
Learning Objectives
Describe the physiology of time and aging
Discuss pregnancy, ectopic pregnancy and spontaneous abortion
Describe how anatomy applies in clinical situations
Describe common disease conditions and symptoms
Explain how pathological conditions affect the uterus
Discuss treatment options
Introduction
The uterus, also known as the womb, is a hollow muscular organ that is part of the genitourinary system. It is characterized by its important role in the female reproductive system.
Part 2 of ‘Applied Anatomy of the Uterus’ will discuss common diseases to include alterations in the structure, which can be congenital or acquired, benign or malignant tumors. Systemic disease, especially infections, can also affect the uterus and uterine cavity. Diseases include fibroid disease, polyps, adenomyosis, cervical stenosis, and carcinoma. The more common disorders are the functional disorders that relate to cyclical events including menstrual cramps, endometriosis, dysmenorrhea, amenorrhea, and menorrhagia. Pain relating to the placement of an intrauterine device is also relatively common.
The developmental uterine anomalies may hinder conception and normal child birth. The changes in position could give rise to chronic pelvic pain. During childbirth there is a risk of injury to the urinary bladder as well as the anal sphincter as the uterus is anatomically closely related to these structures. The uterus may lose its support with age, repeated pregnancies and post menopause and may give rise to uterovaginal prolapse. Uterine fibroids are the most common benign tumors arising from the uterine myometrium. Uterine endometrium can stray and become ectopically placed in the myometrium giving rise to adenomyosis and when positioned in the ovaries or pelvis causing a condition called endometriosis.
The diagnosis of uterine diseases is dependent initially on clinical evaluation, while the most useful imaging modality is ultrasound. Clinically, symptoms include infertility, recurrent abortions, menorrhagia, acute or chronic abdominal pain and urinary complaints. The imaging modalities commonly used include ultrasound, MRI, hysterosalpingography, hysteroscopy and diagnostic laparoscopy.
Treatment options are guided by the disease process and may include hormonal treatment, minimally invasive surgery or open surgery.
The Uterus and Its Neighbors
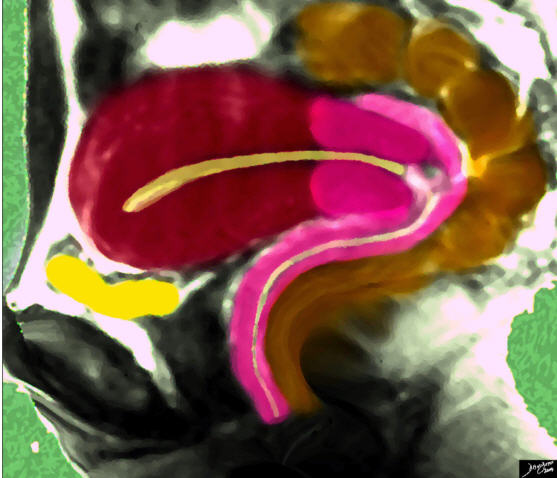
The sagittal diagram of the uterus shows the uterus surrounded by its neighbors, including the empty bladder (yellow) that lies anteriorly and inferiorly and the rectosigmoid colon (brown) that lies superiorly and posteriorly.
Ashley Davidoff MD
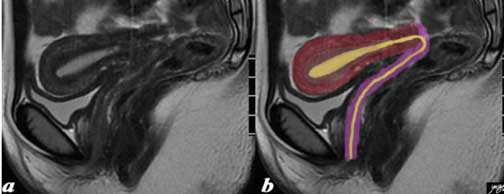
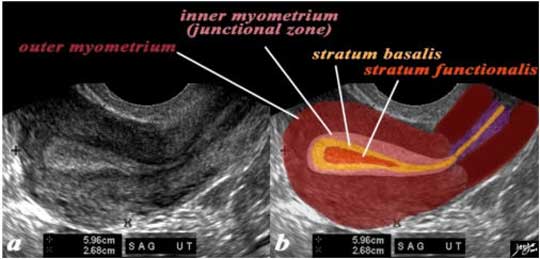
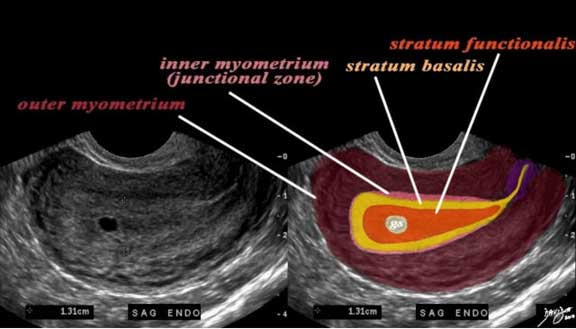
The normal sagittal view of the uterus is a T2-weighted MRI from a 16-year-old female with pelvic pain. It demonstrates that the uterus and more specifically the myometrium, is more complex and consists of an outer part (dark red) and an inner more homogeneous part called the junctional zone. Since a T2-weighted image is sensitive to water we understand from this image that the outer part contains more water, since it has foci of high intensity signal, likely related to greater vascularity. The junctional zone (light brown) and cervix are darker, related to greater fibrous tissue. The endometrial canal, cervical canal and vaginal cavity are outlined in yellow and have higher intensity related to higher water content. The vaginal wall is dark and overlaid in pink.
Images courtesy of Ashley Davidoff, M.D.
Time and Aging
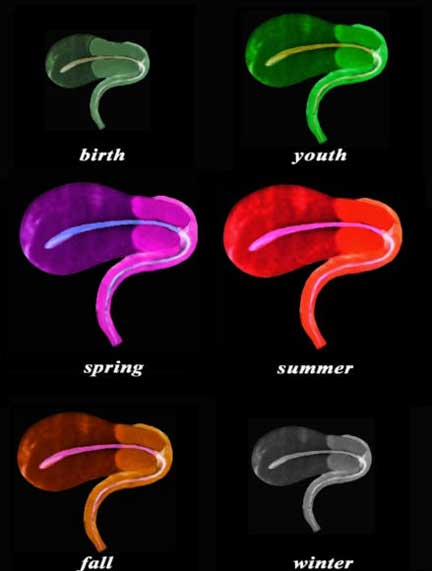
The sagittal diagram of the uterus and vagina through time shows an anteverted uterus at birth, through youth as it slowly matures and enlarges, entering spring as it reaches maturity, summer time when it bears fruit, and then through fall as it starts to involute in the postmenopausal period, and finally in its winter when it shrivels. In this view the uterus, vagina, and the internal cavity starting in the endometrial cavity, coursing through the cervix and then into the collapsed vaginal cavity is exemplified.
Images courtesy of: Ashley Davidoff, M.D.
In the fetus the uterus is contained in the abdominal cavity, projecting beyond the superior inlet of the pelvis and the cervix is considerably bigger then the body.
At puberty the uterus is pyriform in shape and weighs from 14 to 17 gm. It has descended into the pelvis, the fundus being just below the level of the superior aperture of this cavity.
The position of the uterus in the adult is prone to considerable variation, depending chiefly on the condition of the bladder and rectum. When the bladder is empty the entire uterus is directed forward and is at the same time bent on itself at the junction of the body and cervix, so that the body lies upon the bladder. As the latter fills, the uterus gradually becomes more and more erect, until, with a fully distended bladder, the fundus may be directed backward toward the sacrum.
During menstruation the organ is enlarged, more vascular, and its surfaces rounder; the external orifice is rounded, its labia swollen and the lining membrane of the body thickened, softer and of a darker color.
During pregnancy the uterus becomes enormously enlarged and in the eighth month reaches the epigastric region. The increase in size is partly due to growth of preexisting muscle and partly to development of new fibers.
After parturition the uterus nearly regains its usual size, weighing about 42 gms but its cavity is larger than in the virgin state; its vessels are tortuous and its muscular layers are more defined; the external orifice which was round in the nulliparous state may become slit like with one or more fissures.
In old age the uterus becomes atrophied and paler and denser in texture; a more distinct constriction separates the body and cervix.
Time and Aging: Embryology
In females, in the absence of MIS (Mullerian inhibiting substance) and androgens, the nephric (Wolffian) ducts degenerate and the paramesonephric (Mullerian) ducts give rise to the fallopian tubes, uterus, and upper two thirds of the vagina. The remnants of nephric ducts are found in the mesentery of the ovary as the epoöphoron and paroöphoron and near the vaginal introitus and anterolateral vaginal wall as Gartner’s duct cysts. The distal tips of the paramesonephric ducts adhere to each other just before they make contact with the posterior wall of the urogenital sinus. The wall of the urogenital sinus at this point forms a small thickening called the sinusal tubercle. As soon as the fused tips of the paramesonephric ducts connect with the sinusal tubercle, the paramesonephric ducts begin to fuse in a caudal to cranial direction, forming a tube with a single lumen. This tube, called the uterovaginal canal, becomes the superior portion of the vagina and the uterus. The unfused, superior portions of the paramesonephric ducts become the fallopian tubes (oviducts) and the funnel-shaped superior openings of the paramesonephric ducts become the infundibula.
Time and Aging: Function
The uterus has a vital role in reproduction. In the ?receive process export? model it receives the fertilized ovum, enables the growth and development of the fetus and then delivers the baby.
More specifically, the genital tract provides a system that allows the transport of the sperm, while the fallopian tubes provide a tract for the ovum and a site for fertilization; the endometrium provides a site for implantation; the uterus protects and accommodates the growing fetus until child birth and the placenta acts as a secondary endocrine organ and a liaison between mother and child to enable nourishment and removal of waste. During childbirth the muscular layer of the uterus helps in parturition.
The menstrual cycle is the system that allows for cyclical preparation of the endometrium for potential implantation. Although we have discussed this important event throughout the module we will repeat the discussion in the context of pregnancy, discuss more complex changes in the cervix during the cycle and will add clinical entities that reflect disordered menstrual cycles.
Time and Aging: Menstrual Cycle and Applied Physiology
The cyclical changes of the menstrual cycle present a continual change of events controlled by a series of integrated hormonal events. These changes are most easily observed in the endometrium by ultrasound. When performing a pelvic ultrasound, it is of the utmost importance to record the patient?s menstrual history.
Applied Physiology
During the menstrual phase (days 1- 4) the endometrium is thin and typically is seen as a single echogenic line by ultrasound examination, and measuring between 1-4 mm thick reflecting the early development of glands and stroma (Nalaboff). The junctional zone is irregularly thick and the myometrium loses water and thins.

Junctional Zone Prominent In Early Proliferative Phase
The normal sagittal view of the uterus is a transvaginal ultrasound in the first week after menstruation and just prior to the next proliferative phase. It demonstrates that the endometrium becomes a single, echogenic line consisting of opposing walls (orange) and is surrounded by a subendometrial halo of the junctional zone (reddish). This layer is more compacted and relatively hypovascular and is under the influence of progesterone which has just passed its peak. This image is typical of the early proliferative phase. It is during this time that estrogen starts to rise and progesterone has just fallen. The endometrium in this case measures about 3 mms.
Ashley Davidoff MD
Preovulation ? Proliferative Phase
In the proliferative phase (day 4-14) the endometrium thickens to 5-7 mm and becomes more echogenic than the myometrium. This reflects growth of the endometrial glands, blood vessels and stroma, stimulated by estrogen production by the ovarian follicles. This proliferative endometrium is structurally and functionally preparing for implantation of the fertilized egg. In the late proliferative phase (periovulatory phase) the endometrium becomes multilayered with an echogenic basal layer, hypoechoic inner functional layer and a thin echogenic line alongside the junctional zone of the myometrium and measures up to 11 mms. (Nalaboff).
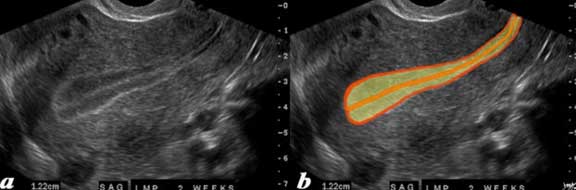
The normal sagittal view of the uterus in a transvaginal ultrasound, 2 weeks after menstruation and just prior to ovulation. It demonstrates that the uterus and more specifically the endometrium are more complex than just a simple columnar epithelium. This is an example of the trilaminar appearance of the endometrium and is characteristic of the appearance of the endometrium in the preovulatory phase. This phase is also called the follicular phase or proliferative phase. It is during this time that estrogen is the dominant hormonal influence. The appearance is also known as a “triple stripe” and conversely, its presence is seen before progesterone is produced. If present with a 9 mm+ diameter, it reflects an ideal potential lining for fertilization. In this case it measured 1.2 cm.
Ashley Davidoff, M.D.
Time and Aging: Changes in the Cervix – Pre Ovulation
The cervix is generally soft in the preovulatory phase and the external os is open and the mucus is like egg white ? thin and watery.

The ultrasound of the normal cervix (salmon pink) is from a 31-year-old female whose LMP was 12 days ago and it shows a fluid filled canal (yellow) surrounded by a thickened mucosa (purple). The lower uterine segment is seen cranially in red and the vagina is seen in pink caudally. At this stage the cervix is soft to clinical examination; the os is open and the cervical fluid is stretchy and thin like egg white.
Ashley Davidoff, M.D.
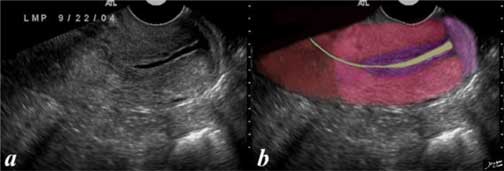
The ultrasound of the normal cervix (salmon pink) is from a 31-year-old female whose LMP was 12 days ago and it shows a fluid-filled canal (yellow) surrounded by a thickened mucosa (purple). The lower uterine segment is seen cranially in red and the vagina is seen in pink caudally. At this stage the cervix is soft to clinical examination; the os is open and the cervical fluid is stretchy and thin-like egg white.
Images courtesy of Ashley Davidoff, M.D.
Time and Aging: Ovulation
The transverse view of the uterus, 2 weeks after menstruation, reveals what appears to be a rupturing follicle with a comet tail at the site of the rupture, and a small collection of free fluid in close association with the comet tail. The pink overlay is the right ovary.
Courtesy of Ashley Davidoff, M.D.
Following ovulation the endometrium is under the influence of progesterone secretion by the corpus luteum. The endometrial glands fill up with mucus. The resulting appearance of the endometrium is a thick, echogenic structure (secretory phase). During the secretory phase (days 15-28) the endometrium is at it?s thickest in the mid-secretory phase and has a typical homogeneously, echogenic appearance. It usually measures between 7-16 mms. (Nalaboff)
The following series is taken in the postovulatory phase as the endometrium evolves into a secretory endometrium.
In this 26-year-old premenstrual female a transvaginal ultrasound in the sagittal plane reveals a normal view of the uterus with characteristic premenstrual appearance (a). The stripe is almost homogeneously echogenic and thick but also shows a hypoechoic halo of the junctional zone or inner myometrium (salmon). The homogeneous stripe is made up from two histological layers (barely distinguished by this ultrasound) ? the inner stratum functionalis (deep orange) that will shed once the spiral arteries vasoconstrict and the outer stratum basalis (deep yellow) that will not shed and will be the basis for regenerating the endometrium in the next cycle. The next layer as stated above is the compact myometrium – the junctional zone (also known as the inner myometrium) and is followed by the thicker outer myometrium (maroon) (b).
Images courtesy of: Ashley Davidoff, M.D.

In this 26-year-old premenstrual female a transvaginal ultrasound reveals a normal transverse view of the uterus with characteristic premenstrual appearance. The stripe is homogeneously echogenic and thick but also shows a hypoechoic halo of the junctional zone or inner myometrium (salmon). The homogeneous stripe is made up of two histological layers (not distinguished by this ultrasound): the inner stratum functionalis (deep orange) that will shed once the spiral arteries vasoconstrict and the outer stratum basalis (deep yellow) that will not shed and will be the basis for regenerating the endometrium in the next cycle. The next layer as stated above is the compact myometrium – the junctional zone (aka inner myometrium), and is followed by the thicker outer myometrium (maroon).
Ashley Davidoff, M.D.
The normal sagittal view of the uterus in a transvaginal ultrasound about 4 weeks after menstruation and just prior to the next menstruation when the endometrium is overripe. It demonstrates that the uterus and more specifically the endometrium are more complex than just a simple columnar epithelium. This is an example of the hyperechoic, homogeneous, thick endometrium characteristic of the secretory phase. It is during this time that progesterone is the dominant hormonal influence and estrogen influence is minimal. The endometrium in this case measures 1.2 cm.
Images courtesy of Ashley Davidoff, M.D.
Thus in summary, the cyclical changes of the endometrium range from a thin, echogenic line progressing to a multi-layered appearance in the preovulatory phase, becoming thick and homogeneously echogenic and then shedding. The changes in the cervix at the time of ovulation show a thin, simple fluid with an open external os. Just prior to menstruation the cervical fluid is thick and dry and complex appearing on ultrasound, but is echogenic and the external os is closed.
Time and Aging: Outer Myometrial Changes during Menstrual Cycle
The myometrium is thickest in the second half of the cycle – the mid-secretory phase, due to mild edema, but this is not easily observed by imaging techniques.
Junctional Zone Changes
During the mid-secretory phase the junctional zone thins out. It is most prominent when under the influence of progesterone and best seen during the menses and the earliest phases of the proliferative phase.
Menstruation
The menstrual cycle is a physiological process of the uterus caused by the cyclic rise and fall of estrogen and progesterone levels.
The result is growth and maturation of the endometrium followed by endometrial degeneration and shedding at menses.
The endometrium consists of two layers: the stratum basalis and stratum functionalis. It is the stratum functionalis that will either receive the fertilized ovum or shed. If there is no implantation then luteinizing hormone levels fall in the latter phase of the cycle and the level of progesterone falls, resulting in shedding of the endometrium.
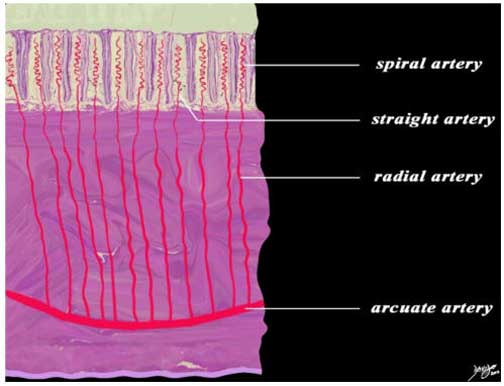
This diagram exemplifies the position of the arteries in the epithelial and muscular layers. The spiral arteries run in the stratum functionalis; the straight arteries run in the stratum basalis, while the radial arteries and the arcuate arteries run in the muscularis.
Ashley Davidoff MD
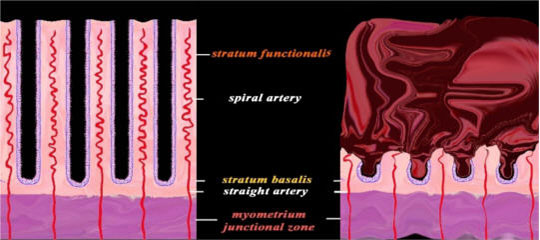
The diagram reflects the premenstrual endometrium (left) and the post menstrual endometrium right, revealing the necrosis of the functional layer with sloughing and hemorrhage. The basal layer with the straight arteries and a small portion of the spiral artery remains intact. The hemorrhage is controlled by spasm of the arteries and contraction of the myometrium. Courtesy of: Ashley Davidoff, M.D.

This patient presents with infertility. The hysterosalpingogram in the frontal view reveals a normal sized endometrial cavity filled with sloughed endometrium (dark maroon filling defects in b). The contrast has been overlaid in a lighter maroon to indicate blood. These are characteristic findings of menstrual products within the endometrial cavity. The fallopian tubes are patent.
Ashley Davidoff, M.D.

This adult patient presents with pain during menstruation. The transvaginal ultrasound in the sagittal plane reveals a slightly thickened and heterogeneous uterus with a sloughed endometrium (functional layer) appearing as the echogenic material within the endometrial cavity (brighter red). The hypoechoic dark regions are overlaid in a darker red reflecting blood in the cavity. These are characteristic findings of menstrual products within the endometrial cavity. The remaining stratum basalis is overlaid in orange. The junctional layer of the myometrium is not evident.
Ashley Davidoff, M.D.
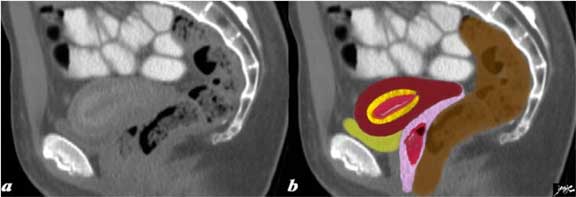
This adult patient presents with pain during menstruation. The CT in the sagittal plane reveals a hypodense endometrial cavity, presumably filled with blood (red) and surrounded by a hyperemic wall that likely represents the stratum basalis (basal layer ? yellow). A surrounding hypodense layer and then a relatively hyperdense outside layer are thought to represent the inner and outer myocardium. The vagina (pink) contains some complex tissue with air bubbles representing blood clots and endometrial slough (red). The bladder (yellow) is empty and the rectum is brown and lies posterior.
Ashley Davidoff, M.D.
Time and Aging: Imaging the Tampon

This 37-year-old female is actively menstruating and the air filled tampon is seen as a tubular structure in the pelvis directed to the patients left. It is overlaid in green in image b.
Ashley Davidoff, M.D.

This 42-year-old female is actively menstruating and the air filled tampon is seen as a tubular structure in the pelvis directed to the patients right. The reformatted CT scan in the coronal section shows an air filled tubular structure in the pelvis representing an air filled tampon in the vagina. The axial images (right) show the tampon as a black circle behind the bladder from its high point, behind the bladder to its inferior aspect in the perineum representing the position of the vagina.
Images courtesy of Ashley Davidoff, M.D.
Time and Aging: Disorders of Menstruation
Amenorrhea
Amenorrhea is a lack of normal menses. A woman who has never had a menstrual period has primary amenorrhea, while a woman whose menstrual periods have ceased has secondary amenorrhea.
There are many causes of amenorrhea. Primary amenorrhea is usually due to a condition present at birth. The most common cause of secondary amenorrhea is pregnancy.
The common result is cessation or lack of menses.
The structural and functional changes vary depending on the cause.
Women with primary amenorrhea generally present clinically in young adulthood when they fail to undergo menarche. Women may present with secondary amenorrhea anytime between menarche and menopause.
Diagnosis is based on clinical history. Secondary amenorrhea is diagnosed after cessation of menses for >6 months.
Treatment depends on the cause found at evaluation.
Oligomenorrhea
Oligomenorrhea is a term used for infrequent menstrual bleeding. The menses may be regular at long intervals or irregular.
There are many causes of oligomenorrhea, but the most common are chronic anovulation and polycystic ovarian syndrome (PCOS).
The result is menstrual bleeding occurring >35 days apart.
Structural and functional changes vary depending on the cause.
Women present clinically with infrequent menses. Women early in pregnancy may present with oligomenorrhea after they begin missing menstrual periods.
Diagnosis is based on clinical history and treatment is based on the cause found at evaluation.
Dysmenorrhea
Menstrual cramps or dysmenorrhea are cramps that occur during menses or more simply painful menstruation. They are caused by uterine muscle contractions which serve to evacuate the denuded mucosa and blood clots from the endometrial cavity. Primary dysmenorrhea is more common but dysmenorrhea may be associated with other pelvic disorders such as endometriosis, adenomyosis, pelvic inflammatory disease (PID) and adhesions in which case the dysmenorrhea may be more severe or prolonged.
Many women experience tolerable discomfort or pain but the pain can become incapacitating. Dysmenorrhea may be associated with excessive blood loss and this is known as menorrhagia.
From a structural standpoint the pain is caused by pressure receptors that sense the increased pressure during muscle contractions or by chemical receptors that may be incited by ischemia when contractions are excessive and temporary ischemia results.
Functionally, muscle contractions of the uterus are normal and are usually not felt. If the contractions are sufficiently strong, pressure receptors are activated or ischemia is induced by obstruction of the intramural arteries, causing the pain.
Clinically the pain presents as cramps during menses in the lower abdomen, usually in the suprapubic region, but may be periumbilical, left or right abdomen or may radiate down the thighs or occur in the back. Associate symptoms include nausea, vomiting, headache, weakness or even fainting. If the pain pattern changes or becomes more severe or the pelvic examination is abnormal then secondary causes should be sought and is best done by starting with an ultrasound of the pelvis.
Treatment is commonly with NSAIDS (non steroidal anti inflammatory agents) or a COX-2 inhibitor. For some patients hormonal contraceptives prove effective. Secondary causes of dysmenorrhea may require surgery.

The longitudinal view of the uterus is shown in the ultrasound of this young patient who was having severe pain during her menses. The images show part of the endometrial lining within the lumen (maroon) with a small amount of blood (bright red) and the remaining endometrial lining (pink). The denuded endometrium and associated clots cause prostaglandins to be released which induce muscle contraction and these are the primary cause of the pain.
Courtesy of Ashley Davidoff, M.D.
Time and Aging: Disorders of Menstruation Continued
Menorrhagia
Menorrhagia is excessive bleeding at menses with multiple causes.
The most common causes of menorrhagia are benign uterine polyps or fibroids. However, menorrhagia may also have more serious causes including bleeding disorders or uterine cancers.
The result is a prolonged period of menstruation (>7 days) or excessive blood flow at menses (>80 cc/cycle).
Structural changes vary depending on cause.
Functional changes also vary with cause, but always include excessive bleeding, giving women their common clinical presentation. Women with menorrhagia often describe soaking through a menstrual pad every hour during menses.
Diagnosis is based on clinical history and treatment depends on the cause found at evaluation.
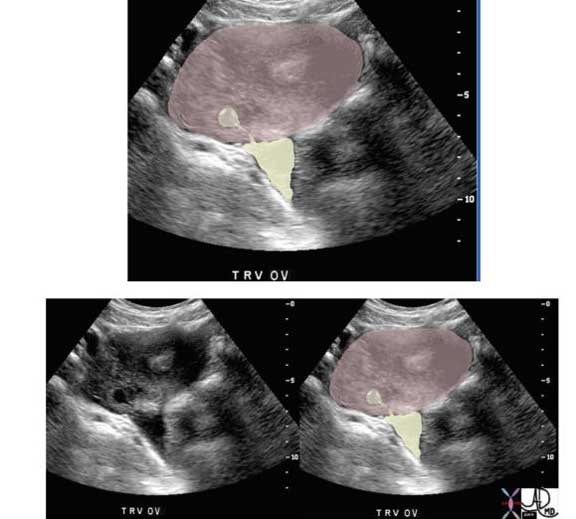
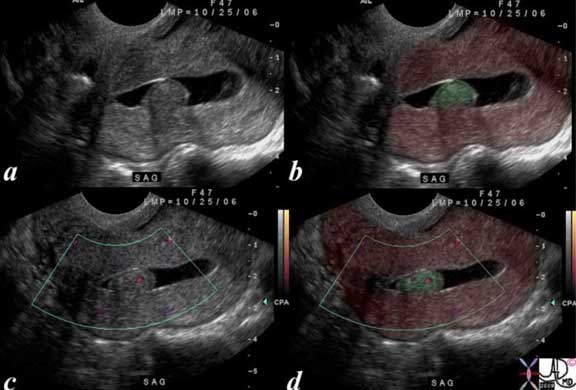
CT axial images (top) and sagittal reconstructions (bottom images) of a young woman show a retroverted uterus with an enhancing filling defect (green overlay in b) in the endometrial cavity (yellow).
These findings are consistent with either an endometrial polyp or a submucosal fibroid. Endometrial carcinoma is a remote possibility.
Endometrial fluid = yellow
Polyp = green
Myometrium = pink
Ashley Davidoff, M.D.
Metrorrhagia
Metrorrhagia is uterine bleeding between menses with multifactorial causes including benign endometrial and cervical polyps, as well as endometrial and cervical cancers.
The result is uterine bleeding between menses in an amount less than or equal to menstrual flow.
Structural and functional changes vary depending on cause. Women present clinically due to their bleeding between menses.
Diagnosis is based on clinical history and treatment depends on the cause found at evaluation.
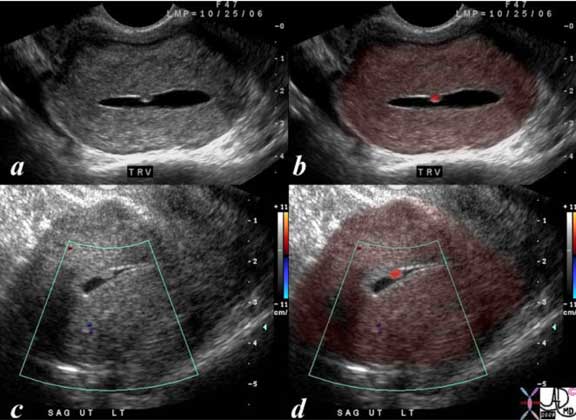
The transvaginal ultrasound is from a 50-year-old perimenopausal female with metrorrhagia. The uterine cavity and cervical cavity are filled with fluid and soft tissue elements are identified in the expanded cervical canal. The findings are consistent with cervical stenosis, but the cause of the metrorrhagia is not obvious. The stenosis was relieved and follow up ultrasound showed resolution. No cervical mass was identified.
Images courtesy of Ashley Davidoff, M.D.
Pregnancy
Pregnancy is a physiologic process caused by the fusion of two gametes after sexual intercourse.
This fusion, called fertilization, takes place in the fallopian tubes and the result is a zygote, a diploid cell that will grow into an embryo.
The function of every biological unit in the body is based on its ability to receive a product, process it and deliver the new product efficiently and effectively to where it is used and needed. The primary function of the uterus is to receive the fertilized egg, support its growth and development throughout gestation and ultimately deliver a well-formed, viable neonate.
Fertilization begins with the ovum being released from the ovary. At the time of ovulation the ovum is fixed within the process of meiosis at the metaphase II stage. It is surrounded by the zona pellucida, a layer of mucopolysaccharide and the cumulus oophorus, a layer of granulosa cells from the ovarian follicle. The ovum is swept up by the fimbriae of the fallopian tubes. If sexual intercourse occurs around the time of ovulation, sperm are released and move from the vagina through the cervical mucus into the uterus and fallopian tubes. The sperm move toward the ovum through a chemical attraction called chemotaxis. In the uterus, the sperm undergo capacitation, a reaction that makes the sperm membrane more permeable and better able to fuse with the oocyte membrane. When the sperm reach the ovum in the fallopian tube they undergo the acrosome reaction, releasing enzymes from the sperm head that allow it to pass through the zona pellucida.
Ashley Davidoff MD
The sperm membrane fuses with the oocyte membrane and the sperm head, containing the gamete?s genetic material, passes into the cytoplasm of the oocyte. The oocyte completes its second meiotic division and the result is a diploid zygote containing two pronuclei, membrane bound structures each containing a maternal or paternal set of chromosomes. The membranes of these pronuclei dissolve and the chromosomes from the sperm and oocyte pair in preparation for the zygote?s first mitotic division. This cell will divide multiple times as the embryo travels through the fallopian tube into the uterine cavity. This process usually takes 3-4 days after fertilization.
As the embryo travels into the uterus, its cells grow, divide and begin to differentiate. The first cells to differentiate are the trophoblastic cells, cells that will become the placenta. Enzymes from the endometrial glands digest the remaining zona pellucida in order to allow these cells to attach to and invade the endometrium. These cells proliferate within the endometrium, invading the small capillaries to form the vascular sinuses of the early placenta. Through these venous sinuses, the cells of the growing placenta secrete progesterone and HCG, which allows detection of the pregnancy with laboratory testing.
After implantation the embryo grows and the cells continue to differentiate. Around the third week of gestation, the cells differentiate into ectoderm, endoderm and mesoderm. The endoderm will develop into the gastrointestinal and respiratory tracts. The mesoderm will differentiate into the cardiovascular, genitourinary and musculoskeletal systems. The ectoderm will form the nervous system, skin and sensory organs. Organogenesis occurs between the 4th and 7th week of gestation. After the 8th week of gestation, the embryo is called a fetus. This fetus will grow and develop within the uterus over 40 weeks of pregnancy. The placenta will grow and invade the arterioles of the endometrium to connect maternal and fetal circulation.
Uterine physiology is influenced by hormones from the hypothalamus-pituitary-ovarian axis. The uterus undergoes many functional changes in pregnancy in the processes of implantation, gestation and childbirth.
Pregnancy: Imaging Pregnancy
As early as the 4th week of pregnancy the gestational sac may be visualized by transvaginal ultrasound. At this stage the gestational sac already contains the yolk sac, embryonic disk and amnion but these structures are too small to be visualized. An echogenic ring surrounding the cystic gestational sac represents the decidua.
Using transvaginal ultrasound the sac may be seen at ß-HCG levels as low as 800 mIU/mL but should be identified when the level is 2,000 mIU/mL (Paul).
Using the transabdominal technique the gestational sac should be visualized when the ß-HCG level is approximately 3,600 mIU/mL (Nyberg, Dashefsky).
Beta HCG levels usually double approximately every 2 days for the first four weeks of pregnancy (Ashitaka). Subsequently by 6 to 7 weeks gestation beta HCG levels may take as long as 3 1/2 days to double (Pittawy). In 15% of normal pregnancies doubling time in early pregnancy may be more than 2 to 3 days. On the other hand in ectopic pregnancy, normal doubling times may be present.
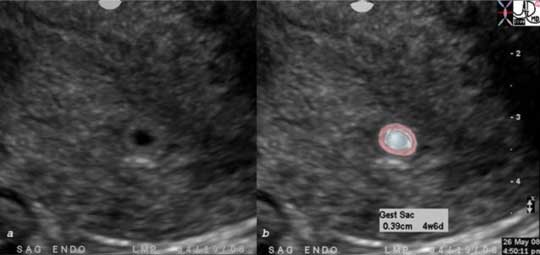
The transvaginal ultrasound in the sagittal plane reveals a magnified view of the uterus with an early pregnancy, characterized by the gestational sac (pale blue in b). The gestational sac measures .39 mm which corresponds to a gestational age of 4 weeks and 6 days. The echogenic ring around the gestational sac represents the decidua. A vague double sac sign is suggested. (Bradley)
Ashley Davidoff MD
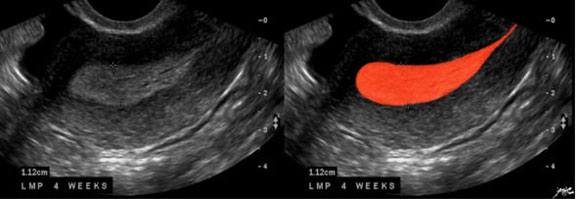
In this 16-year-old patient her LMP was just over 4 weeks ago and she had a positive pregnancy test. The transvaginal ultrasound in the sagittal plane reveals a normal view of the uterus with characteristic early pregnancy appearance, characterized by the gestational sac (gs) embedded in the stratum functionalis (deep orange). The stratum basalis is seen as a slightly more echogenic layer around the functional layer (deep yellow). The stripe is thick measuring about 1.3 cm. The next layer is the barely seen junctional layer (salmon pink) best seen on the anterior, subendometrial layer just beyond the basalis. The next layer is the thicker outer myometrium (maroon) that contains dilated vessels. The echogenic ring around the cystic sac represents the decidua. Images courtesy of Ashley Davidoff, M.D.
During gestation, as the myometrium hypertrophies it also becomes more contractile. In the first trimester the uterus begins having infrequent uncoordinated contractions. These contractions are mild and usually go unnoticed. As pregnancy progresses the contractions increase in intensity and frequency. These contractions become more regular toward the end of the third trimester and become rhythmic as labor begins.
Pregnancy: Processing: Growth and Nourishment
Throughout gestation the uterus grows to accommodate the developing fetus. The myometrium becomes more muscular and elastic. The uterus stretches to 500 times in size, thinning the uterine wall. As the nutritional needs of the fetus increase, the uterine blood supply hypertrophies to increase blood flow in the maternal-fetal circulation.
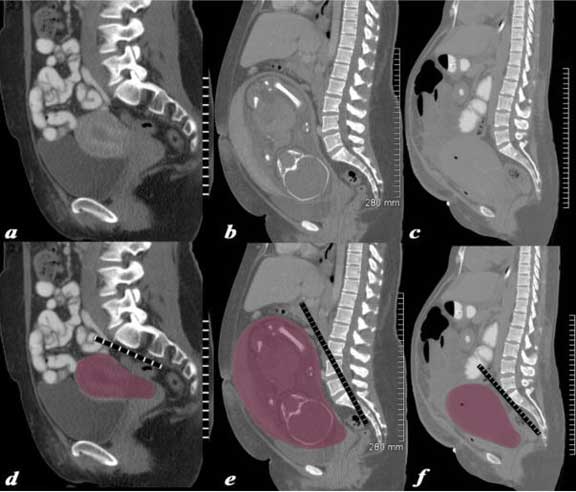
The series of CT scans from different patients are reconstructed in the sagittal plane to show the mature uterus in the non-gravid state (a,d), with a 32 week pregnancy (b,e), and in the postpartum, post cesarean section state (c,f). In the nongravid adult the uterus in the craniocaudad span (C-C) measures about 8.5 cms and in the anteroposterior (A-P) dimension it measures 4.5 cm. The uterus containing the 32 week pregnancy measures 24 cms (C-C) by 16 cms (A-P). In the post cesarean section patient the uterus measures 17cm (C-C) by 9 cms (A-P).
Ashley Davidoff MD
Pregnancy: Labor
Labor is uterine contractions leading to cervical changes caused by contraction of the myometrium in response to the hormone oxytocin. The result is delivery of the fetus and placenta. Between the 36th and 40th week of gestation the irregular contractions of the myometrium become rhythmic. The membranes surrounding the fetus and amniotic fluid rupture. The cervix effaces and dilates up to 10 cm in diameter. As the cervix dilates, the plug of cervical mucus is expelled resulting in the bloody show. The fetus descends into the pelvis and rotates as the strengthening, rhythmic contractions of the uterus propel the fetus through the birth canal. After delivery of the neonate, uterine contractions continue delivering the placenta.
During labor and delivery the uterus undergoes several important structural and functional changes. The cervix dilates and effaces allowing the fetus to pass. The myometrium contracts rhythmically to deliver the neonate and placenta. After childbirth, the uterine vasculature constricts and the myometrium contracts to stop postpartum bleeding.
As labor begins, there is an increase in the number of oxytocin receptors on the myometrial smooth muscle cells. Release of the hormone oxytocin from the posterior pituitary stimulates the strong rhythmic contractions of the myometrium. There is also an increase in the number of gap junctions connecting the smooth muscle cells. As a result, the contraction of the myometrial smooth muscle cells becomes more coordinated. In the cervix, increased prostaglandin levels lead to increased expression of enzymes called matrix metalloproteinases. These enzymes break down cross-linking bonds between collagen fibers.
Simultaneously, cervical hyaluronic acid content increases. These processes cause the softening, effacement and dilation of the cervix. Once the cervix is dilated, rhythmic myometrial contractions move the fetus through the birth canal. The ligaments of the pelvis relax to allow widening of the pelvic outlet, allowing the fetus to pass. After the delivery of the neonate and separation of the placenta, constriction of the uterine vasculature prevents maternal blood loss. Contraction of the myometrium also compresses the arterioles that fed the placenta to prevent blood loss.
Pregnancy: Childbirth
At child birth there is an increasing concentration of oxytocin secreted by the posterior pituitary. There is an increased concentration of prostaglandins while PGE2 brings about softening of the cervix; PGF2 cause contractions. Oxytocin causes the rhythmic contractions manifested as labor pains. The intermittent nature of these contractions helps in child birth without jeopardizing the blood supply to the uterus. Uterine fibers are in different layers: the external layer is arranged transversely, the middle layer is irregular, while the inner layer is like a submucosal muscular layer. The lower segment and cervix are in circular formation. During labor the upper uterine segment contracts and retracts which essentially means that fibers get smaller after each contraction. This action propels the fetus downwards. The lower segments and cervix, on the other hand, dilate with each contraction.
Pregnancy: Post Partum
During the postpartum period the middle muscular layer, which has oblique fibers and a maximum number of vessels, prevents excessive blood loss as criss cross fibers across the vessels act as living ligatures.
Some disorders resulting from aberrant fertilization and implantation include infertility, miscarriage and ectopic pregnancy. Diagnosis is made based on clinical history, physical exam and imaging with ultrasound. Treatment of infertility can include induction of ovulation with hormones, intrauterine insemination or in vitro fertilization. Miscarriage may require no treatment, but dilation and curettage is often used to ensure full removal of the products of conception. Ectopic pregnancy may be treated medically, with methotrexate or surgically with removal of the ectopic gestation.
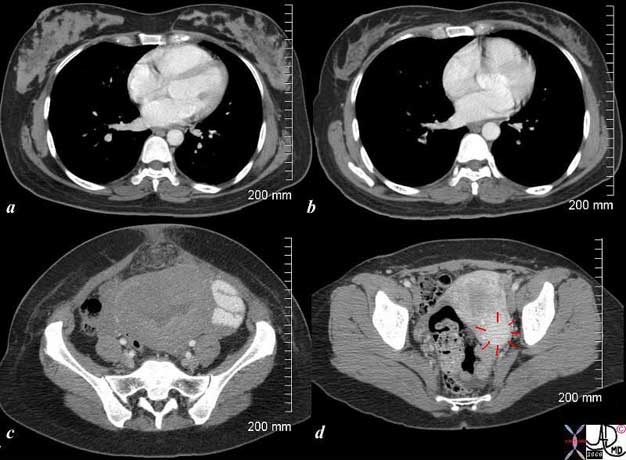
The CT scan is from a 26-year-old female showing breasts and uterus in a post partum post cesarean section state (a,c) and then 18 months later (c,d). The transverse dimension of the uterus in the post partum state is about 11 cm, while 18 months later is about 5 cm. Her breasts in the post partum state are enlarged with prominent glandular tissue (a) and 18 months later are reduced in size and glandular volume (b). Surgical footprints are noted in the subcutaneous tissue in (c) following her cesarean section. A cervical fibroid (red arrows) is suggested post partum image (d). Courtesy of Ashley Davidoff, M.D.
Pregnancy: Complications
Pregnancy complications that occur around or during labor and delivery include placental bleeding, uterine rupture, premature rupture of membranes or labor, cephalopelvic disproportion and malpresentation. Diagnosis of these conditions is made based on clinical history, exam and imaging with ultrasound. Treatment of placental bleeding (placenta previa or placental abruption) depends on the severity of bleeding. Premature rupture of membranes is often treated with antibiotics and sometimes induction of labor. Preterm labor is treated with tocolysis and steroids to promote fetal lung maturity. Uterine rupture is a medical emergency treated with immediate laparotomy and cesarean delivery. Cephalopelvic disproportion and malpresentation both often require cesarean delivery.
Congenital Disorders
There are many congenital disorders resulting from aberrant growth and development of the fetus. Some disorders resulting from uterine dysfunction during gestation include spontaneous abortion and cervical insufficiency. Diagnosis of these conditions is made by clinical history and exam combined with ultrasound imaging during pregnancy. Often no treatment is necessary for spontaneous abortion. Women with recurrent abortions should be tested for uterine structural abnormalities as well as gynecologic infections. Cervical insufficiency may be treated expectantly with steroids to promote fetal lung maturity and bed rest. Cervical cerclage may also be used to treat cervical insufficiency.
Ectopic Pregnancy
Ectopic Pregnancy is a disorder where a gestation is located in a location other than the uterus, most commonly in a fallopian tube, but can occur on an ovary or intra-abdominally. It is characterized by pelvic pain associated with vaginal bleeding and a positive pregnancy test. Predisposing factors include previous ectopic pregnancy and pelvic infections (such as Pelvic Inflammatory Disease (PID)).
The most common location of an ectopic pregnancy is in a fallopian tube, most commonly in the ampullary portion but can occur in the adnexa or rarely in the peritoneal cavity.
Ectopic pregnancy can result in serious complications including hemodynamic instability and death.
The classic clinical presentation of ectopic pregnancy includes amenorrhea (no periods for more than 6-7 weeks), pelvic pain and vaginal bleeding. Many patients do not have this classic presentation, however. Anytime a woman presents with pelvic or abdominal pain associated with amenorrhea, one must consider ectopic pregnancy. A positive pregnancy test along with a normal or slightly enlarged, often tender uterus or adnexal mass is highly suggestive of ectopic pregnancy. However, no combination of physical findings can definitively diagnose an ectopic pregnancy.
The diagnosis is suspected clinically by a positive pregnancy test, pelvic pain and/or vaginal bleeding. It is confirmed by characteristic changes in the f Beta-HCG levels and ultrasound findings.
An ectopic is suspected if the HCG is greater than 1500 and there is no evidence of an intrauterine gestational sac on transvaginal ultrasonography. On transvaginal ultrasonography an ectopic is suspected if an intrauterine pregnancy is not detected with an HCG level of greater than 6500. In a normal pregnancy the HCG level typically will double every 48 hours in early pregnancy but will not in ectopic pregnancy. Typically, the HCG will go do down in spontaneous abortion (SAB). Sometimes, a serum progesterone level can also be helpful in determining the viability of a pregnancy but generally is not considered as reliable a marker as an HCG.
The differential diagnosis includes multiple conditions which can cause acute pelvic pain including pelvic inflammatory disease (PID), spontaneous abortion (SAB), appendicitis and kidney stones. In pelvic inflammatory disease, kidney stones and appendicitis, pregnancy testing is typically negative and vaginal bleeding is less likely. Perhaps most difficult to differentiate are spontaneous abortions from ectopic pregnancies. On physical exam, there may be pregnancy tissue present in the os in a spontaneous abortion which is typically not the case with an ectopic pregnancy. Also, the ultrasound findings may be different and the serum HCG level typically falls more quickly with a SAB.
Ectopic Pregnancy : Imaging
uterus-P-084.jpg
Right Sided Ectopic PregnancyThis 25-year-old female presented with a positive HCG which doubled in 48 hours. The uterus showed proliferative endometrium but no intrauterine pregnancy. Within the right adnexa, alongside the right ovary a rounded echogenic structure with a cystic central cavity was identified (red overlay in b). This structure measured 1.9 by 2 cms and appeared to contain both a gestational sac and a yolk sac. Based on the size of the gestational sac the projected gestational age was 5 weeks and 2 days. These findings were consistent with an ectopic pregnancy
Ashley Davidoff MD

This 25-year-old female presented with a positive HCG which doubled in 48 hours. The uterus showed proliferative endometrium but no intrauterine pregnancy. Within the right adnexa, alongside the right ovary a rounded echogenic structure with a cystic central cavity was identified (red overlay in b). This structure measured 1.9 by 2 cms and appeared to contain both a gestational sac and a yolk sac. Based on the size of the gestational sac the projected gestational age was 5 weeks and 2 days. These findings were consistent with an ectopic pregnancy
Ashley Davidoff MD
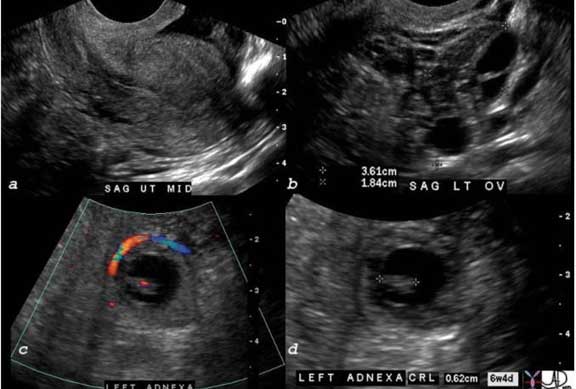
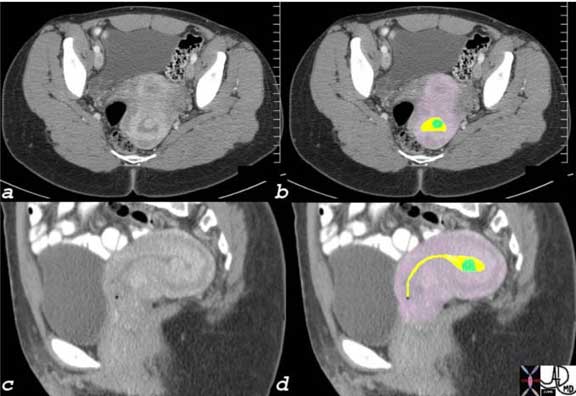
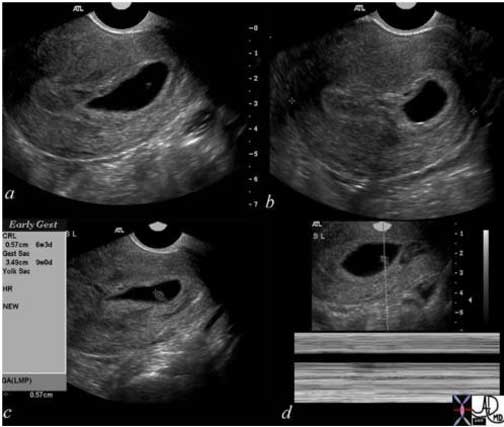
This 32-year-old female presents with abdominal pain and pelvic pain with a positive HCG uterus and no intrauterine pregnancy. There was complex free fluid in the cul de sac probably blood and hemorrhage seen in the top right hand corner of image a. In image b a normal left ovary was identified and in image c a viable fetus was seen in the left adnexa with fetal Doppler flow and a heart beat. In image d a crown rump length of .62 cm was measured corresponding to a gestational age of 6 weeks and 4 days. The findings are consistent with a diagnosis of a left sided ectopic pregnancy.
Ashley Davidoff MD
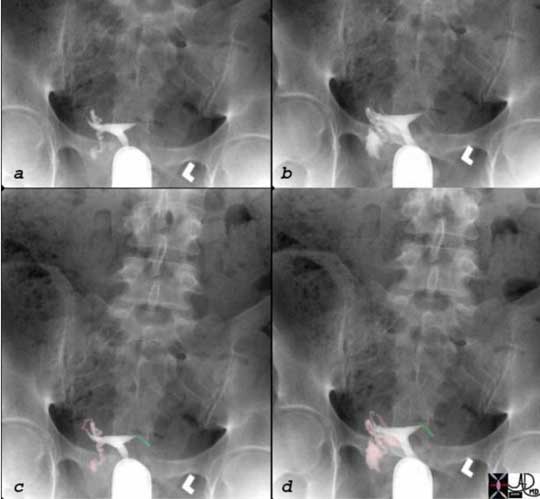
This 32-year-old female had a history of left-sided ectopic pregnancy resulting in surgery and removal of the ectopic. As a result the fallopian tube became obstructed and during the hysterosalpingogram no spillage of contrast is seen from the truncated left fallopian tube (green in c and d) while free spillage is seen on the right side (pink in c and d).
Images courtesy of Ashley Davidoff, M.D.
Ectopic Pregnancy : Treatment and Management
There are several treatment options and the appropriate selection depends on the clinical conditions. The options include expectant management, medical management and surgical management. Expectant management: sometimes if the pregnancy is early (with a serum HCG of < 1000 and declining) and the gestation is small (less than 3 cm) and there is an absent fetal heartbeat, expectant management with close follow-up may be considered. If the patient is hemodynamically stable, it may be possible to treat the ectopic medically. Medical management typically involves methotrexate. Methotrexate is a chemotherapeutic agent which inhibits folate metabolism, therefore inhibiting the growth of rapidly dividing cells such as a new gestation. Surgical intervention typically involves laparoscopic surgery and most recently tubal incision to remove the gestation. Surgery is chosen for the unstable patient, larger, more advanced pregnancies and for medical treatment failures.
Generally, the prognosis of ectopic pregnancy is good if it is diagnosed in a timely fashion. However, this serious condition is also one of the most common causes of maternal death and infertility.
Spontaneous Abortion
Spontaneous abortion is the expulsion of a non viable embryo or fetus usually caused by chromosomal aberrations or environmental factors, occurring before the 20th week, though most occur before 12 weeks.
Structural changes that can lead to spontaneous abortion include uterine septae and anatomic anomalies like bicornuate uterus. Spontaneous abortions in the first trimester usually occur due to chromosomal anomalies of the fetus.
However, functional changes due to maternal infection or toxin exposure can lead to spontaneous abortion in the second trimester.
There are 4 clinical entities including threatened, inevitable, incomplete and complete spontaneous abortion.
Clinically threatened abortion is diagnosed and characterized by some bleeding and sometimes accompanied by pain in the first trimester. About half of these patients will recover and proceed to full term pregnancies.
When the symptoms are accompanied by a dilated cervix then abortion becomes “inevitable”. Bleeding and cramps are usually more prominent with inevitable abortion. The presence of products of conception in the discharged blood warrants examination by ultrasound. If products of conception are identified in the endometrial cavity the diagnosis is compatible with incomplete abortion and their absence confirms the diagnosis of a complete spontaneous abortion. Pain and bleeding subside when the abortion is complete.
Treatment depends on the stage of the the spontaneous abortion. A complete abortion requires no further treatment. An incomplete or inevitable abortion before 13 weeks is treated with suction dilatation and curettage though medical therapy (misorostol) can be used.
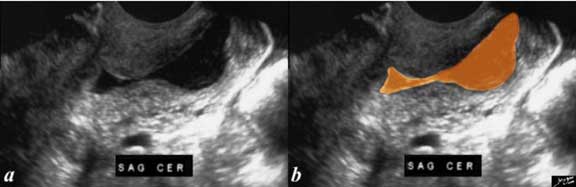
The history is one of a young female presenting with vaginal bleeding with previous positive pregnancy test. The images show a deformed gestational sac bulging into the cervix. By ultrasound the gestational sac measured 3.49 cm consistent with GA of 9 weeks and CRL measures .49 cm consistent with a gestational age of 6 weeks and 3 days. No fetal heart was identified. An evolving spontaneous abortion was diagnosed.
Ashley Davidoff MD
Diseases
We will now review diseases of the cervix, uterus and fallopian tubes.
Diseases of the Uterus and Cervix: Fibroids
Uterine fibroids (leiomyomas) are benign tumors of the myometrium and are the most common female reproductive tract tumor. They occur in women of reproductive age.
Fibroids are caused by clonal proliferation of a single smooth muscle cell in response to estrogen and progesterone. Because their growth is hormone-responsive, they typically regress with menopause.
The structural changes are characterized by single or multiple masses of smooth muscle cells, with some fibrous tissue, within the myometrium. The masses may protrude into the uterine or abdominal cavities. Fibroids vary greatly in size and rarely may grow large enough to fill the abdomen and compress the abdominal organs.
The functional changes are variable and depend on fibroid location and size. For many women the functional change is minimal. However, fibroids that project into the uterine cavity and distend the endometrium may cause increased menstrual bleeding as well as infertility.
Clinically, many women with fibroids are asymptomatic and present clinically with incidental findings on imaging. However, women with multiple or larger fibroids may present with menorrhagia, pelvic pain, infertility or an irregular abdominal mass. Fibroids that outgrow their blood supply can undergo infarction and necrosis causing sudden severe pain.
Imaging evaluation of fibroids is usually done with ultrasound. MRI is useful in evaluation if ultrasound is non-diagnostic.
Diagnosis is made with findings on physical exam and imaging.
Treatment is variable depending on size and symptoms. Asymptomatic women with small fibroids can be managed with observation. Fibroids causing pain or infertility can be removed with laparoscopic or open myomectomy. The blood supply of large individual fibroids can be targeted with uterine artery embolization. Women with large or symptomatic fibroids who have finished childbearing may be treated with hysterectomy.
Diseases of the Uterus and Cervix: Fibroids Impinging on the Endometrium ? MRI
Fibroids are common and most commonly located only in the muscular portion of the uterus. When they are purely intramural they do not cause dysfunctional uterine bleeding (DUB). When they impinge on the endometrium they can be the cause of both DUB and infertility if large enough.

In this sagittal view of a T2-weighted MRI of the uterus of a 42-year-old female with multiple fibroids, two of which impinge on the endometrial cavity (the larger – light green) from posterior and the smaller (dark green) from anterior resulting in a sigmoid shaped cavity (yellow). In addition, incidentally noted Nabothian cysts (orange) are seen within the cervix.
Images courtesy of Ashley Davidoff, M.D.

In this sagittal view of the T2-weighted MRI of the uterus of a 46-year-old female an almost 6 cm, slightly hyperintense fibroid is seen pushing on the endometrial cavity from above. This patient has a large fibroid that impinges on the endometrial cavity.
Images courtesy of Ashley Davidoff, M.D.
Diseases of the Uterus and Cervix: Small Submucosal Fibroid Demonstrated by Sonohysterogram
A sonohysterogram is performed by inserting a small catheter into the endometrial cavity via the cervix and injecting normal saline into the endometrial cavity, which acts as a contrast agent to outline the cavity and then, using ultrasound to evaluate the cavity. Normally the cavity is smooth. Abnormal bleeding is usually the indication for the sonohysterogram and defects caused by polyps or submucosal fibroids become obvious even when small.
The ultrasound (sonohysterogram) scan is from a 41-year-old female who presents with dysfunctional uterine bleeding. The study reveals a 4 mm submucosal nodule, shown at pathology to be a submucosal fibroid.
Courtesy of Ashley Davidoff, M.D.
Diseases of the Uterus and Cervix: Fibroids – Hysterosalpingogram
A hysterosalpingogram is performed by inserting a small catheter into the endometrial cavity via the cervix and injecting water soluble contrast into the endometrial cavity, which acts as a contrast agent to outline the cavity and then using fluoroscopy to evaluate the cavity and integrity of the fallopian tubes. Normally the cavity is smooth and the contrast spills into the peritoneal cavity, confirming patency. Infertility is usually the indication for the sonohysterogram and obstructed tubes or other causes such as congenital abnormalities or submucosal fibroids become obvious even when small.

This 38 year-old-female presents with a history of infertility. The hysterosalpingogram shows non filling of both fallopian tubes and a filling defect (green) in the region of the patient?s left cornu that likely is the cause of the obstructed left tube and in part the cause of the infertility. The lesion is most likely a submucosal fibroid.
Courtesy of Ashley Davidoff, M.D.
Diseases of the Uterus and Cervix: Hyperplasia Ultrasound
Endometrial hyperplasia is a proliferative growth of the endometrium usually caused by high levels of estrogens combined with insufficient levels of progesterone. The excessive estrogen may be exogenous or endogenous. The association between tamoxifen, an anti estrogen hormone used in the treatment of estrogen dependent breast cancer, can result in endometrial hyperplasia and has been associated with the development of endometrial cancer. Endometrial hyperplasia is precancerous and therefore must be diagnosed and treated when recognized. The diagnosis is suggested by a thickened endometrium. In the post menopausal woman the endometrium should not be thicker than 4 mms. The diagnosis is confirmed by dilation and curettage (D&C). It is treated hormonally but when the histology is concerning for atypia or cancer then it is treated like endometrial cancer and hysterectomy may be performed.
Diseases of the Uterus and Cervix: Polyps
Endometrial polyps are benign growths of the endometrium which occur most commonly in middle-aged women.
The cause of most endometrial polyps is unknown. However, they have been associated with the use of the drug Tamoxifen, as well as hypertension and obesity.
The result is a growth of endometrial glands and stroma projecting from the internal uterine surface. The structural change is characterized by a mass of endometrial glands and fibrous stroma that surrounds a core of large vascular channels. This mass usually arises from the uterine fundus and projects from a stalk into the uterine cavity.
The functional change associated with endometrial polyps may be minimal or limited to abnormal uterine bleeding. However, there is some evidence that removal of endometrial polyps may improve fertility.
Endometrial polyps present clinically with abnormal uterine bleeding. This bleeding is most often light bleeding between periods (metrorrhagia), but can also manifest as heavy or extended bleeding at menses (menorrhagia).
Imaging with ultrasound is useful in the initial investigation of abnormal uterine bleeding, and sonohysterography is the most effective imaging modality for endometrial polyps.
Diagnosis of a benign polyp depends on histologic examination to rule out malignancy.
Treatment of endometrial polyps is surgical excision with hysteroscopy, followed by curettage. Although endometrial polyps are benign, there is a small risk of malignancy arising in a polyp, so removal of large (>1 cm) or symptomatic polyps is recommended.
The ultrasound (hysterosonogram) is from a 47-year-old female with a history of metrorrhagia, a form of dysfunctional uterine bleeding. The studies reveal a mass in the uterus within the endometrial cavity The lesion was shown at pathology to be a benign hyperplastic polyp.
Courtesy of Ashley Davidoff, M.D.
Diseases of the Uterus and Cervix: Endometrial Carcinoma
Endometrial carcinoma is a malignant disease of the inner lining of the uterus usually occurring in postmenopausal women.
Most endometrial cancers are caused by excess exposure to estrogen without the opposing influence of progesterone. However, the cause for some endometrial cancers is multifactorial or unknown.
The result is uncontrolled growth of the endometrium.
The structural changes are characterized by proliferation of glands within the endometrium. These glands are filled with tightly packed malignant cells. The functional changes are characterized by growth of the endometrium after menopause, a time when the endometrium usually atrophies since estrogen levels decrease.
When endometrial carcinoma occurs in a premenopausal woman, the functional change is characterized by endometrial growth not regulated by the menstrual cycle.
In both cases, the result is a clinical presentation of abnormal bleeding. This bleeding can be at an abnormal time, for example after menopause or not during menses, or in an abnormally increased amount.
Imaging is useful in the initial evaluation of a patient with abnormal vaginal bleeding by pelvic ultrasound and sonohysterography.
Diagnosis is made by endometrial biopsy and staging is based on findings at lymph node dissection during surgery.
Treatment of endometrial carcinoma is surgical, with total hysterectomy as well as removal of both ovaries and fallopian tubes. As stated above, the pelvic lymph nodes are also removed for staging. Radiation therapy is used for patients who are not candidates for surgery, as well as after surgery for patients with advanced disease. Hormone therapy with progesterone and chemotherapy are used for patients with disease recurrence. Most endometrial carcinomas present with bleeding early in disease progression. As a result, with early treatment, patients often have a good prognosis.
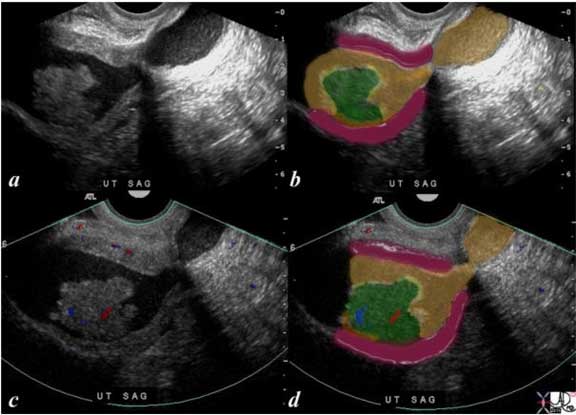
The ultrasound is from a 70-year-old post menopausal female who presents with an enlarged uterus. The endometrial stripe (pink) is enlarged and is filled with fluid (yellow) and an enhancing soft tissue mass (green) consistent with an endometrial carcinoma. Note blood flow (red and blue) as depicted by Doppler exam (c) characterizing the soft tissue as tumor rather than a clot.
Ashley Davidoff, M.D.

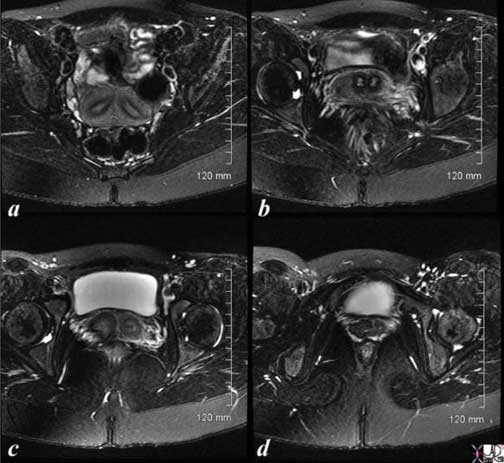
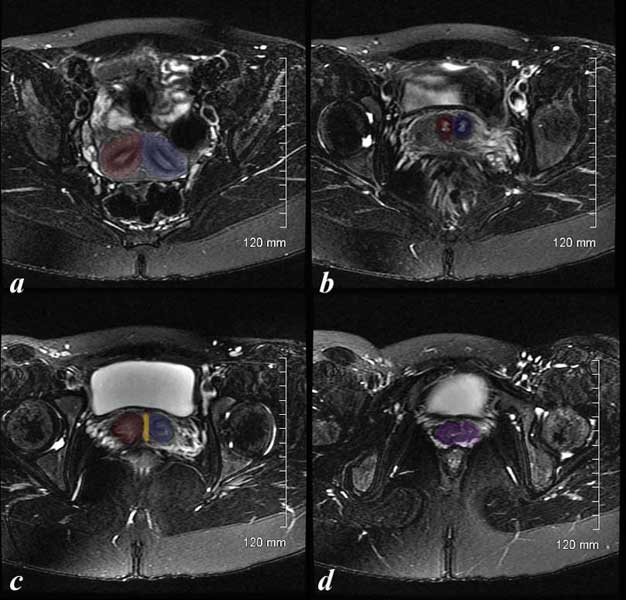
This axial CT (c and d) with reformatted sagittal images (a and b) are from a 46-year-old female with endometrial carcinoma. The images show a focal area of soft tissue thickening (green) on the superior surface (b) and rightward (green d) of the endometrial cavity (orange).
Ashley Davidoff, M.D.

70-year-old female with pelvic discomfort. The CT shows an endometrium filled with complex soft tissue (green), fluid and or blood (orange) and the fallopian tubes which are distended with fluid (yellow) caused by the obstructing carcinoma.
Images courtesy of Ashley Davidoff, M.D.
Diseases of the Uterus and Cervix: Congenital Abnormalities
Congenital abnormalities are most often associated with anomalies of the Mullerian ducts which are a pair of embryonic structures that are precursors to the fallopian tubes, uterus and upper two thirds of the vagina.
The Mullerian duct disorders, including unicornuate, bicornuate and didelphys uteri are characterised by anomalies in the development, fusion or septal regression of the Mullerian ducts.
Structurally the full volume of the uterus and endometrial cavity is compromised, often resulting functionally and clinically with infertility.
The diagnosis is best accomplished with MRI or hysterosalpingography.
Ashley Davidoff, M.D.
Courtesy: Ashley Davidoff, M.D.

34-year-old female who presented with infertility had a hysterosalpingogram which showed a unicornuate uterus (a). An MRI confirms the diagnosis using a T2-weighted sequence (b). The patient subsequently fell pregnant and was scanned with a normal 13 week pregnancy (c).
Ashley Davidoff, M.D.
Diseases of the Uterus and Cervix: Adenomyosis – Abnormal Junctional Zone
Adenomyosis is a disease of the myometrium caused by misplaced or ectopic endometrium in the myometrium, resulting in myometrial hyperplasia and smooth muscle hypertrophy, clinically manifesting as pelvic pain and uterine enlargement. The entity can be focal or diffuse.
The exact cause of the displacement is not known but it is presumed that a breach in the endometrial myometrial barrier enables a small amount of endometrium to translocate and remain viable. There is a high prevalence rate with about 40% of hysterectomy specimens displaying the entity.
Clinically the patient presents with dysmenorrhea and menorrhagia and on exam the uterus is enlarged.
The diagnosis is best made by MRI which shows a thickened junctional zone (>10-12 mms) of the uterus. The deposition of acute blood, blood degradation products such as iron, or the presence of fluid filled microglandular deposits in the junctional zone make the MRI findings highly specific for the diagnosis.
Treatment options include pain management with NSAIDS and hormonal manipulation. Surgery with hysterectomy is the only current option for cure.

This T2-weighted MRI of a 41 year-old female shows a thickened junctional zone (pink) of the uterus (outer myometrium is burgundy) measuring up to 12 mm and characteristic of adenomyosis.
Ashley Davidoff, M.D.

52-year-old patient presents with menorrhagia. Two punctate echogenic nodules are in the subendometrial junctional zone, (overlaid in white in b) that is thought to represent dystrophic areas of calcification in prior foci of adenomyosis. The larger echogenic focus (green) was shown to be a benign hyperplastic polyp by pathology after a D and C. The polyp probably accounted for the patient’s menorrhagia. Note that the uterus is retroverted.
Images courtesy of Ashley Davidoff, M.D.
Diseases of the Uterus and Cervix: Hydrosalpinx
Hydrosalpinx is literally a fallopian tube filled with water. This is usually caused by an obstruction of the distal Fallopian tube most often related to pelvic inflammatory disease.
The entity is often bilateral. When the blood distends the fallopian tubes it is called hematosalpinx and when pus is the cause it is called pyosalpinx.

This 33-old-female with left adnexal discomfort had a prior history of pelvic inflammatory disease. Findings on hysterosalpingogram show a dilated fallopian tube, better appreciated on the patients right side consistent with hydrosalpinx, though pyosalpinx is included in the differential diagnosis.
Ashley Davidoff, M.D.
Diseases of the Uterus and Cervix: Benign Cervical Stenosis and Distended Cervical Canal
The transvaginal ultrasound is from a 50-year-old perimenopausal female with metrorrhagia. The uterine cavity and cervical cavity are filled with fluid and soft tissue elements are identified in the expanded cervical canal. The findings are consistent with cervical stenosis, but the cause of the metrorrhagia is not obvious. The stenosis was relieved and follow up ultrasound showed resolution. No cervical mass was identified.
Images courtesy of Ashley Davidoff, M.D.
Diseases of the Uterus and Cervix: Cervical Cancer
Cervical carcinoma is a malignant disease of the uterine cervix.
Most cases of cervical carcinoma are caused by infection with the human papilloma virus (HPV).
The result is uncontrolled growth of the cervical epithelium.
The structural changes are characterized by proliferation of malignant, squamous, epithelial cells at the junction between the outer cervix and the endocervical canal.
The functional changes may be minimal, but in advanced cases can be characterized by abnormal bleeding or obstruction of the endocervical canal.
The PAP smear is an extremely effective screening tool for premalignant lesions of the cervix and allows many cases of cervical carcinoma to be prevented. As a result, most women in the U.S. present clinically while still asymptomatic during screening pap smears. However, in developing countries, where routine screening is less accessible, women with advanced disease can present with abnormal or post-coital bleeding or pain.
Diagnosis is made by biopsy after a positive pap smear and examination with colposcopy.
Imaging with MRI or CT can be used to evaluate the extent of advanced disease. Chest x-ray to look for distant metastasis is used for staging.
Treatment of premalignant lesions is local excision with a loop electrosurgical excision procedure. Early disease can be treated with radiation therapy or radical hysterectomy with similar results. Advanced disease is treated with chemotherapy and radiation.

31-year-female with a mass in the lower uterine segment of the uterus (green overlay). There is almost total occlusion of the canal (yellow). There are small vessels feeding the tumor (red). The patient subsequently obstructed the endometrial cavity and became secondarily infected.
Ashley Davidoff, M.D.

This sagittal and axial CT scan are from a 31-year-old female with carcinoma. The images show an expanded irregular endometrial cavity (yellow) that contains air (black), soft tissue (green) and fluid (yellow) and a uterus with an enhancing filling defect (green overlay in b). The mass could arise from the cervix based on its position or from the uterus. The former is more likely based on the patient?s age. A solid appearing mass is seen in the right adnexa (dark green), representing either a solid mass in the ovary or an enlarged iliac node. These findings are consistent with cervical carcinoma or less likely endometrial cancer with secondary obstruction and pyometra.
Image courtesy of Ashley Davidoff, M.D.
Diseases of the Uterus and Cervix: Conclusion
The uterus is essential for the survival of our species. The reproductive age of a female starts at about the age of 12 or 13 years and generally lasts till the age of about 52 years.
Every month for approximately 40 years the uterus undergoes preparation for implantation of the fertilized ovum. This equates to almost 500 menstrual cycles and on the average worldwide, results in 2 successful pregnancies per woman. It seems like a significant and time consuming focus of energy and resources of nature with low net result but the low net result is essential for our survival.
It is essential to understand the menstrual cycle and the structural changes that result. The uterus is a small organ but can enlarge to 500 times its size during pregnancy. The organization of its parts allows the receipt and transport of the sperm, unfertilized and fertilized ova, implantation, nourishment and protection of the early pregnancy and developing fetus and the ability to expel and deliver the fetus. The anatomy and physiology is simply a miracle of life.