
1+1=1
In biology, and in the lung in this instance, units bond with other units in a given environment, and create a new and miraculous unit, bigger than the parts, and with greater functionality.
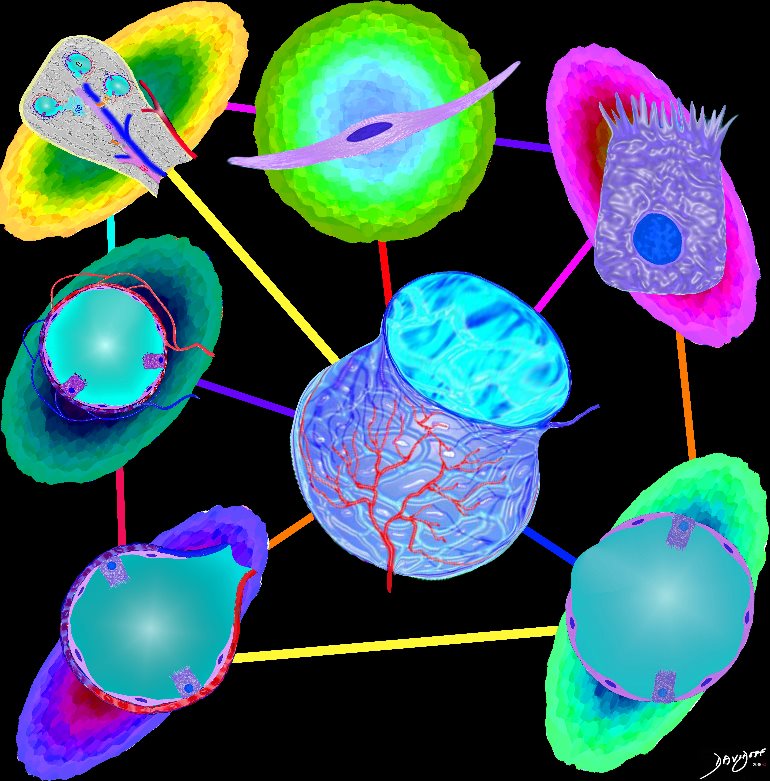
The Anatomical Units that Create the Whole Lung

The image shows some of the major components of the lung that when bonded create a new and powerful unit – a vital organ. In the center is an example of the airways and parenchyma making up the 2 lungs. At 12 o’clock the tracheo-bronchial tree with segmental and subsegmental airways. At 1 o?clock, is a cross section of the lungs showing some of the segments of the lung. At 5o?clock a cross section shows the arteries and veins of the lungs. At 7o?clock the drawing shows the pleura and pleural space of the lungs. At 9o?clock, a coronal reformat of the tracheobronchial tree shows the lymph node stations of the lungs. At 11 o?clock is the golden alveolus, the epicentral unit where gas exchange takes place
Ashley Davidoff MD TheCommonVein.net lungs-0696-lo res
The Secondary Lobule

The secondary lobule is subtended by the lobular arteriole (a) and the lobular bronchiole (b) which which in turn branches into the respiratory bronchioles, alveolar ducts, and nd alveolar sacs (c) The acinus (d) consists of a respiratory bronchiole and its associated alveolar ducts, sacs, and alveoli and represents the functional unit of the lung.
The secondary lobule is drained by the pulmonary venule (e) which runs in the interlobular septum also containing the lymphatics (f). The whole unit is housed and surrounded by a connective tissue framework (g) . The latter 3 structures form the interlobular septum.
Ashley Davidoff MD TheCommonVein.net 0751 -lo resL
The Microscopic Units that Make the Whole Functional Unit – Alveolus
Parts and Bonds
Ashley Davidoff MD
The Organelles That Make the Cell
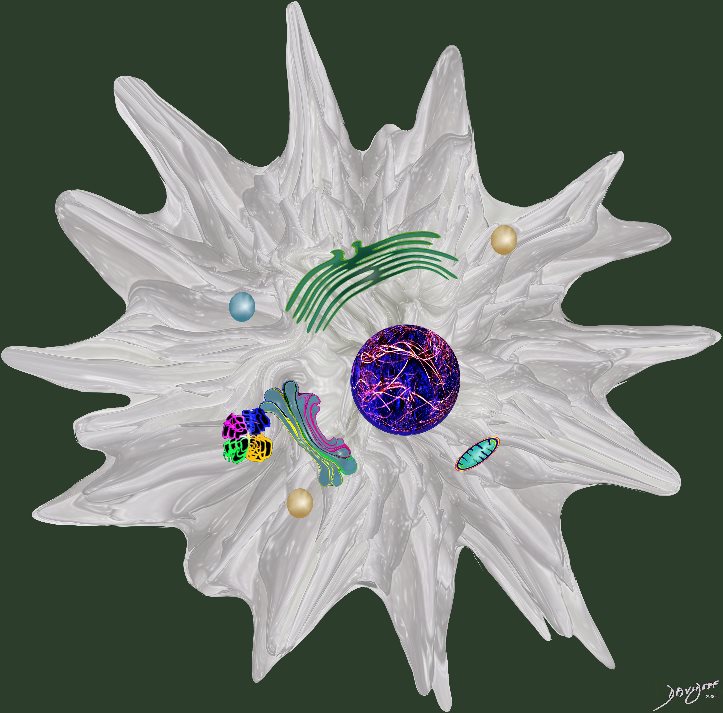
Ashley Davidoff MD
In the World of Medicine and Radiology
During life, the units are in a state of health (order) or disease (disorder), or somewhere in between. It is our function to identify disorder , and help bring disorder back to health.
Flux between order and disorder and health and disease
Courtesy
Ashley Davidoff MD TheCommonVein.net
order disorder-0002
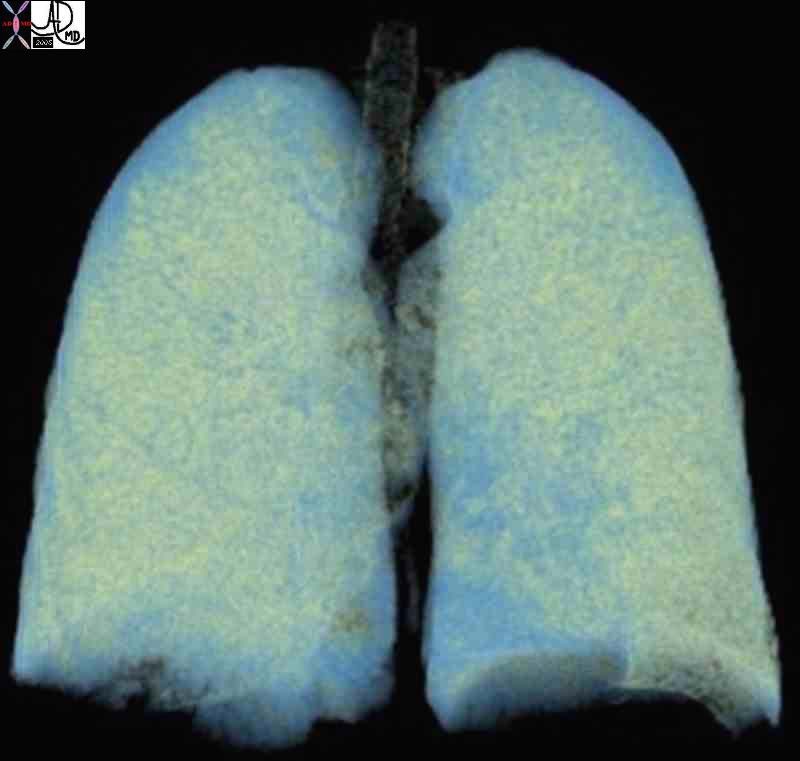
In the Lungs for example the imaging difference between healthy lungs and emphysematous lungs
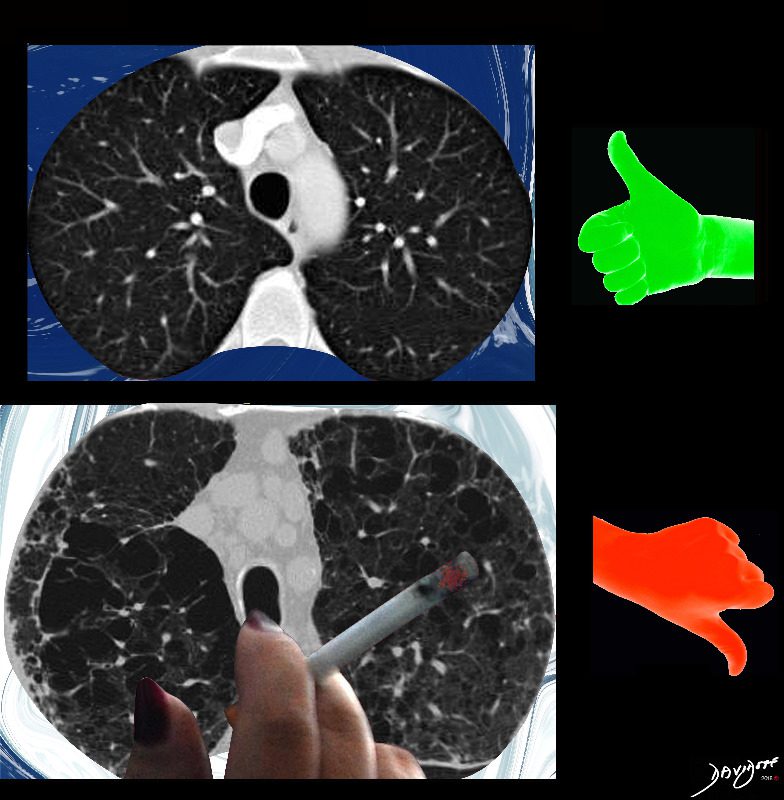
The imaging difference between healthy lungs (thumbs up) and emphysematous lungs (thumbs down)
Ashley Davidoff MD
TheCommonVeein.net lungs-0071-low-res

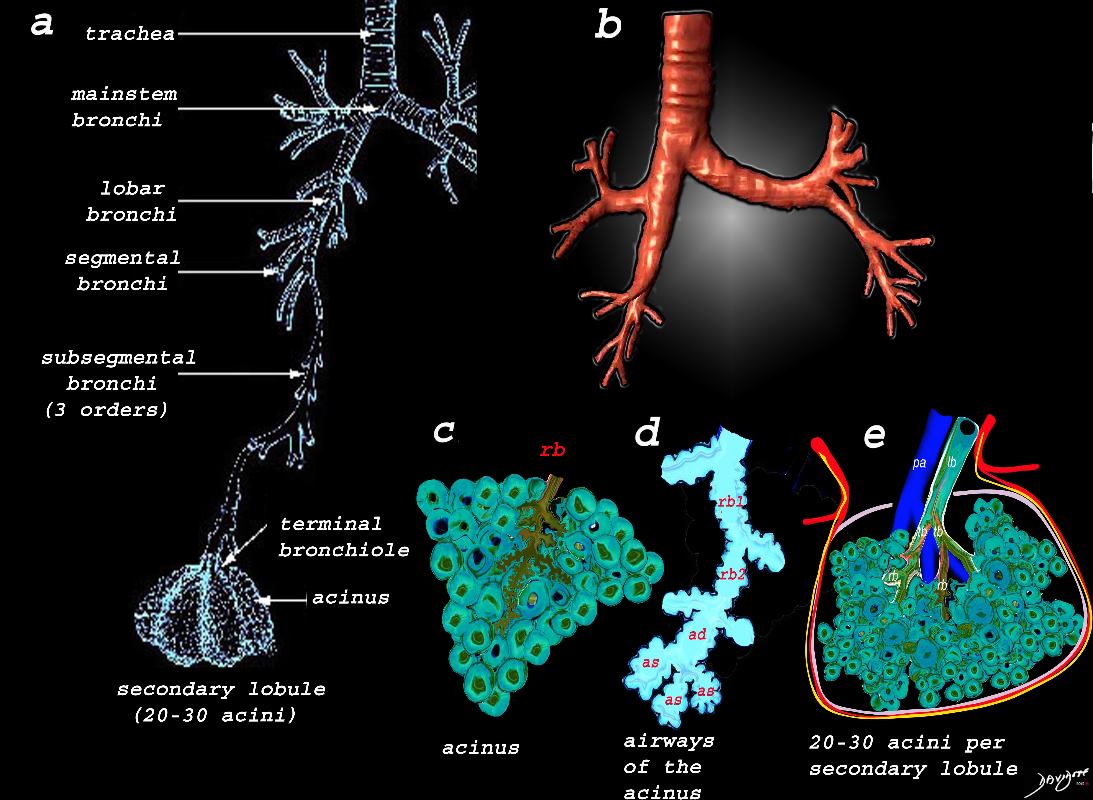
Image a shows the airways starting in the trachea and continuing to the mainstem bronchi, lobar bronchi, segmental bronchi, and subsegmental bronchi,. The subsegmental bronchi have 3 subsequent generations until the bronchiole is reached. The terminal bronchiole is the last of the transporting airways and is considered the most proximal small airway with a diameter of 2mm or less, and it gives rise to the respiratory bronchiole which is the feeding airway for the acinus . The acinus is the functional unit of the lung.
Image b is a 3D reconstruction of a CT scan showing the proximal airways from the trachea to the segmental airways.
Image c shows the structures that make up the acinus and the other parts of the small airways, starting with the respiratory bronchiole (rb) . The diagram in d, shows the detail of the small airways that participate in gas exchange, including the respiratory bronchiole, (rb) alveolar duct, (ad) and alveolar sac (as)
Image e shows the secondary lobule made from about 20-30 acini, arising from a single lobular bronchiole accompanied by a single pulmonary arteriole (pa).. Structure that surround and enclose the secondary lobule include the pulmonary venule, (red) lymphatics,(yellow) and a fibrous septum (pink).
Ashley Davidoff MD TheCommonVein.net
lungs-0739
42651c-1.jpg
This collage reflects the range of the respiratory system from the macroscopic and anatomic to the microscopic – a continuum of structure. Image 2 is a post-mortem specimen taken from the front and slightly above. It shows the trachea and bronchi supplying the two lungs above, with the aortic arch and cardiac structures in the middle and below. Note how pink the lungs are in this specimen from an unfortunate baby with congenital heart disease. Image 3, the chest X-ray, shows the lucent lungs within the thoracic cavity while image 4 is a diagram of the trilobed right lung and the bilobed left lung. Two respiratory units of the lung are shown in the next image each called a pulmonary lobule (5). The lobule consists of a central bronchiole (light blue) and pulmonary arteriole (dark blue), surrounded by the air filled acinus (teal) with its peripheral venules. (red) The acinus is magnified in the next image (6), showing first the tubular terminal bronchiole branching into the respiratory bronchioles, alveolar sacs, and finally the grape like alveoli. The organization of the connective tissues of the lung is shown in image 7. Finally we get down to the grapes or alveoli of the lung with surrounding vessels (8), and a single alveolus is seen in 9. It seems a long way for the air to travel but the system can deliver the air to and from the outside in a single breath, and exchange the gases at the capillary level even more rapidly. It is a remarkable system.42651c
keywords lung chest
Ashley Davidoff TheCommonVein.net
Large Airways and Small Airways
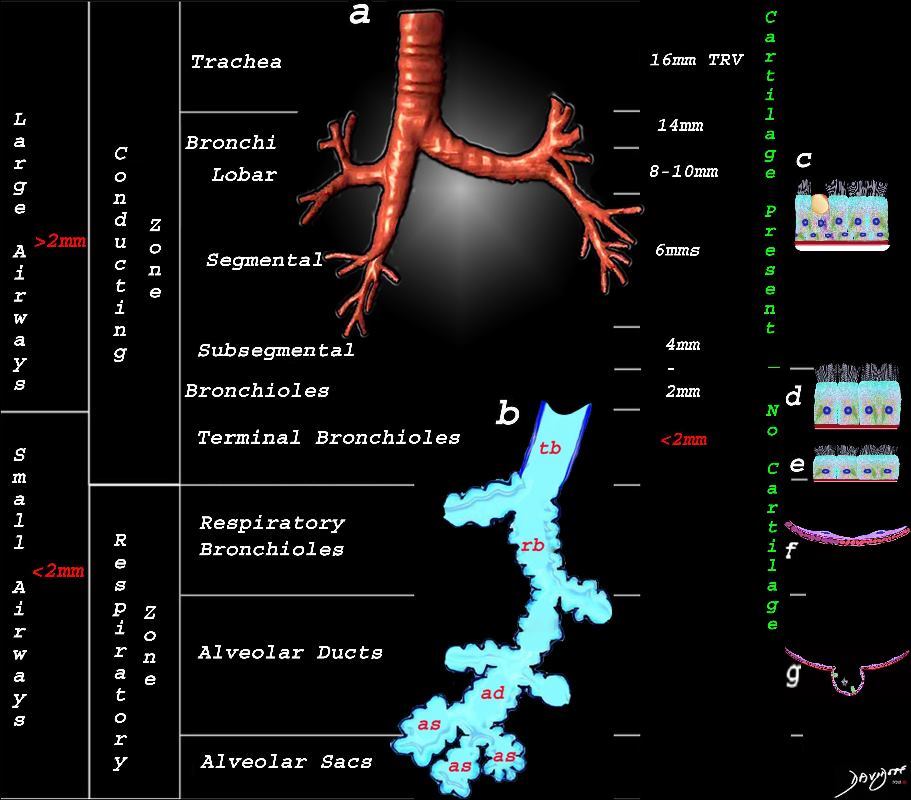
This image shows the division of the airways in the lungs classified as large airways and small airways.
A large airway is considered any airway larger than 2mm, and therefore includes all the airways involved with transport of air except for the terminal bronchiole. Included as seen in image a, are the trachea, mainstem bronchi, lobar bronchi segmental and subsegmental airways and the 3 subsequent divisions of subsegmental bronchi and bronchioles till the last transporting airway ? the respiratory bronchiole which is usually about 2mm and is considered a small airway Image (a) shows the airways starting in the trachea and continuing to the mainstem bronchi, lobar bronchi, segmental bronchi, and subsegmental bronchi.
Image b shows the structures that make up the small airways starting with the terminal bronchiole (tb) followed by the respiratory bronchiole (rb) alveolar duct, (ad) and alveolar sacs (as)
Image (c) shows the histologic makeup of the large airways that include a pseudostratified ciliated columnar epithelium with mucus secreting goblet cells a muscular layer (red) and a prominent cartilage layer (white) In the larger bronchioles (d) the epithelium remains as a pseudostratified, ciliated, columnar epithelium with prominent muscular layer (red). The columnar epithelium transitions to a stratified ciliated cuboidal epithelium by the terminal bronchiole s (f) both still with a muscular layer. The respiratory epithelium transitions from a cuboidal epithelium to a squamous epithelium (f) with alveoli and type I and II pneumocytes starting to branch (g)
Ashley Davidoff MD TheCommonVein.net lungs-0740nL


and progresses to involve more and more lung
The lungs are two huffing and puffing sponge-like organs that dominate the chest cavity, essential in their function as the principle structures of respiration. An understanding of their unique anatomy and physiology brings understanding of how diseases will affect the lungs, and how these changes will be manifest on x-ray and CT evaluation. In this first part of the series on the lung we emphasize principles, and outline how structure is integrated with function, disease and imaging.
The unique structural characteristics of the lungs include their:
- dominance in the chest cavity
- ability to accommodate the entire cardiac output with every heartbeat
- asymmetric nature
- irregular and dichotomous branch pattern of the bronchovascular bundle
- tubular transport system, with a single system functioning for both delivery and removal
- spongy air-filled character
- pyramidal or cone shape
- dual blood supply
The unique functional aspects include
- The ability to move air efficiently
- The ability to exchange gases efficiently
-
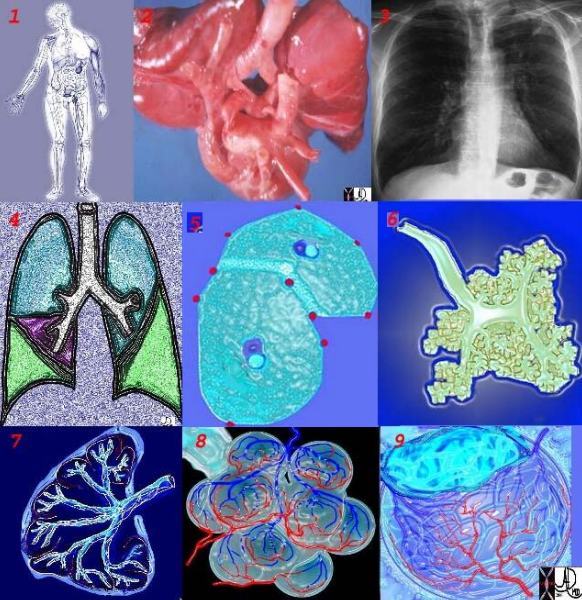
This collage reflects the range of the respiratory system from the macroscopic and anatomic to the microscopic – a continuum of structure. Image 2 is a post-mortem specimen taken from the front and slightly above. It shows the trachea and bronchi supplying the two lungs above, with the aortic arch and cardiac structures in the middle and below. Note how pink the lungs are in this specimen from an unfortunate baby with congenital heart disease. Image 3, the chest X-ray, shows the lucent lungs within the thoracic cavity while image 4 is a diagram of the trilobed right lung and the bilobed left lung. Two respiratory units of the lung are shown in the next image each called a pulmonary lobule (5). The lobule consists of a central bronchiole (light blue) and pulmonary arteriole (dark blue), surrounded by the air filled acinus (teal) with its peripheral venules. (red) The acinus is magnified in the next image (6), showing first the tubular terminal bronchiole branching into the respiratory bronchioles, alveolar sacs, and finally the grape like alveoli. The organization of the connective tissues of the lung is shown in image 7. Finally we get down to the grapes or alveoli of the lung with surrounding vessels (8), and a single alveolus is seen in 9. It seems a long way for the air to travel but the system can deliver the air to and from the outside in a single breath, and exchange the gases at the capillary level even more rapidly. It is a remarkable system. 42651c
keywords lung chest
Ashley Davidoff TheCommonVein.net
Overview
As we progress through the module there is a recurring pattern of the dual function of the respiratory apparatus ? an airway system that transports the air, and an exchange system that enables transfer of the gases across the alveolar membrane.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ashley Davidoff TheCommonVein.net 32634d02 32634b02
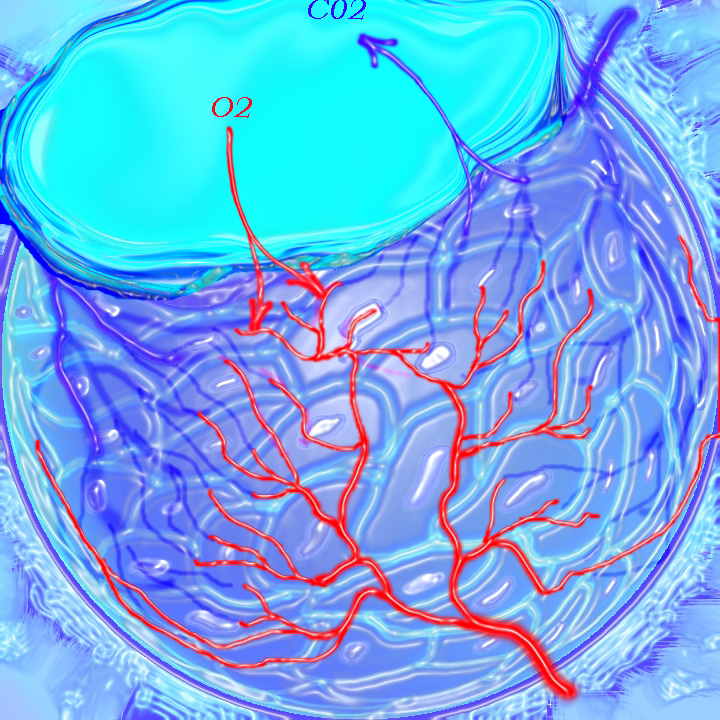
The lungs are part of a larger system called the respiratory system. The role of the lungs is to deliver ambient air (ventilation) to the alveoli and to act as the agent for gas exchange by contributing one layer of epithelium to the bilayered membrane, a double layer which serves as the ultimate interface for gas exchange. The primary role of the pulmonary arterial circulation is to transport blood to the alveolar interface (perfusion) and to also play a part in the exchange of carbon dioxide and oxygen by providing the second layer of the bi-layered filter. It is the homeostatic aim of the body to match the ventilation with the perfusion, in order to maintain uniform ventilation (V) to perfusion (Q) ratio (V/Q).
The lungs are exposed directly to the air in the atmosphere and to the blood within the circulatory system. Through the lungs the blood is therefore exposed to the atmosphere, which on the one hand contains life sustaining oxygen but on the other can present a hostile environment filled with microorganisms, industrial chemicals, and toxic fumes.
Ashley Davidoff TheCommonVein.net 42438b03
The lungs are made of expandable, sponge-like tissues. Their close proximity to the heart and circulatory system allows for rapid exchange of gases between the air and the circulatory system as noted above. This function is easily accomplished during rest, where resting respiratory rate in an adult is about 12 breaths per minute and heart rate 72 beats per minute. During exercise the respiratory rate can increase to 40-50 breaths per minute and the heart rate, increasing in concert, can reach 180-200 per minute. The interface of circulation with the respiratory system has to be sufficiently equipped to allow delivery, uptake, and exchange of gases at this accelerated pace. The key soldier in the exchange of oxygen is a complex protein called hemoglobin which lies in the red cell.
I imagine the hemoglobin molecule scurried by the forces of the right ventricle into the pulmonary circulation. As it enters the chambers of exchange, the open windows of the lungs herald the fresh air. Under basal conditions, the hemoglobin gnome can work at a leisurely pace filling his baskets with oxygen. Under exercise conditions he has to start working like crazy, grabbing molecules of oxygen and stacking these into his storage baskets, surrounded by an accelerated pace with gale-like air forces and flood-like blood conditions. Hemoglobin is a remarkable molecule and can adapt its function to these extremes in physiology.
Carbon dioxide from bodily metabolism is dissolved in the blood. Exchanges between the circulation and alveoli occur rapidly and efficiently across the alveolar membrane due to differences in the partial pressure of gas between the blood and the alveoli.
The presence of a structure in the body that is almost totally filled with air makes it a unique, challenging, and rewarding organ to examine clinically and radiologically. Examination of the lungs with a stethoscope enables the clinician to evaluate inspiratory and expiratory movement of air. Some pathologic conditions, including aspiration of a foreign body, collapsed lung, or inadvertent intubation of the bronchus, result in airway obstruction. In these conditions there is no air entry into the affected bronchus and subtended lung. The clinical finding of the lack of air entry, based simply on the lack of air sound, can be a life saving diagnostic maneuver.
Unusual but interesting words are used to describe the sounds of air character and movement on clinical examination. These include percussion, tactile fremitus, bronchophony, whispering pectoriloquy, and egophony and relate to the way air moves through the airways, and how the transmission may change when there is fluid in the pleural space or in the lungs. When the air mixes with the fluid, characteristic sounds such as rales and crepitus will result.

This artistic rendition of the heart and lungs uses the shape of fruit and vegetables to create an image of the chest. The lungs are made of grapes, the pulmonary arteries are made of carrots, the ribs are made of banana peel and the heat is made of a red pepper. 02032p Ashley Davidoff MD
TheCommonVein.net
{kind=link}
1-1-1-005-lo-res.jpg
1+1=1In biology, units bond with other units in a given environment, and create a new and miraculous unit, bigger than the parts and with greater functionality.
During life, the units are in a state of health (order) or disease (disorder), or somewhere in between. It is our function to identify disorder , and help bring disorder back to health.
Courtesy Ashley Davidoff MD TheCommonVein.net
The concept in 3 words is called “Units to Unity”