
60F ongoing evaluation and management of connective tissue disease diagnosed 1 year ago
recently diagnosed CTD on the Sjogren’s/SLE spectrum (pruritic rash, sicca symptoms with compatible labial biopsy, Raynaud’s, abnormal nail capillaroscopy, ANA+, Ro >8.0, CCP+) complicated by ILD who presents to the ILD clinic
cutaneous findings, she reports the development of dyspnea on exertion which she first noticed over the summer of 9months ago
6 months agopositive ANA multiplex without specified titer
SSA > 8.0, remainder of ENA’s negative;
CRP 20.7 (ref < 5.0 mg/L),
SPEP mildly elevated alpha-2 and hypoalbuminemia,
negative tryptase.
CXR from 4 years ago

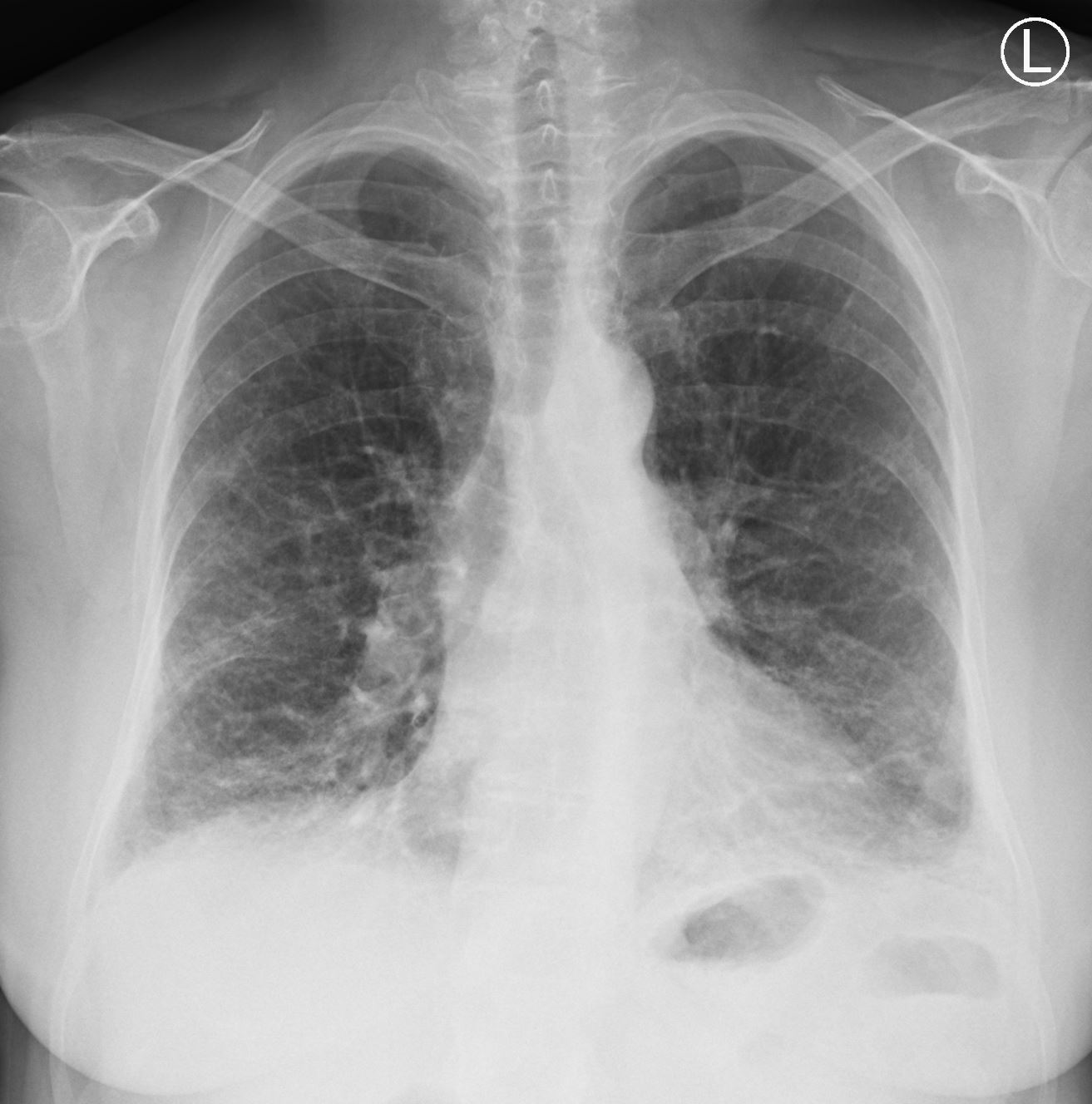
CXR from 6months ago
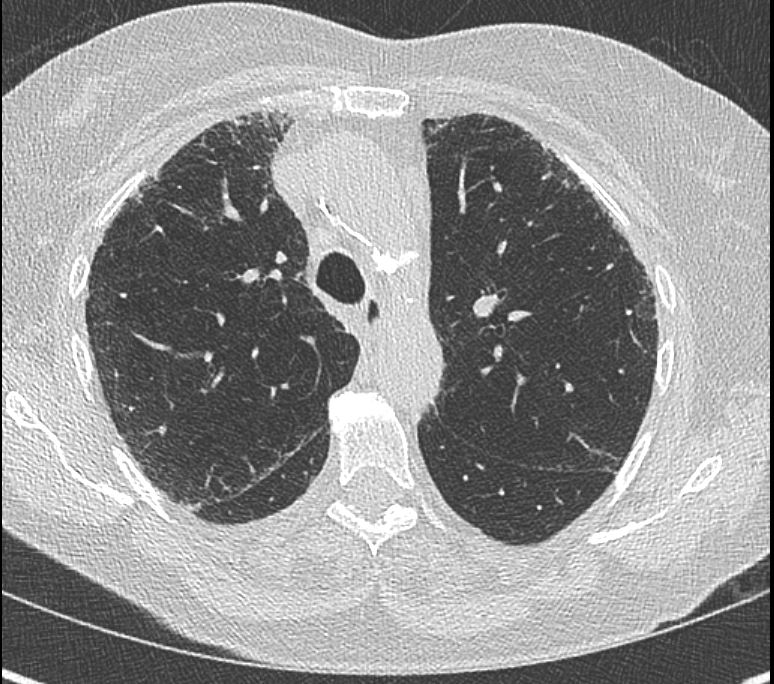
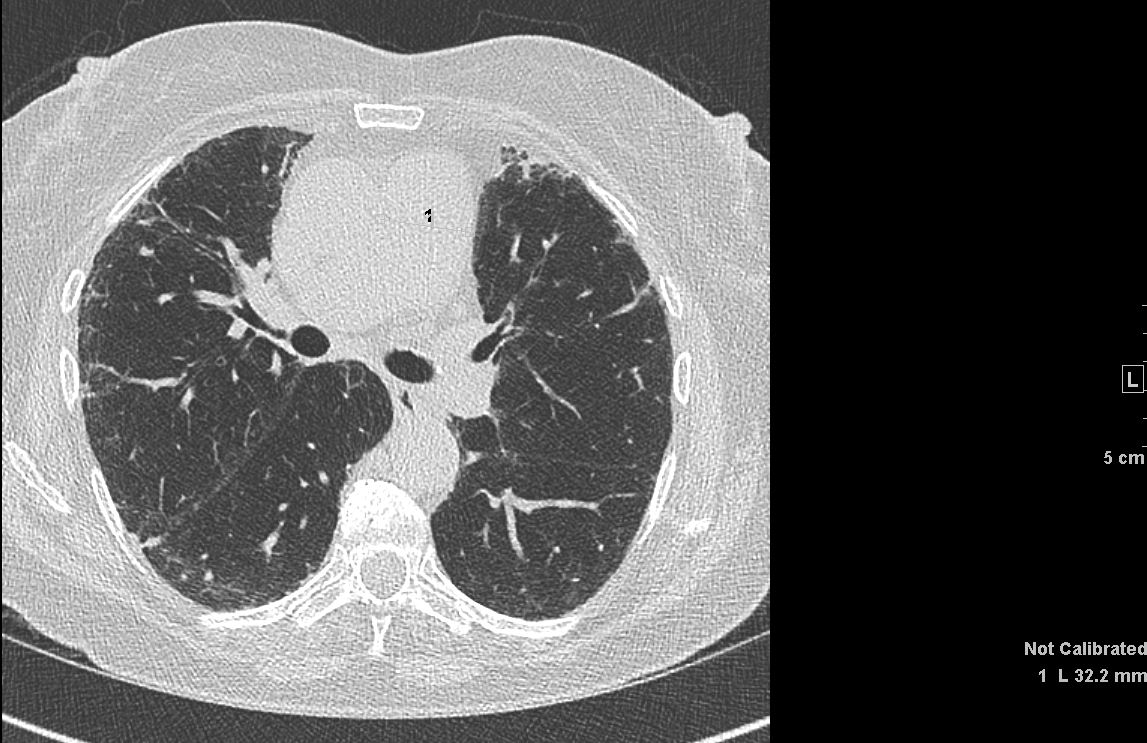
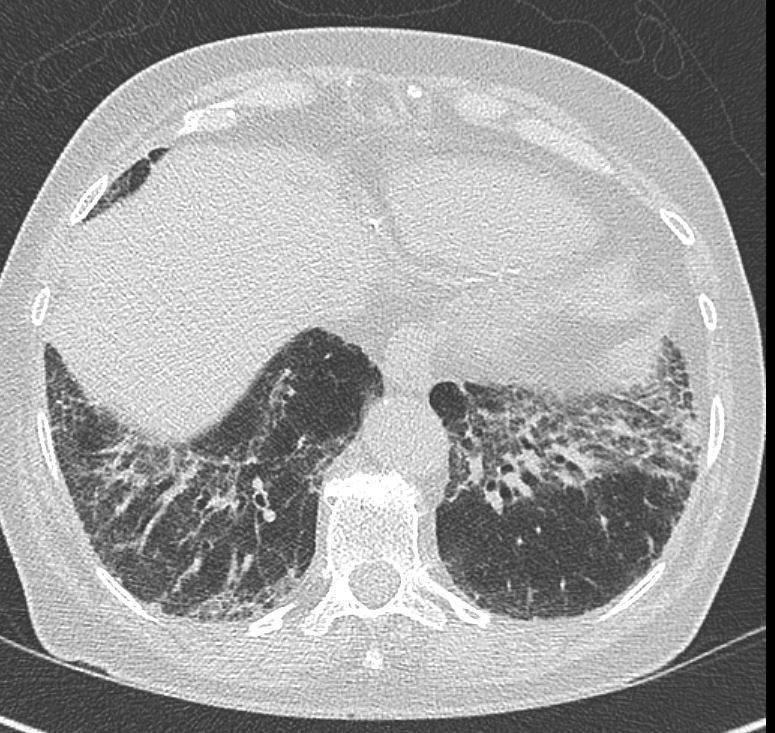
CT from 6months ago

{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Bibasilar reticular abnormalities with areas of intervening traction bronchiectasis and minimal ground-glass opacity but no honeycombing noted.
These findings are nonspecific but raise concern for interstitial fibrotic lung disease.
The imaging findings suggest a UIP versus NSIP pattern.
Clinical correlation isrecommended with any history of connective tissue disorder,occupational or domestic exposures or potential drug toxicity.
2. No lobar pneumonia, pneumothorax or pleural effusion.
Pathology
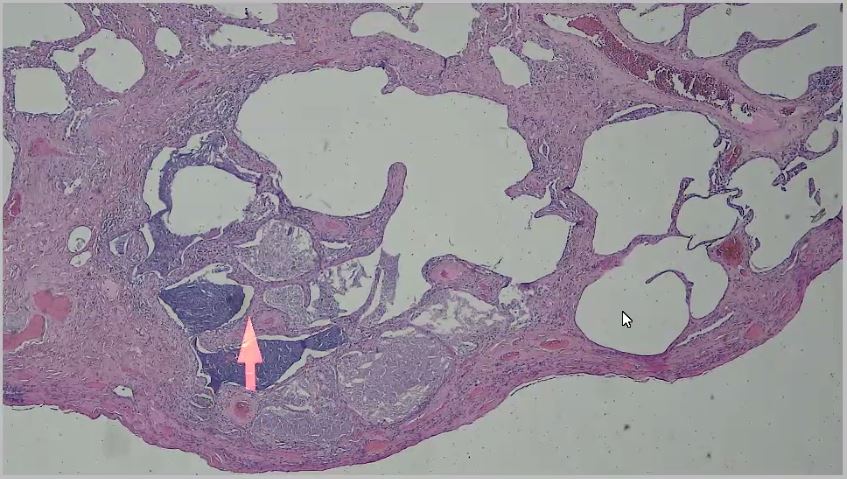
- The lung parenchyma is extensively fibrotic with fibrocystic changes. The interstitium shows only scant chronic inflammatory infiltrate, with a predominance of plasma cells. Fibroblastic foci are vanishingly rare. No granulomas or vasculitis are identified. Findings are consistent with end stage interstitial fibrosis or uncertainty etiology. The plasma cells suggest autoimmune disease.Pulmonary Function Trend ReportDate FVC FEV1 ratio FeF25-75 TLC
3 months ago- FVC2.18 84%
- FEV1 1.61 79%
- ratio 74
- TLC 3.38 74%
- RV —
- DLCO 8.01 41%
- Current
- FVC 2.31 89%
- FEV1 1.76 86%
- ratio 76
- TLC —
- RV–
- DLCO 5.08 26%Assessment and Plan: