
The lungs are located within the thorax, within the thoracic cavity and within the pleura. They occupy about 3/4 of the thoracic cavity, with the rest occupied by the heart and the mediastinum. The right lung occupies almost the entire right hemi thorax and the left is displaced by the heart and occupies a lesser amount of space.
The lungs are divided into upper and lower lobes which is somewhat of a conceptual misnomer since the lower lobes creep up posteriorly to almost the apex of the lungs and the upper lobes (together with the lingula and middle lobe) on the other hand reach more inferiorly in the anterior location. The lobes may have just as well been called the posterior lobes and the anterior lobes but because the upper lobes reach the most superior position in the chest and the lower lobes the most inferior and diaphragmatic parts, they were reasonably labeled upper and lower.
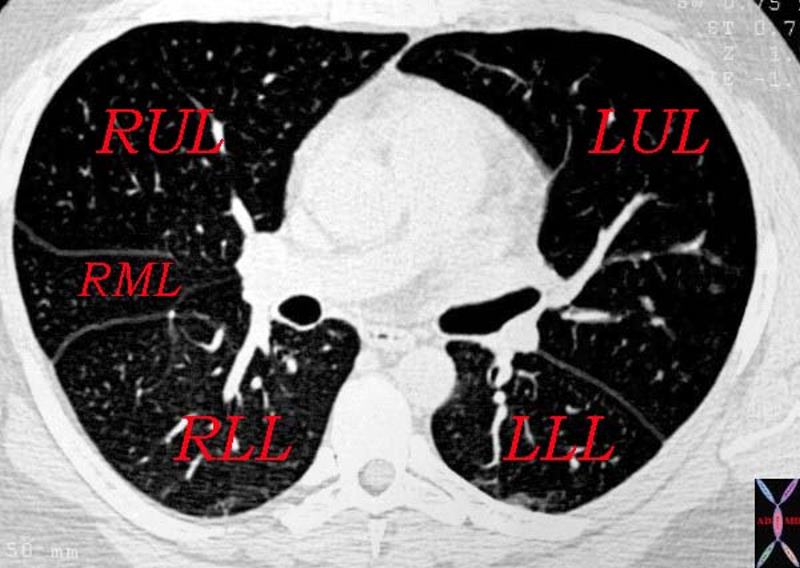
This cross section through the heart shows all the lobes of the lungs with upper lobes taking an anterior location
while the lower lobeTheCommonVein.net 32160d.800
The segments are named according to their position, and include the apical anterior and posterior segments in the upper lobes, the lateral and medial components of the RML, the superior and inferior of the lingula, and the superior (apical) lateral medial anterior and posterior basal segments. Note that all the names relate to the position of the segments. There is a move to give these segment numbers – but it seems far easier to understand the spatial positioning by naming the segments according to their position.
The middle lobe has a very intimate relation to the right heart border (RA), while the lingula has a similar relationship with the left ventricle. This has relevance in the evaluation of infiltrates on the CXR since disease in the RML will cause silhouetting of the right heart border (RA), while an infiltrate in the lingula will silhouette the left heart border. On the lateral examination since both of these are anterior segments they will be seen as anterior infiltrates. Hence the position of infiltrates as seen on the CXR can be accurately localized to segments by looking at the relationship to the heart in the P-A and whether the infiltrate is anterior or posterior on the lateral CXR.
Applied Anatomy
Situs Inversus
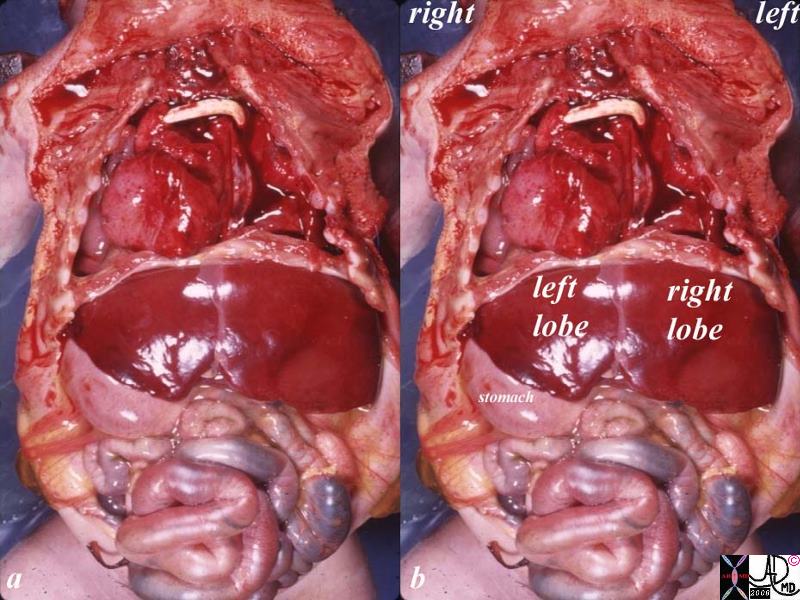
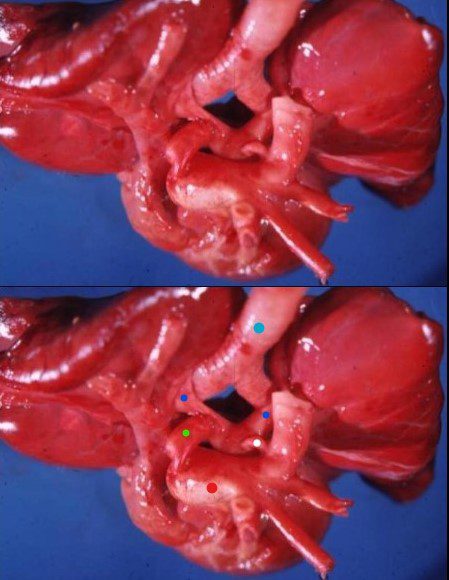
This unfortunate baby has situs inversus associated with complex congenital heart disease. The baby?s right lung had the morphology of a left lung in that it had two lobes rather than three. The left lung had the morphology of the right having 3 lobes. This inversion of the position of the organs is called situs inversus. Complex congenital heart disease is noted with dextrocardia and a white tubular graft is noted in the upper chest from recent surgery. The liver is mainly on the left side, and the stomach on the right.
Ashley Davidoff TheCommonVein.net 10850c01.8s
Situs inversus has a wide variation of clinical presentations. Some patients with situs inversus may live a completely normal life without ever being aware of the condition. At the other extreme, such as in the case above, the aberrant morphology, particularly related to the heart, can be life threatening.
Ashley Davidoff TheCommonVein.net

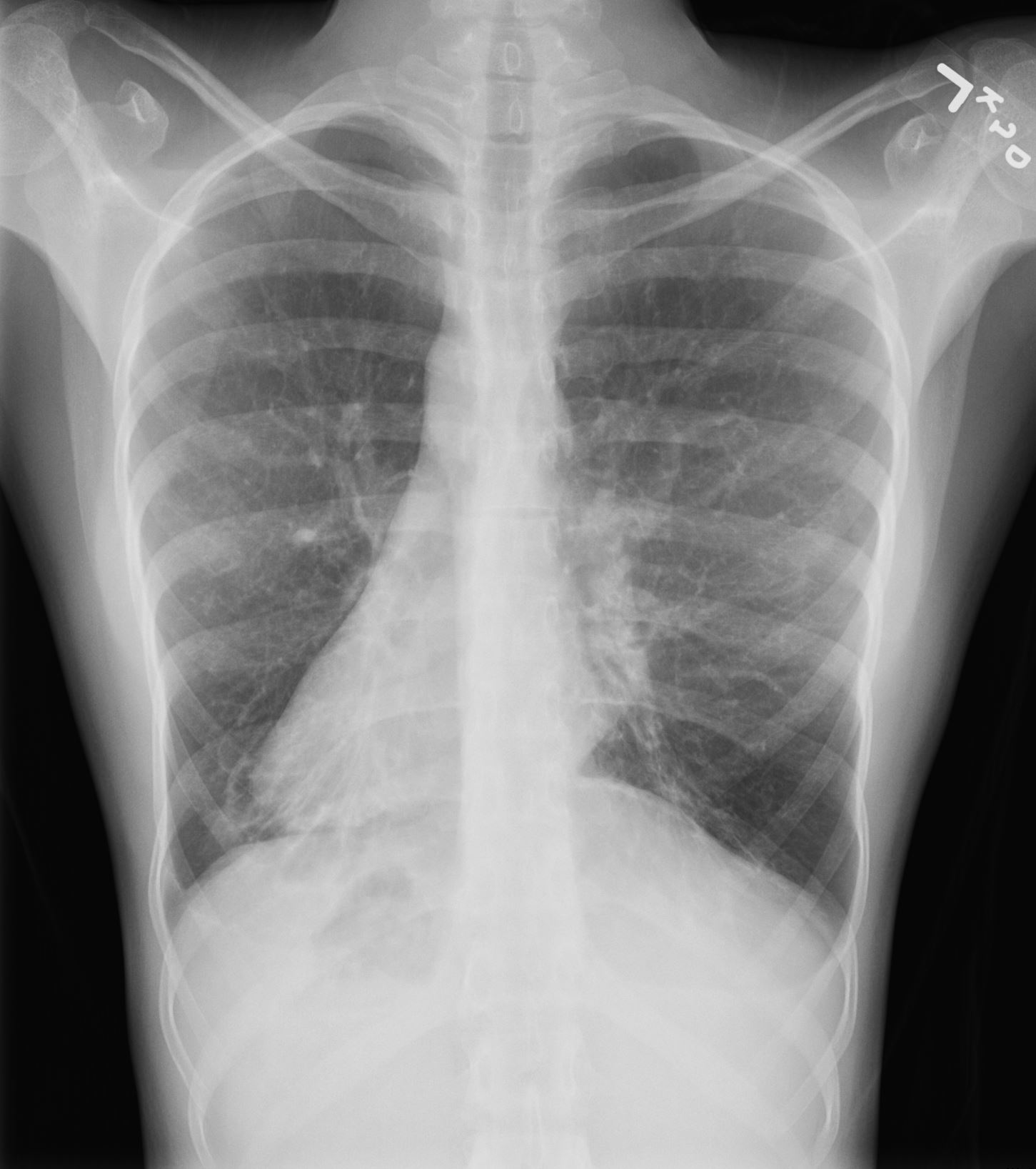
This 30 year old male presents with a long standing history of a productive cough, headaches, and infertility. This obsolete study called a bronchogram outlines the bronchi with contrast revealing situs inversus of the bronchi. In the right upper lobe there are saccular accumulations of contrast representing a region of bronchiectasis. The stomach bubble can be seen on the right and hence there is situs inversus totalis. The heart is seen with apex pointed to the right and hence there is dextrocardia. So we can explain the cough from the bronchiectasis, but how do we explain the headaches and the infertility?
Ashley Davidoff TheCommonVein.net MD 06248
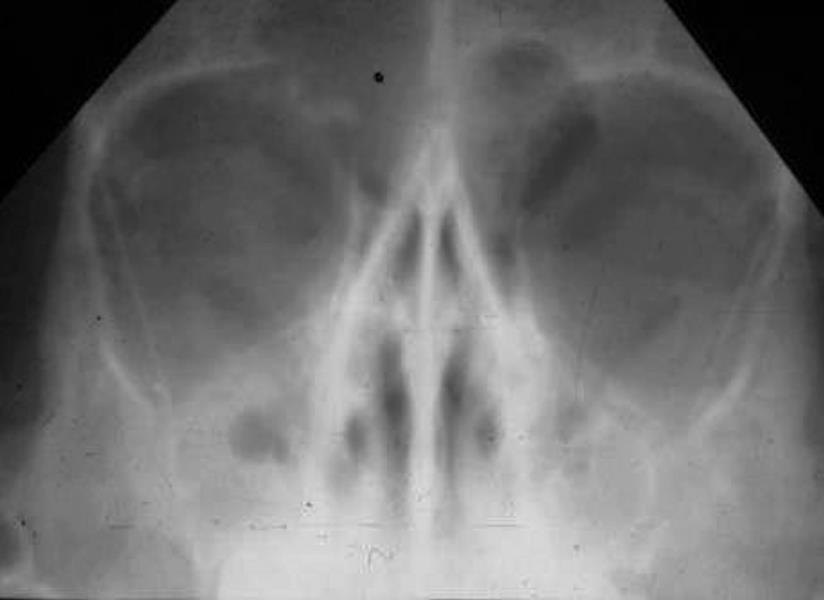
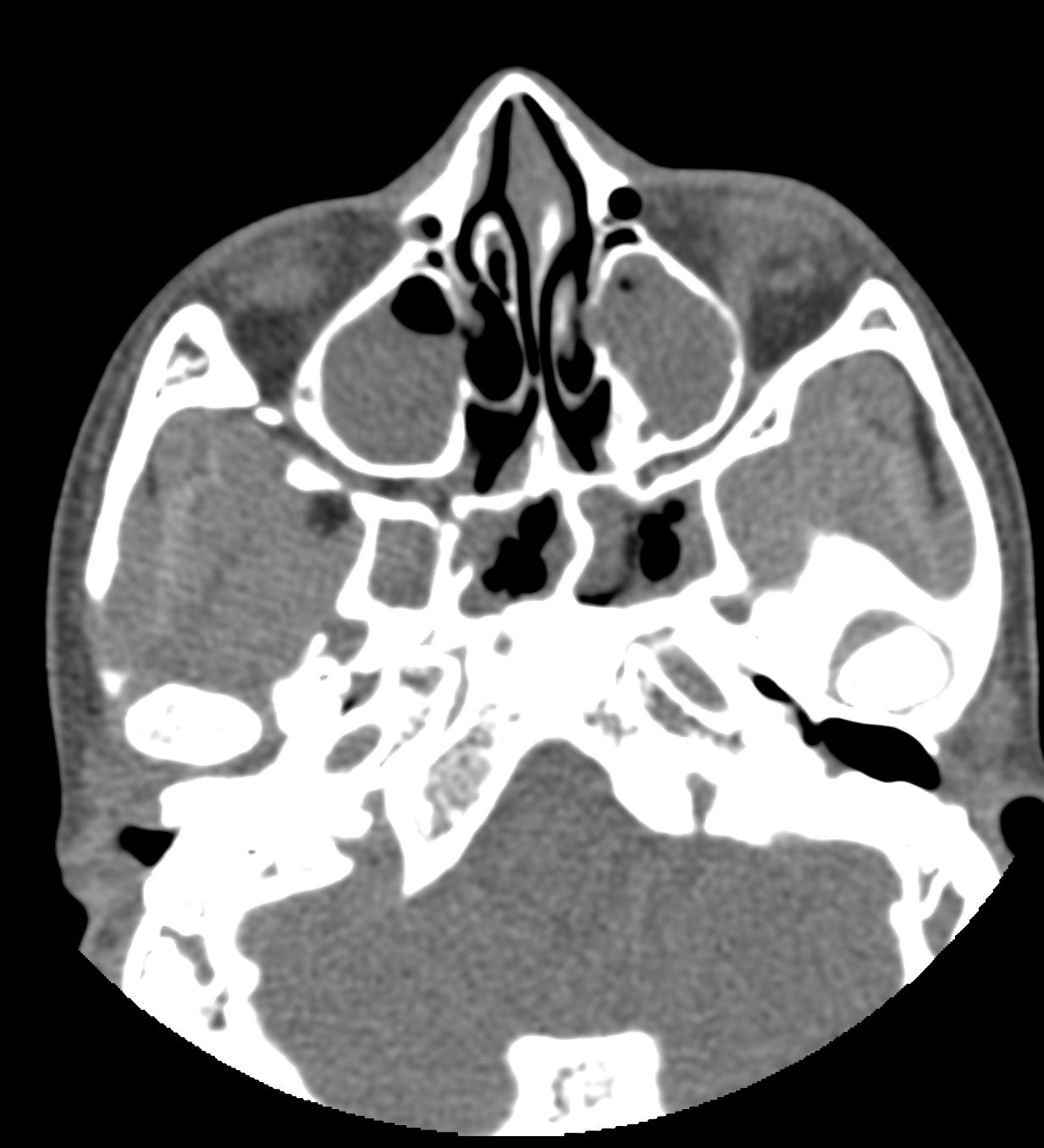
Sinus views show a totally opacified maxillary sinus on the right, and an air fluid level on the left, consistent with acute sinusitis. In the same patient note the total opacification of the left maxillary sinus and air fluid level in the right maxillary sinus characteristic of acute sinusitis. This patient has a syndrome called Kartagener?s syndrome (aka immotile cilia syndrome) where ciliary motility is diminished, resulting in suboptimal defense mechanisms in the bronchial and sinus epithelia, causing sinusitis and bronchiectasis, and decreased sperm motility resulting in sterility.
Ashley Davidoff TheCommonVein.net 06247
Ashley Davidoff TheCommonVein.net
Herniated Lung
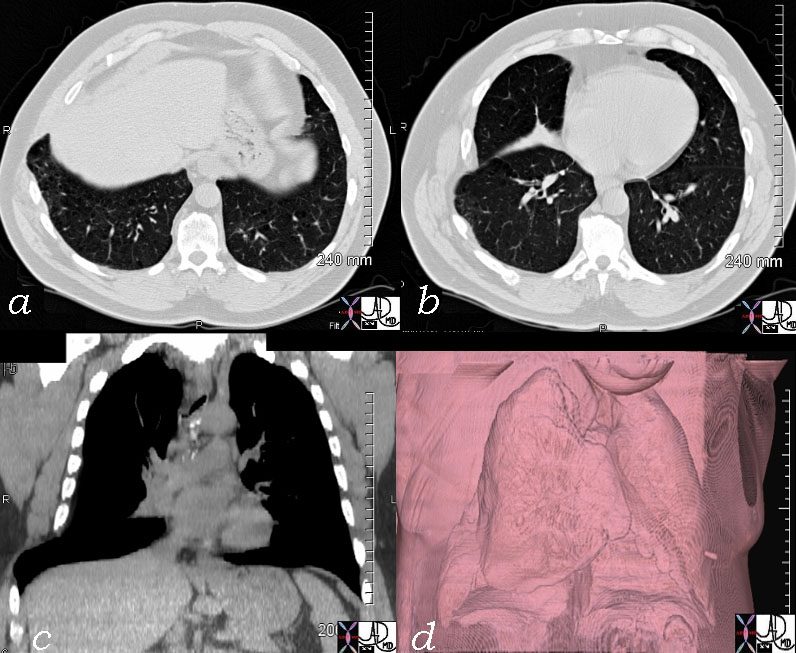
In this patient rib fractures resulted in a focal defect in the right lower lung field and resulting herniation of the lung. This is seen in the cross sectional images in a and b, in the coronal reformat in c, and in the volume rendering image in d.
Ashley Davidoff TheCommonVein.net 46106c02
Anatomy of the Structures Surrounding the Lungs – Neighbours
The lungs are completely surrounded by the pleura, a variety of muscles and the bony thoracic cage. The heart and other structures of the mediastinum form the medial relations of the lungs.
Within the mediastinum lies the heart and pericardium, the trachea and main stem bronchi, esophagus, thoracic duct, lymph nodes, and both phrenic and vagus nerves. The mediastinum is situated anterior to the sternum and ventral to the spinal column, nestled between the pleural sacs of the right and left lungs. Superiorly it reaches the level of the fourth thoracic vertebrae and rests upon the diaphragm inferiorly. Below the diaphragm lie the liver, gall bladder, and spleen.
Surrounding the lungs are the thoracic muscles and the diaphragm itself. These are the muscles related to respiration. Their operation alters the pressure within the thorax. When the thorax expands the pressure decreases, allowing air from the trachea into the lungs. When it contracts, the lungs compress and air leaves the lungs. When the diaphragm contracts it flattens and sinks as much as 7-10 cm below its normal level at rest. As the muscles relax the thorax returns to normal pressure and air from the lungs is released. This is known as abdominal respiration and accounts for approximately 70% of respiration in a resting body.
Position of the Pulmonary Arteries in Relation to the Bronchi
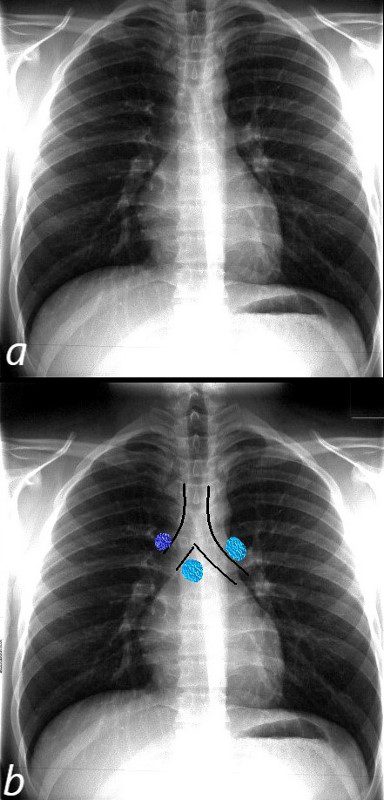
The normal CXR shows the superior position and relationship of the LPA to the left mainstem bronchus. The bronchus is hyparterial ie below the artery.
The RPA (light blue and right in b) runs below the right mainstem bronchus ie the bronchus is eparterial . The azygous vein lies superior to the right mainstem bronchus at the take off of the right mainstem from the trachea.
Ashley Davidoff MD
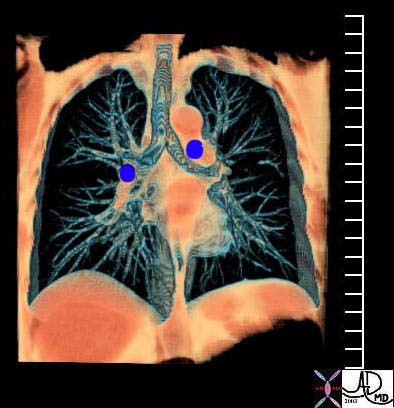
This coronal reformat shows the position of the main branch pulmonary arteries relative to the position of their respective bronchi. While the RPA runs under the right mainstem bronchus, the LPA runs above the left mainstem.
Courtesy Ashley Davidoff MD TheCommonVein.net 32620b01
Patient with Polysplenia Syndrome Abnormal Position of the Right Pulmonary Artery
{kind=link}
Pulmonary Veins and Left Atrium
Normal 3D coronal reconstruction of a CT scan of the heart showing the left atrium (LA) and pulmonary veins and pulmonary arteries. Note the relatively horizontal orientation of the pulmonary veins compared to the lower lobe pulmonary arteries.
Ashley Davidoff MD TheCommonVein.net 34764