
Learning Objectives
Describe the basic anatomy including the division into component parts, the normal size shape, position and character
Discuss the physiology of the thyroid
Describe the common diseases of the thyroid including thyroid cancer, hyperthyroidism, hypothyroidism, and thyroiditis
Describe the commonly used modalities for thyroid imaging, particularly in ultrasound and nuclear medicine
Introduction
The thyroid is one of the largest endocrine glands. It is located immediately inferior to the larynx and thyroid cartilage, or the ?Adam?s apple?, and anterior to and on each side of the trachea. It is an essential part of the endocrine system.
The structure of the thyroid is characterized by its highly vascular nature, bilobed, butterfly-shape, location in the neck, and its upward movement on swallowing due to its attachments to the laryngo-skeleton. It is comprised of a large number of follicles, each filled with its secretion called colloid. The follicles are lined with thyroid hormone secreting follicular epithelial cells, and surrounded by calcitonin secreting parafollicular cells (C cells), and a dense network of capillaries. It is the only endocrine organ in which the products produced are stored in an extracellular location.
As an endocrine organ, the function of the thyroid is to synthesize and secrete hormones into the blood stream. It secretes thyroxine (T4), triiodothyronine (T3) and calcitonin. The thyroxine and triiodothyronine are involved in the basal metabolic rate (oxygen consumption at rest) and are produced by the follicular cells. The calcitonin is produced by the parafollicular cells or C cells. Calcitonin reduces serum calcium, opposing the effects of parathyroid hormone. Thus, through release of these hormones the thyroid plays an important role in regulating both metabolic rate and calcium metabolism.
Common diseases of the thyroid include hyper- and hypothyroidism, thyroiditis, and cancer of the thyroid.
Thorough assessment of a patient?s family history, geographical history, and physical symptoms are key first clinical steps in diagnosing thyroid disease, since some of the disorders are hereditary, some related to iodine content in the soil where people live and grow their own crops, and some to radiation exposure. Laboratory tests for serum levels of thyroid-stimulating hormone (TSH) and nuclear scintigraphy, a tissue-specific imaging technology, are also useful in confirming cases of under or over active thyroid. Diagnosis of thyroid cancer requires additional measures, including ultrasound imaging and needle biopsy.
Treatment for hyperthyroidism includes medication, radioisotope therapy, and surgery. While hypothyroidism is easily treated with a lifelong regimen of hormone replacement therapy, Grave?s disease, an autoimmune hyperthyroid state is treated with antithyroid medication, radioactive iodine and surgery, and thyroid cancer almost always involves surgery.

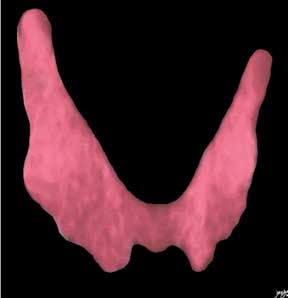
The artistic rendition of the thyroid reveals an almost butterfly-shaped structure. The lobes form the bulk of the tissue and the isthmus that lies between the two lobes may be broad and high but is usually relatively narrow in the anteroposterior dimension. Courtesy: Ashley Davidoff, MD

The coronally reformatted CT scan of the neck has been artistically rendered and demonstrates a normal thyroid in a 26 year old female. The lobes of the thyroid are not necessarily symmetrical as demonstrated in this example and if asymmetric, the right lobe is usually the larger. Courtesy: Ashley Davidoff, MD
As A Biological Unit
The thyroid, like any organ, is simultaneously a distinct biological unit, the sum of many smaller biological units, but also part of a larger physiological whole. As such, it is an indispensable component of the endocrine system and the body.
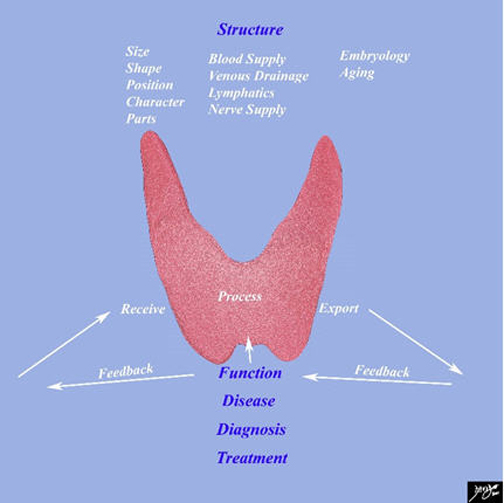
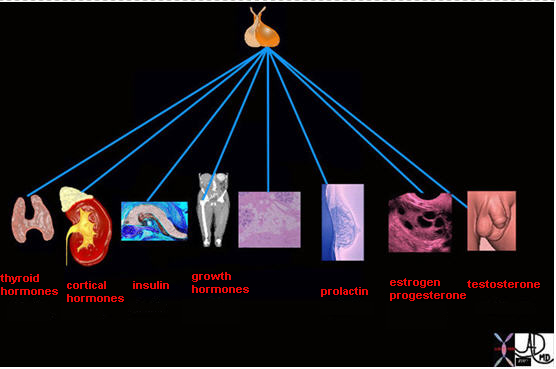
The diagram frames the underlying principles and approach to the thyroid in this module with tenets that are common to all the organs and cells of the body. Its functions are based on its ability to receive and process a raw product, and produce and export a product that has value to the body. When there is disorder of structure and/or function, disease results and the role of medical disciplines is to diagnose and treat the disorders.
Courtesy: Ashley Davidoff, MD
The elements of any organ are rooted in its structure and function, and the module defines the principle elements that govern these two disciplines in the thyroid. Structure is described most commonly by the size, shape, position, character and parts of the organ and also by the elements that connect the organ to other structures including the blood vessels nerves and lymphatics.
The thyroid is but one part of the endocrine system, yet a very central one. Basal metabolic rate, the fire that keeps the body warm and functioning, is an essential component of body function. Without the thyroid, metabolism would be at a standstill. Fortunately, its main function is executed through one type of hormone that can easily be replaced.
These principles are true to the thyroid and true to all the organs of the body. These principles are innately obvious but dogged attention to principles when issues become complex is key to solving the complex problems. The ?devil? therefore from this vantage point is in the principles and also of course in the ?detail?.
Units to Unity
One cell is no cell, and one organ is no organ. This implies that although the individual parts are important, they are nothing unless they combine forces to form something bigger and more powerful than the individual parts.
The cells as separate biological units need to combine forces in order to produce hormones in sufficient quantity in order to be effective. A thyroid cell isolated in the abdominal cavity producing T3 has no functional effect, no matter how hard it works and no matter how talented it is. A genius artist painting in isolation that he or she puts in the closet has no value to the community, and as such cannot ?sell? the ?goods?, and as such cannot survive.
The organization of the cells into acini, groups of cells that are factories of production, allow the cells to build strength in numbers and cohesive effort. The factories of acini in turn need to combine forces to form lobules, and the lobules in turn need to form lobes and eventually form the organ that has the power of number to be effective. As each unit builds, the organization gets bigger and stronger and as long as everybody pulls their weight, and has their eye on the bigger picture (welfare of the body at large) health and orderly pleasurable living can proceed. One part of the puzzle still needs to be added however in order for this to work ? links and connections of the organ to the bigger whole.
Links and Connections
The factories of production need to have input from the outside as to how hard to work, how much to produce and where and how to get the product to the end user. This is executed through connections to the transport systems including the circulatory and lymphatic systems but also the control systems that include endocrine and nervous systems. Circulatory connections deliver raw products, transport processed products, and remove waste. Hormonal connections via the neurohormonal axis of the pituitary and chemical receptors on and in the cells connect it to the chemical milieu of the body and allow the thyroid to have its finger on the pulse meeting supply with demand via feedback mechanisms.
Dependence and Independence
In summary the ?units to unity? concept, together with the ?links and connections? concept allow the thyroid to be unique in its own right, but allows it to participate in the bigger whole, fulfilling a function for the body at large and allowing it to be personally enriched by its contributions. This ?independence/dependence? balance is a key concept to all the biological units from each cell in the body to the societies in which we live.
Time, Growth and Aging
Thyroid development begins in the fetus at three to four weeks of gestation. The precursors consisting of epithelial cells arise from endoderm proliferate from the base of the pharynx. From this moment, the cells of the thyroid are subjected to the forces of time. Over the next several weeks this cell mass migrates to the base of the neck. Shortly thereafter, at eight weeks of gestation the pituitary begins to release thyroid stimulating hormone, prompting the thyroid to begin production of colloid and thyroxine by week ten.
The thyroid ages well, but function does decrease over time and often is the cause of morbidity in the elderly.
Space
The space assigned to the thyroid in the neck has no obvious rationale. It is a thermostat and for this it may be centrally located and near the brain ? the main controlling centre of the body.
It lies on the anterior side of the neck against and around the trachea and extends posteriorly to the esophagus and carotid sheath. Longitudinally it stretches from just below the laryngeal prominence, or Adam?s apple, to the fifth or sixth tracheal ring. Owing to this position, any significant swelling of the thyroid, such as that caused by hyperthyroidism or iodine deficiency, is easily visible and palpable.
Forces
The forces that govern thyroid function are primarily chemical. Like most endocrine organs, the thyroid produces and releases hormones according to negative feedback inhibition loops. For example, low levels of thyroxine prompt the pituitary gland to release TSH. This, in turn, causes the thyroid to release thyroid hormones. As the levels of thyroid hormone increase, TSH is inhibited, which results in a decrease in thyroid hormone production. It is a continual balance of supply and demand and checks and balances.
The involvement of calcitonin abides by the same principles but relate specifically to calcium metabolism.
Thyroid function is also regulated by nervous pathways, specifically the sympathetic nervous system. The sympathetic system and thyroid have very similar effects on the body though the nervous system is more rapid in reacting while thyroid hormone is in the background and slower in response. It may be said that the sound one may hear at the height of the fight or flight response may be likened to a screech, while the sounds of the thyroid hormone may be likened to a hum.
History of the Thyroid
Diagnosis of body disorder in early civilization was easiest performed on superficial structures. It is thought for example, that dental disease was recognized and surgically treated in civilizations as early as Indus Valley Civilization of Pakistan as far back as 7000 BC (Coppa). The thyroid is a superficial structure but not normally seen nor felt. However, goiter has been and is a very common entity in many parts of the world particularly in mountainous areas where soil erosion has washed iodine from the soil and as a result, people who live in the mountains and subsist on their own agriculture are at risk for this entity. Not only has it been a problem for the people of the mountains but also for the fetuses that depended on maternal intake for the iodine. Hence, cretinism went hand in hand with goiter disease of the mountain people.
Diminished iodine intake results in increased size of the gland by hyperplasia as it attempts to maintain a normal level of thyroxine in the blood. This disease thus creates a prominent and sometimes huge and deforming thyroid mass, defined by some ancients as ?elephant of the throat?. The goiter was easily recognized and diagnosed as abnormal and the unsightly appearance necessitated attempts at solving the problem.
The Chinese emperor Shen Nungs prescribed the use of seaweed for the treatment of goiter as early as 2700 BC. It is remarkable that this civilization was aware of a real therapeutic advantage of seaweed, which we now know, like many products of the sea, are high in iodine content. It is one of the first diseases that not only was recognized as the treatment had an effective biochemical component. This is truly remarkable.
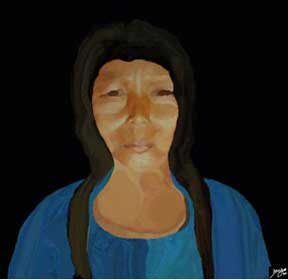
The drawing reveals a mountain person from China who subsists off the land of the region. The soil erosion depletes the soil of iodine resulting in unsightly goiters particularly in females whose needs increase during pregnancy. It is therefore not surprising that the entity was recognized in ancient times due to its easy visibility, and unsightly appearance. However what is surprising was the ability of the Chinese to identify use seaweed in therapy. We now know that seaweed is rich in iodine.
Courtesy: Ashley Davidoff, MD
Here are some other interesting points in history:
1835
Robert James Graves an Irish doctor published his accounts on exophthalmic goiter associated with palpitations and the entity now called Grave?s disease was established.
1914
Edward Calvin Kendall isolated ?thyroxine? as the active principle of the thyroid gland.
Thyroxine became available in the 1920?s. Three tons of animal thyroid yielded 33 grams of thyroxin and it was thus an expensive but necessary drug.
1926
Sir Charles Harrington a British scientist was able to synthesize thyroxine
1945
Hiroshima ?Little Boy? August 6 1945 and ?Fat Man?Nagasaki August 1945 resulted in exposure of large populations to radiation and resulted in an increase in papillary carcinoma and frequency depended on age at exposure and distance from the radiation source.
1952
Rosalind Pitt-Rivers worked under Sir Charles Harington. She subsequently went on to work with her Canadian post doctoral fellow Jack Gross and synthesized tri-iodothyronine which was biologically more active than thyroxine.
1986 April 26th
Chernobyl is small town located in the Ukraine region of the former Soviet Union where the worst nuclear accident occurred when a reactor exploded and released radiation into the atmosphere which by some estimates were 100 greater than Hiroshima The radiation and particularly radioactive iodine became incorporated into the plants and water and people were contaminated by ingestion particularly of milk. One of the main consequences was an increase in thyroid carcinoma in children some of whom were not yet born estimates as a 10 times increase.
Parts of the Thyroid
The thyroid consists of two lobes, a right lobe and left lobe, connected by the isthmus. Sometimes a pyramidal lobe projects from the isthmus or from one of the lobes, which is a normal variant.
The superior poles diverge laterally, are almost cigar-shaped and usually differ slightly in size and shape. Sometimes there may be marked difference in size usually with the right lobe being larger than the left. The lobes are divided into lobules by connective tissue elements that emanate from the fibrous capsule. Each lobule consists of 20-30 follicles.

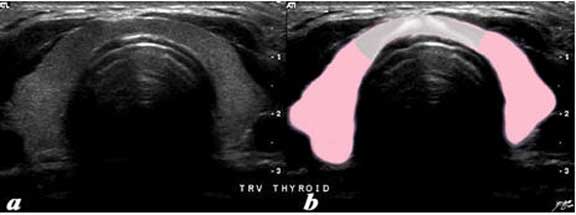
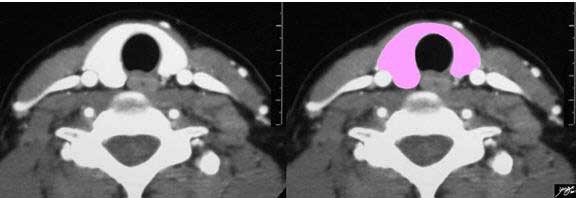
The thyroid is a butterfly-shaped gland with two lobes, each looking like an inverted cone. The right lobe and left lobe are connected by the isthmus (white overlay).
Courtesy: Ashley Davidoff, MD
The isthmus originates from a Greek term which means a narrow neck of land bordered on two sides by water and usually connecting two larger areas of land. It is variably sized, and infrequently absent. The cricoid cartilage is its landmark and it may be encountered during tracheotomy and cognizance of this fact must be considered requiring it to be elevated, depressed or divided during the procedure.
The transverse ultrasound of the thyroid gland shows the asymmetric symmetry of the lobes. In this cut the right lobe is slightly larger than the left and the isthmus consists of a narrow band (pearl white) that is thinner than the lobes and only about 5 mms thick. However, it does take center stage position of the thyroid.
Courtesy: Ashley Davidoff, MD

A variation in shape is a third small cone that lies between the lobes and sometimes originates off one of the lobes more commonly the left. This is called a pyramidal lobe and is an embryological remnant of the thyroglossal duct.
Courtesy: Ashley Davidoff, MD
Histology
At the histological level the unit of the thyroid is the lobule. Each lobule consists of 20-30 follicles.
The thyroid is brownish-red in color, is a highly vascular gland and is composed of multiple lobules separated by thin septations. Each lobule consists of 20-40 follicles and supplied by an intralobular artery.
The thyroid is characterized by three main histological features: colloid containing follicles, follicular epithelium, and parafollicular cells.
The follicles secrete thyroxine and triiodothyronine. The follicles are spherical cavities which contain colloid, a viscous secretion rich gel, primarily a storage for thyroglobulin, which is the precursor for T3 and T4. The colloid serves as a reservoir for raw materials and also as storage for the hormones themselves. The follicles range in size from 50-500 microns but average about 200 microns in diameter. There is sufficient storage of thyroid hormone for about 100 days.
Each follicle is lined by a single layer of follicular epithelial cells, collectively termed the follicular epithelium, whose morphology ranges from cuboid when inactive to columnar when active. These cells trap iodine from the bloodstream and use it to synthesize thyroxine and triiodothyronine from the glycoprotein thyroglobulin. If not needed immediately these hormones remain stored in thyroglobulin and are secreted along with colloid into the follicles. When serum levels of thyroxine and triiodothyronine drop too low, colloid is absorbed back into the thyroid cells where thyroglobulin is cleaved and the hormones are released through the base of the cell into the surrounding capillaries.
Parafollicular cells or C cells surround the follicular epithelium and follicles and synthesize calcitonin, which help regulate calcium metabolism in conjunction with the parathyroid glands.

The histological section at 20X magnification using H&E stain shows normal thyroid tissue with normo-follicular and macrofollicular changes. The single layer of epithelium surrounding the follicle is made up of a simple cuboidal cells and the lumen is filled with pink staining colloid. Thyroglobulin and iodide are contained within the colloid and are used to produce thyroid hormones including thyroxine. Between the cells are the parafollicular cells that produce calcitonin.
Courtesy: Ashraf Khan, MD, Department of Pathology, University of Massachusetts Medical School
Size
The thyroid is one of the largest endocrine organs in the body, but on the other hand is small compared to most other organs. It weighs about 15- 35 grams measuring approximately 4-5 cm long, 2-2.5 cm wide and 1 -2 cm thick, in the average adult. The isthmus is 2-6mm in A-P diameter and is up to 20 mm in width.
The size of the thyroid changes with age. At birth is weighs 2-3 grams, reaches 10-15 gms at puberty and becomes full size by age 25 when it weighs 15-35 gms.
The weight of the gland varies with age, sex, functional status, iodine intake, and geographic location. The thyroid tends to be larger in women and also larger during the menstrual cycle and pregnancy.
From a clinical standpoint, size is an especially important structural characteristic of the thyroid. The gland is not usually palpable on clinical examination. If palpable, it is abnormal.
The enlarged gland may reflect hyperthyroidism, hypothyroidism or a nodular euthyroid gland, and further biochemical and imaging evaluation is necessary.
Fortunately, thyroid size is easily measured with ultrasound, which is a safe and relatively inexpensive tool. Linear measurements are the standard for most evaluations, but measurements that portray a volume or mass are also possible using conventional imaging techniques.

The thyroid gland is one of the largest glands in the body. The right and left lobes vary slightly in size and shape and therefore each may have slightly different weights.
Courtesy: Ashley Davidoff, MD
Size: Imaging the Normal Gland

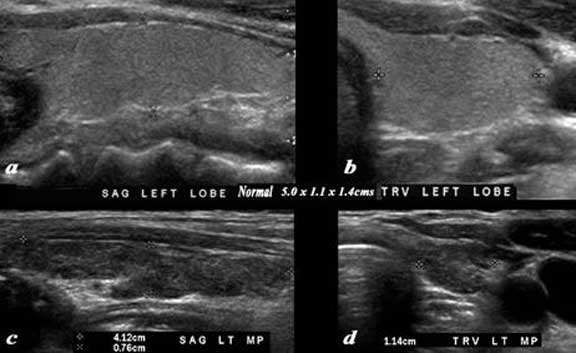
A normal ultrasound of the thyroid gland is demonstrated. Image (a) and (b) are sagittal images, image (c) is a transverse view of both lobes and the isthmus, and image (d) and (e) are individual measurements of the right and left lobe respectively. The normal right lobe (a, d) measures 4.9cm (length) x 1.1cm (A-P anteroposterior) X 1.6 cm (transverse TRV) and the left lobe (b, e) 5.cm(craniocaudal), by 1.1cm (A-P) by 1.8cm (transverse)
Courtesy: Ashley Davidoff, MD

The image shows the artistic rendering of the small hypofunctioning thyroid (gray) the normal thyroid in the middle (pink), and the hyperfunctioning and enlarged thyroid of thyrotoxicosis.
Courtesy: Ashley Davidoff, MD
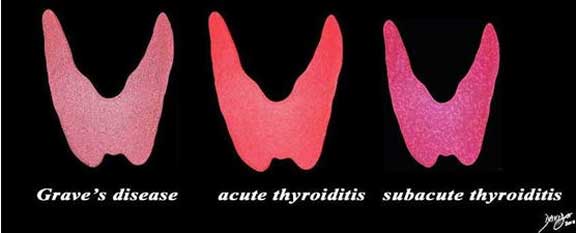
The enlarged, smooth gland is usually seen in patients with thyrotoxicosis and includes Grave’s disease, acute thyroiditis and subacute thyroiditis.
Courtesy: Ashley Davidoff, MD
Size: Imaging of Goiters
A goiter implies a large gland. It may be caused by a diffusely enlarged gland, by multiple nodules or sometimes by a single large nodule.

The plain film (a), with magnified view (b) shows a large mass shifting and compressing the trachea (teal) to the right. The mass is seen on cross-sectional CT as an irregularly, enhancing mass connected to the thyroid gland on more cranial views. Its mass effect on the trachea results in narrowing best appreciated in the transverse dimension. The findings are consistent with a retrosternal thyroid goiter.
Courtesy: Ashley Davidoff, MD

A large retrosternal goiter is seen extending down anterior to the top of the aortic arch is noted in this 74 year old female patient. In image (a) and (b) the visualized portion of the goiter measures 8.8cm, has a central avascular component and an enhancing rind. The goiter is overlaid in (green) and seen displacing the trachea (teal blue) to the right. On the axial cuts the goiter with central avascularity is again noted compressing on the trachea and pushing it to the right (teal blue) the esophagus is also pushed rightward. The brachiocephalic vein (blue) is compressed and there are venous varicosities both on the left and posteriorly on the right of the goiter. Anterior chest veins are also prominent. The findings are consistent with a retrosternal thyroid goiter.
Courtesy: Ashley Davidoff, MD

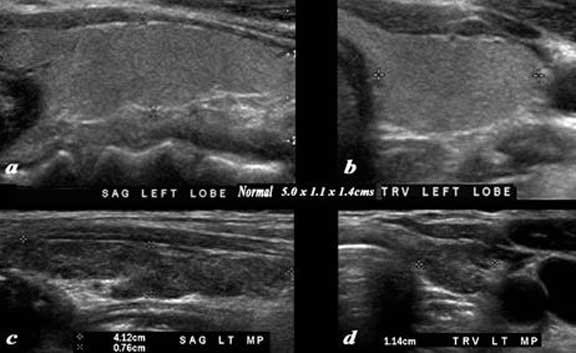
A normal ultrasound of the thyroid gland (a, b) is juxtaposed with the ultrasound of a 78 year female with hypothyroidism (c, d) A diffusely enlarged, heterogeneous thyroid gland is seen in the hypothyroid patient. The normal thyroid measures 5.0cm (length) x 1.1cm (A-P anteroposterior) X 1.4 cm (transverse TRV) and the abnormal thyroid measures 8.5cm (cranio-caudad), by 3.9cm (A-P) by 4.8cm (transverse). Clinical findings were consistent with thyroiditis, with biochemical findings suggesting hypothyroidism. The enlarged gland in the transverse dimension is almost round (d). This rounded shape in the transverse dimension is a clue to the presence of the enlarged gland, even before the measurements are taken and evaluated. The gland is heterogeneous particularly well seen on the sagittal view (c). The findings are consistent with a thyroiditis.
Courtesy: Ashley Davidoff, MD
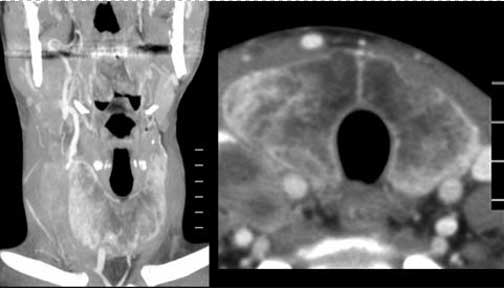
The CT is from a 35 year old man with a complex history including long standing history of Crohn?s disease and a recent history of lymphoma. He has had a goiter for many years and biopsy showed amyloidosis of the thyroid. The image on left is a coronal view of the neck and the (b) is a transverse view of the thyroid. The gland is enlarged measuring 6.2cm in Craniocaudal dimension (length) by 3cm in anteroposterior dimension by 3 cm in transverse dimension. On the transverse view it is not quite round but the gland is full bodied reminiscent of its large size. The density appearance is puzzling. Since no non-contrast CT was performed the peripheral increase in density may be due to enhancement or more likely due to iodine or calcification. The soft densities to the right of the right lobe are related to the patient?s newly diagnosed lymphoma.
Courtesy: Ashley Davidoff, MD
Size: Mass in a Lobe Causing a Goiter
Goiter Caused by Large Hemorrhagic Cyst

Courtesy: Ashley Davidoff, MD
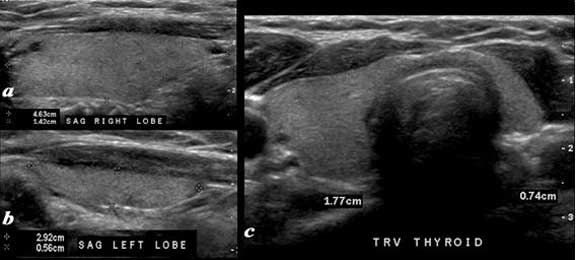
A normal ultrasound of the thyroid gland with a hypoplastic left lobe is demonstrated. Image a is a transverse image, while image (b) is a sagittal view of the right lobe, and image (c) is a sagittal view of the left lobe. The normal right lobe (a, b) measures 4.6cm (length) x 1.4cm (A-P anteroposterior) X .7 cm (transverse TRV) and the hypoplastic left lobe measures 2.9cm (cranio-caudad), by .6cm (A-P) by .7cm (transverse).
Courtesy: Ashley Davidoff, MD
A normal thyroid gland in sagittal (a) and transverse (b) planes is juxtaposed on an abnormal atrophied gland(c, d).
The images shown in (c) & (d) are from a 70 year female who reveals diffuse atrophy of her thyroid by this ultrasound examination. The gland is mildly heterogeneous. The left lobe measures 4.1cm (craniocaudad), by .8 cm (A-P) by 1.1cm (transverse). The sagittal view shows mild coarsening and heterogeneity of the echoexture. The transverse view shows a normal shape. The isthmus is normal in size. These findings suggest age related involution of the gland.
Courtesy: Ashley Davidoff, MD
Shape
The thyroid is a butterfly-shaped gland with two lobes each an inverted cone. Together their shape varies from an H to a U shape in the coronal plane. It is also U-shaped or horseshoe-shaped in the axial projection.
The thyroid gland gets its name from the Greek word for shield given its shape and the shape of the thyroid cartilage on which it rests. In some patients a pyramidal lobe extends cranially from the isthmus representing residual thyroglossal duct tissue that assumes thyroid character.
The shape of the thyroid cannot be observed through clinical examination; however, the ?thyroid neck check,? which requires a patient to observe his/her neck for asymmetrical bulges while swallowing, may reveal irregularities in its shape.

The H V or U shaped form of the thyroid gland is appreciated in this image. The isthmus may be broad in its craniocaudad dimension or may be relatively narrow.
Courtesy: Ashley Davidoff, MD
The shape of the thyroid is well appreciated with the two lobes connected by the isthmus. The size and shapes of the two lobes may vary.
Courtesy: Ashley Davidoff, MD

A variation in this shape of the thyroid gland is created by the presence of a pyramidal lobe, which is an embryological remnant of the thyroglossal duct. It is characterized by a third small cone that lies between the lobes and sometimes originates off one of the lobes more commonly the left.
Courtesy: Ashley Davidoff, MD
Shape: In the Transverse or Axial Projection
The axial CT scan of the neck shows the thyroid gland with the right and left lobes (pink). The gland is horseshoe-shaped, and while on the horse theme the gland in this projection could also be viewed as a saddle with saddle bags n either side. The thyroid surrounds the similarly shaped trachea (black). Note in this case the right lobe is slightly larger than the left.
Courtesy: Ashley Davidoff, MD
Axial Image – Ultrasound Scan
The transverse ultrasound of the thyroid gland shows the asymmetric symmetry of the lobes. In this cut the right lobe is slightly larger than the left and the isthmus consists of a narrow band (pearl white) that is thinner than the lobes and only about 5 mms thick. However, it does take center stage position of the thyroid.
Courtesy: Ashley Davidoff, MD
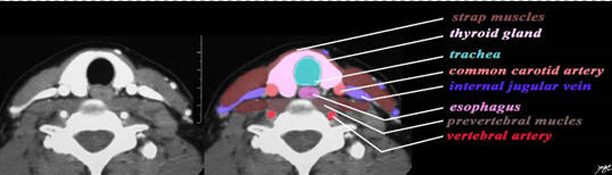
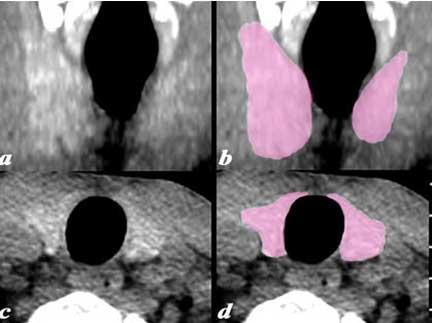
The axial CT demonstrates the central position of the thyroid in the neck and its relations. Anteriorly a group of muscles called the strap muscles (tan) separate the thyroid gland from the skin. The thyroid surrounds the trachea (teal) on its anterior and lateral borders. The esophagus (darker pink) lies posterior to the trachea and medial to the posterior border of the lobes of the thyroid. The common carotid arteries lie posterior to each of the lobes, while the internal jugular veins lie lateral to the lobes. The prevertebral muscles (light brown) and vertebral arteries (bright red) form posterior relations of the thyroid.
Courtesy: Ashley Davidoff, MD
Position
The thyroid lies on the anterior side of the neck, against and around the trachea, and reaches posteriorly to touch the esophagus. It is anchored to the laryngo-skeleton, and thus swallowing causes it to move up as the pharynx rises. It lies just below the cricoid cartilage. The cricoid cartilage is the landmark for the isthmus cartilage.
Relationships – Applied Anatomy
Anatomical relationships of the thyroid gland have clinical relevance; the recurrent laryngeal nerves lie in a groove between the lateral edges of the thyroid and the trachea behind the gland. In addition there are two pairs of parathyroid glands that are usually located in the back of the thyroid in the upper and middle portion of the lobes, but may be located within the gland.
The right recurrent laryngeal nerve originates from the vagus nerve, and after looping around the subclavian artery, it ascends behind the right lobe of the thyroid.
The left recurrent laryngeal nerve comes from the left vagus nerve, and after looping posteriorly around the aortic arch, it and ascends in the tracheoesophageal groove posterior to the left lobe of the thyroid.
The thyroid is also draped around the trachea and the esophagus posteriorly. All these structures can be affected by thyroid diseases like thyroid enlargement causing compression, or thyroid malignancies causing invasion. Surgical interventions may result in injury to these organs due to their close proximity.

The CT scan of the neck shows the thyroid (pink) as a central structure surrounded by the great vessels including the internal jugular veins (blue) and the carotid arteries, (red) and the airway (black).
Courtesy: Ashley Davidoff, MD

The thyroid gland lies anterior to the internal carotid arteries.
Courtesy: Ashley Davidoff, MD
Character
What does it look and feel like?
The thyroid is a brownish-red in color, soft to the feel.
The imaging characteristics of the thyroid are far more revealing. These characteristics are most easily observed using ultrasound.
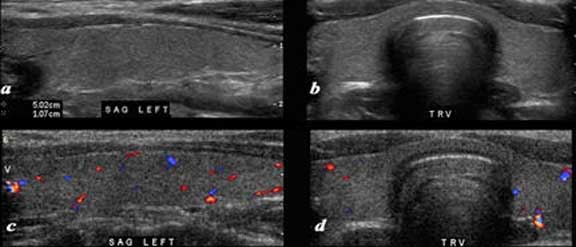
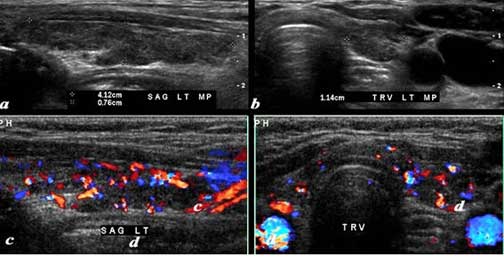
A normal ultrasound of the thyroid gland is demonstrated. Image (a) and (b) are sagittal and transverse images, and images (c) and (d) are comparable views with color flow Doppler. The normal ultrasonographic characteristics demonstrating size shape position and character of the thyroid and normal color flow pattern is well demonstrated. Note the relatively hypoechoic muscle as a thin layer just anterior to the gland and the more echogenic fat as the most superficial tissue.
Courtesy: Ashley Davidoff, MD
The normal gland though small is well seen due to its slightly higher density compared to surrounding tissues as a result of its iodine content. There are differences in the density of the thyroid on CT based on geography and differences in dietary iodine uptake.
There is no difference in density between male and female though the density of the thyroid decreases with age.
This non-contrast CT scan is from a 28 year old normal male and reveals the slight increase in density of the thyroid compared to normal surrounding soft tissue. This is due to the normal uptake of iodine. Images (a) and (b) show a reconstructed coronal view and images (c) and (d) are in the axial plane.
Courtesy: Ashley Davidoff, MD
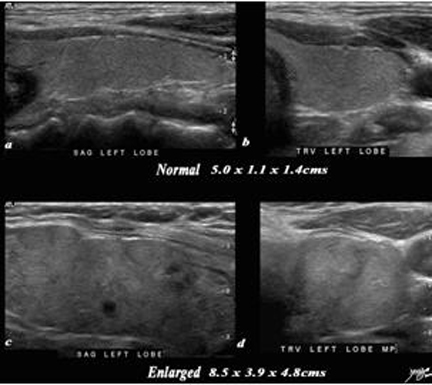
A normal ultrasound of the thyroid gland (a, b) is juxtaposed with the ultrasound of a 78 year female with hypothyroidism (c, d) A diffusely enlarged, heterogeneous thyroid gland is seen in the hypothyroid patient. The normal thyroid measures 5.0cm (length) x 1.1cm (A-P anteroposterior) X 1.4 cm (transverse TRV) and the abnormal thyroid measures 8.5cm (craniocaudad), by 3.9cm (A-P) by 4.8cm (transverse). Clinical findings were consistent with thyroiditis, with biochemical findings suggesting hypothyroidism. The enlarged gland in the transverse dimension is almost round (d). This rounded shape in the transverse dimension is a clue to the presence of the enlarged gland, even before the measurements are taken and evaluated. The gland is heterogeneous particularly well seen on the sagittal view (c). The findings are consistent with a thyroiditis.
Courtesy: Ashley Davidoff, MD

This 80 year old male presents with an asymptomatic multinodular goiter, consisting many nodules of varying size and echogenicity, as seen by sagittal ultrasound (a, b) and transverse imaging images (c, d), and Doppler imaging (e, f). The multiple nodules that are not border forming are within the confines of the parenchyma and do not alter the shape of the gland. The right lobe of the thyroid measures about 4.5 cm in sagittal 1.5cm in A-P dimension, and 1.5cm in the transverse plane. The gland is therefore not enlarged. In addition, the gland has a normal appearance in the transverse projection and the borders are not rounded to suggest enlargement. The Doppler study shows no internal vascularity in any of the nodules visualized. These findings are consistent with a non toxic multinodular thyroid gland, and not truly a goiter since the gland is not enlarged.
Courtesy: Ashley Davidoff, MD
Blood Supply
The thyroid is well supplied with blood from the superior thyroid artery, inferior thyroid artery and sometimes also from the thyroid ima artery. Blood flow through the thyroid is high at about 5mls/g/minute which is about the same volume of blood flow to the brain
The superior thyroid artery is a paired vessel and a branch of the external carotid artery and travels superiorly and anteriorly in the carotid triangle.
The inferior thyroid artery is also a paired vessel and a branch of the thyrocervical trunk which originates off the subclavian artery. It ascends in front of the vertebral artery. The recurrent laryngeal nerve is closely related to the inferior thyroid artery. The nerve may pass anterior, posterior, or through the branches of the inferior thyroid artery. It is of concern during thyroid surgery and damage to the nerve can cause hoarseness.
The superior and inferior thyroid arteries anastomose with each other through consistent collateral pathways.
The thyroid ima artery is a single artery that is present in only 4-10% of patients and supplies the inferior aspect of the thyroid. It ascends anterior to the trachea and is of concern when tracheotomies have to be placed.
In the early days of surgery the high mortality was related to post operative bleeding due to the highly vascular nature of the organ.
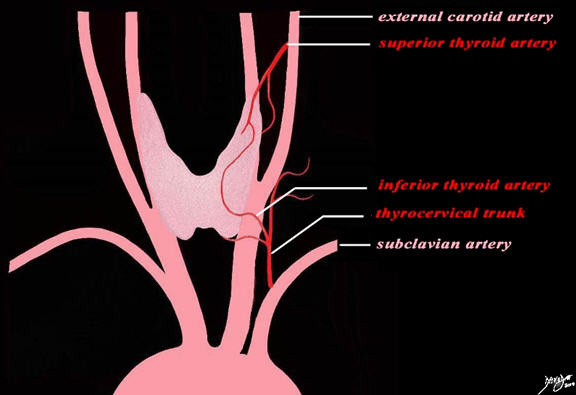
The blood supply of the thyroid gland comes from two sources. The superior thyroid artery arising from the external carotid artery. The inferior thyroid artery arises from the thyrocervical trunk which is a branch of the subclavian artery. Both vessels divide into anterior and posterior branches. The anterior division of the superior artery anastomoses with the anterior division of the inferior thyroid artery. The posterior divisions create the same anastomosis posteriorly.
Courtesy: Ashley Davidoff, MD
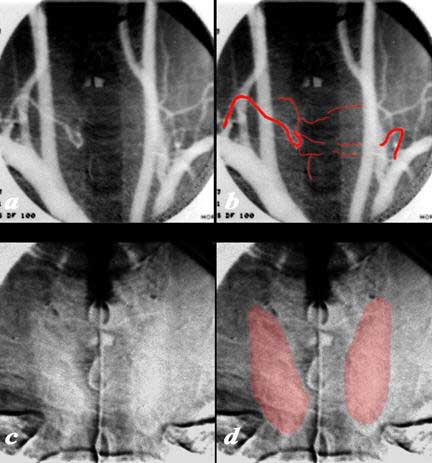
The arch aortogram injection in the A-P projection shows remnants of the right inferior thyroid artery that arises from the subclavian artery (a, and overlaid in b) together with barely seen vessels supplying the thyroid. A small segment of the left inferior thyroid artery is also perceived. In the capillary phase of the angiogram a faint homogeneous blush of thyroid is seen (c and overlaid in d).
Courtesy: Ashley Davidoff, MD
Blood Supply: Superior Thyroid Artery

This selective injection in the A-P projection of the superior thyroid artery that arises from the external carotid artery shows a diffuse normal blush of the left lobe of the thyroid.
Courtesy: Ashley Davidoff, MD
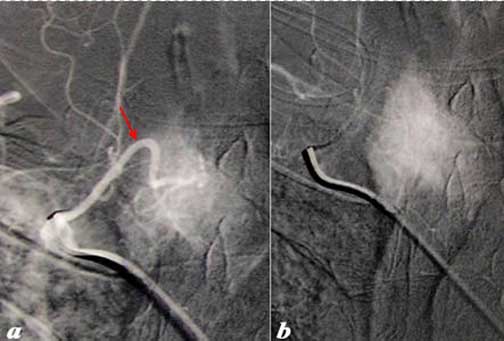
This selective injection in the A-P projection of the inferior thyroid artery (red arrow) that arises from the subclavian artery as a branch of the thyrocervical trunk shows the vessel coursing medially with an early blush in the early arterial phase, followed by a diffuse blush in the capillary phase.
Courtesy: Ashley Davidoff, MD
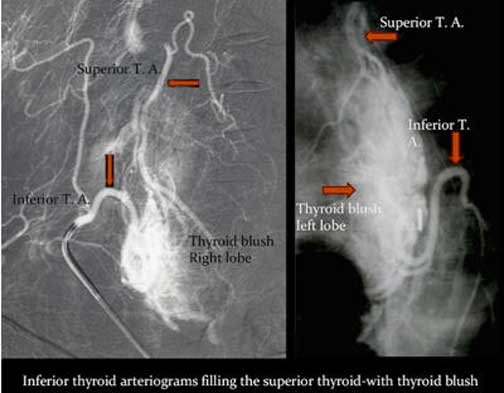
These angiograms demonstrate the collateral connections between the inferior and superior thyroid arteries. In image (a) the selective injection of the right thyrocervical trunk shows filling of the superior thyroid artery conforming their intimate connection and collateral capability. In the second case of selective injection of the left inferior thyroid artery, filling of the superior division is seen as well with large collateral pathways visible (barely) inside the thyroid).
Courtesy: Ashley Davidoff, MD
Venous Drainage
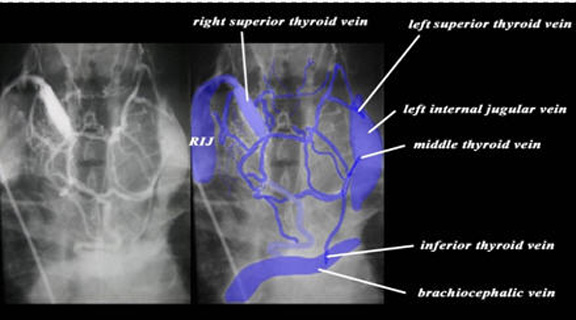
Blood drains from the thyroid via the superior, middle and inferior thyroid veins.
The superior thyroid vein runs with the superior thyroid artery. Each superior thyroid vein drains to ipsilateral internal jugular vein.
The middle veins also drain into the jugular veins bilaterally.
The inferior thyroid vein on the left drains into the brachiocephalic vein. The inferior thyroid vein on the right may drain into a right sided innominate vein (if present) or into the left sided brachiocephalic vein. Sometimes a common vein called the thyroid ima vein drains the left and right inferior veins via a common channel.

This diagram illustrates the venous drainage of the thyroid which is drained by the superior thyroid vein and middle thyroid vein which empty into the jugular vein, and the inferior thyroid vein which usually enters into the brachiocephalic vein.
Courtesy: Ashley Davidoff, MD
The venogram with injection into the right superior thyroid vein demonstrates the collateral venous connections between all the veins of the thyroid including the superior middle and inferior vessels bilaterally. The injection into the left superior thyroid vein causes expansion of that vein accounting for the asymmetry in size of the two veins Additionally there is a large accessory vein (overlaid in lighter blue) entering the brachiocephalic veins with the much smaller inferior thyroid veins. This may be a thyroid ima vein.
Courtesy: Ashley Davidoff, MD
Lymphatic Drainage
The thyroid is surrounded by a rich network of lymphatics. There are approximately 300 lymph nodes in the neck, and flow is in all directions including across the midline, superiorly and inferiorly.
The cervical lymph nodes have muscular and bony/cartilagenous landmarks extending from the ear superiorly to the clavicle inferiorly. The bony/cartilage landmarks starting superiorly include the inferior margin of the mandible, the hyoid bone, the cricoid cartilage and the clavicle. The muscles include the digastric muscle sternocleidomastoid and finally the trapezius. The internal jugular vein is a central landmark for a large number of the cervical nodes.
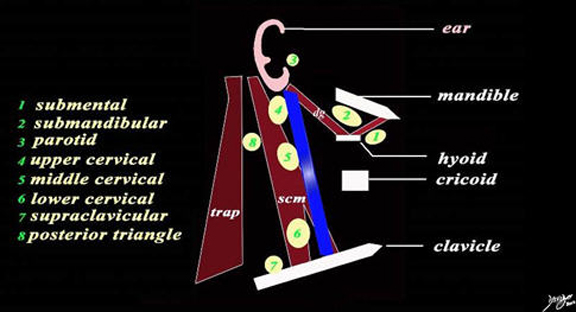
The bony landmarks starting superiorly include the inferior margin of the mandible, the hyoid bone, the cricoid cartilage and the clavicle. The muscles include the digastric muscle (dg) with anterior and posterior bellies superiorly, then the sternocleidomastoid (scm), and finally the trapezius (trap). The internal jugular vein (blue) is a central landmark for a large number o the cervical nodes.
There are 8 basic sets of lymph nodes relating to the structures described. The submental lymph nodes (1) lie inferior to the anterior belly of the digastric muscle. The submandibular glands (2) lie under the mandible and between the two limbs of the digastric muscle. The parotid lymph nodes (3) lie anterior to the ear. The cervical lymph nodes are in close association of the internal jugular vein and sternocleidomastoid muscle.. Their division of upper middle and lower nodes relates to bony landmarks. The upper cervical nodes (4) lie above the hyoid bone, the middle group (5) lie between the hyoid bone and cricoid cartilage, while the lower group (6) lies between the cricoid and clavicle. The supraclavicular group (7) lies above the clavicle, and the posterior triangle group (accessory nodes) lie high in the posterior triangle between the sternocleidomastoid and trapezius.
Courtesy: Ashley Davidoff, MD
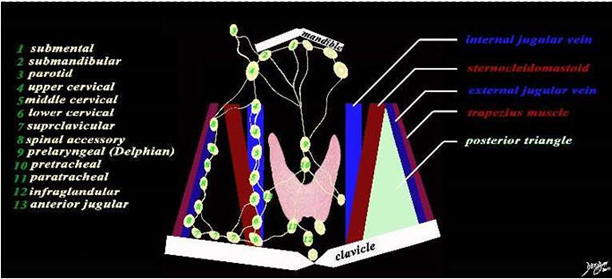
There are about 13 named sets of lymph nodes that serve to drain the neck and the region of the thyroid gland. The submental lymph nodes (1) lie inferior to the anterior belly of the digastric muscle. The submandibular glands (2) lie under the mandible and between the two limbs of the digastric muscle. The parotid lymph nodes (3) lie anterior to the ear The cervical lymph nodes are in close association of the internal jugular vein and sternocleidomastoid muscle. Their division of upper middle and lower nodes relates to bony landmarks. The upper cervical nodes (4) lie above the hyoid bone, the middle group (5) lie between the hyoid bone and cricoid cartilage, while the lower group (6) lies between the cricoid and clavicle. The supraclavicular group (7) lies above the clavicle, and the posterior triangle group (accessory nodes) lies high in the posterior triangle between the sternocleidomastoid and trapezius. The nodes that relate to the posterior triangle and external jugular vein are the spinal accessory nodes (aka posterior triangle nodes) (8). Above the thyroid and in the midline is the prelaryngeal node (Delphian node 9), and just below it and also in the midline is the pretracheal node (10) A pair of paratracheal nodes lie below the thyroid (11), and a midline infra-glandular node also lies below the gland a sits name implies. The anterior jugular vein has a node associate with it and its is called the anterior jugular node (13) The posterior triangle (light green) is formed by the posterior border of the sternocleidomastoid, the anterior border of the trapezius, and the base is formed by the clavicle.
Courtesy: Ashley Davidoff, MD
Lymphatic Drainage: Applied Biology
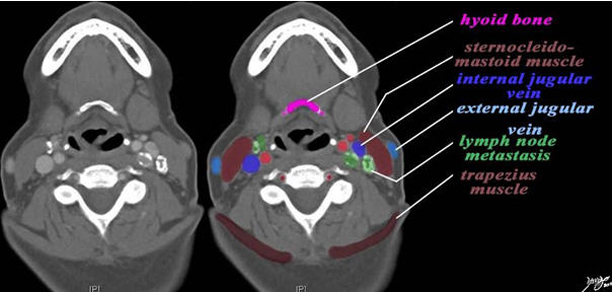
The CT scan is from a middle aged female patient with metastatic papillary carcinoma of the thyroid. Her nodes contain calcification and hence are easily seen. The case exemplifies the metastatic lymph node pattern of thyroid carcinoma. The most superior cut is at the level of the hyoid bone (pink). At this level the nodes associated with the internal jugular vein (royal blue) are the upper cervical nodes. These are posterior to the internal vein on the left and anterior on the right (dark green) There are no nodes associated with the external jugular vein nor in the posterior triangle which lies between the sternocleidomastoid muscle anteriorly and the trapezius posteriorly (maroon).
Courtesy: Ashley Davidoff, MD

Same patient. This cut is at the level of the thyroid cartilage (orange) and the most superior aspect of the cricoid cartilage (purple) . At this level the nodes associated with the internal jugular vein (royal blue) are the middle cervical nodes (green nodes). These lie lateral to the internal jugular vein (royal blue) on the left . The patient complains of hoarseness and there is an adducted left vocal cord (bright green) suggesting involvement of the recurrent laryngeal nerve.
The recurrent laryngeal nerve is intimately associated with the inferior thyroidal artery. There are no nodes associated with the external jugular vein nor in the posterior triangle (light green triangular patch) which lies between the sternocleidomastoid muscle anteriorly and the trapezius posteriorly (maroon).
Courtesy: Ashley Davidoff, MD

The thyroid ultrasound is from a 31 year old female with papillary carcinoma of the right lobe of the thyroid (b, bright green). Two small subcentimeter lymph nodes are identified in the submental area. They are almost anechoic in character.
Courtesy: Ashley Davidoff, MD
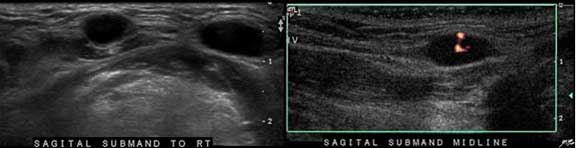
The Doppler study from the same patient as above demonstrate central vascularity.
Courtesy: Ashley Davidoff, MD
Nerve Supply
The thyroid receives innervation from both the sympathetic and parasympathetic nervous systems, which are subsets of the autonomic nervous system.
Sympathetic input is supplied by the superior cervical ganglion and the cervicothoracic ganglion. The superior cervical ganglion lies posterior to the sheath of the internal carotid artery and internal jugular vein.
The parasympathetic input is supplied by the superior laryngeal nerve and the recurrent laryngeal nerve.
It is doubtful that they play a significant role in controlling thyroid metabolism and their exact role is unclear.
Capsule
The thyroid contains a true, thin fibrous capsule of connective tissue that sends septa to divide the thyroid into lobules. There is also a false external capsule formed by a sheath of pretracheal fascia.
Support of the Gland
The thyroid gland is fixed firmly to the laryngo-skeleton accounting for its upward movement during swallowing.
The thyroid gland is covered by a part of the middle layer of deep cervical fascia, which anchors the thyroid to the laryngo-skeleton. In addition, there are suspensory ligaments extending from the superior aspect of each lobe to the cricoid and thyroid cartilages. The posterior aspect of the gland is fixed to the side of the cricoid cartilage, and the first two tracheal rings by the ligament of Berry (also known as the posterior suspensory ligament). It is this latter ligament that causes the thyroid to elevate during deglutition allowing the clinician to distinguish between the thyroid and a lymph node (Lee).
Growth and Aging
The thyroid loses volume with aging and in fact metabolism gradually slows beginning around age 20. However functionally, aging only affects the thyroid in minor ways with a slight decrease in T3 levels. Disease of the thyroid such as autoimmune disorders, become more prevalent with age.
The incidence of thyroid nodules increases with age.
50% of 50 year olds will have at least one thyroid nodule.
60% of 60 year olds will have at least one thyroid nodule.
70% of 70 year olds will have at least one thyroid nodule.
The patient is a 70 year female who shows diffuse atrophy of her thyroid by this ultrasound examination. A normal thyroid gland in sagittal (a) and transverse (b) planes is juxtaposed on the atrophied gland(c,d) The gland is mildly heterogeneous. The left lobe of the thyroid measures 4.1cm (craniocaudad), by .8 cm (A-P) by 1.1cm (transverse). The sagittal view shows mildly coarse heterogeneous echo texture. The transverse view shows a normal shape. The isthmus is normal in size. These findings suggest age related involution of the gland.
Courtesy: Ashley Davidoff, MD
The patient is a 70 year female who shows diffuse atrophy of her thyroid by this ultrasound examination. The gland is mildly heterogeneous. The left lobe of the thyroid measures 4.1cms (craniocaudad), by .8 cms (A-P) by 1.1cms (transverse). The sagittal view shows mildly coarse heterogeneous echo texture. The transverse view shows a normal shape. The isthmus is normal in size. The color flow Doppler study seems hypervascular but the significance of this finding is not known. These findings suggest age related involution of the gland.
Courtesy: Ashley Davidoff, MD
Embryology
The thyroid gland is the first endocrine gland to develop in the embryonic stage at approximately the 24th day of gestation as an outpouching at the base of the tongue in the foramen cecum on the median surface of the developing pharyngeal floor. It takes its origin from the medial anlage which derives from the floor of the foregut. The medial anlage forms the major portion of the thyroid. The thyroid gland grows and descends anterior to the trachea. As it descends it remains attached to the thyroglossal duct which normally degenerates. The thyroid gland reaches its final position in the seventh gestational week overlying the second to fourth tracheal rings. Thereafter it grows laterally to form two lobes.
If the caudal end of the thyroglossal duct persists it becomes the pyramidal process, which is considered a normal variant.
A variation in this shape of the thyroid gland is created by the presence of a pyramidal lobe, which is an embryological remnant of the thyroglossal duct. It is characterized by a third small cone that lies between the lobes and sometimes originates off one of the lobes more commonly the left.
Courtesy: Ashley Davidoff, MD
Function of the Thyroid
The primary function of the thyroid is in regulating the body’s metabolism and to produce and secrete the metabolic hormones, thyroxine (T4) and triiodothyronine (T3), as directed by the pituitary and other control pathways within the endocrine system. This process may be broken down into four sections: Receiving, Processing, Export, and Control.

This diagram focuses on the processing function of the thyroid.
Courtesy: Ashley Davidoff, MD
Receiving
Synthesis of the thyroid hormones thyroxine and triiodothyronine requires a steady supply of iodine, a chemical element found in nature and supplied by diet in most developed countries.
The average adult must consume 50 mg of iodine per year to maintain proper thyroid function. Approximately four fifths of that ingested iodine is excreted by the kidneys, but the remaining one fifth, ~10 mg per year, is selectively gathered by thyroid cells and used to produce mass quantities of thyroxine and triiodothyronine.
This process, commonly referred to as iodine trapping, occurs through the action of a large number of iodide pumps located in the basal membrane of each follicular epithelial cell. In response to endocrine activation these pumps transport free iodide from the bloodstream to the interior of the cell, concentrating it to a level up to 250 times that found in the blood.
Processing
Once inside the cell this free iodide sequentially binds to tyrosine sites in thyroglobulin, a glycoprotein produced by follicular epithelial cells and the precursor to the hormones.
Exporting
When the supply of thyroxine and triiodothyronine in the blood becomes depleted a cascade of endocrine signaling is initiated that induces the pinocytotic uptake of colloid and thyroglobulin by follicular epithelial cells.
Inside the cell thyroglobulin is digested by a series of enzymes, simultaneously releasing thyroid hormone and cleaving iodine to be reused for further hormone synthesis. Thyroxine and triiodothyronine, now freed, diffuse through the base of the thyroid cell and into the surrounding capillaries where they are transported to tissues throughout the body.
Control
Regulation of the synthesis and secretion of thyroid hormone occurs through a negative feedback inhibition pathway in the endocrine system.
When the concentration of thyroxine and triiodothyronine in the blood dips below a certain level, thyrotropin-releasing hormone (TRH) is released from the hypothalamus, resulting in subsequent release of thyroid stimulating hormone (TSH) from the anterior pituitary gland. Receptors on the base of each follicular epithelial cell bind to TSH, activating intracellular cAMP pathways that initiate a series of stimulatory effects in each thyroid cell. These effects include increased proteolysis of thyroglobulin resulting in the release thyroxine and triiodothyronine, increased activity of iodine pumps, increased iodination of tyrosine, increased size and secretory activity of existing thyroid cells, and proliferation of new thyroid cells. While proteolysis of thyroglobulin occurs almost immediately, the majority of the effect of TSH require days or weeks to occur, resulting in a well-choreographed effort to increase and stabilize basal metabolic rate. Once the rate of secretion of the thyroid increases to 1.75 times its normal rate, thyroid hormone acts directly on the anterior pituitary gland to inhibit further secretion of TSH. As a result, thyroid secretion gradually decreases and the concentration of thyroxine and triiodothyronine in the blood is kept constant.
The pituitary controls the function of the thyroid gland by the production of thyroid stimulating hormone (TSH). There is a reciprocal relationship between TSH and thyroid hormone levels.
Courtesy: Ashley Davidoff, MD
Calcitonin is the second hormone secreted by the thyroid. It is a non iodized hormone secreted by the parafollicular cells or so called C cells and responds to elevated serum calcium by diminishing bone resorption and thus, diminishing calcium release. It also increases urinary calcium excretion. Overall, therefore it serves to decrease serum calcium.
Disease
Diseases of the thyroid are common. The common structural changes include nodules and enlargement, and the common diseases that affect the thyroid include hypothyroidism, thyrotoxicosis, multinodular goiter, and thyroid cancer.
Absence or diminished function and iodine deficiency in the fetus, newborns, and young children, leads to devastating physical and mental retardation, or cretinism. Screening programs particularly in high risk regions has virtually eliminated the disease. In the adult, hypothyroidism results in disruption of normal metabolic function and, when severe can be life-threatening. While normal metabolic functioning is entirely salvageable through hormone replacement therapy, normal mental development in children once afflicted with cretinism is not, and permanent developmental delay both physically and mentally results.

A variety of appearances of the thyroid gland in disease including (from top left to right a simple cyst (yellow) the small atrophied gland seen in hypothyroidism, the large hyperemic gland seen in acute thyroiditis and Graves disease, the hemorrhagic cyst (maroon) normal, multinodular goiter of cysts (yellow), heterogeneous (light green) and solid (dark green), the malignant nodule, hot nodule with secondary atrophy of the gland, and the large multinodular retrosternal gland.
Courtesy: Ashley Davidoff, MD
Disease: Thyroid Cancer
Thyroid cancer is a malignant condition usually with no known cause, but sometimes associated with radiation exposure and in patients who are genetically predisposed.
Structurally, the disease usually manifests with a non functioning thyroid nodule. Lymphadenopathy is present in later stages of the disease.
Types of thyroid cancer
Papillary Carcinoma (75-85%)
Follicular Carcinoma (10-20%)
Medullary Carcinoma (5%)
Anaplastic Carcinoma (<3%) Other – squamous type, lymphoma
Clinically, the patient usually presents with a nodule. Causes for concern include age of the patient with younger patients being more likely to have malignant disease. Family history of thyroid cancer and excessive radiation exposure, particularly if exposure during childhood (Hiroshima, Nagasaki, Chernobyl, treatment for lymphoma) are other significant risk factors.
Clinically, concern is initially raised if a nodule is palpated.
Imaging is best performed by ultrasound examination, and concerns for malignancy are raised when there are microcalcifications, thick irregular halo or irregular margins of the mass, or the mass is longer than wide. Malignant lesions are usually hypoechoic and often hypervascular in the central matrix. Fine needle aspiration under ultrasound guidance is performed on any lesion with concerning ultrasound characteristics or in a patient with a high clinical suspicion of thyroid cancer.
The diagnosis is suggested or confirmed by pathologic examination.
Treatments include thyroidectomy or lobectomy. Radioactive iodine 131 is used in patients with papillary and follicular cancer for ablation of residual thyroid tissue after surgery but also for carcinoma that shows uptake of iodine.
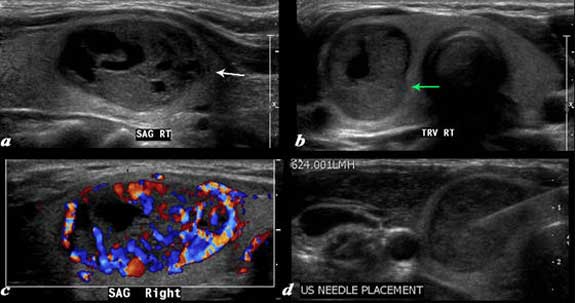
A large complex mass occupies more than half the right lobe of the thyroid gland is seen by ultrasound. The mass measures 2.6cm in sagittal and in A-P dimension measures 1.7cm(a). In transverse it measures 1.7cm. It is characterized by a mildly hypoechoic matrix with cystic type serpiginous components (a). The margins are irregular (white arrow, a). There is an incomplete halo which shows regions of irregularity (green arrow). The lesion is extremely vascular both peripherally and centrally (c). A biopsy was performed and showed medullary carcinoma.
Courtesy: Ashley Davidoff, MD
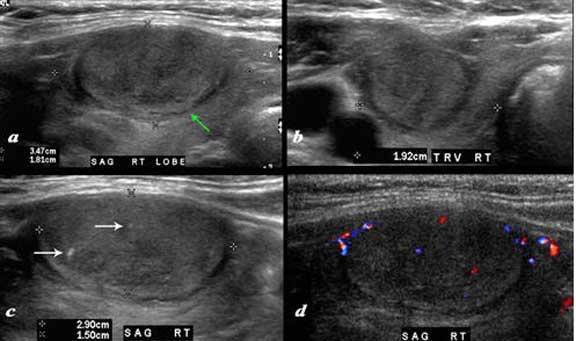
A large nodule in the thyroid occupies almost the entire right lobe (a). The nodule measures 2.9cm by 1.5cm. The gland is not enlarged and measures 3.5cm (craniocaudad), by 1.8cm (A-P) by 2.4cm (transverse). The nodule is almost isoechoic with normal thyroid but shows internal irregular areas of hypoechogenicity, regions of iso echogenicity, as well as microcalcifications (white arrows (c). There is irregularity of the border at the posterior aspect of the nodule green arrow (a). The halo shows irregular borders in this region as well. Internal vascularity is minimal (d). The irregular surface is concerning for a malignant processes. The diagnosis in this patient was papillary carcinoma.
Courtesy: Ashley Davidoff, MD

The patient has a history of papillary thyroid carcinoma treated 16 years ago. The transverse and sagittal image of a cervical lymph node that is heterogeneous with multiple punctate shadowing microcalcifications. These findings are consistent with recurrent papillary thyroid carcinoma.
Courtesy: Ashley Davidoff, MD
Disease: Hyperthyroidism
Hyperthyroidism is a result of an over production of thyroid thyroxine (T4) and triiodothyronine (T3) by the thyroid gland.
Hyperthyroidism can be caused by several different pathologies including Grave?s disease (the most common cause), toxic adenoma, toxic multinodular goiter, thyroiditis, and drugs.
Hyperthyroidism results in a clinical syndrome caused by increased levels of metabolically active free T3 and T4 in the bloodstream. Symptoms typically include tachycardia, agitation, tremors, hyperreflexia, heat intolerance and weight loss. The clinical syndrome of hyperthyroidism, when pronounced, is called thyrotoxicosis.
At its most dangerous, elevated thyroid hormone concentration can cause thyroid storm. This condition is a medical emergency and is accompanied by fever and change in mental status.
Structural changes of hyperthyroidism depend on the underlying cause, but include diffuse hypertrophy of the entire gland (as in Graves’ disease) or a single hyperactive toxic nodule.
Functional changes define the disease and consist of increased production of thyroid hormones despite negative feedback.
Clinically, patients will present with thyrotoxicosis, a large constellation of symptoms which include tremor, weight loss, insomnia, heat intolerance and irritability.
Imaging modalities to diagnose hyperthyroidism mainly include thyroid ultrasound and thyroid scintigraphy. Ultrasound can be used to distinguish between multinodular goiter, single nodule, and diffuse hypertrophy. Thyroid scintigraphy with radioiodine tracer uptake can show either localized increased uptake, such as in a ?hot? or toxic nodule, or diffuse increased uptake, as in Grave?s disease.
Although imaging is available, diagnosis is best made with laboratory tests showing both a decreased TSH level and an increased circulating level of T3 and T4.
Treatment depends on the cause of hyperthyroidism, but includes medications that inhibit thyroid hormone production (methimazole and PTU), and medications that block the increased metabolic effect of the hormones, such as beta blockers. Some cases are best treated with radioisotope (Iodine-131) ablation of the gland. Surgical thyroidectomy is the least common treatment.
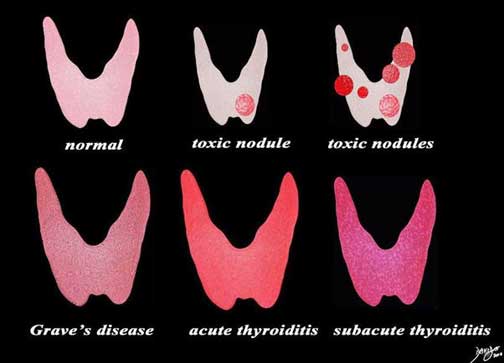
This diagram shows the structural possibilities in a patient who presents with thyrotoxicosis. Reading from upper left the normal thyroid is shown for reference of size and normal activity (pink). Next is the single toxic nodule that suppresses the function of the gland and the also causes the rest of the gland to shrink. This is followed by a diagram of multiple toxic nodules and the gland in this case may also be smaller than normal. The lower series of images include Grave’s disease, which is the most common cause of thyrotoxicosis, followed by acute thyroiditis and then subacute thyroiditis.
Courtesy: Ashley Davidoff, MD
Disease: Hypothyroidism
Hypothyroidism is a disease state in which there is an underproduction of thyroid hormones (T3 and T4) by the thyroid gland.
Hypothyroidism can be caused by infection, trauma, autoimmune disease, or nutritional deficiency.
Thyroid gland dysfunction results in a decreased level of circulating T3 and T4, despite increased TSH.
Structural changes will depend on the cause of hypothyroidism, ranging from enlarged inflammatory gland of Hashimoto?s thyroiditis to an atrophic or absent thyroid gland.
Functional changes define the disease and result in decreased levels of production and circulation free thyroid hormones.
Clinically, a decreased level of thyroid hormones will present with a constellation of symptoms including fatigue, cold intolerance, constipation, depression, and weight gain.
Imaging modalities are not typically used to diagnose hypothyroidism.
Diagnosis is best made with laboratory studies showing high levels of TSH with inappropriate corresponding low levels of circulating T3 and T4.
Treatment for hypothyroidism is replacement of the deficient levels thyroid hormones with synthetic forms such as synthetic T4 (Levothyroxine) or combination T4 and T3 replacement. Treatment adequacy is determined by monitoring TSH levels to ensure adequate physiologic levels are achieved and maintained.
Disease: Thyroiditis
Hashimoto’s thyroiditis is an autoimmune disorder that leads to antibody mediated destruction of thyroid gland.
The most common causative antibodies responsible for Hashimoto?s thyroiditis are anti- thyroid peroxidase (anti-TPO), anti-thyroglobulin (anti-Tg), and anti-TSH receptors.
The immune destruction of the thyroid follicular cells results in glandular destruction and hypothyroidism.
Structural histopathological changes of Hashimoto’s include lymphocytic cell infiltration, fibrotic change, and formation of lymphoid follicles that replace the normal glandular tissue. Structural changes can range from an enlarged goiter to atrophy of the thyroid gland.
Clinically, patients suffering from the disease may have transiently increased thyroid hormone release during initial destruction of the thyroid follicles, but in general the disease is characterized by a hypothyroid state with a non-functioning thyroid gland. Classically, Hashimoto’s will present with insidious onset of hypothyroidism progressing over months to years.
These symptoms include fatigue, constipation, weight gain, cold intolerance, menstrual irregularities.
Imaging is not particularly useful for the diagnosis, but sonographic features of Hashimoto’s thyroiditis are evident and suggestive. Radioactive iodine scans may show a generalized decreased iodine uptake at later stages of the disease.
Treatment for Hashimoto’s thyroiditis is based on thyroid hormone replacement, most often with levothyroxine (synthetic T4).
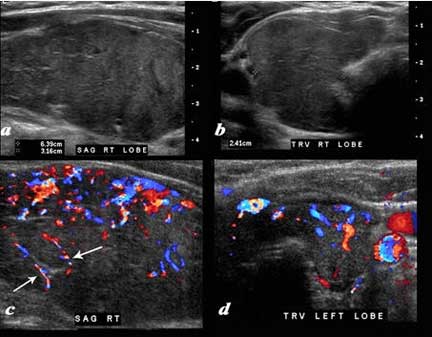
A diffusely enlarged, heterogeneous thyroid gland is seen in this 30 year old hypothyroid female patient. The thyroid measures 6.4cm (craniocaudad), by 3.2cm (A-P) by 2.4cm (transverse). Clinical findings were consistent with thyroiditis, with biochemical findings suggesting hypothyroidism. The sagittal view shows coarse heterogeneous echo texture with fine white bands consistent with fibrosis. The increased vascularity is seen throughout the gland (c, d), but is also seen particularly along some of the bands in the posterior aspect of the gland (c arrows). The enlarged gland in the transverse dimension is almost round (b). This rounded shape in the transverse dimension is a clue to the presence of the enlarged gland, even before the measurements are taken and evaluated. The findings are consistent with a thyroiditis.
Courtesy: Ashley Davidoff, MD
Diagnosis of Thyroid Diseases
For the clinician the approach to diseases of the thyroid is in determining the functional status of the thyroid and whether the patient appears euthyroid, hypothyroid or hyperthyroid. Although the thyroid is superficial it is not normally palpable, but when palpable it is abnormal. Confirmation that it is the thyroid that is palpable is achieved by establishing that moves up with swallowing.
Blood tests measure thyroxine and TSH that enable evaluation of autonomous function, hyperproduction and hypoproduction.
Ultrasound is the study of choice for the morphological evaluation of the thyroid.
It is used initially to evaluate the size of the gland and the presence and nature of nodules. It is also helpful in defining nodules that may require biopsy and used to follow the patient with nodules or the patient who is at risk for cancer. Lastly, it is used as a guide for biopsy when indicated.
The approach to the nodule is quite a difficult imaging problem particularly when there are multiple nodules and the decision to biopsy requires intense analysis of each of the nodules. In the past, the main criterion for biopsy was size and nodules that were greater than 1 cm were biopsied. Currently, important criteria include nodules that are profoundly hypoechoic, contain microcalcifications, have an irregular halo or irregular or lobulated border, or show obvious invasive properties (Kim, Hoang).
Lesser criteria include inner vascularity or a nodule that has a longitudinal dimension greater than the transverse dimension.
Benign disease includes cystic disease without complexity and nodules that have echogenic foci that have ring down artifact suggesting colloid concretions (Hoang). Pathology reports divide findings into either non diagnostic material or diagnostic material. Non diagnostic material is due to inadequate material, while diagnostic material may be categorized as malignant, indeterminate, or benign.
A normal ultrasound of the thyroid gland (a, b) is juxtaposed with the ultrasound of a 78 year female with hypothyroidism (c, d) A diffusely enlarged, heterogeneous thyroid gland is seen in the hypothyroid patient. The normal thyroid measures 5.0cm (length) x 1.1cm (A-P anteroposterior) X 1.4 cm (transverse TRV) and the abnormal thyroid measures 8.5cm (craniocaudad), by 3.9cm (A-P) by 4.8cm (transverse). Clinical findings were consistent with thyroiditis, with biochemical findings suggesting hypothyroidism. The enlarged gland in the transverse dimension is almost round (d). This rounded shape in the transverse dimension is a clue to the presence of the enlarged gland, even before the measurements are taken and evaluated. The gland is heterogeneous particularly well seen on the sagittal view (c). The findings are consistent with a thyroiditis.
Courtesy: Ashley Davidoff, MD
Diagnosis of Thyroid Diseases: Nuclear Medicine
Nuclear medicine is used to determine the overall functional activity of the thyroid or a nodule and specifically to determine whether the thyroid or the nodule is hyperactive (hot) normal, or hypoactive (warm) or inactive (cold).
Imaging can be performed using radioactive iodine or pertechnitate. In the past, radioactive iodine (I) 131 was utilized but because of the relatively high dose to the thyroid it has been mostly supplanted by I 123 and pertechnitate imaging. I 131 emits a beta particle that has a long half life and therefore subjects the thyroid to larger amounts of radiation. In addition, contaminants such as I 124 and I 125 are present and serve to increase the radiation dose. I 131 is given to patients with known thyroid cancer after surgery in order to ablate remnant thyroid gland or any remaining thyroid cancer that is able to take up the iodine.
The thyroid organifies orally administered iodine and therefore imaging can only be done once the iodine is incorporated which is approximately 24 hours later. Intravenous pertechnetate requires a 20 minute wait before the thyroid can be imaged and is relatively inexpensive. However, it is not used for imaging cancer because of low uptake by cancer cells and therefore cannot be used to evaluate for metastases.
A hot gland indicates an overactive thyroid and a cold gland indicates underactivity.
When a nodule is? hot? the chances of malignancy are low. The risk of cancer in a solitary cold nodule is 15-40%.
This is a thyroid scan from a 39 year old female with a clinical history of hyperthyroidism. She was injected with 16.1mCi of 99m Technetium pertechnetate. The scan shows normal uniform uptake of the radioisotope in both lobes of the thyroid gland. The uptake in the thyroid gland is greater than the uptake in the submandibular and parotid glands. These findings are consistent with a normal thyroid gland.
Courtesy: Ashley Davidoff, MD
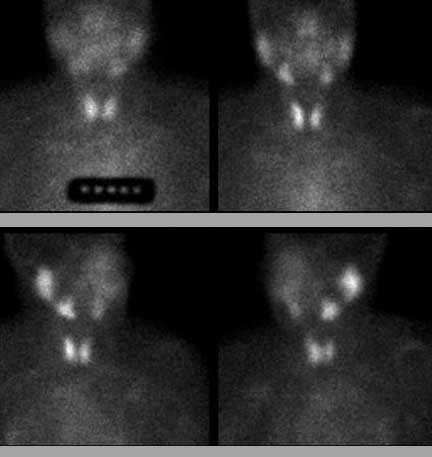
This 74 year old female presents with a multinodular goiter. Thyroid scan is shown. Markers were placed on the sternal notch. She was injected with 8.3mci of 99mTc pertechnetate. Images in the A-P (upper panel) and in right anterior oblique (lower panel right) and left anterior oblique (lower panel left). The images show minimal uptake in the by the enlarged gland. There is normal uptake in the salivary glands These findings are consistent with a benign non toxic multinodular thyroid gland.
Courtesy: Ashley Davidoff, MD
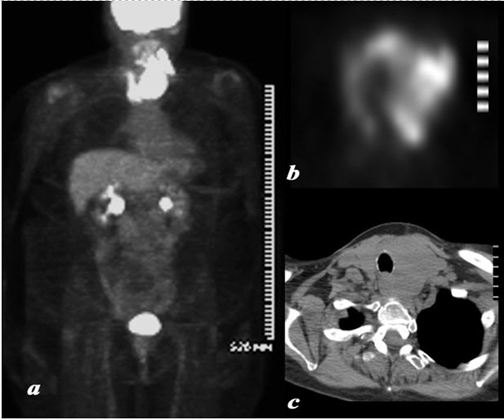
A large and very PET avid left lobe of the thyroid is demonstrated on the body PET (Positron Emission Tomography) scan shown in full body view in (a) and in transverse view of the thyroid (b). The patient is a 62 year female who had a biopsy proven lymphoma of the thyroid. The CT shows asymmetric and smooth and homogeneous enlargement of the thyroid. The findings are consistent with the final biopsy proven diagnosis of lymphoma.
Courtesy: Ashley Davidoff, MD
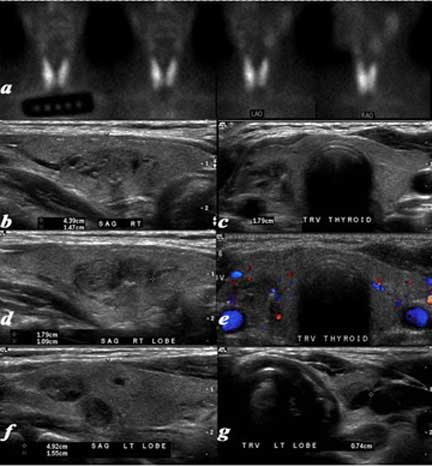
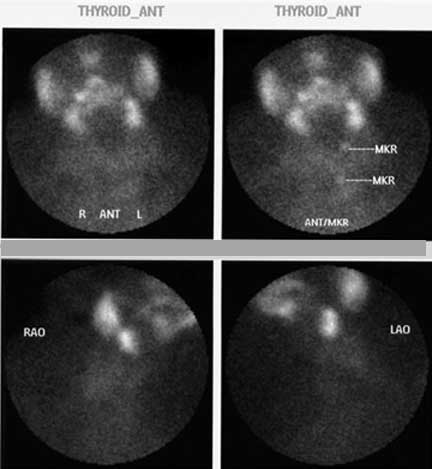
This is a thyroid scan from a 53 year old female with a clinical history of goiter. She was injected with Iodine -123. Twenty-four hours later radioiodine uptake was calculated at 31.8% (normal 8-35%). She was also injected with 14.2 mCi of 99m technetium pertechnetate. The scan (a) shows an enlarged gland bilaterally with uniform uptake of the radioisotope in both lobes of the thyroid gland. The uptake in the thyroid gland is normal relative to the uptake in the submandibular and parotid glands. These findings are consistent with a diffuse goiter. The ultrasound on the other hand shows a normal sized gland with multiple nodules. The right lobe (c,d) measures 4.4cm (length) X 1.5cm (A-P) X 1.8cm (TRV) and the left lobe (f, g) measures 4.9cm (length) X 1.6cm (A-P) X 1.1cm (TRV) In the right lobe there is a nodule in the middle of the gland (b, c, d, e) that is relatively hypovascular that measures 1.8cm X 1.1 cm (d, e). Two 7mm nodules were also seen in the left lobe (f, g) Whereas the thyroid nuclear scan was able to accurately depict function, the ultrasound was more accurate in defining the exact size and nodular character of the gland. The diagnosis based on imaging therefore was a non toxic multinodular normal sized gland.
Courtesy: Ashley Davidoff, MD
Diagnosis of Thyroid Diseases: Computed Tomography (CT)
CT scan is helpful in patients who have large goiters and the effect on structures such as the airway need to be evaluated. It is also helpful in establishing regional nodal disease and distant metastases, particularly small lung metastases. However, these are not mainstream concerns in thyroid evaluation and the role is limited.
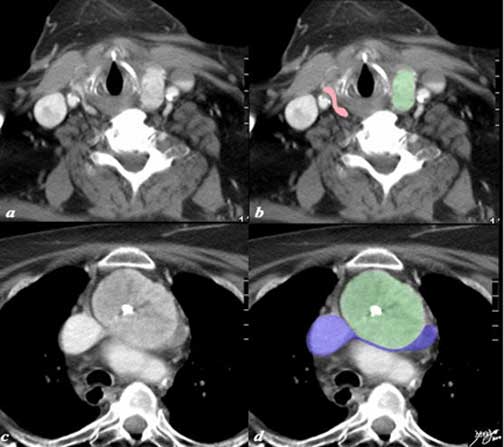
A large retrosternal goiter is seen extending down anterior to the aortic arch and brachiocephalic vein in this 86 year old female patient. In image a and b the atrophied left lobe of the thyroid is overlaid in pink, and the superior aspect of the goiter is overlaid in green. More inferiorly the goiter with central chunky calcification is noted compressing on the brachiocephalic vein (blue) There is mild diffuse almost homogeneous enhancement. The tracheobronchial tree is not affected by this goiter The findings are consistent with a calcified retrosternal thyroid goiter.
Courtesy: Ashley Davidoff, MD
Diagnosis of Thyroid Diseases: Magnetic Resonance Imaging (MRI)
MRI has limited utility in routine thyroid imaging.
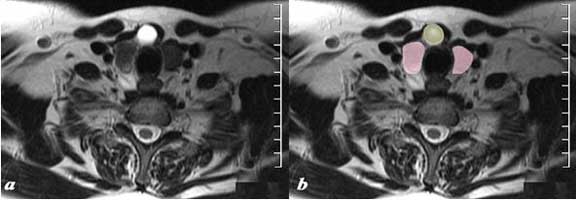
The MRI T2-weighted image through the inferior aspect of the thyroid gland (pink) shows a cystic structure (yellow), intensely T2 bright (a), in the region of the isthmus in the ventral and midline position of the gland. Findings are consistent with a thyroglossal duct cyst.
Courtesy: Ashley Davidoff, MD
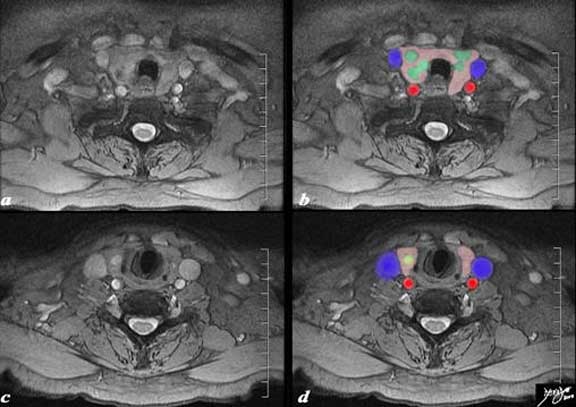
The MRI is from an 80 year old male presents with an asymptomatic multinodular goiter, consisting many nodules of varying size as identified by previous ultrasound. The MRI shows a normal size and shape to the gland but multiple non border forming nodules (green nodules) are identified within the matrix of the gland (pink). One of the nodules (c, d) overlaid in yellow is cystic in nature. It is bright on the STIR (Short T1 Inversion Recovery) sequence (c), a sequence with specific timing so as to suppress the fat. The internal jugular veins (blue) form a lateral neighbor and deform the relatively soft gland. The common carotid arteries (red) form a posterolateral relation to the gland. The trachea (black) is surrounded anteriorly and laterally by the gland. These findings are consistent with a non toxic multinodular thyroid gland, – not truly a goiter since the gland is not enlarged.
Courtesy: Ashley Davidoff, MD
Conclusion
The thyroid gland is a large gland by endocrine standards, but is small compared to most other organs in the body. For such a small organ it has a rather important responsibility to control the basic metabolic rate of the body. Structurally its shape is unique, and its superficial position makes it easy to examine both clinically and with imaging. Functionally its ability to store its products in an extracellular location is unique among endocrine organs.
The diagnosis of the hyperactive and hypoactive gland is fairly straightforward by evaluating serum T4 and T3, and TSH. Ultrasound is the workhorse for structural evaluation while nuclear medicine is the imaging workhorse of functional evaluation. The great affinity of the thyroid for iodine is used for targeted therapy as well, when functional, unwanted thyroid requires ablation with radioactive iodine 131. Its close relationship to the recurrent laryngeal nerves, esophagus and parathyroids requires meticulous technique in surgery.