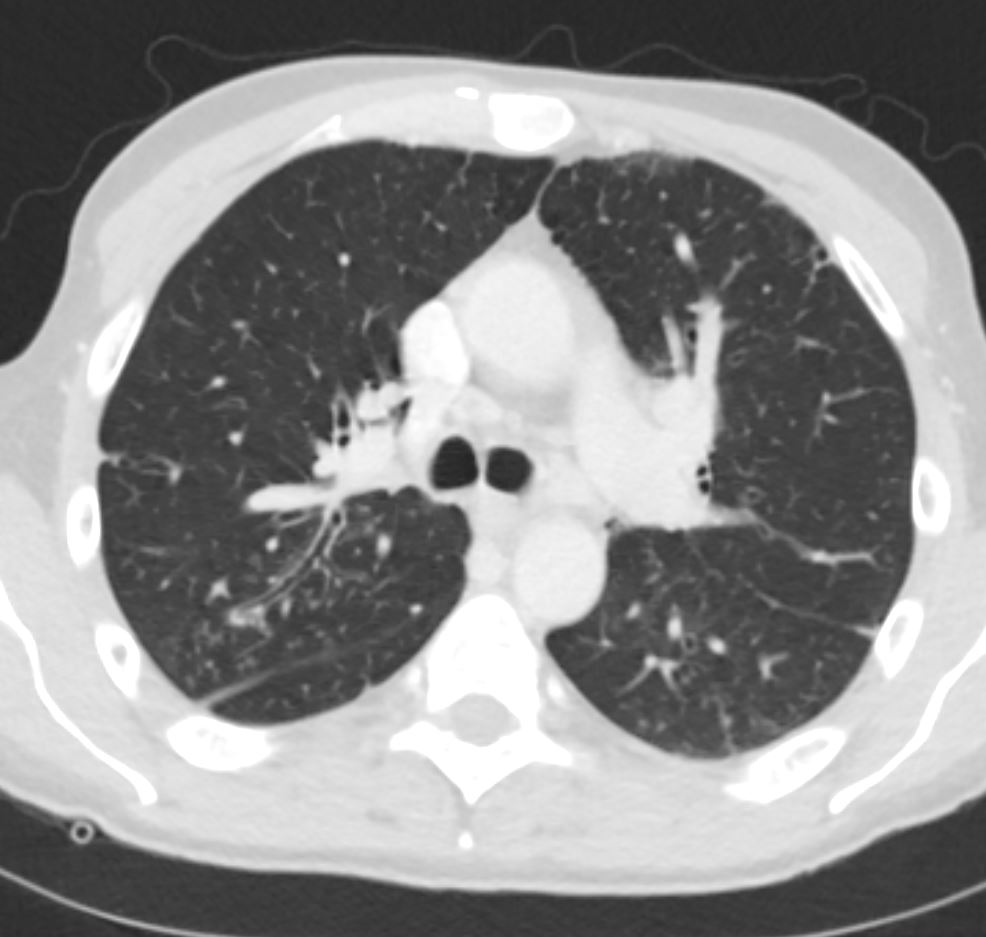
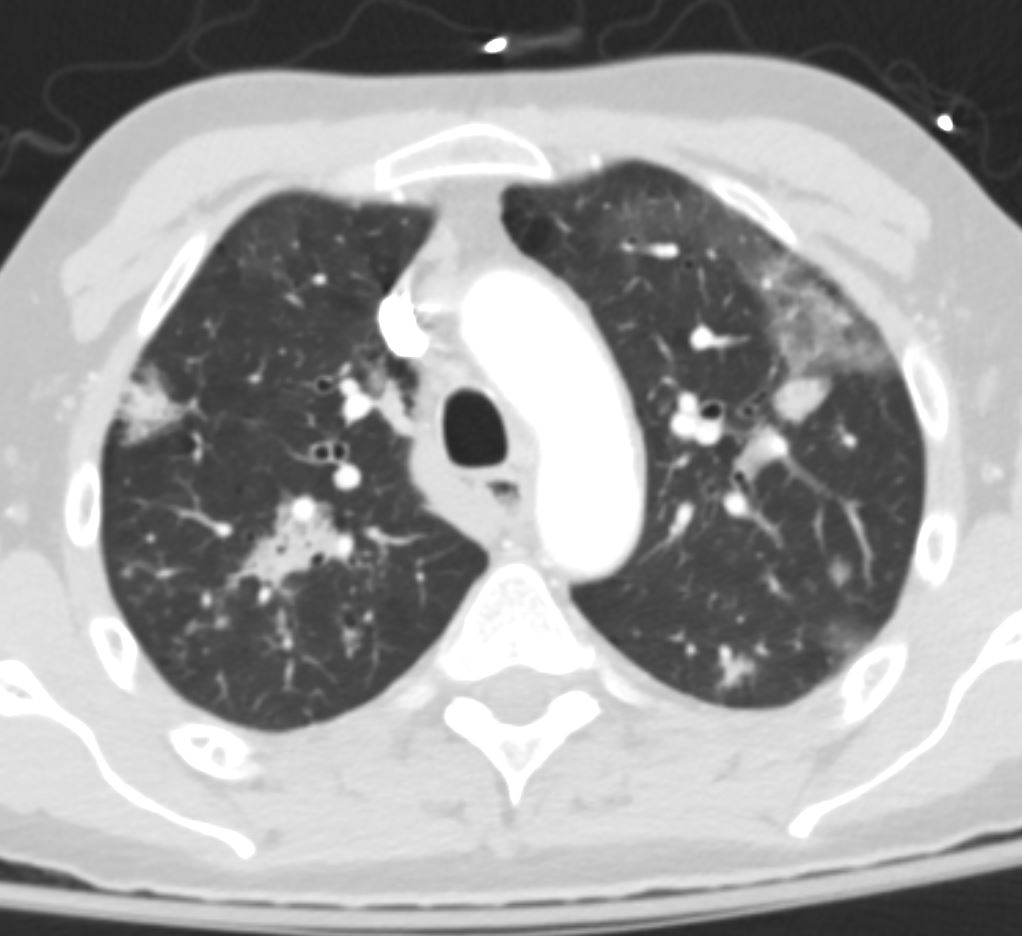
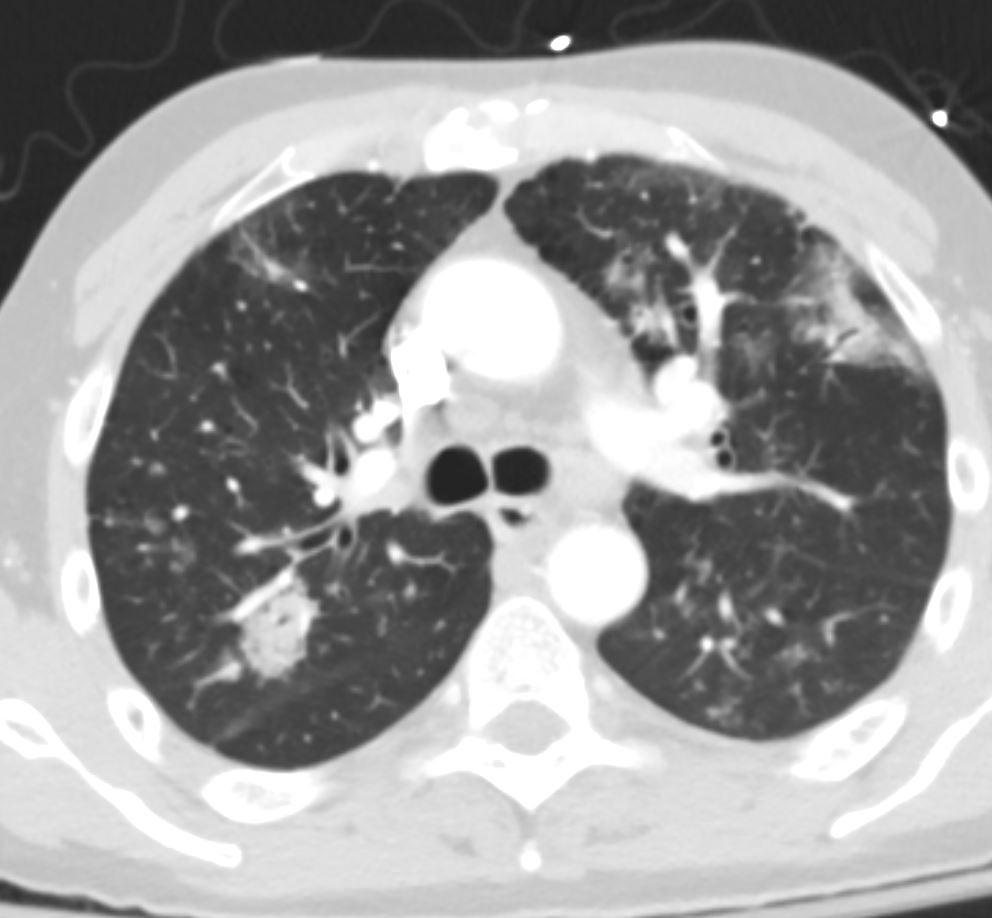
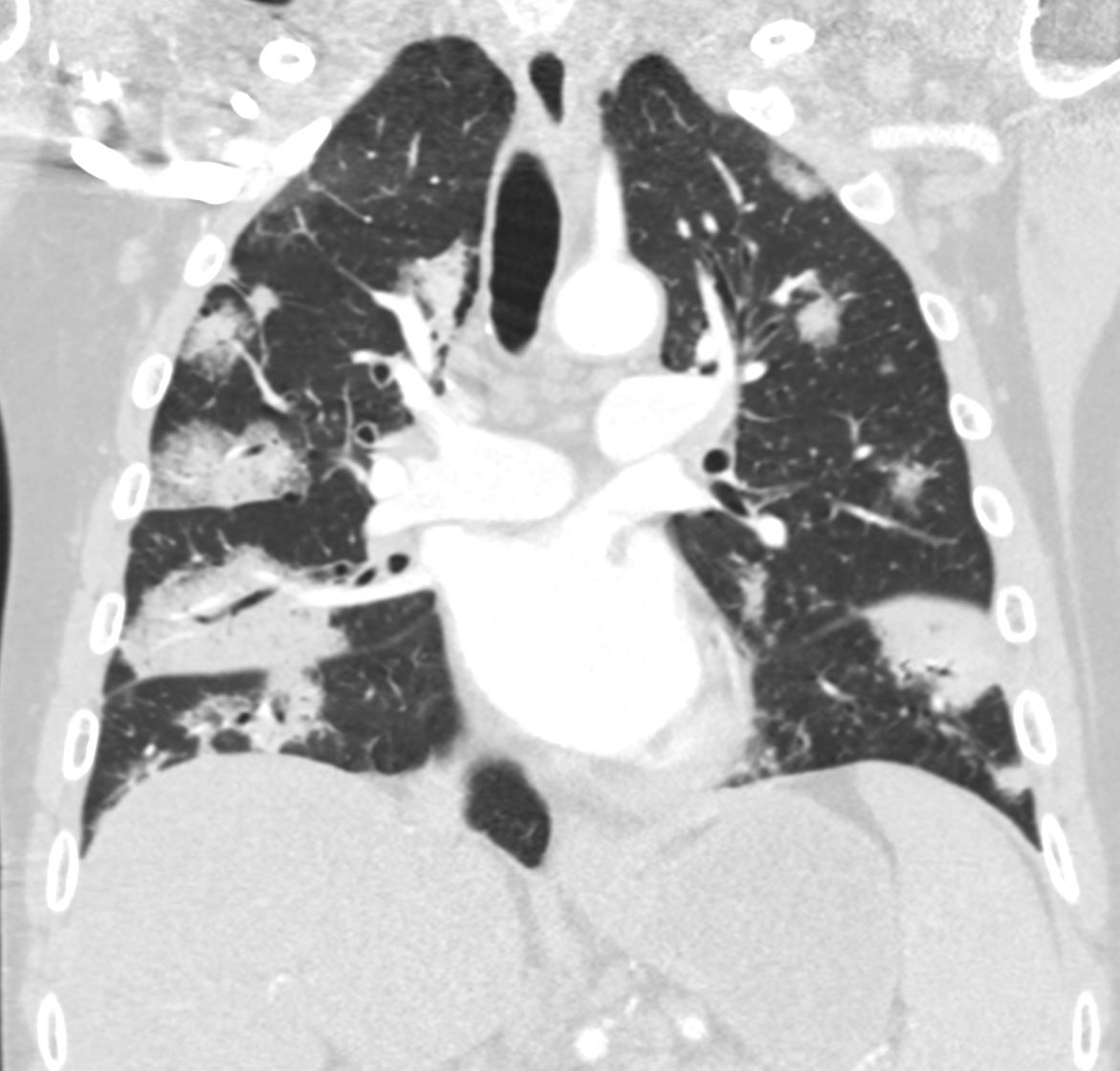
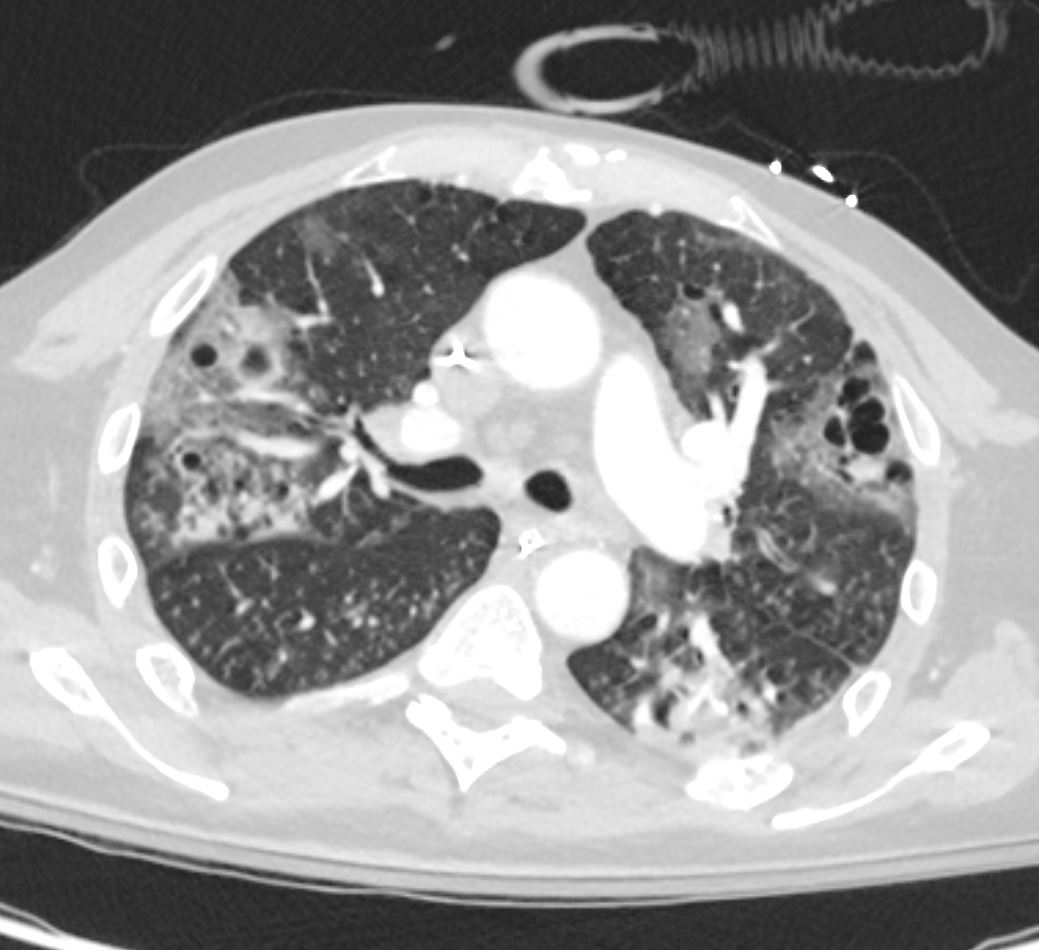
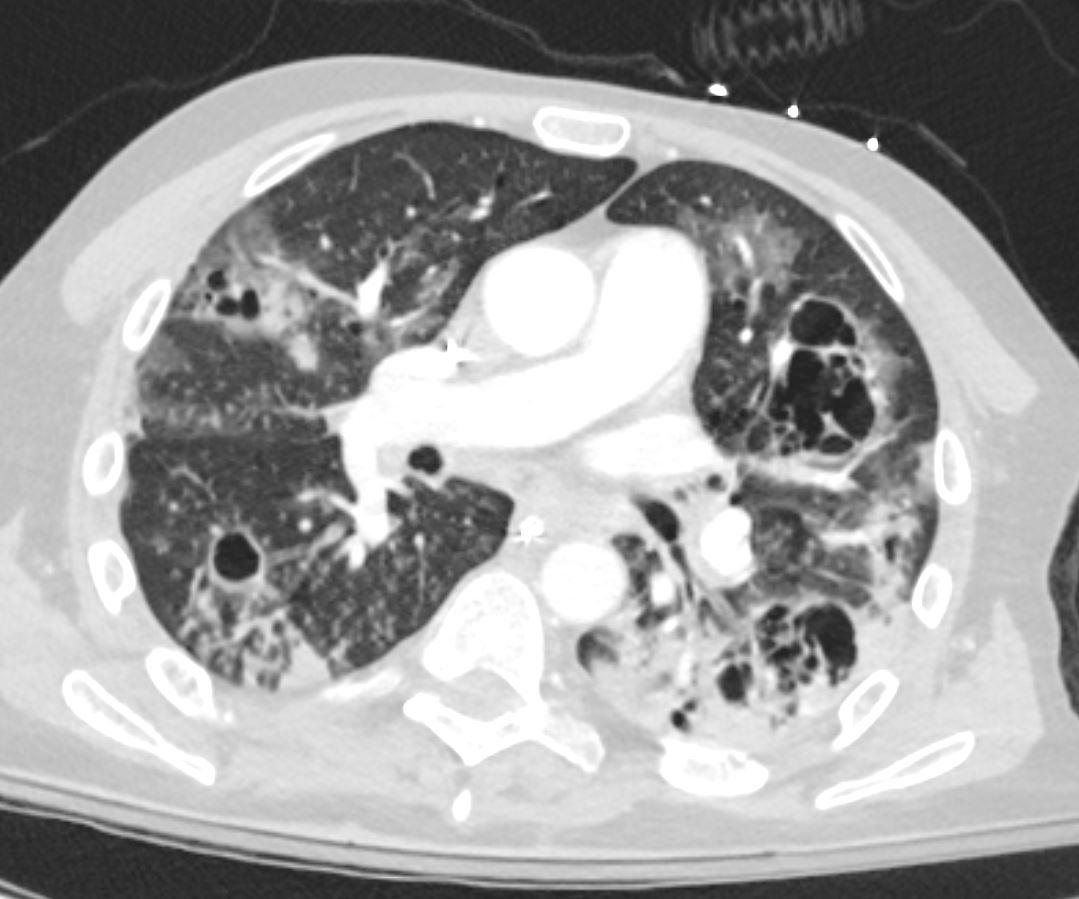
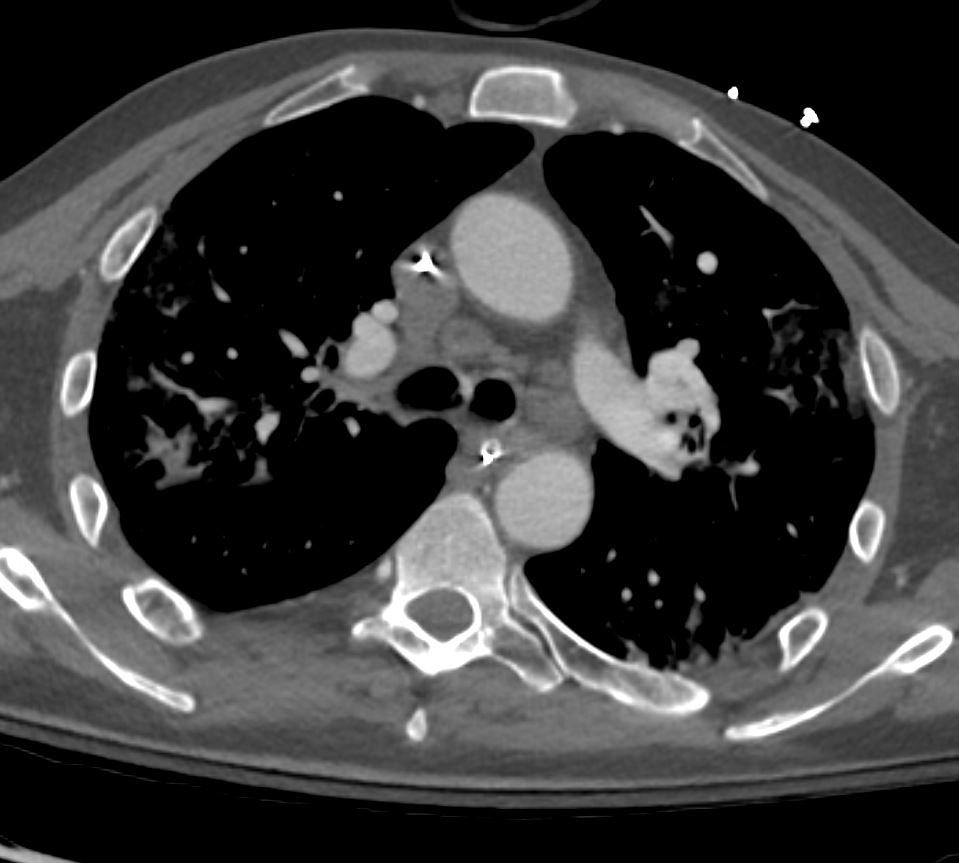
- Imaging 2 weeks ago
- presents with
- Multiple consolidative opacities throughout the lungs consistent with multifocal pneumonia. Consider fungal etiologies within the differential diagnosis.
Lungs-HIV-AIDS-possible-PCP-39M-003d-CT-2-weeks-ago.jpg
Lungs-HIV-AIDS-possible-PCP-39M-003f-CT-2-weeks-ago.jpg
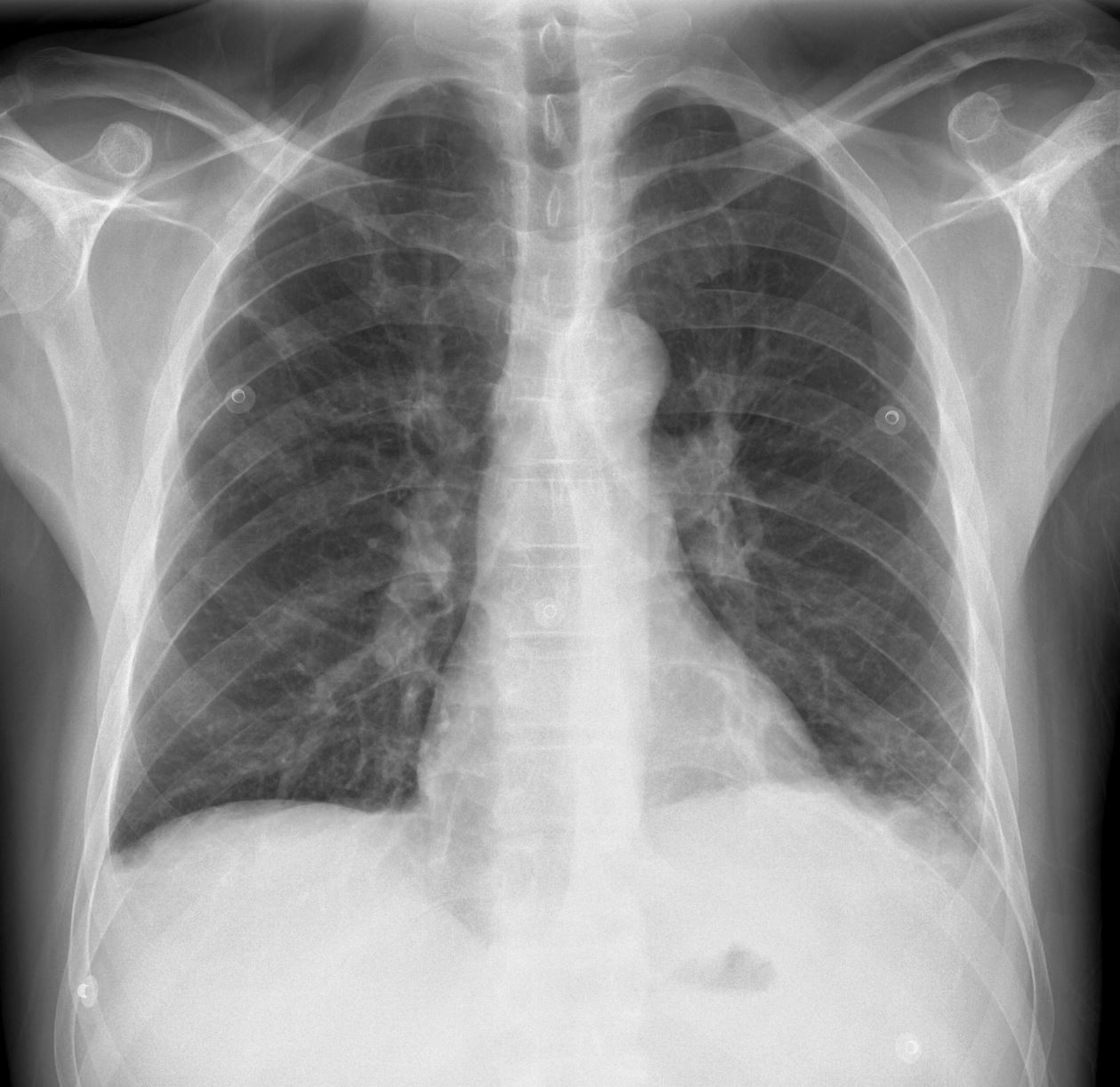
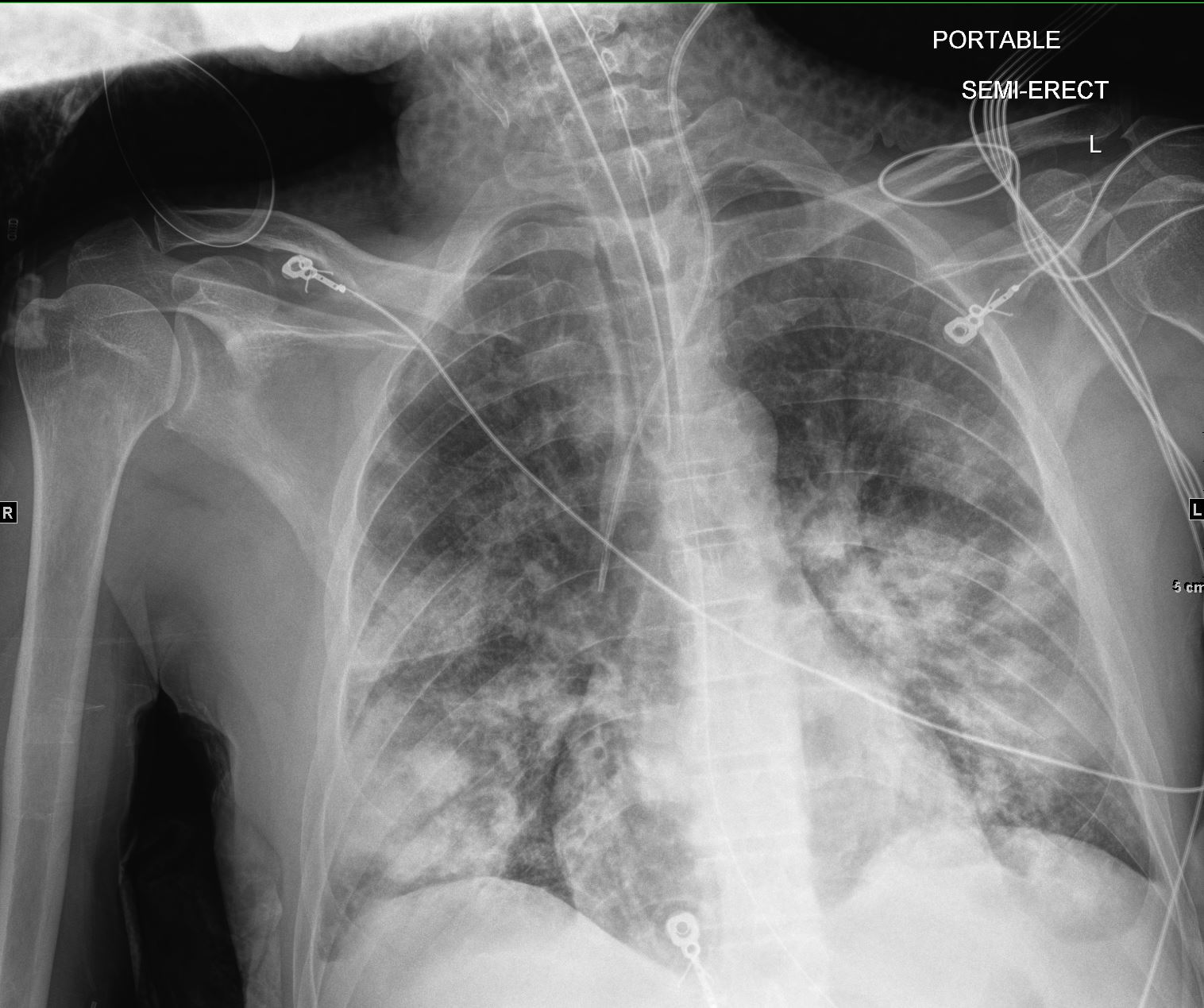
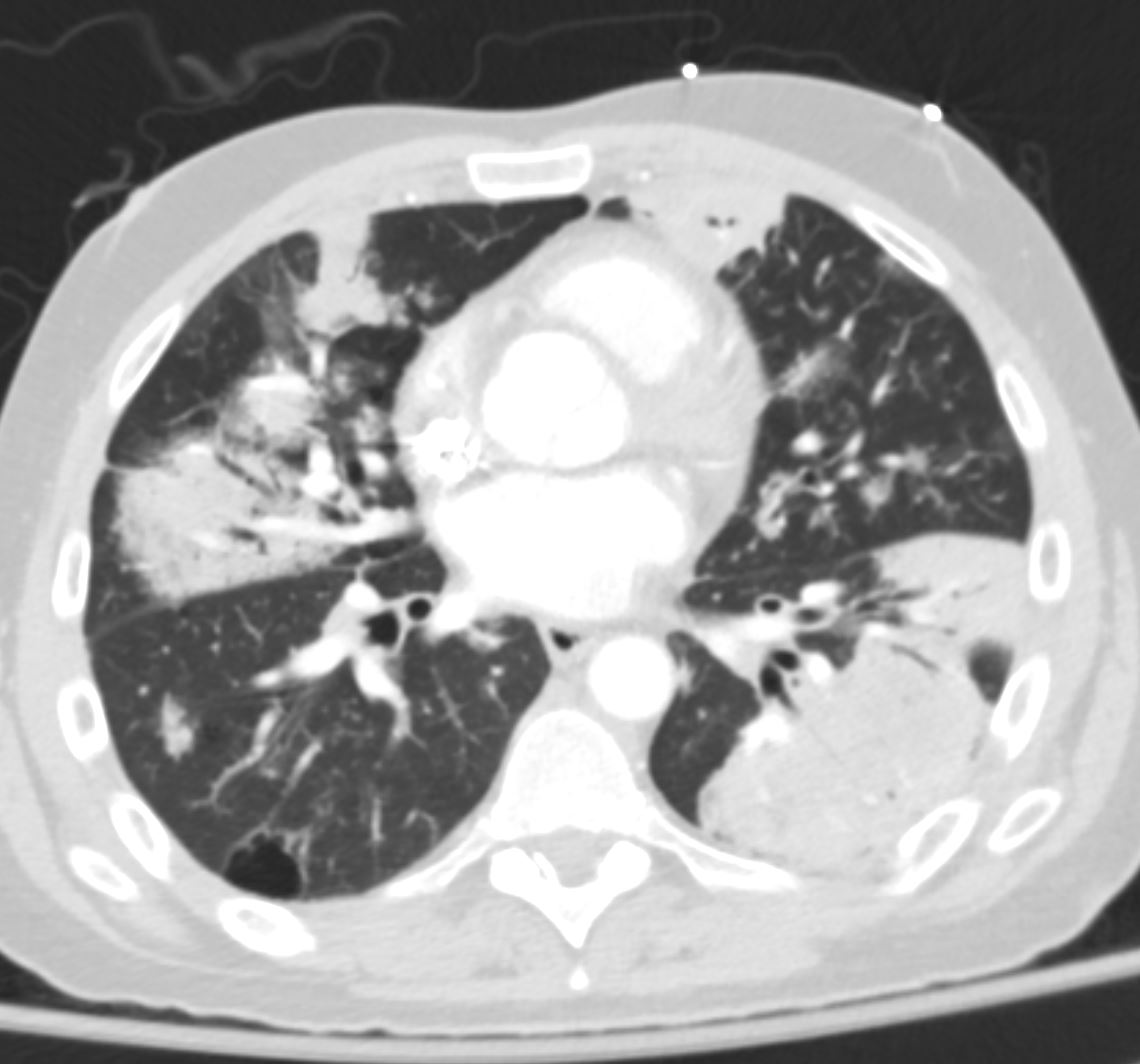
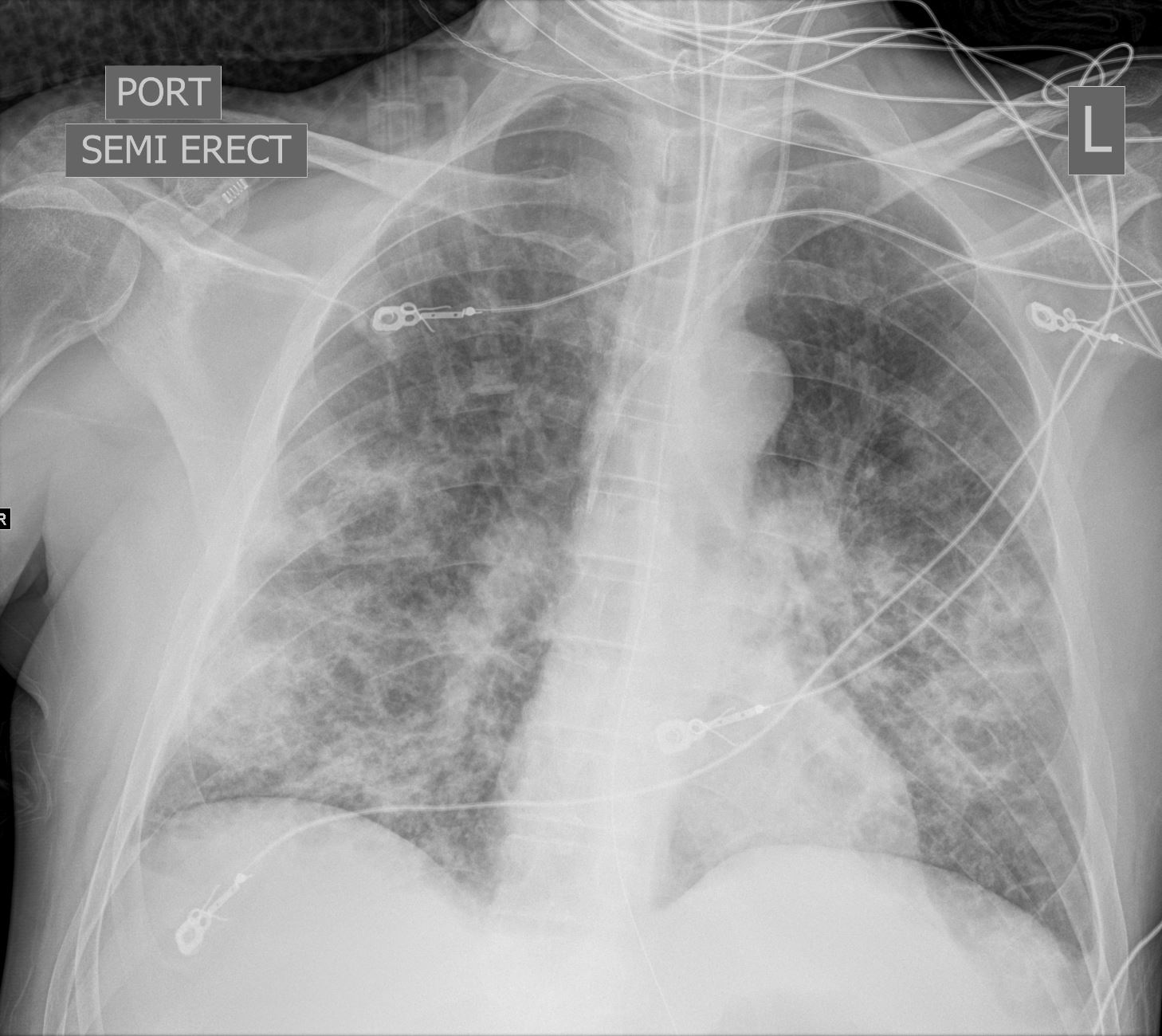
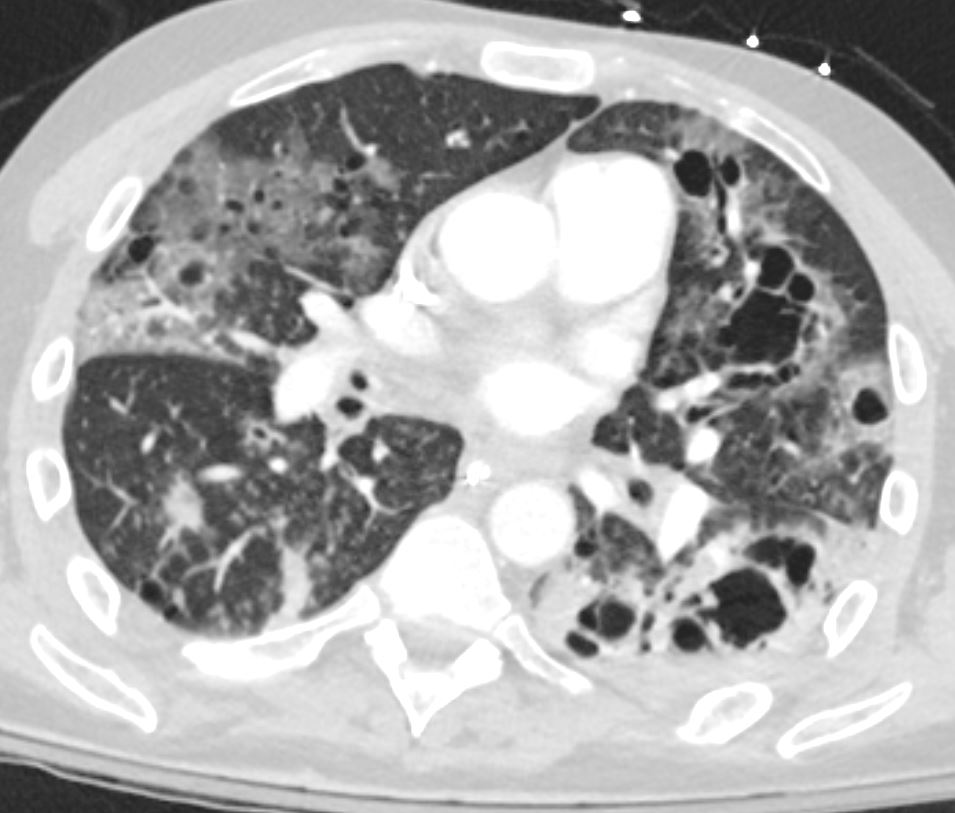
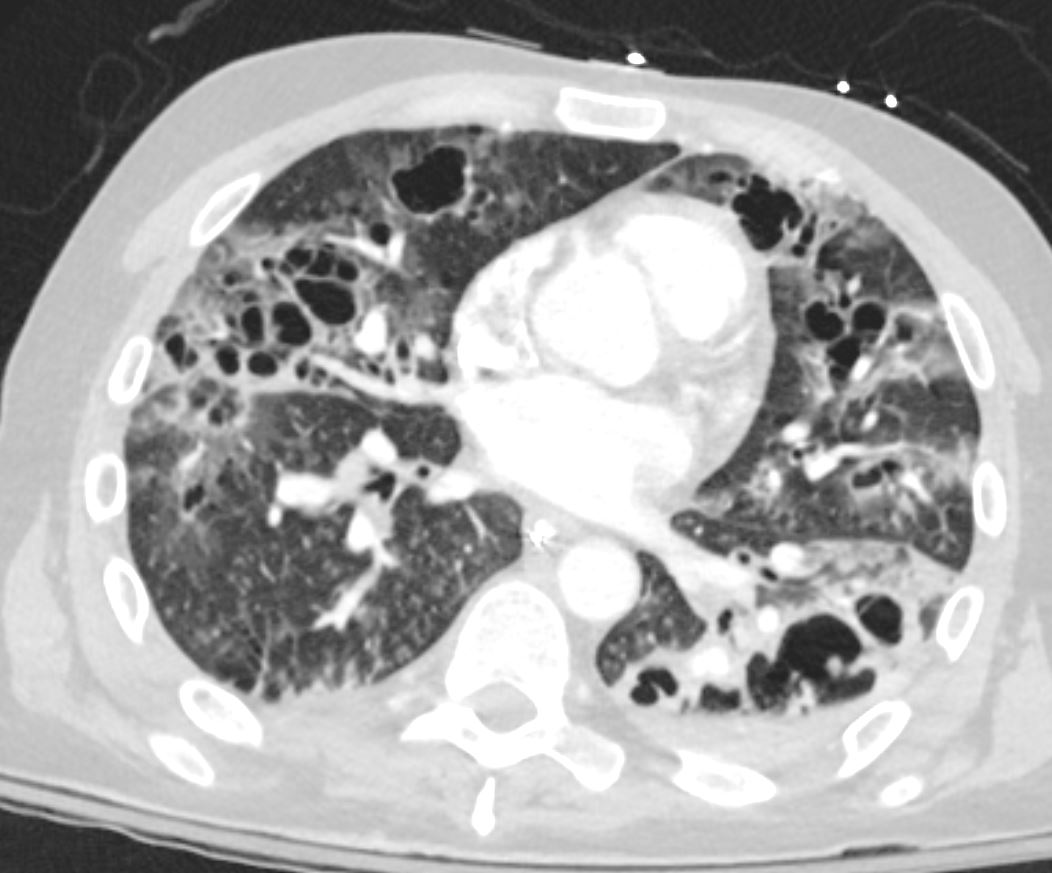
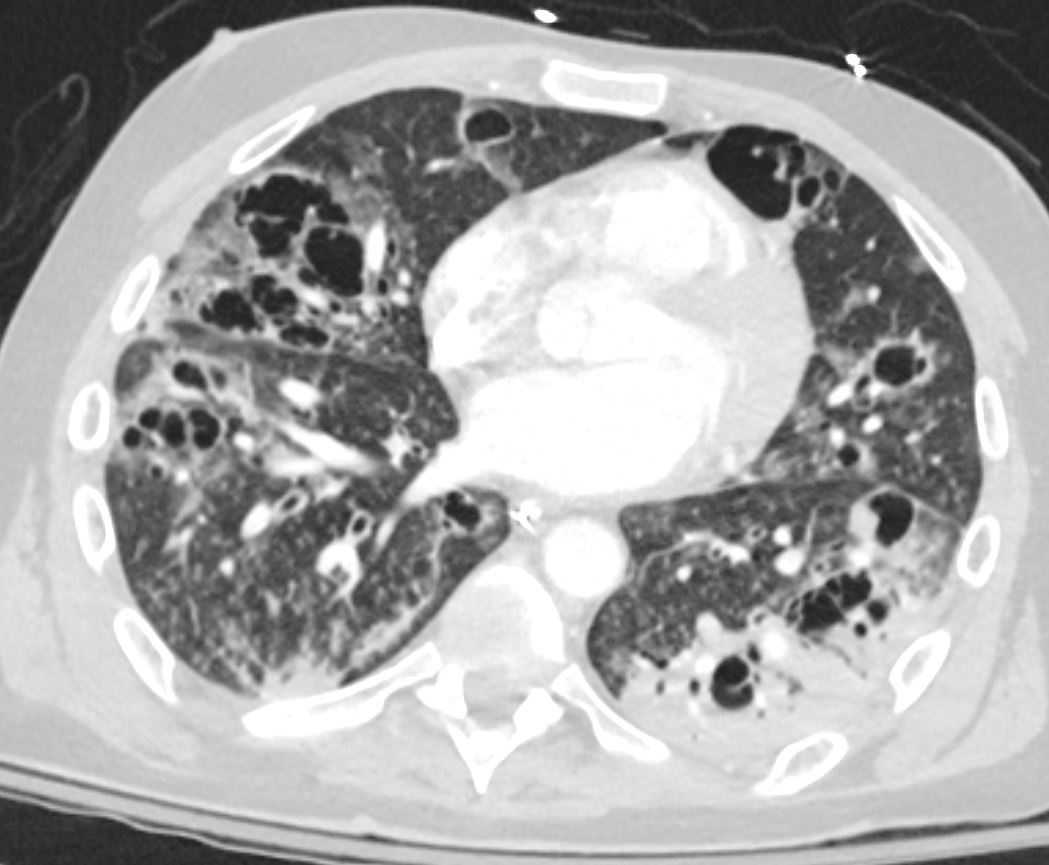
- Current CT
- CT
- multifocal infiltrates.
- blood cultures are positive for strep pneumo
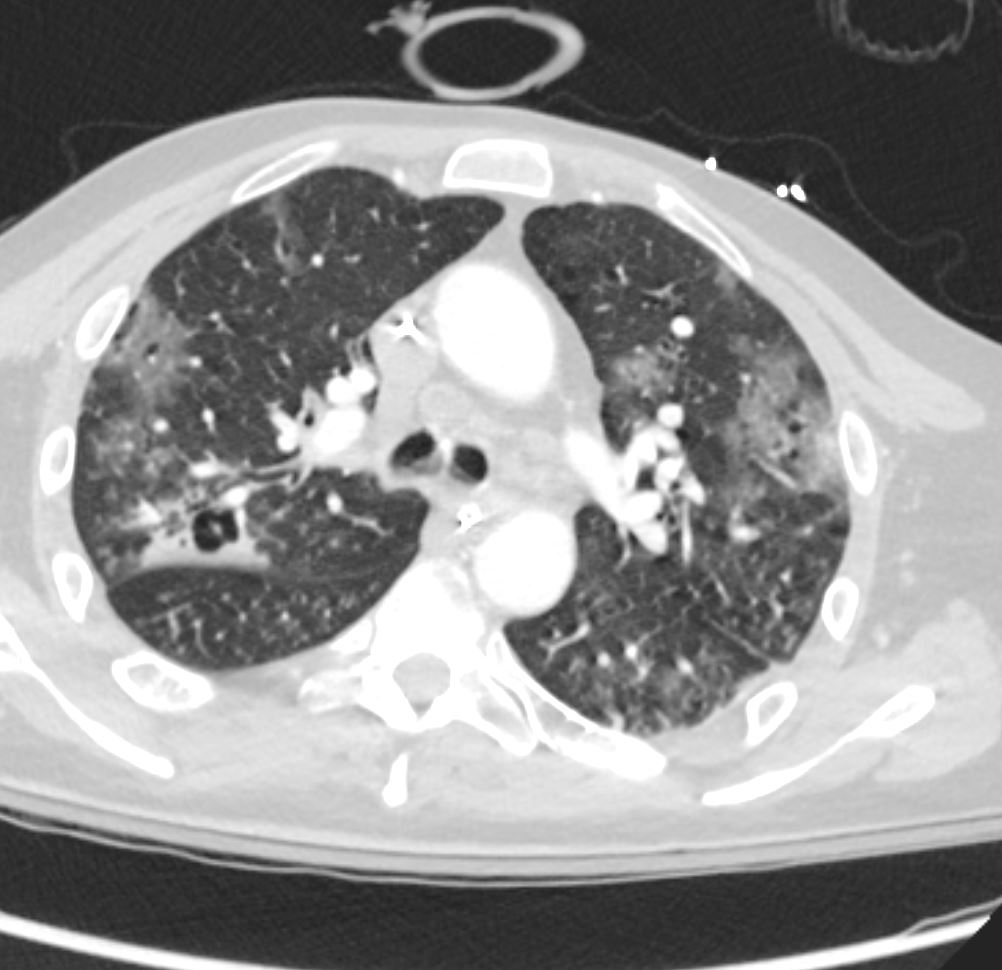
- Evolution of bilateral multilobar consolidative opacities with interval development of pronounced cystic and/or cavitary changes. There is also increased centrilobular nodularity which now extends throughout the bilateral lungs, likely related to infectious bronchiolitis. Main
differential consideration is PJP pneumonia, probably more likely than other fungal or bacterial causes of multi lobar cavitary pneumonia.
- CT





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}