

Learning Objectives
1) Describe the basic anatomy and physiology of the prostate
2) Locate and identify the structures and zones
3) Describe how anatomy applies in clinical situations
4) Describe the physiology of time and aging
5) Describe the common diseases that affect the prostate
Introduction
The prostate is an accessory organ of the male reproductive system and is a member of the genitourinary system. It is part fibromuscular and part glandular and shaped like an inverted cone, often called chestnut in shape, sometimes walnut in shape and to some extent in size, yet sometimes described as a small plum or even a small kiwi fruit in size. It is far from a vital organ since removal does not affect life itself but radical prostatectomy results in infertility. Thus although it is not vital for one individual human, it is vital to the survival of the human race. A lofty attribute for a small kiwi fruit I would say!
Overview
Structurally, it is characterised by its shape, central position, relationship to the urethra, and its close relationship to the seminal vesicles and ejaculatory ducts. It is the only exocrine organ that has a symmetric and central location in the body. In the central portion of the gland the prostatic urethra acts as the repository of the 3 major components of the semen ? the mysterious fluid that keeps our species going. Thus the prostatic urethra is the ?mixing pot? where semen is formed.
The prostate is divided into concentric zones around the urethra. Zonal anatomy has been a more recent method of characterizing the parts of the prostate since it has embryological, histological and pathological implications. The prostate is found deep in the pelvis and not an obvious organ unless deep dissection is performed. It was therefore not obvious to early anatomists.
The function of the prostate is to secrete a milky fluid which combines with the secretions of the seminal vesicles, sperm from the testes and small contribution from Cowper?s gland to form semen. The fluid that the prostate produces provides nutrients for the semen, aids in the liquefaction of semen after deposition in the vagina, and also aids as a chemical buffer. The relatively alkaline secretion of the seminal vesicles and prostate protect the sperm from the relatively acidic environment of the vagina.
The prostate contributes about 20% of the volume to the seminal fluid.
Common diseases include prostatitis, benign prostatic hyperplasia (BPH) and prostate carcinoma.
Diagnostic evaluations include digital rectal examination (DRA), serum prostate specific antigen (PSA) level, and imaging, usually MRI while transrectal ultrasound is used for biopsy. CTscan, and bone scan are useful in staging.
Treatments include medical therapies, such as the use of hormonal agents, alpha adrenergic (smooth muscle) blockers, antibiotics, and chemo therapy although in cancer, surgery and radiation are commonly employed.
The term prostate is derived from Greek- prostates, which means ?one who stands before”, “protector”, “guardian” owing to is position relative to the bladder.
The Mixing Pot Concept
It is important to understand the role of the prostate as a secondary sexual organ not only in that it secretes a portion of semen, but that semen is formed in the confines of the walls of the prostatic urethra which is of course within the confines of the prostate. This implies that if and when the prostate is removed in radical prostatectomy the mixing pot is removed, and there is no place for semen to be formed which results in infertility. The concept of the prostate acting as a mixing pot is a key, unappreciated, and central function of the prostate.
The prostatic urethra also acts as a conduit for urine. If the prostatic tissue around the urethra enlarges it can result in narrowing of the prostatic urethra. This concept is more easily understood and known and results in a clinical syndrome called prostatism and more recently called lower urinary tract syndrome or LUTS.
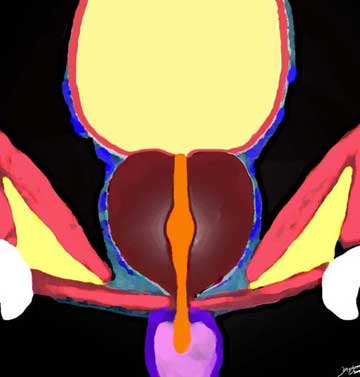
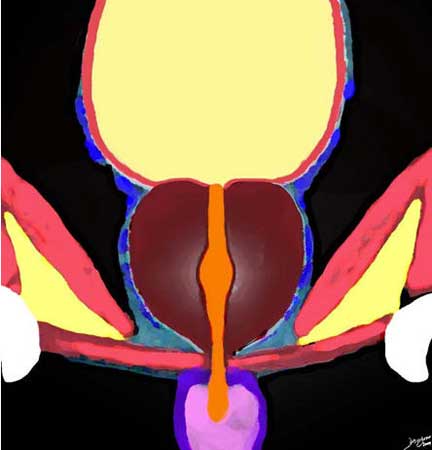
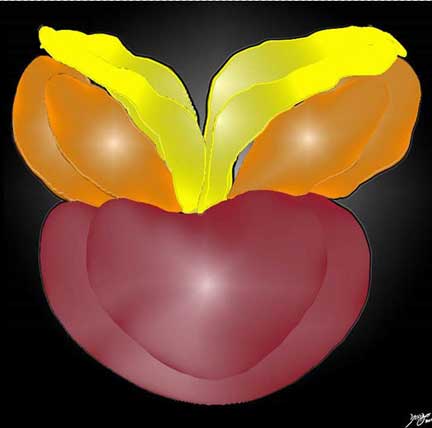
The seminal vesicles (orange), vasa deferentia from the testes (yellow) and the prostate (maroon) are the three major contributors to the formation of semen in the prostatic urethra.
Ashley Davidoff MD

The Mixing Pot in the Prostatic Urethra
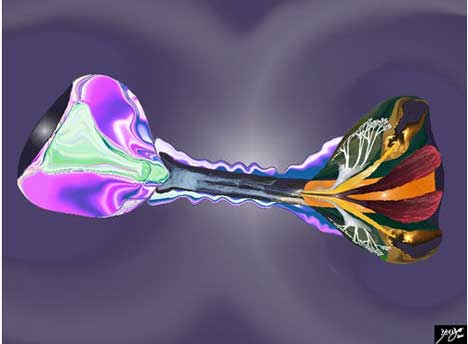
The prostatic urethra serves as the mixing pot for the components of semen by acting as the receptacle of secretions from the prostate itself, the seminal vesicles and the vasa deferentia. This diagram shows the region of the verumontanum which is the site where the mixing pot stands receiving ejaculatory ducts and the region of the 10-15 prostatic ducts empty as well. The prostatic urethra is outlined in orange.
Ashley Davidoff MD
In this diagram the function of the prostate is shown as a mysterious organ acting as a melting pot for the love potions from three structures; testes, seminal vesicles and the prostate itself. It depicts the ?pot? receiving sperm from the testes, breathed into the pot by the alchemist, fluid from the seminal vesicles emanating from the crooked palms of the alchemist, and prostatic secretions entering the brewing pot from the side as white creamy secretions. Cowper?s glands (green) add a tincture of lubricant into the mix in the region of the membranous urethra to complete the formation of semen.
Images courtesy: Ashley Davidoff M.D.

A magnified view of the melting pot and components is depicted with the mysterious melting pot illuminated in orange and pinks in the middle of the image receiving a breath from the contents of the vasa deferentia containing the jewels of the semen, a squirt from the hands representing the contributions from the seminal vesicles to nourish the sperm and the addition of the creamy texture filled with all sorts of goodies from the prostate itself.
Image courtesy of: Ashley Davidoff, M.D.
History
The history of the prostate is one of intermittent and repeated recognition followed by intermittent and repeated neglect. With our aging population and with the incidence of benign prostatic hypertrophy and prostate carcinoma common after 60 and almost universal in the octogenarian population and beyond, it is currently in focus and likely to stay there because of the associated morbidity of prostate disease.
Herophilus of Chalcedon often called the father of anatomy, was a Greek anatomist and physician (335BC -280BC) assigned the name prostate which means ?one standing in front? because he saw it as standing before the testis. Herophilus was one of the founders of the Alexandrian school of medicine which was set up at the end of the 4th century. He probably identified the organ in animals eg monkeys whose prostate consists of two distinct parts.
Rufus of Ephesus was a renowned Greek physician who lived in the first century AD followed Hippocrates and preceded Galen. He noted that in some cases of bladder stone he was able to feel a soft swelling near the bladder neck but he failed to identify the swelling as the prostate gland.
Galen (131 -201 AD) acknowledged the naming of the prostate by Herophilus, and wrote of the prostate as the ?spongy flesh at the side of the neck of the urinary bladder? (Murray).
The prostate was lost to follow up until the 16th century when Niccolo Massa a Venetian physician and anatomist is credited with the accurate identification of the prostate in 1526.
Da Vinci (1452- 1519) was not aware of the existence of the prostate. A drawing by Vesalius in 1538 in his medical treatise “De humani corporis fabrica.”, is the first known diagram of the prostate.
Jean Riolan the younger was a French anatomist (1577-1657) was the first to suggest that obstruction of the bladder could be surgically relieved through the perineum but it is not certain whether he made the association of the prostate with bladder obstruction (Deaver).
There was little medical interest in the enlarged prostate until the late 18th century.
Prostate cancer was first identified by British surgeon John Adams, and published in the “The Lancet” in 1853.
Medical science has been challenged by prostatic hyperplasia and prostatic cancer ever since. Of recent, there are multiple innovations in prostatic therapy the most sophisticated of which is robotic surgery innovated in Vancouver in 1983. The first FDA approved system used in prostatic surgery is called the da Vinci system ? an odd association since Leonardo missed the prostate despite his genius. It was developed by the US army in the hope that skilled surgeons would be able to execute complex surgery from centralized regions on wounded soldiers in geographically remote regions.
Principles
There are universal principles that govern all biological structures.
The principles of structure are in part reflected in the adjectives used to describe them including size, shape, position, character. Biological structures are made of smaller parts and are usually surrounded by a protective capsule. Structures that connect the prostate to the rest of the body include the blood vessels, lymphatics, ducts and nerves. As a biological structure the prostate undergoes changes in time that include the changes that occur in its early development and then in aging.
Biological structures function by receiving raw products, processing and producing, and then exporting products that are useful to the organism.
Disease is the alteration of structure and or function, while diagnosis aims at identifying these structural and functional abnormalities, and treatment aimed at relieving the aberrances.
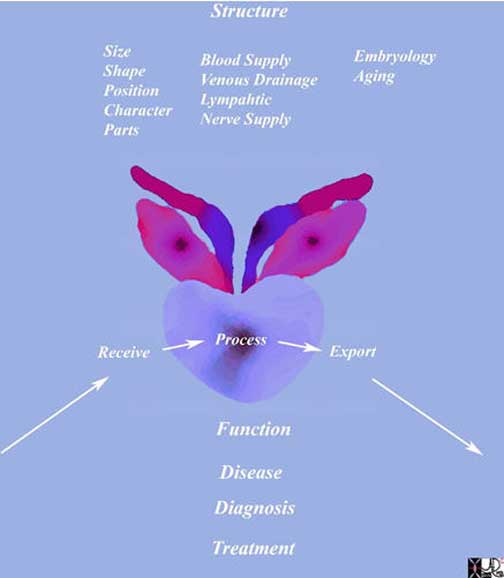
This diagram frames the underlying principles and approach to the prostate in this module. Universal structural principles include size, shape, position character and parts with connections to the rest of the body via blood vessels, nerves and lymphatics. All structures are subjects to the influences of time both in their development and in their aging process.
Physiological principles include receiving raw products processing and producing and exporting an end product.
Disease is an aberrance of structure and or function and health care providers diagnose and treat these disorders.
Courtesy of: Ashley Davidoff, M.D.
Histology
The prostate is comprised of approximately 30% glandular and 70% fibromuscular stromal elements.
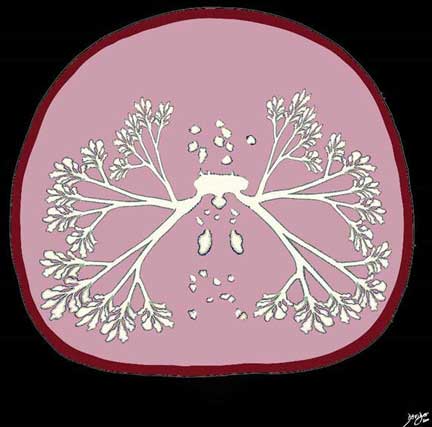
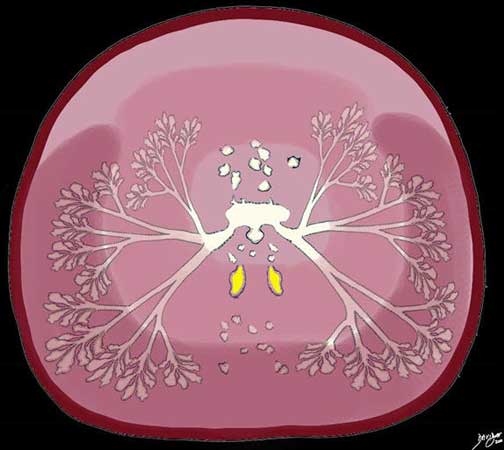
The diagram reflects the basic histological makeup of the prostate in axial projection. It is composed of 30% glandular tissue (white) and 70% stromal tissue (pink). The glandular tissue is made up of branching tubuloalveolar glands and the stroma consists of smooth muscle, collagen, elastic tissue and fibrous tissue.
Ashley Davidoff MD
There are two basic types of cells in the prostate; glandular or epithelial cells, and the stromal cells. Epithelial cells make up the glandular portion of the prostate and stromal cells make up the surrounding muscle and connective tissues. The interaction between the epithelial cells and stromal cells is relevant in the evolution of prostatic disease.
The epithelial cells take two forms;
The columnar cells are the secretory cells, and form 90% of the epithelial population. They are rich in acid phosphatase and prostate-specific antigen.
The other epithelial cell type is the basal cell which is a small, undifferentiated, keratin-rich pluripotential cell. Basal cells form less than 10% of the epithelial cell population. These cells are responsible for regeneration of the epithelium. When they are present they form a second cell layer creating a pseudostratified appearance to the epithelium.
The fibromuscular stroma consists of smooth muscle separated by strands of connective tissue rich in collagenous and elastic fibers. The muscle is scattered in the gland, and also forms a dense ring around the urethra. Muscle is also found beneath the capsule of the prostate.
The glandular elements are organized with tree like morphology and have a tubuloalveolar shape. A tubuloalveolar gland is named because it is a combination of a tube and a sphere meaning in essence that it is tear drop shaped.

The diagram reflects the histological makeup of the prostate characterised by tubuloalveolar glands reflecting their shape combining a tubular shape with a rounded shape to result in a tear drop shape. The epithelium of the glands or acini has irregular contours, and the gland is lined by a single layer of cuboidal or columnar cells. Characteristic also is the accumulation of concretions in the lumen called corpora amylacea which become calcified as the patient ages. These are shown as pink homogeneous concretions organized in layers (lamellated) in the lumen of the gland.
Ashley Davidoff MD
The epithelium or lining of the glands is cuboidal or columnar which describes the shape of the individual cells as being either like a cube or like a column. It is usually a single layer of cells thick but may look pseudostratified and two layered when basal cells are present. The mucosa forms papillary projections into the lumen giving the alveoli an irregular shape.
A characteristic feature of the glands, especially in older patient are hyaline accumulations of thickened secretions that form in layers which are found in the lumen of the acinus or gland. These lamellated concretions are called corpora amylacea. The word corpus is derived from the Latin word corpus which means a body and amylacea is from the Latin word amylum which means starch or gruel. The clinical significance of the corpora amylacea is not known. They may also be found less commonly in the pulmonary alveoli.
The glandular elements comprise of about 30 – 50 tubuloalveolar glands, which empty into 15 – 25 independent excretory ducts. These ducts open into the urethra just lateral to the verumontanum where the ejaculatory ducts enter.
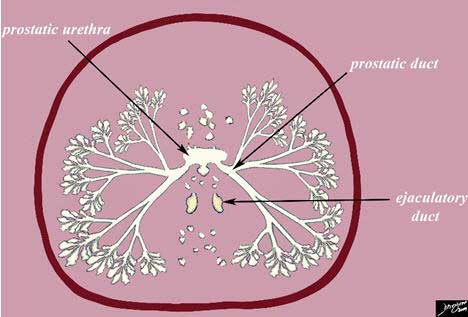
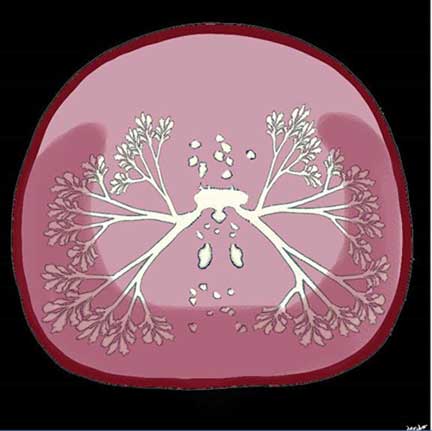
Diagram of a Whole Prostate Mount in Axial Projection
The diagram reflects the histological makeup of the prostate with compound tubuloalveolar acini feeding into a system of ductules and finally forming 30-50 excretory ducts that enter into the prostatic urethra. In this diagram the two ejaculatory ducts are shown posterior to the prostatic urethra, and represent the confluence of the ducts of the seminal vesicles and the vasa deferentia. At a slightly more inferior level of the axial cut, they will enter the prostatic urethra at the verumontanum. Courtesy: Ashley Davidoff, M.D.
The largest component of stroma cells is the smooth muscle contribution. The smooth muscle cells are rich in actin and myosin. The smooth muscle is required for release of seminal secretions during ejaculation. The second major component of the stroma is fibroblastic tissue. The fibroblasts are rich in vimentin and fibronectin, and provide structural support to the gland.
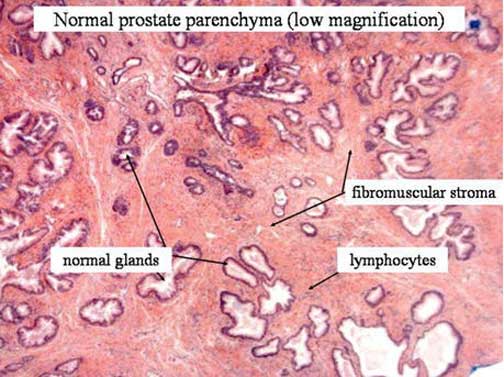
The H&E histological specimen is taken at low power and shows the components of the prostatic gland including the glandular tissue, and fibromuscular stroma. In general the glandular tissue comprises 30% of the tissue and the fibromuscular component comprises 70%. Courtesy: Alex Perepletchikov, M.D.
Carcinoma of the prostate develops from the epithelial cells, but the interaction with the stromal cells is relevant to the prognosis and characteristics of prostate cancer.
BPH develops from the complex interactions between epithelial and stromal cells.
Testosterone interacts with both cell types.
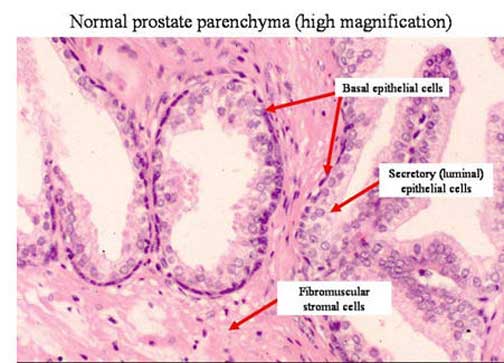
The H&E histological specimen is taken at higher magnification and shows the cellular components of the epithelium. The basal cells are seen with darker nuclei and the secretory columnar cells are seen facing the lumen. The stroma is noted in between the glands consisting of smooth muscle and collagen. Courtesy: Alex Perepletchikov, M.D.
Anatomy Introduction
The prostate is rather unique among exocrine glands since it is the only exocrine gland that occupies a symmetrical central location in the body. The pancreas has both endocrine and exocrine function and is centrally placed, but its parts are eccentrically positioned with less of the gland on the right and more of the gland on the left side of the body.
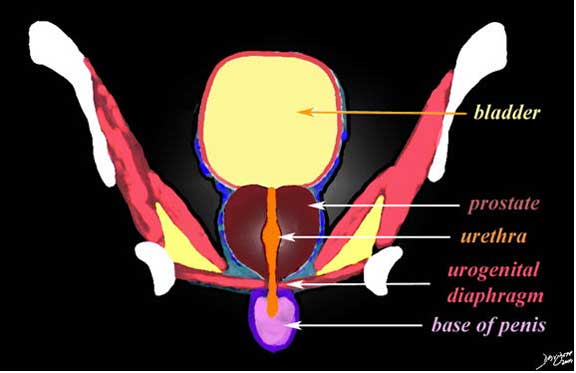
Central Position between the Bladder and the Penis
The diagram reflects the basic anatomy of the chestnut shaped prostate lying in the deep pelvis between the bladder above and the urogenital diaphragm below and surrounded by the obturator internus and levator ani muscles and the inferior aspect of the ischium and pubic bones. The prostatic urethra runs through the prostate and connects the bladder with the penile urethra. Courtesy: Ashley Davidoff, M.D.
If one were to show the non inquisitive person the prostate gland of a bull, he or she might ask – “What is that?” The easiest answer would be – “It is a bull’s prostate,” and that could suffice as an answer. If on the other hand the same prostate was shown to a curious minded, or analytically minded person, they may counter with ?How do you know?” or “Why is it a prostate?” The answer, based on the knowledge of the structure would include describing its unique and characteristic size, shape, position, and character. We may also speak to its parts, and its relationships to other structures its connections to other biological structures, how it changes with time and different cyclical events. The manner with which it functions in vivo would be its physiological characteristics.
The descriptors we used above are universal descriptors that can be applied to all biological structures whether it is the bull?s prostate, the glial cell of the brain or the pancreas of a mountain rat. We can use these descriptors to describe the cell, a tissue, an organ in both health and disease. We can also use these descriptors for clinical findings such as an enlarged prostate felt on transrectal examination that feels hard, nodular, soft, or rubbery.
Advancing the Structural Detail
The size of prostate is smaller than one would imagine. It has been compared to a small kiwi fruit, small plum, an almond and a chestnut. In fact, after a small experiment involving the purchase of these fine fruits and nuts it was found that the chestnut was closest in size in all dimensions.
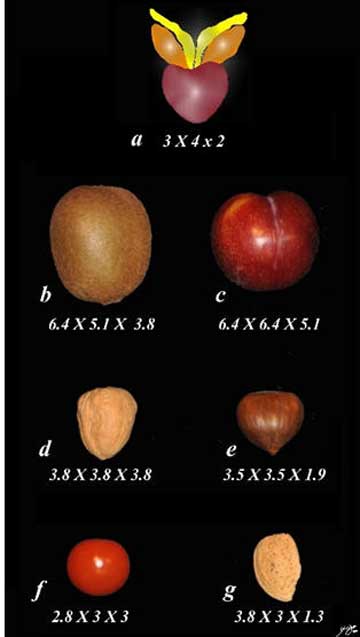
By virtue of its small size, it does not allow it to store large amounts of secretions. A normal prostate gland weighs about 20g-30g in a 30-year-old male. The normal volume is between 20-30 ccs. The prostate normally measures 3 cm in length (height), 4 cm in width (transverse), and 2 cm in depth (anteroposterior dimension).
It remains relatively stable in size until the age of 50 when increasing weight of the gland is observed. By the age of 80, the average prostatic weight is 35-45g.
Advancing the Structural Detail : Prostate Volume Calculation
A simple prorated, ellipsoid formula is commonly used to calculate prostate volume: (anterior-posterior diameter) x (transverse diameter) x (superior-inferior diameter) x ?/6 (approximately 0.52) is accurate and reproducible.
From a practical point of view in imaging the gland is usually enlarged if the transverse dimension is greater than 4cm.
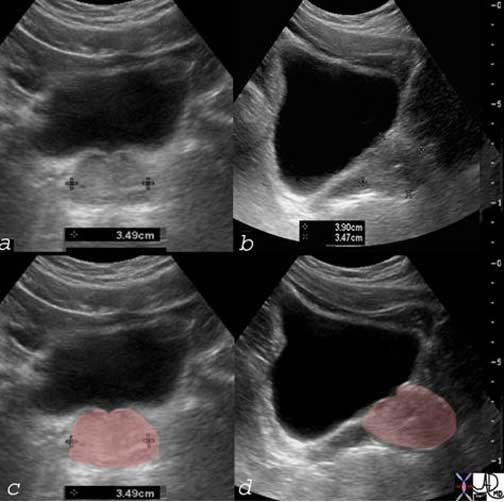
The volume of this gland is calculated by the formula using a simple prorated ellipsoid formula. Thus, transverse diameter of 3.5cm is multiplied by A-P dimension of 3.5cm by the craniocaudal dimension of 3.9cm and then by a correction factor of .52. This calculation reveals a volume of 25cc, which is normal. Courtesy: Ashley Davidoff, M.D.
Applied Biology

Benign Prostatic Hyperplasia (BPH)
The 70-year-old male shows an enlarged prostate 7.2cm in A-P by 6.1cm. in the axial plane. The gland is enlarged based on these measurements. Two distinct zones are identified because the gland is abnormal. The posterior zone is canoe shaped is hypodense and represents the peripheral zone. The anterior region is more hyperdense layer and is combination of zones including the central zone, transition zone and the anterior fibromuscular layer. In this patient who has benign prostatic hyperplasia (BPH) the transitional zone is enlarged due to the hyperplasia. Courtesy: Ashley Davidoff, M.D
Shape
The prostate has been likened to many structures including a cone, a chestnut, a walnut and a heart.
In the A-P projection it is seen as a cone-shaped organ with apex directed inferiorly and base in contact with the bladder superiorly.
Common Descriptors of the Prostate
The diagram reflects a normal chestnut shape of the prostate (maroon overlay) seen in the coronal plane. It could also be seen as a heart, a top, a cone, or an acorn.
The bladder (yellow above), lies superiorly and rests on the base of the prostate ( maroon), which in turn has its apex resting on the pelvic diaphragm. The prostatic urethra (orange) traverses the middle of the prostate. Courtesy: Ashley Davidoff, M.D.
The prostate has anterior, posterior, and lateral surfaces. The anterior surface is rounded, the posterior surface is slightly flattened and the lateral surfaces rounded as well. This shape fits quite accurately with the chestnut as well.
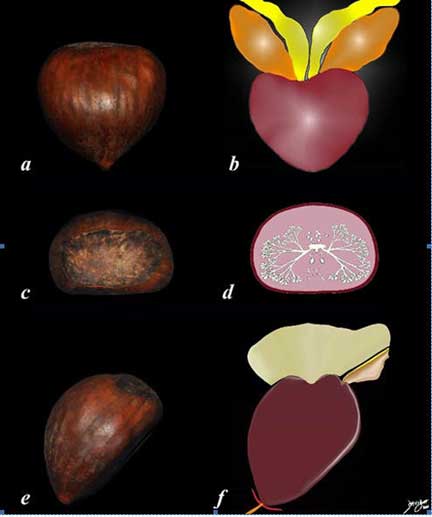
In the transverse dimension the prostate is seen at some levels as heart-shaped.

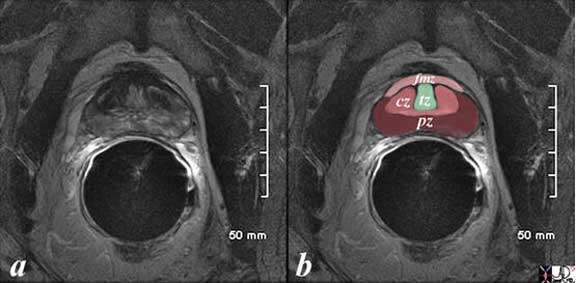
The patient is a 60-year-old man. His MRI was performed with a transrectal coil and the image shows the T1-weighted sequence in the axial projection (a,b). The scan shown demonstrates the normal heart shape of the prostate at this level in the axial projection. Zonal anatomy cannot be distinguished on T1 sequences, since the T1-weighted sequence results in a homogenous signal from all the zones. Courtesy: Ashley Davidoff, M.D.

The CT scan reconstructed in the sagittal plane is from a patient with an enlarged prostate (yellow arrows). The borders become rounded best seen on the superior borders. The superior aspect of the gland protrudes with two symmetrical homogeneous components likely representing an enlarged transitional zone caused by hyperplasia. The matrix of the gland is heterogeneous The bladder wall is thickened anteriorly confirming outlet obstruction. Courtesy: Ashley Davidoff, M.D.
Advancing the Structural Detail : Position
The term prostate is derived from Greek- prostates, which means ?one who stands before”, “protector”, “guardian” owing to its position relative to the bladder although it appears that Herophilus who named the organ implied that it lay before the testes.
It is cradled by the urinary bladder, and fits snugly between the bladder and the membranous and penile urethra. It provides passage both for urine, and semen but also acts as the mixing pot for semen, where the ingredients come together.
The prostate sits between the internal and external sphincters that control the urinary stream. At the bladder neck the detrusor muscle of the bladder becomes confluent with the internal sphincter while smooth muscle of the anterior fibromuscular zone contributes to the internal sphincter as well. On the inferior side, the external urethral sphincter is formed from skeletal muscle from the inferior aspect of the fibromuscular layer and the participation of the perineal membrane. The external sphincter surrounds the membranous urethra and the beginning of the penile urethra. Thus, it is interesting as well that the anterior zone of the prostate contains smooth muscle superiorly and skeletal muscle inferiorly. It shares this unique characteristic of having both smooth muscle and skeletal muscle with the esophagus.

The diagram reflects the position of the prostate (maroon overlay) and surrounding structures as seen in the coronal plane. The bladder lies superiorly and rests on the base of the prostate (maroon), which in turn has its apex resting on the pelvic floor. The prostatic urethra (orange) traverses the middle of the prostate. The prostate is immediately surrounded by the capsule and periprostatic venous plexus (blue tubular structures). The levator ani and obturator internus muscles with the ischiorectal fossa and components of the ischium and pubic bones form the inferolateral border on either side. The urethral sphincter acts as the inferior border, below which is the membranous urethra, the base of the penis and penile urethra. Courtesy: Ashley Davidoff, M.D.
Advancing the Structural Detail : Sagittal Projection
The anterior and posterior relationships of the prostate are appreciated in this projection. The prostate lies immediately behind the pubic symphysis. Between the prostate and the pubic symphysis is the retropubic space of Retzius in which the anterior venous plexus of Santorini is positioned.
Posteriorly, the Denonvilliers’ fascia is found and is made up of a combination of posterior prostatic and anterior rectal coverings. As we have noted in the coronal projection the prostate sits on the perineal membrane. The urethra runs through it, and extends through the membrane, after which it changes direction to enter the shaft of the penis. This change in direction of the urethra is best appreciated in the sagittal projection. Posterolaterally, the prostate is cradled between the levator ani muscles.

The CT scan reflects a normal prostate seen in the sagittal plane. The bladder is distended. Note the position of the prostate posterior to the pubic symphysis and anterior to the rectum (black bubble) covered posteriorly by Denonvillier?s fascia. Superiorly, it supports the bladder base and inferiorly it is supported by the genitourinary (pelvic diaphragm). The bladder is overlaid in yellow and the urethra is the channel overlaid in orange. Courtesy: Ashley Davidoff, M.D.
Advancing the Structural Detail : Applied Biology
The ideal route for examining the prostate is via the rectum, whether one is performing a digital examination or imaging with ultrasound or MRI, due to the proximity of the two organs.
The relationship to the prostate and the urethra is also intimate. When the transitional zone of the prostate enlarges due to hyperplasia it obstructs the urethra resulting in partial obstruction clinically manifesting in a progressively reduced force of the urinary stream. Post void residual increases and the patient then needs to void more frequently. In addition during micturition the bladder muscle tires as it tries to expel the full volume of urine but recovers a short time thereafter (a few seconds) and the patient usually will void an additional small volume after the short rest period. This clinical syndrome resulting from bladder obstruction is called prostatism or more recently referred to as LUTS ? lower urinary tract symptoms.
Advancing the Structural Detail : Character
The character of the prostate is based on its feel on palpation. On clinical examination, the normal prostate gland is described as being smooth, elastic and “rubbery”. Galen described it as that ?spongy flesh at the side of the neck of the urinary bladder?. Abnormalities of the prostate felt on direct clinical examination are nodules, induration, bogginess or fluctuance.
Ultrasound
The prostate gland on ultrasound is almost isoechoic and the gains have to be finely tuned on the ultrasound equipment in order to bring out the subtle differences in the texture of the gland and the surrounding tissue.
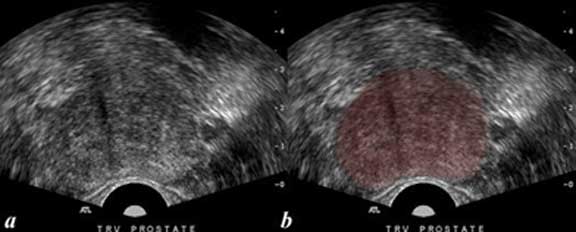
The transrectal transverse view of the prostate shows a normal sized prostate almost homogeneous in texture with echogenicity being isoechoic and very similar to surrounding tissue. The distinction between the peripheral zone, transition zone, central zone and fibromuscular layer is not obvious on this image ad is usually difficult to distinguish. Image b represents an overlay of the prostate to accentuate the position of the prostate. Courtesy: Ashley Davidoff, M.D.
Computed Tomography (CT)
The normal prostate has non specific features on CT scan and demonstrates soft tissue density similar to the muscle surrounding it. The distinction between the various zones of the prostate usually cannot be appreciated on the normal gland.

The CT scan is from a 26-year-old male with a normal prostate seen in the axial plane (a, b). Note the shape of the gland in the transverse plane is heart shaped and it is homogeneous in texture. Courtesy: Ashley Davidoff, M.D.
Magnetic Resonance Imaging (MRI) Characteristics
MRI is the imaging modality that best characterizes the prostate. The T2-weighted sequence optimizes the distinction between the peripheral, central, transitional zones and the anterior fibrous layer.

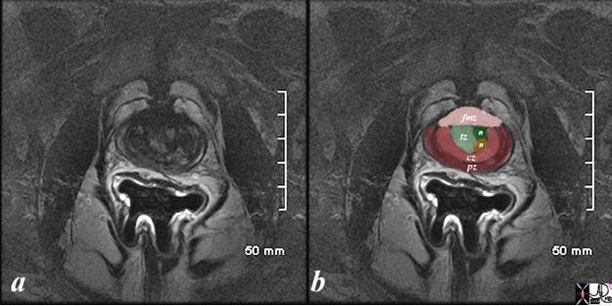
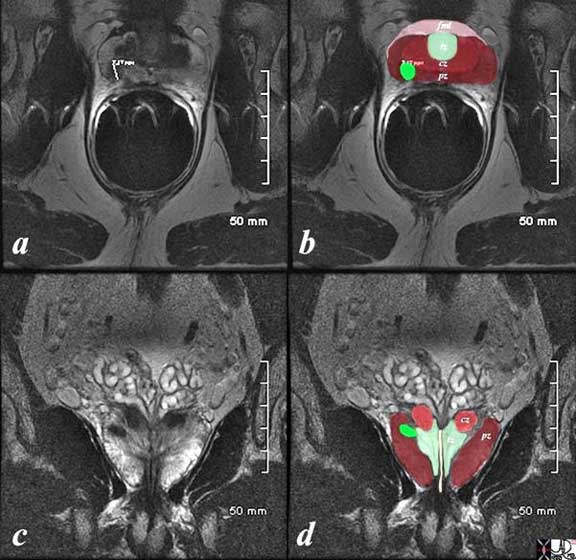
The patient is a 60-year-old man. His MRI was performed with a transrectal coil and the image shows the T2-weighted sequence in the axial projection (a, b). The peripheral zone (pz), central zone (dark pink, cz) the transitional zone (light green), and the fibromuscular zone (light pink, fmz) ? are easily distinguished. The glandular elements in the peripheral zone make this zone T2 bright. The presence of fibrous tissue and muscle in the central zone and anterior fibromuscular layer make them dark on T2. The elements in the transitional zone make them bright on T2-weighted imaging. Courtesy: Ashley Davidoff, M.D
Parts
The parts that make up the extremes of the prostate as we have previously outlined are called the base and the apex. Because the superior aspect of the prostate is broader it is called the base and the since the inferior aspect is pointed aspect is called the apex. Note that the same orientation and nomenclature applies to the heart.
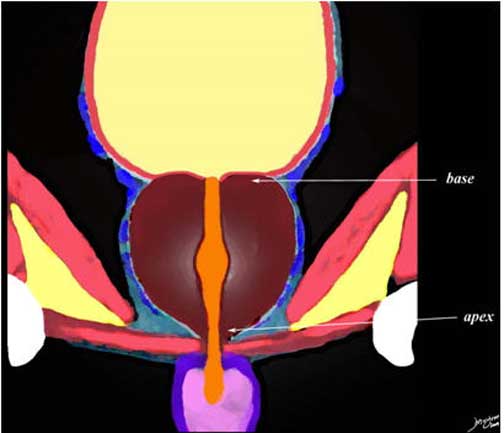
The diagram reflects a normal prostate (maroon overlay) seen in the coronal plane. The base of the prostate is that part of the prostate that lies superiorly and the apex is inferior. The bladder (yellow above), lies superiorly and rests on the base of the prostate ( maroon), which in turn has its apex resting on the pelvic diaphragm. The prostatic urethra (orange) traverses the middle of the prostate. Courtesy: Ashley Davidoff, M.D.
The prostate has anterior, posterior, and lateral surfaces. The anterior surface is rounded, the posterior surface is slightly flattened and the lateral surfaces rounded as well.
The internal parts of the prostate that contribute to the zonal anatomy have embryological, histological and pathological significance. Each zone participates uniquely to the functioning of the gland.
The prostate appears morphologically simple on the outside but is complex internally at both the macroscopic and microscopic levels. The current concepts of its morphology have only evolved since 1968 after the work of McNeal. He suggested that the prostate was composed of three concentric zones that surround the prostatic urethra, and a fourth anterior zone.
The zones of the prostate include the central, peripheral and transition zones as well as an anterior fibromuscular layer.
The peripheral zone accounts for approximately 70%, central zone 20%, the transition zone about 5% and the anterior fibromuscular layer (zone) about 5%.
In the 19th century the prostate was seen as having 4 lobes; 2 lateral lobes, a middle lobe and an inconstant anterior lobe. In 1912 an inconstant posterior lobe was added by Lowsley.
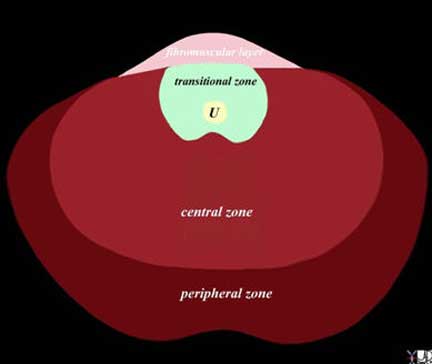
The prostate gland can be viewed as having 4 major zones. In the young adult male the outer zone called the peripheral zone, accounts for 70% of the parenchyma. Inward of the peripheral zone is the central zone that accounts for 20% of the parenchyma. The periurethral zone is called the transitional zone and fibromuscular layer (anterior layer) share the remaining 10% of parenchyma. Courtesy: Ashley Davidoff, M.D.
Parts: Zones
The peripheral zone is the outermost layer of the gland and comprises of the mostly glandular tissue. It has simple glands and loose stroma. It is the site of origin of adenocarcinoma of the prostate.
The diagram reflects the basic histological makeup of the prostate in axial projection and the distribution of about 70% of the glandular tissue in the peripheral zone (maroon overlay). Courtesy: Ashley Davidoff, M.D.
The central zone has both glandular elements and ductal elements and characteristically surrounds the ejaculatory ducts and stromal elements. The epithelial cells are slightly different and are composed of tall columnar cells with eosinophilic cytoplasm, and prominent basal cell layer.
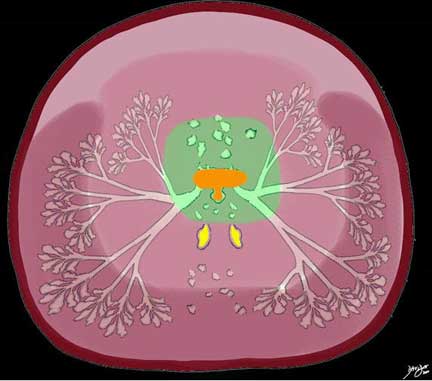
The diagram reflects the basic histological makeup of the prostate in axial projection with a focus on the central zone (intermediate pink). The glandular elements are a minor component of this zone and they are different in nature compared to the epithelial elements of the peripheral zone, while the stromal elements are more prominent in this region functioning as the required force for expulsion of secretions during ejaculation. The central zone incorporates the ejaculatory ducts (yellow). Courtesy: Ashley Davidoff, M.D.
The transitional zone surrounds the urethra and contains the ductal system that eventually terminates in the periprostatic urethra. It is the innermost layer of the prostate and is the region where benign prostatic hyperplasia (BPH) originates.
The diagram reflects the basic histological makeup of the prostate in axial projection and the focus of this diagram is on the transitional zone which contains the periurethral region, consisting of tissues of ductal and stromal origin but devoid of significant glandular tissue. It contains the prostatic urethra (orange) and the small posterior diverticulum like structure off the urethra called the prostatic utricle. Hyperplasia in the transitional zone will impinge on the urethra and result in the symptoms of prostatism usually due to BPH. Courtesy: Ashley Davidoff, M.D.
The anterior zone is composed of fibromuscular stroma. This zone, comprising almost one third of the prostate mass, though of a lesser volume, contains smooth muscle, some skeletal muscle and has no glandular elements.

The diagram reveals the prostate in sagittal view. The peripheral zone is the largest portion and occupies the base, extending the entire length of the posterior wall to the apex. The central zone lies inward of the peripheral zone and is that part through which the ejaculatory duct courses. The transitional zone surrounds the urethra, and the anterior fibromuscular layer runs from the base to the apex anteriorly. The ureter is overlaid in orange and the ejaculatory duct empties into the widened portion of the urethra called the verumontanum. Courtesy: Ashley Davidoff, M.D.
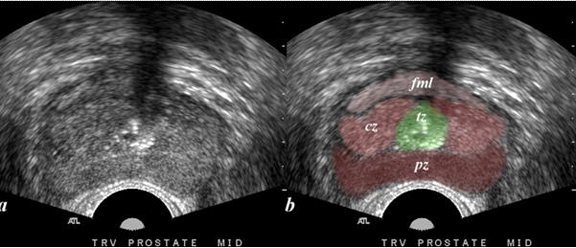
The transrectal transverse view of the prostate shows a normal sized prostate almost homogeneous in texture with echogenicity being isoechoic and very similar to surrounding tissue. The distinction between the peripheral zone (maroon pz), transition zone (green tz), central zone (salmon pink cz) and fibromuscular layer (light pink fml) is shown in image b. The zonal anatomy is better appreciated on MRI. Courtesy: Ashley Davidoff, M.D.
This image was described above in the ?character section but is repeated in the context of the parts of the gland. PZ = peripheral zone, CZ = central zone, tz = transitional zone and fmz = fibromuscular zone or fibromuscular layer
Courtesy: Ashley Davidoff, M.D.
The prostate contributes to both the structure of the internal and external sphincter. The anterior fibromuscular layer contributes smooth muscle to the internal sphincter and skeletal muscle from the inferior aspect of the anterior fibromuscular zone, and is part of the external sphincter. The internal sphincter is under autonomic control while the external sphincter is under voluntary control.
Parts: Applied Biology
When palpating the prostate during digital rectal examination, the most prominent part is the peripheral zone. It is the most common site of prostate cancer.
Benign prostatic hypertrophy/hyperplasia originates in the transitional zone and may also be palpable during digital rectal examination.
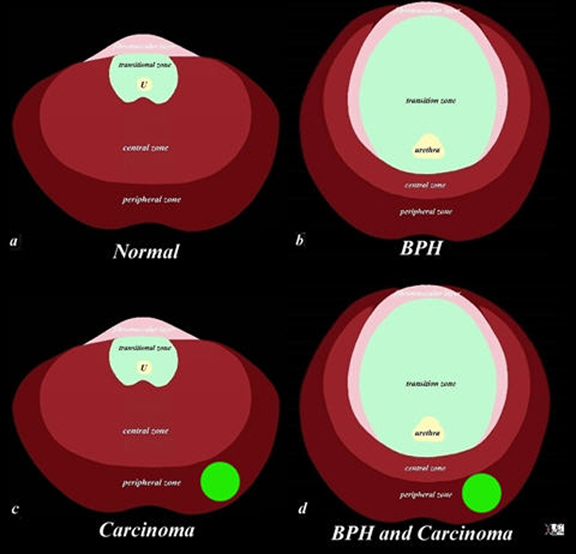
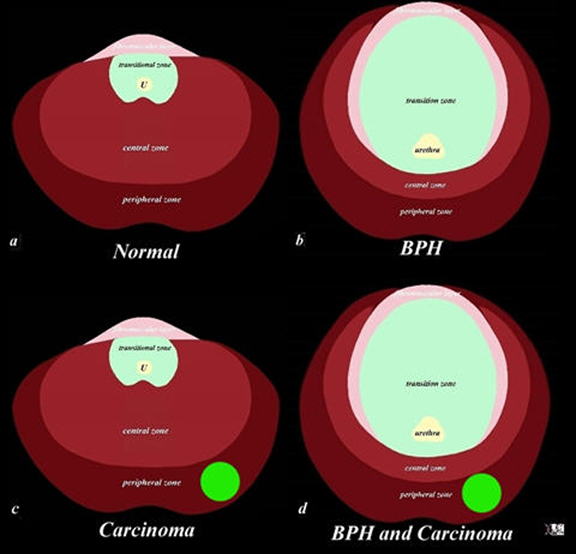
The diagram depicts the zonal morphology relevant to the locations where disease arises. The normal gland is seen in image (a). Image (b) shows BPH (benign prostatic hypertrophy) which is caused by hyperplasia and enlargement of the transitional zone. Image (c) shows carcinoma (bright lime green) arising from the peripheral zone which is the characteristic site of origin of this disease. Image (d) shows a combination of BPH in the transitional zone and carcinoma in the peripheral zone. This is a common combination of diseases in the elderly population.
Courtesy: Ashley Davidoff, M.D.
The patient is a 61-year-old man. His MRI was performed with a transrectal coil and the image shows the T2-weighted sequence in the axial projection (a, b). The scan shown demonstrates the normal zonal anatomy of the prostate but shows early enlargement of the transitional zone with two nodules participating in the expansion (n in b).
Courtesy: Ashley Davidoff, M.D.

The patient is a 61-year-old man with primary prostate carcinoma. His MRI was performed with a transrectal coil. T2-weighted images in the coronal projection (a, b), axial projection (c, d), and sagittal projection (e,f) are shown. The primary lesion is a 8mm lesion (bright green overlay in b, d, f) is hypointense on the T2-weighted image and noted in left sided peripheral zone (pz darker maroon b, d, f). Other zones noted include central zone (lighter red, cz, in d) transitional zone (pale green,white arrow, tz, in d) and fibromuscular layer (light pink, fbl in d). The urethra is shown in yellow in the middle of the tz in d. The lesion was biopsied and shown to be an adenocarcinoma of the prostate. Courtesy: Ashley Davidoff, M.D.
Parts: Capsule
The prostate is surrounded by a firm fibrous capsule that is structurally composed of collagen, elastin, and smooth muscle. These fibers blend with the fibers of the puboprostatic ligament, anchoring the prostate to the posterior aspect of each of the pubic bones. The capsule itself lies within the sheath for the endopelvic fascia, which surrounds it laterally, anteriorly and posteriorly. Under this capsule are circularly oriented smooth muscle fibers and collagen-rich tissue that surround the urethra. The prostatic capsule is not present at the apex (inferiorly) where it transitions into the external sphincter, and is also absent at its base superiorly, where it transitions into the detrusor muscle of the bladder.
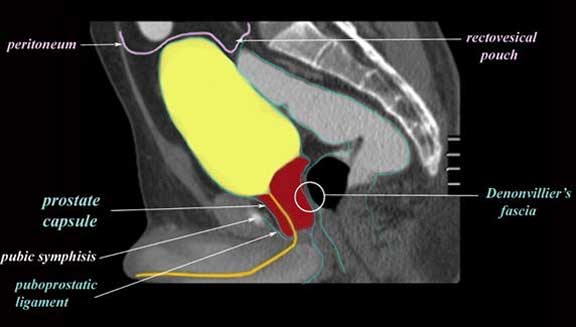
The CT scan reflects a normal prostate (maroon overlay) seen in the sagittal plane. The bladder, prostate and the rectum are all extraperitoneal and are therefore not covered by peritoneum. Their covering is via a capsule which is common to the bladder and prostate (blue overlay). The rectum has its own covering that fuses with the posterior covering of the prostate to form Denovillier?s fascia (aka rectoprostatic fascia, or the rectovesical septum). The bladder is distended. (yellow overlay) The base of the prostate that abuts the bladder is free of a capsule as is the apex. Courtesy: Ashley Davidoff, M.D.
Functionally, the capsule provides a protective barrier to the prostate. In addition, smooth muscle elements aid in the expulsion of prostatic secretions.
When prostate cancer spreads beyond the capsule it carries a poorer prognosis. Nevertheless, as the prostatic capsule is poorly defined at the apex and base, determining extension beyond the capsule at these levels makes this evaluation a challenging problem for the pathologist.
Treatment is rarely focused on the capsule itself, though attempt is made to resect the prostate with the capsule intact so that pathologic examination can determine if the disease is confined within the borders of the capsule.
Parts: Connections of the Prostate
The connections of the prostate to the rest of the genitourinary tract and the rest of the body are via the ducts vessels and nerves. The ductal systems are confluent in the prostatic urethra, its blood supply is via the anterior branch of the internal iliac artery along with the cystic artery, venous drainage via the cystic veins, and lymphatics via the iliac system. Parasympathetic and sympathetic systems connect it to the autonomic system, while the hormonal control is via dihydrotestosterone (DHT).
Parts: Ducts of the Prostate
The lower genitourinary system has dual responsibility for the transport of urine and semen. Urine is the product of the kidneys and semen is the product of the testes, seminal vesicles, prostate and bulbourethral glands (aka Cowper?s glands).
The sperm and fluid from the seminal vesicle are transported via the paired ejaculatory ducts into the verumontanum, which is a mound of tissue in the middle of the prostatic urethra. The prostatic fluid is brought to the urethra by 15-20 ducts.

The diagram reflects the ductal systems involved in the urogenital tract including the ureteral orifices that empty into the bladder, the prostatic urethra (bright orange) which is the receptacle of both urinary and seminal contents, orifices of the ejaculatory ducts that are the confluence of the seminal vesicle and the vas deferens, the 15-20 orifices of the prostatic ducts, and finally the small orifices of the ducts of Cowper?s gland which empty into the region of the penile urethra.
Courtesy: Ashley Davidoff, M.D.
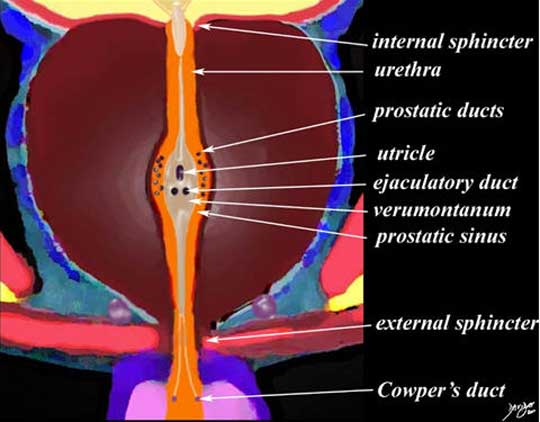
The diagram reflects a magnified view of the ductal systems involved in the urogenital tract including the internal urethral sphincter, the prostatic urethra (bright orange) orifices of the ejaculatory ducts that lie on the verumontanum, and the 15-20 orifices of the prostatic ducts that lie in the prostatic sinus a type of gutter on the sides of the veru. At the distal end is the external sphincter and finally the small orifices of the ducts of Cowper?s gland which empty into the region of the membranous urethra. The utricle is a small blind ending pouch which is the male equivalent of the uterus. Courtesy: Ashley Davidoff, M.D.
The ejaculatory ducts are a paired system that forms by the confluence of the duct of the seminal vesicle and vas deferens. They enter into the prostatic urethra in the verumontanum just below the prostatic utricle (when present).
Parts: Prostatic Urethra
The prostatic urethra is part of the urinary system, structurally characterized by its position in the anterior part of the prostate surrounded by the transitional zone. It is widest in its midportion where the confluence of prostatic ducts, ejaculatory ducts and prostatic utricle are concentrated. It is a multifunctional conduit for the transport of urine and semen, and in fact is the mixing pot where the major ingredients of semen are combined. The prostatic urethra forms semen from three main structures that include the seminal vesicles, vasa deferens and prostate.
Blood Supply
The primary blood supply of the prostate comes from the prostatic artery which is a branch of the inferior vesical artery which is s a branch (direct or indirect) of the anterior division of the internal iliac artery. Some accessory vessels to the prostate are supplied from the middle hemorrhoidal (rectal) and internal pudendal arteries.

The diagram shows the blood supply to the prostate coming off a branch of the anterior division of the internal iliac artery. Courtesy: Ashley Davidoff, M.D.
Venous Drainage
Structurally, the venous drainage of the prostate is through the prostatic plexus. The plexus surrounds the prostate like a net and joins the venous drainage of the penis (deep dorsal vein) in Santorini’s plexus.
The periprostatic plexus consists of the anterior plexus called Santorini?s plexus that lies behind the pubic symphisis in the retropubic space of Retzius and the paraprostatic plexus called the pudendal plexus (vesicoprostatic plexus) which drains both the inferior aspect of the bladder as well as the prostate.
The diagram reflects shows the prostate and bladder with the lateral venous plexuses outlined in blue. They combine with the venous plexus that lies anteriorly in the space of Retzius as well as Batson?s plexus to finally drain into the iliac and azygos systems. Courtesy: Ashley Davidoff, M.D.
The usual drainage of the prostate is via the internal pudendal vein which drains into the anterior branch of the internal iliac vein. The plexus however does collateralize with the external pudendal vein which drains into the external iliac system, and the vertebral venous system or Batson?s plexus, which is the valveless system that drains the spinal cord and vertebral column. The intervertebral veins and the epidural venous plexus, collateralize at all levels of the spinal canal and vertebral bodies and also drains into the azygos system. Thus venous drainage goes three ways; internal iliac, external iliac, and azygos via the collateral systems of Santorini?s plexus, vesicoprostatic plexus and Batson?s plexus.
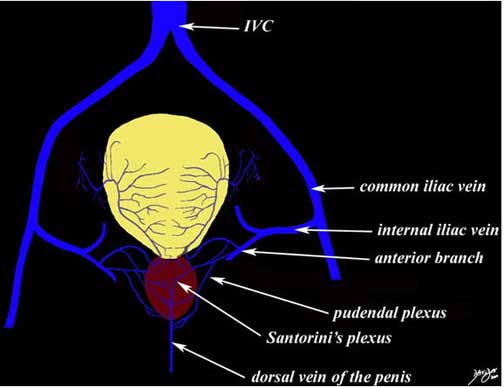
The diagram reflects the venous drainage of the prostate which is in common with the venous drainage of the penis and bladder. The dorsal vein of the penis divides into two forms a plexus anterior to the bladder called the pre prostatic plexus of Santorini. This plexus collateralizes with the pudendal (paraprostatic ) plexus that lies on the lateral aspects of the prostate . The veins finally drain into the anterior branches of the internal iliac venous system via the internal pudendal vein. Courtesy: Ashley Davidoff, M.D.
Blood Supply: Applied Anatomy
Diseases, such as infection and cancer may spread through the venous drainage to the distant organs.
Radiation seeds, used in the treatment of prostate cancer, may also embolize through the venous drainage system either via the iliac or via the azygos system.
The most usual method is via the internal iliac system and into the IVC and then pulmonary circulation.

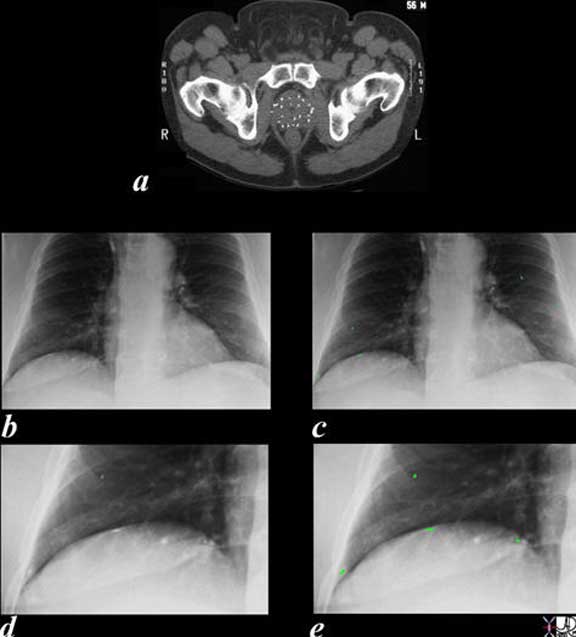
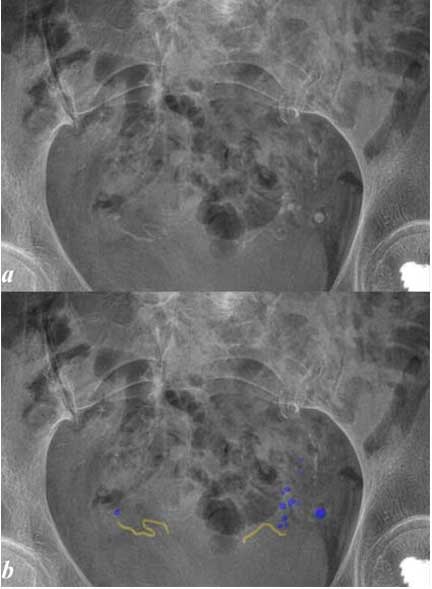
56-year-old male with prostate carcinoma has radiation seeds implanted into the prostate gland. A chest X-ray following the procedure shows at least 4 of the seeds in the base of the right lung and 2 of the seeds in the mid left lung field. An azygos lobe is of incidental note. In the image below the small embolized seeds are overlaid to allow recognition. Courtesy: Ashley Davidoff, M.D.
It is not unusual for metastatic prostate cancer to affect the vertebral column and it does this by it connection with Batson?s plexus which is the valveless system that drains the vertebral bodies and the cord.
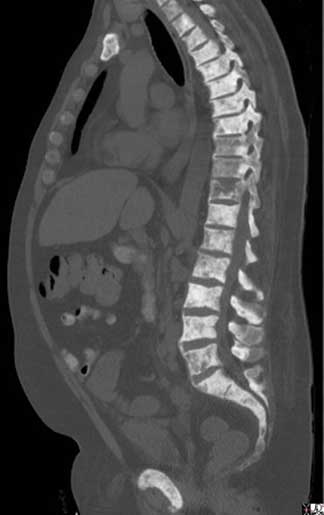
The sagittal reconstruction of the thoracic and lumbar spine is from a 50-year-old male with known prostate carcinoma shows extensive blastic metastases involving almost all the visualized bones including the entire spine, pubic symphisis and probably sternum. The findings are consistent with extensive blastic metastasis from primary prostate carcinoma.
The spread of carcinoma from the prostate to the spine is enabled by the valveless venous system of Batson that is within and surrounds the vertebral column and shares venous drainage with the prostate. Courtesy: Ashley Davidoff, M.D.
The venous plexus is of particular importance in treatment during radical prostatectomy, when division of the dorsal venous complex can result in significantly increased risk of blood loss.
Phleboliths or calcifications within the prostatic veins are common in older patients and may be seen on CT. They have no clinical significance other than causing some difficulties in differentiating ureteric stones from phleboliths.
Courtesy: Ashley Davidoff, M.D.
Lymphatic Drainage
Lymphatic drainage from the prostate is via the internal iliac, sacral, vesical, and external iliac nodes.

The lymphatic drainage from the prostate is accommodated by the external iliac nodes, internal iliac nodes which will both drain to the common and paraaortic systems.
Courtesy: Ashley Davidoff, M.D.

The series of US and CT scans are from a 50-year-old man with an elevated PSA Image (a) is a transverse ultrasound showing a minimally prominent nodular prostate. Image (b) shows the needle tip (teal blue arrow) in the left peripheral zone. Image (c) is a transverse image of the prostate showing a nodular anterior surface while image (d) shows an almost 3 cm external iliac node. The biopsy was positive for prostate carcinoma.
Courtesy: Ashley Davidoff, M.D.
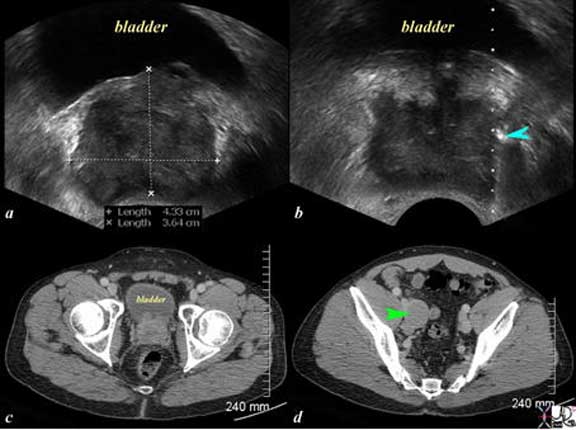
The CT scan of the pelvis is from a 88-year-old man with known prostate carcinoma. Image (a) and (b) are through the bladder (yellow) showing the abnormal prostatic gland (green) which is growing toward the left side. A stent (solid white tube traverses the prostate and a second tube with hollow center represents the tip of a Foley catheter in the bladder. The seminal vesicles (pink) are seen posteriorly as symmetric structures except for mild compression of the left by the tumor. Image (c) and (d) reveal an almost 2 cm left internal iliac node through which the stent passes as well. Its size and participation in the obstruction of the left ureter is incriminating. Courtesy: Ashley Davidoff, M.D.

The Bone scan and CT scan is from a 77-year-old man with known prostate carcinoma. Image a shows multiple hot spots in the ribs consistent with blastic metastatic bone disease. Image b shows extensive lymphadenopathy (green arrows) in the retroperitoneum of the upper abdomen surrounding the ureters resulting in early mild hydronephrosis. . Image c shows a recurrent peritoneal mass (green arrow). These findings are consistent with metastatic prostate carcinoma in the peritoneal cavity, retroperitoneal nodes, and ribs.
Courtesy: Ashley Davidoff, M.D.
Nerve Supply
The autonomic nervous system helps to control the function of the prostate gland. The parasympathetic division of the autonomic nervous system regulates erection, whereas ejaculation is triggered by sympathetic impulses (Ventura).
The hypogastric nerve (sympathetic) join the pelvic splanchnic nerves (parasympathetic S2-S4) to form the pelvic plexus.
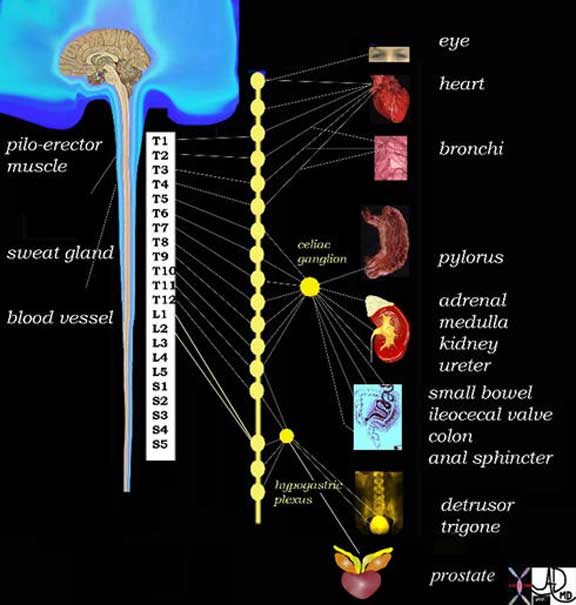
The diagram reveals the sympathetic nervous system of the body and in this instance attention is drawn to the innervation of the prostate by the inferior hypogastric plexus, with contributions of L1 and L2.
Courtesy: Ashley Davidoff, M.D.
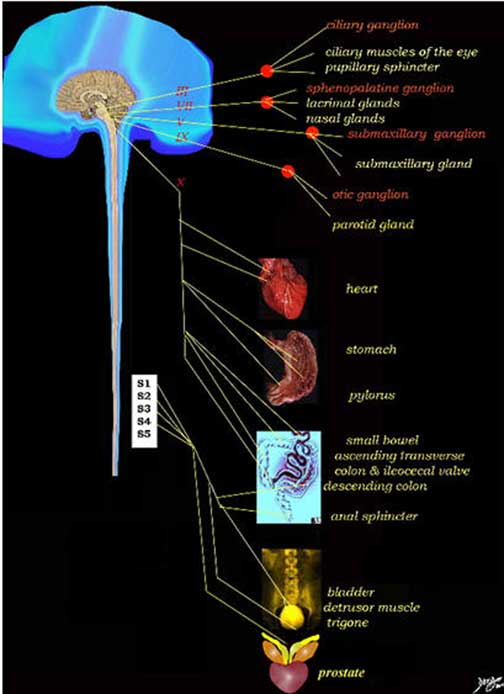
The diagram reveals the parasympathetic nervous system of the body and in this instance attention is drawn to the innervation of the prostate by the pelvic splanchnic plexus formed from the nerves of S2, 3 and 4.
Courtesy: Ashley Davidoff, M.D.
During prostatectomy, the portions of the hypogastric plexus that go to erectile tissues of the penis pass through the prostatic plexus. If these nerves are sacrificed, impotence can develop.
Embryology
The prostate is derived from the urogenital sinus. The prostate develops as 30-50 distinct glands which grow in confluence and gradually fuse. These tubuloalveolar glands originate from the uroepithelium and grow into the surrounding wall of the developing urethra and enlarge. After birth, the size of the prostate remains relatively unchanged for 10-12 years, until puberty. Increased production of androgens stimulates an increase in gland size.
The prostate will attain a mass of approximately 20 grams by the end of puberty, which will again remain stable for several decades.
The prostate first appears during the third month of embryonic development. Five epithelial buds form in a paired manner on the posterior side of the urogenital sinus on both sides of the verumontanum, and they then invade the mesenchyme to form the prostate. The top pairs of buds form the inner zone of the prostate and appear to be of mesodermal origin; the lower buds form the outer zone of the prostate and appear to be of endodermal origin. This is of potential importance since the inner zone gives rise to benign prostatic hyperplasia (BPH) tissue, whereas the outer zone contains the primary origin of cancer. Much of the development, growth, invasion, budding, and branching are genetically controlled and influenced by dihydrotestosterone, which is produced from testosterone in the urogenital sinus. By its 4th month, the fetal prostate is well-developed.
Developmental Abnormalities
Developmental abnormalities are rare. Aplasia and hypoplasia represent incomplete development. This is usually due to a deficiency of androgen production. Cystic changes may occur proximally or distally or in neighboring structures. These changes may lead to infertility but are otherwise asymptomatic. Mesonephric remnants represent incomplete obliteration of these primordial embryological structures.
Aging
At birth the prostatic acini are lined with squamous epithelia.
Stimulation of further development of the gland is dependent on maternal steroids, namely estrogens. As the levels of these hormones decrease, an involutional phase ensues during the first 5 months. Large transient surges of serum androgen, estrogen, and progesterone normally occur very early in postnatal life. This is usually between 2 to 3 months of age. At this time, levels may reach upward of 60 times normal prepubertal levels, approaching adult serum testosterone levels.
The prostate increases rapidly in size at puberty. During the fifth decade, it starts to show the effects of aging either resulting in atrophy but more commonly hyperplasia.
The artistic rendition is of the normal prostate enlarging with time most commonly due to hyperplasia of the transitional zone. The diagram shows the normal cone shaped gland in maroon in the center with the ductus deferens (yellow) and seminal vesicles. The normal prostate is about the size of a kiwi fruit usually weighs between 20-30 gms and has a maximum transverse diameter of 4cms, but can double in size.
Courtesy: Ashley Davidoff, M.D.
The prostatic age is the period in a mans life when he starts to experience the clinical manifestations of the aging prostate which in the past was called prostatism but is now referred to as lower urinary tracts symptoms (LUTS). These symptoms include frequency, urgency, hesitancy, poor emptying, nocturia, and dribbling.

The CT scan is from a 70-year-old patient with an enlarged prostate. The anterior aspect of the gland protrudes with two symmetrical homogeneous components likely representing an enlarged transitional zone and prostate hyperplasia though by the nature of the disease the combination of cancer and BPH commonly coexist. The urinary bladder wall is minimally thickened.
Courtesy: Ashley Davidoff, M.D.
The CT scan reconstructed in the sagittal plane is from a patient with an enlarged prostate (yellow arrows). The borders become rounded best seen on the superior borders. The superior aspect of the gland protrudes with two symmetrical homogeneous components likely representing an enlarged transitional zone caused by hyperplasia. The matrix of the gland is heterogeneous The bladder wall is thickened anteriorly confirming outlet obstruction. Courtesy: Ashley Davidoff, M.D.
Function
This diagram frames the underlying principles and approach to the prostate in this module. Universal structural principles include size, shape, position character and parts with connections to the rest of the body via blood vessels, nerves and lymphatics. All structures are subjects to the influences of time both in their development and in their aging process.
Physiological principles include receiving raw products processing and producing and exporting an end product.
Disease is an aberrance of structure and or function and health care providers diagnose and treat these disorders.
Courtesy of: Ashley Davidoff, M.D.
The prostate is present in all mammals and its function, though still not completely understood, has importance in reproductive physiology. The most obvious function is to participate in the production of semen, but it also has a function in the ejaculatory process by acting as a mechanical pump, and acts as a one way conduit for the semen by clamping off the internal sphincter and opening the external sphincter during ejaculation. Interestingly, it also participates in the pleasurable feeling of the orgasm, with its female counterpart, the Skene?s glands which are purportedly considered the erogenous G spot that brings pleasure to the female during sexual intercourse. Skene?s glands lie lateral to the female urethra.

The prostatic urethra serves as the mixing pot for the components of semen by acting as the receptacle of secretions from the prostate itself, the seminal vesicles and the vasa deferentia. This artistic rendition shows the region of the verumontanum which is the site where the mixing pot stands receiving sperm from the testes via the vasa deferentia (red), the secretions of the seminal vesicles (orange) and the secretions of the prostate gland (white). The last component contributed by the bulbourethral glands (Cowpers?s glands – green) joins the secretions in the penile urethra to form semen. Courtesy: Ashley Davidoff, M.D.
The process of ejaculation and the transport and life cycle of semen is a marvel and we will take you through this chronologically.
Function: Show Time
The components of semen are continually produced and during intercourse the seminal vesicles, seminiferous tubules, and prostatic glands are overflowing with their products.
The diagram below by da Vinci exemplifies coitus.

Preparation for the Event

In this diagram the function of the prostate is shown as a mysterious organ acting as a melting pot of the love potions. It depicts the ?pot? receiving contributions from 3 sources ? sperm from the testes, breathed into the pot by the alchemist, fluid from the seminal vesicles emanating from the crooked palms of the alchemist, and prostatic secretions entering the brewing pot from the side. Cowper?s glands (shocking pink) add a drop into the mix in the region of the membranous urethra to complete the formation of semen. This diagram has been used above but the ?hotting up? just prior to ejaculation is depicted in the reds and oranges.
Courtesy: Ashley Davidoff, M.D.
As the climax is approached the three major organs that produce the semen are all revved up and in full production, and finally ejaculation takes place.
During ejaculation the anterior fibromuscular zone of the prostate plays its part by assisting in closing the internal sphincter with smooth muscle, thus prevents the forward flow of urine into the ejaculate and preventing the ejaculate from going backward into the bladder. The anterior fibromuscular zone also assists in opening the external sphincter using the skeletal muscle allowing the gate to open for the semen to be released. Lastly by contractions of the fibromuscular layer in the central zone the prostate helps to expel the semen.

The diagram reveals the process of ejaculation when the sluice gates open under sympathetic control and semen is transported from the prostatic urethra to the penile urethra and finally exiting with ecstasy through the meatus. The upper sphincter is closed and the lower sphincter is open. The smooth muscle of the central zone of the prostate participates in the ejaculation process by contracting forcing the semen into the urethra. The prostate and urethra are depicted as a wine glass with the prostate depicted in the cup and the penile urethra as the stem.
Courtesy: Ashley Davidoff, M.D.
The prostate, in addition, participates at a higher level in that it enhances the pleasurable sensations during orgasm.
This is an artistic rendering of the prostate in action delivering the magical fluid to the front door of the female. Courtesy: Ashley Davidoff, M.D.
The initial ejaculate is a heterogeneous mixture. The first portion of the ejaculate, about 1-2% of it, is made up of secretions from the Cowper (bulbourethral) and Littre glands that lubricate the urethra and buffer any acidic urine than may be present in the urethra. The second portion derives from the prostate and contributes from 15% to 30% to the ejaculate. It is a milky white to gray in color. Thereafter, sperm from the testes via the vasa deferentia (2-5%) follow and, finally, the contribution of the seminal vesicles, which accounts for the majority of the ejaculate (65-70%), arrives. The normal PH of semen is between 7.05 and 7.8 and normal sperm count should be more than 20 million per mls and is usually closer to more than 40 million per ml and even up to 250 million per ml. It boggles the mind to think of the number of ?hopefuls? looking for the one Miss Right, and only one of which will be successful.

The diagram reveals the components of semen which contains fluid from the seminal vesicles accounting for 65-70% of the volume, prostatic fluid ? 25-30%, sperm 2-5%, and fluid from Cowper?s gland which represents less than 1% of the volume. Each ejaculate contains between .1-10mls (1-2 teaspoons) with an average of 3.5mls). Courtesy: Ashley Davidoff, M.D.
1-2ccs of prostatic fluid is secreted in the urine per day in the absence of ejaculation.
The vaginal environment is acidic (PH about 4), and as such is a protective environment for the vagina against bacteria. On the other hand sperm are also sensitive to the acid environment. Nature has solved this problem by creating a two step process in the safe delivery of sperm. The first step is the deliver the sperm in coagulated form and protected from the acid, and the second step is to liquefy the coagulated form and free the sperm into a safe environment.
Function: Chemical Components of the Prostatic Secretion
The prostate gland produces and stores a fluid that has a high buffering capacity when mixed with other components of semen. The PH of semen is close to body PH and is used to buffer the acidity of the vagina ensuring a safer chemical environment for the sperm which survive longer and have greater motility within the environment of prostatic secretions (Owen).
As the PH is buffered the chemical environment becomes safer for the sperm.
The prostate is also responsible for the production of many other components that comprise semen. It is a milky fluid contains acid phosphatase, citric acid, inositol, calcium, zinc, and magnesium. Enzymes, such as proteases, esterases, phosphatases, prostate specific antigen, amylases, pepsinogen and hyaluronidase are also present.
The concentration of citric acid in prostatic secretion is the highest found in the body (Kandeel) by an order of 100 times. This latter fact adds one more mystery about the prostate. One hypothesis is that the citrate serves to chelate calcium and thus aids the PSA enzyme in liquefying the coagulated semen that initially forms and attaches itself to the cervix.
The presence of zinc from the secretion presumably is an antiseptic. When the semen initially enters the vagina it clots, which glues the semen and trapped sperm to the cervix. The PSA enzyme will lyse this clot and releasing the sperm which will find their way into the uterus and then the Fallopian tube.
The semen coagulates due to a fibrinogen like agent secreted by the seminal vesicles. The semen is also sticky allowing it to become adherent to the cervix. The sperm needs temporary cocoon type protection from the acidic environment of the vagina. The sperm are housed in the coagulum and are nourished by other components of the semen eg fructose produced by the seminal vesicles.

The diagram depicts the white creamy sticky and coagulated ejaculate adherent to the cervix. Once the acidic environment of the vagina is buffered, the ejaculate liquefies and the sperm can be released. Citric acid from the prostatic component of the secretion chelates calcium and assists the prostate specific antigen enzymes in liquefying the semen.
Ashley Davidoff MD
Following ejaculation and formation of the coagulated semen, between about 5-20 minutes is needed for liquefaction to occur that will allow the release of the sperm. This period allows the PH of the acidic vaginal environment to be buffered by the semen in order for the sperm survive.
Liquefaction occurs as a result of proteolytic enzymes within the prostatic secretion that include pepsinogen, amylase, hyaluronidase and prostate specific antigen. The citric aid as stated appears to assist the process by chelating calcium.

The diagram depicts the liquefaction of the coagulated ejaculate now becoming a pale cream releasing the 40-250 million sperm that have one mission in mind ? the race to glory and fertilization of the ovum. With artistic license the diagram amplifies ?free at last? and then the race, showing the sperm storming the gate of the external os of the cervix, – through the cervical canal and then into the wide open space of the endometrial canal and looking for the appropriate tiny opening of the Fallopian tubes where fertilization will finally take place.
Courtesy: Ashley Davidoff, M.D.
The prostate is unique as an androgen-receptor expressing organ in that it remains sensitive to androgens throughout life. This occurs through a process of differential gene expression known as imprinting and may be of importance in the development of benign prostatic hyperplasia (BPH).
Diseases
The most common diseases that affect the prostate are benign prostatic hyperplasia (BPH) and prostate carcinoma. Prostate cancer is the most commonly diagnosed cancer in men and the second leading cause of cancer death in men second to lung cancer. Prostate hyperplasia is an aging phenomenon that can give rise to significant morbidity in the aging male. Prostatitis and prostatic abscess are two other relatively common diseases.
The diagram depicts the zonal morphology relevant to the locations where disease arises. The normal gland is seen in image (a). Image (b) shows BPH (benign prostatic hyperplasia) which is caused by hyperplasia and enlargement of the transitional zone. Image (c) shows carcinoma (bright lime green) arising from the peripheral zone which is the characteristic site of origin of this disease. Image (d) shows a combination of BPH in the transitional zone and carcinoma in the peripheral zone. This is a common combination of diseases in the elderly population.
Courtesy: Ashley Davidoff, M.D.
Diseases: Prostate Carcinoma
Prostate carcinoma is a malignant disease usually originating in the secretory cells of the prostate glands. It is the most commonly diagnosed cancer in men and the second leading cause of cancer death in men second to lung cancer.
Tumors of the prostate are estimated to be found in about half of the men in their 70’s and almost all men in their 90’s. The incidence of prostate cancer differs among different ethnicities. The incidence is highest among African Americans and lowest among Asian Americans.
Structurally, it can present with a focal thickening in the peripheral zone, along with irregularities in the prostate contour.
Functionally, there is limited impairment, and diagnosis is often made incidentally or during screenings.
Complications include early spread to the regional nodes and spread to distal areas, such as the skeleton.
Clinically, the patient is usually asymptomatic with localized disease. With progression patients may experience bony pain, urinary symptoms from obstruction, or hematuria. Survival rates vary depending on how aggressive the disease is at the time of diagnosis.
The diagnosis is suspected by digital rectal examination (DRE) showing a nodule or induration, as well as and elevated serum prostate specific antigen (PSA), but is often found incidentally at autopsy. As such it is a highly heterogeneous disease with varying degrees of impact on morbidity and mortality. Biopsy is the gold standard for diagnosis. It is believed that screening has played a significant role in reducing mortality from prostate cancer. Screening utilizes various measurements of PSA levels.
From an imaging standpoint, ultrasonography can reveal a hyperechoic, hypoechoic, or isoechoic nodule or region. Endorectal T2-weighted MRI may be more specific. CT is of little use in the diagnosis of the primary disease, though contrast-enhanced CT may demonstrate enhancement in tumors. It is best used in the evaluation of nodal disease and systemic spread. Bone scintigraphy is sensitive and useful for the evaluation of osseous metastases.
Treatment of prostate cancer depends on several factors, namely the grade and stage of the tumor, life expectancy of the patient, and the ability to ensure disease-free survival. Surgical treatment provides the only opportunity for cure and is indicated in the presence of aggressive disease (Gleason 7-10), and is dependent on the age at diagnosis. Gleason 6 is considered by many to be non-operative but should undergo close surveillance. The role of neoadjuvant therapy prior to surgery is indicated in patients with T3 disease, followed by external beam radiotherapy. If a resection results in positive tumor margins, adjuvant radiotherapy may also be indicated.

The diagram depicts the zonal morphology relevant to the locations where disease arises. The peripheral zone, accounts for 70% of the parenchyma and is the site of origin of 90% of the patients with adenocarcinoma of the prostate (bright lime green).
Courtesy: Ashley Davidoff, M.D.

The patient is a 61-year-old man with primary prostate carcinoma. His MRI was performed with a transrectal coil. T2-weighted images in the coronal projection (a, b), axial projection (c, d), and sagittal projection (e, f) are shown. The primary lesion is a 8mm lesion ( bright green overlay in b, d, f) is hypointense on the T2-weighted image and noted in left sided peripheral zone (pz darker maroon b, d, f). Other zones noted include central zone (lighter red, cz, in d) transitional zone (pale green,white arrow, tz, in d) and fibromuscular layer (light pink, fbl in d). The urethra is shown in yellow in the middle of the tz in (d). The lesion was biopsied and shown to be an adenocarcinoma of the prostate.
Courtesy: Ashley Davidoff, M.D.
The patient is a 60-year-old man with primary prostate carcinoma. His MRI was performed with a transrectal coil and T2-weighted images in the axial projection (a,b) and coronal projection are shown. The primary lesion is a 8mm lesion ( bright green overlay in b and d) is hypointense on the T2-weighted image (a, b) and noted in the right sided of the peripheral zone (pz darker maroon). Other zones noted include central zone (lighter maroon, cz, in b, d) transitional zone (pale green, tz, in b, d) and fibromuscular layer (light pink, fbm in b) The lesion was biopsied and shown to be an adenocarcinoma of the prostate.
Courtesy: Ashley Davidoff, M.D.
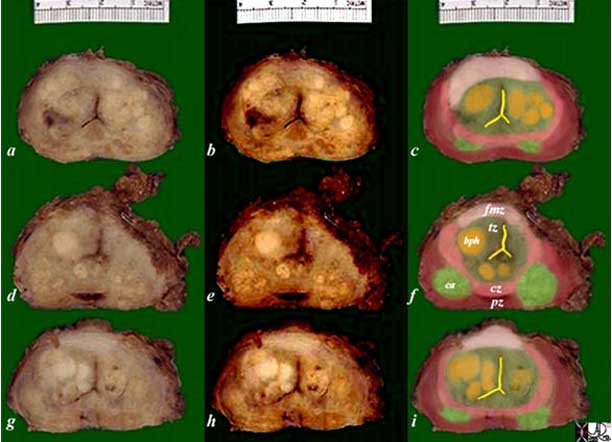
The pathology specimen is from a patient with prostate carcinoma and benign prostatic hyperplasia.
The gland shows multifocal heterogeneous nodules and it is difficult to differentiate a benign from neoplastic component based purely on the macroscopic appearance.
The image is organized into 3 columns reflecting the original images in the first column (a, d, g) the second column in which the contrast is increased to bring out differences in character (b, e, h) and the last column where the interpretation of the diseases is overlaid on an approximation of the zonal anatomy (c, f, )
The peripheral zone is overlaid in maroon and labeled pz in image (f).
The central zone is overlaid in dark pink and is labeled cz in image (f)
The transitional zone is overlaid in darker green and is labeled tz in image (f)
The anterior fibromuscular zone is overlaid in light pink and labeled fmz in image (f)
Carcinoma lesions are overlaid in bright lime green and are situated in the peripheral zone. They are seen as tan-white ill-defined nodules.
BPH nodules are overlaid in yellow and tend to be in the transitional zone. BPH nodules usually demonstrate tan-yellow (glandular hyperplasia) and tan-gray (stromal hyperplasia) macroscopic appearance.
Image Courtesy Alexander Perepletchikov, MD PhD
Diseases: Prostate Specific Antigen (PSA)
PSA or Prostate Specific Antigen plays a role in liquefying the semen that is formed after ejaculation. It has a half biologic half-life of approximately 2-3 days.
There is considerable debate regarding the role of PSA in screening for prostate cancer. PSA can be elevated in a variety of situations, including prostate cancer, BPH, and prostatitis. The sensitivity of PSA is about 80%, but the specificity of PSA in detecting prostate cancer is only 65%.
Diseases: Metastasis
Prostate metastasis spreads primarily by contiguous spread locally via lymphatic vessels to regional lymph nodes, as well as hematogenously to distant sites. Initially spread to distant sites is mostly within the axial skeleton. In later stages of disease spread to the lungs, liver, and kidneys may also occur.
Regional Spread
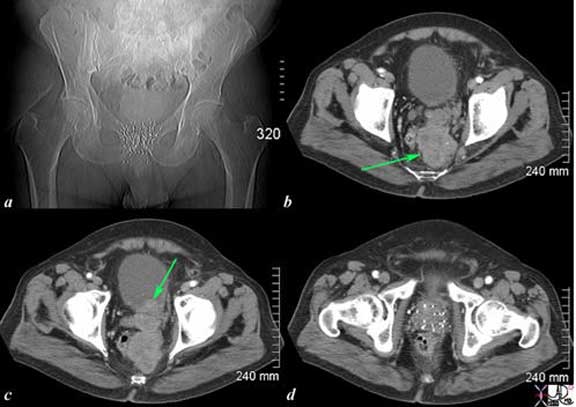
The CT scan of the pelvis is from an 76-year-old man with known prostate carcinoma treated with implanted radiation seeds. Image (a) shows multiple radiation seeds within the prostate gland Image (b) (light green arrow) shows an irregular heterogeneous mass measuring about 5cm extending above the treated field and progressing posteriorly to the presacral space. Image (c) shows the same mass as (b) extending into the base of the bladder (green arrow). Image (d) shows multiple prostatic seeds in the prostate gland. These finding are consistent with prostate carcinoma treated with implanted radiation seeds but with the tumor now continuing to grow superiorly beyond the confines of the treatment, and inward to the base of the bladder.
Courtesy: Ashley Davidoff, M.D.
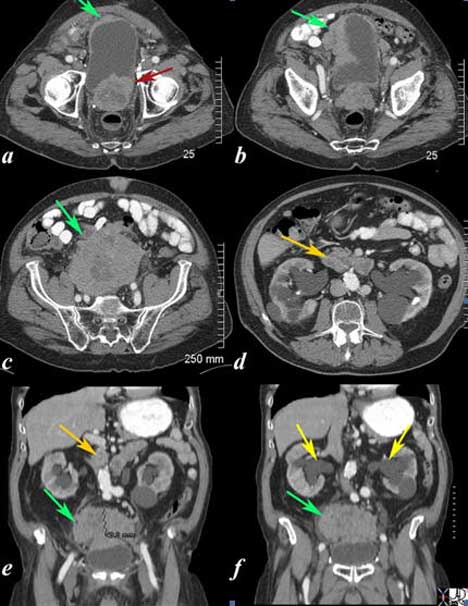
The CT scan is from a 88-year-old man with known prostate carcinoma. Image (a) shows multiple the mildly enlarged prostate (maroon arrow) with irregular margins extending to the left of the bladder but with a thickened right anterolateral wall (green arrow). Image (b) shows extensive irregularity of the superolateral wall which reflects tumor growth superior to and rightward of the bladder (see images below) (green arrow) . Image (c, e, f) shows the large mass (green arrow) which has its epicenter above the bladder. Image d and e shows lymphadenopathy (orange arrows ) anterior to the aorta resulting in hydronephrosis (yellow arrows in f). These findings are consistent with metastatic prostate carcinoma with extensive local extension above the bladder and to retroperitoneal nodes complicated by hydronephrosis.
Courtesy: Ashley Davidoff, M.D
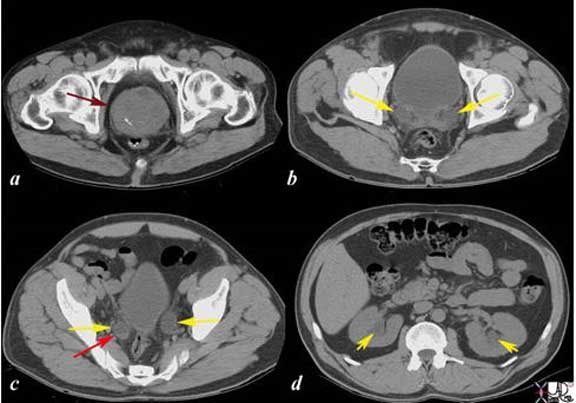
The CT scans show an enlarged prostate (a) with hydroureters (b, c yellow arrow) blood-urine level or sediment urine level (red arrow (c) with mild hydronephrosis (yellow arrows (d) These findings are consistent with obstruction of the kidneys as a result of prostatic enlargement, and in this case prostatic carcinoma.
Courtesy: Ashley Davidoff, M.D.
Diseases: Nodal metastases
The series of US and CT scans are from a 50-year-old man with an elevated PSA Image (a) is a transverse ultrasound showing a minimally prominent nodular prostate. Image (b) shows the needle tip (teal blue arrow) in the left peripheral zone. Image (c) is a transverse image of the prostate showing a nodular anterior surface while image (d) shows an almost 3 cm external iliac node. The biopsy was positive for prostate carcinoma.
Courtesy: Ashley Davidoff, M.D.
The series of US and CT scans are from a 50-year-old man with an elevated PSA Image (a) is a transverse ultrasound showing a minimally prominent nodular prostate. Image (b) shows the needle tip (teal blue arrow) in the left peripheral zone. Image (c) is a transverse image of the prostate showing a nodular anterior surface while image (d) shows an almost 3 cm external iliac node. The biopsy was positive for prostate carcinoma.
Courtesy: Ashley Davidoff, M.D.
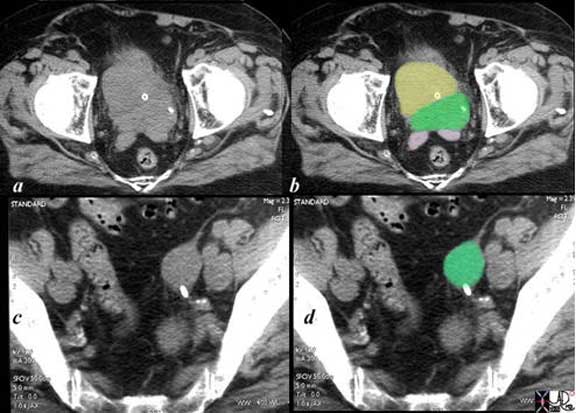
The CT scan of the pelvis is from a 88-year-old man with known prostate carcinoma. Image (a and b) are through the bladder (yellow) showing the abnormal prostatic gland (green) which is growing toward the left side. A stent (solid white tube traverses the prostate and a second tube with hollow center represents the tip of a Foley catheter in the bladder. The seminal vesicles (pink) are seen posteriorly as symmetric structures except for mild compression of the left by the tumor. Image (c) and d reveal an almost 2cm left internal iliac node through which the stent passes as well. Its size and participation in the obstruction of the left ureter is incriminating. Courtesy: Ashley Davidoff, M.D.
Metastatic Disease Bone
Spread to bones is common, and spread of disease to the bones is often monitored via bone scintigraphy. The association of a common venous drainage via the valveless Batson?s plexus, enables the early spread of the disease to the spine. While new foci of disease may be appreciated, the resulting blastic activity is not particularly effective in demonstrating a response to therapy.
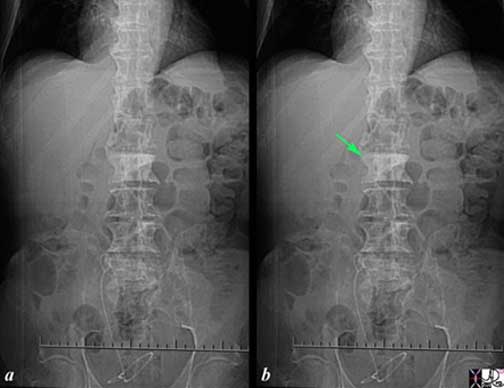
The scout film prior to a CT scan of the abdomen and pelvis shows an ivory vertebra (green arrow b) in this patient with known diagnosis of prostate carcinoma. A stent in the right urinary collecting system is likely misplaced and has the proximal portion in the right mid ureter, and distal portion coiled in the ureter. The findings are consistent with blastic metastasis of L2 from prostate carcinoma. Courtesy: Ashley Davidoff, M.D.
The sagittal reconstruction of the thoracic and lumbar spine is from a 50-year-old male with known prostate carcinoma shows extensive blastic metastases involving almost all the visualized bones including the entire spine, pubic symphysis and probably sternum. The findings are consistent with extensive blastic metastasis from primary prostate carcinoma.
The spread of carcinoma from the prostate to the spine is enabled by the valveless venous system of Batson that is within and surrounds the vertebral column and shares venous drainage with the prostate. Courtesy: Ashley Davidoff, M.D.
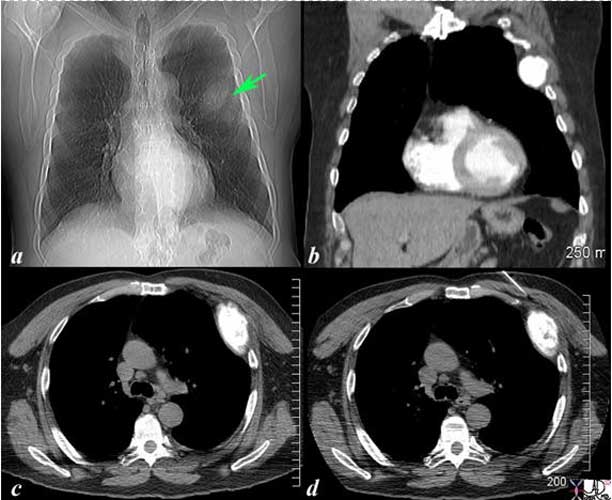
The scout film (a) of the chest prior to a CT scan shows a vague mass off the left upper chest (green arrow b) in this 68-year-old man with known diagnosis of prostate carcinoma. Image (b) is a coronal reconstruction of the chest and shows an obvious blastic lesion in the lateral aspect of one of the upper ribs, probably 5. Image (c) shows the blastic metastasis as an expanded hyperdense area. Image (d) shows a needle on its way to biopsy the rib which confirmed metastatic prostate carcinoma. The findings are consistent with blastic metastasis of a left rib from primary prostate carcinoma.
Courtesy: Ashley Davidoff, M.D.
Diseases: Benign Prostatic Hyperplasia (BPH)
Benign prostatic hyperplasia or BPH is a benign process of the prostate whose cause is uncertain, but is dependent on androgens to evolve.
Structurally, the disorder is characterized by a proliferation of the epithelial and stromal cells in the periurethral area of the prostate.
Functionally, this disorder may contribute to neurogenic changes in the bladder contractility. As a result of proliferation and hypertrophy, pressure exerted on the urethra obstructs bladder outflow. The increased filling of the bladder results in urgency. Since greater pressure is required to overcome the obstruction, incomplete voiding of the bladder is common. This elevated post-void residual leaves the bladder little additional capacity for urine produced, resulting in frequency and nocturia. As the bladder overflows, dribbling may also result.
Clinically, this process contributes to the majority of lower urinary tract symptoms in men. The long term clinical consequences of BPH are uncertain, as the natural history is poorly understood.
Imaging is not routinely performed for the evaluation of BPH, however, ultrasound and MRI are useful. Determination of prostatic size may also be estimated using digital rectal examination As it is technically a histologic diagnosis, confirmation usually requires examination of tissue from biopsy, surgery or autopsy. The greatest impact of BPH is on quality of life, related to urinary symptoms, and thus severity is most usefully measured using the American Urological Association Symptom Index (AUASI), developed in 1992. This is a questionnaire of 7 questions pertaining to urinary symptoms, i.e. frequency, urgency, hesitancy. Alternatively, urinary flow rates, and measurements of Prostate Specific Antigen may be used as adjuncts.
Treatment may span from pharmacologic, such as androgen deprivation therapy, minimally invasive surgical therapy, and transurethral resection of the prostate (TURP). Medical therapy includes alpha adrenergic blockers that inhibit smooth muscle contraction and relax prostatic smooth muscle and smooth muscle of the bladder receptors causes relaxation of smooth muscles in the bladder neck and prostate.
Benign Prostatic Hyperplasia (BPH): Diagnosis
A general approach to evaluation of the prostate is that the first line of diagnosis is usually physical examination, via the digital rectal examination. An experienced practitioner can characterize the various zones, and their composition, in addition to a gross assessment of size, shape, and symmetry.
Prostate specific antigen levels is a blood test that aids in the diagnosis of prostate cancer.
The most important disease processes where imaging is used as an aid is in prostate cancer. Although no imaging modality is reliable in diagnosing or ruling out malignancy, imaging serves as an adjunct in the diagnosis and staging.
Biopsy is performed with ultrasound guidance. MR, usually with the aid of endorectal coils and transrectal ultrasound are useful in staging local disease.
Clinical Examination
A normal prostate gland feels smooth and “rubbery”. Abnormalities of the prostate felt on DRE are nodules, induration, bogginess or fluctuance.
Benign Prostatic Hyperplasia (BPH): Labs
Urine analysis to look for hematuria or signs of infection.
BUN and Creatinine level to look for ureteral obstruction.
PSA is controversial because it lacks specificity to detect prostate cancer, however in combination with a physical exam it is still the best test we have to screen for prostate cancer.
Voided sample after prostatic massage to look for prostatitis
Benign Prostatic Hyperplasia (BPH): Imaging
The most important disease processes where imaging is used as an aid is in prostate cancer. Although no imaging modality is reliable in diagnosing or ruling out malignancy, imaging serves as an adjunct in the diagnosis and staging.
Biopsy is performed with ultrasound guidance. MR, usually with the aid of endorectal coils and transrectal ultrasound are useful in staging local disease.
Finally CT and MR are useful in staging in the presence of nodal or distant metastases. PET-CT does not have a well-defined role in the evaluation of prostate cancer, as areas of disease do not typically have significantly elevated metabolic rates. CT is also useful in radiation treatment planning. T2-weighted endorectal MRI has the unique ability to consistently identify the zonal anatomy of the gland .
Bone scintigraphy is often useful for assessing the spread of prostate cancer to bony areas, usually within the axial skeleton.
Diseases: Conclusion
The prostate is a remarkable organ that is situated deep in the pelvis in a central location. Although it was identified and named by Herophilus (335BC -280BC) it was neglected and ignored for many centuries. With the aging population, this small, chestnut sized and chestnut shaped organ has become central to morbidity and mortality.
From a structural aspect, seminal work by Mcneal in 1988 enhanced the understanding of the embryology, histology, anatomy and disease of the gland. Functionally it is more than just an exocrine gland, since it acts as a mixing pot for the semen, inhibits backflow of the semen into the bladder, favors forward flow by opening the external sphincter, protects the sperm from acid environment of the vagina, participates in the emancipation of the sperm from its coagulated cocoon, and enhances the physical pleasure of the sexual acts? all tied up (and probably more) in this one chestnut shaped organ.
MRI has the ability to identify the zonal anatomy of the gland, but accurate and satisfying diagnosis and management of BPH and prostate cancer is elusive at this time. Many technical innovations have evolved recently including robotic surgery, but all challenged by real and potential pitfalls of removing the gland including incontinence, impotence and infertility.