adenocarcinoma, e.g. gastrointestinal tract, breast
sarcoma
Congenital Growth Abnormalities
Pulmonary sequestration
Mechanical
`Bullae or cysts with air fluid level
Pneumatoceles from trauma
Circulatory
Vasculitis (eg, granulomatosis with polyangiitis)
Pulmonary embolism with infarction
Other
Pulmonary Langerhans histiocytosis
Foreign body aspiration
Pulmonary embolism with infarction
Vasculitis (eg, granulomatosis with polyangiitis)
Neoplasm (eg, bronchogenic cancer, lymphoma, and metastatic head and neck, bladder, colon, pancreatic, and uterine cancer).
Pulmonary sequestration
Bullae or cysts with air fluid level
Bronchiectasis
Cryptogenic organizing pneumonia
Sarcoidosis
Rheumatoid nodules
Pulmonary Langerhans histiocytosis
Foreign body aspiration
Infection
TB
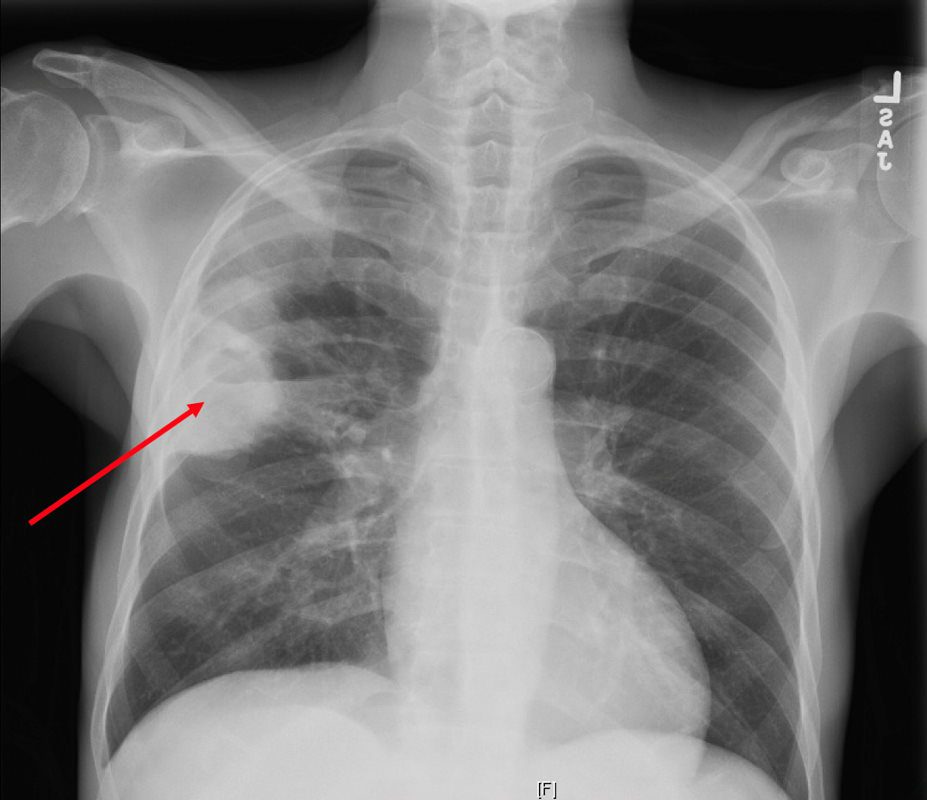
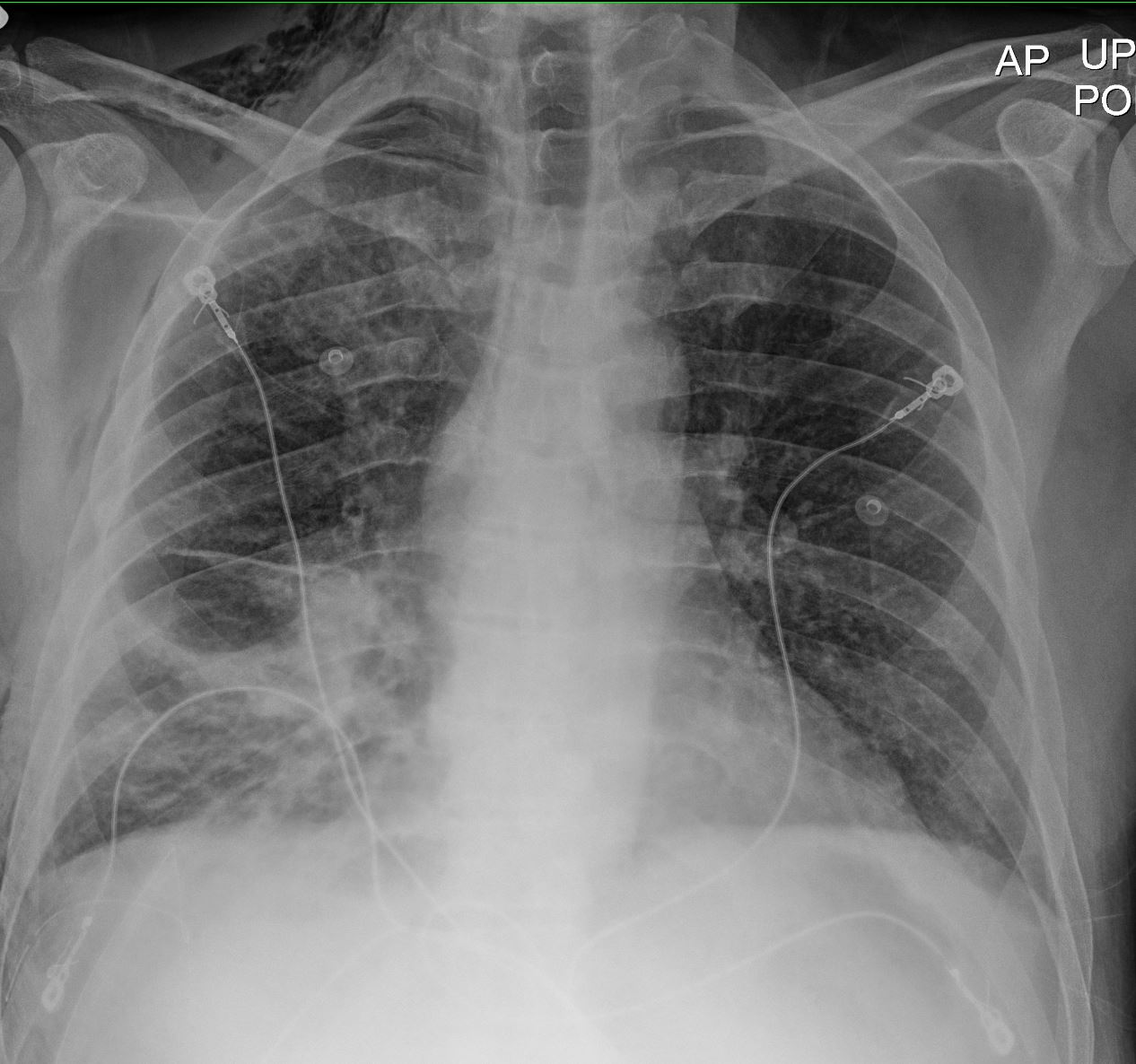
Reactivation TB CXR reveals a dense consolidation in the right upper lobe (red arrow) with questionable air-fluid level. No pneumothorax. No pleural effusions. Differential includes right upper lobe pneumonia or tuberculosis. CT is recommended for further evaluation if there is concern for a cavity. Courtesy Joseph Cannella, Dr. Christina LeBedis, MD, MS
CTPA reveals a large consolidation in the right upper lobe and superior segment of the right lower lobe spans approximately 8.8 x 5.6 x 9.4 cm and extends to the pleura. There are multiple internal cavitations (red arrows) with air-fluid levels. These large predominately right upper lobe cavitary lesions are consistent with clinical concern for tuberculosis pneumonia, however follow-up with chest CT in 3 months post-treatment is recommended to exclude other less likely causes of cavitary lesions, such as malignancy. Courtesy Joseph Cannella, Dr. Christina LeBedis, MD, MS
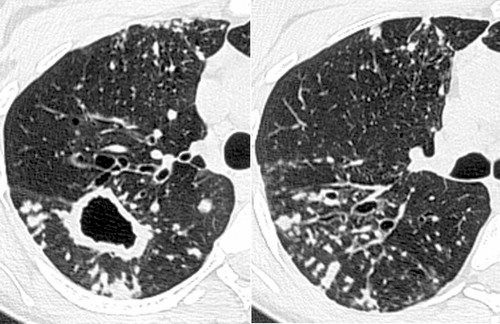
Postprimary active tuberculosis in a 34-year-old man with weight loss and a chronic cough. (a) High-resolution CT scan of the left lung shows a thick-walled cavity and multiple peripheral small nodules and branching linear structures (arrows). Note the thickening of the bronchial walls (arrowhead). (b) Photomicrograph (original magnification, ×400; hematoxylin-eosin stain) shows impacted caseous material (*) in small peripheral airways (arrow). Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
Infection with M avium-intracellulare complex in a 44-year-old woman with malaise and a chronic cough. High-resolution CT scans of the right lung show multiple peripheral small nodules connected to branching linear opacities and a thick-walled cavity in the superior segment of the lower lobe. Note the thickening of the bronchial walls, bronchial dilatation, and mucus impaction. The diagnosis was confirmed with bronchoalveolar lavage. Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
62 M cavitatating nodule from necrotizing strep intermedius infection 3 months prior
62 M cavitatating nodule necrotizing strep intermedius infection 001 CT 3 months prior Ashley Davidoff MD thecommonvein.net
3 months later following Augmentin Rx
62 M cavitatating nodule necrotizing strep intermedius infection 3 months later CT post Rx augmentin Ashley Davidoff MD thecommonvein.net
Infection
TB
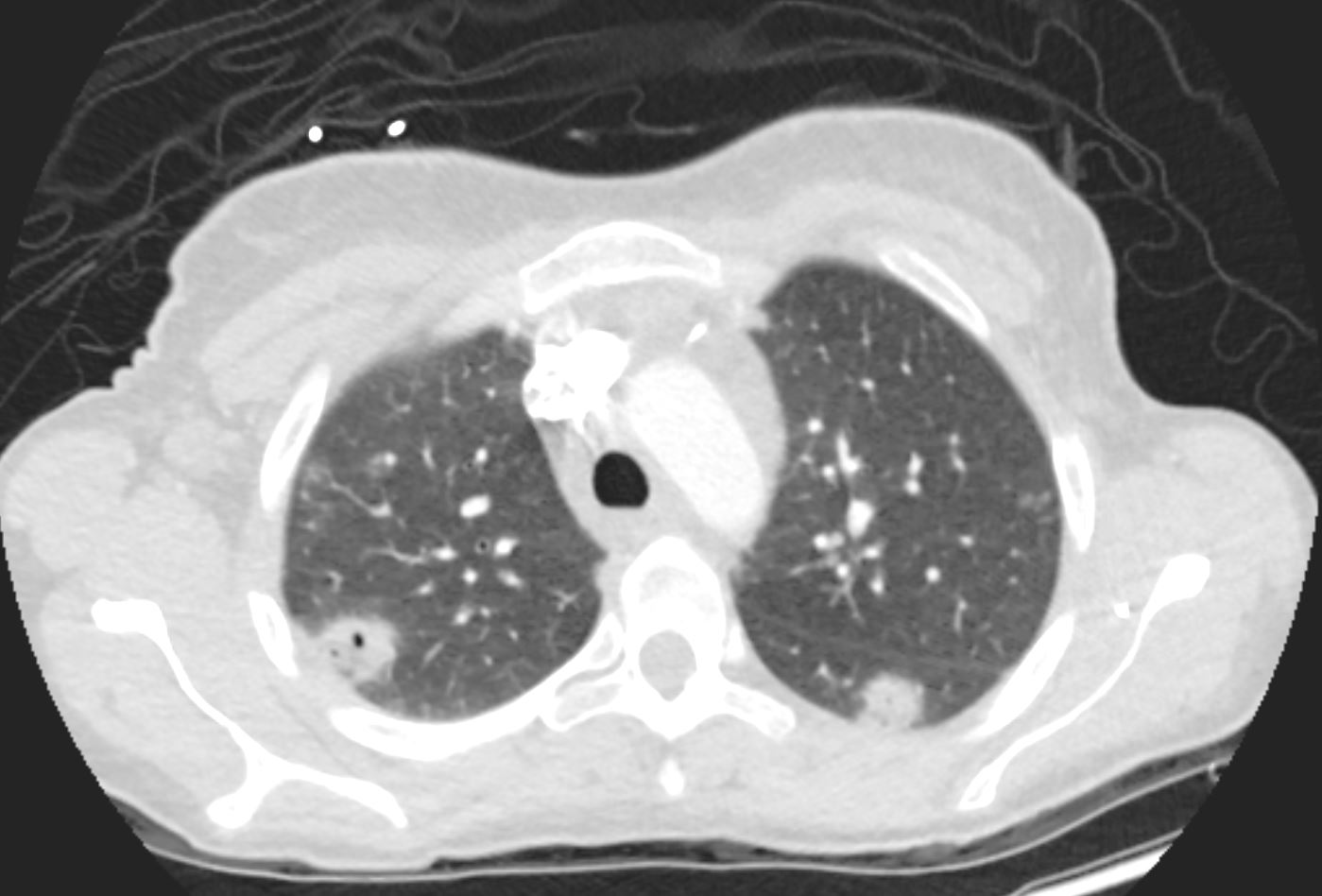
50M with Cavitating Nodule on CXR BAL yielded Mycobacterium Mycobacterium Kansasii Ashley Davidoff MD TheCommonVein.net 50M with Cavitating Nodule on CT scan. BAL yielded Mycobacterium Kansasii Ashley Davidoff MD TheCommonVein.net
Septic Emboli
24 year old female with bacterial endocarditis with multiple pulmonary emboli, some cavitating. The CXR shows multiple foci of consolidation with a wedge shaped defect in the posterior segment of the left upper lobe consistent with a Hamptons hump caused by an embolic infarction Ashley Davidoff MD TheCommonvein.net 24f PE Hampton’s hump 001 24 year old female with bacterial endocarditis with multiple pulmonary emboli, some cavitating. The CT shows multiple foci of consolidation with a foci of consolidations in the posterior segments of the upper lobes bilaterally The focal consolidation in the right upper lobe is cavitating Ashley Davidoff MD TheCommonvein.net 24f PE Hampton’s hump 002 24 year old female with bacterial endocarditis with multiple pulmonary emboli, some cavitating. The CT scan shows a wedge shaped conglomerate region of cosolidation in the posterior segment of the left upper lobe consistent with a Hamptons hump caused by an embolic infarction Ashley Davidoff MD TheCommonvein.net 24f PE Hampton’s hump 003
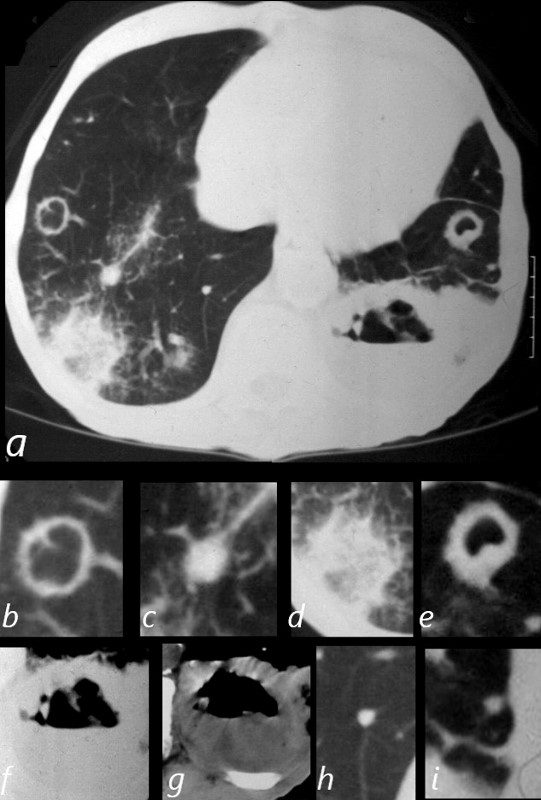
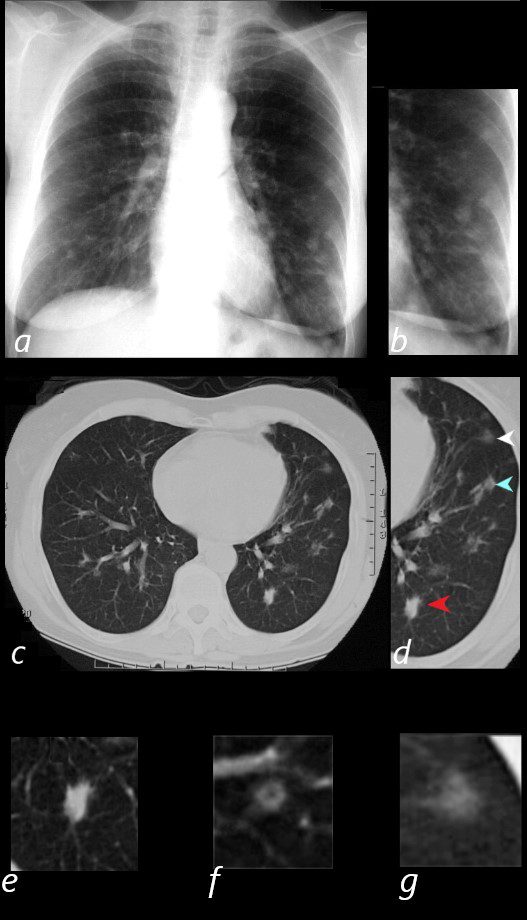
CAVITATING NODULES, HALO SIGN IN WEGENER?S GRANULOMATOSIS WITH POLYANGIITIS, GPA. 81-year-old male with weight loss, renal failure, and hemoptysis CT axial view (a) shows cavitating masses in the upper lobes bilaterally magnified (b and e). In addition there is a large necrotic mass with an air fluid level in the left lower lobe (a), magnified ( f and g). A mass with a halo sign noted in the RLL is magnified in d, and scattered bilateral smaller nodules are magnified (c and h) in the RLL and in (i) in the LLL . Priscilla Slanetz MPH MD NODULES OF WEGENER”S GRANULOMATOSIS, aka GRANULOMATOSIS WITH POLYANGIITIS, GPA 65 year old female presents with epistaxis and with nodular changes on CXR (a) magnified in b. CT scan in axial projection (c) and magnified in d, reveals 3 types of nodules. A spiculated solid nodule (red arrow head) is magnified in e, a bronchocentric nodule (teal arrowhead) is magnified in e. This may represent a cavitating nodule or hemorrhagic change around a bronchiole (cheerio sign) A ground glass nodule (white arrowhead) is magnified in g. Ashley Davidoff MD
Cancer
Bubble Lucencies – Pseudocavitation
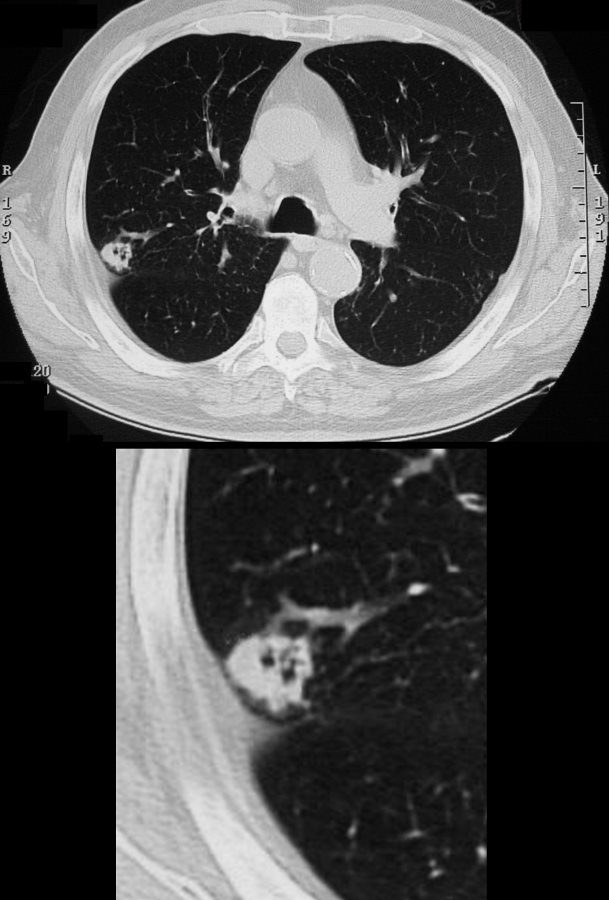
Bubble Lucencies (Pseudocavitation) “Nodules containing round or oval foci of air attenuation are highly suspicious for malignancy, particularly lung adenocarcinoma ( Fig. 4.9 ). These bubble lucencies (synonym: pseudocavitations) are rarely identified in benign lesions. Correlation with pathologic findings has shown that the lucencies usually represent patent airways, often ectatic, or foci of emphysema surrounded by carcinoma.” radiologykey.com
Bubble Lucencies
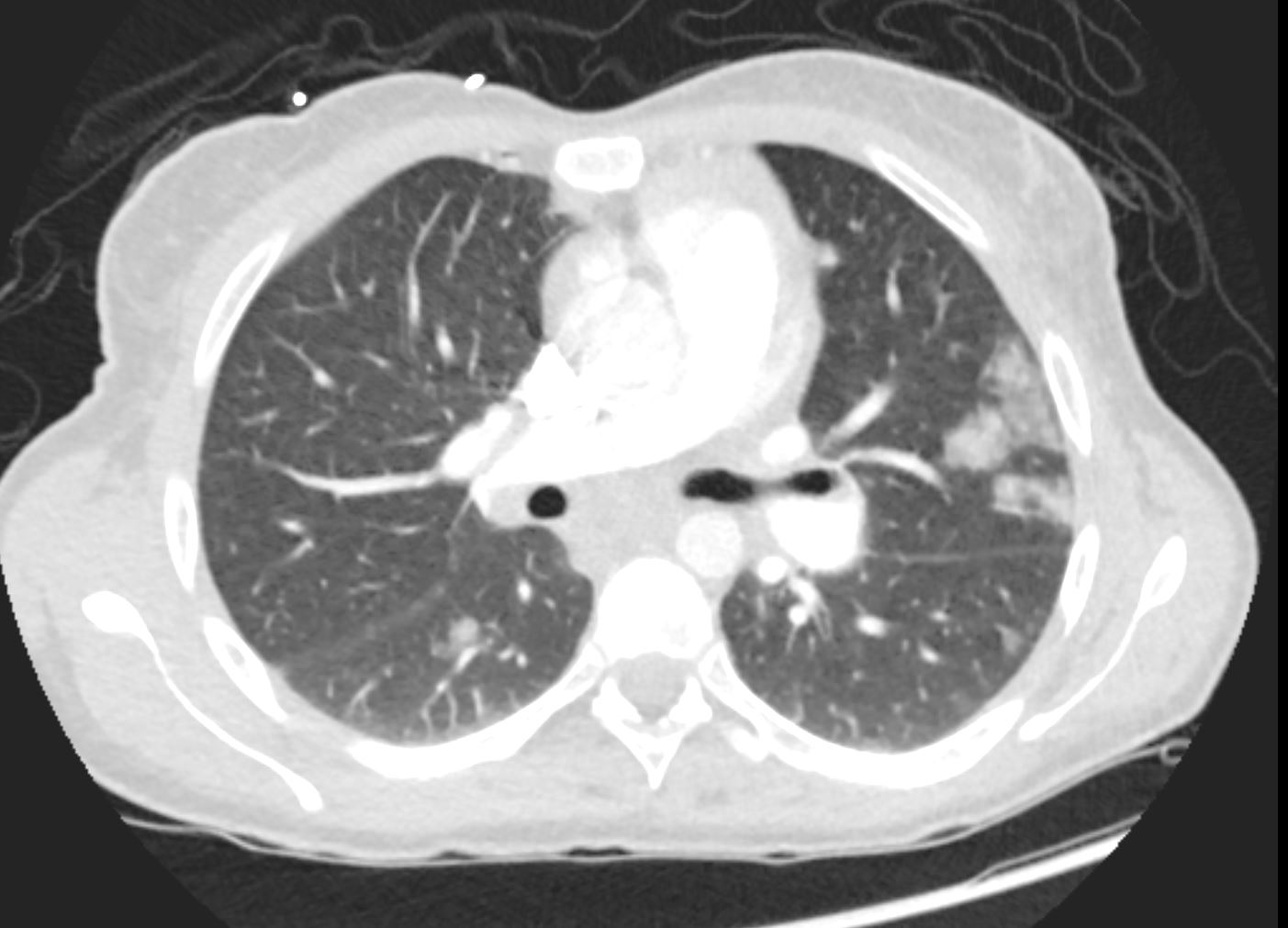
Cavitating Squamous Cell Carcinoma 65 year male with peripheral lung nodule characterized by cavitation that was not present 2 years earlier . Pathology revealed squamous cell carcinoma Ashley Davidoff TheCommonVein.net
Cavitating Head and Neck Squamous Carcinoma
64 year old male with cavitating metastasis from head and neck squamous cell carcinoma Ashley Davidoff MD TheCommonVein.net
Cavitating Pneumonia
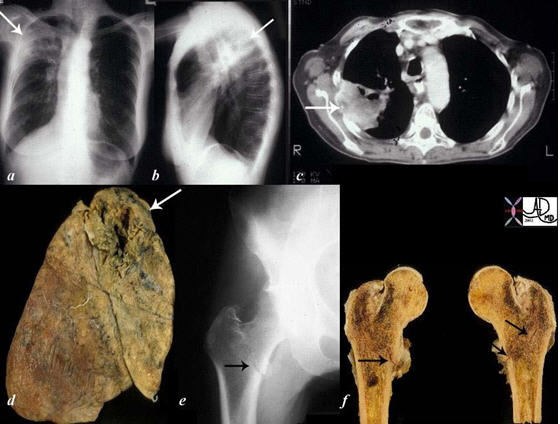
Peripheral Large Upper Lobe Mass with Cavitation The collage of images reflects a patient with stage IV, cavitating, primary, squamous carcinoma of the right upper lobe (RUL) (a, b, c, d – white arrows) with COPD. A metastatic lesion to the right femur was complicated by a pathological fracture. (e, f black arrows). Courtesy Ashley Davidoff, M.D. TheCommonVein.net Lung cancer P 018