

Upon completion of this course, the participant will be able to:
-
- define lung carcinoma and discuss the structural and functional changes seen with this type of cancer
-
- identify the structures of the lung and briefly discuss the blood supply
-
- describe lung cancer including its prevalence, cause and predisposing factors
-
- review the imaging procedures utilized for the patient with lung cancer
-
- discuss the most common treatment modalities for a patient with lung cancer
Introduction
Carcinoma of the lung is a malignant disease originating in the epithelium of the airways or respiratory alveoli, with the exact cause not known but with multiple well known high risk factors including cigarette smoking as the major contributor.
The result is a space occupying abnormality in the lung or bronchus with both mechanical and functional effects.
The patient is usually asymptomatic in the early stages, but as the disease progresses symptoms may include coughing, shortness of breath, hemoptysis, chest pain, weight loss, loss of appetite, wheezing, fever, and hoarseness.
The diagnosis is initially suspected based on the patients clinical background and a suspicious CXR, and then may be confirmed by sputum cytology,CT scan, bronchoscopy, positron tomography (PET) scan, lung biopsy, or mediastinoscopy.
Treatment options include surgery, radiotherapy, and chemotherapy. Stenting of occluded bronchi with metallic stents helps open obstructed bronchi. Newer techniques in therapy include endobronchial laser therapy and photodynamic therapy (PDT).
Lung cancer is treated according to the histological type and the stage of the disease. Small cell carcinoma is managed primarily by chemotherapy and sometimes radiotherapy, while non-small cell carcinoma has a wider variety of options including surgery, radiotherapy, and chemotherapy.
Cancer, named as such by Hippocrates as “karkinos,” meaning crab, because the blood vessels surrounding malignant tumors resembled crabs (32222).

The post mortem specimen of the lung and overlying pleura is from a patient who died of metastatic cancer. A surface metastasis to the pleura causes obstruction and distension of the pleural lymphatics and is seen as white irregular vessels coursing to (or from) the mass. These lymphatics are normally about the thickness of a hair and not commonly visualized. In this instance, they are obstructed by the tumor, and are therefore distended with white lymph and at about .05mm (thickness of the pin) they are readily seen. This image, to the author’s eye, has a crab-like shape with the nodule representing the body, and the lymphatics reminiscent of the legs.
Courtesy of: Ashley Davidoff, M.D.

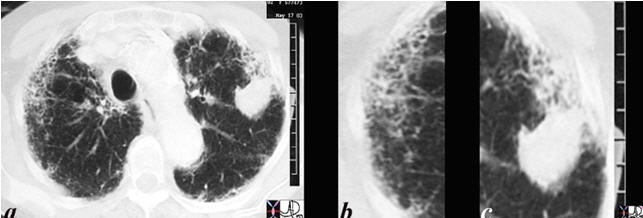
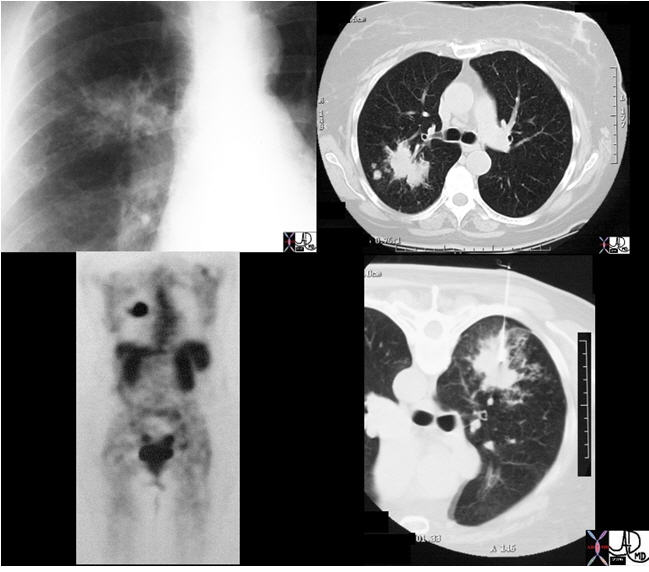
The CT scan is from a middle-aged male with a mass in the left upper lobe (b in green) characterized by a spiculated border (c) extending to the pleura, an ipsilateral A-P window node (overlaid in green in d) and profound emaciation. It is very likely that this is a cancer ? but the approach requires a thoughtful manner of diagnosis and treatment.
Courtesy: Ashley Davidoff, M.D.
Principles
In this section we discuss the principles of structure and then the principles of malignant growth and the structural changes that occur.
Structural Principles
From the outset is important to understand the classification of lung cancer since the biology and approach to therapy depends significantly on this understanding.
There are two broad categories of lung cancer:
Small Cell Lung Cancer (SCLC)
Non-Small Cell Lung Cancer (NSCLC)
The reason for dividing them in this way is that SCLC is an aggressive, non surgical disease with no curative possibility at this time, while treatment of NSCLC depends dominantly on staging, where earlier stages have surgical and curative possibilities.
Non-small lung cancers also are divided into:
- Squamous cell carcinoma
- Adenocarcinoma
- Bronchioloalveolar carcinoma (adenocarcinoma with lepidic Growth)
- Large Cell Carcinoma
The lung cancers are structurally divided into those that have a predilection for the larger airways and are called central cancers (more commonly small cell cancer, and squamous cell cancer) and the peripheral cancers that occur in the smallest airways and alveoli (more commonly adenocarcinoma and its subtypes bronchioloalveolar carcinoma and large cell carcinoma).
There are many implications in this structural division of tumors but of great significance is the fact that the major vessels including arteries, veins, and lymphatics take origin or converge at the hilum centrally so that space occupation in this region has far reaching effects on the tree-like structures more peripherally. The peripheral tumors, on the other hand, are close to the end of the line of the branching structure and so the structural implications are not as great.
Principles: Central Cancer
The central system in this context incorporates the main bronchi, through 16-23 divisions to, but not including the terminal bronchioles. The first division after the trachea results in the right and left main stem bronchi, and then branching follows to lobar bronchi (right upper, middle and lower, left upper, and lower), segmental, subsegmental bronchi and then lobular bronchioles. At this point, the central airways transitions into the peripheral system at the level of the terminal bronchioles.
About 75% of lung cancers originate from the first order, second order and third order bronchi. Within this group of central airways, the dominant tumors include small cell carcinomas (75-80% of SCLC occur in this region) and squamous cell carcinomas (65% of squamous cases occur in this region). The flexible bronchoscope has an external diameter that ranges between 4.9-6.2mm which will allow access to the 5th and even 6th generation bronchus (Naidich). Ultra-thin bronchoscopes enable access to the 10th generation bronchus (outer diameter 2.7mm -3.8mm).
The Central Airways
An axial and a sagittal view of a centrally placed carcinoma that lies on the major fissure of the right lung code lung mass fissure likely carcinoma central probability of it being a squamous cell carcinoma or a small carcinoma is high because of its central location.
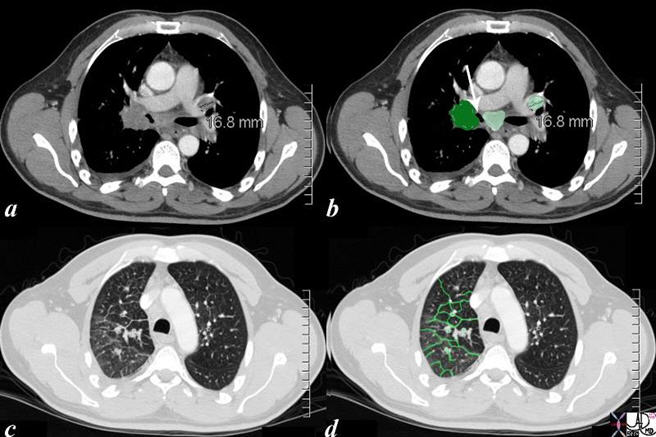
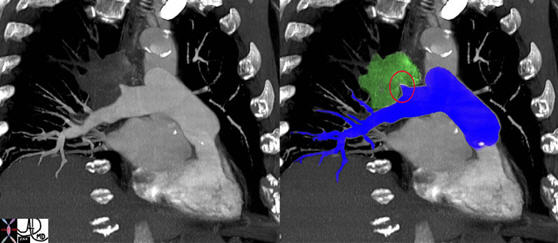
The CT scan of the centrally positioned small cell carcinoma has structural implications as a result of its central location, and close proximity to large arteries, veins, airways and lymphatics. In this case the centrally placed tumor (dark green in image (b) is pushing on the right mainstem bronchus (shown with white arrow). There is extension into the interlobular septa (bright green in d). Subcarinal nodal involvement and left hilar involvement (light green in b) together with small right effusion (a, b) are also noted suggesting advanced disease.
Courtesy: Ashley Davidoff, M.D.
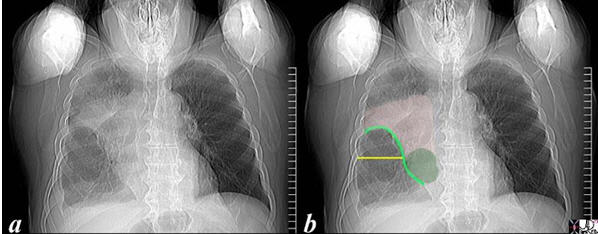
The scout film performed prior to a CT scan from a 76-year-old man with chest pain and shortness of breath. The appearance suggests atelectasis of the right upper lobe with the normal position of the minor fissure (yellow) altered so that the upper portion (light green above the yellow line) is shifted upward caused by volume loss of an atelectatic right upper lobe (pink). The lower portion of the fissure (light green below the yellow line) is bulging rightward and outward caused by an implied mass (dark green). The “reversed S sign of Golden” is demonstrated in this case and infers a central mass causing obstruction and resulting in the shape described by the light green line of the minor fissure.
Courtesy: Ashley Davidoff, M.D.
Principles: Peripheral Cancer
The peripheral system starts at the terminal bronchiole, which after it divides becomes the respiratory (acinar) bronchiole, alveolar duct, and finally the termination of the system ? the alveoli. It is in this region that the peripheral carcinomas commonly arise including adenocarcinoma, its variant bronchioloalveolar carcinoma (BAC) and large cell carcinomas.

This artistic rendition of the small parts of the lung shows the beginning of the peripheral system just before it enters the acinus. This duct is called the terminal duct and it is the last part of the ductal system that has no ability for gas exchange. After its first division, the bronchioles become the respiratory bronchioles, and they are the first in the system to have an ability to both transport the gases as well as enable gas exchange.
Courtesy of: Ashley Davidoff, M.D.
Principles: The Terminal Bronchiole and Acinus
The terminal bronchiole is the last airway of the tracheobronchial tree whose sole function is to transport air but without the ability to enable gas exchange. It measures about 0.7mm.
It terminates by dividing into sac-like protrusions, which allow gas exchange to start taking place. The first branch that is able to perform this gas exchange is called the respiratory bronchiole (acinar bronchiole) which measures about 0.5mm. After three divisions the respiratory bronchioles become alveolar ducts and after further division become alveolar sacs. Finally, at the terminal end of this pathway, the alveoli emerge.
The acinus is defined as the portion of lung that is distal to the terminal bronchiole (Webb) and is supplied by the respiratory bronchiole and usually measures about 6-10mm in diameter (Osborne).
The acinus is functionally characterized by having the ability to both conduct air as well as enable gas exchange. When it is filled with fluid, it can be visualized on a chest x-ray (CXR) as a 6-7mm density called an “acinar shadow.” As a structural entity it has little diagnostic utility. We will expand on the pulmonary lobule in the next section which has greater implications for the imaging of the lung. Functionally, however, the acinus can be considered as the unit of gas exchange in the lung.

This is a drawing of a terminal bronchiole and an acinus which resembles a bunch of grapes. The most upstream component is the terminal bronchiole (the main stalk of the bunch of grapes) which is the first order branch in the peripheral system. It does not have alveoli associated with it and for this reason is not part of the acinus. Its function is to transport the air to the respiratory bronchiole, alveolar sac and alveoli, all of which have the ability to exchange gas.
Courtesy: Ashley Davidoff, M.D.
42650
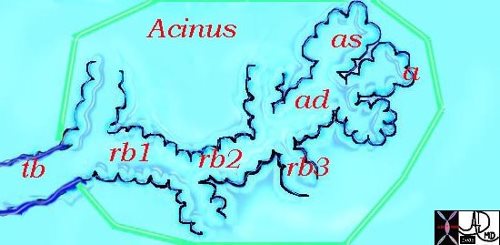
This diagram illustrates the terminal bronchiole and the acinus which consists of the respiratory bronchioles (rb 1, 2, 3), the alveolar duct (ad), the alveolar sac (as) and the alveoli (a). The green border defines the acinus.
Courtesy: Ashley Davidoff, M.D.
42446b12
Principles: The Secondary Lobule
The secondary lobule (Webb) is the fundamental functional and structural unit that is enclosed in a membrane, measuring between 1-2.5cm in diameter and is subtended by a small bronchiole and arteriole. There are usually between 8-12 acini per lobule, but this number varies between 3 and 24 (Itoh).

This drawing shows about 3-4 respiratory bronchioles that serve to make a secondary lobule. Alveolar sacs and individual alveoli are also seen. The yellow border represents the visceral pleura on the surface.
Courtesy of: Ashley Davidoff, M.D.

This image is a panoramic view of the lung, showing in this case, almost rectangular secondary lobules surrounded by interlobular septa (cream borders). The distal bronchioles (teal) and pulmonary arteriole (royal blue) are shown in the centre of a lobule in the right lower corner. The branches of these two structures are shown in the secondary lobule with the acinar airways shown in teal and the presumed course artistically inferred in royal blue. Within the interlobular septa (light pink), remnants of the pulmonary venules (red – inferred) and lymphatics (yellow inferred) are present, traveling in the opposite direction to the arteriole and the airways as they take oxygenated blood and lymphatics toward the hila.
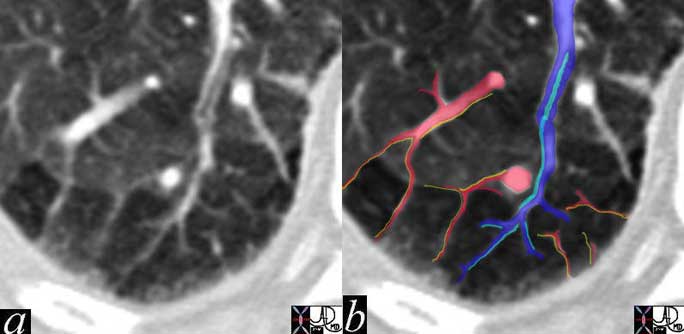
In this remarkable CT we were able to identify a few secondary lobules at the periphery of the lung that have a rectangular shape in this instance. The branching structure that enters the lobule (blue in b), is characterized as an arteriole for two reasons. Firstly, it is paired with a tubular airway seen in (a) in its most proximal portion as a lucent tubule, and subsequently interpolated in light blue in b. Secondly, it branches in the center of the lobule. It is distinct from the border forming interlobular septum which surrounds it. A second relatively large vessel colored in red receives a branch from the interlobular septum and by virtue of its size and position it has to be a pulmonary venule. We know that the lymphatic vessel accompanies the venule, and so the yellow lymphatic has been implied but not visualized. We also know that connective tissue surrounds these two structures. In this instance, the matrix of the lobule that consists of the alveoli is less dense than it should be and is surrounded by normal alveoli. Lucency implies air trapping and air trapping implies small airway disease. Thus this image tells us that the criminal in this case of disorder is the small airway. We now can focus on the small airways with a pathological differential diagnosis, and from there plan the treatment.
Courtesy of: Ashley Davidoff, M.D.
The peripheral lesions from the terminal bronchiolar and alveolar epithelium are mostly, but not universally, adenocarcinomas and are distinguished by a glandular epithelium with fibrous and stromal response around tumor cell nests. Adenocarcinoma destroys the tissues and connective tissue infrastructure, incites desmoplasia and invades the lymphatics. It sometimes produces mucus.
Bronchioloalveolar carcinoma (BAC) arises from and grows along alveolar surfaces, spreading along the infrastructure, and uses the framework to spread without tissue destruction, with resulting pneumonia-like appearance on the CT scan.
Cancers arising in the periphery are mostly asymptomatic in the early stages ? and therefore at the time of presentation are usually more advanced.
Principles: Draining Lymph Nodes
Two sets of lymphatic vessels drain the lung of lymph. A sub pleural lymphatic network collects the lymph from the peripheral lung tissue and drains it along the veins leading toward the hilum. There is a deeper lymphatic system that originates around the bronchi and the bronchioles. The deep system joins the lymphatics around the larger bronchi and pulmonary arteries and they finally enter the mediastinum where they join the bronchomediastinal trunks. The final common pathway for all the lymphatics is via the thoracic duct which enters the left subclavian vein.
Most of the visible lymph nodes are within the hila and mediastinum. However, there are lymph nodes that lie close to the periphery of the lung. These are relatively small measuring approximately 2mm in diameter. They become larger towards the hila, reaching diameters of between 5 to 10mm.
There are four basic groups of nodes:
Superior Mediastinal Nodes
1=Highest Mediastinal Nodes
2=Upper Tracheal Nodes
3=Prevascular and Retrotracheal Nodes
4=Lower Paratracheal Nodes
Aortic Nodes
5=Subaortic Nodes (A-P window)
6=Paraaortic Nodes (Ascending Aorta or Phrenic)
Inferior Mediastinal Nodes
7=Subcarinal nodes
8=Paraesophageal Nodes
9=Pulmonary Ligament Nodes
N Nodes
10=Hilar Nodes
11=Interlobar Nodes
12=Lobar Nodes
13=Segmental Nodes
14=Subsegmental Nodes
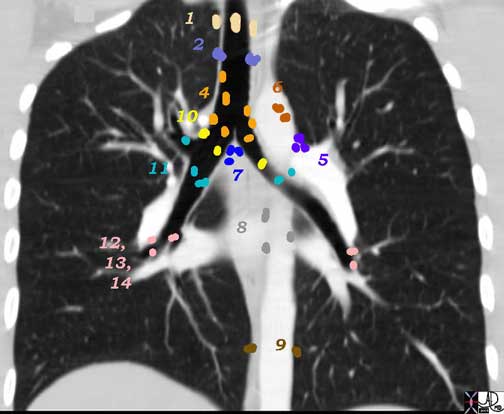
Reference numbers are a means of standardizing the nomenclature of lymph nodes in the chest and the above diagram defines and demonstrates the nomenclature.Superior Mediastinal Nodes
1 Highest Mediastinal Nodes
2 Upper Tracheal Nodes
3 Prevascular and Retrotracheal Nodes
4 Lower Paratracheal Nodes
Aortic Nodes
5 Subaortic Nodes (A-P window)
6 Paraaortic Nodes (Ascending Aorta or Phrenic)
Inferior Mediastinal Nodes
7 Subcarinal Nodes
8 Paraesophageal Nodes
9 Pulmonary Ligament Nodes
N Nodes
10 Hilar Nodes
11 Interlobar Nodes
12 Lobar Nodes
13 Segmental Nodes
14 Subsegmental Nodes
Ashley Davidoff MD
Principles of Malignant Disease
Malignant cells occupy the space of normal tissue but they do not contribute to the structural or functional welfare of the body at large. They arise in the lung more commonly in the proximal airways and they either occupy the lumen or extend beyond the lumen and occupy parenchymal space, which may cause mass effect on other neighboring structures including blood vessels, lymphatics, pericardium, pleura, heart, and esophagus. Partial or total blockage of the bronchi results in obstruction and atelectasis, which can be complicated by secondary infection and bleeding.
Normal cells reproduce about 50 times before dying. Malignant cells, however, grow uncontrollably.
Malignant cells lack contact inhibition, meaning that they do not stop growing when they make contact with another object. The tumor may invade a neighboring tissue or organ and impede its function. A malignant tumor may release an angiogenetic growth factor, enabling the formation of feeding blood vessels.
Invasion of the lymphatics and venous structures is inevitable though invasion of arterioles does not usually occur. Once in the mainstream of the venous or lymphatic system they can metastasize and reestablish a new colony with similarly aggressive and parasitic features. The usual “next stop” for hematogenously spread lung primaries is the brain. In the end, malignant disease dominates the body and the healthy structures succumb to the unbearable burden.
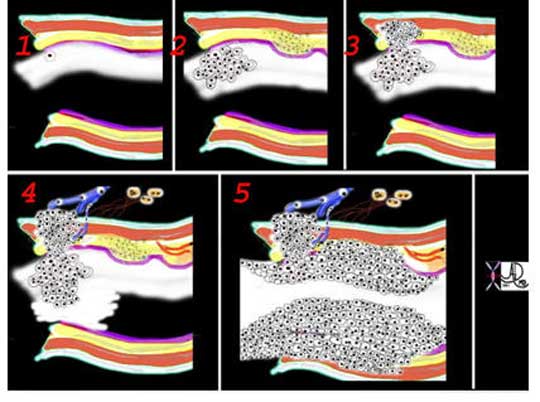
This is a collage showing the evolution of a malignant cell (1) into a nodule restricted to the epithelium (2) which with time penetrates the basement membrane and progressively extends into the submucosa and muscularis (3). Subsequent extension into local lymph nodes and blood vessels occurs (4) as well as growth into the lumen. As it grows circumferentially, narrowing and eventually obstruction of the lumen complicates the process (5). Space in tubular systems is limited and malignant growth has no respect for this space or for boundaries. By definition malignant disease is space occupying.
Courtesy: Ashley Davidoff, M.D.
Causes and Predisposing Factors
Although tobacco and smoking have been around since antiquity, lung carcinoma was a rare disease in the early part of the 20th century. In the 19th century, cigars were in vogue, and cigarettes were confined to the poorer people and were made from the remnants of the leaves that were not used for the cigars.
During World War I (WWI), cigarettes were distributed freely by the companies to the soldiers, and the culture received their dividend for this ?kind? deed 20-30 years later when cancer unfolded.
The medical community started to understand the dangerous relationship between cigarettes and cancer in the 1940’s, but WWII and the movie industry introduced a second popular wave in the 30’s and 40’s, so that the medical knowledge was not sufficiently in the public consciousness and was preempted by the movie industry. The second wave caught the fancy of the female population, as cigarettes were portrayed as the elegant and “in” thing to do, and the 60’s saw a second peak of the disease – 20-30 years later.
The earlier carcinomas were dominated by squamous carcinoma, but there has now been a shift to adenocarcinoma. The reason for this is not obvious but two explanations are forth coming. It is well known that adenocarcinoma is more likely to occur in females and squamous in males and since a large part of the second wave was the introduction of smoking in females, an appropriate rise in adenocarcinoma occurred. It is unknown why females have a tendency to adenocarcinoma, (rather then squamous) but this seems to be well recognized. The second explanation relates to the modification and reduction of nicotine content and development of filters by the companies as a result of the evolving knowledge of the relationship to cancer. This was the compromise of the companies to take “responsible? action. Cigarette smokers reacted by deeper and longer draws on the cigarette, bringing the smoke and carcinogens into contact with the alveolar epithelium and hence the evolution of the peripheral carcinoma – ie adenocarcinoma.
Deaths
The World Health Organization maintains that approximately 3,000,000 people die worldwide each year as a result of smoking. In the 20th century approximately 100 million people died from tobacco associated diseases. It is the most common type of new cancer cases at 1.2 million new cases, or 12.3% of new cancer cases in the world (Huq). Overall, lung cancer is the most frequent fatal malignancy and accounts for more than 7% of all deaths in both sexes.
The annual number of deaths from lung cancer in the United States increased from 18,000 in 1950 to an estimated 158,000 in 1997 and 162,000 in 2008 (American Cancer Society).
In the USA, lung cancer is the leading cause of cancer deaths in both men and women.
171,600 new cases of lung cancer account for 31% of cancer deaths in men and 25% cancer deaths in women, resulting in a total of 158,900 deaths.
In other areas of the world, it is the leading cause in men and the second or third cause in women.

The CT scan through the chest of an 80-year-old male shows a large lung mass in the posterior aspect of the right upper lobe (overlaid in green) and three small nodules in the left upper lobe (overlaid in green). The patient is obviously a smoker and the incriminating pack of cigarettes is identified in his right shirt pocket containing 9 cigarettes. The lung cancer was shown to be an adenocarcinoma. The pathology of the nodules may either represent metastatic disease or multicentric foci of bronchioloalveolar cell carcinoma. An associated finding of a thinned, anterior junction line suggests hyperinflation and emphysema, and the thickened bronchial walls noted in the right lung suggest chronic bronchitis. A saber-shaped trachea is also reminiscent of emphysema. The patient is emaciated, a finding that relates both to his chronic lung disease and his cancer.
Courtesy of: Ashley Davidoff, M.D.
Cigarette Smoking
95% of cases of lung cancer are directly related to cigarette smoking.
Patients who have asbestosis and are smoker’s have a 90 times increase risk to develop lung carcinoma.
One pack of cigarettes per day increases the risk of developing lung cancer by 20-25 fold
Two packs a day for 20 years increases the risk of developing lung cancer by 60-70 fold when compared to a non smoker
Adults – approximately 45 million smoke cigarettes
Teenagers – approximately 2.4 million smoke cigarettes
High school seniors – 38% smoke.
It takes about 10 years for a previous smoker to reach a non smokers risk levels.
Cessation of smoking for 10 years reduces risk to control levels.
Smokers lose an average of 15 years of life.
Only 6% of smokers are successful in permanent cessation and 70 to 80% who do stop smoking return to the habit.
Changing Histological Patterns
Non-Small Cell Lung Carcinoma (NSCLC) accounts for almost 80% of cases, consisting of adenocarcinoma and squamous cell carcinoma. Small Cell Lung Carcinoma (SCLC) makes up 20% of cases.
Adenocarcinoma (a NSCLC) is the most common type of lung cancer, and makes up 30-35% of all cases. Adenocarcinoma has replaced squamous cell carcinoma as the most frequent histological subtype.
Squamous cell carcinoma (also a NSCLC) is the second most common type, making up about 30% of all lung cancers.
Large-cell cancer makes up 10% of all cases.
Extent of Disease at Clinical Presentation
15% of patients have only localized disease at diagnosis
25% have disease spread to regional lymph nodes
>55% have distant metastases
Treatment and Prognosis
At presentation, approximately one-third of patients are stage I, II,or IIa, meaning they have disease localized enough for a curative attempt with surgery or radiotherapy. A further 30% have IIIA or IIIB with local or regional disease that has equivocal curative capability and the last 30% are stage IV meaning they have distant metastatic disease and are incurable.
Eighty-six percent of patients with lung cancer die within 5 years of diagnosis and only about 14% of people who develop lung cancer survive for 5 years
Genetics
There is no strong pattern of Mendelian inheritance. However, in patients who have inherited disorders, such as in adult retinoblastoma (inherited mutation is rb) and Li-Fraumeni syndrome (p53 gene), there is an increased incidence in lung cancer. First degree relatives of patients with lung carcinoma have a predisposition to develop all types of carcinoma and so patients with lung carcinoma should be educated, so that their families can become aware of this fact. There has been an association between the p450 enzyme and lung cancer.

Courtesy: Ashley Davidoff, M.D.
Statistics
In 2001, there were about 1,238,861 new cases of lung cancer in the world. There were 337,115 cases in females and there were 901,746 cases in males, a ratio of 1:2.7.
Lung cancer accounts for 31% of all cancer deaths in men and 25% in women in the USA. When the non smoking cancer population is considered, women appear to have a ~1.5 fold higher susceptibility to lung cancer than men.
Dietary Factors
Beneficial Effects
Fruits and vegetables contain nutrients called phytochemicals, which have reported beneficial effects. Phytochemicals in vegetables include:
- Isothiocyanates, found in broccoli, cauliflower, and brussels sprouts
- Flavonoids, found in apples, grapefruit, onions, red wine, and tea
- Soy protein and Lycopene, found in tomatoes
Vitamin C, selenium, cod liver oil, folic acid, vitamin B12, Vitamin E, and Vitamin A may also decrease the risk of getting lung cancer.
Detrimental Effect
Fat and alcohol may increase the risk.

Predisposing and Associated Diseases
Predisposing factors include smoking, exposure to second-hand smoke, radon, asbestos, arsenic, and pollution, other respiratory diseases, and having lung cancer previously. The strongest risk factors for lung cancer are tobacco exposure, previous history of lung or head and neck cancer and family history of lung cancer.
Diseases associated with smoking and lung cancer include emphysema, chronic bronchitis, and chronic obstructive pulmonary disease (COPD). Patients with these disorders should be closely monitored for carcinoma. This is a large and very important group in whom selective screening techniques should be applied. A patient with COPD who is a non smoker has a five-fold increased risk of lung cancer.
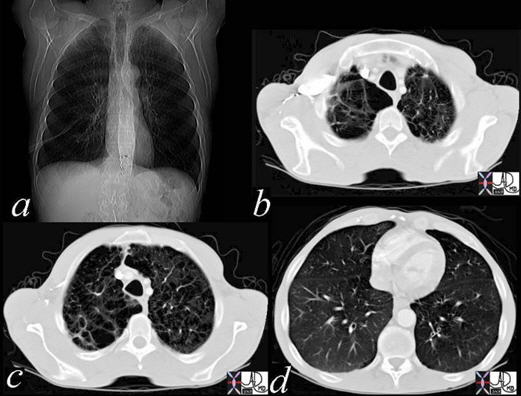
The flattened diaphragms in (a) are a clue to the hyperinflated lungs, confirmed by the architectural distortion, loss of structural integrity, and large bullous spaces particularly in the right upper lobe (b, c,). The loss of the subcutaneous fat and muscle is also characteristic of the disease (d).
Courtesy: Ashley Davidoff, M.D.
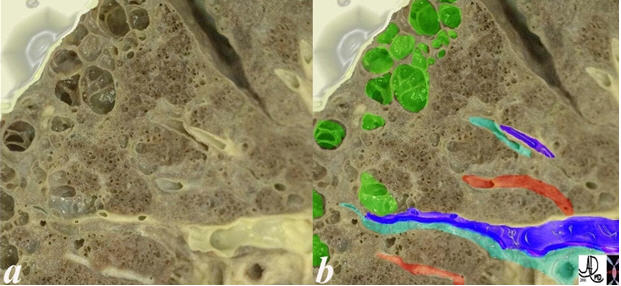
This anatomic specimen reveals the appearance of an emphysematous lung. Note the larger air spaces (lime green), bronchovascular bundle containing an artery (royal blue artery) and an airway (teal ). The pulmonary vein (red) lies between two bronchovascular bundles.
Courtesy: Ashley Davidoff, M.D.

An artistic interpretation of centrilobular emphysema. The first image is the normal terminal bronchiole and acinus. The second (green) shows the characteristic proximal dilatation of the respiratory bronchiole, (rb) with some sparing of the distal part of the acinus.
Courtesy: Ashley Davidoff, M.D.
Patients with other chronic lung diseases such as tuberculosis (TB) and chronic interstitial disease of scleroderma are at increased risk. These cancers usually arise in scars and are called scar carcinomas. When a calcification becomes eccentrically placed, it is a clue to the malignant transformation of the lesion.
This CT scan is from an 82-year-old male with interstitial lung disease who developed a peripheral lung cancer within the reticular disease in the periphery of the lung. The interstitial disease is highlighted and magnified in image (b) and the mass among the interstitial disease in the left upper lung is shown in (c). In this instance, the pathology showed squamous cell carcinoma, which is the type usually associated with chronic irritation.
Courtesy: Ashley Davidoff, M.D.
Predisposing and Associated Diseases: Asbestos, Radon, Uranium, Nickel and Other Metals
Asbestos exposure increases the risk of lung cancer by five times. A combination of asbestos exposure and cigarette smoking compounds the risk by as much as 50 times, and if the patient has asbestosis and is a smoker, the risk almost doubles to a 90 times increase. Lung cancer among asbestos workers is more common than mesothelioma. These patients also develop gastrointestinal cancers.

The CT through a mass in the LUL shows focal pleural calcification overlaid in green (2, 4) in this patient with asbestos related disease. A pneumothorax followed the biopsy revealing that the pleural plaques are positioned on the parietal pleura (3, 4). A small amount of air introduced from the xylocaine injection outlines the parietal pleura (5,6 – green).
Courtesy: Jorge Medina, M.D.
Lung cancer in non smoking, uranium miners occur 4 times more frequently than in the general population, and occurs even more frequently among miners who smoke. People who work with nickel, chromates, coal, mustard gas, arsenic, beryllium, and iron are more susceptible to develop lung cancer. Radon is ubiquitous and miners may be exposed to particularly high concentrations. A higher incidence of lung cancer in gold miners has also been noted.
In the environment, pollution, radon, and radiation are predisposing elements to the development of lung cancer. An increased incidence of lung cancer among survivors of the Hiroshima and Nagasaki atomic bomb was noted.
Etiological Agent ? Cigarettes
John Hill, a London physician, first recognized an environmental cause from the dangers of tobacco use in 1761 and published a book ?Cautions Against the Immoderate Use of Snuff?. The carcinogenic effects of tobacco are due to the polycyclic aromatic hydrocarbons, which are found in the tars, produced by combustion of tobacco. However, there are innumerable (more than 1200), potentially carcinogenic substances in cigarette smoke as well. None of these have been shown to produce classical carcinoma in animals in the lab, but some have produced alveolar cell carcinoma – a carcinoma that bears the least causal relationship to smoking. Nicotine also contains carcinogens. It forms nitrosamines such as 4-(N-methyl-N-nitrosamino)-1-(3-pyridyl)-1-butanone (NNK) which is a carcinogen identified in tobacco smoke by Hoffmann and Hecht.
Cigarette smoking has the highest causative link with carcinoma of the lung. Cancer risks for cigar and pipe smokers are significant, but less than those for cigarette smokers.

These diseases are all about cigarettes and the garbage that they deposit in our lungs, predisposing to bronchitis emphysema and lung cancer.
Courtesy of: Ashley Davidoff, M.D.
Factors that increase the risk of developing cancer in smokers include the number of cigarettes/day, the length of the habit, and the depth of inhalation.
Number of Cigarettes Per Day And Risk
One pack of cigarettes per day increases the risk of developing lung cancer by 20-25 fold
Two packs a day for 20 years increases the risk of developing lung cancer by 60-70 fold when compared to a non smoker
Change of Cigarette Design
In the US, cigarettes now have a lower tar content and are almost all filtered, which has resulted in a decrease in the amount of polycyclic aromatic hydrocarbons (PAHs), and appears to be lowering the risk of lung cancer. However, there has also been an increase in the amount of carcinogenic tobacco-specific n=”nitrosamines” (TSNAs) which have been shown to induce adenocarcinoma in lab animals.
Pathogenesis
In this section we deal with the back and forth battle of the malignant process with the body?s defense mechanism and with the structural and functional result that follows.
Pathogenesis: Initiating Event and Growth
The initiating event is presumably the effect of a carcinogen on the genetic makeup of a cell or group of cells that survive the insult and continue to grow and thrive at the expense of the host tissue and organ. The oncogenes become dominant and there tends to be a reduced effect of recessive tumor-suppressor genes. Ten to twenty genetic mutations of the aberrant cells may occur by the time the tumor is clinically apparent. The lack of contact inhibition allows the local spread of the disease.
Growth
An area in the epithelium of in situ cytological atypia presumably forms resulting from a small space occupying lesion on the mucosa. With progression, the conglomerate of malignant cells elevates the mucosa which may eventually ulcerate.
This is a collage showing the evolution of a malignant cell (1) into a nodule restricted to the epithelium (2), which with time, penetrates the basement membrane and progressively extends into the submucosa and muscularis (3). Subsequent extension into local lymph nodes and blood vessels occurs (4) as well as growth into the lumen. As it grows circumferentially, narrowing and eventually obstruction of the lumen complicates the process (5). Space in tubular systems is limited and malignant growth has no respect for this space nor for boundaries. By definition malignant disease is space occupying.
Courtesy: Ashley Davidoff, M.D.
The mass grows along lines of least resistance but can overcome natural planes. Therefore, it may grow into the lumen, or through subsequent layers of basement membrane, muscularis and adventitia or through the lung parenchyma.
The invasion of the lymphatics, venous structures and pleura is inevitable with time.
The frequency of nodal involvement varies slightly with the histological pattern but averages greater than 50%. The adrenals are involved almost 50% while the liver (30 to 50%), brain (20%), and bone (20%) are commonly involved.
The body is able to respond to this aggressor, but it has to recognize the cell or group of cells as foreign. Most the time it is able. There are presumably many instances when such activity is identified as clandestine and is treated effectively by the immune system. However, there are instances where the malignant cells get away with murder, perhaps under the continued stimulus of a carcinogen in a background of genetic predisposition, and find the loophole in the immune system that allows the malignant cells to survive.
The result is space occupying disease and depending on the location and degree of structural change symptomatology, clinical and radiological findings will differ. Partial obstruction may cause focal emphysema while a total obstruction may lead to segmental or subsegmental atelectasis. Secondary infection may result in bronchitic, and or pneumonic change and subsequently even abscess formation.
Venous structures can also be compressed, the most dramatic of which is the involvement of the SVC and resulting SVC syndrome with total obstruction of the SVC, and head and brain swelling.
Classification and Histopathology
The two most important classifications are the histological and the Tumor (T) status descriptors for tumor, node, and metastasis (TNM) staging classifications. The histopathological classifications divide the disease into two fundamental groups: small cell and non small cell carcinomas. This distinction is important in the approach to the management and prognostication of the disease.
The staging classification divides the disease into groups based on size of tumor, extent of adenopathy, and systemic extent of disease. Other classifications that are helpful include the functional status of the patient in considering surgery, and the radiological classifications of lung tumor based on morphology.
Carcinoma of the lung most commonly presents as a mass and less commonly as an alveolar process which is the mode of presentation for the bronchioloalveolar type. However, because it originates in a tubular system and because of its infiltrative nature, the macroscopic picture will depend on the presence or absence of atelectasis, localized emphysema, associated pneumonia, lymphangitis, pleural involvement and pericardial involvement.
Size
Malignant tumors range in size from a few mms to up to 10 or even 15cm.
Large cell carcinoma is usually large, bulky, and well-circumscribed.
Shape
The tumors themselves are mostly nodular or round or irregularly-shaped, except for alveolar cell which may look like a segmental pneumonia. Bronchoalveolar carcinoma may also take the form of a single nodule or more often, as multiple diffuse nodules that coalesce to produce a pneumonia-like consolidation.
Ashley Davidoff MD
Position
Squamous and small cell carcinomas tend to be central while adenocarcinomas, including alveolar carcinomas, tend to be peripheral, often near a pleural surface. The pleural surface is often pinched over the tumor. Squamous cell carcinoma also tends to be found more commonly in the upper bronchi.
Character
Adenocarcinoma is usually hard to the feel with a white or grey and glistening matrix.
Squamous cell carcinoma usually presents as a well-circumscribed, rubbery mass appearing as a gray-white and dry matrix, often associated with hemorrhage, necrosis, and cavitation. (10-20%) (32202c)
Large cell carcinoma is usually a well-delineated, bulky tumor with a pink-gray cut surface often complicated by hemorrhage and necrosis.
Bronchioloalveolar carcinoma, may present as a mucinous mass, as a diffuse multinodular lesion, or as an infiltrate.
Classification and Histopathology: Natural History
The two disease types – small cell and non-small cell have very different natural histories. Small cell is aggressive, fast moving and has virtually no chance for cure as most patients have metastatic disease at presentation and surgery is not usually an option for these patients. Untreated, the survival time for patients with small cell cancer is 6 to 17 weeks. The percentage of patients who survive with lung cancer for one year is around 42%.
Non-small cell carcinoma has a slower course and depending on staging at the initial presentation, chance for cure is greater. However, the overall outlook is dismal with a 5 year survival rate of 14%.
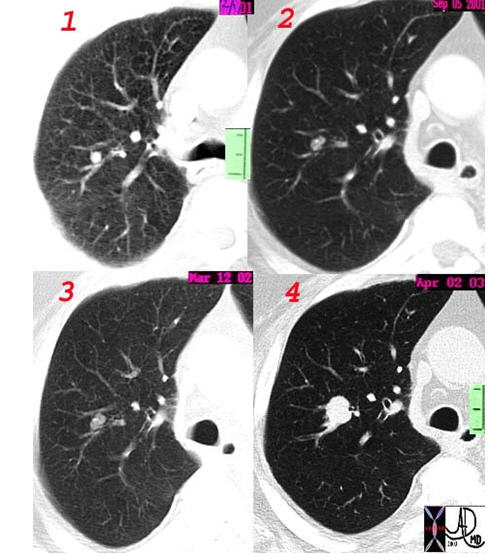
This CT collage shows the growth of a smooth nodule in February 2001 (1) and its evolution of malignant growth through September 2001 (2) as a 4-5mm bi-lobed nodule, then as a <1cm nodule in March of 2002 (3), and finally as a 1.4cm nodule in April 2003 (4), just over two years later.
Courtesy: Ashley Davidoff, M.D.
Extent of Disease at Presentation
15% of patients have local disease at diagnosis
25% have disease spread to regional lymph nodes
55% have distant metastases
Time of Diagnosis to Death
86% of patients with lung cancer die within 5 years of diagnosis and only 14% of people who develop lung cancer survive 5 years
Non-Small Cell Carcinoma
Non-small cell lung cancer (NSCLC) is the more common type of lung cancer and tends to grow and spread more slowly. The three subtypes which have very different morphological characteristics share the potential for cure with surgical resection.
Non Small Cell Carcinoma: Squamous Cell Carcinoma
Squamous cell carcinoma (also know as epidermoid carcinoma) is a malignant condition of the airway epithelium, usually arising from the central portions of the airways and has a strong causative association with smoking. It is the second most common lung cancer, making up 30% of cases.
Structurally, squamous cell carcinoma (SCC) is characterized by its central location and occurs more commonly in the upper lobes. It tends to spread locally to regional nodes and may cavitate, which is a characteristic feature of squamous cell carcinomas, in general.
The histopathology is characterized by the proliferation of flat fish-scale like cells and may be associated and characterized by the production of keratin and intercellular bridges. Well-differentiated SCC contains keratin pearls. The cells have large irregular nuclii, large nucleoli, and coarse chromatin. The cells are arranged in sheets.
Metaplasia, dysplasia, and carcinoma in situ are sometimes present in the tissue surrounding the carcinoma.
Metastatic disease does occur but compared to other lung cancers it is relatively uncommon, occurring in <20% at presentation.
Clinically, it often produces symptoms of cough, dyspnea, or atelectasis, and wheezing or hemoptysis since it is more central in its location and affects larger airways. It is also the lung malignancy that is most often associated with hypercalcemia.
From a diagnostic point of view, its central location and tendency to exfoliate enables cytological diagnosis from the sputum or bronchial washings.
Treatment is based on staging so that stages I, II, and IIIA have curative and surgical possibility, stage IIIb and more advanced are treated with combinations of radiotherapy and chemotherapy.
Axial CT scan through the chest in a 53-year-old male shows a central 2.9cm cavitating lesion, consistent with a squamous cell carcinoma of the lung.
Courtesy: Ashley Davidoff, M.D.
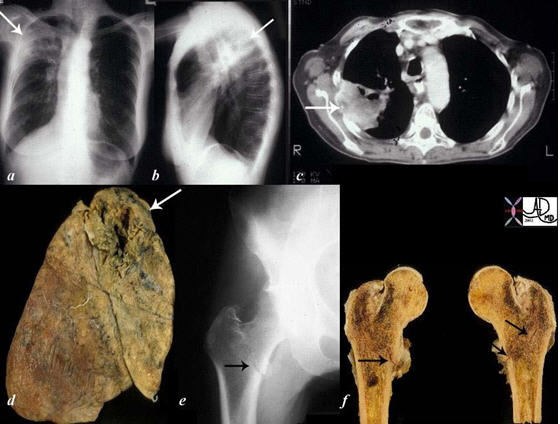
The collage of images reflects a patient with stage IV, cavitating, primary, squamous carcinoma of the right upper lobe (RUL) (a, b, c, d – white arrows) with COPD. A metastatic lesion to the right femur was complicated by a pathological fracture. (e, f black arrows).
Courtesy Ashley Davidoff, M.D.
Non Small Cell Carcinoma: Adenocarcinoma
Adenocarcinoma is a malignant condition of the epithelial lining of the airways, most commonly the peripheral airways and is now the most common type of lung cancer, accounting for 30-40% of all cases.
The causative factors are not as clear as in squamous cell cancer and the association with smoking although present, is not as strong as with squamous cell carcinoma. It occurs in secretory cells. A subtype of adenocarcinoma is called bronchioalveolar cell carcinoma (BAC). Thus, adenocarcinoma can originate from the bronchial mucosa, or from the acinus in which case it results in the bronchioloalveolar type. A pattern from adenomatous hyperplasia, through pure bronchioloalveolar carcinoma, to a combination of BAC and adenocarcinoma, to adenocarcinoma is noted, similar to the hyperplasia, adenoma, dysplasia, malignancy pattern noted in colon carcinoma.
Structurally, it is characterized by its location in the periphery and the occasional association with a known scar. It rarely cavitates but it may calcify. At a histopathological level, rosettes of glandular epithelium, often with mucus, are noted.
Adenocarcinomas tend to grow more slowly than squamous cell carcinomas. It is complicated by early metastasis to local nodes and to distal parts of the body, commonly the pleura, brain, adrenals and bone.
Clinically, adenocarcinoma tends to manifest as peripherally-placed tumors and hence, they are often asymptomatic, but their relationship to the pleura, may incite pleuritic pain or pleural effusion. Their initial silent nature often precludes early diagnosis and so presentation is relatively late and it is not uncommon for the patient to present with metastatic disease.
The diagnosis is made after endoscopic or CT guided biopsy, and after staging with PET scan or with additional biopsy of remote sites; treatment is initiated based on the staging.
Stage I, II, and IIIA are treated surgically with a hope of cure and the more advanced stages are treated with combinations of radiotherapy and chemotherapy.
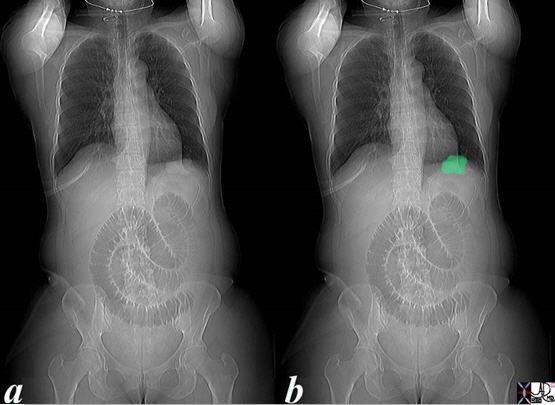
This plain film of the chest and abdomen is from a 51-year-old female who presented with nausea, vomiting, and abdominal distension. A loop of dilated small bowel is associated with absence of air in the decompressed colon and rectum. In addition, a mass is seen in the left lower lobe (green overlay). A barium study showed thumb printing consistent with distal ischemia of the small bowel. The diagnosis in the lung was shown to be adenocarcinoma.
Ashley Davidoff MD
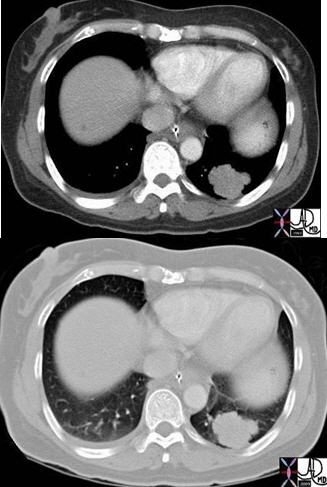
Axial images of the case shown above through the lung mass in a 51-year-old female who presents with nausea vomiting and abdominal distension and who was shown to have a small bowel obstruction. The mass is situated in the left lower lobe and was an incidental asymptomatic finding. It measures in the 3cm range, is lobulated and peripherally located. Pathology showed an adenocarcinoma.
Courtesy: Ashley Davidoff, M.D.
Non Small Cell Carcinoma: Adenocarcinoma with Lepidic Growth (Previously known as Bronchioloalveolar Carcinoma)
Bronchioloalveolar carcinoma, also known as bronchioalveolar and BAC, is a subtype of adenocarcinoma and accounts for about 5% of lung carcinomas, but up to 20% are histologically mixed, adenocarcinoma and BAC.
It has an indolent course and in its pure form, is really a carcinoma in situ, showing no invasive changes. It does have the potential to evolve into frankly malignant and invasive disease. Smoking appears to some extent, to be a causative link, though it has a disproportionate high incidence among non smokers, women and occurs in a slightly younger population. About 30% of patients with BAC have never smoked. It also has a higher incidence in Japan. BAC is sometimes associated with patients suffering from interstitial lung disease (eg scleroderma), and also with the uncommon entity of exogenous lipoid pneumonia. .
Structurally, it is characterized by its unique, relatively slow, lepidic growth, meaning it grows by scaling along the structure of the alveolus or acinus, but does not destroy the architecture. In addition, in its pure form it does not invade vascular, lymphatic, or pleural elements.
When it shows invasive properties, then it is defined as a mixed BAC adenocarcinoma Raz. There appears to be an evolving spectrum from benign to malignant, starting with premalignant atypical adenomatous hyperplasia, then BAC, and then into a subtype of adenocarcinoma (Travis).
There is a mucinous form (80%) originating in the mucus secreting columnar cells, and tending to a multicentric pattern. The non mucinous form (20%) arises from the type II pneumocytes of the alveolus, is localized and has a better prognosis.
Clinically, patients in most instances are asymptomatic and many patients are identified by CT screening programs. When the disease is diffuse, bronchorrhea may occur.
The diagnosis is initially suspected radiologically, presenting as a solitary ground glass opacity (GG0) (45%), as multicentric nodules (GGOs) (25%), or as a consolidation (30%). Inflammatory or infectious disease is considered in the differential diagnosis, but if the radiologic findings fail to respond to conservative therapy, BAC and its variants become more likely, and surgical biopsy is necessary.
When GGO?s are less than 2cm, they are usually pure BAC. As solid components within the GGO become more apparent, adenocarcinoma becomes more likely. When the disease is multifocal, it defines itself as IIIb or IV. PET scanning has limited sensitivity so that only about 50% of lesions have a diagnostic SUV >2.5. The final diagnosis is made at pathology, and requires histological examination to determine invasion. Cytological aspiration is insufficient.
Treatment depends on staging. When in pure form ? as an in situ disease by definition, treatment is surgical and curative. Surgery usually consists of lobar resection, and ipsilateral mediastinal lymphadenectomy. When in the mixed form, 10-25% have lymph node involvement and 5% have distant metastases and therefore, require additional radiation and chemotherapy.
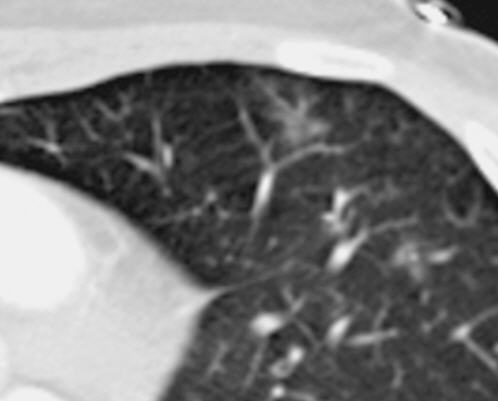
Ground glass opacity in the secondary lobule reflects alveolar process and is one of the presenting appearances of unifocal or multifocal BAC. It is a slow growing in situ disease that may not change in size over two years, but continued surveillance is necessary.
Courtesy: Ashley Davidoff, M.D

The CT is from a 51-year-old male who is a smoker, who shows a ground glass opacity (GGO), mixed with a solid mass (arrow in (a) and multicentric BAC in a lower cut (b), characterised by three areas in the right lower lobe of partial alveolar opacification. Ground glass appearance is the result of partial opacification of the alveoli. Two of the GGOs measure close to 2 cm each and the third more anterior measures about 8mm. In this instance, a PET scan was positive in the area (green ring in d). It is likely that the solid component in image a represents the transformation of BAC – (really a carcinoma in situ) into adenocarcinoma.
Courtesy: Ashley Davidoff, M.D.
Non Small Cell Carcinoma: Large Cell Carcinoma
Large cell carcinoma, also know as large cell anaplastic, is a malignant disease of the epithelial lining of the airways and is the least common of the NSCLC and accounts for 10% of lung cancers. It is characterized by large, clear, undifferentiated, sometimes heterogeneous cells.
Structurally, it is characterized by its peripheral location, highly atypical cells, without evidence of keratinization, or glandular formation, but with areas of focal necrosis. Recent suggestions propose that the large cell carcinomas represent an undifferentiated form of adenocarcinoma.
Small Cell Carcinoma
Small cell lung cancer, also known as SCLC and oat cell cancer, is a malignant condition of the epithelium usually arising from the central airways and specifically arising from the enterochromaffin or Kulchitsky cell, which embryologically originates from the neural crest. Small cell lung cancer accounts for 15-25% of lung cancers, and thus is less common than NSCLC. There is a definite causal relationship with cigarette smoking. The age population is slightly younger than the NSCLC group (27-66 yrs SCLC versus 44-61 yrs in NSCLC). SCLCs grow more quickly than NSCLCs and are more likely to metastasize early. Often, they have already spread to other parts of the body when the disease is diagnosed.
Structurally, the tumor tends to be central, is bulky, fast growing, and usually with early hilar and mediastinal involvement. The malignant cells are characterized by their small size (as their name implies) being <21 microns, which is slightly smaller than 2-3 lymphocyte diameters. They also resemble the lymphocyte in shape and character. Most of the population of cells is round to oval in shape but spindle-or polygonal forms occur as well.
The cytoplasm is usually sparse and the nuclei show a high mitotic rate as a result of the rapid growth. The nuclei are granular and characterized by a salt and pepper appearance with small or inconspicuous nucleoli. The characteristic feature of malignant cells with a high nuclear to cytoplasmic ratio, is also present.
Since they are central tumors, diagnosis is sometimes attained by cytological washings.
Clinically, the patient may manifest with the effects of the tumor on the larger airways, which includes cough, hemoptysis, dyspnea, and wheezing. The central location and tendency to bulky mediastinal involvement sometimes results in SVC syndrome. Paraneoplastic syndromes are characteristic of the disease as well.
The diagnosis is suspected by the CT appearance which shows bulky disease in the hilum and mediastinum. The approach to management is based on whether the disease is ?limited?, which would allow single port treatment with XRT as opposed to ?extensive? disease, which implies it has spread beyond the chest or requires more than one XRT port. PET scanning is extremely useful in staging the disease.
Treatment invokes both XRT and chemotherapy. The tumor has a remarkable and characteristic response to chemotherapy, being specifically sensitive to mitotic inhibitors. It is this characteristic and unique response to chemotherapy that prompted the division and classification of lung cancers into SCLC and NSLC.
Overall median survival for SCLC is 6-10 months. Patients with limited disease have two year survival of 10% and for extensive disease it is only 3%. 70 % of patients have extensive disease on presentation.

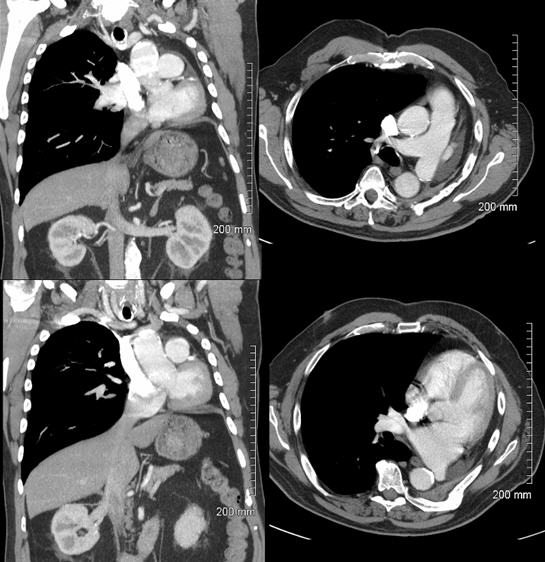
This CT scan is from a middle-aged female with poorly differentiated small cell carcinoma, with extensive mediastinal and hilar involvement (dark green in b) extending into and almost occluding the right main stem bronchus (light green with black air in the centre) and occluding the smaller airways (light green surrounded by white bronchial cartilage). A complex right effusion (yellow) and atelectasis is seen (light pink). The relationship to the SVC (light blue) is noted without mass effect at this time, with the aorta in red and left pulmonary artery in royal blue. Parenchymal disease is suspected based on the increased soft tissue noted in the mediastinal windows in the right lower lobe.
Courtesy: Ashley Davidoff, M.D.

Courtesy: Ashley Davidoff, M.D.
The coronal image shows a centrally placed small cell carcinoma (green mass in right image) occluding the right upper lobe pulmonary artery (red ring).
Images courtesy: Ashley Davidoff, M.D.
Complications of Lung Cancer in General
The result of neoplastic disease is space-occupying disease. Depending on the location – different structural and functional effects and hence, complications will result. Local obstruction of the airways will expectedly result in localized atelectasis. Involvement of the pleura will be complicated by pleural effusion and if the pericardium is involved – pericardial effusion. If these accumulate rapidly or sizably they may respectively affect the function of the lung and heart. Acute tamponade can be life-threatening.
Invasion into the lymphatics can result in lymhangitis obliterans, sometimes with significant respiratory compromise and marked dyspnea. Obstruction of the SVC may result in SVC syndrome, sometimes with dramatic face swelling and discoloration.

76-year-old female with central lung cancer and superior vena cava (SVC) syndrome as noted by this scout film following contrast injection, where contrast is trapped in the right subclavian system because of the obstruction of inflow. Note also the significant swelling of the face and neck which was new for this patient.
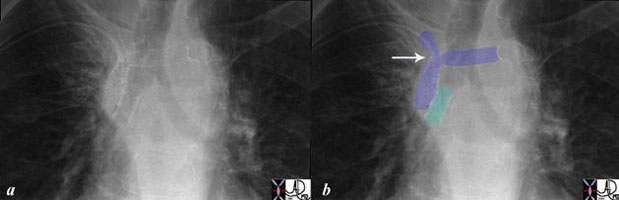
This is a case of a central squamous carcinoma causing obstruction of the right mainstem bronchus and SVC, requiring stents in both. The right main stem bronchus has been opened with a single short stent (teal). The obstruction of the SVC was at the confluence of the right internal jugular and brachiocephalic vein. A residual narrowing (arrow) where the tumor is located is still noted. A second stent is in the brachiocephalic vein (royal blue horizontal stent). This image tells the story of how tubular transport function is compromised by reduced size and how size can be restored by modern technology.
Images courtesy: Ashley Davidoff, M.D.
Metastatic Disease
Metastatic disease to the bone can result in a pathological fracture to the spine which at the extreme can cause significant neurological compromise and a need for urgent radiation therapy.
Another dramatic clinical presentation may be as a result of brain metastases, while bilateral adrenal metastases, in the extreme, can cause an Addisonian crisis.
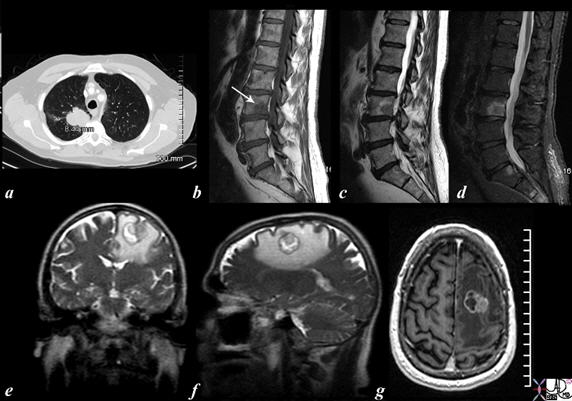
The CT scan and MRI images are from a 56-year-old male who presented with back pain and a neurological deficit. The CT scan of the chest shows a right upper lobe lung mass and the MRI of the spine (b= T1, c =T2 and d= STIR) confirms the presence of a metastasis in L3 while the MRI of the brain (e= T2 coronal, f = T2 sagittal and g= post gadolinium study) reveals a mass in the high left parietal lobe with surrounding edema {white around the round tumor in (e) and (f) and showing enhancement (g)}.
Courtesy: Ashley Davidoff, M.D.

This coronal reformat of the thoracic spine in a patient with known lung carcinoma and blastic metastasis reveals an ivory vertebra. It is characterized by diffuse involvement with blastic disease. Other focal blastic changes in the vertebra are present as is a large layering posterior pleural effusion.
Images courtesy: Ashley Davidoff, M.D.
Clinical Presentation
In this section we discuss how the structural changes translate into the functional effects in the patient. We include the symptoms and signs of lung cancer and advance to the clinical assessment, the process of clinical decision-making and diagnostic and therapeutic courses available.
The symptoms are usually quite insidious since the patients that we are talking about are usually long time smokers who have adapted to the chronic cough of bronchitis and a degree of dyspnea from emphysema or COPD. However, these symptoms may become slightly more accentuated and it takes the patient about 7 months to realize that there is something different happening.
The structural changes usually translate into symptoms of irritation and changes or loss of function. Since the tumor is of the airway epithelium, irritation manifests as a cough (75%) and less commonly as increased sputum production. Direct extension into the pulmonary parenchyma, or associated collapse or frank pneumonia may translate into increasing dyspnea (20%). The involvement of the pleura by the carcinoma or by atelectatic/pneumonic complications may result in chest pain (40%). Systemic symptoms such as weight loss (40%) are common. A nodule on a CXR in the asymptomatic patient occurs in about 10% of patients.
Examination and Clinical Decisions
The following quote from Sherlock Holmes cannot be repeated often enough for all professions that involve diagnostic aspects.
“Not invisible but unnoticed Watson. You did not know where to look so you missed all that was important.”
Hence, in a patient who is suspected of having lung cancer, special considerations should be given to a unique combination of findings including: fever, wasting, clubbing, acanthosis nigricans, Cushingoid features, Horner?s Syndrome, and skin nodules, for example. Other signs and symptoms can include: dyspnea (shortness of breath), hemoptysis (coughing up blood), chronic coughing, weight loss, or hoarse voice. The chest examination should include a specific search for pleural effusion, pneumonia, wheezing and stridor. Pericardial effusion and tamponade are less common associations. Evaluation of neurological function is essential to exclude subtle dysfunction from metastases.
For any patient who has been a long time heavy smoker, concern for lung cancer must always be on the clinicians mind. As the active search for lung cancer is initiated, sputum cytology and a CXR are mandatory.
Once the space occupying change is suspected, the next step is to establish a histological diagnosis. This can be done, depending on the accessibility of the lesion. Techniques utilized include bronchoscopy for bronchial or transbronchial biopsy, mediastinoscopy for node biopsy during CT guided percutaneous biopsy of a nodule or metastatic lesion, and thoracentesis. The distinction between small cell and non-small carcinoma is essential.
Once the histological diagnosis is established – TNM classification of the tumor is required to develop a treatment plan.

This middle-aged male has lung carcinoma, COPD, and extreme emaciation.
Courtesy: Ashley Davidoff, M.D.
Diagnostic Work-up
In the workup of a patient with known lung carcinoma the following are recommended;
Complete blood count with platelet determination
Measurement of serum electrolytes, glucose, calcium, and phosphorus, renal and liver function tests
Electrocardiogram
Skin test for tuberculosis
Pulmonary function studies and arterial blood gas measurements if signs or symptoms of respiratory insufficiency are present
Sputum cytology is a test in which a sample of sputum is obtained so it can be examined under a microscope for cancer cells.
Bronchoscopy
Mediastinoscopy
Lung biopsy
Transbronchial needle aspiration (TBNA)
Lung function tests
Imaging
Imaging is essential to the diagnosis and staging of lung cancer and therefore, intimately related to the treatment. The advances made in imaging over the last two decades have radically changed the diagnostic approach to cancer. Although chest X-ray is an important study, in the face of the new technology it lags significantly in sensitivity and specificity. High resolution CT has enabled the detection of very small nodules, but in view of the lack of specificity, many unnecessary scans were being performed for small indeterminate nodules at great cost and with unnecessary radiation in the hope that a two year follow up would be able to distinguish between benign and malignant disease. The protocol for these indeterminate nodules has been revised now that adequate data has accumulated ((McMahon).
As a result of the identification of small ground glass opacity lesions by CT, understanding of the connection and implications of premalignant atypical adenomatous hyperplasia, BAC, (carcinoma in situ) and adenocarcinoma is evolving (Travis).
Positron Emission Tomography (PET) scanning and specifically PET-CT has been a major advance in the characterization of lesions > 7mm and now is an integral and essential part of staging.
Imaging: Chest X-ray
The chest X-ray (CXR) often uncovers the asymptomatic nodule, but generally, has a relatively low sensitivity for identifying lung nodules and mediastinal disease. Attention to the lateral examination is important; posterior and medial lesions as well as retrocardiac lesions are often hidden in the PA exam and will be identified by the experienced radiologist on the lateral examination. If a chest x-ray is normal in a patient with high clinical suspicion, Computed Tomography (CT) scan is recommended.
Atelectasis that does not resolve with time should also raise suspicion for a proximal obstructing lesion and requires further evaluation with bronchoscopy and CT scan.
The CXR is limited and a CT needs to be performed to further characterize the lesion and define the extent of the disease.

In this instance, a well-defined nodule is noted in the right upper lobe without other obvious adenopathy. There is a fracture of the left humerus (white ring in c) which may be due to minor trauma in this osteoporotic elderly female though a metastatic lesion to the bone is included as a possibility. The lungs are hyper inflated characterized by flattened hemidiaphragms and increase in the retrosternal space suggesting emphysema. The yellow rings show wrinkling of the skin reflecting loss of subcutaneous fat and loss of elasticity of the skin. This is a common association in patients with chronic obstructive lung disease and cancer.
Courtesy: Ashley Davidoff, M.D.
Imaging: Computerized Tomography
Lung lesions with an irregular, spiculated border and a diameter > 3cm should be regarded as highly suspicious for malignancy. It is, however, important to maintain a high level of suspicion for all lung nodules that do not contain central calcification, particularly in smokers and patients with COPD.
Small (<5mm), smooth nodules in low risk patients are being viewed with less suspicion and 99% of such nodules are benign (McMahon).
If there has been no change in the size of an indeterminate nodule on serial chest computed tomography (CT) scans over a period of two or more years, then the lesion can be considered benign. The exception is the ground glass opacity (GGO) which if it represents BAC, may be sufficiently slow growing to show no change in two years.
Bronchioloalveolar carcinoma presents as ground glass opacities (GGO) either single and focal or multiple, or as an infiltrate.
The distinction between peripheral and central masses is better evaluated by axial imaging and CT is also more sensitive to subtle calcification and cavitation of squamous malignancy.
Enhancement of a solitary pulmonary nodule by more than 20 HU following intravenous contrast is a good predictor of malignancy (Swensen).
A lung lesion that is < 3cm in size, with well-defined margins and high attenuation values >164 suggesting that it contains calcium, is considered benign.
Low dose CT screening is more sensitive than CXR to small nodules, particularly for peripheral lesions. However, false positive rates are high (25% have abnormal tests, only 10% of which are cancers).

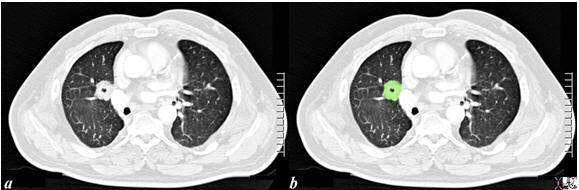
A non specific nodule without defining characteristics is shown in this CT scan. In this instance a positron emission tomography (PET) scan followed to determine activity in the lesion.

The PET scan of the patient above not only showed activity in the right upper lobe nodule but also in the mediastinum. Although an infection such as a granulomatous disease is considered, histological diagnosis is necessary if the patient fails to show other evidence of granulomatous disease (e.g. skin test serology).
The nodule in the lingula has central calcification and is classical of granulomatous disease. No further work up for malignancy is required.
Image courtesy: Ashley Davidoff, M.D.
CT is reported to have a sensitivity of 44% to 79% for detecting mediastinal adenopathy; however, its specificity is low (65%), with “enlarged” nodes sometimes proving to be tumor free (McCloud). In the past, lymph nodes that measured <10mm in the short axis were considered normal. PET scan has disproved this practice since nodes smaller than 10mm in the short axis have been shown to contain metastases. However, when the nodes are larger than 10mm in the short axis, then the suspicion for metastatic involvement is raised. In the end, PET scanning and then intraoperative biopsy are used to determine staging of the cancer.
The presence of lymphadenopathy is an extremely important aspect of the disease since TNM staging is the second most important diagnostic consideration after characterizing the disease into either the small cell type and/or the non- small type.
Positron Emission Tomography (PET)
Positron Emission Tomography (PET) scanning and, specifically, PET-CT has provided a major advance in the characterization of lung lesions. It is true functional imaging and reflects the metabolic activity of a nodule or mass in question. Tumor cells are typically metabolically active and hence, will take up more glucose than most normal cells.
The PET tracer (usually FDG) consists of two parts; glucose and a radioactive component. The most widely used compound is a glucose analogue 18F-fluoro-2deoxy-D glucose (FDG), which becomes trapped inside tumor cells which use the glucose in metabolism. In general, the patient is scanned about 45-60 minutes after the compound is administered intravenously. The emitted positrons from the radioactive component can be detected by a scanner and is reflected as a 3D image.
Because PET scanning measures functional changes, it will reflect changes in biologic activity before structural changes are apparent. Thus, changes in management can be made earlier as result of functional evaluation.
The combined use of PET and CT allows for combined structural and functional imaging. In essence, FDG activity is overlaid on the CT scan which will allow accurate structural localization.
FDG is normally distributed in the brain, heart, stomach, kidneys, and bladder. In the sphere of lung cancer, PET is used to differentiate benign from malignant pulmonary nodules, stage the cancer by defining involvement of the mediastinum and distant sites, detect recurrent or residual disease after therapy, and finally to define the prognosis. FDG is also taken up in tissues that are inflamed and hence, infection and inflammatory disorders will show higher activity and are the source of false positives.
The size of the nodule is important since, in general, only nodules larger than about 7mm can be detected. Standard uptake values (SUV) are a measure of the concentration of a radiotracer. The higher the SUV, the greater the accumulation and therefore, the higher the metabolic activity. An SUV of 2.5 or greater is more likely to be cancer and an SUV of less than 2.5 is more likely to be benign disease. Bronchioloalveolar carcinoma, however, has lower metabolic activity and may even have no uptake of FDG. Well-differentiated adenocarcinoma and carcinoid tumors may also have a low SUV.

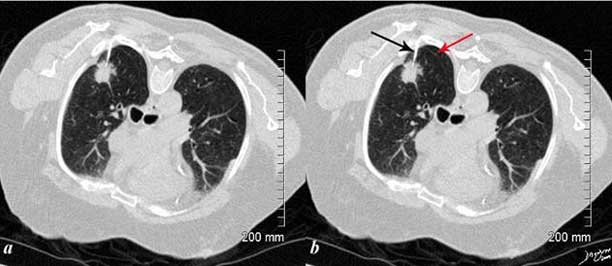
A small nodule (red arrow a, b,c) was identified on the CT in this 60-year-old female who is a smoker. The SUV at 1.3 was low (usually >2.5 in malignancy). At pathology, it was found to be a necrotizing pneumonia. Most necrotizing granulomas are related to infection.
Ashley Davidoff MD
The plain film (top left) and CT (top right, bottom right) features of this mass in a 66-year-female who is a smoker are concerning, with size being greater than 3cm, and the shape having spiculated borders and satellite nodules seen in the top right image. The PET scan (bottom left) was positive and biopsy confirmed the diagnosis. The (bottom right) was performed during a CT biopsy and the patient is lying prone.
Courtesy: Ashley Davidoff, M.D.
Imaging: Other Imaging Modalities
Magnetic resonance imaging (MRI) appears to be more accurate than CT for demonstrating contiguous invasion of the mediastinum by lung cancers, but this selected advantage is not of sufficient value to use MRI routinely for lung cancer patients.
Ultrasound (US) scans are used mostly as a guide to aspirate pleural fluid.
Imaging: Biopsy
Percutaneous biopsy of the lung offers the ability to characterize lung lesions with very few contraindications. Complications include pneumothorax (10-49%) and hemoptysis (8-20%) which generally resolve without treatment. (Gohari).
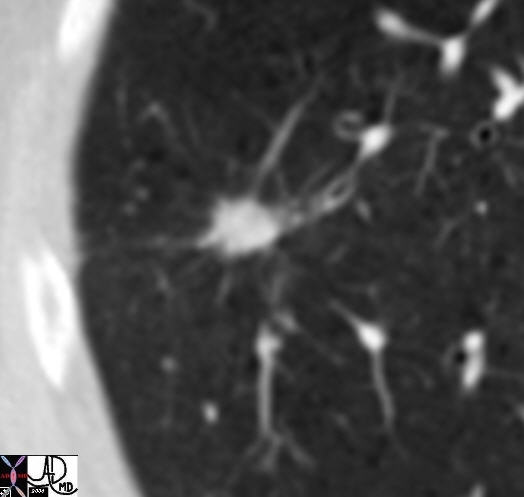
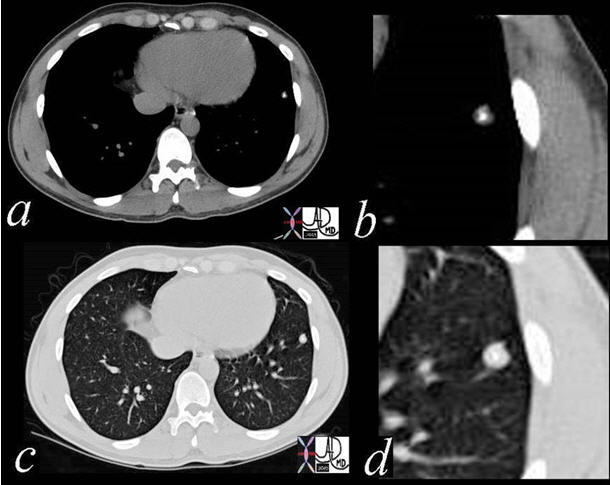
The CT is from an 81-year-old man with remote history of smoking who presents with an asymptomatic lung mass. The lesion was PET positive, without nodal activity suggesting that it was either an infection, inflammatory lesion or a primary lung cancer. A biopsy revealed adenocarcinoma of the lung. In the image, the patient has been placed in the prone projection. The needle (arrow is shown) within the spiculated lesion. The radiologist needed to avoid the major fissure which is seen as a fine curvilinear structure posteriorly (red arrow), negotiate the scapula and two closely spaced ribs. Without CT guidance this procedure would have been almost impossible to biopsy.
Courtesy of: Ashley Davidoff, M.D.
With transbronchial evaluation of central lung cancers, when the lesions are visible, washings have a yield of 79%, brushings 92%, and forceps 93%. For peripheral lesions that are <2cm the yield is 20% and when they are >2cm the yield is 50-80%. It is a safe procedure, sometimes complicated by pneumothorax (10%) and less commonly by hemorrhage (.2%).
Staging
Meticulous staging of lung cancer is necessary because treatment options and prognosis depend on accurate staging.
Tumor (T) status descriptors, lymph node (N) involvement descriptors and distant metastasis (M) descriptor ratings are assigned for staging.
In 1997, the American Joint Committee on Cancer and the Union Internationale Contre le Cancer revised the stage groupings of the TNM subsets in the International System for Staging Lung Cancer (Mountain).
This classification facilitated the evaluation of the extent of the disease based on the size of the primary tumor, extent of adenopathy and extent of the disease in the body.
Treatment
Surgery is required for cure. Surgical candidates include patients with stage I or II disease and in some patients who are stage IIIA. These categories account for 20-25% of patients.
The treatment algorithm is based on the histological diagnosis. A tumor is classified as a small cell carcinoma or as one of the non-small cell varieties (squamous, adenocarcinoma, large cell carcinoma, bronchioloalveolar carcinoma). Staging of the carcinoma based on its anatomical extent, and functional evaluation of the patient are mandatory steps prior to therapeutic decisions. Intraoperative staging is accomplished by frozen section evaluation of mediastinal nodes.
By the time small cell carcinomas present, metastatic disease is usual (70%). Surgery, therefore, is unlikely to be curative, and the disease is treated with chemotherapy, occasionally augmented by radiotherapy. If clinical assessment and staging suggest localized disease (30%), the surgical option should be considered.
At presentation for non small cell carcinoma, approximately one-third of patients are stage I, II, or IIa, meaning they have disease localized enough for a curative attempt with surgery or radiotherapy. A further 30% have IIIA or IIIB with local or regional disease that has equivocal curative capability and the last 30% are stage IV, meaning they have distant metastatic disease and are incurable. Non-small cell cancers do not respond as well to chemotherapy as small cell cancers. Surgery is an absolute necessity in an attempt to cure; the patient with XRT has fewer opportunities to accomplish cure. A lobe of a lung is usually removed but the whole lung can be removed if necessary.
Surgery is indicated for stages I or II and sometimes for III. Contraindications to surgery include:
- systemic metastatic disease or lymphadenopathy beyond the ipsilateral hemithorax
- malignant pleural effusion
- tumor within 2cm of the carina
- involvement of the main pulmonary artery
- superior vena cava syndrome
- vocal cord paralysis, phrenic nerve paralysis
- cardiac tamponade
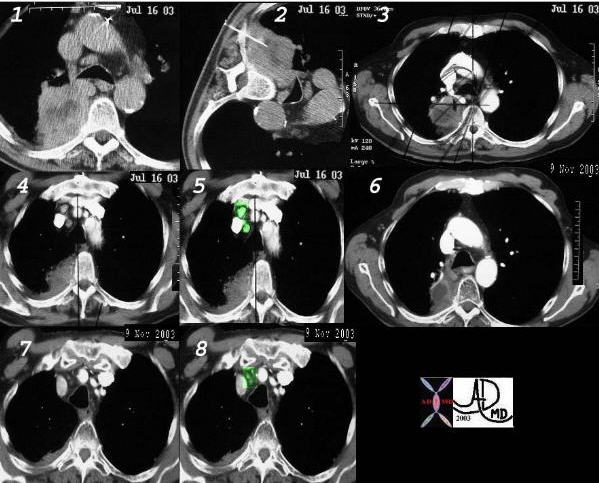
This is a case of poorly differentiated non small cell carcinoma presenting as a large necrotic mass, with a percutaneous biopsy (2) treated with radiation therapy (3), with associated small nodes (4) overlaid in green, (5) with a response as seen by shrinkage of the tumor 4 months later (6) as well shrinkage of the nodes (7, 8).
Courtesy: Ashley Davidoff, M.D.
Radiotherapy and Chemotherapy
Radiotherapy is used as the main treatment for NSCLC and as a secondary treatment for small-cell carcinoma. Used alone in certain situations it sometimes has a chance to cure. For example a Stage I or II NSC carcinoma within 2cm of the carina cannot be treated surgically and is best treated and cured by XRT. Other situations where it is extremely helpful is in patients with bilateral endobronchial tumor and contralateral mediastinal node metastases, where XRT has an opportunity for cure and where surgery is contraindicated.
Chemotherapy is used as an additional treatment for NSCLC and the main treatment for SCLC.
On this CT scan, the heart has shifted into the left chest following pneumonectomy.
Courtesy: Ashley Davidoff, M.D.
Prognosis
The strongest prognostic factor for survival is whether the tumor can be completely resected. The most important prognostic indicator therefore is the extent of disease and lymph node involvement.
In General:
- The overall outlook is poor for most patients with bronchogenic carcinoma.
- The percentage of patients who survive with lung cancer for one year is around 42%.
- The overall 5-year survival rate is on the order of 10-20%.
With Localized Disease
The 5-year overall lung cancer survival rate has nearly doubled in the last 30 years due to advances in combined-modality treatment. In stage I disease, 5-year survival for squamous cell is up to 40% and for patients with adenocarcinoma it is up to 30%. With local disease, 5 year survival for T1 and stage T2 is 75% and 67% respectively.
For Regional Disease
It is 20% for patients with regional disease. The estimated survival for patients with advanced NSCLC, with chemotherapy, is 6-12 months which is only minimally better than with supportive care alone. For the undifferentiated lesions, 5 year survival is closer to 3%.
Conclusion
The story of lung cancer, unfortunately, is closely tied to the story of cigarette smoking. The cultural fashions and habits that were promoted by the industry have created a problem for vast numbers of people worldwide.
The World Health Organization maintains that approximately 3,000,000 people die worldwide each year as a result of smoking. In the 20th century approximately 100 million people died from tobacco associated diseases. It is the most common type of new cancer cases at 1.2 million new cases in the world (Huq). Overall, lung cancer is the most frequent fatal malignancy and accounts for more than 7% of all deaths in both sexes.
Much has been accomplished in the medical sciences with the advent of CT scanning and PET scanning, together with advances in radiation therapy and chemotherapy. However, as with many diseases, prevention is better than cure, and in this instance a truer word could not be said.