
chest integrated “lp5”













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
image number
image 2
Title
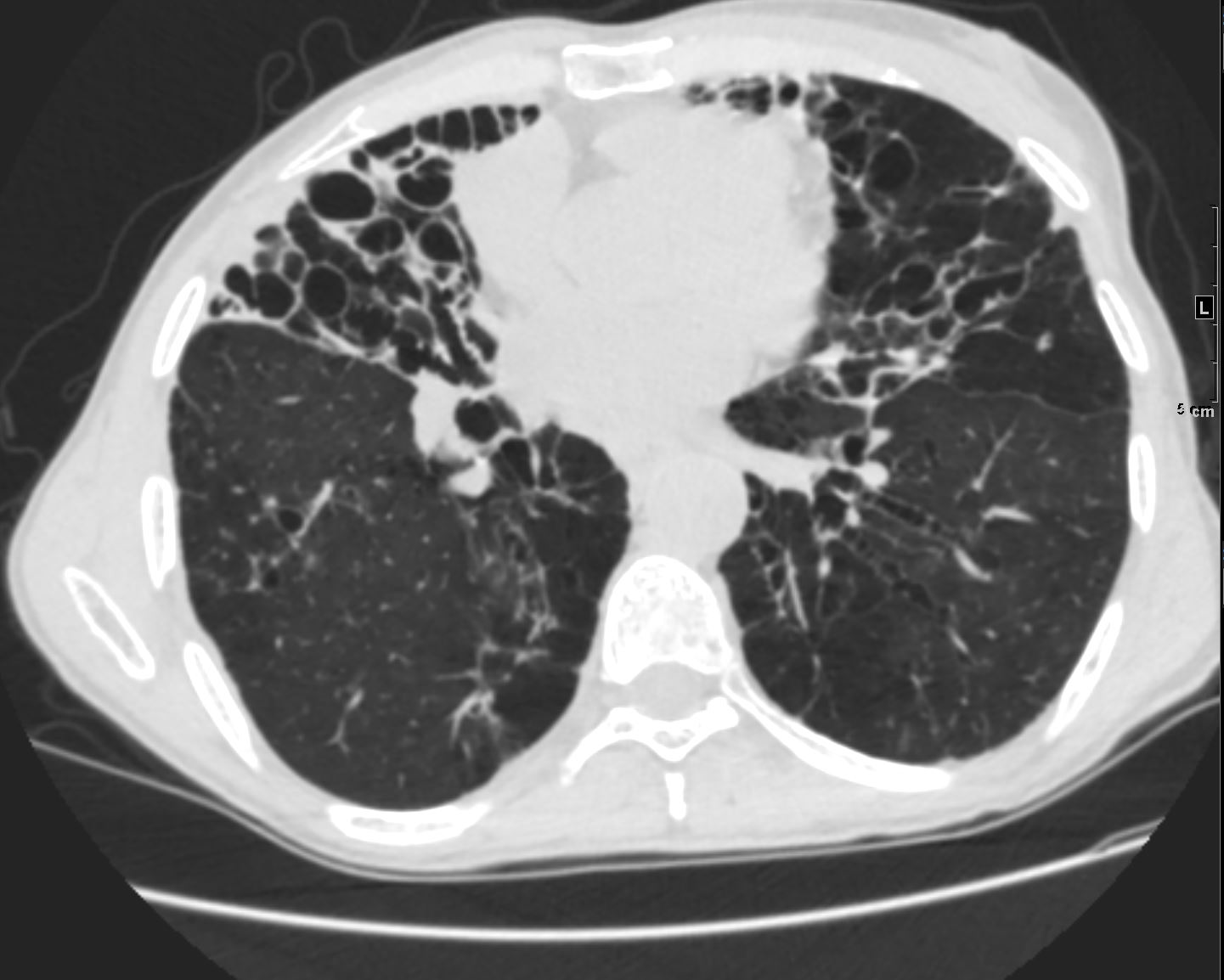
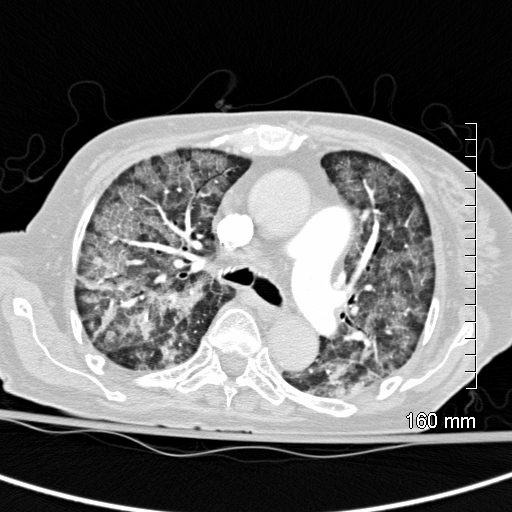
CT Emphysema, Paraseptal Emphysematous Changes Bilateral Lower Lobes65-year-old male with emphysema of the lungs presents with a cough, fever and leukocytosis. CT in the axial plane shows bibasilar paraseptal emphysematous changes and centrilobular changes in the lingula and RUL. Hyperinflation with resultant small heart is noted.Ashley Davidoff MD TheCommonVein.net 259Lu 117504
bleb
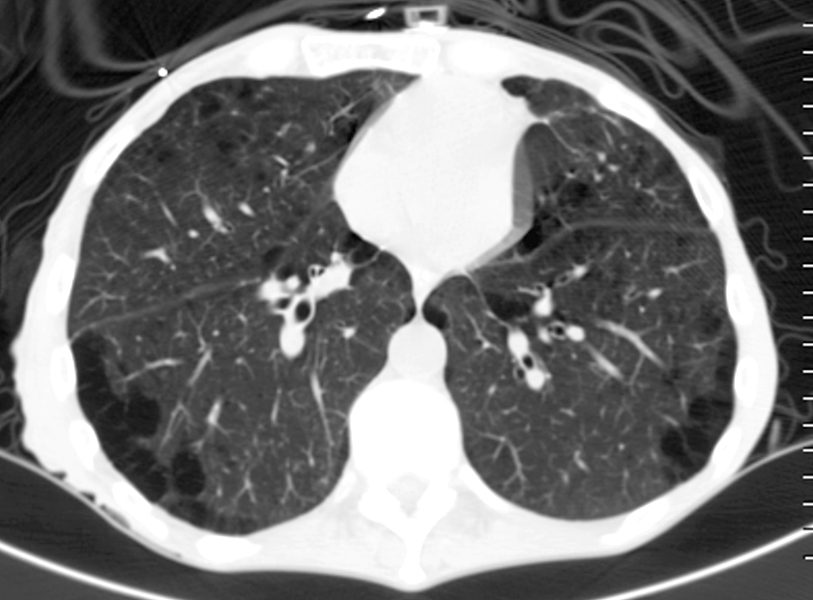
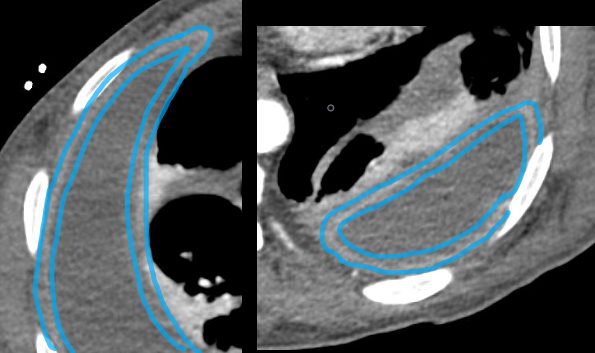
Axial CT – Lady Windermere Syndrome61-year-old male with a history of treated mycobacterial infections including MAC and chronic cough.Axial CT at the level of the mid to lower chest shows mildly ectatic segmental airways to the lower, and middle lobe bronchi but significant bronchiectasis to the middle lobe and lingula involving the subsegmental airways. There is a relative paucity of mucus in the ectatic airways. The history of MAC and the distribution of the bronchiectasis in the middle lobe and lingula are reminiscent of the diagnosis of Lady Windermere syndromeAshley Davidoff MD TheCommonVein.net 250Lu 135876
Axial CT – Lady Windermere Syndrome61-year-old male with a history of treated mycobacterial infections including MAC and chronic cough.Axial CT at the level of the mid to lower chest shows mildly ectatic segmental airways to the lower, and middle lobe bronchi but significant bronchiectasis to the middle lobe and lingula involving the subsegmental airways. There is a relative paucity of mucus in the ectatic airways. The history of MAC and the distribution of the bronchiectasis in the middle lobe and lingula are reminiscent of the diagnosis of Lady Windermere syndromeAshley Davidoff MD TheCommonVein.net 250Lu 135876
bronchiectasis
136598c
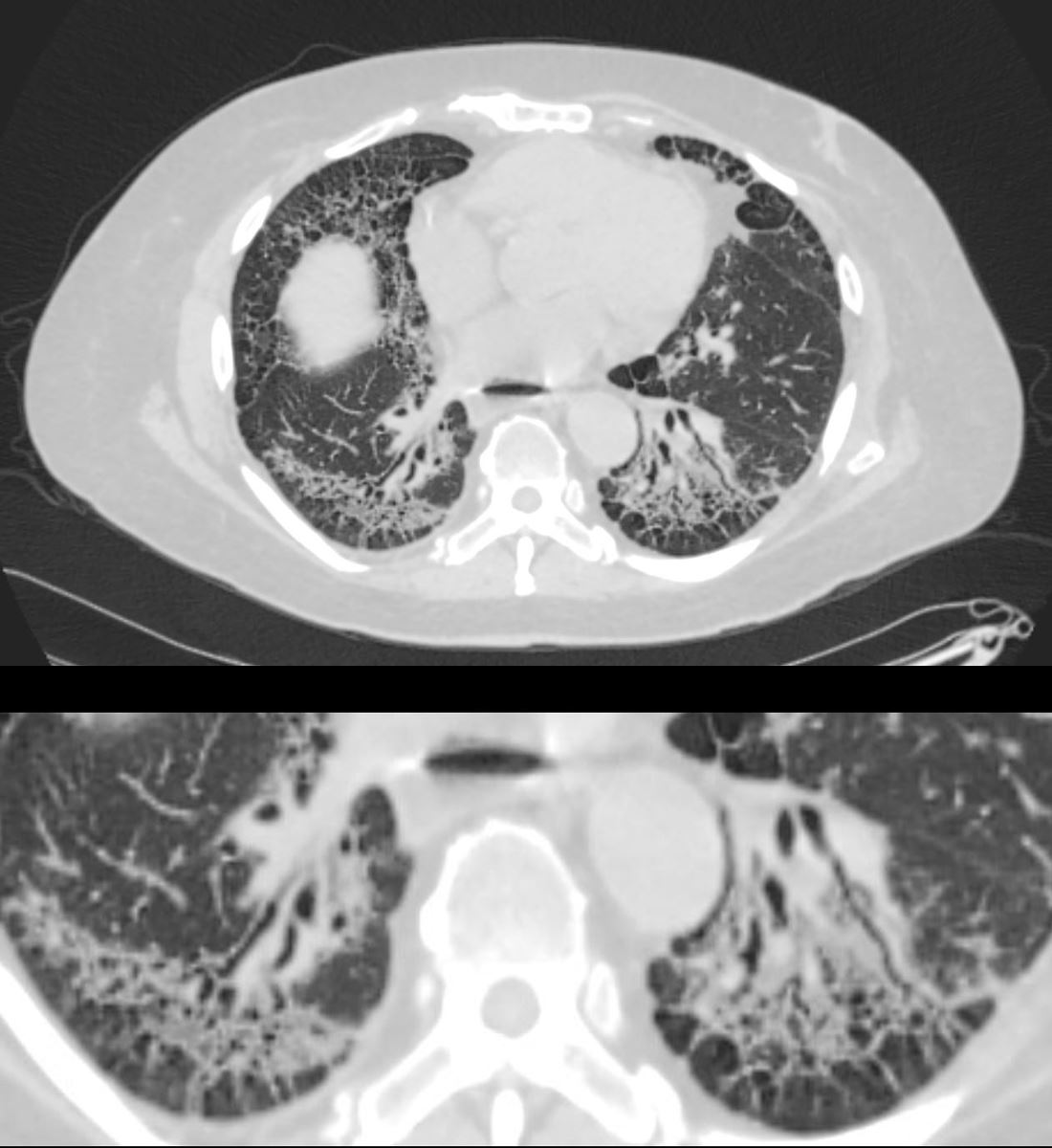
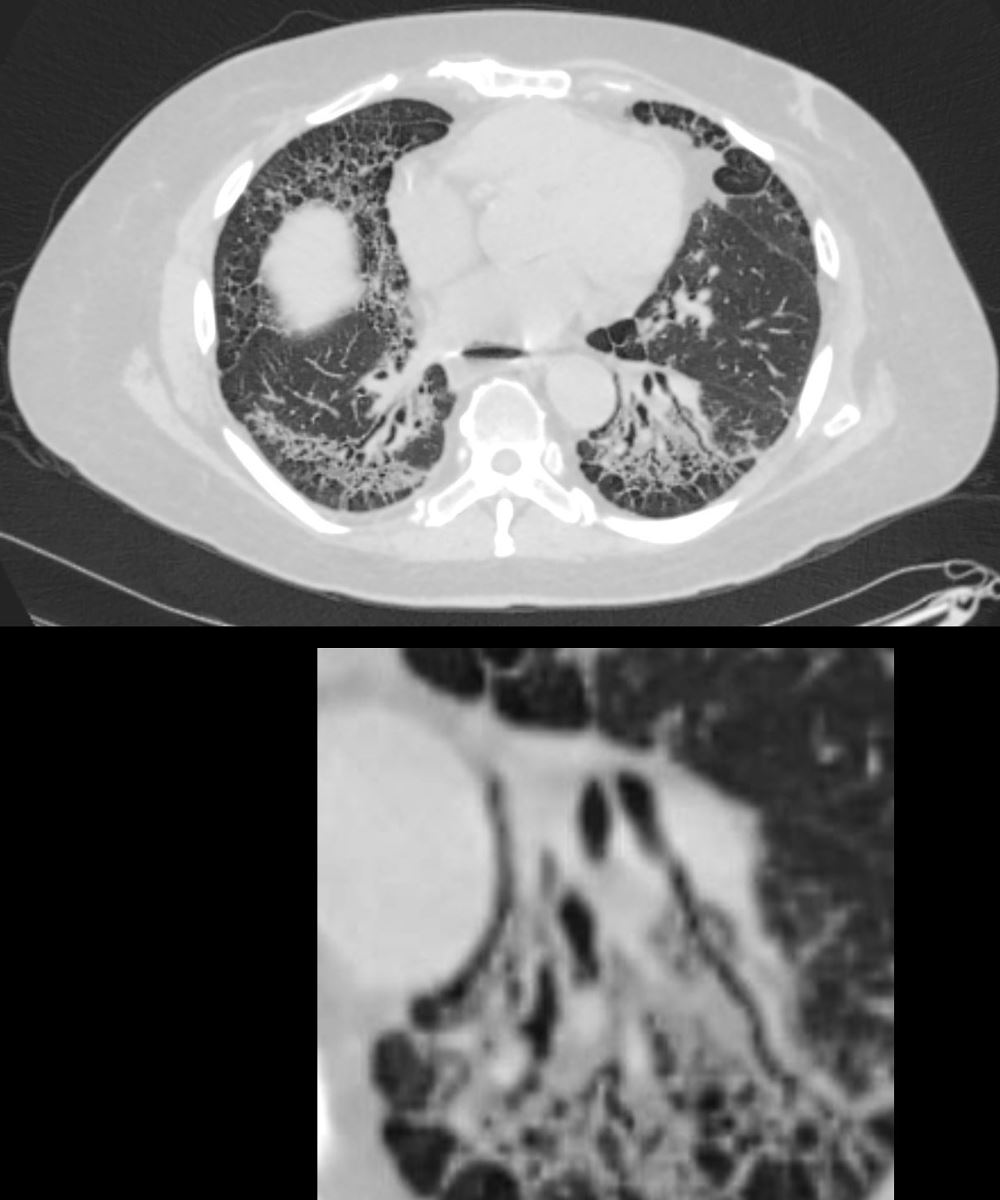
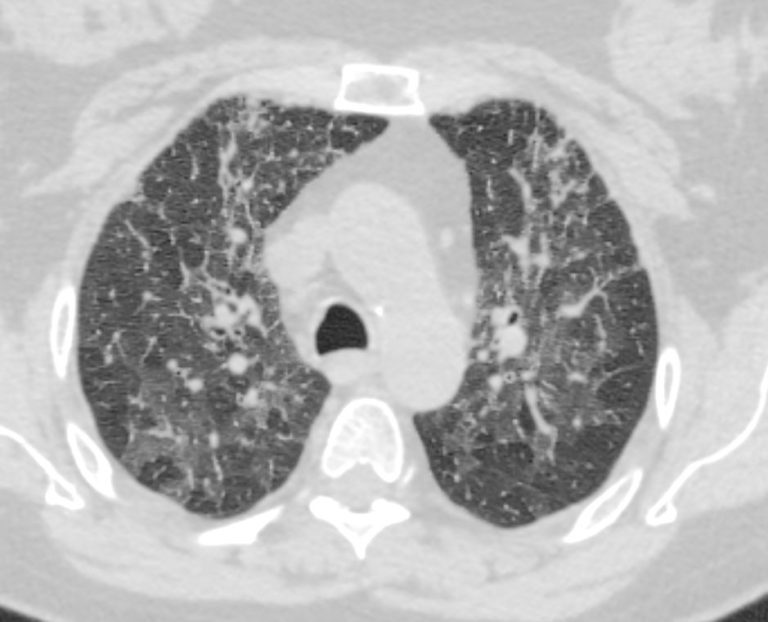
Fibrotic NSIP59-year-old male presents with history of scleroderma, Raynaud’s disease, and ILDUpper ImageAxial CT shows bibasilar ground glass, bronchiectasis, and bronchiolectasis with volume loss and with crowding of the bronchovascular bundles posteriorly. There is subpleural sparing. Note air-fluid level in the distended esophagus.The lower image focuses on the peripheral sparing. The spared secondary lobules have also undergone enlargement secondary to the fibrotic processAshley Davidoff MD TheCommonVein.net 110Lu 136598c01
136598c
Fibrotic NSIP59-year-old male presents with history of scleroderma, Raynaud’s disease, and ILDUpper ImageAxial CT shows bibasilar peripheral reticular changes, ground glass, bronchiectasis, and bronchiolectasis with volume and with crowding of the bronchovascular bundles posteriorly. There is subpleural sparing posteriorly. Note air-fluid level in the distended esophagus.Lower ImageThe lower image focuses on the traction bronchiectasis caused by the fibrotic processAshley Davidoff MD TheCommonVein.net 110Lu 136598c
bronchiolectasis
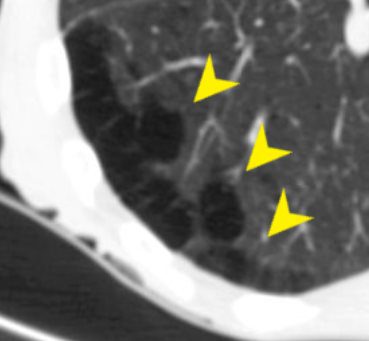
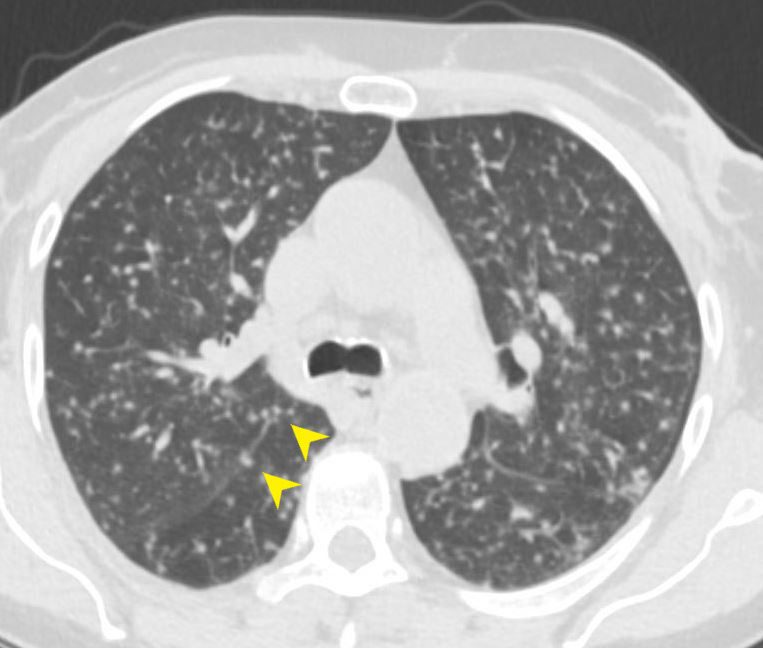
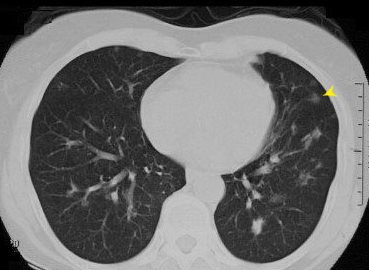
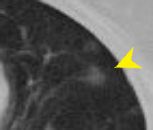
Chest CT above shows bronchiolitis which is characterized by peribronchial thickening which is thickening of the small airways of lung (yellow arrows)Ashley Davidoff MD TheCommonVein.net 81F-bronchiolitis-infection-inflammation-004
Chest CT above shows bronchiolitis which is characterized by peribronchial thickening which is thickening of the small airways of lung (yellow arrows)Ashley Davidoff MD TheCommonVein.net 81F-bronchiolitis-infection-inflammation-004
bronchiolitis
Frontal and Lateral CXR shows follicular bronchiolitis which is characterized by a coarsened nodular interstitial pattern. Ashley Davidoff MD TheCommonVein.net 132Lu 136650c B.A
Frontal and Lateral CXR shows follicular bronchiolitis which is characterized by a coarsened nodular interstitial pattern. Ashley Davidoff MD TheCommonVein.net 132Lu 136650c B.A
bronchiolitis (CXR)
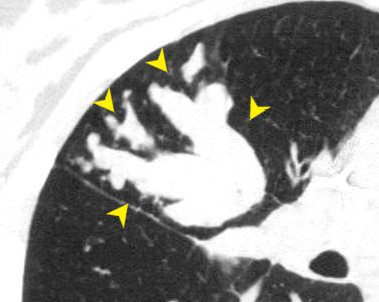
Finger in Glove Sign19 year old female with cystic fibrosis and bronchiectasisCT scan through the upper lung fields shows mucin filled subsegmental bronchi of the right upper lobe with morphology reminiscent of the “finger in glove” signCourtesy Priscilla Slanetz MD MPH TheCommonVein.net 31966 B.A
Finger in Glove Sign
19 year old female with cystic fibrosis and bronchiectasis
CT scan through the upper lung fields shows mucin filled subsegmental bronchi of the right upper lobe with morphology reminiscent of the “finger in glove” sign (point to by yellow arrows)
Courtesy Priscilla Slanetz MD MPH TheCommonVein.net31966cl B.A
bronchocele
bronchocentric
bronchocentric
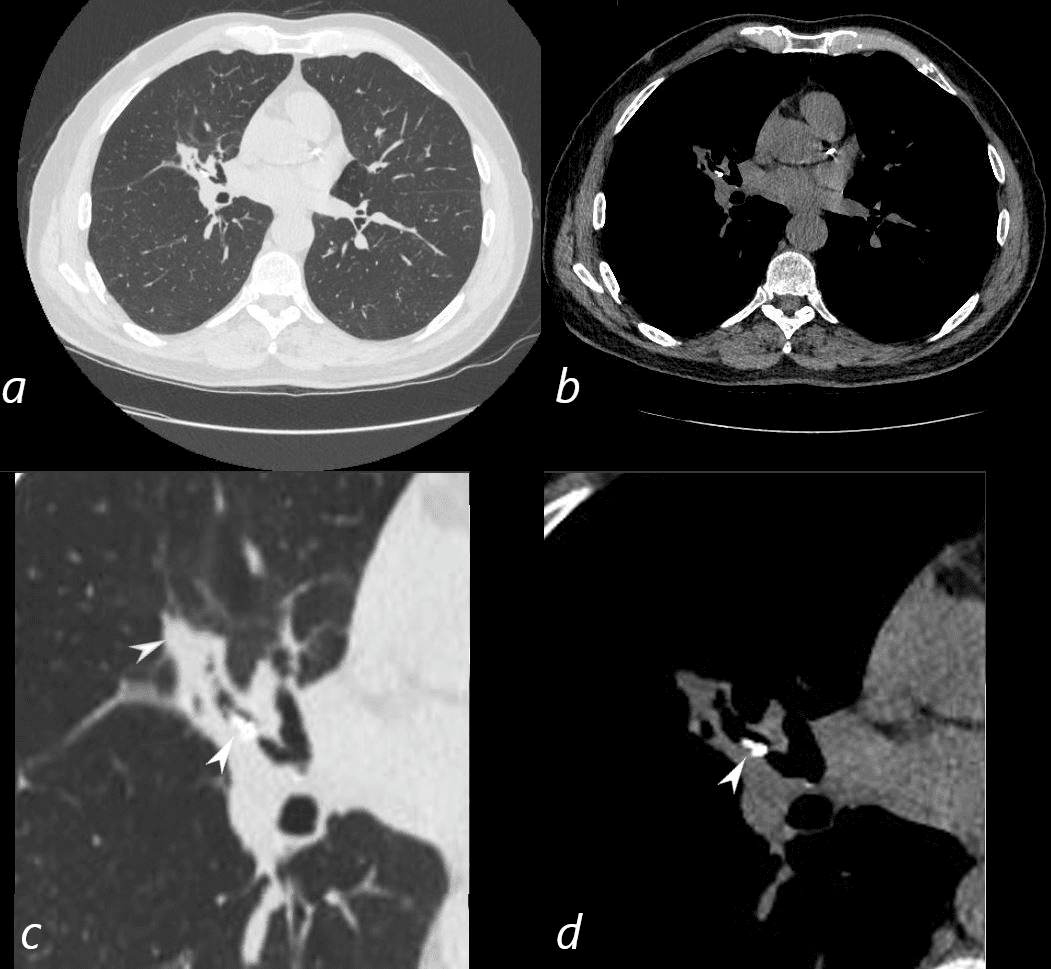
CT in the axial plane shows a bilobed calcified broncholith in the lateral segment of the middle lobe (c, d white arrowheads) with post obstructive atelectasis (c, blue arrowhead)Ashley Davidoff MD TheCommonVein.net 136585cL B.A
1
CT in the axial plane shows a bilobed calcified broncholith in the lateral segment of the middle lobe (c, d white arrowheads) with post obstructive atelectasis (c, blue arrowhead)
Ashley Davidoff MD TheCommonVein.net 136585cL B.A
broncholith
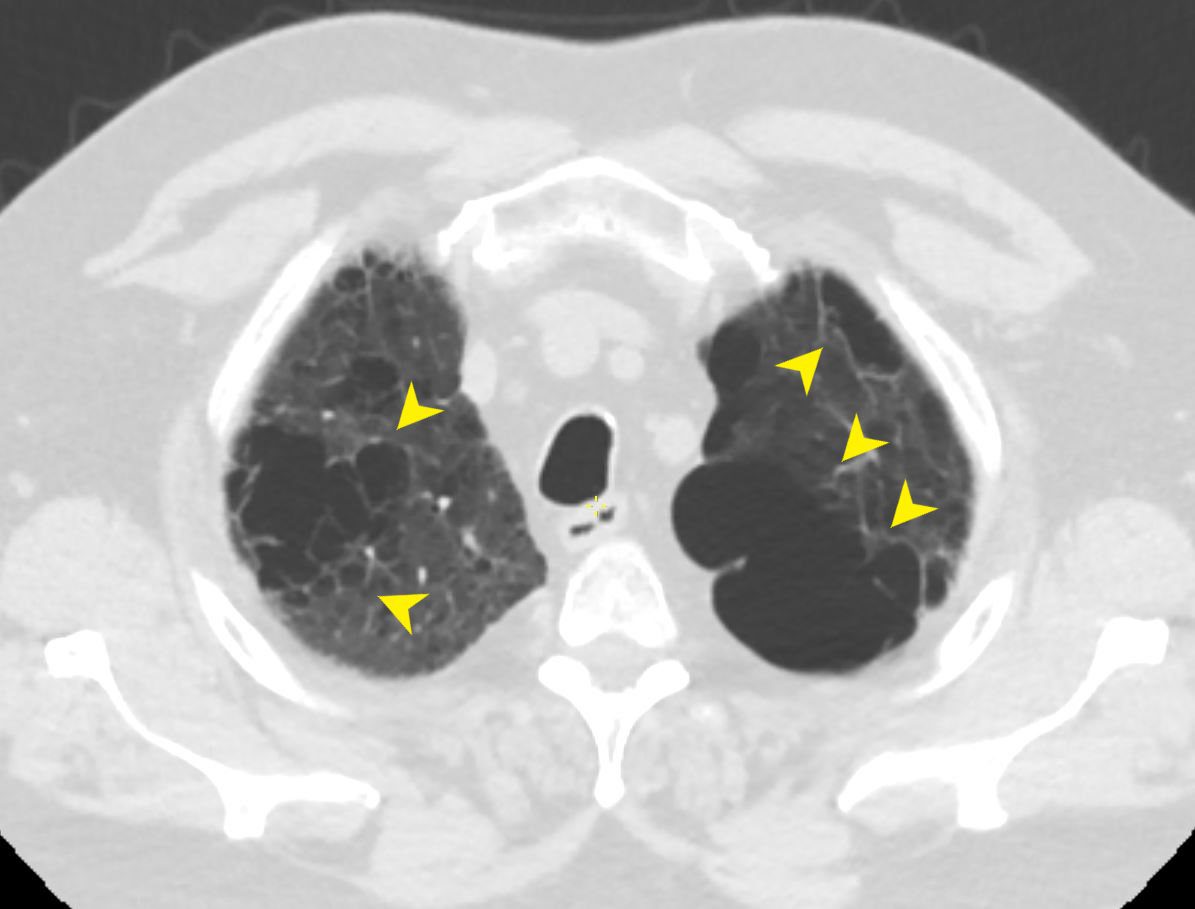
CT Scan Bilateral Apical Builla Centrilobular EmphysemaCT scan in the axial plane shows bilateral apical bullous lung disease, most commonly seen in emphysema Ashley Davidoff MD TheCommonVein.Net 136440 B.A
CT Scan Bilateral Apical Builla Centrilobular Emphysema
CT scan in the axial plane shows bilateral apical bullous lung disease, most commonly seen in emphysema
Ashley Davidoff MD TheCommonVein.Net 136440 B.A
bulla
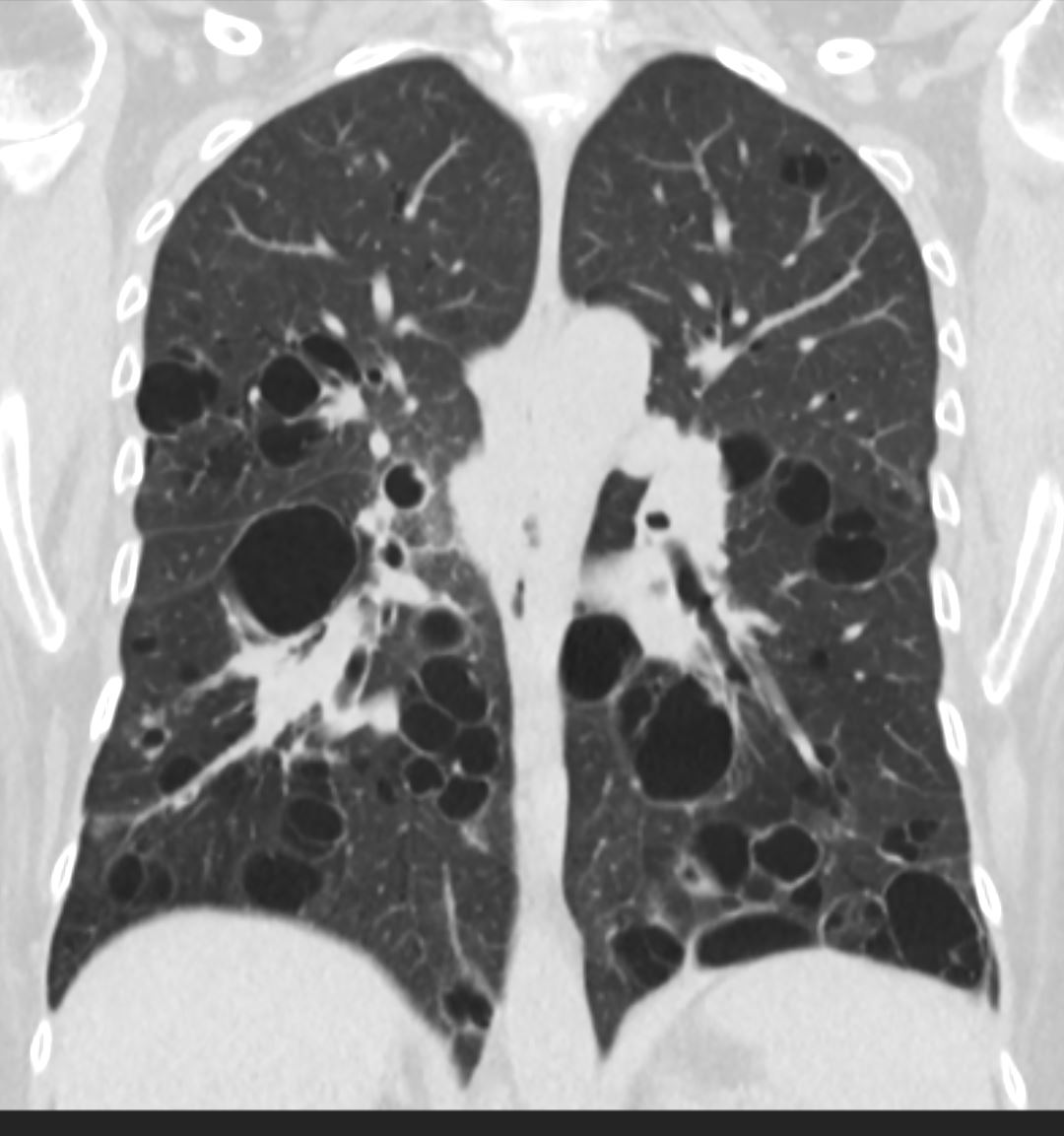
CT Scan Bilateral Apical Bulla Centrilobular EmphysemaCT scan in the coronal plane shows bilateral apical bullous lung disease, magnified in the lower imageAshley Davidoff MD TheCommonVein.Net 136439c B.A
CT scan in the coronal plane of shows bilateral apical bullous lung disease, magnified in the lower imageAshley Davidoff MD TheCommonVein.Net 136439c B.A
bullous emphysema
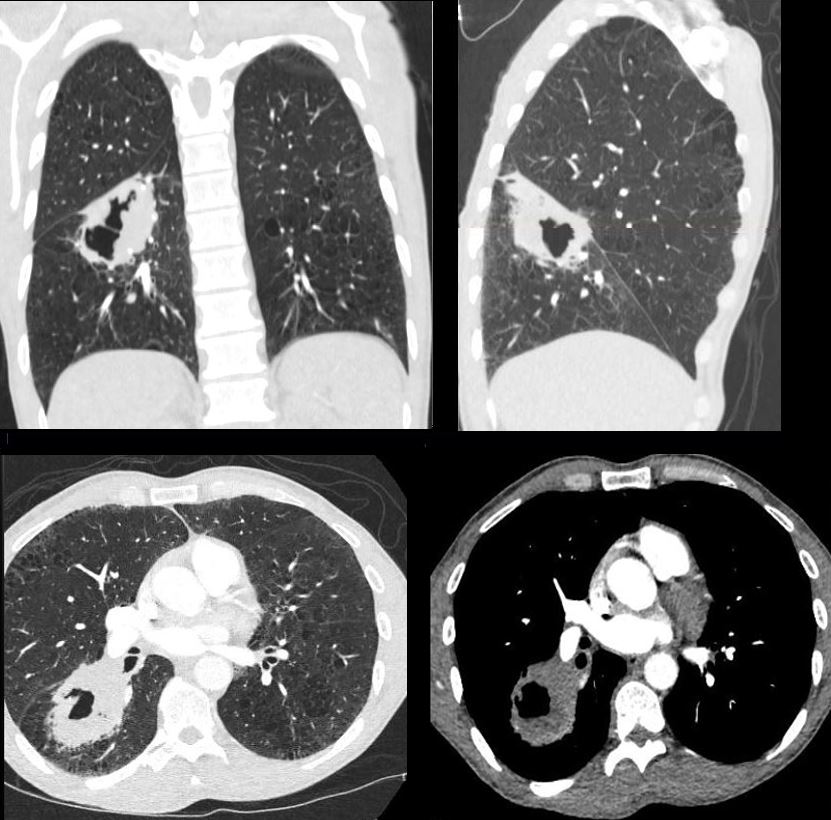
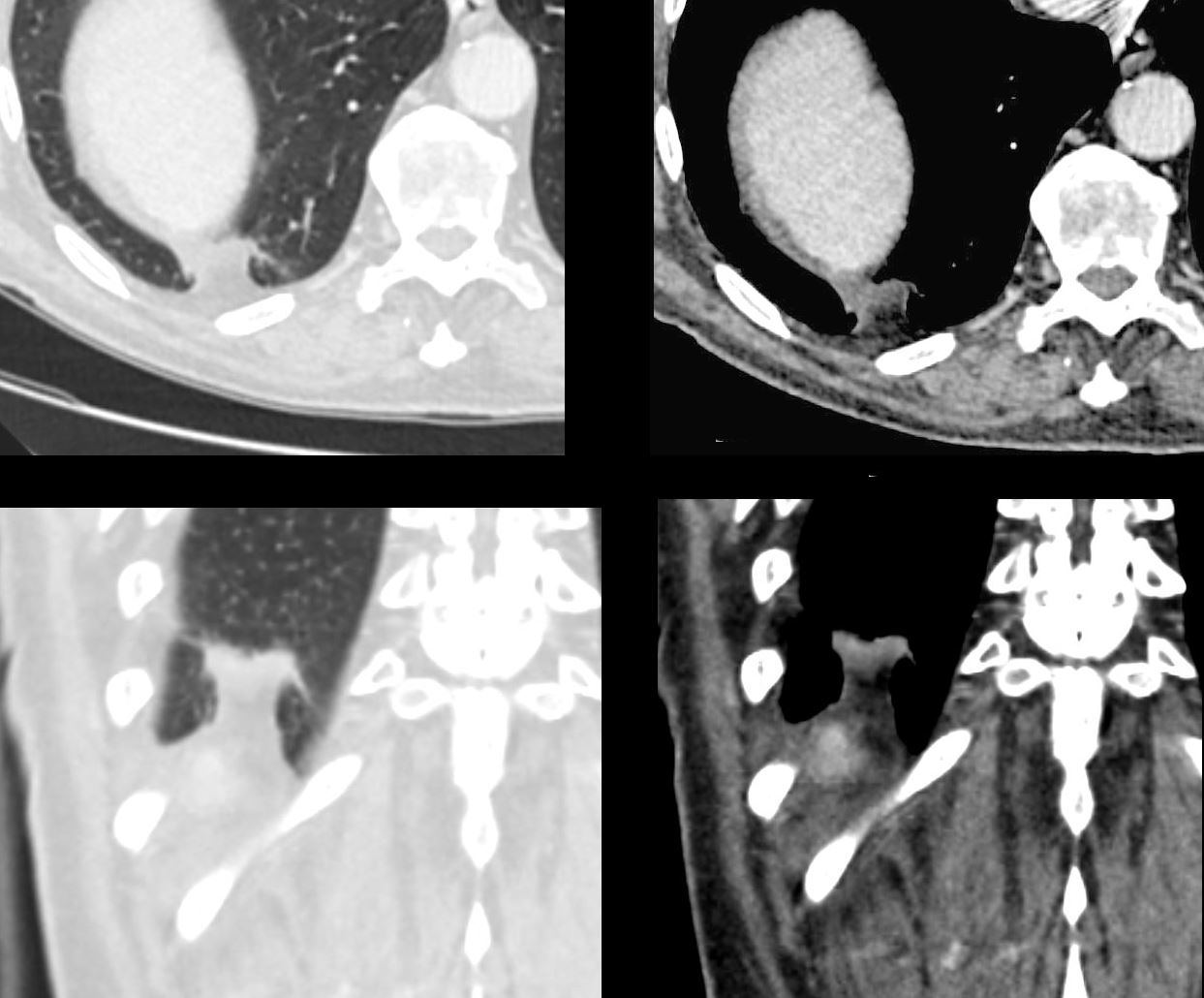
Coronal and sagittal CT reconstructions show a cavitating mass in the superior segment of the right lower lobe (upper images) correlated with axial images (lower panel)Ashley Davidoff MD TheCommonVein.net 176Lu 136737 B.A
Coronal and sagittal CT reconstructions show a cavitating mass in the superior segment of the right lower lobe (upper images) correlated with axial images (lower panel)Ashley Davidoff MD TheCommonVein.net 176Lu 136737 B.A
cavity (lungs)
132575.8bL
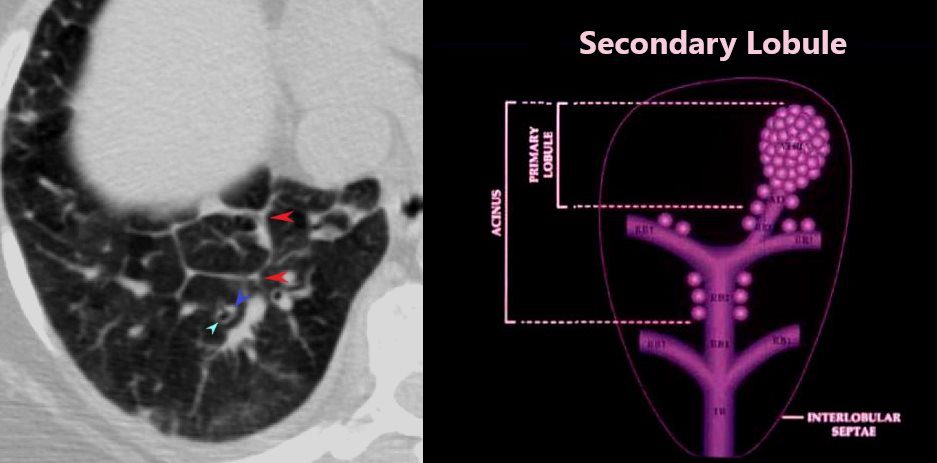
CT above shows a secondary lobule which is the smallest identifiable unit of the lung (made up of around 30 a0cni supplied by a common distal bronchiole and pulmonary artery)and its boundaries can be visualized by assessing the interlobular speta (red arrows)Ashley Davidoff MD TheCommonVein.net B.A
CT above shows a secondary lobule which is the smallest identifiable unit of the lung (made up of around 30 a0cni supplied by a common distal bronchiole and pulmonary artery)and its boundaries can be visualized by assessing the interlobular speta (red arrows)Ashley Davidoff MD TheCommonVein.net B.A
centrilobular (secondary lobule)
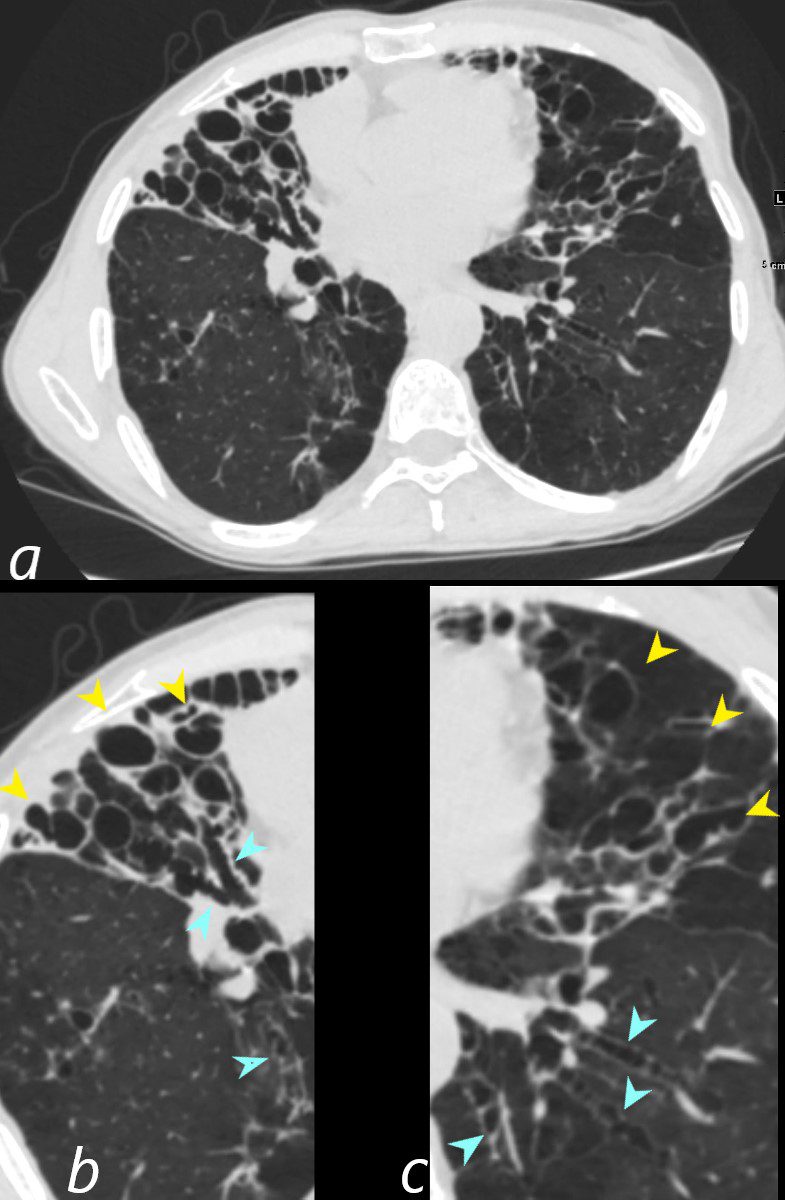
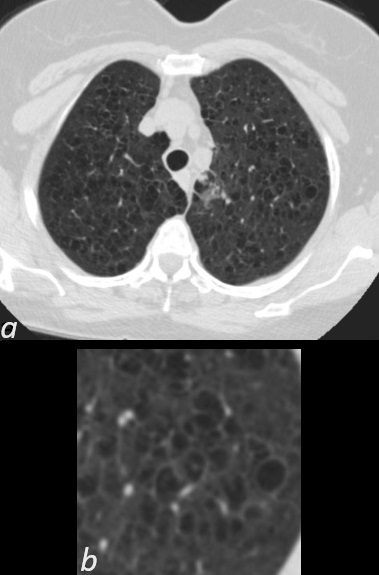
Centrilobular Emphysema in the Upper Lobes of the LungsAxial CT (a) with magnified view of the upper lobes of a 66year female with centrilobular emphysema shows an expanded lobule with a centrilobular vessel in the middle characteristic of centrilobular emphysemaAshley Davidoff MD TheCommonvein.net RnD B.A
Centrilobular Emphysema in the Upper Lobes of the LungsAxial CT (a) with magnified view of the upper lobes of a 66year female with centrilobular emphysema shows an expanded lobule with a centrilobular vessel in the middle characteristic of centrilobular emphysemaAshley Davidoff MD TheCommonvein.net RnD B.A
centrilobular emphysema
Lingular Pneumonia52 year old male presents with a cough and feverCT scan in the axial plane shows a lingular consolidation with air bronchograms and a positive silhouette sign. Both the superior and inferior lingular segments are involvedAshley Davidoff MD TheCommonVein.net135190 B.A
Lingular Pneumonia52 year old male presents with a cough and feverCT scan in the axial plane shows a lingular consolidation with air bronchograms and a positive silhouette sign. Both the superior and inferior lingular segments are involvedAshley Davidoff MD TheCommonVein.net135190 B.A
consolidation in the lungs
CT shows alveolar proteinosis- central distribution which is characterized by diffuse bilateral ground-glass opacities involving both the upper and lower lobes Ashley DavidoffTheCommonVein.net117513 B.A
CT shows alveolar proteinosis- central distribution which is characterized by diffuse bilateral ground-glass opacities involving both the upper and lower lobes Ashley DavidoffTheCommonVein.net117513 B.A
consolidation in the lungs
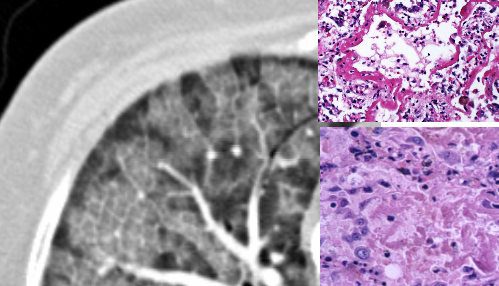
CT above shows the pathologic cryptogenic organizing pneumonia (COP) which is characterized by bilateral and asymmetrical ground-glass opacities and areas of consolidation that can overlap with the ground glass opacities Ashley Davidoff MD TheCommonVein.netlungs-COP-005-path-52f-CT B.A
CT above shows the pathologic cryptogenic organizing pneumonia (COP) which is characterized by bilateral and asymmetrical ground-glass opacities and areas of consolidation that can overlap with the ground glass opacities Ashley Davidoff MD TheCommonVein.netlungs-COP-005-path-52f-CT B.A
cryptogenic organizing pneumonia (COP)
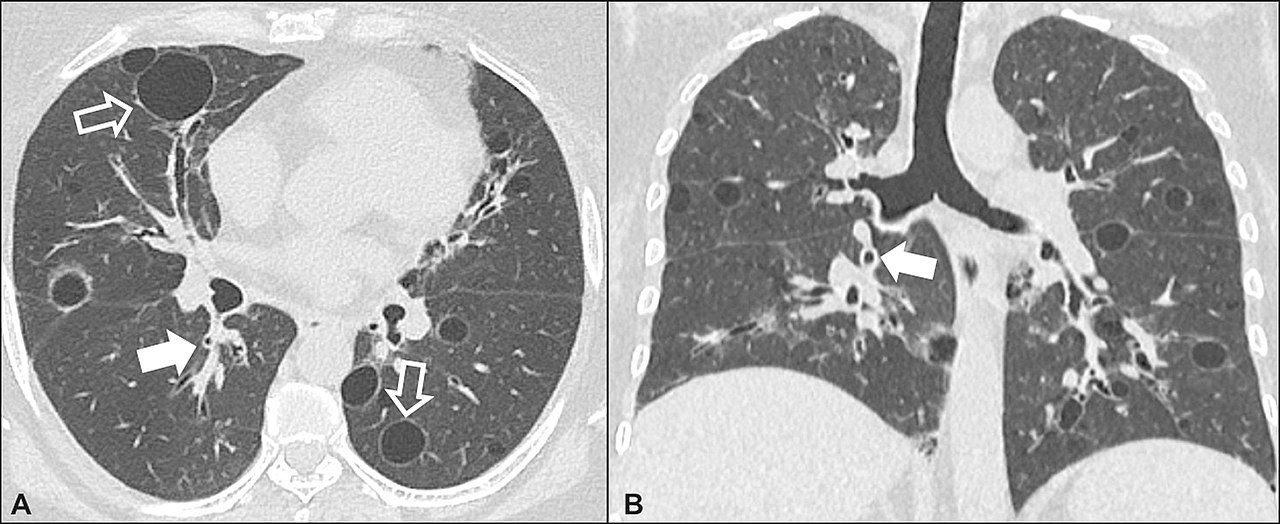
A 62-year-old female patient with Sjögren?s syndrome. Axial high-resolution computed tomography scan of the chest (A) and coronal reformatting (B). In A, diffuse thickening of the bronchial walls (closed arrows), some ground-glass opacities and thin-walled cysts of varying sizes, with a diffuse, bilateral distribution (open arrows). In B, distribution predominantly in the lower fields.Daniel Simões Oliveira et alRadiologia Brasileira 51 (5): 321?327. web-lungs-0013.jpg B.A
A 62-year-old female patient with Sjögren?s syndrome. Axial high-resolution computed tomography scan of the chest (A) and coronal reformatting (B). In A, diffuse thickening of the bronchial walls (closed arrows), some ground-glass opacities and thin-walled cysts of varying sizes, with a diffuse, bilateral distribution (open arrows). In B, distribution predominantly in the lower fields.Daniel Simões Oliveira et alweb-lungs-0013.jpg B.A
cyst in the lungs
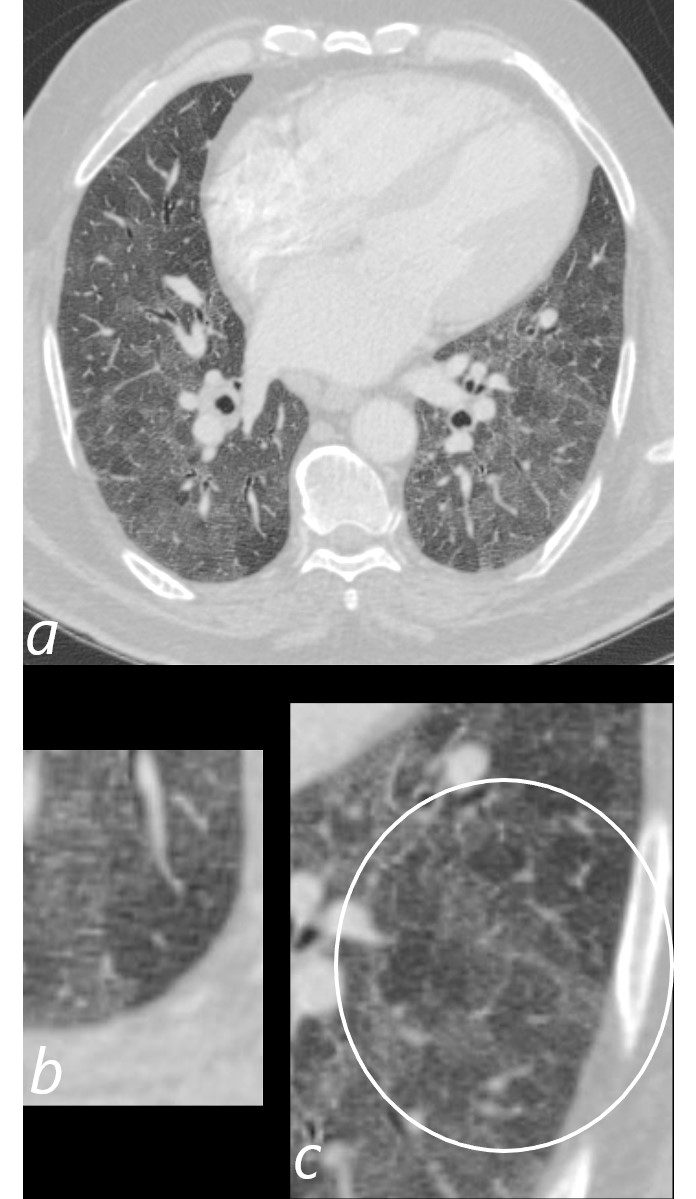
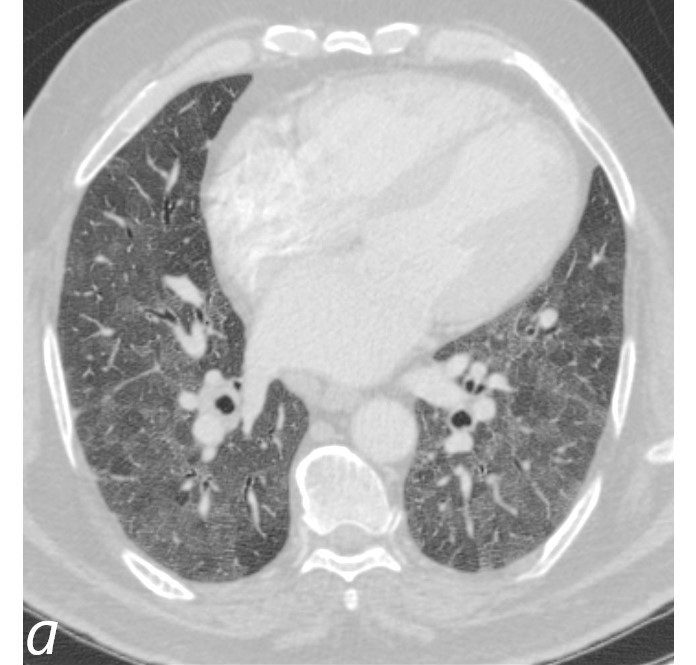
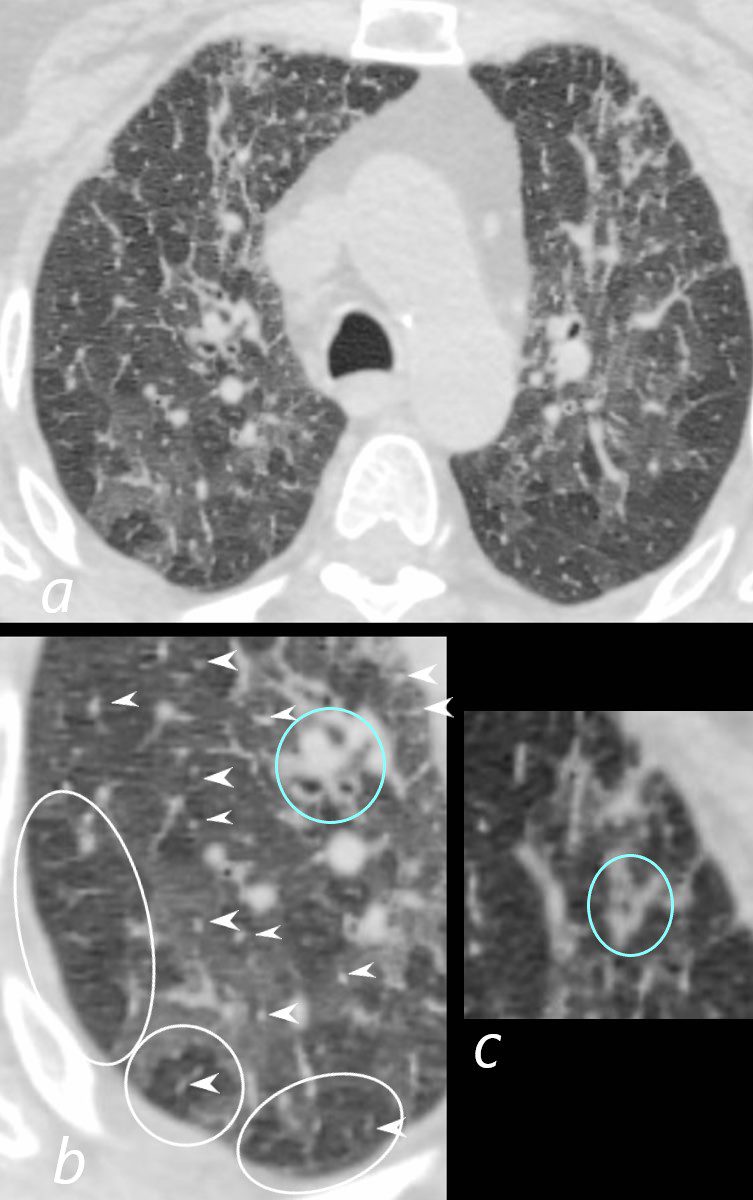
Axial CT through the lower lung fields at the level of the left atrium shows desquamative interstitial pneumonia (DIP) which is characterized by diffuse ground glass changes with more prominent heterogeneity (b and c). Some of secondary lobules are expanded, with some with slightly thickened septa and prominent centrilobular nodules likely indicating small airway involvement (c, white ring).Ashley Davidoff MD TheCommonVein.net 253Lu 136008 B.A
Axial CT through the lower lung fields at the level of the left atrium shows desquamative interstitial pneumonia (DIP) which is characterized by diffuse ground glass changes with more prominent heterogeneity (b and c). Some of secondary lobules are expanded, with some with slightly thickened septa and prominent centrilobular nodules likely indicating small airway involvement (c, white ring).
Ashley Davidoff MD TheCommonVein.net 253Lu 136008 B.A
desquamative interstitial pneumonia (DIP)
CHF – Alveolar EdemaCT scan shows Diffuse ground glass pattern with thickening of the interlobular septa and manifesting as crazy paving patternAshley Davidoff MD TheCommonVein.net 131742 B.A
CHF – Alveolar Edema
CT scan shows Diffuse ground glass pattern with thickening of the interlobular septa and manifesting as crazy paving pattern
Ashley Davidoff MD TheCommonVein.net 131742cL B.A
diffuse alveolar damage (DAD)
Position of DiseaseSubpleural SparingAshley Davidoff MD TheCommonvein.net lungs-0775 0775-lo res subpleural sparing
diffuse lung changes
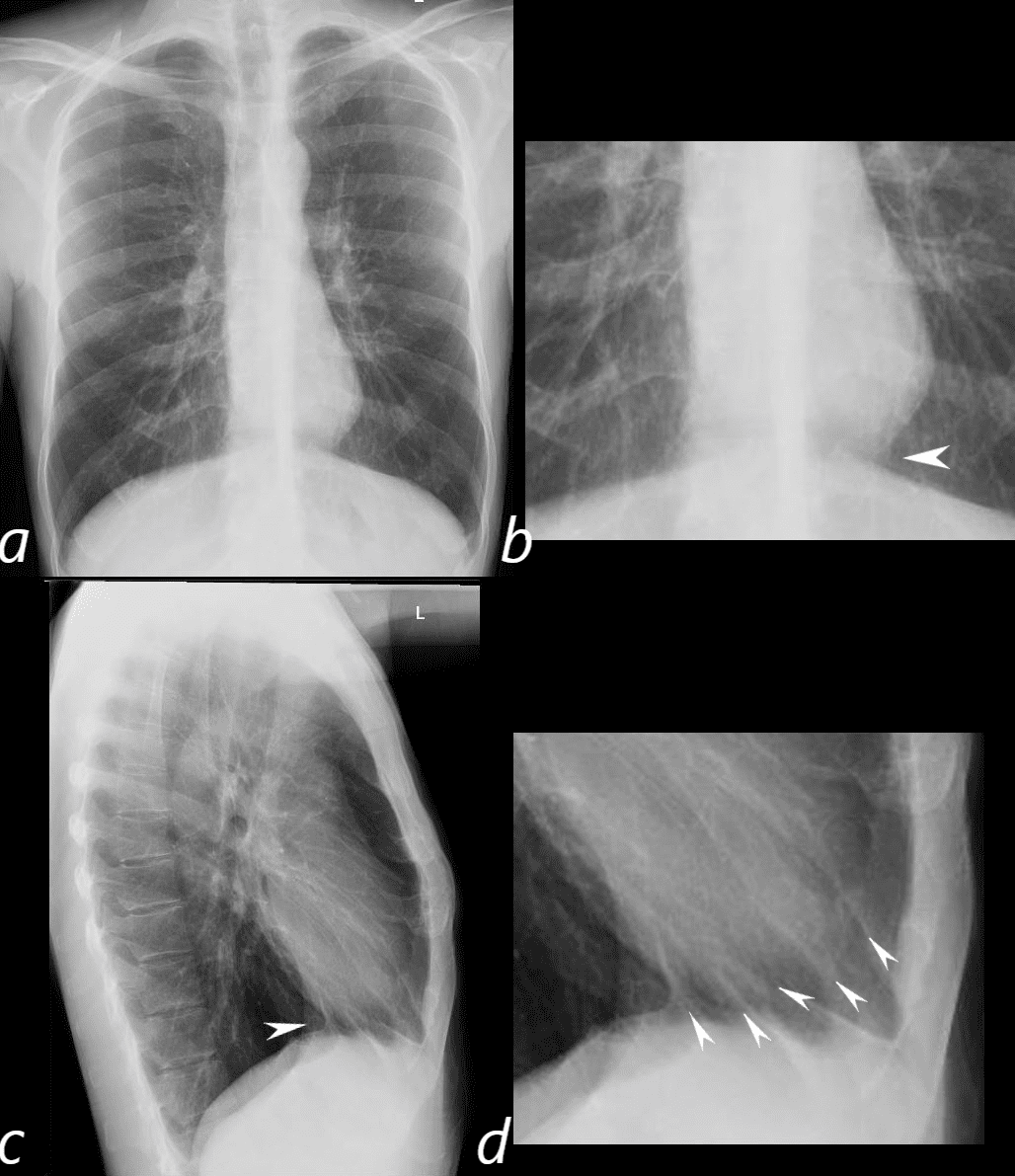
CXR Emphysema and Small Heart58-year-old male presents with dyspnea. The lungs are hyperinflated with flattening of the diaphragms and increase in the retrosternal space on the lateral examination. The person also has an asthenic build with a relatively straight back and narrow A-P dimension. Frontal CXR shows a small heart with structures of the heart visualized to the right of the midline caused by compression of the low-pressure right atrium. The increased in the retrosternal airspace also compresses the relatively low pressure anteriorly positioned right ventricle. The heart is also lifted off the diaphragm (band c white arrowheads) and results in juxtaphrenic lung markings and peaks below the heart (d, arrowheads)Ashley Davidoff MD TheCommonVein.net 136232c01L B.A
CXR Emphysema and Small Heart58-year-old male presents with dyspnea. The lungs are hyperinflated with flattening of the diaphragms and increase in the retrosternal space on the lateral examination. The person also has an asthenic build with a relatively straight back and narrow A-P dimension. Frontal CXR shows a small heart with structures of the heart visualized to the right of the midline caused by compression of the low-pressure right atrium. The increased in the retrosternal airspace also compresses the relatively low pressure anteriorly positioned right ventricle. The heart is also lifted off the diaphragm (band c white arrowheads) and results in juxtaphrenic lung markings and peaks below the heart (d, arrowheads)Ashley Davidoff MD TheCommonVein.net 136232c01L B.A
emphysema
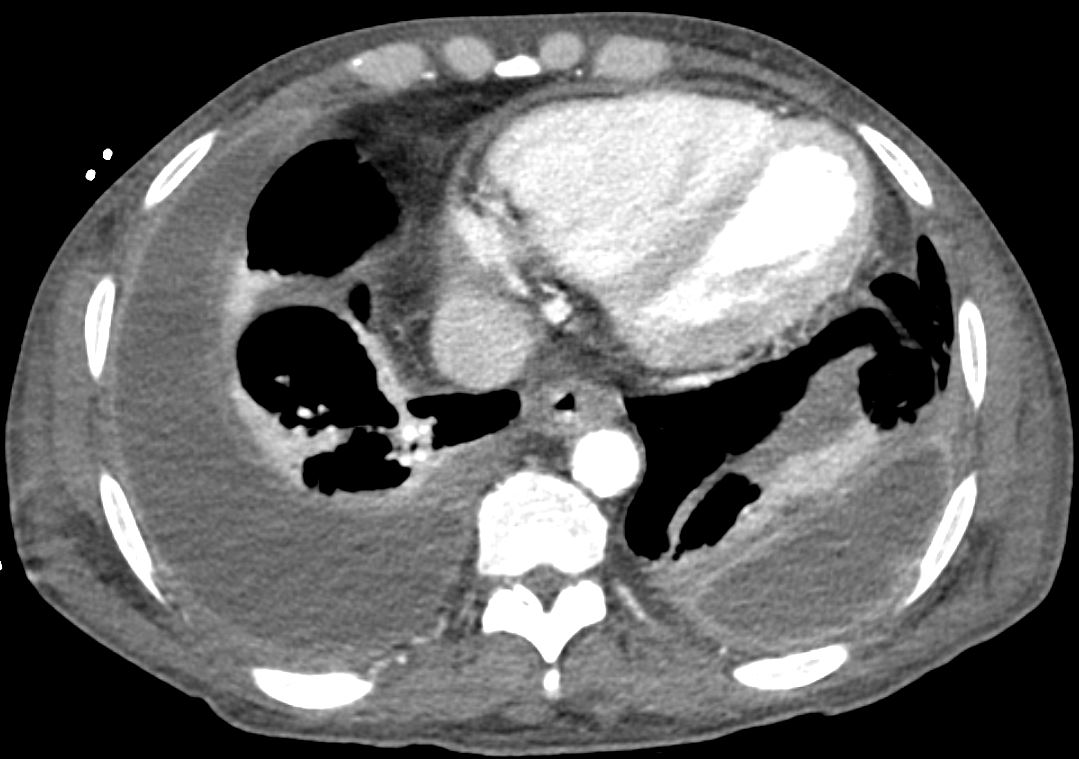
Axial CT scan with contrast shows bilateral complex and loculated effusions with thickened enhancing pleura. Ashley Davidoff MD TheCommonVein.net 135684 B.A
Axial CT scan with contrast shows bilateral complex and loculated effusions with thickened enhancing pleura.
Ashley Davidoff MD TheCommonVein.net 135684cL B.A
empyema
CT in the axial plane shows an obstructing lesion in the left mainstem bronchus of the lung (green arrowhead) with post obstructive atelectasis of the lingula (black arrowhead) and a small portion of left upper lobe anteriorly (white arrowhead). The major fissure is displaced anteriorly.Ashley Davidoff MD TheCommonVein.net 257Lu 136110cL B.A
CT in the axial plane shows an obstructing lesion in the left mainstem bronchus of the lung (green arrowhead) with post obstructive atelectasis of the lingula (black arrowhead) and a small portion of left upper lobe anteriorly (white arrowhead). The major fissure is displaced anteriorly.Ashley Davidoff MD TheCommonVein.net 257Lu 136110cL B.A
endobronchial finding
CT Extra-Pleural Fat SignCT shows extra fat sign which is characterized by focal subsegmental area of atelectasis in the right lower lobe abutting the diaphragm associated with extra pleural fat proliferation secondary to the parenchymal infiltrate.Ashley Davidoff MD TheCommonVein.net 136036c B.A
CT Extra-Pleural Fat SignCT shows extra fat sign which is characterized by focal subsegmental area of atelectasis in the right lower lobe abutting the diaphragm associated with extra pleural fat proliferation secondary to the parenchymal infiltrate.Ashley Davidoff MD TheCommonVein.net 136036c B.A
extrapleural finding (fat sign)
This CT shows fissural nodules which are usually benign round masses with well-defined margins that usually appear within fissural lines (yellow around)Ashley Davidoff MD TheCommonVein.net136201cL01 B.A
1
This CT shows fissural nodules which are usually benign round masses with well-defined margins that usually appear within fissural lines (yellow around)Ashley Davidoff MD TheCommonVein.net136201cL01 B.A
fissural (nodules)
fissures
fissuresL
fissures
focal lung finding
Axial CT of the chest at the level of the aortic arch shows ollicular bronchiolitis (BALT) which is characterized by centrilobular nodules, ground-glass opacities and bronchial wall thickening. Ashley Davidoff MD TheCommonVein.net 132Lu 136652 B.A
Axial CT of the chest at the level of the aortic arch shows ollicular bronchiolitis (BALT) which is characterized by centrilobular nodules, ground-glass opacities and bronchial wall thickening. Ashley Davidoff MD TheCommonVein.net 132Lu 136652 B.A
follicular bronchiolitis (BALT)
geographic changes (lungs)
This CT shows a ground glass nodule in the lung which is characterized by a small round hazy opacity that are usually less than 3cm in size (yellow arrows)Ashley Davidoff MD TheCommonVein.net29787L B.A
This CT shows a ground glass nodule in the lung which is characterized by a small round hazy opacity that are usually less than 3cm in size (yellow arrows)Ashley Davidoff MD TheCommonVein.net29787cL B.A
ground glass nodule in the lungs
This shows diffuse ground glass opacities involving the upper lobes and lower lobes. A finding commonly seen in patients with sarcoidosis Ashley Davidoff MD TheCommonVein.net 029Lu 29064a002.8 B.A.
CT shows diffuse ground glass opacities involving the upper lobes and lower lobes. A finding commonly seen in patients with sarcoidosis Ashley Davidoff MD TheCommonVein.net 029Lu 29064a002.8 B.A
ground glass opacity (GGO)
28-M-Normal-CXR-001L
28-M-Normal-CXR-001L02
hilum
134902-lungs-UIP
134902-lungs-UIPL
honeycomb lung
idiopathic pulmonary fibrosis IPF (UIP radiologic equivalent?)
incomplete fissure
135180.bronchopneumonia
135180.bronchopneumoniac
infiltrate lungs (see opacity)
47152c02
47152c01e
interlobular septum
interstitial fibrosis (combined with UIP, ILD)
82-ILD-honeycomb-006-3-years-later
82-ILD-honeycomb-006-3-years-latercL
interstitial lung disease
interstitium
28-M-Normal-CXR-001L04
28-M-Normal-CXR-001L04
left paratracheal stripe
cancer-poorly-differentiated-adebocarcinoma-66f
cancer-poorly-differentiated-adebocarcinoma-66fL
lobulation
Lymphsadenopathy-low-demsity-TB-04-CT-5-years-ago
Lymphsadenopathy-low-demsity-TB-04-CT-5-years-agoL
low density lymphadenopathy (LAD)
32682n01n.800_2
lymph nodes of the chest: superior mediastinal nodes
32682n07n.800_2
lymph nodes of the chest: aortic nodes
32682n06n.800_2
lymph nodes of the chest: inferior mediastinal nodes
135804
135804c
lymphadenopathy in the chest (LAD)
lungs-large-adenocarcinoma-necrosis-001-53m-CXR
lungs-large-adenocarcinoma-necrosis-001-53m-CXRcL
mass in the lung
heart-membranous-VSD-000b-37F-CXR-normal_L
heart-membranous-VSD-000b-37F-CXR-normal_L02
mediastinal compartments
42260bb01
mediastinum
131745.8L
131745.8L02
micronodules lungs
136197
136197cL
miliary nodular pattern
web-lungs-0011
mosaic attenuation pattern
heart-SLE-congestive-cardiomyopathy-mitral-regurgitation-002-CT-mucoid-impaction-40F_L
mucoid impaction lungs
multifocal lung finding
20760c
20760c
mycetoma fungal mass
web-lungs-0161b
web-lungs-0161b_c
nodular pattern in the lungs
72-m-lung-screen-ca-02-currentc
72-m-lung-screen-ca-02-currentcL
nodule lung
nodules interlobular septum lungs (CT)
136607
136607L
nonspecific interstitial pneumonia (NSIP)
60-M-scleroderma-NSIP-006
60-M-scleroderma-NSIP-006L
nonspecific interstitial pneumonia (NSIP) cellular form
136669c
136669c
obliterative bronchiolitis
web-lungs-0074
web-lungs-0074
oligemia lungs
opacity lungs
lung-COVID-Organizing-pneumonia-53M-013_OP
lung-COVID-Organizing-pneumonia-53M-013_OP_L
organizing pneumonia (OP)
116533.panlobular-emphysema-alpha-1-antitrypsin
panlobular emphysema
parenchyma of lung
134273L
134273L
peribronchovascular finding
peribronchovascular interstitium
136202cl_03
136202cL_02
perilymphatic
33679c04.8c
33679c04.8c
pleura (anatomy)
132135
132135.8L
pleura-based finding
136550c_effusion
136550c.lungs-small-pleural-effusion
pleural effusion
42016c01
42016c01L
pleural plaque
134375b01L
134375b01cL
pleural tag (CT)
chest-lungs-pneumomedistinum-001-CXR-trauma_c
chest-lungs-pneumomedistinum-001-CXR-trauma_cL
pneumomediastinum
130900c.8
130900c.8L
pneumonia
b11431-004
b11431-004L
pneumonitis
130979.8
130979.8c
pneumopericardium
46709c02_e
46709c02
pneumothorax
lung-cancer-adenocarcinoma-pseudocavitation-001-CT-000L
lung-cancer-adenocarcinoma-pseudocavitation-001-CT
pseudocavity lungs
pulmonary blood flow redistribution
COPD-Pulmonary-Fibrosis-65-003
pulmonary fibrosis
131475.8
Lungs-P-0137
pulmonary infarct
neo_interstitial_emphysema
neo_interstitial_emphysema
pulmonary interstitial emphysema
66M-Langerhans-017-CT-micronodules
66M-Langerhans-017-CT-micronodulescL
random micronodules lungs
web-lungs-298
web-lungs-298cL
respiratory bronchiolitis ILD
135741c05
135741c05c
reticular pattern lungs
131990.8
reticulonodular pattern lungs
28-M-Normal-CXR-001L03
28-M-Normal-CXR-001L03
right paratracheal stripe
118433
118433c
rounded atelectasis (CT)
lung-72-M-saber-trachea-001L
lung-72-M-saber-trachea-001cL
saber-sheath trachea
lungs-0785-lo-res-secondary-lobule.jpg
secondary lobule
32686b05L
segment of lung
118433
segmental atelectasis
bronchus-segmental-normal
bronchus-segmental-normalL
segmental bronchi
lungs-large-adenocarcinoma-necrosis-001-53m-CXR
lungs-large-adenocarcinoma-necrosis-001-53m-CXRcL
solid lung mass
rad-det-63-f-LLL-nodule-001-CXR
rad-det-63-f-LLL-nodule-001-CXRcL
solitary pulmonary nodule
31828L
31828cL
spiculated lung lesion (CT)
83063c.8L
83063c.8L
subpleural bands parenchymal bands
132089.8L
132089.8cL
subpleural changes (nodules)
30602b01L02
30602b01L_subsegmental
subsegmental bronchi
42106b
42106c04
tension pneumothorax
tracheobronchomalacia_insp_exp
tracheobronchomalacia_insp_expL
tracheomalacia,
136079
136079cL
tree-in-bud appearance (CT)
web-lungs-0166
web-lungs-0166L
usual interstitial pneumonia (UIP)
reticulation-70-male-uip-001-cxr
reticulation-70-male-uip-001-cxrL
usual interstitial pneumonia (UIP) (CXR)
75679c02
75679c03
carcinoid
135684
135684cL
split pleura sign
135925lungs-inhalational-pneumoniis-crazy-paving
crazy paving
RUL
Right upper lobe
RML
Right middle lobe
RLL
Right lower lobe
LUL
Left upper lobe
LLL
Left lower lobe
web-lungs-0069
web-lungs-0069L
signet ring sign
135184.ligular-pneumonia-silhouette
135184L
silhouette sign (lingular PNA)
42073b02
42073b02L
alveolar pattern (edema/batwing)
135865
135865
halo
47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago
lymphocytic interstitial pneumonia
bronchomalacia
pulmonary embolism
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
image number
image 2
Title
CT Emphysema, Paraseptal Emphysematous Changes Bilateral Lower Lobes65-year-old male with emphysema of the lungs presents with a cough, fever and leukocytosis. CT in the axial plane shows bibasilar paraseptal emphysematous changes and centrilobular changes in the lingula and RUL. Hyperinflation with resultant small heart is noted.Ashley Davidoff MD TheCommonVein.net 259Lu 117504
bleb
Axial CT – Lady Windermere Syndrome61-year-old male with a history of treated mycobacterial infections including MAC and chronic cough.Axial CT at the level of the mid to lower chest shows mildly ectatic segmental airways to the lower, and middle lobe bronchi but significant bronchiectasis to the middle lobe and lingula involving the subsegmental airways. There is a relative paucity of mucus in the ectatic airways. The history of MAC and the distribution of the bronchiectasis in the middle lobe and lingula are reminiscent of the diagnosis of Lady Windermere syndromeAshley Davidoff MD TheCommonVein.net 250Lu 135876
Axial CT – Lady Windermere Syndrome61-year-old male with a history of treated mycobacterial infections including MAC and chronic cough.Axial CT at the level of the mid to lower chest shows mildly ectatic segmental airways to the lower, and middle lobe bronchi but significant bronchiectasis to the middle lobe and lingula involving the subsegmental airways. There is a relative paucity of mucus in the ectatic airways. The history of MAC and the distribution of the bronchiectasis in the middle lobe and lingula are reminiscent of the diagnosis of Lady Windermere syndromeAshley Davidoff MD TheCommonVein.net 250Lu 135876
bronchiectasis
136598c
Fibrotic NSIP59-year-old male presents with history of scleroderma, Raynaud’s disease, and ILDUpper ImageAxial CT shows bibasilar ground glass, bronchiectasis, and bronchiolectasis with volume loss and with crowding of the bronchovascular bundles posteriorly. There is subpleural sparing. Note air-fluid level in the distended esophagus.The lower image focuses on the peripheral sparing. The spared secondary lobules have also undergone enlargement secondary to the fibrotic processAshley Davidoff MD TheCommonVein.net 110Lu 136598c01
136598c
Fibrotic NSIP59-year-old male presents with history of scleroderma, Raynaud’s disease, and ILDUpper ImageAxial CT shows bibasilar peripheral reticular changes, ground glass, bronchiectasis, and bronchiolectasis with volume and with crowding of the bronchovascular bundles posteriorly. There is subpleural sparing posteriorly. Note air-fluid level in the distended esophagus.Lower ImageThe lower image focuses on the traction bronchiectasis caused by the fibrotic processAshley Davidoff MD TheCommonVein.net 110Lu 136598c
bronchiolectasis
Chest CT above shows bronchiolitis which is characterized by peribronchial thickening which is thickening of the small airways of lung (yellow arrows)Ashley Davidoff MD TheCommonVein.net 81F-bronchiolitis-infection-inflammation-004
Chest CT above shows bronchiolitis which is characterized by peribronchial thickening which is thickening of the small airways of lung (yellow arrows)Ashley Davidoff MD TheCommonVein.net 81F-bronchiolitis-infection-inflammation-004
bronchiolitis
Frontal and Lateral CXR shows follicular bronchiolitis which is characterized by a coarsened nodular interstitial pattern. Ashley Davidoff MD TheCommonVein.net 132Lu 136650c B.A
Frontal and Lateral CXR shows follicular bronchiolitis which is characterized by a coarsened nodular interstitial pattern. Ashley Davidoff MD TheCommonVein.net 132Lu 136650c B.A
bronchiolitis (CXR)
Finger in Glove Sign19 year old female with cystic fibrosis and bronchiectasisCT scan through the upper lung fields shows mucin filled subsegmental bronchi of the right upper lobe with morphology reminiscent of the “finger in glove” signCourtesy Priscilla Slanetz MD MPH TheCommonVein.net 31966 B.A
Finger in Glove Sign
19 year old female with cystic fibrosis and bronchiectasis
CT scan through the upper lung fields shows mucin filled subsegmental bronchi of the right upper lobe with morphology reminiscent of the “finger in glove” sign (point to by yellow arrows)
Courtesy Priscilla Slanetz MD MPH TheCommonVein.net31966cl B.A
bronchocele
bronchocentric
bronchocentric
CT in the axial plane shows a bilobed calcified broncholith in the lateral segment of the middle lobe (c, d white arrowheads) with post obstructive atelectasis (c, blue arrowhead)Ashley Davidoff MD TheCommonVein.net 136585cL B.A
1
CT in the axial plane shows a bilobed calcified broncholith in the lateral segment of the middle lobe (c, d white arrowheads) with post obstructive atelectasis (c, blue arrowhead)
Ashley Davidoff MD TheCommonVein.net 136585cL B.A
broncholith
CT Scan Bilateral Apical Builla Centrilobular EmphysemaCT scan in the axial plane shows bilateral apical bullous lung disease, most commonly seen in emphysema Ashley Davidoff MD TheCommonVein.Net 136440 B.A
CT Scan Bilateral Apical Builla Centrilobular Emphysema
CT scan in the axial plane shows bilateral apical bullous lung disease, most commonly seen in emphysema
Ashley Davidoff MD TheCommonVein.Net 136440 B.A
bulla
CT Scan Bilateral Apical Bulla Centrilobular EmphysemaCT scan in the coronal plane shows bilateral apical bullous lung disease, magnified in the lower imageAshley Davidoff MD TheCommonVein.Net 136439c B.A
CT scan in the coronal plane of shows bilateral apical bullous lung disease, magnified in the lower imageAshley Davidoff MD TheCommonVein.Net 136439c B.A
bullous emphysema
Coronal and sagittal CT reconstructions show a cavitating mass in the superior segment of the right lower lobe (upper images) correlated with axial images (lower panel)Ashley Davidoff MD TheCommonVein.net 176Lu 136737 B.A
Coronal and sagittal CT reconstructions show a cavitating mass in the superior segment of the right lower lobe (upper images) correlated with axial images (lower panel)Ashley Davidoff MD TheCommonVein.net 176Lu 136737 B.A
cavity (lungs)
132575.8bL
CT above shows a secondary lobule which is the smallest identifiable unit of the lung (made up of around 30 a0cni supplied by a common distal bronchiole and pulmonary artery)and its boundaries can be visualized by assessing the interlobular speta (red arrows)Ashley Davidoff MD TheCommonVein.net B.A
CT above shows a secondary lobule which is the smallest identifiable unit of the lung (made up of around 30 a0cni supplied by a common distal bronchiole and pulmonary artery)and its boundaries can be visualized by assessing the interlobular speta (red arrows)Ashley Davidoff MD TheCommonVein.net B.A
centrilobular (secondary lobule)
Centrilobular Emphysema in the Upper Lobes of the LungsAxial CT (a) with magnified view of the upper lobes of a 66year female with centrilobular emphysema shows an expanded lobule with a centrilobular vessel in the middle characteristic of centrilobular emphysemaAshley Davidoff MD TheCommonvein.net RnD B.A
Centrilobular Emphysema in the Upper Lobes of the LungsAxial CT (a) with magnified view of the upper lobes of a 66year female with centrilobular emphysema shows an expanded lobule with a centrilobular vessel in the middle characteristic of centrilobular emphysemaAshley Davidoff MD TheCommonvein.net RnD B.A
centrilobular emphysema
Lingular Pneumonia52 year old male presents with a cough and feverCT scan in the axial plane shows a lingular consolidation with air bronchograms and a positive silhouette sign. Both the superior and inferior lingular segments are involvedAshley Davidoff MD TheCommonVein.net135190 B.A
Lingular Pneumonia52 year old male presents with a cough and feverCT scan in the axial plane shows a lingular consolidation with air bronchograms and a positive silhouette sign. Both the superior and inferior lingular segments are involvedAshley Davidoff MD TheCommonVein.net135190 B.A
consolidation in the lungs
CT shows alveolar proteinosis- central distribution which is characterized by diffuse bilateral ground-glass opacities involving both the upper and lower lobes Ashley DavidoffTheCommonVein.net117513 B.A
CT shows alveolar proteinosis- central distribution which is characterized by diffuse bilateral ground-glass opacities involving both the upper and lower lobes Ashley DavidoffTheCommonVein.net117513 B.A
consolidation in the lungs
CT above shows the pathologic cryptogenic organizing pneumonia (COP) which is characterized by bilateral and asymmetrical ground-glass opacities and areas of consolidation that can overlap with the ground glass opacities Ashley Davidoff MD TheCommonVein.netlungs-COP-005-path-52f-CT B.A
CT above shows the pathologic cryptogenic organizing pneumonia (COP) which is characterized by bilateral and asymmetrical ground-glass opacities and areas of consolidation that can overlap with the ground glass opacities Ashley Davidoff MD TheCommonVein.netlungs-COP-005-path-52f-CT B.A
cryptogenic organizing pneumonia (COP)
A 62-year-old female patient with Sjögren?s syndrome. Axial high-resolution computed tomography scan of the chest (A) and coronal reformatting (B). In A, diffuse thickening of the bronchial walls (closed arrows), some ground-glass opacities and thin-walled cysts of varying sizes, with a diffuse, bilateral distribution (open arrows). In B, distribution predominantly in the lower fields.Daniel Simões Oliveira et alRadiologia Brasileira 51 (5): 321?327. web-lungs-0013.jpg B.A
A 62-year-old female patient with Sjögren?s syndrome. Axial high-resolution computed tomography scan of the chest (A) and coronal reformatting (B). In A, diffuse thickening of the bronchial walls (closed arrows), some ground-glass opacities and thin-walled cysts of varying sizes, with a diffuse, bilateral distribution (open arrows). In B, distribution predominantly in the lower fields.Daniel Simões Oliveira et alweb-lungs-0013.jpg B.A
cyst in the lungs
Axial CT through the lower lung fields at the level of the left atrium shows desquamative interstitial pneumonia (DIP) which is characterized by diffuse ground glass changes with more prominent heterogeneity (b and c). Some of secondary lobules are expanded, with some with slightly thickened septa and prominent centrilobular nodules likely indicating small airway involvement (c, white ring).Ashley Davidoff MD TheCommonVein.net 253Lu 136008 B.A
Axial CT through the lower lung fields at the level of the left atrium shows desquamative interstitial pneumonia (DIP) which is characterized by diffuse ground glass changes with more prominent heterogeneity (b and c). Some of secondary lobules are expanded, with some with slightly thickened septa and prominent centrilobular nodules likely indicating small airway involvement (c, white ring).
Ashley Davidoff MD TheCommonVein.net 253Lu 136008 B.A
desquamative interstitial pneumonia (DIP)
CHF – Alveolar EdemaCT scan shows Diffuse ground glass pattern with thickening of the interlobular septa and manifesting as crazy paving patternAshley Davidoff MD TheCommonVein.net 131742 B.A
CHF – Alveolar Edema
CT scan shows Diffuse ground glass pattern with thickening of the interlobular septa and manifesting as crazy paving pattern
Ashley Davidoff MD TheCommonVein.net 131742cL B.A
diffuse alveolar damage (DAD)
Position of DiseaseSubpleural SparingAshley Davidoff MD TheCommonvein.net lungs-0775 0775-lo res subpleural sparing
diffuse lung changes
CXR Emphysema and Small Heart58-year-old male presents with dyspnea. The lungs are hyperinflated with flattening of the diaphragms and increase in the retrosternal space on the lateral examination. The person also has an asthenic build with a relatively straight back and narrow A-P dimension. Frontal CXR shows a small heart with structures of the heart visualized to the right of the midline caused by compression of the low-pressure right atrium. The increased in the retrosternal airspace also compresses the relatively low pressure anteriorly positioned right ventricle. The heart is also lifted off the diaphragm (band c white arrowheads) and results in juxtaphrenic lung markings and peaks below the heart (d, arrowheads)Ashley Davidoff MD TheCommonVein.net 136232c01L B.A
CXR Emphysema and Small Heart58-year-old male presents with dyspnea. The lungs are hyperinflated with flattening of the diaphragms and increase in the retrosternal space on the lateral examination. The person also has an asthenic build with a relatively straight back and narrow A-P dimension. Frontal CXR shows a small heart with structures of the heart visualized to the right of the midline caused by compression of the low-pressure right atrium. The increased in the retrosternal airspace also compresses the relatively low pressure anteriorly positioned right ventricle. The heart is also lifted off the diaphragm (band c white arrowheads) and results in juxtaphrenic lung markings and peaks below the heart (d, arrowheads)Ashley Davidoff MD TheCommonVein.net 136232c01L B.A
emphysema
Axial CT scan with contrast shows bilateral complex and loculated effusions with thickened enhancing pleura. Ashley Davidoff MD TheCommonVein.net 135684 B.A
Axial CT scan with contrast shows bilateral complex and loculated effusions with thickened enhancing pleura.
Ashley Davidoff MD TheCommonVein.net 135684cL B.A
empyema
CT in the axial plane shows an obstructing lesion in the left mainstem bronchus of the lung (green arrowhead) with post obstructive atelectasis of the lingula (black arrowhead) and a small portion of left upper lobe anteriorly (white arrowhead). The major fissure is displaced anteriorly.Ashley Davidoff MD TheCommonVein.net 257Lu 136110cL B.A
CT in the axial plane shows an obstructing lesion in the left mainstem bronchus of the lung (green arrowhead) with post obstructive atelectasis of the lingula (black arrowhead) and a small portion of left upper lobe anteriorly (white arrowhead). The major fissure is displaced anteriorly.Ashley Davidoff MD TheCommonVein.net 257Lu 136110cL B.A
endobronchial finding
CT Extra-Pleural Fat SignCT shows extra fat sign which is characterized by focal subsegmental area of atelectasis in the right lower lobe abutting the diaphragm associated with extra pleural fat proliferation secondary to the parenchymal infiltrate.Ashley Davidoff MD TheCommonVein.net 136036c B.A
CT Extra-Pleural Fat SignCT shows extra fat sign which is characterized by focal subsegmental area of atelectasis in the right lower lobe abutting the diaphragm associated with extra pleural fat proliferation secondary to the parenchymal infiltrate.Ashley Davidoff MD TheCommonVein.net 136036c B.A
extrapleural finding (fat sign)
This CT shows fissural nodules which are usually benign round masses with well-defined margins that usually appear within fissural lines (yellow around)Ashley Davidoff MD TheCommonVein.net136201cL01 B.A
1
This CT shows fissural nodules which are usually benign round masses with well-defined margins that usually appear within fissural lines (yellow around)Ashley Davidoff MD TheCommonVein.net136201cL01 B.A
fissural (nodules)
fissures
fissuresL
fissures
focal lung finding
Axial CT of the chest at the level of the aortic arch shows ollicular bronchiolitis (BALT) which is characterized by centrilobular nodules, ground-glass opacities and bronchial wall thickening. Ashley Davidoff MD TheCommonVein.net 132Lu 136652 B.A
Axial CT of the chest at the level of the aortic arch shows ollicular bronchiolitis (BALT) which is characterized by centrilobular nodules, ground-glass opacities and bronchial wall thickening. Ashley Davidoff MD TheCommonVein.net 132Lu 136652 B.A
follicular bronchiolitis (BALT)
geographic changes (lungs)
This CT shows a ground glass nodule in the lung which is characterized by a small round hazy opacity that are usually less than 3cm in size (yellow arrows)Ashley Davidoff MD TheCommonVein.net29787L B.A
This CT shows a ground glass nodule in the lung which is characterized by a small round hazy opacity that are usually less than 3cm in size (yellow arrows)Ashley Davidoff MD TheCommonVein.net29787cL B.A
ground glass nodule in the lungs
This shows diffuse ground glass opacities involving the upper lobes and lower lobes. A finding commonly seen in patients with sarcoidosis Ashley Davidoff MD TheCommonVein.net 029Lu 29064a002.8 B.A.
CT shows diffuse ground glass opacities involving the upper lobes and lower lobes. A finding commonly seen in patients with sarcoidosis Ashley Davidoff MD TheCommonVein.net 029Lu 29064a002.8 B.A
ground glass opacity (GGO)
28-M-Normal-CXR-001L
28-M-Normal-CXR-001L02
hilum
134902-lungs-UIP
134902-lungs-UIPL
honeycomb lung
idiopathic pulmonary fibrosis IPF (UIP radiologic equivalent?)
incomplete fissure
135180.bronchopneumonia
135180.bronchopneumoniac
infiltrate lungs (see opacity)
47152c02
47152c01e
interlobular septum
interstitial fibrosis (combined with UIP, ILD)
82-ILD-honeycomb-006-3-years-later
82-ILD-honeycomb-006-3-years-latercL
interstitial lung disease
interstitium
28-M-Normal-CXR-001L04
28-M-Normal-CXR-001L04
left paratracheal stripe
cancer-poorly-differentiated-adebocarcinoma-66f
cancer-poorly-differentiated-adebocarcinoma-66fL
lobulation
Lymphsadenopathy-low-demsity-TB-04-CT-5-years-ago
Lymphsadenopathy-low-demsity-TB-04-CT-5-years-agoL
low density lymphadenopathy (LAD)
32682n01n.800_2
lymph nodes of the chest: superior mediastinal nodes
32682n07n.800_2
lymph nodes of the chest: aortic nodes
32682n06n.800_2
lymph nodes of the chest: inferior mediastinal nodes
135804
135804c
lymphadenopathy in the chest (LAD)
lungs-large-adenocarcinoma-necrosis-001-53m-CXR
lungs-large-adenocarcinoma-necrosis-001-53m-CXRcL
mass in the lung
heart-membranous-VSD-000b-37F-CXR-normal_L
heart-membranous-VSD-000b-37F-CXR-normal_L02
mediastinal compartments
42260bb01
mediastinum
131745.8L
131745.8L02
micronodules lungs
136197
136197cL
miliary nodular pattern
web-lungs-0011
mosaic attenuation pattern
heart-SLE-congestive-cardiomyopathy-mitral-regurgitation-002-CT-mucoid-impaction-40F_L
mucoid impaction lungs
multifocal lung finding
20760c
20760c
mycetoma fungal mass
web-lungs-0161b
web-lungs-0161b_c
nodular pattern in the lungs
72-m-lung-screen-ca-02-currentc
72-m-lung-screen-ca-02-currentcL
nodule lung
nodules interlobular septum lungs (CT)
136607
136607L
nonspecific interstitial pneumonia (NSIP)
60-M-scleroderma-NSIP-006
60-M-scleroderma-NSIP-006L
nonspecific interstitial pneumonia (NSIP) cellular form
136669c
136669c
obliterative bronchiolitis
web-lungs-0074
web-lungs-0074
oligemia lungs
opacity lungs
lung-COVID-Organizing-pneumonia-53M-013_OP
lung-COVID-Organizing-pneumonia-53M-013_OP_L
organizing pneumonia (OP)
116533.panlobular-emphysema-alpha-1-antitrypsin
panlobular emphysema
parenchyma of lung
134273L
134273L
peribronchovascular finding
peribronchovascular interstitium
136202cl_03
136202cL_02
perilymphatic
33679c04.8c
33679c04.8c
pleura (anatomy)
132135
132135.8L
pleura-based finding
136550c_effusion
136550c.lungs-small-pleural-effusion
pleural effusion
42016c01
42016c01L
pleural plaque
134375b01L
134375b01cL
pleural tag (CT)
chest-lungs-pneumomedistinum-001-CXR-trauma_c
chest-lungs-pneumomedistinum-001-CXR-trauma_cL
pneumomediastinum
130900c.8
130900c.8L
pneumonia
b11431-004
b11431-004L
pneumonitis
130979.8
130979.8c
pneumopericardium
46709c02_e
46709c02
pneumothorax
lung-cancer-adenocarcinoma-pseudocavitation-001-CT-000L
lung-cancer-adenocarcinoma-pseudocavitation-001-CT
pseudocavity lungs
pulmonary blood flow redistribution
COPD-Pulmonary-Fibrosis-65-003
pulmonary fibrosis
131475.8
Lungs-P-0137
pulmonary infarct
neo_interstitial_emphysema
neo_interstitial_emphysema
pulmonary interstitial emphysema
66M-Langerhans-017-CT-micronodules
66M-Langerhans-017-CT-micronodulescL
random micronodules lungs
web-lungs-298
web-lungs-298cL
respiratory bronchiolitis ILD
135741c05
135741c05c
reticular pattern lungs
131990.8
reticulonodular pattern lungs
28-M-Normal-CXR-001L03
28-M-Normal-CXR-001L03
right paratracheal stripe
118433
118433c
rounded atelectasis (CT)
lung-72-M-saber-trachea-001L
lung-72-M-saber-trachea-001cL
saber-sheath trachea
lungs-0785-lo-res-secondary-lobule.jpg
secondary lobule
32686b05L
segment of lung
118433
segmental atelectasis
bronchus-segmental-normal
bronchus-segmental-normalL
segmental bronchi
lungs-large-adenocarcinoma-necrosis-001-53m-CXR
lungs-large-adenocarcinoma-necrosis-001-53m-CXRcL
solid lung mass
rad-det-63-f-LLL-nodule-001-CXR
rad-det-63-f-LLL-nodule-001-CXRcL
solitary pulmonary nodule
31828L
31828cL
spiculated lung lesion (CT)
83063c.8L
83063c.8L
subpleural bands parenchymal bands
132089.8L
132089.8cL
subpleural changes (nodules)
30602b01L02
30602b01L_subsegmental
subsegmental bronchi
42106b
42106c04
tension pneumothorax
tracheobronchomalacia_insp_exp
tracheobronchomalacia_insp_expL
tracheomalacia,
136079
136079cL
tree-in-bud appearance (CT)
web-lungs-0166
web-lungs-0166L
usual interstitial pneumonia (UIP)
reticulation-70-male-uip-001-cxr
reticulation-70-male-uip-001-cxrL
usual interstitial pneumonia (UIP) (CXR)
75679c02
75679c03
carcinoid
135684
135684cL
split pleura sign
135925lungs-inhalational-pneumoniis-crazy-paving
crazy paving
RUL
Right upper lobe
RML
Right middle lobe
RLL
Right lower lobe
LUL
Left upper lobe
LLL
Left lower lobe
web-lungs-0069
web-lungs-0069L
signet ring sign
135184.ligular-pneumonia-silhouette
135184L
silhouette sign (lingular PNA)
42073b02
42073b02L
alveolar pattern (edema/batwing)
135865
135865
halo
47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago
lymphocytic interstitial pneumonia
bronchomalacia
pulmonary embolism
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pulmonary embolism
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pulmonary embolism
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => bronchomalacia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => bronchomalacia
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => lymphocytic interstitial pneumonia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lymphocytic interstitial pneumonia
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => halo
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => halo
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 135865
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 135865
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 135865
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 135865
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => alveolar pattern (edema/batwing)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => alveolar pattern (edema/batwing)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 42073b02L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 42073b02L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 42073b02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 42073b02
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => silhouette sign (lingular PNA)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => silhouette sign (lingular PNA)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 135184L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 135184L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 135184.ligular-pneumonia-silhouette
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 135184.ligular-pneumonia-silhouette
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => signet ring sign
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => signet ring sign
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => web-lungs-0069L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => web-lungs-0069L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => web-lungs-0069
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => web-lungs-0069
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Left lower lobe
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Left lower lobe
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => LLL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => LLL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Left upper lobe
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Left upper lobe
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => LUL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => LUL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Right lower lobe
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Right lower lobe
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => RLL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => RLL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Right middle lobe
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Right middle lobe
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => RML
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => RML
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Right upper lobe
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Right upper lobe
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => RUL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => RUL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => crazy paving
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => crazy paving
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 135925lungs-inhalational-pneumoniis-crazy-paving
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 135925lungs-inhalational-pneumoniis-crazy-paving
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => split pleura sign
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => split pleura sign
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 135684cL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 135684cL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 135684
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 135684
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => carcinoid
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => carcinoid
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 75679c03
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 75679c03
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 75679c02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 75679c02
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => usual interstitial pneumonia (UIP) (CXR)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => usual interstitial pneumonia (UIP) (CXR)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => reticulation-70-male-uip-001-cxrL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => reticulation-70-male-uip-001-cxrL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => reticulation-70-male-uip-001-cxr
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => reticulation-70-male-uip-001-cxr
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => usual interstitial pneumonia (UIP)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => usual interstitial pneumonia (UIP)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => web-lungs-0166L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => web-lungs-0166L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => web-lungs-0166
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => web-lungs-0166
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => tree-in-bud appearance (CT)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => tree-in-bud appearance (CT)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 136079cL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 136079cL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 136079
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 136079
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => tracheomalacia,
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => tracheomalacia,
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => tracheobronchomalacia_insp_expL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => tracheobronchomalacia_insp_expL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => tracheobronchomalacia_insp_exp
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => tracheobronchomalacia_insp_exp
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => tension pneumothorax
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => tension pneumothorax
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 42106c04
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 42106c04
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 42106b
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 42106b
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => subsegmental bronchi
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => subsegmental bronchi
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 30602b01L_subsegmental
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 30602b01L_subsegmental
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 30602b01L02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 30602b01L02
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => subpleural changes (nodules)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => subpleural changes (nodules)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 132089.8cL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 132089.8cL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 132089.8L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 132089.8L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => subpleural bands parenchymal bands
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => subpleural bands parenchymal bands
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 83063c.8L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 83063c.8L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 83063c.8L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 83063c.8L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => spiculated lung lesion (CT)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => spiculated lung lesion (CT)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 31828cL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 31828cL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 31828L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 31828L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => solitary pulmonary nodule
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => solitary pulmonary nodule
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => rad-det-63-f-LLL-nodule-001-CXRcL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => rad-det-63-f-LLL-nodule-001-CXRcL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => rad-det-63-f-LLL-nodule-001-CXR
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => rad-det-63-f-LLL-nodule-001-CXR
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => solid lung mass
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => solid lung mass
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => lungs-large-adenocarcinoma-necrosis-001-53m-CXRcL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lungs-large-adenocarcinoma-necrosis-001-53m-CXRcL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => lungs-large-adenocarcinoma-necrosis-001-53m-CXR
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lungs-large-adenocarcinoma-necrosis-001-53m-CXR
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => segmental bronchi
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => segmental bronchi
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => bronchus-segmental-normalL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => bronchus-segmental-normalL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => bronchus-segmental-normal
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => bronchus-segmental-normal
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => segmental atelectasis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => segmental atelectasis
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 118433
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 118433
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => segment of lung
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => segment of lung
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 32686b05L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 32686b05L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => secondary lobule
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => secondary lobule
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => lungs-0785-lo-res-secondary-lobule.jpg
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lungs-0785-lo-res-secondary-lobule.jpg
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => saber-sheath trachea
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => saber-sheath trachea
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => lung-72-M-saber-trachea-001cL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lung-72-M-saber-trachea-001cL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => lung-72-M-saber-trachea-001L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lung-72-M-saber-trachea-001L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => rounded atelectasis (CT)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => rounded atelectasis (CT)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 118433c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 118433c
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 118433
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 118433
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => right paratracheal stripe
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => right paratracheal stripe
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 28-M-Normal-CXR-001L03
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 28-M-Normal-CXR-001L03
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 28-M-Normal-CXR-001L03
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 28-M-Normal-CXR-001L03
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => reticulonodular pattern lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => reticulonodular pattern lungs
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 131990.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 131990.8
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => reticular pattern lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => reticular pattern lungs
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 135741c05c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 135741c05c
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 135741c05
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 135741c05
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => respiratory bronchiolitis ILD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => respiratory bronchiolitis ILD
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => web-lungs-298cL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => web-lungs-298cL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => web-lungs-298
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => web-lungs-298
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => random micronodules lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => random micronodules lungs
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 66M-Langerhans-017-CT-micronodulescL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 66M-Langerhans-017-CT-micronodulescL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 66M-Langerhans-017-CT-micronodules
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 66M-Langerhans-017-CT-micronodules
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pulmonary interstitial emphysema
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pulmonary interstitial emphysema
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => neo_interstitial_emphysema
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => neo_interstitial_emphysema
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => neo_interstitial_emphysema
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => neo_interstitial_emphysema
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pulmonary infarct
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pulmonary infarct
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => Lungs-P-0137
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Lungs-P-0137
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 131475.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 131475.8
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pulmonary fibrosis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pulmonary fibrosis
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => COPD-Pulmonary-Fibrosis-65-003
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => COPD-Pulmonary-Fibrosis-65-003
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pulmonary blood flow redistribution
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pulmonary blood flow redistribution
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pseudocavity lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pseudocavity lungs
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => lung-cancer-adenocarcinoma-pseudocavitation-001-CT
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lung-cancer-adenocarcinoma-pseudocavitation-001-CT
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => lung-cancer-adenocarcinoma-pseudocavitation-001-CT-000L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lung-cancer-adenocarcinoma-pseudocavitation-001-CT-000L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pneumothorax
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pneumothorax
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 46709c02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 46709c02
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 46709c02_e
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 46709c02_e
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pneumopericardium
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pneumopericardium
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 130979.8c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 130979.8c
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 130979.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 130979.8
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pneumonitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pneumonitis
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => b11431-004L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => b11431-004L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => b11431-004
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => b11431-004
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pneumonia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pneumonia
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 130900c.8L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 130900c.8L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 130900c.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 130900c.8
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pneumomediastinum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pneumomediastinum
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => chest-lungs-pneumomedistinum-001-CXR-trauma_cL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => chest-lungs-pneumomedistinum-001-CXR-trauma_cL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => chest-lungs-pneumomedistinum-001-CXR-trauma_c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => chest-lungs-pneumomedistinum-001-CXR-trauma_c
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pleural tag (CT)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pleural tag (CT)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 134375b01cL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 134375b01cL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 134375b01L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 134375b01L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pleural plaque
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pleural plaque
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 42016c01L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 42016c01L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 42016c01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 42016c01
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pleural effusion
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pleural effusion
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 136550c.lungs-small-pleural-effusion
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 136550c.lungs-small-pleural-effusion
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 136550c_effusion
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 136550c_effusion
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pleura-based finding
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pleura-based finding
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 132135.8L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 132135.8L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 132135
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 132135
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => pleura (anatomy)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => pleura (anatomy)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 33679c04.8c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 33679c04.8c
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 33679c04.8c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 33679c04.8c
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => perilymphatic
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => perilymphatic
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 136202cL_02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 136202cL_02
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 136202cl_03
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 136202cl_03
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => peribronchovascular interstitium
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => peribronchovascular interstitium
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => peribronchovascular finding
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => peribronchovascular finding
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 134273L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 134273L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 134273L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 134273L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => parenchyma of lung
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => parenchyma of lung
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => panlobular emphysema
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => panlobular emphysema
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 116533.panlobular-emphysema-alpha-1-antitrypsin
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 116533.panlobular-emphysema-alpha-1-antitrypsin
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => organizing pneumonia (OP)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => organizing pneumonia (OP)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => lung-COVID-Organizing-pneumonia-53M-013_OP_L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lung-COVID-Organizing-pneumonia-53M-013_OP_L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => lung-COVID-Organizing-pneumonia-53M-013_OP
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lung-COVID-Organizing-pneumonia-53M-013_OP
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => opacity lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => opacity lungs
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => oligemia lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => oligemia lungs
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => web-lungs-0074
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => web-lungs-0074
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => web-lungs-0074
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => web-lungs-0074
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => obliterative bronchiolitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => obliterative bronchiolitis
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 136669c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 136669c
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 136669c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 136669c
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => nonspecific interstitial pneumonia (NSIP) cellular form
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => nonspecific interstitial pneumonia (NSIP) cellular form
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 60-M-scleroderma-NSIP-006L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 60-M-scleroderma-NSIP-006L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 60-M-scleroderma-NSIP-006
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 60-M-scleroderma-NSIP-006
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => nonspecific interstitial pneumonia (NSIP)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => nonspecific interstitial pneumonia (NSIP)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 136607L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 136607L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 136607
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 136607
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => nodules interlobular septum lungs (CT)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => nodules interlobular septum lungs (CT)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => nodule lung
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => nodule lung
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 72-m-lung-screen-ca-02-currentcL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 72-m-lung-screen-ca-02-currentcL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 72-m-lung-screen-ca-02-currentc
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 72-m-lung-screen-ca-02-currentc
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => nodular pattern in the lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => nodular pattern in the lungs
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => web-lungs-0161b_c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => web-lungs-0161b_c
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => web-lungs-0161b
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => web-lungs-0161b
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => mycetoma fungal mass
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => mycetoma fungal mass
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 20760c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 20760c
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 20760c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 20760c
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => multifocal lung finding
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => multifocal lung finding
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => mucoid impaction lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => mucoid impaction lungs
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => heart-SLE-congestive-cardiomyopathy-mitral-regurgitation-002-CT-mucoid-impaction-40F_L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => heart-SLE-congestive-cardiomyopathy-mitral-regurgitation-002-CT-mucoid-impaction-40F_L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => mosaic attenuation pattern
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => mosaic attenuation pattern
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => web-lungs-0011
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => web-lungs-0011
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => miliary nodular pattern
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => miliary nodular pattern
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 136197cL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 136197cL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 136197
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 136197
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => micronodules lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => micronodules lungs
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 131745.8L02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 131745.8L02
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 131745.8L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 131745.8L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => mediastinum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => mediastinum
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 42260bb01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 42260bb01
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => mediastinal compartments
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => mediastinal compartments
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => heart-membranous-VSD-000b-37F-CXR-normal_L02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => heart-membranous-VSD-000b-37F-CXR-normal_L02
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => heart-membranous-VSD-000b-37F-CXR-normal_L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => heart-membranous-VSD-000b-37F-CXR-normal_L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => mass in the lung
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => mass in the lung
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => lungs-large-adenocarcinoma-necrosis-001-53m-CXRcL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lungs-large-adenocarcinoma-necrosis-001-53m-CXRcL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => lungs-large-adenocarcinoma-necrosis-001-53m-CXR
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lungs-large-adenocarcinoma-necrosis-001-53m-CXR
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => lymphadenopathy in the chest (LAD)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lymphadenopathy in the chest (LAD)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 135804c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 135804c
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 135804
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 135804
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => lymph nodes of the chest: inferior mediastinal nodes
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lymph nodes of the chest: inferior mediastinal nodes
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 32682n06n.800_2
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 32682n06n.800_2
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => lymph nodes of the chest: aortic nodes
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lymph nodes of the chest: aortic nodes
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 32682n07n.800_2
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 32682n07n.800_2
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => lymph nodes of the chest: superior mediastinal nodes
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lymph nodes of the chest: superior mediastinal nodes
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 32682n01n.800_2
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 32682n01n.800_2
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => low density lymphadenopathy (LAD)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => low density lymphadenopathy (LAD)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => Lymphsadenopathy-low-demsity-TB-04-CT-5-years-agoL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Lymphsadenopathy-low-demsity-TB-04-CT-5-years-agoL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => Lymphsadenopathy-low-demsity-TB-04-CT-5-years-ago
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Lymphsadenopathy-low-demsity-TB-04-CT-5-years-ago
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => lobulation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => lobulation
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => cancer-poorly-differentiated-adebocarcinoma-66fL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => cancer-poorly-differentiated-adebocarcinoma-66fL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => cancer-poorly-differentiated-adebocarcinoma-66f
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => cancer-poorly-differentiated-adebocarcinoma-66f
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => left paratracheal stripe
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => left paratracheal stripe
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 28-M-Normal-CXR-001L04
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 28-M-Normal-CXR-001L04
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 28-M-Normal-CXR-001L04
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 28-M-Normal-CXR-001L04
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => interstitium
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => interstitium
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => interstitial lung disease
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => interstitial lung disease
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 82-ILD-honeycomb-006-3-years-latercL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 82-ILD-honeycomb-006-3-years-latercL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 82-ILD-honeycomb-006-3-years-later
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 82-ILD-honeycomb-006-3-years-later
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => interstitial fibrosis (combined with UIP, ILD)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => interstitial fibrosis (combined with UIP, ILD)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => interlobular septum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => interlobular septum
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 47152c01e
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 47152c01e
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 47152c02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 47152c02
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => infiltrate lungs (see opacity)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => infiltrate lungs (see opacity)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 135180.bronchopneumoniac
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 135180.bronchopneumoniac
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 135180.bronchopneumonia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 135180.bronchopneumonia
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => incomplete fissure
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => incomplete fissure
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => idiopathic pulmonary fibrosis IPF (UIP radiologic equivalent?)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => idiopathic pulmonary fibrosis IPF (UIP radiologic equivalent?)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => honeycomb lung
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => honeycomb lung
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 134902-lungs-UIPL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 134902-lungs-UIPL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 134902-lungs-UIP
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 134902-lungs-UIP
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => hilum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => hilum
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 28-M-Normal-CXR-001L02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 28-M-Normal-CXR-001L02
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 28-M-Normal-CXR-001L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 28-M-Normal-CXR-001L
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => ground glass opacity (GGO)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => ground glass opacity (GGO)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT shows diffuse ground glass opacities involving the upper lobes and lower lobes. A finding commonly seen in patients with sarcoidosis Ashley Davidoff MD TheCommonVein.net 029Lu 29064a002.8 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT shows diffuse ground glass opacities involving the upper lobes and lower lobes. A finding commonly seen in patients with sarcoidosis Ashley Davidoff MD TheCommonVein.net 029Lu 29064a002.8 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2020/02/29064a002.8.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
This shows diffuse ground glass opacities involving the upper lobes and lower lobes. A finding commonly seen in patients with sarcoidosis Ashley Davidoff MD TheCommonVein.net 029Lu 29064a002.8 B.A.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This shows diffuse ground glass opacities involving the upper lobes and lower lobes. A finding commonly seen in patients with sarcoidosis Ashley Davidoff MD TheCommonVein.net 029Lu 29064a002.8 B.A.
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2020/02/29064a002.8.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => ground glass nodule in the lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => ground glass nodule in the lungs
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => This CT shows a ground glass nodule in the lung which is characterized by a small round hazy opacity that are usually less than 3cm in size (yellow arrows)Ashley Davidoff MD TheCommonVein.net29787cL B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This CT shows a ground glass nodule in the lung which is characterized by a small round hazy opacity that are usually less than 3cm in size (yellow arrows)Ashley Davidoff MD TheCommonVein.net29787cL B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/11/29787cL-1.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
This CT shows a ground glass nodule in the lung which is characterized by a small round hazy opacity that are usually less than 3cm in size (yellow arrows)Ashley Davidoff MD TheCommonVein.net29787L B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This CT shows a ground glass nodule in the lung which is characterized by a small round hazy opacity that are usually less than 3cm in size (yellow arrows)Ashley Davidoff MD TheCommonVein.net29787L B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/11/29787L-1.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => geographic changes (lungs)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => geographic changes (lungs)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => follicular bronchiolitis (BALT)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => follicular bronchiolitis (BALT)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Axial CT of the chest at the level of the aortic arch shows ollicular bronchiolitis (BALT) which is characterized by centrilobular nodules, ground-glass opacities and bronchial wall thickening. Ashley Davidoff MD TheCommonVein.net 132Lu 136652 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Axial CT of the chest at the level of the aortic arch shows ollicular bronchiolitis (BALT) which is characterized by centrilobular nodules, ground-glass opacities and bronchial wall thickening. Ashley Davidoff MD TheCommonVein.net 132Lu 136652 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/02/136652cL.lungs-contrictive-bronchiolitis-rheumatoid-arthritis-RA.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Axial CT of the chest at the level of the aortic arch shows ollicular bronchiolitis (BALT) which is characterized by centrilobular nodules, ground-glass opacities and bronchial wall thickening. Ashley Davidoff MD TheCommonVein.net 132Lu 136652 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Axial CT of the chest at the level of the aortic arch shows ollicular bronchiolitis (BALT) which is characterized by centrilobular nodules, ground-glass opacities and bronchial wall thickening. Ashley Davidoff MD TheCommonVein.net 132Lu 136652 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/02/136652.lungs-contrictive-bronchiolitis-rheumatoid-arthritis-RA.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => focal lung finding
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => focal lung finding
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => fissures
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => fissures
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => fissuresL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => fissuresL
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => fissures
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => fissures
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => fissural (nodules)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => fissural (nodules)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 1
This CT shows fissural nodules which are usually benign round masses with well-defined margins that usually appear within fissural lines (yellow around)Ashley Davidoff MD TheCommonVein.net136201cL01 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 1
This CT shows fissural nodules which are usually benign round masses with well-defined margins that usually appear within fissural lines (yellow around)Ashley Davidoff MD TheCommonVein.net136201cL01 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/11/136201cL01-1.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
This CT shows fissural nodules which are usually benign round masses with well-defined margins that usually appear within fissural lines (yellow around)Ashley Davidoff MD TheCommonVein.net136201cL01 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This CT shows fissural nodules which are usually benign round masses with well-defined margins that usually appear within fissural lines (yellow around)Ashley Davidoff MD TheCommonVein.net136201cL01 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/11/136201cL01-1.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => extrapleural finding (fat sign)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => extrapleural finding (fat sign)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT Extra-Pleural Fat SignCT shows extra fat sign which is characterized by focal subsegmental area of atelectasis in the right lower lobe abutting the diaphragm associated with extra pleural fat proliferation secondary to the parenchymal infiltrate.Ashley Davidoff MD TheCommonVein.net 136036c B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT Extra-Pleural Fat SignCT shows extra fat sign which is characterized by focal subsegmental area of atelectasis in the right lower lobe abutting the diaphragm associated with extra pleural fat proliferation secondary to the parenchymal infiltrate.Ashley Davidoff MD TheCommonVein.net 136036c B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/12/136036c.-lung-pleura-extrapleural-fat-sign.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT Extra-Pleural Fat SignCT shows extra fat sign which is characterized by focal subsegmental area of atelectasis in the right lower lobe abutting the diaphragm associated with extra pleural fat proliferation secondary to the parenchymal infiltrate.Ashley Davidoff MD TheCommonVein.net 136036c B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT Extra-Pleural Fat SignCT shows extra fat sign which is characterized by focal subsegmental area of atelectasis in the right lower lobe abutting the diaphragm associated with extra pleural fat proliferation secondary to the parenchymal infiltrate.Ashley Davidoff MD TheCommonVein.net 136036c B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/12/136036c.-lung-pleura-extrapleural-fat-sign.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => endobronchial finding
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => endobronchial finding
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT in the axial plane shows an obstructing lesion in the left mainstem bronchus of the lung (green arrowhead) with post obstructive atelectasis of the lingula (black arrowhead) and a small portion of left upper lobe anteriorly (white arrowhead). The major fissure is displaced anteriorly.Ashley Davidoff MD TheCommonVein.net 257Lu 136110cL B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT in the axial plane shows an obstructing lesion in the left mainstem bronchus of the lung (green arrowhead) with post obstructive atelectasis of the lingula (black arrowhead) and a small portion of left upper lobe anteriorly (white arrowhead). The major fissure is displaced anteriorly.Ashley Davidoff MD TheCommonVein.net 257Lu 136110cL B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/12/136110.lungs-atelectasis-lingula-bronchus-carcinoid-.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT in the axial plane shows an obstructing lesion in the left mainstem bronchus of the lung (green arrowhead) with post obstructive atelectasis of the lingula (black arrowhead) and a small portion of left upper lobe anteriorly (white arrowhead). The major fissure is displaced anteriorly.Ashley Davidoff MD TheCommonVein.net 257Lu 136110cL B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT in the axial plane shows an obstructing lesion in the left mainstem bronchus of the lung (green arrowhead) with post obstructive atelectasis of the lingula (black arrowhead) and a small portion of left upper lobe anteriorly (white arrowhead). The major fissure is displaced anteriorly.Ashley Davidoff MD TheCommonVein.net 257Lu 136110cL B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/12/136110cL.lungs-atelectasis-lingula-bronchus-carcinoid.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => empyema
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => empyema
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Axial CT scan with contrast shows bilateral complex and loculated effusions with thickened enhancing pleura.
Ashley Davidoff MD TheCommonVein.net 135684cL B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Axial CT scan with contrast shows bilateral complex and loculated effusions with thickened enhancing pleura.
Ashley Davidoff MD TheCommonVein.net 135684cL B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/11/135684cL.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Axial CT scan with contrast shows bilateral complex and loculated effusions with thickened enhancing pleura. Ashley Davidoff MD TheCommonVein.net 135684 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Axial CT scan with contrast shows bilateral complex and loculated effusions with thickened enhancing pleura. Ashley Davidoff MD TheCommonVein.net 135684 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/11/135684.lungs-loculated-effusion-HHV-associated-lymphoma-71m-CT-split-pleura-primary-effusion-lymphoma.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => emphysema
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => emphysema
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CXR Emphysema and Small Heart58-year-old male presents with dyspnea. The lungs are hyperinflated with flattening of the diaphragms and increase in the retrosternal space on the lateral examination. The person also has an asthenic build with a relatively straight back and narrow A-P dimension. Frontal CXR shows a small heart with structures of the heart visualized to the right of the midline caused by compression of the low-pressure right atrium. The increased in the retrosternal airspace also compresses the relatively low pressure anteriorly positioned right ventricle. The heart is also lifted off the diaphragm (band c white arrowheads) and results in juxtaphrenic lung markings and peaks below the heart (d, arrowheads)Ashley Davidoff MD TheCommonVein.net 136232c01L B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CXR Emphysema and Small Heart58-year-old male presents with dyspnea. The lungs are hyperinflated with flattening of the diaphragms and increase in the retrosternal space on the lateral examination. The person also has an asthenic build with a relatively straight back and narrow A-P dimension. Frontal CXR shows a small heart with structures of the heart visualized to the right of the midline caused by compression of the low-pressure right atrium. The increased in the retrosternal airspace also compresses the relatively low pressure anteriorly positioned right ventricle. The heart is also lifted off the diaphragm (band c white arrowheads) and results in juxtaphrenic lung markings and peaks below the heart (d, arrowheads)Ashley Davidoff MD TheCommonVein.net 136232c01L B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/12/136232c01L.lungs-emphysema-heart-small-straight-back.png
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CXR Emphysema and Small Heart58-year-old male presents with dyspnea. The lungs are hyperinflated with flattening of the diaphragms and increase in the retrosternal space on the lateral examination. The person also has an asthenic build with a relatively straight back and narrow A-P dimension. Frontal CXR shows a small heart with structures of the heart visualized to the right of the midline caused by compression of the low-pressure right atrium. The increased in the retrosternal airspace also compresses the relatively low pressure anteriorly positioned right ventricle. The heart is also lifted off the diaphragm (band c white arrowheads) and results in juxtaphrenic lung markings and peaks below the heart (d, arrowheads)Ashley Davidoff MD TheCommonVein.net 136232c01L B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CXR Emphysema and Small Heart58-year-old male presents with dyspnea. The lungs are hyperinflated with flattening of the diaphragms and increase in the retrosternal space on the lateral examination. The person also has an asthenic build with a relatively straight back and narrow A-P dimension. Frontal CXR shows a small heart with structures of the heart visualized to the right of the midline caused by compression of the low-pressure right atrium. The increased in the retrosternal airspace also compresses the relatively low pressure anteriorly positioned right ventricle. The heart is also lifted off the diaphragm (band c white arrowheads) and results in juxtaphrenic lung markings and peaks below the heart (d, arrowheads)Ashley Davidoff MD TheCommonVein.net 136232c01L B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/12/136232c01L.lungs-emphysema-heart-small-straight-back.png
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => diffuse lung changes
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => diffuse lung changes
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Position of DiseaseSubpleural SparingAshley Davidoff MD TheCommonvein.net lungs-0775 0775-lo res subpleural sparing
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Position of DiseaseSubpleural SparingAshley Davidoff MD TheCommonvein.net lungs-0775 0775-lo res subpleural sparing
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/03/lungs-0775-lo-res-subpleural-sparing.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => diffuse alveolar damage (DAD)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => diffuse alveolar damage (DAD)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => CHF – Alveolar Edema
CT scan shows Diffuse ground glass pattern with thickening of the interlobular septa and manifesting as crazy paving pattern
Ashley Davidoff MD TheCommonVein.net 131742cL B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => CHF – Alveolar Edema
CT scan shows Diffuse ground glass pattern with thickening of the interlobular septa and manifesting as crazy paving pattern
Ashley Davidoff MD TheCommonVein.net 131742cL B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/11/131742cL.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CHF – Alveolar EdemaCT scan shows Diffuse ground glass pattern with thickening of the interlobular septa and manifesting as crazy paving patternAshley Davidoff MD TheCommonVein.net 131742 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CHF – Alveolar EdemaCT scan shows Diffuse ground glass pattern with thickening of the interlobular septa and manifesting as crazy paving patternAshley Davidoff MD TheCommonVein.net 131742 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2020/02/131742.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => desquamative interstitial pneumonia (DIP)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => desquamative interstitial pneumonia (DIP)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => Axial CT through the lower lung fields at the level of the left atrium shows desquamative interstitial pneumonia (DIP) which is characterized by diffuse ground glass changes with more prominent heterogeneity (b and c). Some of secondary lobules are expanded, with some with slightly thickened septa and prominent centrilobular nodules likely indicating small airway involvement (c, white ring).
Ashley Davidoff MD TheCommonVein.net 253Lu 136008 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Axial CT through the lower lung fields at the level of the left atrium shows desquamative interstitial pneumonia (DIP) which is characterized by diffuse ground glass changes with more prominent heterogeneity (b and c). Some of secondary lobules are expanded, with some with slightly thickened septa and prominent centrilobular nodules likely indicating small airway involvement (c, white ring).
Ashley Davidoff MD TheCommonVein.net 253Lu 136008 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/11/136008.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Axial CT through the lower lung fields at the level of the left atrium shows desquamative interstitial pneumonia (DIP) which is characterized by diffuse ground glass changes with more prominent heterogeneity (b and c). Some of secondary lobules are expanded, with some with slightly thickened septa and prominent centrilobular nodules likely indicating small airway involvement (c, white ring).Ashley Davidoff MD TheCommonVein.net 253Lu 136008 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Axial CT through the lower lung fields at the level of the left atrium shows desquamative interstitial pneumonia (DIP) which is characterized by diffuse ground glass changes with more prominent heterogeneity (b and c). Some of secondary lobules are expanded, with some with slightly thickened septa and prominent centrilobular nodules likely indicating small airway involvement (c, white ring).Ashley Davidoff MD TheCommonVein.net 253Lu 136008 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/12/136008cL.lungs-desquamative-interstitial-pneumonia-DIP-60M.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => cyst in the lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => cyst in the lungs
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
A 62-year-old female patient with Sjögren?s syndrome. Axial high-resolution computed tomography scan of the chest (A) and coronal reformatting (B). In A, diffuse thickening of the bronchial walls (closed arrows), some ground-glass opacities and thin-walled cysts of varying sizes, with a diffuse, bilateral distribution (open arrows). In B, distribution predominantly in the lower fields.Daniel Simões Oliveira et alweb-lungs-0013.jpg B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
A 62-year-old female patient with Sjögren?s syndrome. Axial high-resolution computed tomography scan of the chest (A) and coronal reformatting (B). In A, diffuse thickening of the bronchial walls (closed arrows), some ground-glass opacities and thin-walled cysts of varying sizes, with a diffuse, bilateral distribution (open arrows). In B, distribution predominantly in the lower fields.Daniel Simões Oliveira et alweb-lungs-0013.jpg B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2019/10/web-lungs-0013.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
A 62-year-old female patient with Sjögren?s syndrome. Axial high-resolution computed tomography scan of the chest (A) and coronal reformatting (B). In A, diffuse thickening of the bronchial walls (closed arrows), some ground-glass opacities and thin-walled cysts of varying sizes, with a diffuse, bilateral distribution (open arrows). In B, distribution predominantly in the lower fields.Daniel Simões Oliveira et alRadiologia Brasileira 51 (5): 321?327. web-lungs-0013.jpg B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
A 62-year-old female patient with Sjögren?s syndrome. Axial high-resolution computed tomography scan of the chest (A) and coronal reformatting (B). In A, diffuse thickening of the bronchial walls (closed arrows), some ground-glass opacities and thin-walled cysts of varying sizes, with a diffuse, bilateral distribution (open arrows). In B, distribution predominantly in the lower fields.Daniel Simões Oliveira et alRadiologia Brasileira 51 (5): 321?327. web-lungs-0013.jpg B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2019/10/web-lungs-0013.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => cryptogenic organizing pneumonia (COP)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => cryptogenic organizing pneumonia (COP)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT above shows the pathologic cryptogenic organizing pneumonia (COP) which is characterized by bilateral and asymmetrical ground-glass opacities and areas of consolidation that can overlap with the ground glass opacities Ashley Davidoff MD TheCommonVein.netlungs-COP-005-path-52f-CT B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT above shows the pathologic cryptogenic organizing pneumonia (COP) which is characterized by bilateral and asymmetrical ground-glass opacities and areas of consolidation that can overlap with the ground glass opacities Ashley Davidoff MD TheCommonVein.netlungs-COP-005-path-52f-CT B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/02/lungs-COP-002-path-52f-CT.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT above shows the pathologic cryptogenic organizing pneumonia (COP) which is characterized by bilateral and asymmetrical ground-glass opacities and areas of consolidation that can overlap with the ground glass opacities Ashley Davidoff MD TheCommonVein.netlungs-COP-005-path-52f-CT B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT above shows the pathologic cryptogenic organizing pneumonia (COP) which is characterized by bilateral and asymmetrical ground-glass opacities and areas of consolidation that can overlap with the ground glass opacities Ashley Davidoff MD TheCommonVein.netlungs-COP-005-path-52f-CT B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/02/lungs-COP-002-path-52f-CT.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => consolidation in the lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => consolidation in the lungs
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT shows alveolar proteinosis- central distribution which is characterized by diffuse bilateral ground-glass opacities involving both the upper and lower lobes Ashley DavidoffTheCommonVein.net117513 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT shows alveolar proteinosis- central distribution which is characterized by diffuse bilateral ground-glass opacities involving both the upper and lower lobes Ashley DavidoffTheCommonVein.net117513 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2021/10/117513.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT shows alveolar proteinosis- central distribution which is characterized by diffuse bilateral ground-glass opacities involving both the upper and lower lobes Ashley DavidoffTheCommonVein.net117513 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT shows alveolar proteinosis- central distribution which is characterized by diffuse bilateral ground-glass opacities involving both the upper and lower lobes Ashley DavidoffTheCommonVein.net117513 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2021/10/117513.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => consolidation in the lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => consolidation in the lungs
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Lingular Pneumonia52 year old male presents with a cough and feverCT scan in the axial plane shows a lingular consolidation with air bronchograms and a positive silhouette sign. Both the superior and inferior lingular segments are involvedAshley Davidoff MD TheCommonVein.net135190 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Lingular Pneumonia52 year old male presents with a cough and feverCT scan in the axial plane shows a lingular consolidation with air bronchograms and a positive silhouette sign. Both the superior and inferior lingular segments are involvedAshley Davidoff MD TheCommonVein.net135190 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/10/135190.ligular-pneumonia-silhouette.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Lingular Pneumonia52 year old male presents with a cough and feverCT scan in the axial plane shows a lingular consolidation with air bronchograms and a positive silhouette sign. Both the superior and inferior lingular segments are involvedAshley Davidoff MD TheCommonVein.net135190 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Lingular Pneumonia52 year old male presents with a cough and feverCT scan in the axial plane shows a lingular consolidation with air bronchograms and a positive silhouette sign. Both the superior and inferior lingular segments are involvedAshley Davidoff MD TheCommonVein.net135190 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/10/135190.ligular-pneumonia-silhouette.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => centrilobular emphysema
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => centrilobular emphysema
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Centrilobular Emphysema in the Upper Lobes of the LungsAxial CT (a) with magnified view of the upper lobes of a 66year female with centrilobular emphysema shows an expanded lobule with a centrilobular vessel in the middle characteristic of centrilobular emphysemaAshley Davidoff MD TheCommonvein.net RnD B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Centrilobular Emphysema in the Upper Lobes of the LungsAxial CT (a) with magnified view of the upper lobes of a 66year female with centrilobular emphysema shows an expanded lobule with a centrilobular vessel in the middle characteristic of centrilobular emphysemaAshley Davidoff MD TheCommonvein.net RnD B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/10/66f-centrilobular-emphysema-001c.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Centrilobular Emphysema in the Upper Lobes of the LungsAxial CT (a) with magnified view of the upper lobes of a 66year female with centrilobular emphysema shows an expanded lobule with a centrilobular vessel in the middle characteristic of centrilobular emphysemaAshley Davidoff MD TheCommonvein.net RnD B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Centrilobular Emphysema in the Upper Lobes of the LungsAxial CT (a) with magnified view of the upper lobes of a 66year female with centrilobular emphysema shows an expanded lobule with a centrilobular vessel in the middle characteristic of centrilobular emphysemaAshley Davidoff MD TheCommonvein.net RnD B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/10/66f-centrilobular-emphysema-001c.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => centrilobular (secondary lobule)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => centrilobular (secondary lobule)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => CT above shows a secondary lobule which is the smallest identifiable unit of the lung (made up of around 30 a0cni supplied by a common distal bronchiole and pulmonary artery)and its boundaries can be visualized by assessing the interlobular speta (red arrows)Ashley Davidoff MD TheCommonVein.net B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => CT above shows a secondary lobule which is the smallest identifiable unit of the lung (made up of around 30 a0cni supplied by a common distal bronchiole and pulmonary artery)and its boundaries can be visualized by assessing the interlobular speta (red arrows)Ashley Davidoff MD TheCommonVein.net B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/11/132575.8bL_32698-1.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 132575.8bL
CT above shows a secondary lobule which is the smallest identifiable unit of the lung (made up of around 30 a0cni supplied by a common distal bronchiole and pulmonary artery)and its boundaries can be visualized by assessing the interlobular speta (red arrows)Ashley Davidoff MD TheCommonVein.net B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 132575.8bL
CT above shows a secondary lobule which is the smallest identifiable unit of the lung (made up of around 30 a0cni supplied by a common distal bronchiole and pulmonary artery)and its boundaries can be visualized by assessing the interlobular speta (red arrows)Ashley Davidoff MD TheCommonVein.net B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/11/132575.8bL_32698-1.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => cavity (lungs)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => cavity (lungs)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Coronal and sagittal CT reconstructions show a cavitating mass in the superior segment of the right lower lobe (upper images) correlated with axial images (lower panel)Ashley Davidoff MD TheCommonVein.net 176Lu 136737 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Coronal and sagittal CT reconstructions show a cavitating mass in the superior segment of the right lower lobe (upper images) correlated with axial images (lower panel)Ashley Davidoff MD TheCommonVein.net 176Lu 136737 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/02/136737.lungs-cavitating-squamous-cell-carcinoma.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Coronal and sagittal CT reconstructions show a cavitating mass in the superior segment of the right lower lobe (upper images) correlated with axial images (lower panel)Ashley Davidoff MD TheCommonVein.net 176Lu 136737 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Coronal and sagittal CT reconstructions show a cavitating mass in the superior segment of the right lower lobe (upper images) correlated with axial images (lower panel)Ashley Davidoff MD TheCommonVein.net 176Lu 136737 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/02/136737.lungs-cavitating-squamous-cell-carcinoma.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => bullous emphysema
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => bullous emphysema
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT scan in the coronal plane of shows bilateral apical bullous lung disease, magnified in the lower imageAshley Davidoff MD TheCommonVein.Net 136439c B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT scan in the coronal plane of shows bilateral apical bullous lung disease, magnified in the lower imageAshley Davidoff MD TheCommonVein.Net 136439c B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/01/136439c.lungs-emphysema-bulla.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT Scan Bilateral Apical Bulla Centrilobular EmphysemaCT scan in the coronal plane shows bilateral apical bullous lung disease, magnified in the lower imageAshley Davidoff MD TheCommonVein.Net 136439c B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT Scan Bilateral Apical Bulla Centrilobular EmphysemaCT scan in the coronal plane shows bilateral apical bullous lung disease, magnified in the lower imageAshley Davidoff MD TheCommonVein.Net 136439c B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/01/136439c.lungs-emphysema-bulla.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => bulla
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => bulla
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT Scan Bilateral Apical Builla Centrilobular Emphysema
CT scan in the axial plane shows bilateral apical bullous lung disease, most commonly seen in emphysema
Ashley Davidoff MD TheCommonVein.Net 136440 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT Scan Bilateral Apical Builla Centrilobular Emphysema
CT scan in the axial plane shows bilateral apical bullous lung disease, most commonly seen in emphysema
Ashley Davidoff MD TheCommonVein.Net 136440 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/11/136440cL-1.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT Scan Bilateral Apical Builla Centrilobular EmphysemaCT scan in the axial plane shows bilateral apical bullous lung disease, most commonly seen in emphysema Ashley Davidoff MD TheCommonVein.Net 136440 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT Scan Bilateral Apical Builla Centrilobular EmphysemaCT scan in the axial plane shows bilateral apical bullous lung disease, most commonly seen in emphysema Ashley Davidoff MD TheCommonVein.Net 136440 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/01/136440.lungs-emphysema-bulla-.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => broncholith
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => broncholith
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 1
CT in the axial plane shows a bilobed calcified broncholith in the lateral segment of the middle lobe (c, d white arrowheads) with post obstructive atelectasis (c, blue arrowhead)
Ashley Davidoff MD TheCommonVein.net 136585cL B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 1
CT in the axial plane shows a bilobed calcified broncholith in the lateral segment of the middle lobe (c, d white arrowheads) with post obstructive atelectasis (c, blue arrowhead)
Ashley Davidoff MD TheCommonVein.net 136585cL B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/02/136585cL.lungs-broncholith-middle-lobe-atelectasiss.png
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT in the axial plane shows a bilobed calcified broncholith in the lateral segment of the middle lobe (c, d white arrowheads) with post obstructive atelectasis (c, blue arrowhead)Ashley Davidoff MD TheCommonVein.net 136585cL B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT in the axial plane shows a bilobed calcified broncholith in the lateral segment of the middle lobe (c, d white arrowheads) with post obstructive atelectasis (c, blue arrowhead)Ashley Davidoff MD TheCommonVein.net 136585cL B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/02/136585cL.lungs-broncholith-middle-lobe-atelectasiss.png
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => bronchocentric
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => bronchocentric
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => bronchocentric
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => bronchocentric
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => bronchocele
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => bronchocele
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Finger in Glove Sign
19 year old female with cystic fibrosis and bronchiectasis
CT scan through the upper lung fields shows mucin filled subsegmental bronchi of the right upper lobe with morphology reminiscent of the “finger in glove” sign (point to by yellow arrows)
Courtesy Priscilla Slanetz MD MPH TheCommonVein.net31966cl B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Finger in Glove Sign
19 year old female with cystic fibrosis and bronchiectasis
CT scan through the upper lung fields shows mucin filled subsegmental bronchi of the right upper lobe with morphology reminiscent of the “finger in glove” sign (point to by yellow arrows)
Courtesy Priscilla Slanetz MD MPH TheCommonVein.net31966cl B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/11/31966cl.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Finger in Glove Sign19 year old female with cystic fibrosis and bronchiectasisCT scan through the upper lung fields shows mucin filled subsegmental bronchi of the right upper lobe with morphology reminiscent of the “finger in glove” signCourtesy Priscilla Slanetz MD MPH TheCommonVein.net 31966 B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Finger in Glove Sign19 year old female with cystic fibrosis and bronchiectasisCT scan through the upper lung fields shows mucin filled subsegmental bronchi of the right upper lobe with morphology reminiscent of the “finger in glove” signCourtesy Priscilla Slanetz MD MPH TheCommonVein.net 31966 B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/08/31966.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => bronchiolitis (CXR)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => bronchiolitis (CXR)
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Frontal and Lateral CXR shows follicular bronchiolitis which is characterized by a coarsened nodular interstitial pattern. Ashley Davidoff MD TheCommonVein.net 132Lu 136650c B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Frontal and Lateral CXR shows follicular bronchiolitis which is characterized by a coarsened nodular interstitial pattern. Ashley Davidoff MD TheCommonVein.net 132Lu 136650c B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/02/136650c01.lungs-contrictive-bronchiolitis-rheumatoid-arthritis-RA.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 7
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Frontal and Lateral CXR shows follicular bronchiolitis which is characterized by a coarsened nodular interstitial pattern. Ashley Davidoff MD TheCommonVein.net 132Lu 136650c B.A
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Frontal and Lateral CXR shows follicular bronchiolitis which is characterized by a coarsened nodular interstitial pattern. Ashley Davidoff MD TheCommonVein.net 132Lu 136650c B.A
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/02/136650c.lungs-contrictive-bronchiolitis-rheumatoid-arthritis-RA.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => bronchiolitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => bronchiolitis
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Chest CT above shows bronchiolitis which is characterized by peribronchial thickening which is thickening of the small airways of lung (yellow arrows)Ashley Davidoff MD TheCommonVein.net 81F-bronchiolitis-infection-inflammation-004
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Chest CT above shows bronchiolitis which is characterized by peribronchial thickening which is thickening of the small airways of lung (yellow arrows)Ashley Davidoff MD TheCommonVein.net 81F-bronchiolitis-infection-inflammation-004
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/11/81F-bronchiolitis-infection-inflammation-004cL-1.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Chest CT above shows bronchiolitis which is characterized by peribronchial thickening which is thickening of the small airways of lung (yellow arrows)Ashley Davidoff MD TheCommonVein.net 81F-bronchiolitis-infection-inflammation-004
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Chest CT above shows bronchiolitis which is characterized by peribronchial thickening which is thickening of the small airways of lung (yellow arrows)Ashley Davidoff MD TheCommonVein.net 81F-bronchiolitis-infection-inflammation-004
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/11/81F-bronchiolitis-infection-inflammation-004cL-1.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => bronchiolectasis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => bronchiolectasis
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 136598c
Fibrotic NSIP59-year-old male presents with history of scleroderma, Raynaud’s disease, and ILDUpper ImageAxial CT shows bibasilar peripheral reticular changes, ground glass, bronchiectasis, and bronchiolectasis with volume and with crowding of the bronchovascular bundles posteriorly. There is subpleural sparing posteriorly. Note air-fluid level in the distended esophagus.Lower ImageThe lower image focuses on the traction bronchiectasis caused by the fibrotic processAshley Davidoff MD TheCommonVein.net 110Lu 136598c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 136598c
Fibrotic NSIP59-year-old male presents with history of scleroderma, Raynaud’s disease, and ILDUpper ImageAxial CT shows bibasilar peripheral reticular changes, ground glass, bronchiectasis, and bronchiolectasis with volume and with crowding of the bronchovascular bundles posteriorly. There is subpleural sparing posteriorly. Note air-fluid level in the distended esophagus.Lower ImageThe lower image focuses on the traction bronchiectasis caused by the fibrotic processAshley Davidoff MD TheCommonVein.net 110Lu 136598c
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/02/136598c.lungs-ILD-NSIP-scleroderma.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] => 136598c
Fibrotic NSIP59-year-old male presents with history of scleroderma, Raynaud’s disease, and ILDUpper ImageAxial CT shows bibasilar ground glass, bronchiectasis, and bronchiolectasis with volume loss and with crowding of the bronchovascular bundles posteriorly. There is subpleural sparing. Note air-fluid level in the distended esophagus.The lower image focuses on the peripheral sparing. The spared secondary lobules have also undergone enlargement secondary to the fibrotic processAshley Davidoff MD TheCommonVein.net 110Lu 136598c01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 136598c
Fibrotic NSIP59-year-old male presents with history of scleroderma, Raynaud’s disease, and ILDUpper ImageAxial CT shows bibasilar ground glass, bronchiectasis, and bronchiolectasis with volume loss and with crowding of the bronchovascular bundles posteriorly. There is subpleural sparing. Note air-fluid level in the distended esophagus.The lower image focuses on the peripheral sparing. The spared secondary lobules have also undergone enlargement secondary to the fibrotic processAshley Davidoff MD TheCommonVein.net 110Lu 136598c01
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/02/136598c01.lungs-ILD-NSIP-scleroderma.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => bronchiectasis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => bronchiectasis
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Axial CT – Lady Windermere Syndrome61-year-old male with a history of treated mycobacterial infections including MAC and chronic cough.Axial CT at the level of the mid to lower chest shows mildly ectatic segmental airways to the lower, and middle lobe bronchi but significant bronchiectasis to the middle lobe and lingula involving the subsegmental airways. There is a relative paucity of mucus in the ectatic airways. The history of MAC and the distribution of the bronchiectasis in the middle lobe and lingula are reminiscent of the diagnosis of Lady Windermere syndromeAshley Davidoff MD TheCommonVein.net 250Lu 135876
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Axial CT – Lady Windermere Syndrome61-year-old male with a history of treated mycobacterial infections including MAC and chronic cough.Axial CT at the level of the mid to lower chest shows mildly ectatic segmental airways to the lower, and middle lobe bronchi but significant bronchiectasis to the middle lobe and lingula involving the subsegmental airways. There is a relative paucity of mucus in the ectatic airways. The history of MAC and the distribution of the bronchiectasis in the middle lobe and lingula are reminiscent of the diagnosis of Lady Windermere syndromeAshley Davidoff MD TheCommonVein.net 250Lu 135876
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/11/135876cL-lungs-trachea-bronchi-Mounier-Kuhn-bronchiectasis-61M.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Axial CT – Lady Windermere Syndrome61-year-old male with a history of treated mycobacterial infections including MAC and chronic cough.Axial CT at the level of the mid to lower chest shows mildly ectatic segmental airways to the lower, and middle lobe bronchi but significant bronchiectasis to the middle lobe and lingula involving the subsegmental airways. There is a relative paucity of mucus in the ectatic airways. The history of MAC and the distribution of the bronchiectasis in the middle lobe and lingula are reminiscent of the diagnosis of Lady Windermere syndromeAshley Davidoff MD TheCommonVein.net 250Lu 135876
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Axial CT – Lady Windermere Syndrome61-year-old male with a history of treated mycobacterial infections including MAC and chronic cough.Axial CT at the level of the mid to lower chest shows mildly ectatic segmental airways to the lower, and middle lobe bronchi but significant bronchiectasis to the middle lobe and lingula involving the subsegmental airways. There is a relative paucity of mucus in the ectatic airways. The history of MAC and the distribution of the bronchiectasis in the middle lobe and lingula are reminiscent of the diagnosis of Lady Windermere syndromeAshley Davidoff MD TheCommonVein.net 250Lu 135876
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/11/135876-lungs-trachea-bronchi-Mounier-Kuhn-bronchiectasis-61M.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => bleb
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => bleb
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2024/11/117504cL.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CT Emphysema, Paraseptal Emphysematous Changes Bilateral Lower Lobes65-year-old male with emphysema of the lungs presents with a cough, fever and leukocytosis. CT in the axial plane shows bibasilar paraseptal emphysematous changes and centrilobular changes in the lingula and RUL. Hyperinflation with resultant small heart is noted.Ashley Davidoff MD TheCommonVein.net 259Lu 117504
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT Emphysema, Paraseptal Emphysematous Changes Bilateral Lower Lobes65-year-old male with emphysema of the lungs presents with a cough, fever and leukocytosis. CT in the axial plane shows bibasilar paraseptal emphysematous changes and centrilobular changes in the lingula and RUL. Hyperinflation with resultant small heart is noted.Ashley Davidoff MD TheCommonVein.net 259Lu 117504
)
https://beta.thecommonvein.net/wp-content/uploads/2023/03/47f-SLE-Sjogrens-LIP-vs-Birt-Hogg-Dube-basilar-thin-walled-cysts-lymphadenopathy-010-CT-1year-ago.jpg
https://lungs.thecommonvein.net/wp-content/uploads/2023/12/117504.jpg