
The Common Vein Copyright 2008
Definition
Pulmonary hypertension is a circulatory characterized by an abnormally high pressure in the pulmonary arteries. The diagnosis is defined as a systolic pressure that is greater than 30mmhg or a mean pressure that is greater than 20mmhg.
There are many causes for the disorder including, left heart failure, mitral valve disease, chronic lung disease, (cor pulmonale) and left to right shunts. Patients with chronic thromboembolic disease may have hypertension and acute embolic disease may be associated with acute hypertension. When the cause is known it is called secondary hypertension. In many the cause is unknown in which case it is called primary pulmonary hypertension. In some some cases there is a genetic predisposition.
Clinically the entity results and manifests in shortnes of breath, coughing, wheezing, chest pain, fatigue, fainting, dizziness, light-headedness, and swelling in the legs. The diagnosis is confirmed by identifying an enlarged right ventricle, abnormally loud P2 sound, a systolic ejection murmur, and perhaps a pulmonarydiastolic murmur, by electrocardiography which shows right ventricular hypertrophy. Echocardiography can not only evaluate right ventricular and right atrial size, but can accurately estimate the pulmonary arterial pressure if there is tricuspid regurgitation. While the CXR CTscan and MRI can evaluate pulmonary arterial size and right ventricular size, the most acurate evaluatio of the entity is via cardiac cateterization which measures the pressures directly. Treatment is directed to the cause when known, usually with medication, and oxygen. In patients with underlying mechanical causes such as left to right shunts a surgical option is possible if the fixed component of the hypertension is not excessive.
|
Pulmonary Hypertension
Web References
|

Links and References
eMedicine Secondary Hypertension Sat Sharma MD
eMedicine Primary Hypertension Ronald Oudiz MD
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
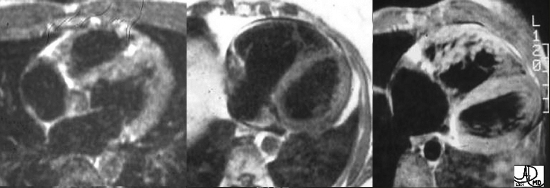
Normal, Dilated, and Hypertrophied Right Ventricles
These three images represent T1 weighted images of the RV reflecting normal, dilated, and hypertrophied conditions. Normal thin-walled capacious RV (1) ASD (Atrial Septal Defect) with volume overloaded – thin-walled but dilated RV (2) Pressure overloaded , hypertrophied RV, with accentuated trabeculations (3) Courtesy of Ashley Davidoff M.D. 32095
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal, Dilated, and Hypertrophied Right Ventricles
These three images represent T1 weighted images of the RV reflecting normal, dilated, and hypertrophied conditions. Normal thin-walled capacious RV (1) ASD (Atrial Septal Defect) with volume overloaded – thin-walled but dilated RV (2) Pressure overloaded , hypertrophied RV, with accentuated trabeculations (3) Courtesy of Ashley Davidoff M.D. 32095
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => These three images represent T1 weighted images of the RV reflecting normal, dilated, and hypertrophied conditions. Normal thin-walled capacious RV (1) ASD (Atrial Septal Defect) with volume overloaded – thin-walled but dilated RV (2) Pressure overloaded , hypertrophied RV, with accentuated trabeculations (3) Courtesy of Ashley Davidoff M.D. 32095
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => These three images represent T1 weighted images of the RV reflecting normal, dilated, and hypertrophied conditions. Normal thin-walled capacious RV (1) ASD (Atrial Septal Defect) with volume overloaded – thin-walled but dilated RV (2) Pressure overloaded , hypertrophied RV, with accentuated trabeculations (3) Courtesy of Ashley Davidoff M.D. 32095
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal, Dilated, and Hypertrophied Right Ventricles
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal, Dilated, and Hypertrophied Right Ventricles
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
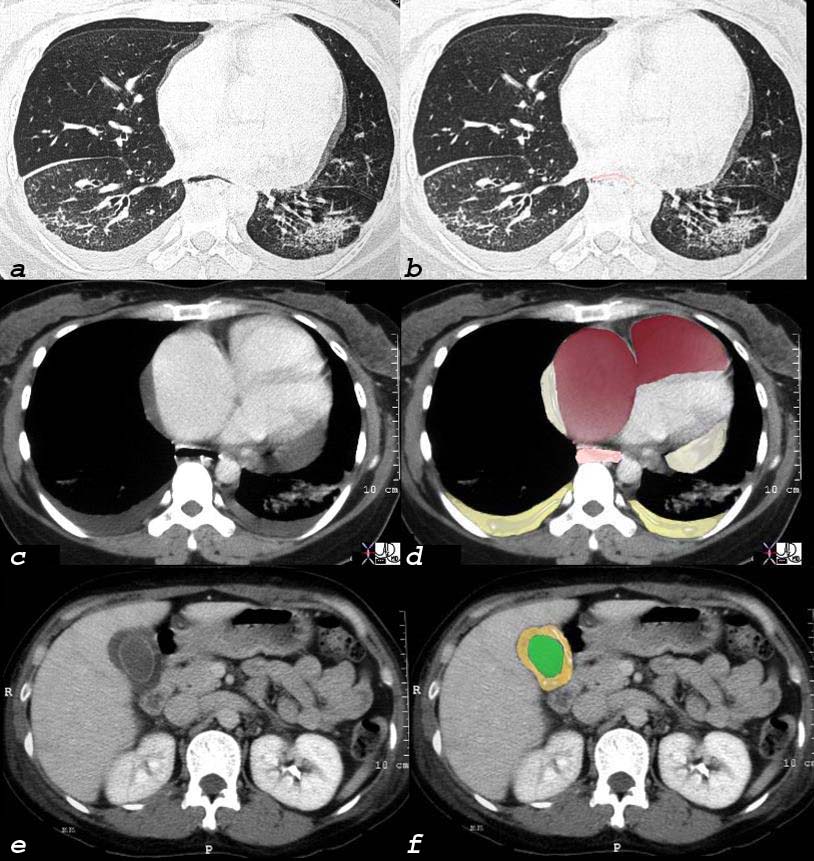
Scleroderma Pulmonary Hypertension and Right Heart Failure
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Scleroderma Pulmonary Hypertension and Right Heart Failure
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Scleroderma Pulmonary Hypertension and Right Heart Failure
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Scleroderma Pulmonary Hypertension and Right Heart Failure
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
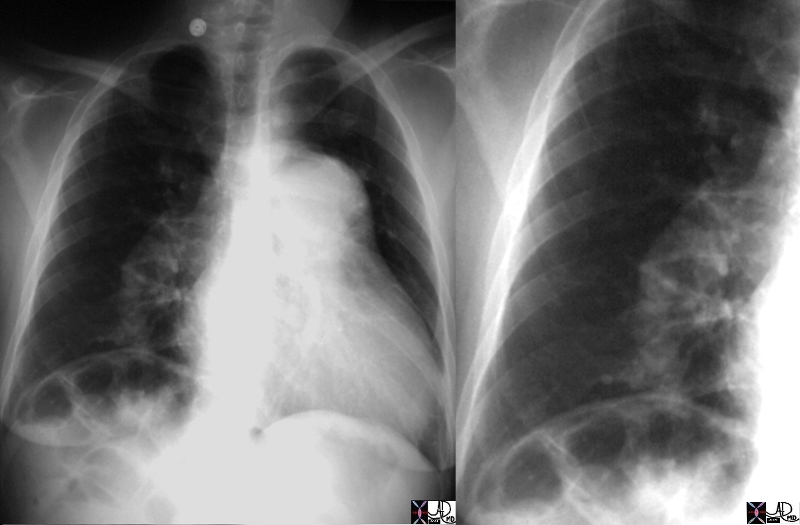
Normal and Pruning
15406c05 heart cardiac right ventricle RV fx enlarged MPA main pulmonary artery fx enlarged pulmonary arteries DD ASD VSD PDA septal defects Eisenmenger’s CXR plain X-ray of chest Davidoff MD fx pruned pruning dx Eisenmenger’s Davidoff MD 15406.800 15406c02 15406c04 15406c05
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal and Pruning
15406c05 heart cardiac right ventricle RV fx enlarged MPA main pulmonary artery fx enlarged pulmonary arteries DD ASD VSD PDA septal defects Eisenmenger’s CXR plain X-ray of chest Davidoff MD fx pruned pruning dx Eisenmenger’s Davidoff MD 15406.800 15406c02 15406c04 15406c05
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 15406c05 heart cardiac right ventricle RV fx enlarged MPA main pulmonary artery fx enlarged pulmonary arteries DD ASD VSD PDA septal defects Eisenmenger’s CXR plain X-ray of chest Davidoff MD fx pruned pruning dx Eisenmenger’s Davidoff MD 15406.800 15406c02 15406c04 15406c05
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 15406c05 heart cardiac right ventricle RV fx enlarged MPA main pulmonary artery fx enlarged pulmonary arteries DD ASD VSD PDA septal defects Eisenmenger’s CXR plain X-ray of chest Davidoff MD fx pruned pruning dx Eisenmenger’s Davidoff MD 15406.800 15406c02 15406c04 15406c05
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal and Pruning
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal and Pruning
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
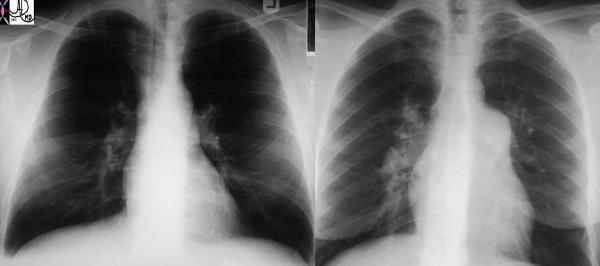
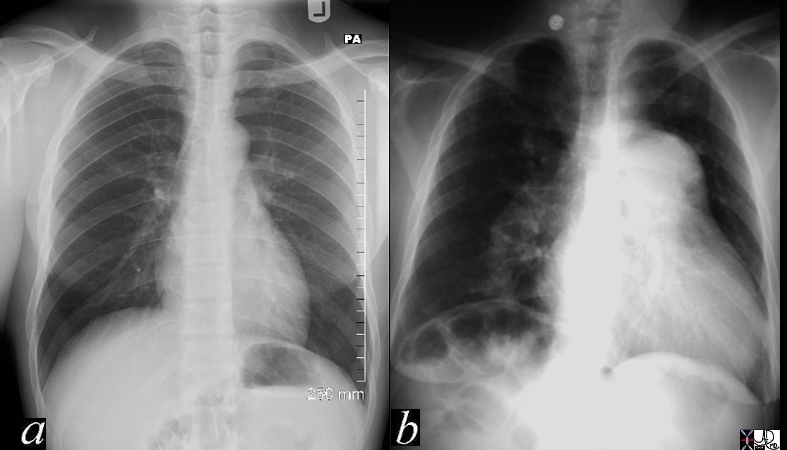
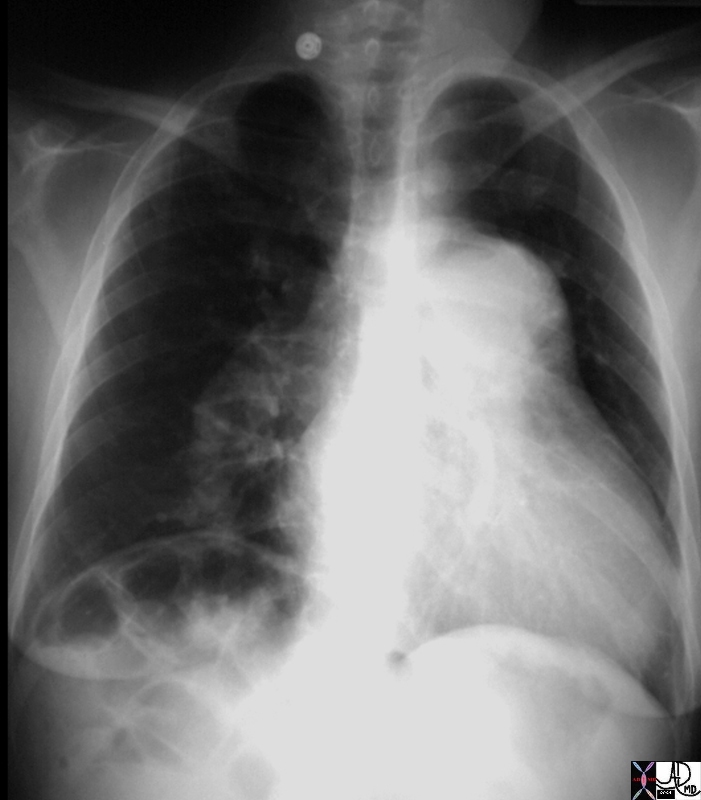
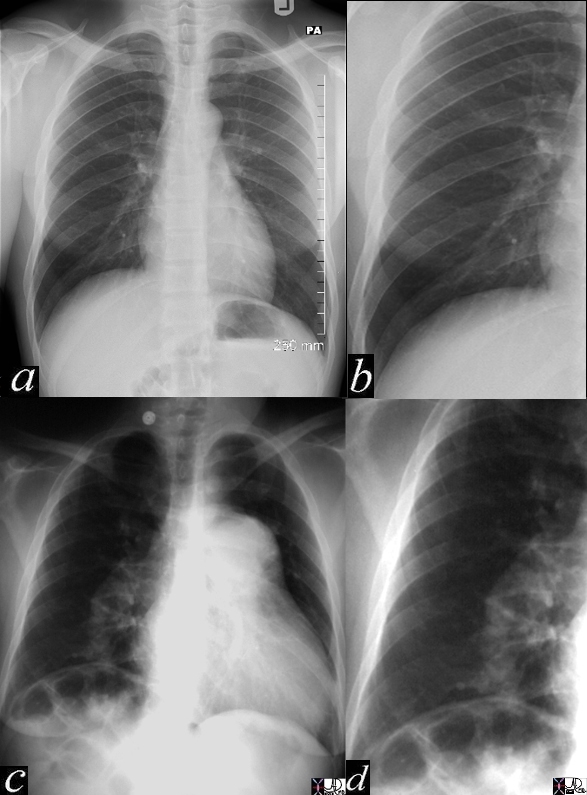
Normal and Pulmonary Hypertension
These two P-A chest X-rays show a normal cardiomediastinal image on the left and an enlarged MPA and RPA on the right in this patient with pulmonary hypertension. Courtesy Ashley Davidoff MD (22089 c) code lung main pulmonary artery MPA RPA large hypertension heart cardiac imaging plain film CXR
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal and Pulmonary Hypertension
These two P-A chest X-rays show a normal cardiomediastinal image on the left and an enlarged MPA and RPA on the right in this patient with pulmonary hypertension. Courtesy Ashley Davidoff MD (22089 c) code lung main pulmonary artery MPA RPA large hypertension heart cardiac imaging plain film CXR
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => These two P-A chest X-rays show a normal cardiomediastinal image on the left and an enlarged MPA and RPA on the right in this patient with pulmonary hypertension. Courtesy Ashley Davidoff MD (22089 c) code lung main pulmonary artery MPA RPA large hypertension heart cardiac imaging plain film CXR
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => These two P-A chest X-rays show a normal cardiomediastinal image on the left and an enlarged MPA and RPA on the right in this patient with pulmonary hypertension. Courtesy Ashley Davidoff MD (22089 c) code lung main pulmonary artery MPA RPA large hypertension heart cardiac imaging plain film CXR
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal and Pulmonary Hypertension
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal and Pulmonary Hypertension
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Pulmonary Hypertension – Scleroderma
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Pulmonary Hypertension – Scleroderma
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Pulmonary Hypertension – Scleroderma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Pulmonary Hypertension – Scleroderma
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Pulmonary Hypertension
Pulmonary Hypertension – Scleroderma
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
Normal and Pulmonary Hypertension
These two P-A chest X-rays show a normal cardiomediastinal image on the left and an enlarged MPA and RPA on the right in this patient with pulmonary hypertension. Courtesy Ashley Davidoff MD (22089 c) code lung main pulmonary artery MPA RPA large hypertension heart cardiac imaging plain film CXR
Normal and Pruning
15406c05 heart cardiac right ventricle RV fx enlarged MPA main pulmonary artery fx enlarged pulmonary arteries DD ASD VSD PDA septal defects Eisenmenger’s CXR plain X-ray of chest Davidoff MD fx pruned pruning dx Eisenmenger’s Davidoff MD 15406.800 15406c02 15406c04 15406c05
Scleroderma Pulmonary Hypertension and Right Heart Failure
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
Normal, Dilated, and Hypertrophied Right Ventricles
These three images represent T1 weighted images of the RV reflecting normal, dilated, and hypertrophied conditions. Normal thin-walled capacious RV (1) ASD (Atrial Septal Defect) with volume overloaded – thin-walled but dilated RV (2) Pressure overloaded , hypertrophied RV, with accentuated trabeculations (3) Courtesy of Ashley Davidoff M.D. 32095
Web References
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Pulmonary Hypertension
Pulmonary Hypertension – Scleroderma
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
Normal and Pulmonary Hypertension
These two P-A chest X-rays show a normal cardiomediastinal image on the left and an enlarged MPA and RPA on the right in this patient with pulmonary hypertension. Courtesy Ashley Davidoff MD (22089 c) code lung main pulmonary artery MPA RPA large hypertension heart cardiac imaging plain film CXR
Normal and Pruning
15406c05 heart cardiac right ventricle RV fx enlarged MPA main pulmonary artery fx enlarged pulmonary arteries DD ASD VSD PDA septal defects Eisenmenger’s CXR plain X-ray of chest Davidoff MD fx pruned pruning dx Eisenmenger’s Davidoff MD 15406.800 15406c02 15406c04 15406c05
Scleroderma Pulmonary Hypertension and Right Heart Failure
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
Normal, Dilated, and Hypertrophied Right Ventricles
These three images represent T1 weighted images of the RV reflecting normal, dilated, and hypertrophied conditions. Normal thin-walled capacious RV (1) ASD (Atrial Septal Defect) with volume overloaded – thin-walled but dilated RV (2) Pressure overloaded , hypertrophied RV, with accentuated trabeculations (3) Courtesy of Ashley Davidoff M.D. 32095
Web References
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => These three images represent T1 weighted images of the RV reflecting normal, dilated, and hypertrophied conditions. Normal thin-walled capacious RV (1) ASD (Atrial Septal Defect) with volume overloaded – thin-walled but dilated RV (2) Pressure overloaded , hypertrophied RV, with accentuated trabeculations (3) Courtesy of Ashley Davidoff M.D. 32095
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => These three images represent T1 weighted images of the RV reflecting normal, dilated, and hypertrophied conditions. Normal thin-walled capacious RV (1) ASD (Atrial Septal Defect) with volume overloaded – thin-walled but dilated RV (2) Pressure overloaded , hypertrophied RV, with accentuated trabeculations (3) Courtesy of Ashley Davidoff M.D. 32095
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal, Dilated, and Hypertrophied Right Ventricles
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal, Dilated, and Hypertrophied Right Ventricles
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Scleroderma Pulmonary Hypertension and Right Heart Failure
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Scleroderma Pulmonary Hypertension and Right Heart Failure
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 15406c05 heart cardiac right ventricle RV fx enlarged MPA main pulmonary artery fx enlarged pulmonary arteries DD ASD VSD PDA septal defects Eisenmenger’s CXR plain X-ray of chest Davidoff MD fx pruned pruning dx Eisenmenger’s Davidoff MD 15406.800 15406c02 15406c04 15406c05
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 15406c05 heart cardiac right ventricle RV fx enlarged MPA main pulmonary artery fx enlarged pulmonary arteries DD ASD VSD PDA septal defects Eisenmenger’s CXR plain X-ray of chest Davidoff MD fx pruned pruning dx Eisenmenger’s Davidoff MD 15406.800 15406c02 15406c04 15406c05
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 5
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal and Pruning
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal and Pruning
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => These two P-A chest X-rays show a normal cardiomediastinal image on the left and an enlarged MPA and RPA on the right in this patient with pulmonary hypertension. Courtesy Ashley Davidoff MD (22089 c) code lung main pulmonary artery MPA RPA large hypertension heart cardiac imaging plain film CXR
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => These two P-A chest X-rays show a normal cardiomediastinal image on the left and an enlarged MPA and RPA on the right in this patient with pulmonary hypertension. Courtesy Ashley Davidoff MD (22089 c) code lung main pulmonary artery MPA RPA large hypertension heart cardiac imaging plain film CXR
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal and Pulmonary Hypertension
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal and Pulmonary Hypertension
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Pulmonary Hypertension – Scleroderma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Pulmonary Hypertension – Scleroderma
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 9
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Pulmonary Hypertension
Pulmonary Hypertension – Scleroderma
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
Normal and Pulmonary Hypertension
These two P-A chest X-rays show a normal cardiomediastinal image on the left and an enlarged MPA and RPA on the right in this patient with pulmonary hypertension. Courtesy Ashley Davidoff MD (22089 c) code lung main pulmonary artery MPA RPA large hypertension heart cardiac imaging plain film CXR
Normal and Pruning
15406c05 heart cardiac right ventricle RV fx enlarged MPA main pulmonary artery fx enlarged pulmonary arteries DD ASD VSD PDA septal defects Eisenmenger’s CXR plain X-ray of chest Davidoff MD fx pruned pruning dx Eisenmenger’s Davidoff MD 15406.800 15406c02 15406c04 15406c05
Scleroderma Pulmonary Hypertension and Right Heart Failure
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
Normal, Dilated, and Hypertrophied Right Ventricles
These three images represent T1 weighted images of the RV reflecting normal, dilated, and hypertrophied conditions. Normal thin-walled capacious RV (1) ASD (Atrial Septal Defect) with volume overloaded – thin-walled but dilated RV (2) Pressure overloaded , hypertrophied RV, with accentuated trabeculations (3) Courtesy of Ashley Davidoff M.D. 32095
Web References
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Pulmonary Hypertension
Pulmonary Hypertension – Scleroderma
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
Normal and Pulmonary Hypertension
These two P-A chest X-rays show a normal cardiomediastinal image on the left and an enlarged MPA and RPA on the right in this patient with pulmonary hypertension. Courtesy Ashley Davidoff MD (22089 c) code lung main pulmonary artery MPA RPA large hypertension heart cardiac imaging plain film CXR
Normal and Pruning
15406c05 heart cardiac right ventricle RV fx enlarged MPA main pulmonary artery fx enlarged pulmonary arteries DD ASD VSD PDA septal defects Eisenmenger’s CXR plain X-ray of chest Davidoff MD fx pruned pruning dx Eisenmenger’s Davidoff MD 15406.800 15406c02 15406c04 15406c05
Scleroderma Pulmonary Hypertension and Right Heart Failure
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
Normal, Dilated, and Hypertrophied Right Ventricles
These three images represent T1 weighted images of the RV reflecting normal, dilated, and hypertrophied conditions. Normal thin-walled capacious RV (1) ASD (Atrial Septal Defect) with volume overloaded – thin-walled but dilated RV (2) Pressure overloaded , hypertrophied RV, with accentuated trabeculations (3) Courtesy of Ashley Davidoff M.D. 32095
Web References
)