

Introduction
The esophagus is a tube-like structure that provides a conduit from the mouth and oropharynx to the stomach and it is a key component of the digestive system.
Structurally it is characterized by its muscular and tube-like properties. Functionally it acts as a conduit which enables the rapid transport of recently ingested, relatively large food and fluid products from the mouth to the stomach. While not essential to life, its inherent properties and function provide a normal mechanism of digestion. Proper coordinated contraction and relaxation, hence propagation, is key to its proper functioning.
Many different diseases can affect the esophagus. These range from anatomic alterations within the lumen, to systemic conditions that alter the normal function. These pathologic conditions can cause significant complications ranging from difficulty swallowing to cancer.
Diagnosis of esophageal disease requires careful attention to the detail of clinical symptoms such as dysphagia, while modalities that include endoscopy, endoscopic ultrasound and barium swallow are essential to diagnosis.
Medical therapy, minimally invasive techniques and surgical options are available depending on the disease process in question and treatment of the conditions that affect the esophagus.

The double contrast barium swallow shows the esophagus as a distended featureless tubular structure with smooth mucosa. This appearance is an artificial appearance of the esophagus since it is as a result of reflux of air from the stomach and inhibition of the primary stripping wave induced by the method of the study.
Courtesy of: Ashley Davidoff, M.D.
Principles
The unique structural characteristics of the esophagus include its:
- histopathology characterized by an inner lining of sqaumous mucosa and lack of a distinct, serosal or adventitial cover
- it is the most muscular part of the gastrointestinal tract and contains both striated type and smooth musculature
- ability to change shape to accommodate a swallowed bolus
The unique functional aspects include its:
- ability to coordinate contraction and relaxation functions
- ability to prevent reflux into the airways and from the stomach back up into the esophagus
It may be helpful to think of the esophagus as a tube of toothpaste. To expel the toothpaste, one typically squeezes the tube at the end furthest from where the tooth paste is dispensed. If you squeeze from the middle, toothpaste can be expelled in both directions (normally and out the back end). In the esophagus, if there is a motility disorder and the wave of contraction starts in the middle this would result in ineffective emptying of the esophagus.

The drawing on the left demonstrates the primary stripping wave noted as a constriction above the food bolus. Both the upper and lower sphincters are closed. The primary stripping wave progresses from proximal to distal. The image on the right is from a double contrast barium swallow and it demonstrates the top of the primary stripping wave.
Courtesy of: Ashley Davidoff, M.D.
There are many common disease processes that can be encountered in the esophagus. The most common is gastroesophageal reflux disease (GERD). The reflux of low pH gastric juices through the normally tight lower esophageal sphincter (LES) results in a multitude of complaints. These can range from the classic retrosternal burning to chest pain, water brash, halitosis, to chest pain that simulates angina. Other common conditions encountered include rings/webs, motility disorders, esophagitis, Barrett?s esophagus, and malignancy. These conditions will be discussed in the diseases section below.
Several modalities exist to evaluate a patient?s complaints as they relate to the esophagus. The best study greatly depends on what the diagnostician is looking for. To evaluate the mucosa, examine for luminal lesions, biopsy or treat a ring, an upper endoscopy would be the study of choice.
Radiographic studies are invaluable in the workup of a patient with dysphagia. The barium swallow requires the patient to swallow a combination of barium and effervescent tablets in order to evaluate in real-time, the process of swallowing. This study allows for excellent review of the anatomy and various pathologic processes such as narrowed regions, dilatations, as well as providing an ability to evaluate motility.
A Computed Tomography (CT) scan of the chest and abdomen allows for a global view of the esophagus within the mediastinum and chest cavity.
Endoscopic ultrasound (EUS) is an excellent modality that can be used in conjunction with traditional endoscopy to evaluate the structural integrity of the esophagus as well regional lymph nodes. As we discuss specific diseases, a more lengthy description of the diagnostic approach will be included.
If any part of the mucosal, muscular, or neurologic function is not functioning properly, swallowing can be greatly affected. This could lead to dysphagia, odynophagia (pain with swallowing), or a multitude of processes that will be discussed in this module.
Structural Principles
The tube-like structure of the esophagus is key to its proper function as a conduit from the mouth to the rest of the digestive system. In essence, the esophagus is simply a long tube. However, it is more complex than that with several distinct regions, each of which has different properties and functions. The segments differ from being tight muscular sphincters at either end of the tube that allow one way flow, preventing reflux, to segments that have varying contraction and relaxation peristaltic properties.

The esophagus lies between two sphincters. The upper esophageal sphincter (UES) enables food to enter the esophagus while the lower esophageal sphincter (LES) prevents reflux of gastric contents.
Courtesy of: Ashley Davidoff, M.D.
As the most muscular organ in the gastrointestinal tract its function is to rapidly transfer the bolus of food or fluid from the upper esophageal sphincter (UES) to the lower esophageal sphincter (LES) and then to the stomach. This requires exquisite coordination of muscle contraction and relaxation. As the bolus reaches the back of the oropharynx, reflex relaxation of the UES has to occur, briefly to allow the food to enter, and then it has to close rapidly to prevent reflux. At the UES, the coordination is quite complex because it also requires the participation of the epiglottis to close the airways as the bolus passes through, after which the airways must be rapidly opened again to allow the person to breathe.
The esophagus itself isn?t needed for life, but the organ provides unity to the intestinal system. It provides continuity such that food can enter one end, be processed, and be excreted, albeit in a different form, out the other. Surgery can remove the esophagus and a person can live and eat, but the unity of the gatrointestinal (GI) system is interrupted and dietary changes are needed.
As long as the lumen is greater than 13mms in diameter, food will not get stuck. As the lumen narrows in disease to 13mms. or less, dysphagia will occur.

The esophagus is basically a tube as seen in the first image on left, which has the ability to initiate strong contractions (middle image) as well as actively relax. (right image).
Courtesy of: Ashley Davidoff, M.D.
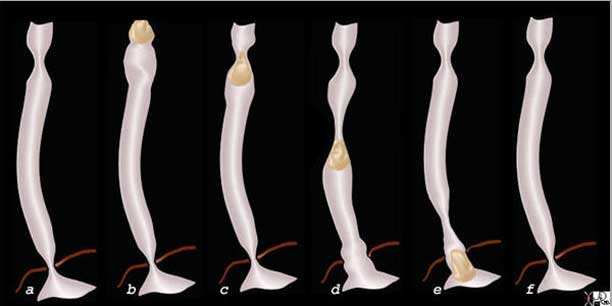
The six drawings above reflect the contractile and relaxation efforts of the esophagus in order to transport a food and or fluid bolus from the back of the mouth to the stomach. The resting phase in a, shows the UES and LES in basal state with both sphincters contracted. As the food enters the oropharynx from the mouth, the UES relaxes, and the receiving segment of the esophagus just distal to the UES reflexly relaxes as well. (b) In c, the UES contracts behind the bolus and a primary stripping wave are formed that rapidly advances the bolus. Simultaneously the LES relaxes (d). The bolus gets pushed through the LES which subsequently contracts behind the bolus and we are back to the basal state (f).
Images courtesy of: Ashley Davidoff, M.D.
Structural CharacteristicsThe esophagus lies in the posterior mediastinum. It courses behind the trachea and left mainstem bronchus and in front of the aorta. The actual length varies but ranges between 18-26cm. It is important to note that the length changes slightly with each swallow.
The wall of the esophagus is comprised of four distinct structural layers: It is important to note the lack of a serosal lining. In the rest of the gastrointestinal tract an outer lining exists throughout and is called either a serosa or an adventitia. This is an important fact since disease such as malignancy in the esophagus has little resistance to prevent it from spreading through the wall.
The mucosa is comprised of a nonkeritinized stratified squamous epithelium. This acts as a permeability barrier and contains the regenerative capacity of the esophagus.
Just below the mucosa is the submucosa. Within this layer one finds connective tissue, blood vessels, lymphatic structures, as well as neurons. Acini, or clumps of cuboidal cells are also present in this layer and these provide various substances such as mucus, bicarbonate, and growth factors that are key in maintaining the proper function and structure of the esophagus.
The muscularis propria is the next layer is comprised of two layers of muscle: the innermost circular layer and the outer longitudinal layer. The esophagus is the most muscular portion of the gastrointestinal tract.
The esophagus begins at the upper esophageal sphincter (UES) where the cricopharyngeus and inferior pharyngeal constrictor muscles meet. This is at about the level C6, 15 cm from the central incisors.
The UES is critical in preventing patients from swallowing air as it remains in the contracted or high pressure position when the patient isn?t swallowing. Upon initiation of a swallow, the UES relaxes (see above diagram) and allows the bolus to enter the esophagus. From there, the musculature propels the bolus towards the stomach.
The upper 5-33% of the esophageal muscle is of the skeletal type while the distal 33% is smooth muscle. The region in between is a mixture of both skeletal and smooth muscle. This is a very important fact since diseases such as myasthenia gravis that affect skeletal muscle will affect esophageal function, and those that affect smooth muscle such as scleroderma and polymyositis will affect function of the esophagus as well. This structural makeup of these two types of muscle in one organ is unique.
At the distal end of the esophagus is another important sphincter known as the lower esophageal sphincter (LES). The main function of this sphincter is to prevent the reflux of gastric contents back into the esophagus. The distal esophagus terminates 3-5 cm below the diaphragm.
The transition from esophageal to gastric mucosa, easily recognizable by a color and texture change, takes place along an irregular dentate or zigzag line, known as the ?ZZ? line or the ?Z? line.

The gastroesophageal junction (also know as the Z line, ZZ line or squamocolumnar junction) is clearly outlined as the squamous epithelium (white) transitions to the gastric epithelium (reddish pink mucosa). It is also exquisitely demonstrated in the double contrast barium swallow as a sharp, contrast and air-filled esophagus and the stomach where no contrast is present.
Courtesy of: Joshua Namias, M.D. and Ashley Davidoff, M.D.
Parts
The cervical esophagus starts around C5 (5th cervical vertebra), or approximately 15cm from the incisors. The trachea runs just anterior to the cervical esophagus. Several nerve fibers, such as the recurrent laryngeal nerve course between these structures. The thyroid can overlap the upper portion of the esophagus.
The barium swallow shows contrast moving from the back of the mouth into the pharynx into an open upper esophageal sphincter (UES), as it enters the cervical esophagus (pink) at C5. The trachea is overlaid in blue and lies anterior to the esophagus.
Courtesy of: Ashley Davidoff, M.D.
Structural Characteristics : Upper Esophageal Sphincter
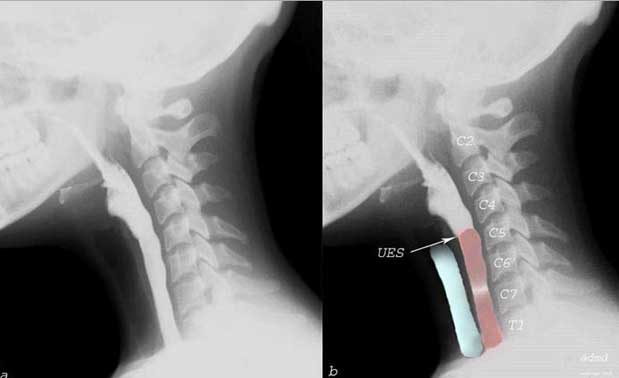
Upper Esophageal Sphincter (UES, a.k.a cricopharyngeal sphincter) starts at about the C5-C6. It is usually contracted preventing reflux of gastric contents into the airways. When swallowing is initiated, the UES relaxes and once the bolus has passed it returns to its contracted state.
Shown is a barium swallow demonstrating normal swallowing.
Left image: closed upper esophageal sphincter (UES)
Right image: open pharyngeal phase
Courtesy of: Ashley Davidoff, M.D.
Structural Characteristics : Thoracic Esophagus
The thoracic portion can itself be subdivided into the upper, middle, and lower regions. The upper region runs from the aortic arch superiorly while the middle region courses from the aortic arch to the inferior pulmonary vein. Finally, the lower third, the most distal portion of the esophagus, runs from the inferior pulmonary vein to the LES or gastro-esophageal (GE) junction.
Moderate thickening of both the circular and longitudinal muscles takes place in the lower end of the esophagus, commencing about 1 or 2 cm above the diaphragmatic hiatus and extending to the cardia. This region has been termed the esophagogastric vestibule and is also known as the epiphrenic ampulla.
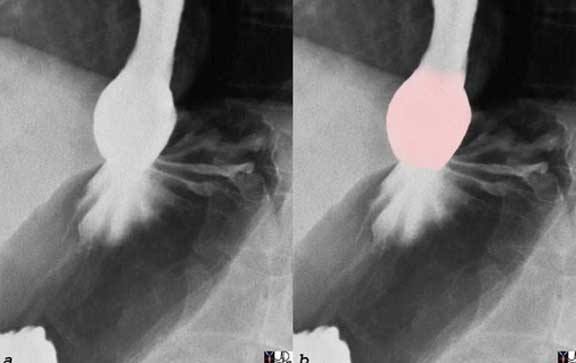
The distal esophagus becomes slightly rotund just before the GE junction due to moderate thickening of both the circular and longitudinal muscles. A small pouch-like structure called the esophagogastric vestibule or epiphrenic ampulla is formed (pink).
Courtesy of: Ashley Davidoff, M.D.
The GE junction is an important landmark since it marks the transition between the pearly white, squamous epithelium of the esophagus and the pink columnar epithelium of the stomach. The distinction between the two is easily recognized by endoscopy and also by barium examination marked by the zig zag ?z line. The structure and function of the two different layers is also distinct. Whereas the esophagus can withstand the temperature of boiling water it cannot tolerate the acid secretions of the stomach. Repeated exposure of the esophageal lining to the acid, not only can cause esophagitis, but can in some cases lead to carcinoma of the esophagus.
The esophagus does not have a capsule and it is attached to the other mediastinal structures by loose connective tissue. The musculature of the esophagus consists of an outer longitudinal muscle layer and an inner muscular layer, generally described for convenience as the circular muscular layer. The anterior wall of the esophagus is firmly applied to the posterior tendinous wall of the trachea in its upper portion, where the two organs are attached to each other by fibro-elastic membranous tissue containing some muscle fibers.
Ligaments
In its passage through the esophageal hiatus of the diaphragm, the esophagus is surrounded by the phreno-esophageal ligament, also known as the phrenico-esophageal ligament and diaphragmatico-esophageal ligament. The phreno-esophageal ligament arises from the circumference of the hiatus as an extension of the inferior fascia of the diaphragm, which is continuous with the transversalis fascia. At the margin of the hiatus, it divides into an ascending leaf and a descending leaf. The ascending leaf passes upward through the hiatus and surrounds the esophagus in a tent-like fashion. It extends for several centimeters above the hiatus, where it is inserted circumferentially into the loose outer fibrous layer of the esophagus. The descending leaf passes downward and is inserted around the cardia deep to the peritoneum. It is this ligament that gets stretched in the aging process resulting in loss of GE junction anchorage and the evolution of hiatal hernia.
At the GE junction, the distal esophagus is attached to the liver by the gastrohepatic ligament at the fissure for the ligamentum venosum.
Structural Characteristics : Histology
The esophageal wall is comprised of a mucosal, submucosal, muscularis and an incomplete adventitia or fibrosa. The mucosal layer is comprised of epithelium, lamina propria and the muscularis mucosae. There is no discrete adventitia. This connective tissue layer blends in with the trachea and other surrounding structures.
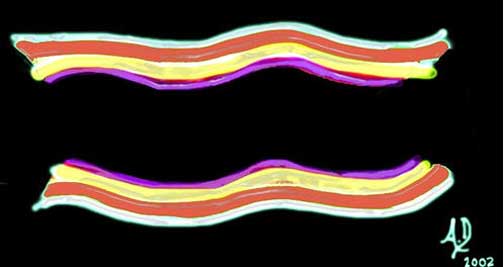
The wall of the esophagus is made up from three main layers including the mucosa (purple) submucosa, (yellow) and muscular layer. (red) The adventitial layer (white) is poorly formed in the esophagus and consists of loose connective tissue that blends with mediastinal fibrous tissue.
Courtesy Ashley Davidoff, M.D.
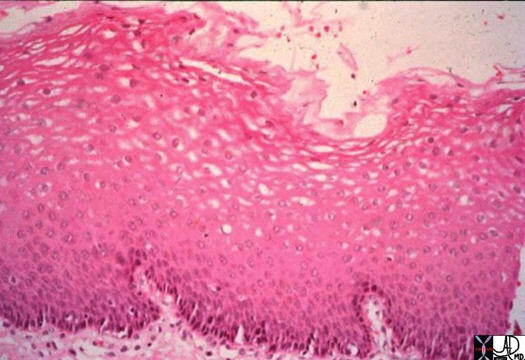
The mucosa of the esophagus is relatively thick and is made from a stratified, squamous epithelium. Stratified means that there are multiple layers of cells, and squamous refers to the flat shape of the cells. This is distinctly different to the remaining mucosa of the gastrointestinal tract which in general is made of a single layer of cells that are rectangular in shape. The image above demonstrates the stratified squamous layer and a small portion of the submucosa.
Image courtesy of: Ashley Davidoff, M.D. and Barbara Banner, M.D.
The esophagus is lined by stratified, squamous epithelium (as shown above), which is a continuation from the pharyngeal lining. The surface cells of this epithelium are flattened and contain a few keratohyalin granules but are not cornified as would be seen in the squamous lining of the skin. This type of lining is adapted to enable the esophagus to be protected from rough, hot or cold food.
An abrupt transition takes place between the stratified squamous epithelium of the esophagus and the columnar epithelium of the stomach along the ?Z-line? as described above.
The submucosa is quite dense and contains both elastic and collagen fibers. A moderate number of lymphocytes is scattered through both the lamina propria and the submucosa.
The muscular coat consists of an inner layer, called the circular layer, and an outer longitudinal layer. A thin layer of connective tissue, in which is embedded the myenteric plexus of Auerbach, is spread between the two muscular layers. This part of the nervous system provides the neurologic motor innervation to the esophagus (both circular and longitudinal muscles) as well innervation to the secretomotor innervation of the mucosal layer.
The submucosa contains Meissner?s plexus and also part of the vascular system supplying the esophagus.
The adventitia consists of loose connective tissue, connecting the esophagus to surrounding structures. This lack of a complete outer lining seemingly offers little advantage to the esophagus and in fact is a distinct disadvantage. In some disease processes, such as cancer, the absence of a complete outer serosa or adventitia allows the disease to spread easily to surrounding vital structures like the airways and aorta.
Two types of glands can be recognized in the esophagus. One of them, the esophageal glands proper, or deep glands, is irregularly distributed throughout the entire length of the tube. They are small, compound racemose glands of the mucous type. Their ducts penetrate the muscularis mucosae, and their branched tubules lie in the submucosa. The glands of the other type are known as the cardiac glands or superficial glands because they closely resemble, or are identical, to the cardiac glands of the stomach. They are found at both ends of the esophagus, i.e for a few centimeters below the level of the cricopharyngeus muscle and also just above the cardia. They differ from the esophageal glands proper in that their ducts do not penetrate from the muscularis mucosae and their branched and coiled tubules are located in the lamina propria, not in the submucosa.
Structural Characteristics : Size
The esophagus varies in size from person to person. There is a fluctuation in size within one person as the muscular forces with swallowing alter the overall length by up to 2cm. On average, the esophagus ranges between 18-26cm.
The overall width is approximately 2cm but it too varies with the width of a swallowed bolus. Various conditions can cause significant changes in the size of the lumen. Achalasia, for example, can result in a diffusely dilated esophagus, whereas benign and malignant strictures usually cause focal narrowing.

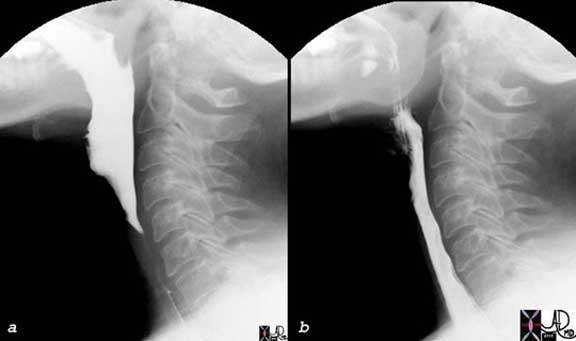
The two images from a single contrast barium swallow show a normal esophagus and GE junction on the left and a dilated esophagus with a hypertonic LES on the right. The appearance of the image on the right is reminiscent of a condition called achalasia.
Courtesy Ashley Davidoff MD
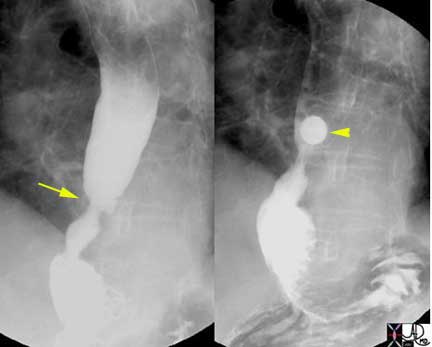
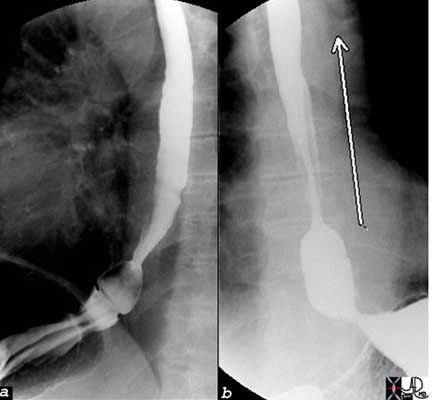
In this barium swallow a stricture in the distal esophagus represents a focal narrowing of the esophagus caused by longstanding reflux esophagitis. The 13mm barium pill shown in the image on the right was not able to pass through this stricture. This finding explains the cause of dysphagia in this patient. Endoscopy is required to ensure the benignity of the stricture.
Images courtesy of: Ashley Davidoff, M.D.
Structural Characteristics : Shape
When viewed from the front, it assumes the form of a gentle reversed ?S?. The upper of the two lateral curvatures is convex toward the left. The lower curvature, in the lower thorax and abdomen, is convex toward the right. From its commencement at the lower margin of the cricoids cartilage, the esophagus inclines slightly to the left until its left border projects approximately ¼? to the left of the tracheal margin. It then swings somewhat to the right, reaching the midline at about the level of the fourth thoracic vertebra behind the aortic arch. It continues its inclination to the right until about the level of the seventh thoracic vertebra, where it again turns left somewhat more sharply than in its precious curves, and in this direction it passes through the esophageal hiatus.
The course of the esophagus is marked by several indentations and constrictions:
- The first narrowing of the esophagus is found at its commencement, caused by the cricopharyngeus muscle and the cricoid cartilage.
- The esophagus is indented on its left side by the arch of the aorta.
- The left main bronchus causes, generally, an impression on the left anterior aspect of the esophagus.
- At its lower end the esophagus is narrowed by the inferior esophageal sphincter and the esophagogastric vestibule.
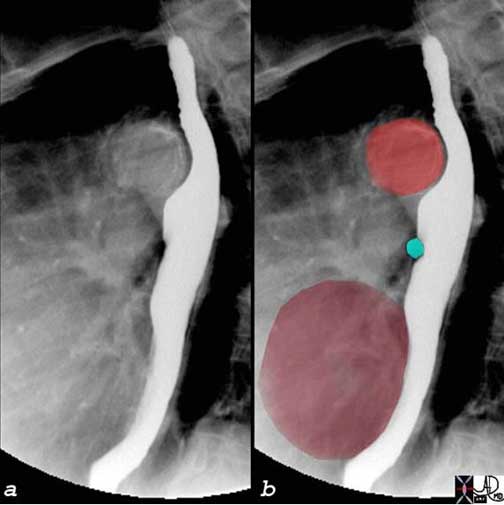
The normal indentations on the esophagus include the aortic arch and knob seen in bright red in b. The left bronchus is usually seen as a oblique line crossing the back of the esophagus, but in this case is seen as a focal indentation on the anterior wall. The left atrium is seen pulsating against the distal esophagus (maroon) usually when the left atrium is enlarged.
Courtesy of: Ashley Davidoff, M.D.
Although the esophagus is usually described as tube-like, in the resting state it is flattened anteroposteriorly so that the transverse axis is larger than its anteroposterior axis. In the resting state the esophageal walls approximate each other.
Given this property, air insufflation is a key component of endoscopic evaluation so that proper distension and visualization can be obtained. Below is a video capsule image of a normal esophagus which shows the narrow and non-distended lumen.

As the esophagus ages the primary stripping wave may become weaker and the secondary waves stronger. This leads in some patients to thickening of muscle and results in the corkscrew appearance of the esophagus. Diffuse esophageal spasm may have the same appearance.
Courtesy of: Ashley Davidoff, M.D.
Structural Characteristics : Position
The esophagus extends downward through the lower portion of the neck and the superior and posterior mediastinum of the thorax. It then passes through the esophageal hiatus of the diaphragm to join the cardia of the stomach at about the level of the tenth thoracic vertebra. It is found in both the thoracic cavity and to a much lesser extent in the abdominal cavity. In the chest it is part of the mediastinum and forms a gentle reversed “S” shape around the midline.
Cranially it is slightly to the right and caudally slightly to the left. It lies relatively posterior in close contact with the vertebral bodies.
The cervical portion lies within the lower portion of the neck and projects approximately 1/4″ to the left of the tracheal margin.
The upper thoracic portion lies in the superior and posterior mediastinum. It is a midline structure at the level of T4 behind the aortic arch. It has an inclination to the right until about the level of T7. At about the level of the 10th thoracic vertebra, it again turns left more sharply than in its previous curves and passes through the esophageal hiatus.
The abdominal portion resides in the upper abdomen for a short distance before it connects with the stomach at the GE junction.

The CT scan of the upper chest shows the esophagus (yellow) at the thoracic inlet (a) leftward of the trachea (black) and medial to the left subclavian artery (a and b). Lower down the trachea remains medial while the aortic arch becomes an anterior and lateral relation(c). Below the carina, (d) the left main stem bronchus is an anterior and leftward relation while the descending aorta lies lateral.
Courtesy of: Ashley Davidoff, M.D.
Structural Characteristics : Character
The esophagus itself is a distensible and muscular organ. The mucosa of the esophagus is smooth and rather pale in color. In the contracted state the mucosa has irregular, longitudinal folds. The gastroesophageal junction is characterized by color change and at the ?Z line.? It changes from the whitish, squamous epithelium to the pink epithelium of the gastric mucosa.
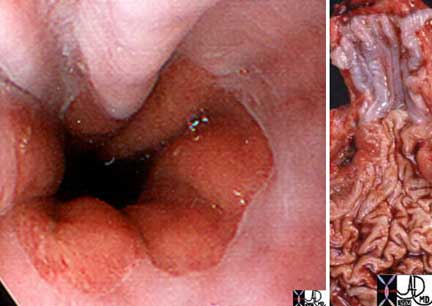
The normal esophagus changes from a whitish hue to a salmon pink at the Z-line. The white color is due to the squamous epithelium of the esophagus and the pink hue is due to the columnar epithelium of the stomach. The image on the left is an endoscopic view and on the right in an anatomical specimen.
Courtesy Josh Namias MD Ashley Davidoff MD

The two images are from a barium swallow and show a distended air-filled esophagus on the left and a collapsed decompressed esophagus on the right.
Ashley Davidoff, M.D.
Structural Characteristics : Blood Supply
The main supply of the cervical portion is derived from the inferior thyroid artery. The anterior cervical esophageal arteries give twig-like branches to both esophagus and trachea. Accessory arteries to the cervical esophagus derive frequently from the subclavian, common carotid, vertebral, ascending pharyngeal, superficial cervical and costocervical trunk. The thoracic segment of the esophagus is supplied by branches from (1) bronchial arteries, (2) aorta and (3) right intercostals. The abdominal esophagus receives branches from the left gastric (cardio-esophageal branches), short gastrics, and from the left inferior phrenic artery.
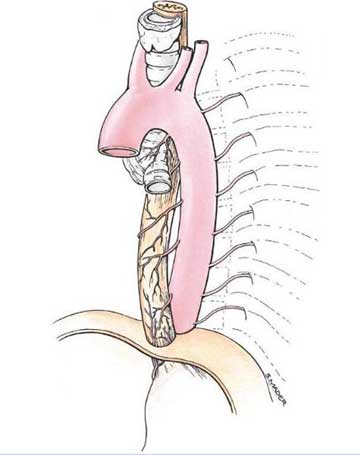
The thoracic segment of the esophagus is supplied by branches from bronchial arteries, aorta and right intercostals.
Courtesy of: Lippincott Williams & Wilkins

Arterial supply from celiac axis and left gastric artery. Courtesy of: Lippincott Williams & Wilkins.
Venous Drainage
In the neck, the final common pathway of cervical esophageal venous drainage is via the brachiocephalic vein. Small venous tributaries from the esophagus drain into the inferior thyroid vein which then empties into the right and/or left brachiocephalic vein. The right and left brachiocephalic veins ultimately join and form the superior vena cava (SVC).
In the chest, the final common pathway of thoracic esophageal venous drainage is via the azygos or brachiocephalic on the right or the hemiazygos, accessory hemiazygos, or brachiocephalic vein on the left. Again, venous blood ultimately ends up in the SVC.
In the abdomen, the final common pathway of lower esophageal venous drainage is via the portal vein or splenic vein. Tributaries from the short abdominal esophagus drain mostly into the left gastric (coronary) vein but also into short gastric veins (and thereby also the splenic and left gastro-epiploic veins).
Venous drainage begins in a submucosal venous plexus piercing the muscle layers. Another venous plexus is formed on the external surface of the esophagus.
Structural Characteristics : Nerve Supply
Below the tracheal bifurcation the esophageal plexus of nerves and the anterior and posterior vagal trunks are closely applied to the esophagus.
The esophagus is innervated by both the parasympathetic and sympathetic nervous system. As described in previous sections, the esophageal motility pattern is quite complex with a voluntary and involuntary component. As such, there is a quite sophisticated efferent and afferent system that provides ongoing regulation and impulse control to the muscular component of the esophagus.
Within the cervical portion of the esophagus the recurrent laryngeal nerve and vagus nerve provide the innervating fibers. The course of the recurrent laryngeal that comes off the vagus is different on the right and left. The left wide has to wrap around the aortic arch while the right side wraps around the right subclavian artery.
Within the superior mediastinum the left recurrent laryngeal nerve, in addition to the right and left vagus nerve proper, provide the nerve fibers. Sympathetic trunks join with the small vagal fibers to form the anterior and posterior pulmonary plexi. As the vagus continues its course through the mediastinum, it continues to branch and provide more distal innervating fibers. These smaller plexi and branches reconstitute into 1 or 2 main vagal trunks.
Sympathetic fibers originate in the intermediolateral corneal cells in the spinal cord. They traverse out of the spinal column and can travel up, down, or in the region where they exit. These nerves provide the efferent innervation. The afferent signals travel back, much along the same route, but enter the spinal cord through the posterior spinal nerve roots. This afferent/efferent communication is the key to proper muscle contractions.
The upper esophageal portion is innervated by the pharyngeal plexus with the more distal portion from branches of the superior cervical ganglia.
The stellate ganglia provide smaller nerve fibers, known as the ansae subclavia, that supply the thoracic esophagus. While in the lower thoracic portion, the greater thoracic splanchnic nerves are important.
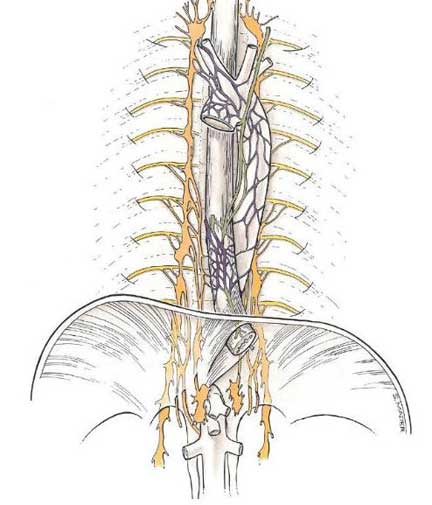
The nerve supply to the esophagus is complex from sympathetic and parasympathetic ganglia.
Courtesy of: Lippincott Williams & Wilkins
Within the abdomen, the celiac plexus is formed, while the greater splanchnic nerve fibers and the right inferior phrenic nerve innervate the abdominal portion of the esophagus.
Lymphatic Drainage
There is a rich network of lymphatic vessels that drain the esophagus. The lymphatics are predominantly found within the lamina propria layer of the mucosa but can be found traversing the other layers as well.
The cervical esophagus drains chiefly to the lower internal jugular nodes which then drain to the upper tracheal nodes.
The thoracic esophagus drains posteriorly to the posterior parietal nodes and diaphragmatic nodes. Anteriorly, the upper part drains to the tracheal and tracheobronchial nodes, and lower down to the retrocardiac and infracardiac nodes

This patient has esophageal carcinoma and a large metastatic lymph node is seen attached to the esophagus.
Courtesy of: Ashley Davidoff, M.D.
Embryology
Early in development, the esophagus, oropharynx, larynx, trachea, bronchi, and lungs derive from a common tube comprised of endoderm. At four gestational weeks the respiratory components differentiate from a diverticulum off this common system. A second ?bud? of this common structure forms into the foregut. This primitive foregut grows with its columnar epithelium, destined to form the digestive tract. Over several weeks, this growth continues with many changes along the way. The columnar epithelium, which remains in the more distal GI tract, starts to change to squamous mucosa at week sixteen and continues until birth.
Physiology
Simply put, the esophagus? main function is the transport of the products of mastication (food) from the mouth and posterior oropharynx to the stomach.
There are several phases of the swallowing mechanism. It originates with the cerebral aspect of thinking about food, followed by mastication and bolus propulsion into the posterior oro-pharynx. What follows is the esophageal component of swallowing:
At the upper esophageal sphincter (UES), the visceral, striated muscle keeps the UES closed until there is the stimulation of a food bolus. The UES then relaxes with a swallow and is integrated with the tongue and posterior oropharynx. Regardless of the size of the bolus, the degree of UES relaxation is the same, however, the amount the UES opens is based on size of the bolus. Relaxation of the UES precedes the sphincter opening by 0.1 seconds. Once the food enters the esophagus proper, the UES again regains its tonicity.
Within the esophagus the longitudinal muscles begin to contract causing an overall shortening of the esophageal body. The esophagus can shorten approximately 2-2.5 cm in total length. This is followed by the contraction of the circular muscles that propel the bolus down the esophagus. The bolus typically travels 2-4cm/second which means that a normal esophagus (length 20cm) should empty its bolus in 10 seconds.
The movement of the bolus through the esophagus should be one directional and somewhat uniform. There are two types of peristaltic waves that empty the esophagus.
Primary peristalsis is initiated by the pharyngeal phase of swallowing and thus is a voluntary process. A single wave caused by contraction of the circular muscles essentially strips the esophagus of its content and deposits it into the stomach. This may be followed by secondary peristalsis which is an involuntary process initiated by the neurologic properties of the esophagus itself. In response to distension from the lack of complete emptying with primary peristalsis or reflux of debris back into the esophagus.
Therefore, the competence of the lower esophageal sphincter (LES) is quite important to maintaining proper esophageal peristalsis. The LES relaxes about two seconds after a swallow is initiated to allow for bolus passage. The normal resting pressure is thought to be 15-25mmHg and relaxes to near zero with swallowing and a rebound higher value once the muscles tense.
Swallowing
Once the food or fluid is placed in the mouth and after it is chewed it is held in the oral cavity until the function of swallowing is initiated.
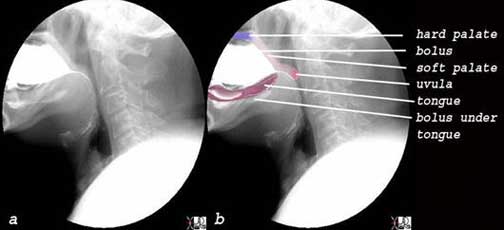
blue = hard palate, light pink = soft palate, bright pink = uvula, white = bolus in mouth, maroon = tongue
Courtesy of: Ashley Davidoff, M.D.
The food or fluid needs to be moved from the mouth to the oropharynx. Reflux of the bolus needs to be prevented from going up the nasopharynx and instead needs to be directed to the oropharynx.
The pharynx is the intermediary pathway between the mouth and the esophagus. There are three basic parts to the pharynx; nasopharynx, oropharynx and hypopharynx. The bolus has to b prevented from going into the nasopharynx and needs to be directed to the oropharynx and the hypopharynx.
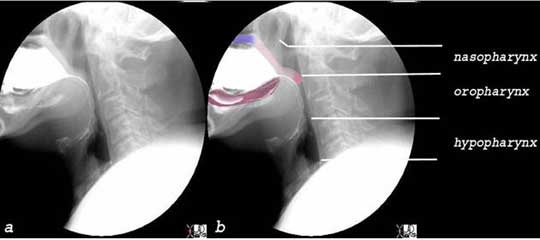
Nasopharynx, Oropharynx and Hypopharynx
Courtesy of: Ashley Davidoff, M.D.
Once the swallow is initiated the bolus is moved from the mouth to the posterior oropharynx. The tongue pushes the bolus into the oropharynx. A peristaltic wave then propels the bolus controlled by the cerebral cortex and medulla. The soft palate moves upward preventing the bolus from entering the nasopharynx and the bolus is directed to the oropharynx and then hypopharynx by the tongue and directed by pharyngeal muscles.

Courtesy of: Ashley Davidoff, M.D.
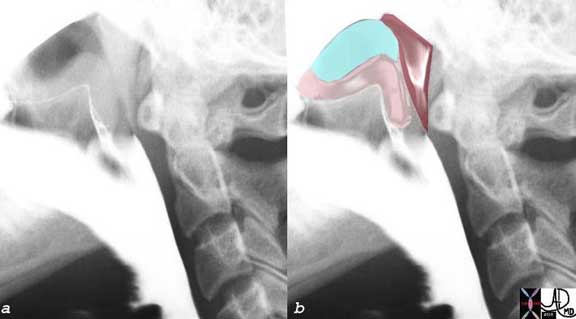
teal = nasopharynx, pink = soft palate, maroon = superior constrictors
The soft palate elevates, the superior constrictors converge on the soft palate, and food and fluid pass into the oropharynx.
Courtesy of: Ashley Davidoff, M.D.
The bolus has to be directed toward the esophagus and away from the airway. The latter is accomplished by the elevation and backward tilting of the epiglottis. The larynx elevates and tilts the epiglottis horizontally. The thyroepiglottic muscles contract and tilt the epiglottis backward. In so doing the vestibule above the vocal cords is closed and the airway becomes sealed.
During the second phase once the bolus leaves the mouth, the epiglottis tilts back first caused by the elevation of the larynx (epiglottis becomes horizontal) and secondly by the active contraction of the thyroepiglottic muscle (epiglottis flips back). This causes the laryngeal aditus to be protected and the food bolus is directed into the pyriform sinuses and valleculae and then down the esophagus.
The bolus in the hypopharynx causes the UES to open and the bolus passes into the proximal esophagus, and the primary stripping wave is initiated. The UES is also called the cricopharyngeal sphincter because it is formed mainly by the cricopharyngeus muscle.
Courtesy Ashley Davidoff MD
Regardless of the size of the food bolus being swallowed, the UES muscle fibers relax the same amount. In other words, if one were to measure the muscle tonicity during the swallow of a sip of water versus a large piece of steak, they would be equal. However, the diameter that the region opens to is related to the bolus size. So that same piece of steak would cause the UES to open, or stretch, to a greater degree than the sip of water.
The UES relaxes 0.1 seconds before the sphincter actually opens to allow for the bolus to pass. This shows the importance of proper efferent and afferent cooperation.
Once the bolus has passed, the UES closes and the posterior pharyngeal constrictor muscles contract.
This provides a high pressure in the hypopharynx, with a lower pressure in the esophagus. Once the bolus passes through the cricopharyngeus muscle, the esophageal phase has begun. The longitudinal muscles contract, causing an overall shortening of the esophagus by 2-2.5cm. Soon after this longitudinal muscle contraction, the circular muscles contract forcing the bolus more distally. Hence, the peristaltic wave that was initiated in the oropharyngeal phase continues to propel down the esophagus. This is known as a primary peristaltic wave. Normal ranges for primary contraction pressures range from 30-120mmHg. It is a rapid contraction, with the peak strength reached in approximately one second. Relaxation of the muscles needs to be just as rapid so the bolus can continue passing smoothly in a uniform direction. The bolus should travel with the primary peristaltic wave at a rate of 2-4cm/second.
If, however, the esophagus is not completely emptied of the bolus, the efferent vagal nerves that arise in the medulla sense this distension and cause another peristaltic wave. This wave is known as secondary peristalsis. It is completely an involuntary process.
The bolus then reaches the distal esophagus and passes through the LES which typically relaxes, and therefore opens, approximately two seconds after a swallow is initiated.
There is a unique inhibitory process within the esophagus, known as ?deglutive inhibition.? This is the rapid and complete inhibition of a second peristaltic process if the previous peristaltic wave hasn?t been completed. It results from hyper-polarization of the neurons of the myenteric plexus innervating the smooth muscles responsible for peristalsis. This, along with the above discussed efferent/afferent signaling, allows for unidirectional passage of a food bolus to the stomach for digestion.

The normal propagation can be seen in the above diagram of a motility study that follows the pressure gradient within the esophagus during a wet swallow. The initial dip on the diagram at the upper sphincter indicates a relaxation of this muscle to allow for passage of food and then the rapid return to the closed state indicated by the rapid upswing. Similarly, there is a drop in muscle pressure at the lower sphincter approximately 2 seconds (2 boxes) after the swallow indicating relaxation of the muscle to allow food to enter the stomach.
Courtesy Ashley Davidoff MD
There is a unique inhibitory process within the esophagus, known as ?deglutive inhibition.? This is the rapid and complete inhibition of a second peristaltic process if the previous peristaltic wave hasn?t been completed. It results from hyper-polarization of the neurons of the myenteric plexus innervating the smooth muscles responsible for peristalsis. This, along with the above discussed efferent/afferent signaling, allows for unidimensional passage of a food bolus to the stomach for digestion.

Images courtesy of: Ashley Davidoff, M.D.
Diseases
The most common disorders that affect the esophagus and the swallowing mechanism include neuromuscular disorders, inflammatory and neoplastic diseases. The functionally unique disorders relate to the neuromuscular muscular dysfunction. These diseases result from pathology involving the complex innervation and muscular function of the esophagus. The esophagus is unique in that it contains both skeletal muscle and smooth muscle and hence diseases that affect either of these will manifest with swallowing problems. The clinical manifestations of these disorders include aspiration, dysphagia, and odynophagia. The evaluation of the diseases requires attention to the pharyngeal area, the upper esophageal sphincter, the mucosal surface, and the lower esophageal sphincter.
Mechanical Diseases
Under the broad category of mechanical diseases we include all the neuromuscular diseases that affect swallowing. Some of these diseases are relatively common and include the manifestations of stroke and Parkinson?s disease on swallowing, while others are relatively uncommon and include amyotrophic lateral sclerosis, bulbar palsy, muscular dystrophy, myasthenia gravis, spinal muscular atrophy, polymyositis and scleroderma. In the assessment of these diseases the diagnostic evaluation usually starts with a barium swallow, and or a modified barium swallow to evaluate the hypopharynx and UES.
Mechanical Diseases: Laryngeal Penetration
Laryngeal penetration is a mechanical disorder of swallowing caused by a variety of diseases that affect neural and or muscular function of swallowing resulting in spillage of food or fluid into the laryngeal vestibule, superior to the cords (glottis) without traversing the cords.
Clinically, it is usually silent and is diagnosed by radiographic techniques.
The severity of the penetration is based on whether a residue remains in the vestibule at the end of the swallow, for example, whether it clears spontaneously once the swallow is completed. The severity of penetration is also based on whether the penetrated material comes into contact with the cords.
Treatment is directed to the underlying cause of the disease
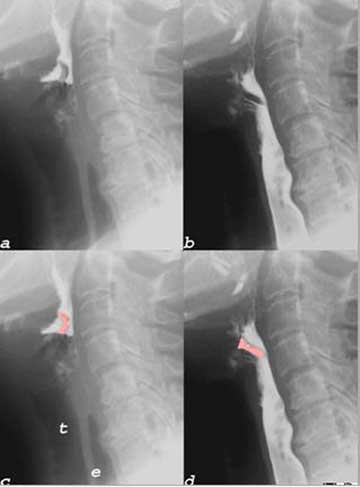
In this lateral projection of the plain film of the neck, the vestibule (teal) is filled with air. The epiglottis is shown in pink and the laryngeal ventricle is shown in royal blue. During a normal barium swallow it should remain free of barium since the epiglottis and constrictors of the pharynx, together with the elevation of the glottis should momentarily occlude the airways.
Courtesy of: Ashley Davidoff, M.D.

The anterior-posterior (A-P) and lateral examination of the neck following a barium swallow shows penetration (green) into the laryngeal ventricle. This case shows severe penetration since the barium has not cleared spontaneously after the swallow, remains in the vestibule above the vocal cords. However, it remains above the false vocal cords and has not come into contact with the true vocal cords.
Courtesy of: Ashley Davidoff, M.D.
Mechanical Diseases: Aspiration
Aspiration is a mechanical disorder of swallowing caused by a variety of diseases that affect neural and or muscular function of swallowing resulting in spillage of food or fluid into airways. Clinically, it usually induces the patient to cough and is diagnosed by radiographic techniques. The severity of the aspiration is based on whether a residue remains in the airways at the end of the swallow, and whether the patient can clear the residue. The most severe form is in the patient who aspirates and has no response to the aspiration.
Complications include aspiration pneumonia which can be a fatal entity.
Treatment is directed to the underlying cause of the disease. Special diets and mechanical maneuvers such as changing the head position during the swallow can be applied to limit aspiration in selected patients.
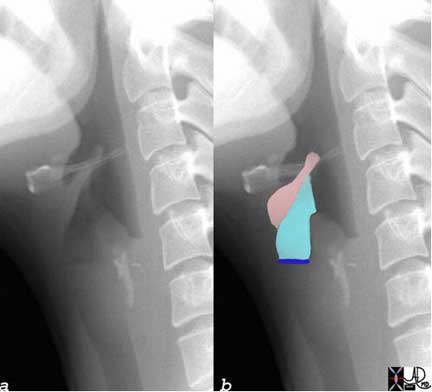
The barium swallow in this patient shows spillage and penetration of the contrast medium into the vestibule (pink) into the laryngeal ventricle (orange) and subsequently aspiration through the vocal cords and into the trachea. (lime green) The trachea is overlaid in a hunter green color and the lime green spillage is seen trailing down its right wall.
pink = spillage and penetration into vestibule
orange = penetration into the laryngeal ventricle
lime green = aspiration into right side of trachea
hunter green = trachea.
|
Table 1 Scaling penetration and Aspiration
|
||||||||||||||||||||||
| Adapted from Rosenbek JC et al 1996 and Gramigna 2006 |
At the other end of the esophagus at the LES, there are a few mechanical disorders that either result in excessive contraction and failure of the LES to relax or result in incompetence of the LES such as in reflux.
Mechanical Diseases: Achalasia
Achalasia is an uncommon mechanical disorder of the esophagus characterized by neuromuscular dysfunction. It is caused by the loss of ganglion cells in the muscular layer of the esophagus. An immune process is thought to cause destruction of the ganglion cells. The loss of the ganglion cells results in spasm of the LES, aperistalsis of the thoracic esophagus, and consequent dilatation of the esophagus. Complications include weight loss, malnutrition, vomiting, piration and esophagitis.
Clinically, symptoms include liquid and solid dysphagia, weight loss, aspiration, chest pain, and regurgitation.
The diagnosis is confirmed by single contrast barium swallow or by endoscopy and it is treated surgically with myotomy and plication.
The two images from a single contrast barium swallow show a normal esophagus and GE junction on the left and a dilated esophagus with a hypertonic LES on the right. The appearance of the image on the right is reminiscent of a condition called achalasia. The focal obstruction at the GE junction and dilatation of the upstream esophagus is caused by failure of the LES to relax.
Courtesy Ashley Davidoff MD

A CT scan through the chest on a patient with achalasia with an enormous esophagus filled with solid food(a, b). A bezoar (arrow) is present in the esophagus. In (d) the transition from the distended esophagus to the obstruction is seen as a focal pointed narrowing (arrowhead)? reminiscent of the beginning of the rat-tail.
Courtesy of: Ashley Davidoff, M.D.
Mechanical Diseases: Gastroesophageal Reflux Disease
Gastroesophageal Reflux Disease (GERD) is a common mechanical disorder of the lower esophageal sphincter and it is caused by multiple factors including obesity, transient relaxation of the LES and hiatus hernia. The reflux of acidic gastric contents onto the esophageal mucosa results in distension of the esophagus and inflammatory changes commonly complicated by erosive esophagitis.
Up to 15% of adults in Western society report GERD symptoms monthly or weekly, while 7% report daily symptoms.
The diagnosis is probably best made clinically. The clinical presentation varies from the classic retrosternal burning sensation to chest pain, waterbrash (hypersalivation), and halitosis. It has been suggested that up to 60% of non-cardiac chest pain can be attributed to GERD. The absence of gastroesophageal reflux in a barium swallow does not exclude the diagnosis. A hiatus hernia sometimes causes reflux, but finding a hiatus hernia on a barium swallow does not necessarily imply that there is reflux.
The mainstay of therapy for GERD remains the Proton Pump Inhibitors (PPI) and the H2 Blockers.
Courtesy of: Ashley Davidoff, M.D.
Mechanical Diseases: Esophagitis
Esophagitis is an inflammatory response of the esophagus to multiple causes, the most common of which is due to reflux of acidic gastric contents through an incompetent lower esophageal sphincter into the distal esophagus. It is thus considered in this instance as a chemical burn.
It is characterized by a reddened inflamed and swollen and often erosive mucosa, resulting in pain that may be epigastric or substernal. This presentation may simulate cardiac pain.
Long standing esophagitis may be complicated by a peptic stricture or Barrett’s esophagus which is a premalignant condition.
The diagnosis is suspected clinically by the classical presentation of substernal burning in the presence of symptoms of reflux, waterbrash (hypersalivation), and halitosis, with relief from antacid therapy. Documentation of the disease is best achieved by endoscopy, with double contrast barium swallow being less sensitive to the disease.
The mainstay of therapy for GERD with esophagitis, remains the proton pump inhibitors (PPI) and the H2 Blockers
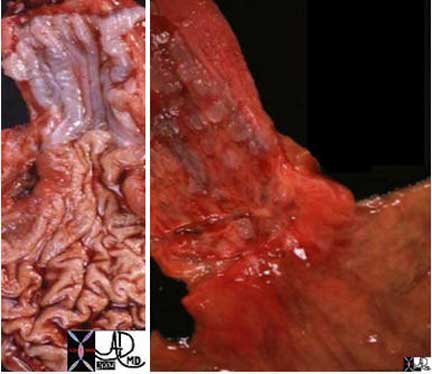
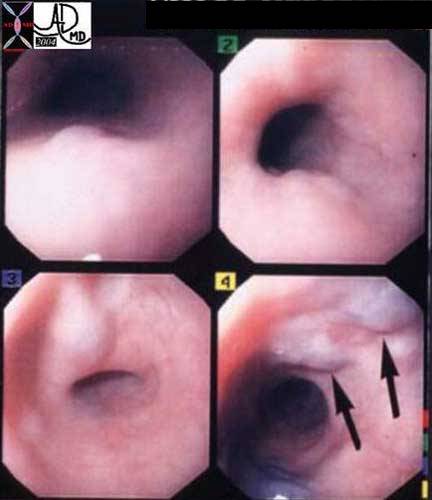
The GE junction is a distinct border as seen normally in the left image. The distal esophagus is normally a pearl white hue, while the gastric mucosa is a pink hue. In esophagitis the hyperemic inflammatory changes make the border less distinct (right image).
Courtesy of: Ashley Davidoff, M.D.
Mechanical Diseases: Hiatus Hernia
A hiatus hernia is a common mechanical abnormality of the GE junction, characterized by an abnormal position of the GE junction and superior components of the stomach (cardia and sometimes fundus.) There are two types; the sliding hiatus hernia and the paraesophageal hernia.
The underlying cause appears to be multifactorial including ligamentous laxity, obesity, and raised intraabdominal pressure.
The widening of the esophageal hiatus results in a variable amount of stomach in the chest cavity. The GE junction is usually displaced cranially but may be normal in the patients with a paraesophageal hernia. Reflux may or may not be an associated consequence of the entity.
Complications include the association with reflux and esophagitis and paraesophageal hernias are prone to gastric volvulus.
The diagnosis, in the absence of reflux is asymptomatic, and is usually diagnosed by imaging techniques including barium swallow, upper GI or endoscopy. It is not uncommon to suspect the diagnosis on routine chest X-ray, with the hernia best seen in the lateral examination.
Treatment is not usually warranted in patients without significant reflux, but surgery is indicated when the patients fail to respond to conservative therapy. All patients with paraesophageal hernias should undergo surgical correction because of the propensity to torsion.
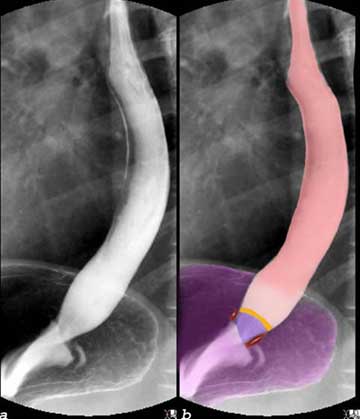
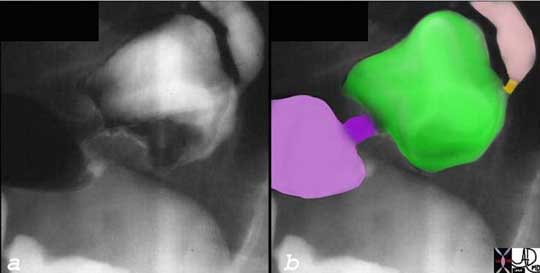
The barium swallow shows a normal GE junction. The position of the diaphragm is inferred (marron).
Other structures include:
salmon = thoracic esophagus
light pink = epiphrenic ampulla
orange = GE junction
purple = region of stomach surrounded by diaphragm
light purple = fundus and cardia of stomach
Courtesy of: Ashley Davidoff, M.D.
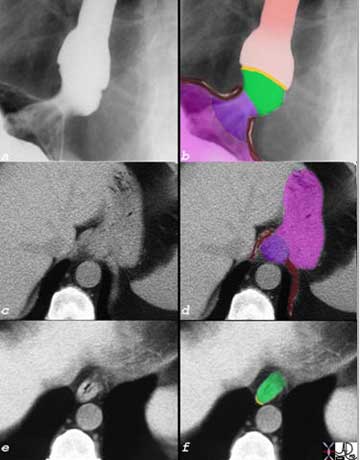
In this instance there is a small sliding hiatus hernia (green)(b) identified in the barium swallow (a and b). The GE junction(orange) lies in the within the chest, and the epiphrenic ampulla is more cranial than it should be. A new portion of the stomach (purple) is now positioned in the region of the esophageal hiatus.
The correlative CT scan (c-f) shows that the space between the two crura (maroon in d) is abnormally widened and is associated with redundant gastric mucosa (purple), while the sliding hiatus hernia (green in f) is positioned in the chest. The orange line of the GE junction is an inferred position for the GE junction.
Courtesy of: Ashley Davidoff, M.D.
stomach, gastric mucosa, Z line esophagus = salmon
epiphrenic ampulla = light pink
GE junction Z line = orange
diaphragm = maroon
sliding hiatus hernia = lime green
purple stomach pulled into hiatus stomach = dark pink
Courtesy of: Ashley Davidoff, M.D.
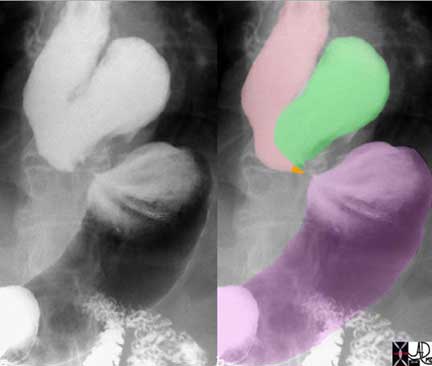
In this barium swallow the GE junction (orange) is in normal position but a portion of the fundus (green) has slid through the esophageal hiatus into the chest cavity. The narrow neck with mobile stomach above and below predisposes this hernia to torsion which can be a life-threatening emergency. Once diagnosed this hernia requires surgical correction.
pink = esophagus
orange GE junction (inferred)
paraesophageal hernia = green
normal positioned stomach = purple
Images courtesy of: Ashley Davidoff, M.D.
Mechanical Diseases: Barrett?s Esophagus
Barrett?s esophagus is an abnormal growth disorder of the gastroesophageal junction characterized by metaplastic change of the squamous epithelium into a glandular columnar epithelium caused by longstanding gastroesophageal reflux. With this change there may be resulting alteration in the DNA rendering the entity a premalignant condition.
The clinical presentation is non specific and includes the dyspeptic symptoms of GERD . The diagnosis is made by endoscopy, where the extension of the gastric mucosa into the squamous territory is seen as cracks of salmon colored areas in the white esophageal mucosa. Biopsies need to be taken to evaluate for dysplasia. In the absence of dysplasia treatment includes ongoing surveillance, with aggressive medical treatment of the GERD. In the presence of dysplasia removal of the dysplastic abnormalities is indicated. A variety of endoscopic ablative therapies and surgical options are available.

The extension of the gastric mucosa as ?cracks? in the otherwise pearly white esophageal mucosa represents metaplasia (a growth and character change) of the normal squamous mucosa into gastric mucosa.
Courtesy of: Joshua Namias, M.D. and Ashley Davidoff, M.D.
Carcinoma
Esophageal cancer is a malignant growth disorder of esophageal mucosa. Historically squamous cell cancer was the predominant type; however, more recently, a surge in adenocarcinoma as the more common entity has evolved. Sqaumous cell carcinoma characteristically occurs in the thoracic esophagus while adenocarcinoma occurs at the GE junction.
Many different causative factors have been associated with this condition including GERD, Barrett?s esophagus, dietary factors, smoking and geographic location.
The disease results in an aggressive, space occupying mass that progressively impinges on the lumen of the esophagus to cause dysphagia.
It is most commonly diagnosed by endoscopy and biopsy, staged with CT and PET scan, and best treated with a combination of surgical and medical therapies.
The overall prognosis is quite poor, with 5 year survival estimated to be between 10-13% for advanced disease. With the increased diagnosis of Barrett?s esophagus and the routine surveillance that follows, earlier detection of cancer allows for treatment and better survival rates. Survival rates are much improved with more superficial cancers that are found with increasing frequency during endoscopic surveillance.
Ashley Davidoff, M.D.

Courtesy of: Ashley Davidoff, M.D.
Varices
Esophageal varices are dilated and tortuous veins that are found in and around the lower esophagus. The cause is portal hypertension as a result of cirrhosis. The distorted and fibrotic architecture of the liver, increases resistance to blood flow, thus causing a rise in the portal pressure. The varicose veins that result enable the flow of blood to find alternate routes back to the heart acting as portosystemic shunts which bypass the liver.
Esophageal varices are often complicated by hemorrhage which can be life-threatening.
Varices are silent clinically until they hemorrhage. Documentation of varices is accomplished non-invasively by CT scan with contrast, but is commonly diagnosed by endoscopy and endoscopic ultrasound.
Endoscopic therapy includes banding of the varices and sclerotherapy. TIPS procedure is an ingenious percutaneous method that enables shunting of portal venous blood into the hepatic veins via an implanted stent.
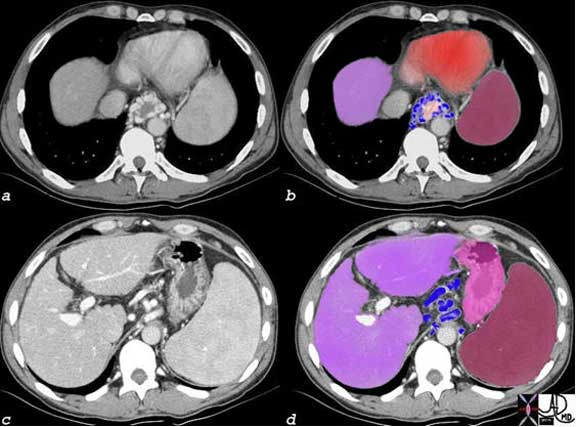
Esophageal varices (a) and overlaid in blue in (b) are noted surrounding the esophagus (light pink), but are also seen in the gastrohepatic ligament near the GE junction in (c) and overlaid in blue in (d). The patient has cirrhosis as seen as a faintly irregular margin of the liver (purple) and an enlarged spleen. (maroon) The stomach is overlaid in shocking pink.
Courtesy of: Ashley Davidoff, M.D
In the endoscopic image above, there are a few varices with the largest traversing in the right upper portion of the esophagus.
Courtesy of: Joshua Namias, M.D. and Ashley Davidoff, M.D.
Clinical Aspects
A myriad of complaints can lead a patient to the gastroenterologist for evaluation for an esophageal process. The most common complaint is of heartburn or reflux, while dyspagia is quite common as well. Retrosternal burning, acidic or metallic taste in the mouth, or regurgitation of foods is the typical complaint. Other common complaints that suggest an esophageal etiology include odynophagia, and atypical chest pain.
Endoscopy
Endoscopy of the esophagus is a procedure that enables diagnostic evaluation and often treatment of esophageal diseases.
The endoscope is a flexible fiberoptic camera that can be placed via the mouth for real-time visualization of the gastrointestinal tract. Derived for the Greek words ?endo? (within) and scope (view), the first reference to this modality was by Hippocrates in regards to an anal evaluation.
The more modern scope was prototyped by Basil Hirshowitz in 1958 and the more advanced scopes used today were built on his advances.
Indications
Endosocopy has an important role in diagnosing esophageal disorders, in addition to those of the upper intestinal tract. Typically endoscopic studies are performed when there is concern for a luminal irregularity such as esophagitis, Barrett?s esophagus (in the setting of long standing GERD), rings/strictures, and malignancy.
Endoscopic ultrasound is especially useful in delineating the extent (depth) of esophageal mucosal lesions such as cancer.
It is important to realize that endoscopic studies are often used in conjunction with many other tests to be described below.
Contraindications
When done in the appropriate clinical setting, endoscopy is a safe and helpful diagnostic tool. However, it is an invasive procedure and with it comes possible complications. To avoid complications, the endoscopist must be able to identify those patients in whom endoscopy could cause more harm than benefit from the procedure.
As such, contraindications for endoscopy include patients whose hemodynamic status prevents safe administration of the required sedatives. The sedatives and narcotics given can cause a drop in blood pressure in addition to suppressing respiration.
To properly perform endoscopy, the lumen must be insufflated with air. If a patient has concern for, or has a documented, perforated viscus, air insufflation would worsen the condition. Referring to LaPlace?s law, the diameter of the lumen would increase thus increasing surface tension and the risk of perforation.
Advantages and Disadvantages
Advantages
The advantage of endoscopy is that the pathology can be biopsied through the scope. The scope has several channels that allow objects to be passed into the organ being evaluated. The biopsy forceps can be directed directly to the abnormal tissue and the tissue removed for histopathological evaluation.
Therapeutic intervention can also be performed through the endoscope. As described above, treatment of Barrett?s esophagus can be accomplished with the endoscope. Treatment modalities include Argon Plasma Coagulation (APC), photodynamic therapy, and mucosal resection, amongst others.
Dilation of strictures or rings can be accomplished with balloons passed through the endoscope. This allows for visualization of the mechanical disruption with these devices.
Retrieval of foreign bodies is a common therapeutic intervention performed with the endoscope. Patients who present with food bolus that can?t pass on their own are often scoped with the goal of removing the bolus. Patients who ingest objects, intentionally or unintentionally, that get stuck in the esophagus can have them removed. Again, through the scope, baskets, snares, nets, can all be passed to retrieve foreign material or even large pieces of food such as steak that may become impacted.
Endoscopic ultrasound is a relatively new modality that incorporates traditional endoscopy and the properties of ultrasonography. A special ultrasound is fitted onto the distal end of the scope and thus provides excellent visualization of the layers of the esophagus and the surrounding structures. Biopsies can also be taken of the identified pathology including the esophagus proper, masses, lymph nodes and other masses near the esophagus.
Disadvantages
The main disadvantage to endoscopy is that it is a invasive procedure that requires sedation. While typically thought of as a relatively benign invasive test, complications can quickly arise.
Patients need to be hemodynamically stable and able to withstand the anesthesia and the stress of the procedure itself.
Aim
The upper endoscope has multiple important uses in regards to evaluating, diagnosis, and treating esophageal pathology. This modality allows the gastroenterologist to visualize the esophageal mucosa and lumen. Evidence of inflammation, ulcers, strictures, and masses all can therefore be appreciated.
Patient Preparation
For upper endoscopy the patient is kept in the fasting state for at least 4-6 hours. The main reason this is required is to reduce the risk of aspiration with the anesthesia. Visualization is often impaired with upper endoscopy if food is present in the stomach.
The day of the procedure, the patient presents in the fasting state.
Ideally, patients should be off of all anticoagulation and platelet inhibitors. Most standardized preparations ask the patient to hold all aspirin and NSAIDs for approximately one week so as to avoid increased risk of bleeding.
Equipment
Each procedure room is equipped with patient monitoring systems that allow for continuous measurements of blood pressure, heart rate, respiratory rate, and oxygen saturation. A TV screen is located across from the endoscopist with the scope processor capturing images. One to two nurses are present to assist with sedation, patient monitoring, and therapeutic interventions. Each room typically has all the equipment that may be needed during cases such as biopsy forceps, snares, clips, baskets and the like.
Procedure
Patients are typically brought into the procedure room and placed in the left lateral decubitus position. An IV is placed so sedative medications can be given intraveniously. When performing an endoscopy, once the patient is sedated the endoscope is placed into the mouth. Visualization of the tongue and posterior oropharynx allows for passage into the esophagus. The scope is then carefully passed through the esophagus into the stomach and small intestine.
Images are displayed on television sets which are often located on both sides of the room.
Once the test is completed, the patient is brought to the recovery area where they rest for approximately one hour while the medications wear off. The patients are discharged to home with an escort and instructed not to drive, drink alcohol, or perform manual labor for the remainder of the day.
The overall risk of complications during endoscopic procedures is quite low, especially in the hands of a experienced endoscopist. In addition to the risk of received conscious sedation (allergic reaction to sedatives, respiratory compromise, hemodynamic changes), the risks of the procedure itself include aspiration, bleeding, perforation.
Aspiration is higher in patients undergoing upper endoscopy given the passage of the camera through the mouth.
Bleeding can occur for various reasons. Trauma from the passage of the scope can occur, although is quite rare. Bleeding can occur when diagnostic or therapeutic interventions are performed. With biopsy of the mucosa, local bleeding can occur, but typically are self-limiting. A common scenario seen by the endoscopist is of a patient who has a polyp removed at colonoscopy and who restarts their aspirin earlier that the recommended time (typically 1-2 weeks). The anti-platelet function of the aspirin results in bleeding from the polypectomy site.
Perforation is a rare, but often serious complication of both upper and lower endoscopic procedures. In experienced hands, the perforation rate of colonoscopy is thought to be approximately 1/1000 for a diagnostic colonoscopy.
Endoscopy is an extremely useful and safe diagnostic as well as a therapeutic tool . It is also provides a life-saving measure in certain conditions.
Barium Swallow
A barium swallow is a diagnostic study that uses a contrast medium to evaluate the structure and real time function of the esophagus.
The patient is given a barium or gastrograffin drink and examined fluoroscopically. The patient swallows the contrast and images are taken of the barium passage from the mouth down the esophagus.
It is usual also to perform both a double and single contrast study. The double contrast requires the patient to precede the thick barium drink with a small cup of an effervescent mixture, similar to a bubbly carbonated drink. This creates an air contrast column enabling optimal evaluation of the mucosa. The single contrast study uses thin barium and is important to evaluate for aspiration, strictures, reflux, and hiatus hernias.
A barium study is often used to assist in the diagnosis of various esophageal pathologies such as rings/strictures, masses/polyps, ulcers, hernias, altered anatomy such as a corkscrew esophagus, and even disorders of swallowing such as aspiration, esophageal spasm and achalasia. Reflux can also be evaluated. When a ruptured esophagus is suspected it is the procedure of choice and should be performed with gastrograffin.
Alternative or adjunctive tests include upper endoscopy and manometry. Aspiration and reflux are best observed with the barium swallow. Esophageal leaks and identification of foreign bodies are well evaluated by the swallow in emergency situations. It is a good first test in the patient with dysphagia.
Patients who are unable to swallow the barium material or who are high risk for aspiration should not undergo barium radiography.
Advantages and Disadvantages
Barium has the advantage of being less invasive than the some of the other modalities. While there are risks, such as aspiration and allergic reactions, it is thought to be a safe and helpful study especially in those patients who may be at higher risk for one of the other alternate tests.
The main disadvantage of barium radiography is the inability to perform therapeutic modalities when abnormal finding are identified.
The aim of a barium test is to allow for real-time evaluation of the esophageal contour, anatomy, and swallowing function.
Barium Swallow: Patient Preparation
Patients present to the fluoroscopy suite within the division of radiology in the fasting state.
After the test they should drink large volumes of water to ensure that the barium is assisted in its passage through the gastrointestinal tract.
Contrast material and a fluoroscopic x-ray machine are required for proper visualization.
Procedure
Patients are asked to drink the barium material while the radiologist obtains images documenting the passage of barium down the esophagus. The thick barium is used in the double contrast study and the thin in the single contrast study. Gastrograffin is used if there is a clinical concern for perforation. When aspiration is at issue, then gastrograffin is contraindicated because its hypertonic nature will cause significant fluid shift into the lungs.
The double contrast is best used for mucosal evaluation. When possible it is performed on all patients. The patient is standing for the examination. The patient is first asked to swallow a mixture of effervescent powder (“fizzies”) mixed in 10 mls of water. Carbon dioxide is released and distends the stomach but also refluxes into the esophagus causing it to distend. 4-5 sips of barium are then “gulped” down in attempt to inhibit peristalsis and distend the esophagus. A perfect double contrast study is not achieved in all patients. This study is best used to study the mucosal surface of the esophagus.
The single contrast study is also performed on all patients and is first performed in the upright projection to evaluate the oropharyngeal phase of the swallow. The patient is asked to holds a mouthful of barium until instructed to swallow. The swallow is followed from the back of the mouth, posterior soft palate, through the valleculae, pyriform sinuses and into the proximal esophagus using rapid film technique because the bolus moves so quickly. This is viewed and filmed in two views. The bolus is then tracked through the upper esophagus, mid and distal esophagus using a variety of filming techniques including changing degrees of obliquity, variation in the rapidity of filming and degree of magnification.
The patient is then placed in the prone position, with left side slightly up and is again asked to swallow the thin barium. The prone view is best for the evaluation of the distal esophagus and GE junction and hence diseases such as hiatus hernia, peptic strictures are best demonstrated. A full column view of the esophagus is often obtained
Throughout the exam attention to the GE junction is paid in order to evaluate for spontaneous reflux.
The patient is then returned to the upright position and is asked to swallow a 13mm barium pill to determine if there are any significant strictures.
Barium Swallow: Results
Images are obtained that allow for evaluation of the swallowing pattern based on the flow of barium. Luminal irregularities can be identified such as ulcers, strictures, and extrinsic compressions.
The fully distended mucosal surface should be smooth and featureless. In about 10% of the older population flat lesions representing glycogenic acanthosis may be seen. Distally the z -line representing the squamocolumnar junction is seen as a zigzagging line at the level of the diaphragm and esophageal hiatus.
The relief view represents the collapsed esophagus and longitudinal folds are seen extending the entire length of the esophagus.
Transverse folds (also know as the feline esophagus or shivering esophagus ) represent contraction of the longitudinal folds of the muscularis mucosa. This finding is seen both in normal patients and in patients with reflux.

Occasionally the transverse folds of the esophagus are seen on a double contrast barium swallow. This is seen both in normal patients and those with reflux disease.
Courtesy Ashley Davidoff MD
Two impressions on the esophagus are almost always observed. The first is that of the aortic arch and the second of the left mainstem bronchus. The pulsating impression of the left atrium especially when enlarged can be seen on the lower one third of the esophagus.
The abnormal esophagus may show nodularity, punctate collections of barium surrounded by a rim of edema, or linear ulcers with surrounding edema. The surface edge of the esophagus should be smooth. Any irregularity usually suggests esophagitis.
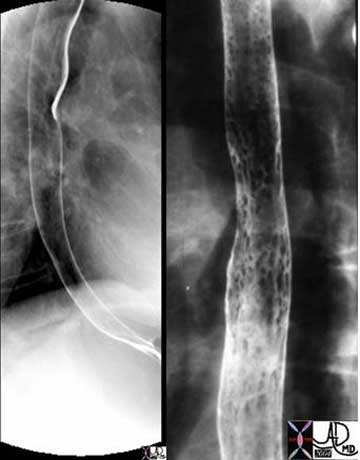
Double contrast barium swallow shows a normal esophagus with smooth mucosa on the left and a nodular mucosa on the right reminiscent of Candida esophagitis. The patient had Candida identified on his buccal mucosa.
Courtesy of: Ashley Davidoff, M.D.
Complications related to barium esophography are rare. The main complication patients are informed of is aspiration of the contrast material. In patients with slow gastrointestinal transit, the barium can also solidify and form a bezoar, but this is a rare complication.
A barium swallow offers a safe and effective means of evaluating the structure and function of the esophagus, offering a unique ability to evaluate for aspiration.
Other Modalities
CT is an essential examination in systemic diseases when structures outside the esophagus need evaluation. Hence, it is an essential examination in the work up of a patient with carcinoma of the esophagus in order to stage and therefore treat the patient appropriately. Regional lymph nodes and the liver are common sites of spread and these are best evaluated with CT scan. In diseases that affect multiple organs such as scleroderma, involvement of the lungs and heart require evaluation. CT scanning offers global evaluation of these structures and the body as a whole.

This unfortunate 32-year-old female patient has severe scleroderma. The esophagus is enlarged and patulous (pink b and d)) the right-sided structures of the heart (maroon d) are enlarged secondary to pulmonary hypertension, the bases of the lungs are fibrotic (a and b) there are bilateral effusions (yellow (c and d) there is a small pericardial effusion (pale yellow c and d) and the gall bladder is edematous (orange and green e and f). CT scanning offers a global view of all these disorders.
Courtesy of: Ashley Davidoff, M.D.
PET scan is also extremely useful and an essential tool in staging esophageal carcinoma. Nodes that are enlarged in the mediastinum may be reactive or may be neoplastic in nature. A positive PET scan would favor malignant involvement though false positives do exist.
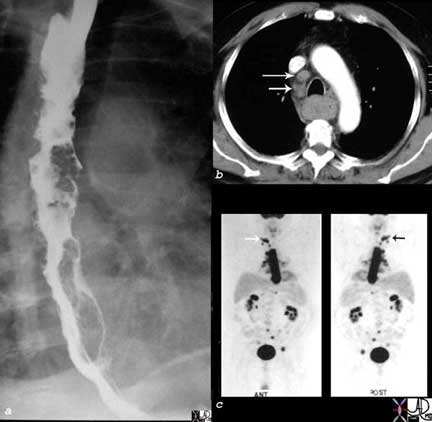
The barium swallow in image a shows diffuse irregularity of the lower 2/3 of the esophagus which was due to carcinoma of the esophagus. Enlarged lymph nodes on the CT scan are suspicious, (b arrows) but the distinction between reactive disease and malignant disease could not be made. The PET scan was positive making metastases likely (c arrows).
Courtesy of: Ashley Davidoff, M.D
Conclusion
The esophagus is a simple tube with complex function. Meticulous coordination is required in the region of the UES and the LES in order to prevent reflux. Aspiration pneumonia in the elderly is a common disease and can even be fatal.
The esophagus is the most muscular component of the GI tract, with the upper portion being skeletal and the lower part which has smooth muscle in the wall. Common diseases include GERD and esophagitis. Chronic esophagitis is complicated by stricture formation and Barrett?s esophagus. The latter is a premalignant disease. Carcinoma itself carries a poor prognosis.
Endoscopy and barium swallow remain the mainstay of diagnostic armamentarium.
Therapy for the common ailments of GERD, esophagitis is for the most part treated with medication. Some diseases such as strictures and bleeding can be treated by endoscopic techniques. Surgery is reserved for paraesophageal hiatus hernias and carcinoma.