
Etymology
- Derived from the Latin word linea, meaning “line,” and the Greek word atelectasis, meaning “incomplete expansion.”
AKA
- Discoid atelectasis
- Plate atelectasis
What is it?
- Linear atelectasis refers to a focal, thin, linear area of lung collapse, typically seen on imaging, often due to transient or reversible factors.
- Frequently an incidental finding and asymptomatic, especially in postoperative or immobile patients.
Characterised by
- Thin, linear, band-like opacity on imaging.
- Represents partial collapse of a small area of lung parenchyma.
- Frequently located in dependent regions of the lungs.
Anatomically affecting
- Commonly affects the lower lobes and subsegmental areas, particularly in dependent portions of the lungs.
Pathophysiology
- Results from decreased alveolar inflation due to hypoventilation, obstruction, or compression.
- Air absorption from poorly ventilated alveoli leads to localized volume loss.
Causes include
- Most Common Causes
- Postoperative hypoventilation or bedrest.
- Pleural effusion causing compression of lung parenchyma.
- Other Causes include:
- Infection: Pneumonia causing adjacent atelectasis.
- Inflammation: Radiation pneumonitis or chronic inflammatory lung disease.
- Neoplasm: Adjacent mass effect causing local atelectasis.
- Mechanical: Mucus plugging, foreign body aspiration.
- Trauma: Rib fractures leading to localized hypoventilation.
- Metabolic: Uremic pneumonitis causing secondary atelectasis.
- Circulatory: Hypoperfusion leading to hypoventilation.
- Immune: Autoimmune diseases like lupus or rheumatoid arthritis.
- Infiltrative: Pulmonary fibrosis causing localized atelectasis.
- Inherited and Congenital: Cystic fibrosis with mucus plugging.
- Iatrogenic: Postsurgical atelectasis, post-radiation fibrosis.
- Idiopathic: Idiopathic pulmonary fibrosis (IPF).
Histopathology
- Collapsed alveoli with possible minor inflammatory changes.
- Adjacent areas may show mild hyperinflation or compensatory changes.
Imaging Radiology
- Applied Anatomy to CT
- Parts: Linear bands of atelectasis within the lung parenchyma.
- Size: Thin (typically <5 mm in thickness) because it reflects the collapse of a small, superficial region of alveoli without involving deeper lung structures.
- Shape: Linear, band-like opacities.
- Position: Frequently seen in dependent regions (posterior or basal segments).
- Character: Non-specific linear opacity without mass effect.
- Time: Often transient; resolves with treatment of underlying cause or improved ventilation.
- Associated Findings: May co-exist with pleural effusion or adjacent consolidation.
- CXR
- Findings: Thin, linear opacities, often horizontal or oblique in orientation.
- Associated Findings: Basilar elevation in pleural effusion, mediastinal shift if significant volume loss.
Labs
- Dependent on underlying etiology:
- Elevated white blood cell count in infection.
- Markers of autoimmune disease in inflammatory causes.
PFTs
- Linear atelectasis typically does not cause abnormal pulmonary function tests (PFTs) because the affected lung volume is too small to significantly impact overall lung function.
Differential Diagnosis
- Subsegmental pneumonia (distinguished by associated airspace opacity).
- Scarring or fibrosis (more permanent and associated with distortion).
- Early pulmonary embolism-related changes.
Clinical relevance
- Frequently an incidental finding on imaging.
- Often asymptomatic and self-limiting in nature.
- Commonly associated with postoperative or immobility-related hypoventilation.
Recommendations
- Encourage deep breathing and physiotherapy to resolve atelectasis.
- Investigate underlying causes if persistent or recurrent.
- Use CT to rule out structural or neoplastic causes in unclear cases.
Key Points and Pearls
- Linear atelectasis is typically a transient and reversible finding.
- Most often related to hypoventilation or compression, particularly in dependent lung regions.
- Resolves with improved ventilation or treatment of the underlying cause.
- Recognizing its often benign and incidental nature is essential to avoid unnecessary interventions.
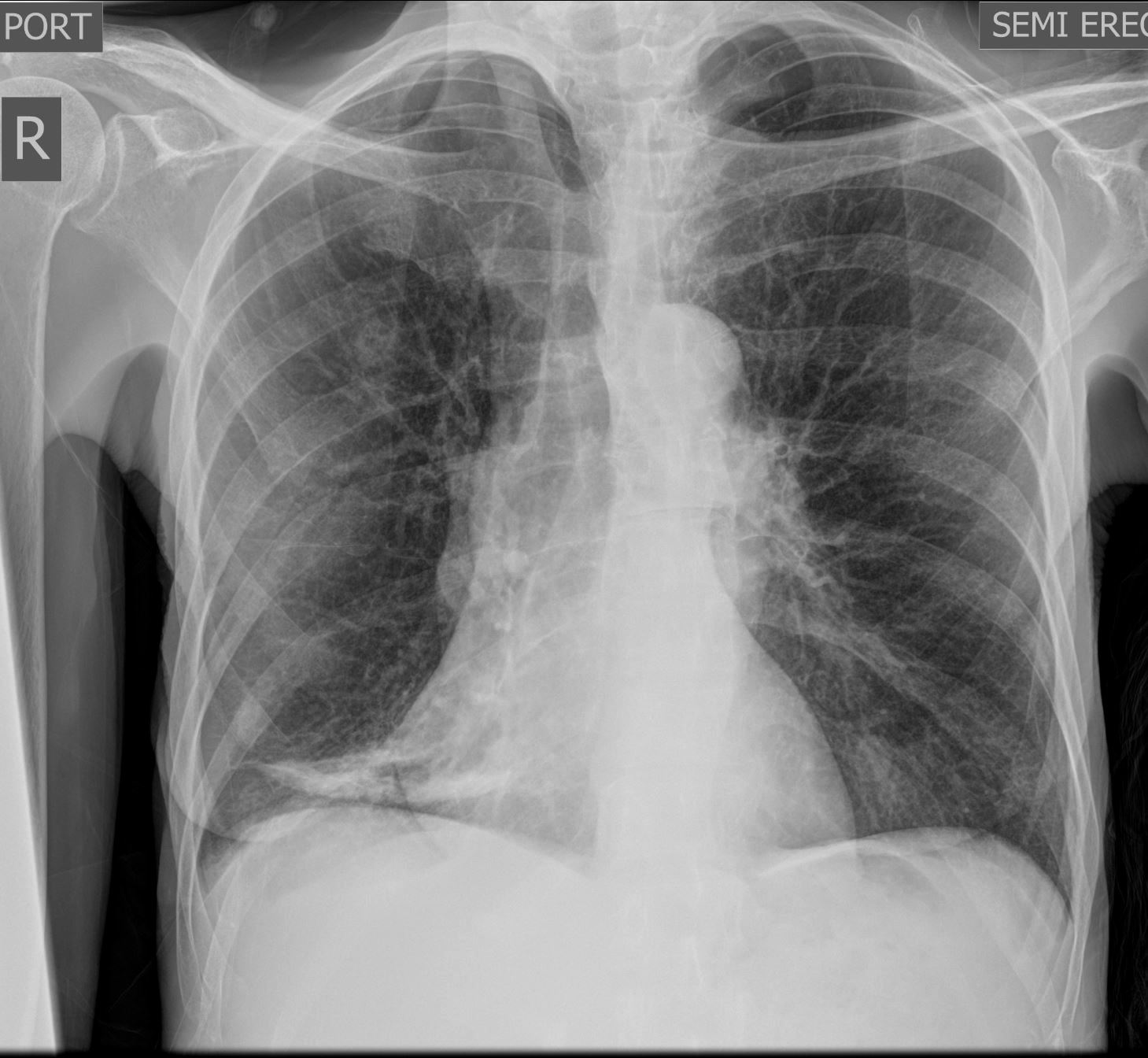
Frontal Chest Xray of a 55-year-old female shows a region of discoid atelectasis (aka linear atelectasis plate atelectasis ) in the right lower lung zone
Courtesy Ashley Davidoff MD TheCommonVein.net 136548
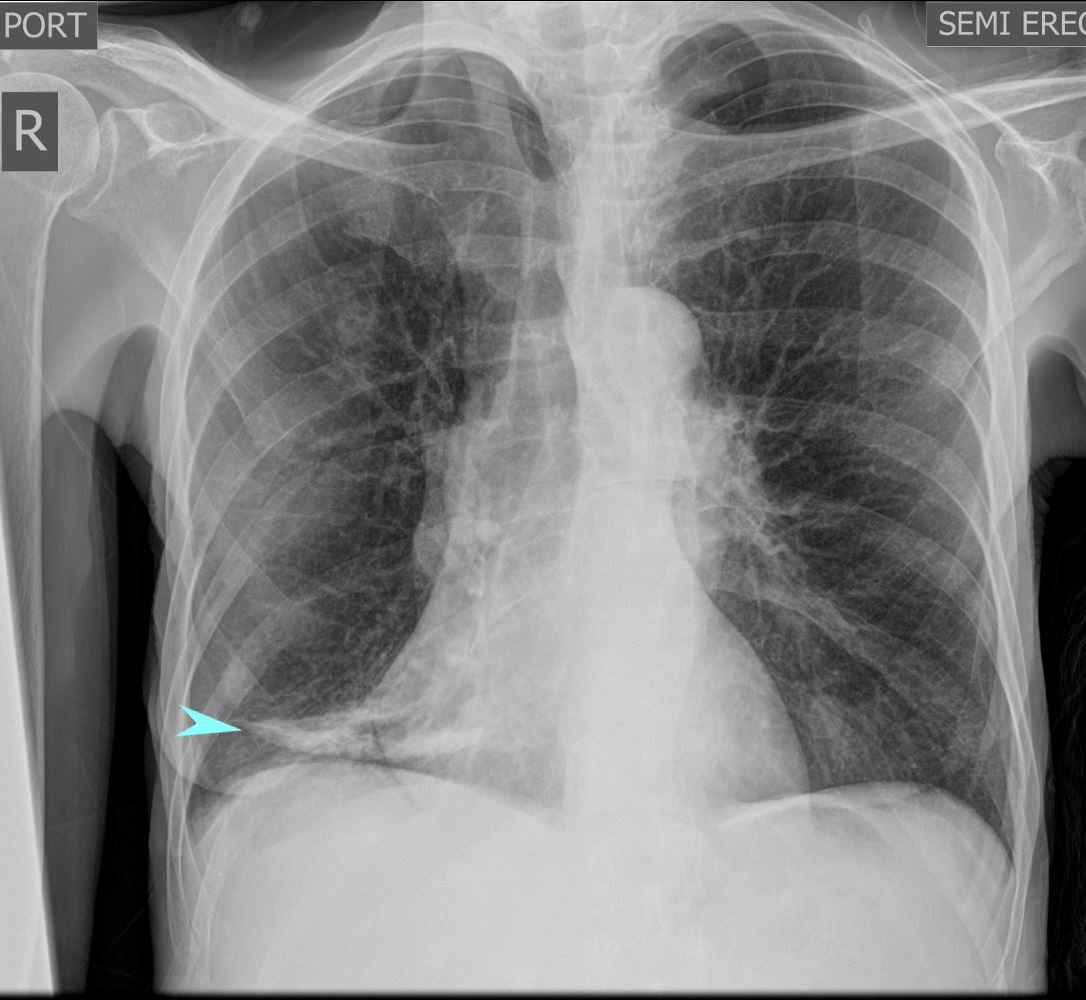
Frontal Chest Xray of a 55-year-old female shows a region of discoid atelectasis (aka linear atelectasis plate atelectasis ) in the right lower lung zone (teal arrow)
Courtesy Ashley Davidoff MD TheCommonVein.net 136548
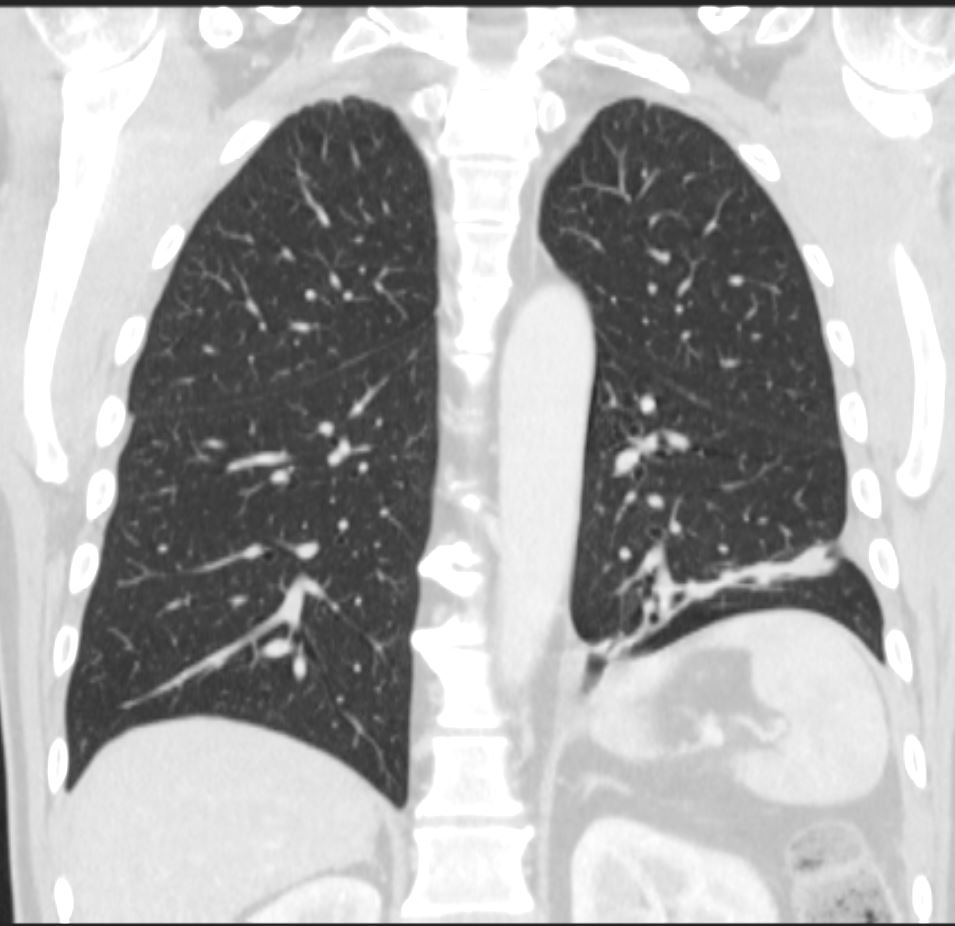
CT scan in the coronal plane 3 months later shows significant improvement of the atelectasis involving a basal segment of the left lower lobe associated with persistent elevation of the left hemidiaphragm indicating volume loss. The atelectasis now has a discoid, linear, or plate-like appearance
Ashley Davidoff MD TheCommonVein.net 276Lu 136238
aka discoid atelectasis aka plate-like atelectasis
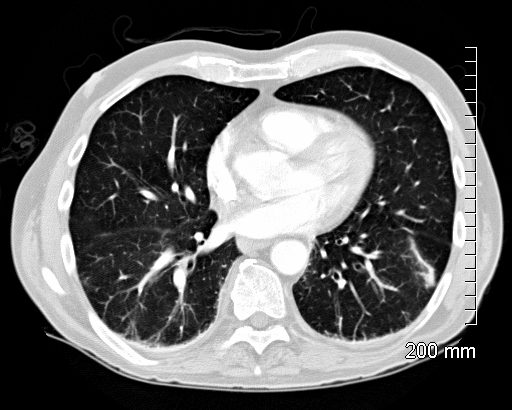
66 year old male with linear (discoid) atelectasis in the left lower lobe on CT
Ashley Davidoff MD TheCommonVein.net

60 year old male with linear (discoid) atelectasis in the middle lobe and the left upper lobe on CT. Note moderate sized bilateral pleural effusion. Minor compressive atelectasis caused by the left effusion.
Ashley Davidoff MD TheCommonVein.net
66 year old male with linear (discoid) atelectasis in the left lower lobe on CT
Ashley Davidoff MD TheCommonVein.net
Radiographic Appearance
- Linear Opacity: Appears as a thin, straight or slightly curvilinear band of increased density, usually 1?3 cm wide.
- Location: Often seen in the lower lobes of the lungs, particularly along the costophrenic angles.
- Orientation: Usually parallel to the pleural surface, often horizontal or oblique in alignment.
Common Causes
Linear or discoid atelectasis can result from various factors that cause localized alveolar collapse, including:
- Hypoventilation: Commonly occurs post-operatively or in patients with prolonged bed rest.
- Shallow Breathing: Seen in patients with pleuritic pain, rib fractures, or abdominal discomfort, as these conditions limit deep inspiration.
- Obstruction: Mucus plugging in smaller airways can cause localized atelectasis.
- Compression: External pressure from pleural effusion, a mass, or pneumothorax can collapse nearby alveoli.
Clinical Significance
Linear or discoid atelectasis is generally a benign finding and often transient. It does not usually indicate significant pathology, although it can sometimes be a marker of poor ventilation or underlying lung disease. It is important to differentiate it from more concerning findings, such as infiltrates or fibrotic bands, which may indicate chronic or progressive disease.
Summary
In radiographic terms, linear or discoid atelectasis is a thin, linear opacity representing areas of localized alveolar collapse, often due to hypoventilation or compression, and is typically a temporary and benign finding.
Links and References
Chat GPT – What is radiographic definition of linear or discoid atelectasis?