A comprehensive course on the anatomy of the great veins and how to apply that knowledge within medical imaging. by Dr. Ashley Davidoff
Introduction: Definition
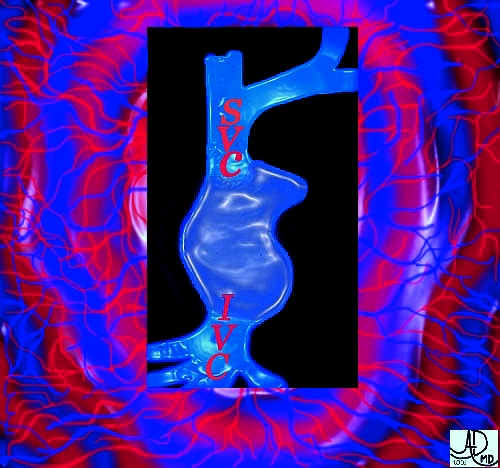
The venae cavae are the great veins of the body. They are the final common pathways for transport of deoxygenated blood collected from the body en route to the lungs via the right side of the heart. The superior vena cava (SVC), as its name implies, drains blood mostly from the superior aspects of the body including the head, upper limbs, and chest cavity, while the inferior vena cava (IVC) drains the abdominal cavity and lower limbs. The IVC is laden with the products of digestion, which have been processed and packaged for distribution by the liver. In this course, we will examine the anatomy of the venae cavae, and apply the anatomy to imaging these vessels in health and disease.
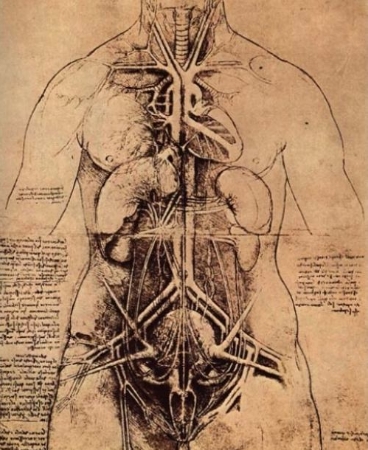
With limited knowledge of biology, da Vinci drew a fairly accurate representation of human anatomy in the late 1400’s. The depiction of the circulatory system reflects remarkable attention to detail and careful dissection of the human body. Dissection was considered taboo in the Dark ages until the spirit of inquiry awakened in the dawning of the Renaissance period. Courtesy of: Ashley Davidoff, M.D.
Historical Perspective
Hippocrates, the Father of Medicine, wrote, “The vessels which spread themselves over the whole body, filling it with spirit, juice, and motion,are all of them but branches of an original vessel. I protest, I do not know where it begins or where it ends, for in a circle there is neither a beginning nor an end.” Although Hippocrates did not have the opportunity to view the body with today’s imaging modalities, the assumptions that he made in 470 B.C. were fairly accurate. In the course, we analyze one portion of this mysterious circle – the vena cava.
It goes round and around, fetching and taking, in circles and cycles, always moving in pulsatile fashion, mostly forward, but sometimes a little backward. This is the circulation. Although Hippocrates had a hint of a continuum and a cycle, his perceptions were not fully realized until Harvey’s work in the early 1600’s. Image courtesy of Ashley Davidoff M.D
Tubes, Branches, Circles and Cycles
The body is made of a series of tubes and a series of organs. The way the body is structured is a microcosm of our cities towns and villages. The tubes that transport fluids, secretions, metabolic products and neuroelectrical impulses, are the roads, sewers, cables and wires of our environment that enable us to function. Tubes are also structurally and functionally essential in all biological systems, including plant and animal life. Tubes are designed to transport material effectively, and the venae cavae are designed to transport deoxygenated blood effectively. The venous system in general, is slow in flow, low in pressure, and adaptable to changing volume.
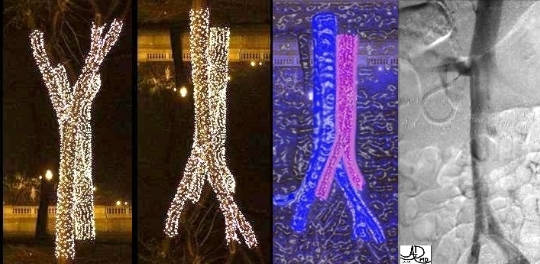
If you have studied the module on the aorta, this image from the RSNA will be familiar. The Christmas lights in the parks along Michigan Avenue in Chicago during the RSNA are not only beautiful to look at, but their branching pattern is reminiscent of all branching structures in biology. If you add a little color and a little artistry the trees can be very quickly transformed into jugulars and carotids. Turn them upside down, (which we will do for you later) and they will become the iliacs. Image courtesy of Ashley Davidoff M.D.Now imagine yourself as a red cell, deplete of oxygen, flowing down the middle of either caval system – each a major highway of the body. You can only travel at a slow speed, (30 mph – see sign) and at low pressure. As you course through the venae cavae you will see large trucks of molecules filled with all sorts of materials being transported from the food basins, factories, and even the brain of it all, to the supermarkets for delivery and dumpsters and recycling plants for offloading. Your first destination will be the heart, and the right atrium in particular (the yellow sign points the way). The lungs will exchange your carbon dioxide for some fresh air, and as you return to the heart, you should put on your seatbelt because it is going to be a high velocity, high pressure experience before you return back to the slow easy and adaptable pace of the venous system. Image courtesy of Ashley Davidoff M.D.
Veins: General Principles About Veins
The following facts should be kept in mind when learning the names and locations of veins:
Veins are the ultimate extensions of capillaries, just as capillaries are the eventual extensions of arteries. Whereas arteries branch into vessels of decreasing size to form arterioles and eventually capillaries, capillaries unite into vessels of increasing size to form venules and eventually, veins.
Although all vessels vary considerably in location and number of branches (and whether they are even present), the veins are especially variable. For example, the median cubital vein in the forearm is absent in many individuals.
Many of the main arteries have corresponding veins bearing the same name and are located alongside or near the arteries.
The large veins of the cranial cavity, formed by the dura mater, are not usually called veins but are instead called dural sinuses, or simply, sinuses. They should not be confused with the bony, air-filled sinuses of the skull.
Veins communicate (anastomose) with each other in the same way as arteries. Such venous anastomoses provide for the collateral return blood flow in cases of venous obstruction.
The arteries do not have valves except where they take their origin from the heart. Most veins have valves. The superior vena cava does not have any valves and the inferior vena cava has an ineffective valve positioned at its entrance into the heart.
The veins are slow in flow, low in pressure, with variable capacitance to accommodate to changing volume needs. They act as a “storage” house for volume, and can hold onto unneeded volume, or can increase delivery of volume when required.
Flow of venous blood is maintained by multiple mechanisms including the push and pull actions of the heart, the changing intrathoracic and intrabdominal pressures caused by breathing mechanisms, and by the effect of skeletal muscle contraction.
General Considerations About the Venae Cavae
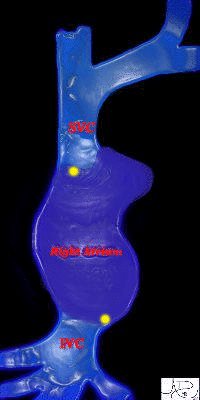
The venae cavae enter the right atrium at opposite poles of the chamber. At the entrance to the atrium, which is the entrance hall for the right ventricle, the electrical switches of the heart are positioned. The SVC is positioned near the Sino-Atrial node(S-A node) and the IVC is positioned near the Atrio-Ventricular(A-V node). (yellow inlays). Image courtesy of Ashley Davidoff M.D.
The venae cavae are the main receiving vessels for systemic blood returning to the heart from the various tissues and organs of the body. The superior vena cava (SVC) returns blood from the upper extremities and the brain, originating at the confluence of the left and right innominate veins (which are in turn formed by the internal jugular and subclavian veins). The SVC enters the upper back portion of the right atrium. The inferior vena cava (IVC) receives blood from the lower extremities and abdominal cavity. It is larger than the superior vena cava. The larger veins that enter the IVC include the iliacs, renals and hepatics, while the smaller veins include the lumbar, right gonadal, right adrenal, and inferior phrenic veins. The largest connecting vein that allows the two systems to communicate is the azygos vein.
This drawing of the venae cavae and their major tributaries reflects a rather asymmetric system of veins. The azygos vein is the main connector between the SVC and IVC and it acts as the most important collateral pathway when either of the great veins is occluded. The azygos sits rightward of the lymphatic duct (in yellow) which transports lymph from the the entire lymphatic system to the left subclavian vein. Image courtesy of LifeART Lippincott Williams & Wilkins All rights reserved
The Superior Vena Cava: The Superior Vena Cava (SVC) – Big Blue from Above
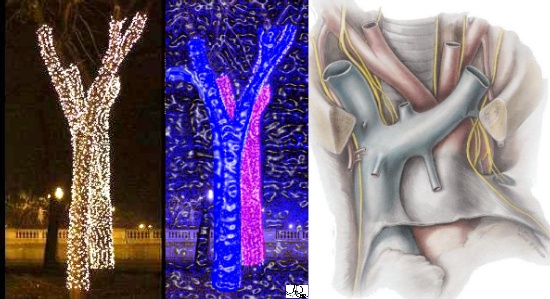
Right panel image courtesy of LIFEART Lippincott Williams & Wilkins All rights reserved. Before we embark on more detail, we want you to take another look at the Chicago Christmas tree line alongside a drawing of the SVC to conceptually understand the similarities – and now onward to the detail. Left and center Images courtesy of Ashley Davidoff M.D.
The SVC measures about 7 cm. in length and is formed by the junction of the two innominate (brachiocephalic) veins. The SVC begins immediately below the cartilage of the right first rib close to the sternum, and, descending vertically behind the first and second intercostal spaces, ends in the upper part of the right atrium opposite the upper border of the third right costal cartilage. Half of the vessel is within the pericardium and there is no valve at the entrance to the atrium.
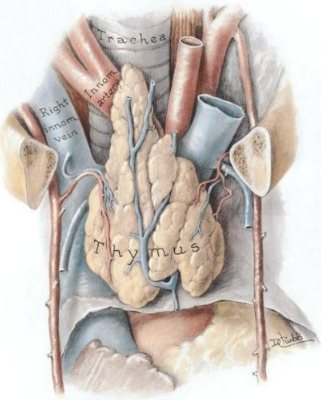
Image courtesy of LifeART Lippincott Williams & Wilkins. All rights reserved. The two innominate (brachiocephalic) veins, left and right, merge behind the thymus gland to form the SVC. The SVC travels a very short distance (~7 cm.) to the right atrium. The pericardium can be seen just below the thymus gland that appears to be comfortably resting on the heart’s covering. Note how part of the SVC lies within the pericardium, while the more superior aspect is free of pericardial covering.
Normal Transverse View
Image courtesy of LifeART Lippincott Williams & Wilkins. All rights reserved. The two innominate (brachiocephalic) veins, left and right, merge behind the thymus gland to form the SVC. The SVC travels a very short distance (~7 cm.) to the right atrium. The pericardium can be seen just below the thymus gland that appears to be comfortably resting on the heart’s covering. Note how part of the SVC lies within the pericardium, while the more superior aspect is free of pericardial covering.The great vessels of the mediastinum are positioned in an oblique line from left and anterior to right and posterior as the right ventricular outflow tract, the ascending aorta, and the SVC. Additionally the right atrial appendage and descending thoracic aorta are noted. Image courtesy of Ashley Davidoff M.D. and John Cooke PhD.
These are the great vessels of the superior aspect of the mediastinum. They remind me of a story – “Once upon a time there were three bears -a big papa bear, a mama bear and a little baby bear. Papa was usually the largest – but only by a bit – and walked on the left and always in front. Mama was always by his side but just behind and to the right, while baby was always behind and to the right. They went for a walk starting out from the quiet neck (of the woods) making their way toward the heart of activity…”
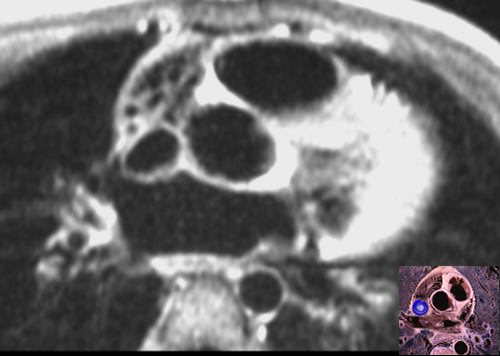
This axial MRI T1 weighted image is taken at about the same level as the previous anatomic image. The vessels are not exactly aligned – but that is biology – it is not always by the book. However from left to right and from anterior to posterior we see the right ventricular outflow tract, the aorta and the SVC. The anatomic specimen is inserted to help you identify the vessels and in particular the SVC. (blue overlay) Image courtesy of Ashley Davidoff M.D.
Nature of the Vessel
The SVC is part of a low-pressure system and its walls are thin. It is tubular but pliable, enabling it to accommodate changes in intravascular volume and pressure. With this ability, its shape varies depending on how “full” the system is, and hence its shape in cross section varies between round, oval, lenticular to slit-like. It is sometimes pushed around by the more powerful and high pressured aorta which sits leftward of it.
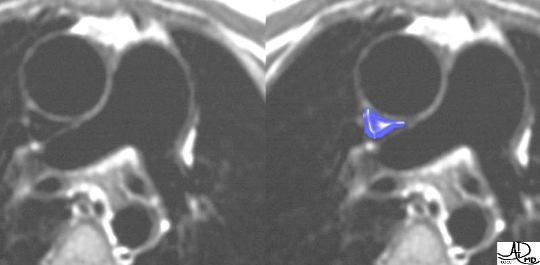
The SVC in this image is very densely enhanced and it reveals a normal rounded appearance. Image courtesy of Ashley Davidoff M.D.This T1 weighted gated MRI, shows the larger, high-pressured aorta deforming the low pressured, more pliable SVC. (blue overlay) Image courtesy of Ashley Davidoff M.D.
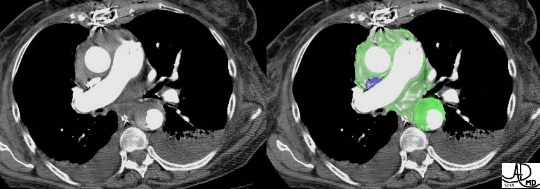
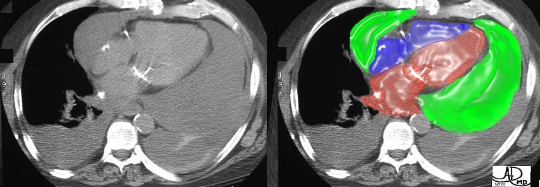
This patient has a ruptured dissecting aorta and is in a hypovolemic state. The SVC (blue overlay) is narrow and slit-like, reflecting a combination of hypovolemia and compression by the surrounding mediastinal hematoma. The dissection is well seen in the descending aorta (bright green), and the mediastinal hematoma (other green) can be seen surrounding the mediastinal structures. Image courtesy of Ashley Davidoff M.D.
Landmarks – Branch Points
A good method of observing, remembering, and evaluating a structure is to identify and recognize certain landmarks. In the case of the SVC, there are four important landmarks, three of which are recognized by a “head and tail” configuration. These landmarks imaging from cranial to caudal include:
SVC origin
Azygos vein entry into the SVC
SVC positioning when the arm of the right pulmonary artery gives it a hug
SVC entrance into the right atrium
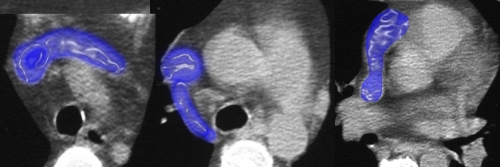
The following images detail the three “head and tail” landmarks (1, 2, & 4)and focus on the specific branch points. The “pulmonary artery hug,” (3) follows on the next page.
This patient has a ruptured dissecting aorta and is in a hypovolemic state. The SVC (blue overlay) is narrow and slit-like, reflecting a combination of hypovolemia and compression by the surrounding mediastinal hematoma. The dissection is well seen in the descending aorta (bright green), and the mediastinal hematoma (other green) can be seen surrounding the mediastinal structures. Image courtesy of Ashley Davidoff M.D.The landmarks have been overlaid in blue. Note how in each case there is a consistency of shape – an elongated tail and a rounded head – almost like a tadpole or a strange shaped fish. Keep on the lookout for these three strange-headed structures as you review axial images – they can almost always be observed. Image courtesy of Ashley Davidoff M.D.
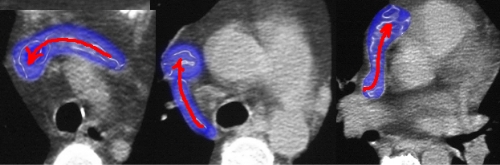
The landmarks have been overlaid in blue. Note how in each case there is a consistency of shape – an elongated tail and a rounded head – almost like a tadpole or a strange shaped fish. Keep on the lookout for these three strange-headed structures as you review axial images – they can almost always be observed. Image courtesy of Ashley Davidoff M.D.
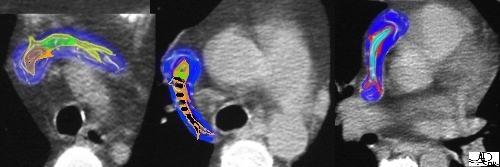
It is far more appealing to think of the colorful fish swimming in the direction of the blood flow. Image courtesy of Ashley Davidoff M.D.
Landmarks – The Pulmonary Artery Hug
This is a view of the “pulmonary artery hug”, the fourth landmark. Test yourself on the first image and see if you can recognize the three big vessels – does “papa bear” remind you of a previous lesson? The SVC is colored in blue overlay in the second image while the aorta (red) and the main right branch of the pulmonary artery (blue) are added in the third image. Note how the right arm of the pulmonary artery (“papa”)- embraces the aorta and SVC (“mama and baby”). Only the right pulmonary artery shows this affection for the SVC since they are both on the right side of the mediastinum. What do you think would happen if there was a left sided SVC? Image courtesy of Ashley Davidoff M.D.
SVC – Origin
As previously detailed, the SVC extends caudally for 6-8 centimeters, terminating in the superior and posterior aspect of the right atrium, anterior to the right main stem bronchus. The SVC is joined posteriorly by the azygos vein as it loops over the right main stem bronchus and lies posterior to and to the right of the ascending aorta.
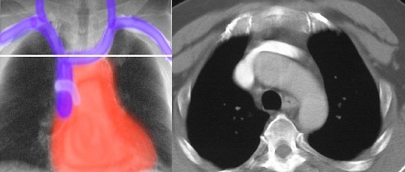
This is a view of the “pulmonary artery hug”, the fourth landmark. Test yourself on the first image and see if you can recognize the three big vessels – does “papa bear” remind you of a previous lesson? The SVC is colored in blue overlay in the second image while the aorta (red) and the main right branch of the pulmonary artery (blue) are added in the third image. Note how the right arm of the pulmonary artery (“papa”)- embraces the aorta and SVC (“mama and baby”). Only the right pulmonary artery shows this affection for the SVC since they are both on the right side of the mediastinum. What do you think would happen if there was a left sided SVC? Image courtesy of Ashley Davidoff M.D.This contrast enhanced CT of the upper chest reveals the “head and tail” view of the origin of the SVC. Image courtesy of Ashley Davidoff M.D.
The images are placed side by side to enable you to correlate the two views – frontal and axial. Image courtesy of Ashley Davidoff M.D.
Azygos Position
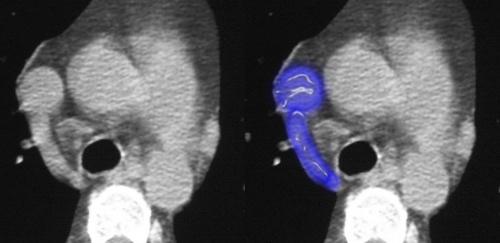
The next landmark is the “head and tail” view of the azygos vein’s entry into the SVC. The azygos vein takes its origin opposite the first or second lumbar vertebra and enters the thorax through the aortic hiatus in the diaphragm, passes along the right side of the vertebral column to the fourth thoracic vertebra, arches forward over the root of the right lung, and finally ends in the SVC superior to the pericardial attachment.
Before reaching the SVC, the azygos vein has collected blood from the right intercostal and subcostal veins, the hemiazygos vein, the right bronchial vein and several mediastinal, esophageal, and pericardial veins. This image is a frontal view showing the position of azygos entry into the SVC. Image courtesy of Ashley Davidoff M.D.This contrast enhanced CT of the upper chest reveals the “head and tail” view of the entry of the azygos vein into the SVC. This occurs just inferior to the aortic arch and above the carina. Image courtesy of Ashley Davidoff M.D.
The images are placed side by side to enable you to correlate the two views – frontal and axial. Image courtesy of Ashley Davidoff M.D.
Right Pulmonary Artery Position
The third most superior landmark is the “pulmonary artery hug”. The pulmonary artery originates from the right ventricle of the heart and conveys venous blood to the lungs. The main pulmonary artery is short and relatively wide (about 5 cm. in length and 3 cm. in diameter). The pulmonary artery extends obliquely upward and backward, passing at first in front and then to the left of the ascending aorta, as far as the under surface of the aortic arch, and then divides into right and left branches of nearly equal size.
This frontal view shows the relatively inferior position of the right pulmonary artery relative to the azygos vein. This occurs just below the carina. Image courtesy of Ashley Davidoff M.D.The axial view shows the oblique lineup of the pulmonary artery hug. As previously described, the “papa bear, mama bear and baby bear” line up, reflecting the relative sizes of the three vessels, with papa bear placing his arm around the family. Also note that the trachea has split at the level of the carina into the main left and right bronchi. (black tubes behind the vessels). Image courtesy of Ashley Davidoff M.D.
The images are placed side by side to enable you to correlate the two views – frontal and axial. Image courtesy of Ashley Davidoff M.D.
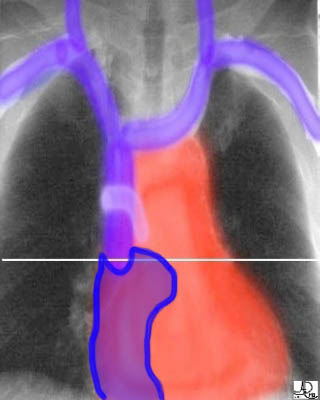
Junction With The Right Atrium
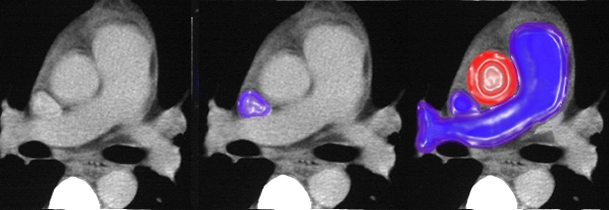
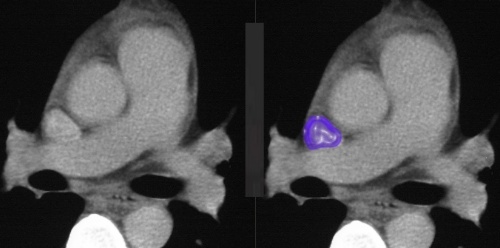
The last and most inferior landmark is the “head and tail” image of the SVC as it enters the right atrium from a posterior position. In this frontal image, the right atrium is outlined in blue. The right atrial appendage (“tail”) is the most superior and most medial component of the right atrium, and hence, is first into view as we scan from superior to inferior. Image courtesy of Ashley Davidoff M.D.This contrast enhanced CT of the mid chest reveals the “head and tail” view of the entry of the SVC into the right atrium. In the second image, the SVC is noted in blue overlay (“head”), and the right atrial appendage (“tail”) is added in the third image. Image courtesy of Ashley Davidoff M.D.
This correlative anatomic specimen is taken at about the same position as the axial CT image revealing the posterior entry of the SVC into the right atrium via the right atrial appendage. Image courtesy of Ashley Davidoff M.D.
The images are placed side by side to enable you to correlate the two views – frontal and axial. Image courtesy of Ashley Davidoff M.D.
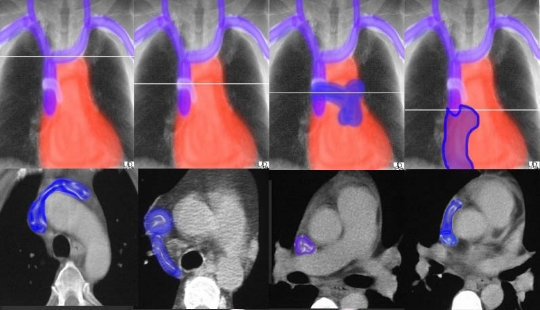
SVC – Review of the Four Landmarks
The first series of images reveal the four landmarks as they are taken from the frontal view. The bottom series details the landmarks as they are seen in the axial view. Viewing and remembering the landmarks in both the frontal and axial views is a helpful exercise. Image courtesy of Ashley Davidoff M.D.
Abnormal SVC – Trouble at the Origin
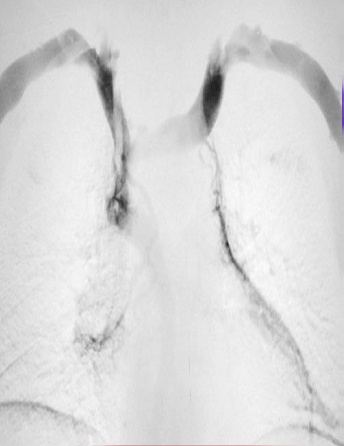
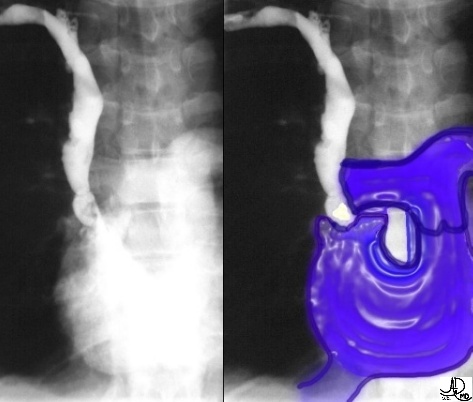
This venogram reveals total occlusion of the SVC at its origin. The occlusion was caused by a tumor encasing the SVC at its origin. Note all the small collateral vessels at the site of the obstruction. The image inset reflects what the normal SVC should look like. Image courtesy of Ashley Davidoff M.D.
Trouble at the Azygos
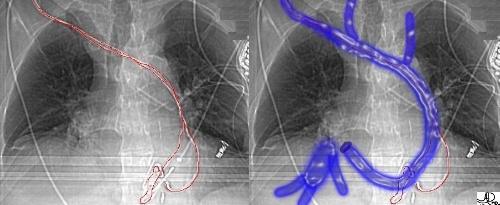
This venogram shows occlusion of the SVC caused by a thrombus at the level of the entry of the azygos vein into the SVC. Since flow could not proceed down toward the heart, it took the line of least resistance down the azygos vein itself. Hence the flow in the azygos was reversed. Can you see the faint opacification of the azygos vein? Image courtesy of Ashley Davidoff M.D.This venogram shows occlusion of the SVC caused by a thrombus at the level of the entry of the azygos vein into the SVC. Since flow could not proceed down toward the heart, it took the line of least resistance down the azygos vein itself. Hence the flow in the azygos was reversed. Can you see the faint opacification of the azygos vein? Image courtesy of Ashley Davidoff M.D.
How does the blood get back to the heart? The azygos vein is the bridge between the SVC and IVC – and blood will find its way to the IVC via this collateral pathway and back to the right atrium
Trouble at the Right Pulmonary Artery
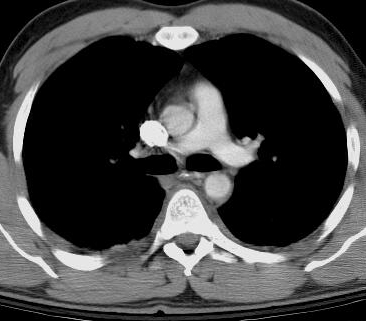
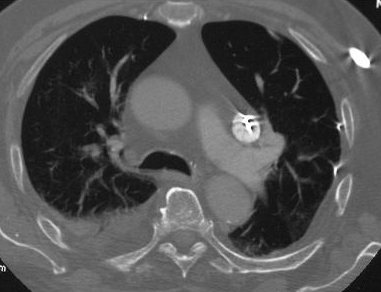
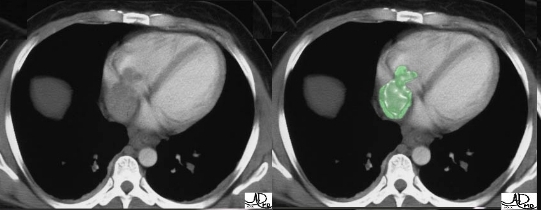
In this case, the trouble is not in the SVC itself but within the pulmonary artery. Do you know what the filling defect represents? This is a “saddle” pulmonary embolus, characterized by a large clot straddling the pulmonary bifurcation. The clot usually arises from a vein in the legs, and travels or embolizes to the pulmonary artery – a life-threatening situation. Image courtesy of Ashley Davidoff M.D.
Trouble at the Right Atrium
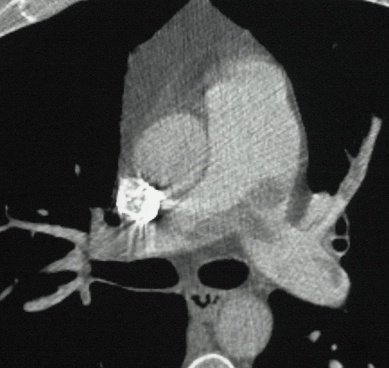
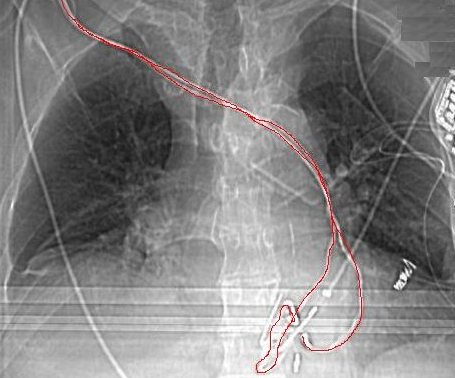
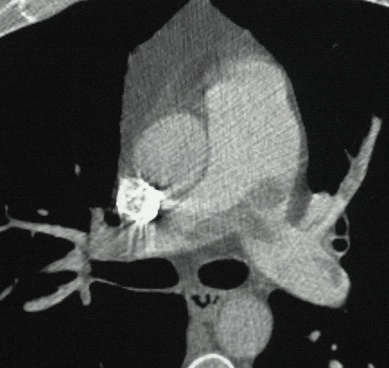
This venogram shows irregularity and narrowing of the SVC at its entrance into the right atrium caused by a long-term ventriculo-atrial shunt placed at birth for hydrocephalus. A thrombus developed at the tip of the catheter and eventually calcified, resulting in an obstruction and the development of SVC syndrome. This condition was treated with thrombolytics. Image courtesy of Ashley Davidoff M.D.The calcification can be seen as a filling defect at the most distal tip of the SVC. The defect can be seen as a dark triangular structure in the first image, and a bright white defect in the second image. The right atrium, right ventricle and pulmonary artery have been overlaid in blue. Image courtesy of Ashley Davidoff M.D.
Position
In this axial CT image, we do not see the normal right sided SVC behind the aorta. Instead we see a left sided SVC filled with contrast and a bright artifact of a pacemaker wire. In this case the SVC gets a hug from the left pulmonary artery. Image courtesy of Ashley Davidoff M.D.
The SVC is sometimes placed on the left side of the mediastinum, and as such is called a “left sided SVC” or “LSVC”. In the early stages of embryonic development, the great veins tend to be symmetrical structures, and with time, the right grows and the left side regresses. Occasionally bilaterality persists, or the left sided component grows while the right side regresses. When this occurs in the SVC, it is called an “LSVC”. The LSVC does not enter directly into the right atrium but rather via the coronary sinus.
In this frontal view of the chest we observe the pacemaker wires in red coursing along the left side in a patient with an LSVC. Image courtesy of Ashley Davidoff M.D.The LSVC course has been overlaid in blue, showing its distribution and entry into the horizontally positioned coronary sinus. Note also that the coronary sinus enters the right atrium close to the entry of the confluence of the hepatic veins and IVC. Image courtesy of Ashley Davidoff M.D.
Inferior Vena Cava (IVC) – Big Blue From Below
The inferior vena cava (IVC) returns blood to the heart from the tissues and organs below the diaphragm. The IVC is formed by the junction of the two common iliac veins, and ascends along the front of the vertebral column on the right side of the aorta.
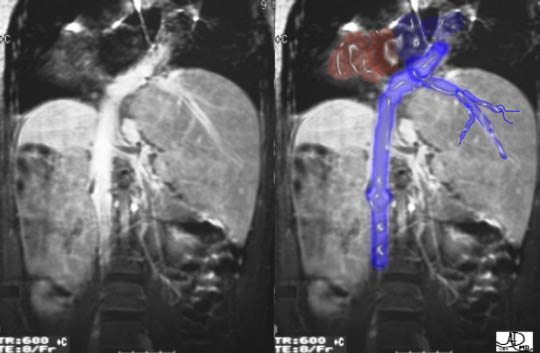
Our now infamous RSNA Christmas lights. By turning the trees upside down, we can visualize the junction of the iliacs and the genesis of the IVC. Image courtesy of Ashley Davidoff M.D.This coronal T2 weighted image of the inferior vena cava provides an overview of the IVC. The image depicts the relative rightward position of the IVC, the origin at the level of the junction of the iliacs, the renal veins near its center, its relation to the liver, the position of the hepatic veins just below the diaphragm, and its connection to the right atrium. The aorta (red) runs parallel and leftward of the IVC. Image courtesy of Ashley Davidoff M.D.
The IVC, as stated previously, is not isolated from the SVC. The azygos and hemiazygos veins are important connecting veins that run between the two great veins. These are particularly important as collateral pathways when either one is blocked. Image courtesy of LifeART Lippincott Williams & Wilkins. All rights reserved.
Overview
The inferior vena cava (IVC) returns blood to the heart from the tissues and organs below the diaphragm. Below the diaphragm, the abdominal portion of the IVC receives blood from the common iliacs, lumbar, right gonadal, renal, suprarenal, inferior phrenic, and hepatic veins. The thoracic portion of the IVC is very short (about 2.5 cm.), and does not receive any additional veins prior to entering the right atrium.
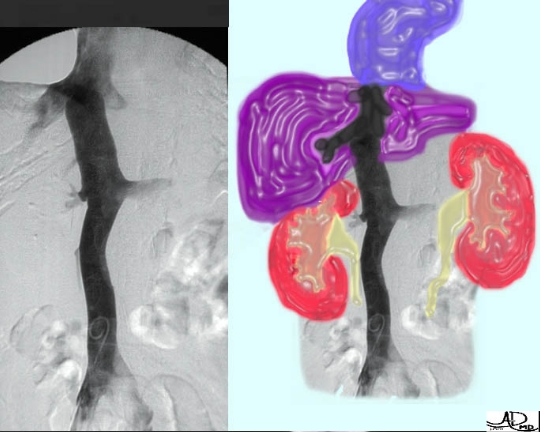
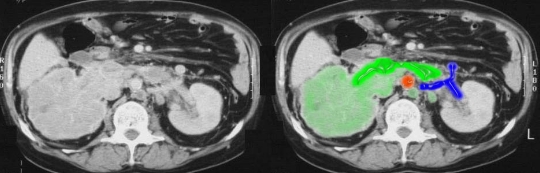
The IVC runs just rightward of center and has three major organs that it drains – the lower limbs, kidneys, and liver. The venous blood from the intestinal tract returns via the portal system to the liver. Image courtesy of Ashley Davidoff M.D.The image on the left is a rather confusing diagram revealing a number of small and large tributaries of the inferior vena cava. The major veins shown in the second image are clearer and include the iliacs from the legs, the renals and the hepatic veins. Left panel image courtesy of LifeART Lippincott Williams & Wilkins. All rights reserved. Right panel image courtesy of Ashley Davidoff M.D.
The major veins are again shown in the first image and include the iliacs from the legs, the renals and the hepatic veins. The image on the right details the more important small veins and includes the venous drainage from the adrenals and the gonads. Although the gonads and adrenals are symmetric structures, and have symmetric arterial supply, their venous drainage is quite asymmetric. The right ovary or testis and right adrenal drain directly into the IVC, while the left equivalents drain into the left renal vein. Image courtesy of Ashley Davidoff M.D.
This sagittal view of the intra and retrohepatic portion of the inferior vena cava reveals its pliability. Note the variability in shape of the low pressure IVC. The size and shape of the IVC will depend on the phase of respiration, the intravascular volume, and the effect of pressure from surrounding structures. The pliable characteristics of the great veins are in sharp contrast to the high pressure and rigid but elastic aorta that only significantly changes its size and shape in disease. Image courtesy of Philips Medical Systems
Normal Frontal View
The coronal T2-weighted image of the inferior vena cava shows the relative rightward position of the IVC, its relation to the liver, its position of origin in relation to the right iliac vein, and the position of the hepatic veins high in the liver, and its connection to the right atrium. Image courtesy of Ashley Davidoff M.D.
This image represents the venographic representation of the IVC, its three major sets of veins, and where the IVC drains into the right atrium. Image courtesy of Ashley Davidoff M.D.
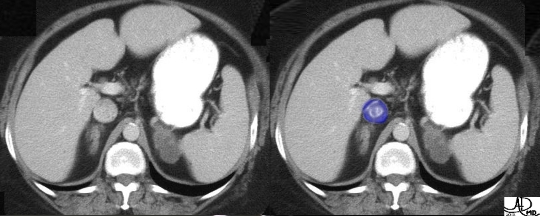
This T1-weighted “out-of-phase” image through the abdomen reveals the normal lenticular shaped IVC in blue overlay. The IVC will normally change in shape depending on the phase of respiration and the intra-vascular volume. Image courtesy of Ashley Davidoff M.D.
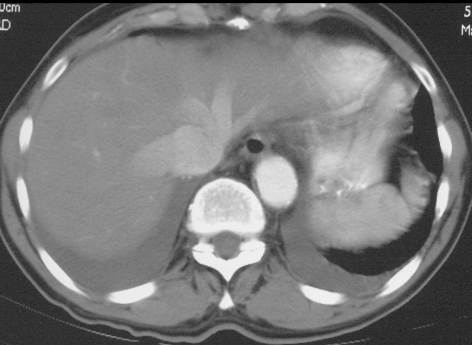
In this case the IVC is more rounded, also a normal finding. This patient is probably breath holding which causes an increase in the thoracic pressure as well as an increase in intravenous pressure. Did you notice the abnormal masses in the adrenals? See the adrenal module to learn all about it. Image courtesy of Ashley Davidoff M.D.
Size
The IVC perforates the diaphragm at T8 and eventually runs into the lower and back part of the right atrium. The thoracic portion of the IVC measures only 2.5 cm. in length, half of which is enveloped by the pericardium. The abdominal portion of the IVC begins at L5 and measures between 24 and 28 cm. The transverse diameter of the IVC is similar to that of the aorta measuring on average about 2.5cm.
These two images of the IVC are both normal but look quite different. On the left, the image is taken with a shallow breath hold, showing the IVC to be less distended with a lack of filling of the renals and hepatics. The second image is taken with a Valsalva maneuver, which causes a significant rise in the thoracic pressure and hence a rise in the IVC pressure. This rise in pressure results in contrast “backup” into the major branches. Note how much more plump the IVC appears in the second image. Image courtesy of Ashley Davidoff M.D.This longitudinal color flow Doppler study of the IVC in beautiful green shows a distended vessel of approximately 2.5 cm. Image courtesy of Philips Medical Systems
The conventional gray scale image of the IVC shows the variable size of the low pressure IVC, deformed by surrounding structures, which include the liver anteriorly and the right renal artery posteriorly. Image courtesy of Philips Medical Systems
Shape
The inferior vena cava is a large, valveless, venous trunk. The IVC is a deep vein that accompanies the aorta through the abdomen, wrapped in the same outer sheath. As we have so often stated, the physiology of the IVC demands that it is pliable to accommodate breath-to-breath and beat-to-beat changes in volume and pressure. The IVC therefore does not have a single shape but is characterized by the low pressure, low volume lenticular or oval shape on the one hand, and the more rounded higher volume higher pressure shape on the other. The esophagus and vagina share this cross-sectional shape when in the “relaxed” or non-distended state, and will become rounded in the distended state.
These two images of “big blue” are both normal. The variability of size and shape are dependant on the phases of respiration. The first image shows the rounded high volume IVC, and the second the low volume lenticular shape. A lack of change in the shape and size of the IVC during inspiration and expiration is abnormal. Image courtesy of Ashley Davidoff M.D.This transverse projection of a Doppler ultrasound shows the IVC in a “relaxed” position, with characteristic lenticular shape, placed just anterior to the right renal artery. This is the classical shape of the IVC, with a transverse measurement just slightly larger than the A-P measurement. Image courtesy of Philips Medical Systems
Which is normal? The first image is of course. The corkscrew appearance of the IVC in the second venogram is caused by multiple surrounding masses pushing on soft “big blue”. Image courtesy of Ashley Davidoff M.D.
Position
The legs and most of the pelvis are drained through the paired common iliac veins, which merge to form the origin of the IVC to the right of the fifth, or last lumbar vertebra. The IVC will span the entire, more cranial, portion of the abdominal cavity and will end its abdominal portion at the diaphragm as it enters the thoracic cavity for its short, 2.5cm. course. The IVC is a retroperitoneal structure, and more specifically, lies in a special ensheathed portion of the anterior pararenal space referred to by some as the central retroperitoneum. “Big blue” and “big red” are vital transport systems and have to be protected. The adventitial layers and retroperitoneal fibrous sheath are fine but strong, intimate protective layers. More global protection is provided as a consequence of its position in front of the bony spine and behind all the organs of the abdominal cavity.
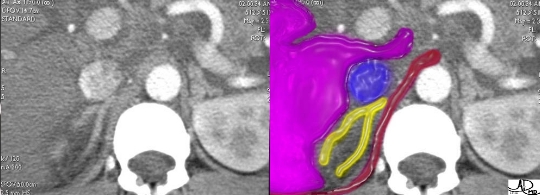
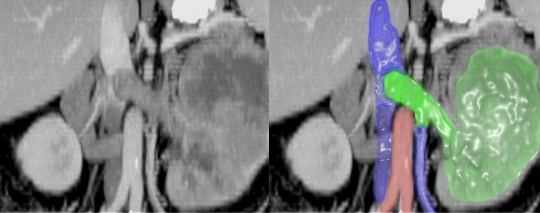
The central highway of the body is located in the posterior aspect where all the major transport systems run, including the great veins, aorta, spinal cord, lymphatic duct, and autonomic ganglia. It is no wonder that the vertebral column, the body’s backbone, runs in support and protection of these precious and vital transport systems. This coronal view of the IVC shows its position in relation to the vertebral column. Image courtesy of Ashley Davidoff M.D.The IVC is a retroperitoneal structure, and together with the aorta, is isolated and protected from the other structures of the anterior pararenal space. This image shows the position of the IVC just before it dives intrahepatically. From anterior to posterior we have portal vein (gray in front of the slither of purple liver), the liver (purple), IVC (blue), adrenal (yellow), and crus (maroon). The aorta and spine are medial and posteromedial respectively. Image courtesy of Ashley Davidoff M.D.
As previously mentioned, the IVC is sometimes placed on the left side of the aorta, as high as the left renal vein, and, after receiving the renal vein, crosses over to its usual position on the right side. Sometimes the IVC may be placed altogether on the left side of the aorta, and in such a case, the abdominal and thoracic viscera, together with the great vessels, are all transposed.
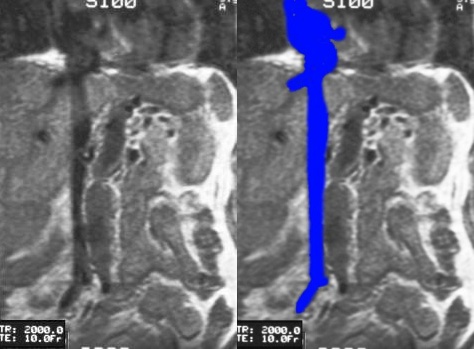
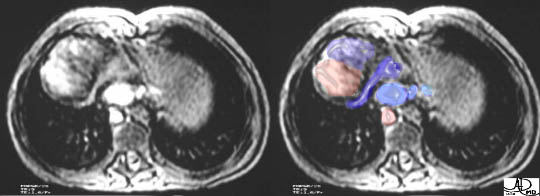
This is a case of “double IVC” with both a left and right sided IVC. In this case, the left sided IVC enters the left renal vein more cranially, which in turn crosses the midline as is usual, to join the right IVC. Thus there are two IVCs in the lower abdomen with one IVC above the renal veins. Image courtesy of Ashley Davidoff M.D.This axial MRI using a SPoiled GRadient (SPGR) echo sequence shows two great vessels in the retroperitoneum. Can you guess why the left sided structure is the venous structure? Look at the shape of the two vessels. The left sided structure is not completely round and its shape is deformed by the hard vertebral body suggesting that it is a low pressure, venous structure. The diagnosis in this case is polysplenia syndrome, with absence of the intrahepatic portion of the IVC with azygos extension. In essence “big blue” in this case is a large azygos vein. There is no IVC at this level, and the azygos vein is assigned the function of returning systemic venous blood from the legs, and kidneys to the heart via the SVC. Image courtesy of Ashley Davidoff M.D.
Character
The pliable nature of the low-pressure great veins (-1 to +5mmHg range) is in sharp contrast to the rigid yet elastic nature of the aorta, which has to deal with the higher systemic pressures (120 mm Hg.). The last image revealed the importance of applying this fact to enable the distinction between artery and vein.
You have seen this set of images before in the “size” section, but they are relevant here as well to reveal the pliability and capacitance of the venous system. These two images of the IVC are both normal but look quite different. In the first instance, the image is taken in a suspended shallow respiration, showing the IVC to be relatively less distended with a lack of filling of the renals and hepatics. The second image is taken with Valsalva maneuver, which causes a significant rise in the thoracic pressure, a rise in the pressure of the IVC, and an increase in venous volume. The rise in pressure and volume results in contrast “backup” into the major branches and distension of the system. Note how much plumper the IVC appears in the second image. Image courtesy of Ashley Davidoff M.D.This sagittal view of the intra and retrohepatic portion of the inferior vena cava reveals its pliability. Note the variability in shape of the low pressure IVC as it is put upon by the posteriorly positioned right renal artery, and the anteriorly positioned liver. Image courtesy of Philips Medical Systems
5 Landmarks
As with the SVC, a good method of observing, remembering, and evaluating a structure is to identify and recognize certain landmarks. In the case of the IVC, there are 5 important landmarks. These landmarks include: 1.) IVC origin: Confluence of the common iliacs 2.) Left renal vein entry into the IVC 3.) Right renal vein entry into the IVC 4.) Confluence of the hepatic veins 5.) Junction of the IVC and the right atrium The following pages will define these landmarks.
In the above image, we can clearly see the 5 key landmarks for the IVC: starting with the distal formation of the IVC where the iliacs merge, the left and right entry points of the renal veins, the confluence of the hepatic veins, and finally the terminal point at the entry into the inferior aspect of the right atrium. Image courtesy of Ashley Davidoff M.D. 24149
Origin
At the level of the inguinal ligament (which is at the anterior, diagonal border between the trunk and the thigh), the femoral vein becomes known as the external iliac vein. The external iliac unites with the internal iliac vein to form the common iliac vein. The internal iliac vein drains the pelvic walls, viscera, external genitalia, buttocks, and a portion of the thigh. The legs and most of the pelvis are drained through the paired common iliac veins, which merge to form the origin of the IVC to the right of the fifth (and last) lumbar vertebra.
The vessels outlined in blue are the two common iliac veins as they move toward the junction that will form the IVC. Image courtesy of Ashley Davidoff M.D. 27516cW540The junction is sometimes reminiscent of the “head and tail” images we have seen at other junction points. The appearance in this instance is caused by the slight horizontal orientation of the left common iliac vein, combined with the compression of the vein by the anteriorly positioned and higher pressured distal aorta and iliac arteries. Image courtesy of Ashley Davidoff M.D.
Junction With The Left Renal Vein
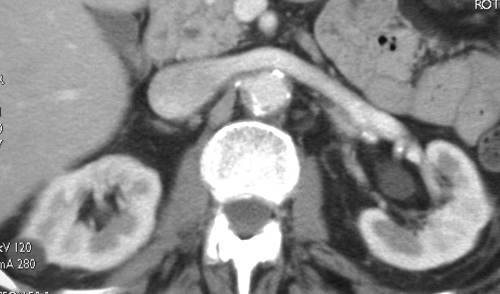
The renal veins are fairly large in size and are positioned in front of the renal arteries. The left renal vein, which is longer than the right, passes in front of the aorta just below the origin of the superior mesenteric artery. The left renal vein receives the left gonadal and left inferior phrenic veins, and, generally, the left adrenal vein (in some cases, the left adrenal may join the left inferior phrenic prior to joining the renal). The left renal vein usually opens into the inferior vena cava at a slightly higher level than the right. NB: The right adrenal vein usually drains directly into the IVC – take a glance at the sword fight at Bunker Hill in the adrenal section.
The junction of the left renal vein is a classical “head and tail” image. If you are lucky you will see this classical “head and tail” view with a similar appearance of the splenic vein – superior mesenteric vein confluence on the same axial cut. It is truly a beautiful sight to behold – like a pair of dolphins, or two fish romping in the ocean together – hold your breath – you may get lucky! Image courtesy of Ashley Davidoff M.D.If you replace the organs with a diffuse aquamarine blue, add a little seaweed (and imagination), you behold a mother and child pair of romping blue headed vein fish – a formerly unknown breed! Image courtesy of Ashley Davidoff M.D.
In the above case, the combination of an abnormally perfusing liver, a large IVC (that would not have changed significantly with respiration), and an appropriate clinical history leads to a diagnosis of right heart failure. Image courtesy of Ashley Davidoff M.D.
Junction With The Right Renal Vein
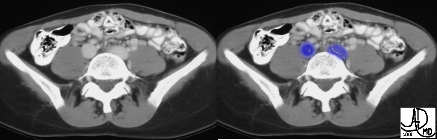
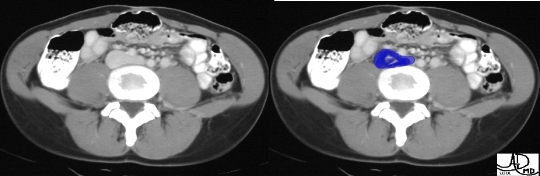
The right renal vein – IVC confluence either presents as a “head and tail” structure, or as a “two headed” structure – one small (right renal) and one large (IVC).
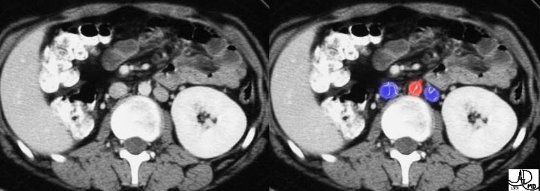
The right renal vein is short and variable in its position. In this instance it is horizontal and therefore presents as another example of the “head and tail” confluence on the axial section. Image courtesy of Ashley Davidoff M.D.In the left-hand image, the right renal vein is almost vertical. When we look at this same situation in cross section (image on the right), the appearance is of two heads – one small, the right renal vein and one big, the IVC. Can you identify the right renal vein? It contains contrast and is bright white. Image courtesy of Ashley Davidoff M.D.
Confluence Of The Hepatic Veins
The hepatic veins are formed in the liver as the central vein of the liver lobule where the sinusoids become confluent. The main branches of the hepatic veins are the right, middle, and left. The middle and left hepatic veins often join together to form a common trunk before entering the IVC. In addition, there are several short venous segments that drain the posterior surface of the liver directly into the IVC. We have mentioned that most veins run in conjunction with their counterpart, the artery. In the liver, the hepatic veins run without a neighboring artery. The hepatic artery runs with the portal vein and bile duct in the portal triad of the liver.
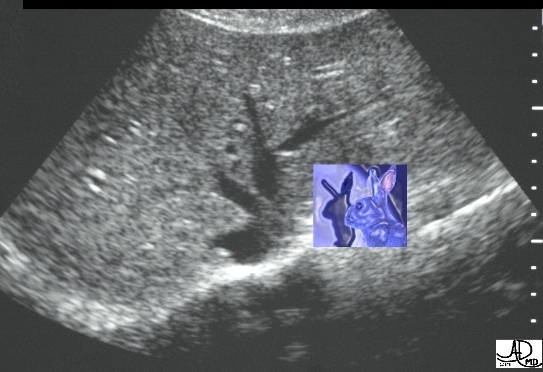
For those of you that have completed the Liver Anatomy Course, this image of the rabbit should be familiar. It represents the confluence of the right, middle, and left hepatic veins and has the shape of a rabbit’s head. The reason for this shape is because the left and middle vein (rabbit’s ears) usually join before they enter the IVC, while the right hepatic vein (rabbit’s nose) enters the IVC (head) separately. Image courtesy of Ashley Davidoff M.D.This color flow Doppler shows the confluence of the right and middle hepatic veins with the IVC. This is our rabbit, peeking his head out to take a look. Image courtesy of Ashley Davidoff M.D.
Junction With The Right Atrium
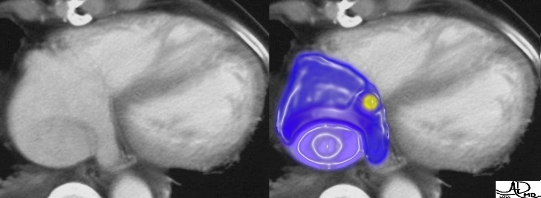
The vena cava enter the right atrium at opposite poles of the chamber. The electrical switches of the heart are also similarly positioned. The SVC is positioned near the SA node and the IVC is positioned near the A-V node. (yellow inlays) Image courtesy of Ashley Davidoff M.D.The junction with the IVC (light blue) with the right atrium (dark blue) is characterized by the presence of the tail-like coronary sinus, which is also entering the right atrium. Invisible but invariably present is the sino-atrial node (yellow). The trio (IVC, RA, and coronary sinus) presents a rather odd shape, but with a little imagination you can see Napoleon Bonaparte donning his characteristic headgear. Image courtesy of Ashley Davidoff M.D
.
Let us present the famous Napoleon to you – right in the heart of action. The three structures are not consistently shaped as seen in this image, (and hence Napoleon is not always seen) but the relationship of the three structures is constant. If you first look for the tubular or tail-like coronary sinus, you will then be able to identify the posteriorly positioned IVC and rightward and anteriorly positioned right atrium. The dashes and dots that represent the eyes, nose and mouth have no anatomical equivalent and are purely an artistic facelift. Image courtesy of Ashley Davidoff M.D.
The sagittal gray scale image of the IVC- RA junction is noted just above the highly echogenic diaphragm. Note the entry of a hepatic vein just below the diaphragm and the separate entry of the caudate lobe vein more inferiorly. Image courtesy of Ashley Davidoff M.D.
Abnormal IVC – Trouble at the Origins
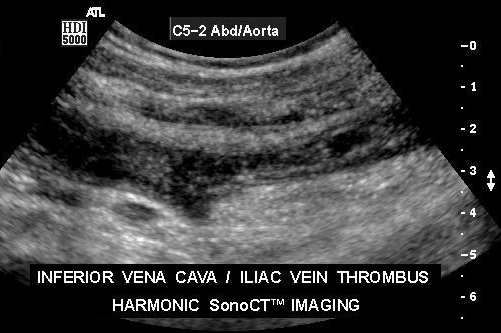
The femoral veins, noted in blue overlay, are asymmetric in size, which is abnormal. The femoral veins are normally only slightly larger than the femoral arteries and thus the problem is a left femoral vein aneurysm. Image courtesy of Ashley Davidoff M.D.The above image is a longitudinal harmonic gray scale image of the iliac vein. This image reveals abnormal echoes within the vessel, representing thrombus at the confluence of the iliac vein and IVC. Image courtesy of Philips Medical Systems
This venogram of the left common iliac shows a long segment of irregular filling and multiple collateral vessels. This represents a case of chronic thrombosis with attempted and partial recanalization. Image courtesy of Ashley Davidoff M.D.
Trouble at the Renals
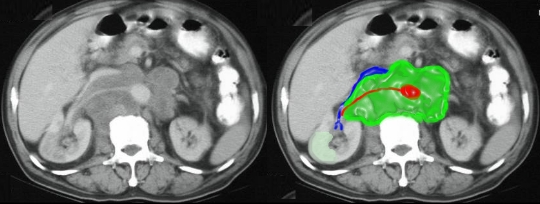
One of the unique features of the left renal vein is its relationship to the aorta (posterior) and the superior mesenteric artery (anterior), which on occasion can result in the renal vein being squeezed between the two. This is called the pinchcock effect, or nutcracker effect, and can result in a build up of pressure in the renal vein causing hematuria. This image shows the pinchcock effect resulting in an enlarged left renal vein. Image courtesy of Ashley Davidoff M.D.In this case the renal veins are too small, and the IVC is similarly flattened. This is a case of a patient with severely depleted intravascular volume, which can be caused by dehydration, severe hemorrhage or shock and vascular collapse. Image courtesy of Ashley Davidoff M.D.In this case the renal veins are too small, and the IVC is similarly flattened. This is a case of a patient with severely depleted intravascular volume, which can be caused by dehydration, severe hemorrhage or shock and vascular collapse. Image courtesy of Ashley Davidoff M.D.The CT coronal reconstruction shows a renal carcinoma (light green) that has infiltrated the right renal vein (darker green), the gonadal vein and the IVC. Image courtesy of Ashley Davidoff M.D.The tumor (green) in this case is a lymphoma that has a tendency to push structures around rather than to infiltrate. The right renal vein and IVC have been squeezed and pushed anteriorly. The pale green area in the kidney is a malperfused region of the kidney due to either arterial or venous compromise. Image courtesy of Ashley Davidoff M.D.
Trouble at the Hepatics
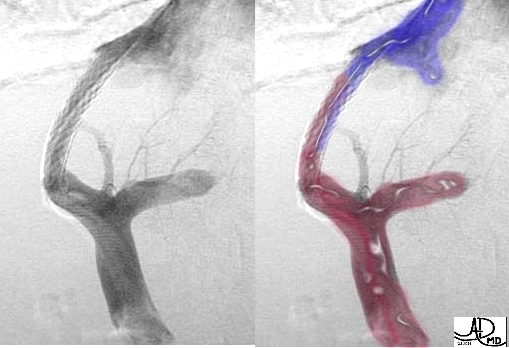
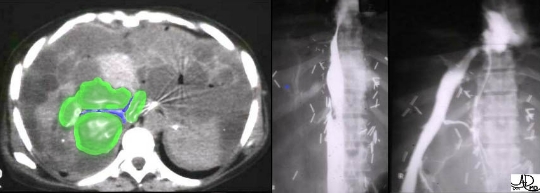
This case demonstrates a TIPS procedure, in which a metallic stent has been percutaneously positioned between the portal system (maroon), and the hepatic vein and IVC (blue). This shunt enables decompression of the portal system into the systemic venous system, preventing bleeding from the esophageal varices – a complication of liver cirrhosis. Image courtesy of Ducksoo Kim M.D. and Ashley Davidoff M.D.This is a case of invasion of the IVC by a hepatocellular carcinoma at the level of the hepatic venous confluence in a child. The rabbit’s face has been replaced by an ugly infiltrating tumor. The consequences of this situation are disastrous. Image courtesy of Ashley Davidoff M.D.Not only is the rabbit’s face too plump, but also his nose and ears are similarly voluminous. In tricuspid regurgitation, blood in the right ventricle that should be heading toward the lung, leaks back into the right atrium that is connected to the valveless IVC and hepatic veins. These structures therefore reflect the right ventricular pressure that is much higher than normal, forcing them to become congested and distended. Image courtesy of Ashley Davidoff M.D.
Trouble at the Right Atrium
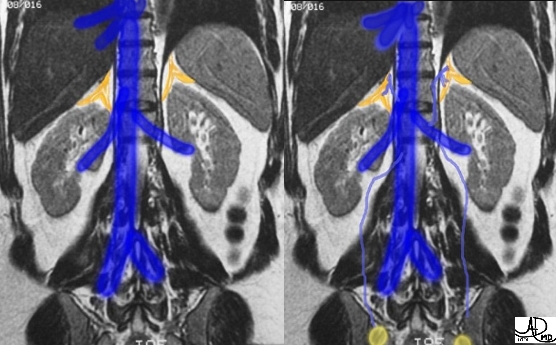
This patient has a diagnosis of hepatocellular carcinoma. The image shows non-filling of the IVC caused by extension of a tumor from the liver via the hepatic veins. The tumor extends into the right atrium and through the tricuspid valve. A small tumor embolus was also noted in a branch of the right pulmonary artery. Image courtesy of Ashley Davidoff M.D.This patient has a large pericardial effusion (green overlay) that has resulted in pericardial tamponade. The pressure of the pericardial effusion prevents the heart from distending, resulting in both an inability to receive blood as well as to pump it out. Image courtesy of Ashley Davidoff M.D.Asplenia is usually a fatal condition, typically associated with severe congenital cardiac disease and situs ambiguous – the organs sometimes appear to be “confused” as to exactly where they should be positioned. In this case of asplenia syndrome there is dextrocardia, with a left sided right atrium and a midline IVC that sits right in front of the aorta. Despite the presence of the coronary sinus-RA junction, (dark blue) the IVC has not yet gathered the hepatic veins (light blue) and it seems to want to continue northward in order to do so. Image courtesy of Ashley Davidoff M.D.This MRI is a flow sensitive coronal view of the patient with asplenia syndrome noted above. Note how the IVC seems indecisive about its position in life. It starts out on the right, becomes central, heads to the left where it collects a few hepatic veins from a left sided liver, (see correlative transverse section above), and then it continues on its way to enter the left sided right atrium more superiorly than expected. Image courtesy of Ashley Davidoff M.D.
Ultrasound of the Vena Cava: SVC – Ultrasound
The superior vena cava by itself is quite difficult to image with ultrasound, but its tributaries, such as the subclavian and jugular veins, are superficial and are well within the reach of probe. Evaluation for thrombosis and patency of stents is both easily accomplished technically and very helpful clinically.
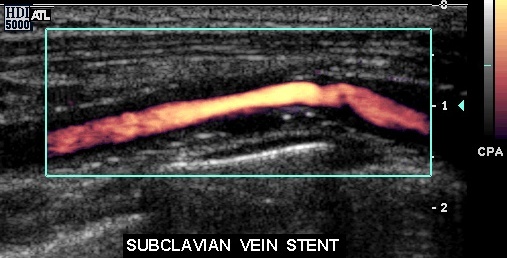
This transverse color flow Doppler of the internal jugular vein (blue) fails to fill the whole vein because the middle of the vein is blocked by a thrombus surrounding the highly echogenic catheter (seen in the posterior aspect of the thrombus). Image courtesy of Philips Medical SystemsIn this color flow Doppler of the subclavian vein a stent is shown within the confines of a vein that is about double the diameter of the stent. Can you identify the margins of the vein in which the stent lies? Presumably there has been endothelial proliferation within the stent that has reduced the effective size of the stent. Image courtesy of Philips Medical Systems
IVC – Ultrasound
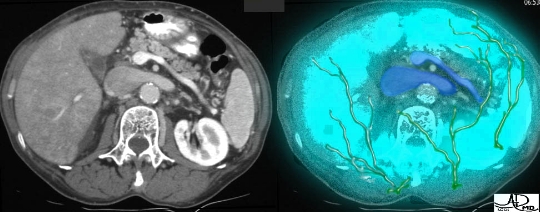
The ability to examine the IVC in its entirety is sometimes limited by the patients’ body habitus and by the presence of intervening bowel gas. The intrahepatic portions are almost always accessible, using the liver as a window, and the hepatic confluence is well seen. Color and spectral Doppler are very useful in evaluating the patency of the hepatic veins. In cirrhotic patients the hepatic veins become small and distorted and US is frequently the only study, short of venography, which can identify these diminutive hepatic veins.
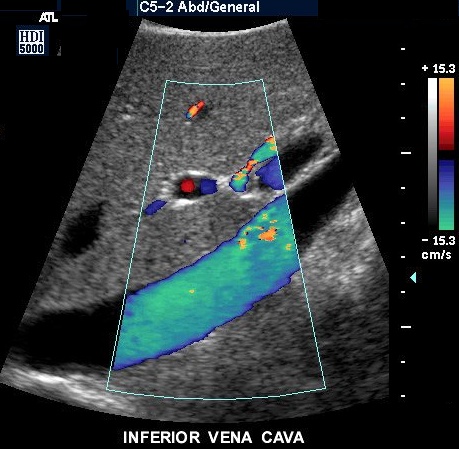
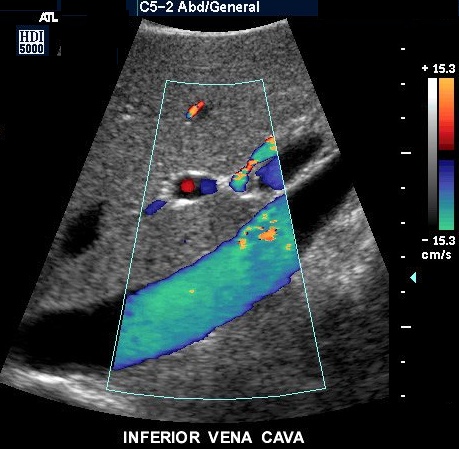
This clear image of the IVC and surrounding structures is unmatched by any other modality – a dream image for technologists and radiologists. Unfortunately, US is extremely patient dependent and not every study yields this result. Image courtesy of Philips Medical SystemsUltrasound also provides imaging specialists with the ability to add functional tools that enable the measurement of flow characteristics such as velocity, direction and the nature of the flow. (e.g., laminar, non-laminar, turbulent) This beautiful aquamarine sagittal image of the IVC looks so refreshing one almost wants to dive straight into it, though swimming in the IVC is not recommended since it contains byproducts of metabolism on their way to the dumpsters! Note the color code to the right of the image with orange above and green below. Since the color of the vessel in this case is green, it implies that the direction of flow is away from the transducer (labeled C5-2) and implies the flow is normal, from inferior of patient (by convention right of screen) to superior (left screen). Image courtesy of Philips Medical Systems
CT of the Vena Cava: SVC – CT
The SVC is easily identified and imaged by CT, but the presence of an artifact caused by the mixing of unopacified with opacified blood is a frequent occurrence. Imaging in the early phase (first pass) of vascular enhancement can also be limited by misregistration artifact. This occurs when contrast is densely concentrated and has not had time to diffuse and mix with the blood pool at large. If the study is dedicated to SVC evaluation, then a two-phase study will enable better mixing and better visualization of the vessel. In the setting of SVC obstruction in the oncologic patient, CT is very helpful in determining whether the obstruction is caused and/or originates from the lumen or from the extrinsic pressure of metastases.
The CT in the first pass phase shows dense contrast in the SVC with spray artifact, resulting in an uninterpretable image of the SVC. The “saddle” embolus however is clearly seen in the pulmonary artery. Image courtesy of Ashley Davidoff M.D.
IVC – CT
The IVC is also an easy target for CT, but is wrought with artifacts, particularly in the region of the renal vein confluence. The reason for these artifacts – the kidneys receive nearly 20% of the cardiac output and circulation from the renal arterial to the renal venous phase is very rapid. In contrast, the circulation from the lower limbs is comparatively slower. Hence in the first and sometimes even in the second pass, opacified blood from the kidneys mixes with the unopacified blood from the lower body, resulting in the artifactual appearance of a filling defect. However the IVC is consistently seen in CT, and multiphase imaging enables us to evaluate the IVC in its later and more homogeneous phases.
This arterial phase CT shows contrast in the renal cortex and renal vein with early spill into the IVC. The IVC contains mostly unopacified blood and hence there is a mixing artifact. Sometimes this artifact masquerades as a filling defect. Image courtesy of Ashley Davidoff M.D.This is a case of polycystic liver disease with cysts (green overlay) surrounding the IVC that have caused a compression of the hepatic veins and the IVC (slit-like blue overlay). The venogram on the right reveals the compression but is unable to “see” the surrounding cysts. Image courtesy of Ashley Davidoff M.D.
MRI of the Vena Cava: SVC and IVC – MRI
Imaging the great veins with MRI has the advantage of multiplane imaging. Primary imaging in the coronal, sagittal, oblique or axial planes is now routine. T1-weighted, or SPGR, imaging provides the ability to see the blood as black or white, each having their respective advantages and disadvantages. However, because of the slow flow of the venous system, MRI is wrought with flow artifacts that often limit its use.
This coronal T1-weighted image reveals the SVC and IVC on one image. Primary imaging in any plane gives MRI considerable advantage. Image courtesy of Ashley Davidoff M.D.
Venography of the Vena Cava: SVC and IVC – Venogram
Venography continues to remain the gold standard for great vein imaging, but it has lost its place as the primary imaging modality, which it held for so many years. In difficult cases where the lumen of the vessel needs to be imaged it still remains the final word, and in cases where intervention is required it is untouched by other modalities. The problem with venography is that it does not have the ability to “see” beyond the lumen. As a result, extrinsic masses can only be implied by the shape of the lumen but not primarily imaged. For adequate SVC imaging, both arms need to be injected or otherwise a mixing artifact precludes optimal enhancement. Adequate IVC imaging requires Valsalva maneuver to allow visualization of the iliac renal and hepatic branches.
The execution of a TIPS shunt can only be done at this time using fluoroscopic technique. Although venography has lost its throne as the modality of choice for first line diagnosis, it still remains a final arbitrator and is unequalled in therapeutic procedures. Image courtesy of Ducksoo Kim M.D. and Ashley Davidoff M.D.
Conclusion: Final Thoughts
by Dr. Ashley Davidoff
The great veins are slow in flow, low in pressure and have the ability to accommodate changing intra-vascular volumes. They can, of course, only transport that which they receive, and in the end the net outflow from the left heart has to equal the net return to the right heart. One of the functions of the venous system is to regulate blood volume, and by virtue of the capacitance of the venous system, it can “hold” on to blood by dilating, or it can supply the system with volume, by contracting. The great veins have been designed as pliable tubes to accommodate and transport these changing volumes. Thrombosis is the most common disease plaguing the great veins, particularly as venous access devices are used in increasing frequency. Fortunately, in most cases of thrombosis, only one of the great veins is affected. The ability of veins to bypass obstructions is unequalled in the body and in the case of the great veins, the main bridge and collateral between the two, is the azygos system. US for the veins is a powerful multifunctional tool in that when the vessel is accessible it can measure functional aspects such as the velocity, direction, and the nature of flow, together with structural detail such as size and shape. Since both great veins are deep and are protected and surrounded by structures that may be difficult to penetrate with US, other modalities are frequently called upon to assist. CT and MRI have a global perspective and can view the innards as well as the outer aspects of the vessels. Venography may be called upon to be a final arbitrator, but in the end, also has the final and only word in acute therapeutic intervention.