
Introduction
The heart is the only organ that supplies its own circulation. The arteries that supply blood to the heart are the right and left coronary arteries, which take origin from the right and left coronary ostia at the base of the aorta. The blood vessels travel on or just below the epicardial surface and then enter the myocardium at either an oblique angle or at a 90 degree angle. The capillary network is quite extensive and results in a 1:1 ratio of capillary to myofibril, which is very high, but is necessary to meet the high metabolic demand of the myofibril and the heart. Capillary density is less in the interventricular septum and AV nodal tissue making them more susceptible to ischemia, putting the conduction systems in these areas at a relatively higher risk to ischemic injury.
About 5% of cardiac output is supplied to the coronary arteries. Blood flow is during diastole, since the myocardium around the intramyocardial vessels is relaxed.
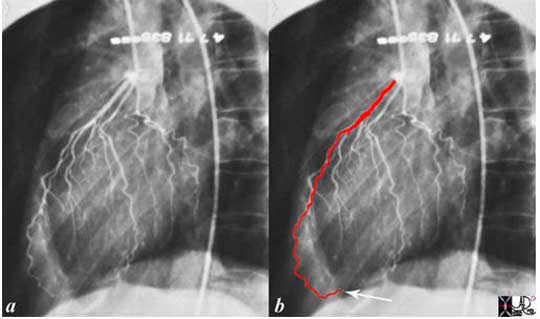
The word coronary arises from the Latin word ?corona? meaning crown. The reason for this term is exemplified below.
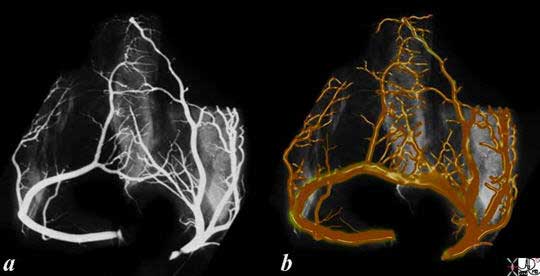
The origin of the word coronary is from the Latin word ?corona? which means crown. A post mortem heart was inflated and the coronary arteries were injected with barium. The subsequent angiogram was turned upside down so that the apex is pointing straight upward and the base of the heart is inferior, The shape of the heart when oriented this way is much like a crown.
Courtesy: Ashley Davidoff, M.D
Infrastructure of the Coronary Artery
The infrastructure of the coronary artery conforms to the cross of scaffolding described in the introduction to the applied anatomy of the heart.
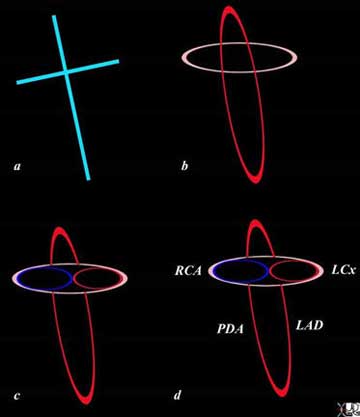
The infrastructure of the heart as a cross, has horizontal and vertical components that have 3 dimensions (b). The tricuspid valve and annulus (blue ring) and mitral valve and annulus (red horizontal ring) are aligned in the horizontal plane (c). The right coronary artery (RCA) and circumflex (LCx) supply the right and left side respectively, while the left anterior descending (LAD) and posterior descending artery (PDA) align along the vertical limb.
Courtesy: Ashley Davidoff M.D.

Another way of visualizing the distribution of the coronary arteries around the scaffolding is described in the drawing which demonstrates how the arteries are organized around the scaffolding of the heart. Both coronary arteries (dotted red) are closely linked in position to the cross. They both start off just above the horizontal component, and each has a horizontal component that winds around the atrioventricular (A-V) groove starting out anteriorly and ending posteriorly. The vertical components are called the descending arteries and they run anterior and posterior in relation to the interventricular septum. The left anterior descending artery runs in the anterior position between the ventricles, and the posterior descending coronary artery runs in a posterior position between the ventricles.
Courtesy: Ashley Davidoff, M.D.
The left coronary artery supplies most of the left ventricle and septum together with the left atrium. Blood supply to the posterior portion of the heart is highly variable.
The left coronary artery originates from the left coronary sinus, which is slightly posterior and superior to the right coronary cusp. After the left main coronary artery branches into the LAD and circumflex, the LAD proceeds in the interventricular groove and supplies the anterolateral aspect of the heart and most of the septum, including the anterior fascicle of the left bundle and the right bundle branch. The circumflex proceeds in the left A-V groove first, coursing anteriorly and then posteriorly, and supplies the posterolateral aspect of the left ventricle to variable extent, as well as the left atrium.
The right coronary artery originates from the right coronary sinus. It makes a loop in the anterior groove and then proceeds to the posterior part of the atrioventricular groove, and usually ends as the posterior descending artery in the posterior interventricular groove. Distribution includes the anterior, lateral, and posterior aspects of the right ventricle, the right atrium and the lower one third of the interventricular septum. It also supplies the the posterior fascicle of the left bundle branch, often supplies the AV nodal artery (85-90%), the SA nodal artery (60% of cases), and sometimes a portion of the posterior aspect of the left ventricle.
The vessels enter the myocardium from the surface and proceed into the myocardium at variable angles.
Coronary Dominance
The supply of the posterior and inferior parts of the heart is quite variable. Sometimes the RCA is the dominant artery and less commonly the region is supplied by the LCA. Coronary dominance defines the vessel that supplies this area of the heart. The classical definition of dominance has been related to which of the two vessels give rise to the posterior descending artery. The right coronary artery feeds the posterior descending artery in 85% of patients and by inference in this context is dominant in 85% of hearts.
However, a more useful definition relates to the posterior circulation of the heart that includes the origins of the PDA, A-V nodal artery and the posterior left ventricular artery. If all these vessels originate from the right coronary artery, then it is a right dominant system. If the origin of these three vessels is shared by both vessels, it is called a co-dominant or balanced circulation. When the vessels all arise from the LCA then it is a left dominant system.
With this latter definition, the RCA is dominant in 70%, LCA is dominant in 10%, and co-dominance occurs in about 20% of people.
The detail of each of the vessels will be advanced and exemplified in anatomical and angiographic situations.
The Left Coronary Artery
There are three major branches of the left coronary artery (LCA):
? left main coronary artery.
? left anterior descending artery
? left circumflex coronary artery

The normal coronary arteries of the post mortem specimen have been injected with barium. The heart is projected in the anteroposterior (A-P -a) and lateral projection (b). In the AP projection the LAD is seen in the interventricular groove and in the lateral projection the LAD is shown anteriorly and branches of the circumflex are shown posteriorly.
Courtesy: Ashley Davidoff, M.D.
The Left Coronary Artery: The Left Main Coronary Artery
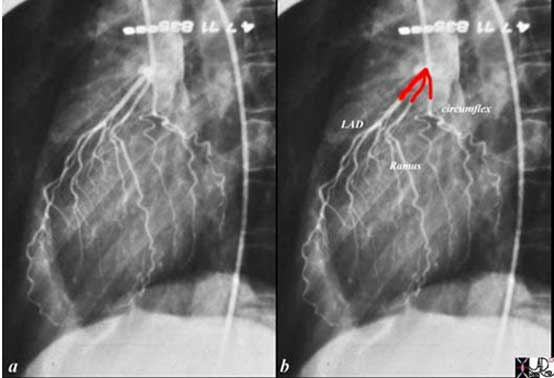
The left main coronary artery is between 1 and 25mm long, typically about 10-20mm, but can be up to 40mm. It is about 4.5mms in diameter (3-6mm), arises from the left coronary ostium and terminates in the bifurcation into the LAD and circumflex coronary artery. It is best viewed in the A-P projection during angiography. Occasionally it is absent (1%) in which case the LAD and circumflex have separate origins (Mill). In about 35% of cases there is a trifurcation and the third and middle branch is called the ramus medianus, which acts like a first diagonal artery.
The left main proceeds in a leftward direction and courses behind the pulmonary artery and right ventricular outflow tract.

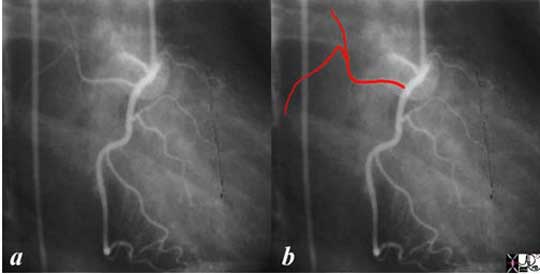
The angiogram in the anteroposterior projection shows the left main coronary artery overlaid in red, just before it branches into the LAD and circumflex coronary artery. In angiography the A-P view is the best view to identify the full extent of the left main coronary artery.
Courtesy: Ashley Davidoff, M.D.
CT Angiography (CTA) allows for the evaluation of the left main coronary artery in any plane. Since the vessel lies posterior to the pulmonary outflow tract, it is necessary to digitally manipulate the image in order to expose left main from the surrounding tissues.
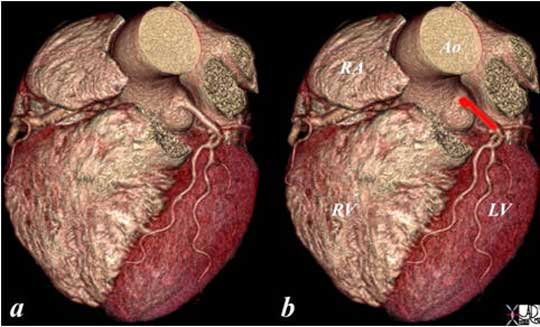
The volume rendering of the normal left main coronary artery (red overlay) is seen in image (b). The left atrial appendage and right ventricular outflow tract have been digitally removed to expose the left main coronary artery.
Courtesy: Ashley Davidoff, M.D.
After a short distance the left main terminates usually by bifurcating into the LAD and circumflex vessels.
Left Main Terminates as the LAD and Circumflex
Courtesy: Ashley Davidoff, M.D.
The coronary angiogram in the LAO projection shows a trifurcation of the left main into the left anterior descending artery, (LAD), ramus medianus, and circumflex coronary artery. The trifurcation is a variant of normal and the ramus supplies the anterolateral aspect of the heart. The ramus acts like a first diagonal artery in the territory it serves.
Courtesy: Ashley Davidoff, M.D.
The Left Coronary Artery: The Left Anterior Descending Coronary Artery
The left anterior descending artery (LAD) measures about 4mm in diameter proximally and about 2mm distally. It originates at the bifurcation of the left main and often terminates in characteristic moustache-shaped branching pattern, as it passes around the apex (80%). Less commonly, it falls short of the apex and the posterior diagonal artery (PDA) passes around the apex from the posterior location. The LAD and PDA form an anastomoses at the apex.
In about 4% of patients there are two LAD?s that travel in parallel, with one vessel supplying the septal perforators and the other the diagonals (Mills).
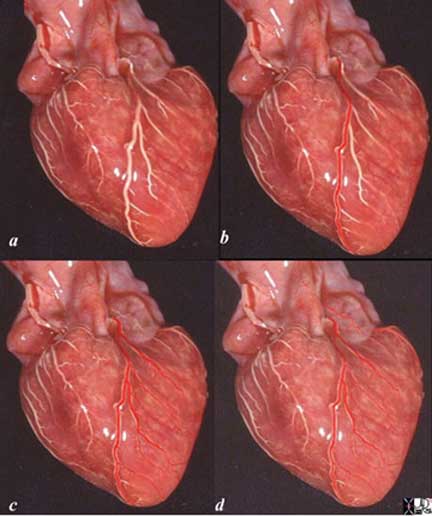
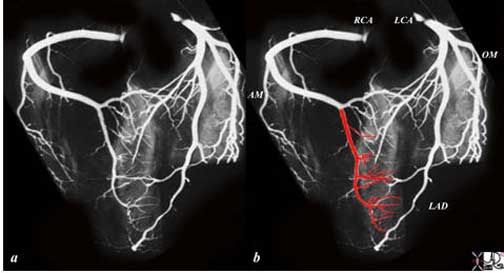
The heart specimen has been injected with barium into the coronary arteries and in this instance the left coronary artery is demonstrated. In image (b), the red overlay represents the LAD in the interventricular groove which reflects the position of the interventricular septum. Image (c) shows the diagonal arteries supplying the anterolateral aspect of the left ventricle. The last image (d) shows a few branches of the barely visible circumflex coronary artery. These vessels will be detailed below.
Courtesy: Ashley Davidoff, M.D.
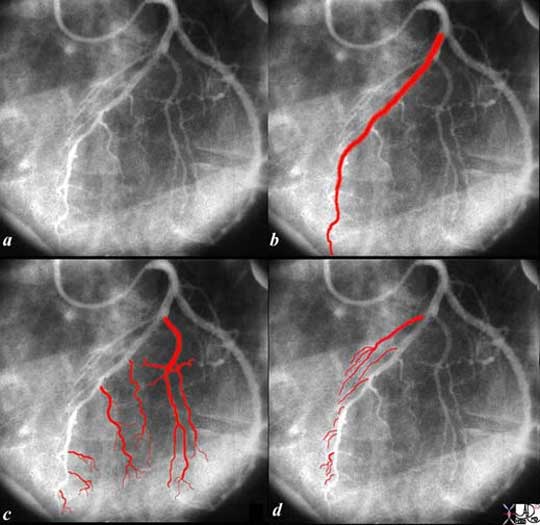
The left coronary angiogram is taken in the left anterior oblique projection showing the left anterior descending artery (LAD) in (b, red overlay) and the diagonal branches in (c). The septal branches are the other main branches of the LAD and they are shown in (d).
Courtesy: Ashley Davidoff, M.D.
The angiogram is from an infant with hypoplastic left heart syndrome and aortic atresia and shows the classical moustache shape bifurcation of the distal LAD.
Courtesy: Ashley Davidoff, M.D.
The left coronary angiogram in the LAO projection shows the usual distribution of the distal LAD as it proceeds around the apex of left ventricle. The anastomosis with the PDA is not demonstrated.
Courtesy: Ashley Davidoff, M.D.
The Left Coronary Artery: Conal Artery
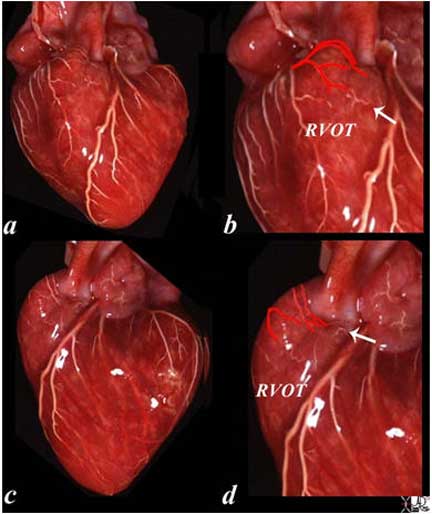
The first branch of the LAD is a small and barely seen conal artery that together with the right coronary artery supplies the right ventricular outflow tract. This anastomosis is a major collateral pathway when there is a stenosis in the left main, proximal LAD or proximal RCA. The conal artery is also called the artery of Vieussens and is named after the French anatomist Raymond de Vieussens (1641 – 1715).
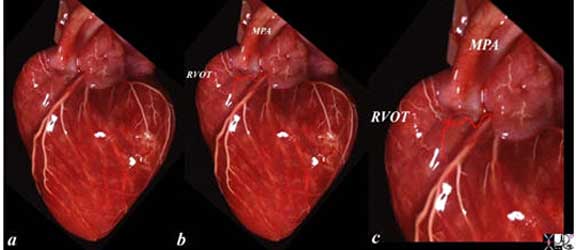
The normal coronary arteries of the post mortem specimen have been injected with barium. The heart is projected in lateral projection. It is displayed with red overlay in (b) and magnified in (c). The counterpart branches from the right coronary artery are seen outlined with white barium.
RVOT – right ventricular outflow tract
MPA – main pulmonary artery
Courtesy: Ashley Davidoff, M.D.

The angiogram in the LAO projection shows the conal artery usually arising as the first vessel off the LAD, but in this instance seems to arise after the first diagonal, although the origin of the vessel may be hidden by the LAD. The anastomosis with the conal branch from the right side is noted at the edge of the upper terminal branch where a small branch of the right-sided component of the conal artery is seen.
Courtesy: Ashley Davidoff, M.D.
The Left Coronary Artery: Diagonal Arteries
There are usually 2-6 diagonal branches that travel over the anterolateral surface of the heart and supply this region as well the anterolateral papillary muscle. The diagonals initially run on the surface of the heart and therefore can be visualized by CT imaging. At variable distances from their origin they gradually dive into the myocardium. The first diagonal is generally the largest branch, but there is a wide variation in size and number of diagonal arteries.

The normal coronary arteries of the post mortem specimen have been injected with barium. The heart is projected in the anteroposterior (A-P) (a,b) and lateral projection (c, d). In the AP projection the LAD is seen in the interventricular groove and in the lateral projection the LAD is shown anteriorly with branches of the circumflex shown posteriorly, and the diagonals noted between these major branches.
The diagonals supply the anterolateral aspects of the left ventricle. They are overlaid in red both in their epicardial and their subepicardial distribution (b, d). As they travel on the epicardial surface the white barium is well visualized (a, c) and while they travel subepicardial a shadow of their distribution is noted. They dive into the myocardium at variable distances and at variable angles and become invisible as they traverse the myocardium.
Courtesy: Ashley Davidoff, M.D.
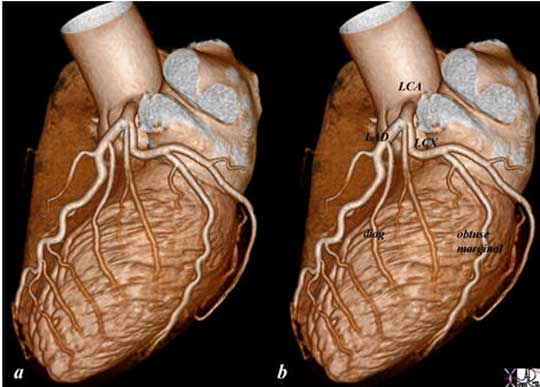
The reconstructed CT image of the normal left coronary circulation from a lateral projection shows the left coronary artery arising from the left aortic cusp starting out as the left main, which is a short vessel and not well demonstrated in this view. The diagonals are well demonstrated in this view with distribution to the anterolateral parts of the left ventricle.
Courtesy: Philips Healthcare
The Left Coronary Artery: Septal Perforators
Multiple septal perforators (typically between 4-6 in number) originate at right angles from the LAD, and are directed toward the diaphragm. The first septal artery usually arises just after the first diagonal and it is the largest of the septal arteries. The septal vessels arising from the LAD, supply the upper 2/3rds of the septum. The right bundle and the anterior fascicle of the left bundle are supplied by the LAD perforators. In general the density of the capillaries is reduced in the septum making the conduction system in this area susceptible to ischemia. The lower 1/3rd is supplied by the posterior descending artery and these vessels anastomose seamlessly. The anastomosis allows the perforators to act as a major collateral pathway between the left and right circulation. Thus, a significant stenosis in the LAD will result in a lower pressure distally in the vessel and the right coronary artery will be able to supply this area via the septal arteries distal to the stenosis. These collaterals require time to mature and function optimally when an atherosclerotic stenosis evolves slowly. In the event of an acute thrombosis, collaterals are not well developed and this results in more devastating consequences to the myocardium.
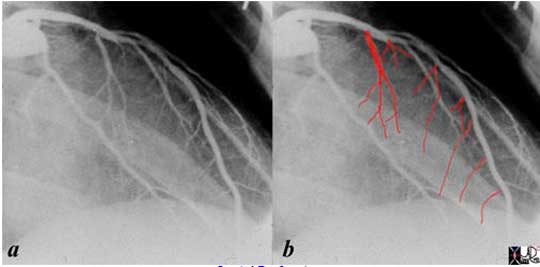
The angiogram is performed in the RAO projection and the left anterior descending artery is recognized by the fine septal perforators that supply the upper 2/3rds of the septum. The direction of the septal perforators is characteristic in that they head toward the diaphragm. The lower 1/3 of the septum is supplied by the septal perforators of the PDA. The septal perforators from the LAD and the PDA form a seamless anastomosis. These vessels are not visualized by CT because they are intramural and very small. The first septal perforator is usually larger than the other septal vessels.
Courtesy: Ashley Davidoff, M.D.
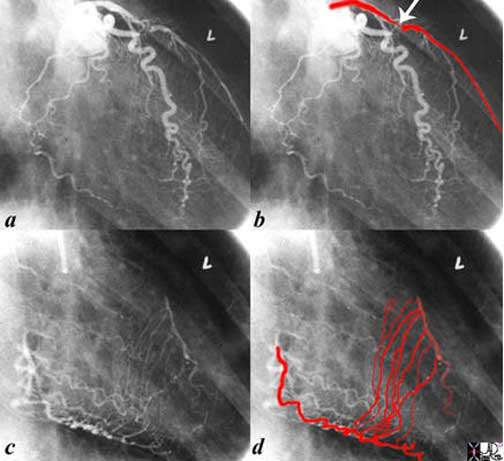
The first angiogram (a, b) is from an injection of the left coronary artery in the RAO projection. A subtotal occlusion in the proximal LAD (arrow) is noted. There is an implied high pressure gradient between the proximal and distal LAD and a predicted low pressure in the distal LAD based on the severity of the stenosis. The second injection (c, d) is into a normal right coronary artery with delayed imaging when most of the contrast has washed out from the upstream portion of the RCA vessel and shows septal collateral vessels supplying the downstream LAD from a high pressure RCA to the low pressure of the distal LAD.
Courtesy: Ashley Davidoff, M.D.
.
The Left Coronary Artery: Circumflex Coronary Artery
The proximal circumflex artery in a right dominant systems measures about 3.5mm in diameter. In left dominant systems it is larger and measures about 4mm.
In a right dominant system, it arises as a branch of the left main and terminates as a small vessel in the posterior portion of the heart (85%).
Proximally, it proceeds under the left atrial appendage to enter the anterior portion of the atrioventricular groove. In general, it gives off 3-5 obtuse marginal vessels feeding the anterolateral portion of the heart (usually OM1) , the lateral margin? obtuse marginal proper (usually the largest vessel) as the second branch (OM2) and the third (usually OM3) feeding the posterolateral aspect. Sometimes there are smaller unnamed branches between the obtuse marginals. The number and size of the obtuse marginal vessels is variable. A posterior left ventricular branch may arise as the terminal vessel off the circumflex.
The obtuse marginals typically supply the posterolateral aspects of the LV, as well as the posterolateral papillary muscle.
The circumflex also gives rise to the left atrial branches. In about 40% of individuals it gives rise to the SA nodal vessel, and supplies the A-V node in about 10%.

The normal coronary arteries of the post mortem specimen have been injected with barium. The heart is projected in lateral projection. The branches of the circumflex coronary artery have been overlaid in red (b) as they supply the lateral and posterolateral portion of the left ventricle. In this case there are at least 4 obtuse marginal vessels with OM4 supplying the ?buttocks? of the LV.
Courtesy: Ashley Davidoff, M.D

Courtesy: Ashley Davidoff, M.D.
The distal circumflex can be a confusing vessel to define in angiography, since often one of the marginals, usually second, is so large, that the distal true circumflex becomes inordinately small, quite insignificant in appearance. Its position in the A-V groove can be confirmed by identifying the coronary sinus which fills on the later phase of the coronary angiogram, and which also runs in the A-V groove.

The left coronary angiogram is taken in the left anterior oblique projection showing the distal circumflex artery in (b) as a small tortuous almost insignificant vessel compared to the proximal circumflex.
The second marginal (2 in b) is so large that the distal circumflex seems insignificant. Since in this patient the RCA is dominant, the distal circumflex plays a small part in supplying the posterior and inferior portions of the LV.
The first obtuse marginal (1) overlaid in red in (c), arises from the anterior portion of the circumflex. The second obtuse marginal (2) is huge. The 3rd obtuse marginal (3) arises from the posterior portion of the circumflex artery. The last branch is a tiny posterior left ventricular artery. In (d) two small vessels are shown. The first, off the larger anterior portion is likely the S-A nodal artery and or left atrial branch, and the second arises from the smaller posterior portion and is a small left atrial branch.
Courtesy: Ashley Davidoff, M.D.
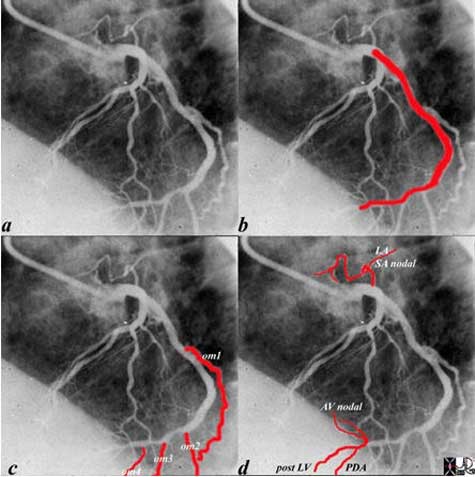
The left coronary angiogram in this instance demonstrates a dominant left system. Both the anterior and posterior component of the circumflex, overlaid in red in b, are of a large caliber. In c, the first second third and fourth obtuse marginals are shown. In d the origin of the PDA, posterior left ventricular branch, and the AV nodal artery are shown at the crux of the heart. Since the inferolateral portion of the heart and the A-V nodal artery arise from the left coronary artery it is a left dominant system (about 10% of cases).
Courtesy: Ashley Davidoff, M.D.
The Right Coronary Artery
The proximal right coronary artery (RCA) in a right dominant system is about 4mm and in a left dominant system it is about 3mm. The RCA enters the anterior AV groove under the right atrial appendage. The first branch is the conus branch, and then multiple, unnamed right-sided branches supply the anterior wall of the right ventricle (RV).
The acute marginal artery courses along the lateral margin of the RV.
Thereafter, the RCA courses posteriorly in the AV groove, and in 85% of patients it gives rise to the posterior descending artery in a typical 90 degree change in direction.
In 60% of patients the RCA gives rise to the SA nodal artery from its anterior portion and in 90% of patients it gives rise to the AV nodal artery from its posterior portion. As a completely right dominant system it will supply both the AV nodal artery and posterior left ventricular artery.
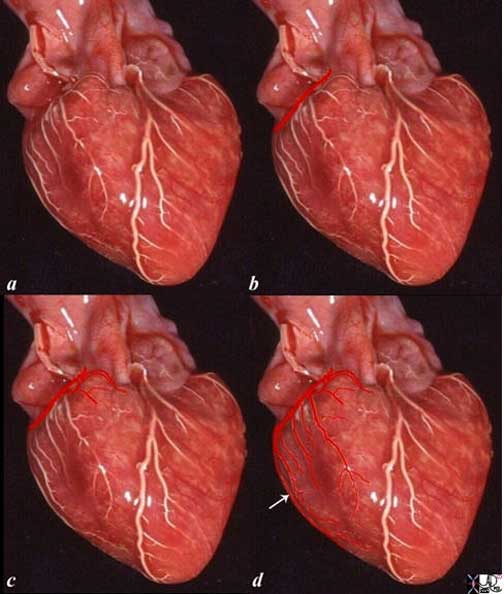
The heart specimen has been injected with barium into the coronary arteries and in this instance the right coronary artery is demonstrated. In image (b), the RCA is deep and hidden and the red overlay represents the expected position of the proximal RCA in the anterior part of the A-V groove. Image (c) shows the conal artery or the artery of Vieussens supplying the right ventricular outflow tract. The specimen shows many branches in (d) that supply the anterior wall of the RV but the only named vessel is the acute marginal artery (arrow) that travels along the right lateral aspect of the right ventricle (white arrow).
Courtesy: Ashley Davidoff, M.D.

The posterior aspect of the heart shows a barium injection of the right coronary artery. Image (a) shows the continuation of the RCA after it has given off the acute right marginal artery. Image (b) shows the posterior descending artery that runs along the interventricular groove. Image (c) adds the posterior left ventricular branches while image (d) shows the completion of the posterior cross as the atrioventricular nodal artery courses superiorly toward the IVC (overlaid in blue). This system is a completely dominant right coronary system since the posterior crux is totally supplied by the RCA.
Courtesy: Ashley Davidoff, M.D.
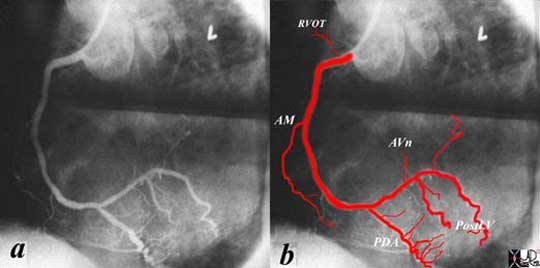
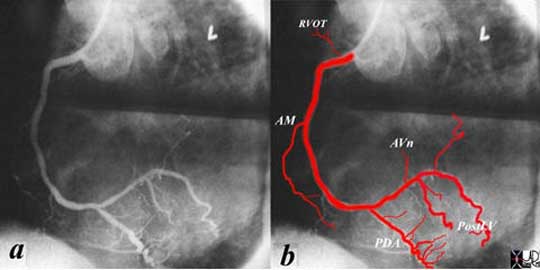
The coronary angiogram of the RCA is taken in the left anterior oblique projection showing the proximal vessel giving rise (in order of origin) to the branch to the right ventricular outflow tract (RVOT) (conal artery), and acute marginal branch (AM). The RCA then continues in the posterior aspect of the AV groove. The first branch to be given off is the PDA and then in this instance the vertical small branch is the AV nodal artery (AVn). Two large posterior LV branches course inferiorly on the posterior aspect of the left ventricle and the last small branch courses cranially to the left atrium as a left atrial branch.
Courtesy: Ashley Davidoff, M.D.

The injection into the right coronary artery is displayed in the right anterior oblique projection revealing in order of branching the sinoatrial nodal artery (SAn) the acute marginal artery (AM) that separates the anterior portion of the heart from the posterior. The RCA continues in the posterior A-V groove. The next branch off the RCA is the right atrial branch (RA). When the RCA reaches the posterior interventricular groove it takes a 90 degree turn as it gives off the posterior descending artery ( PDA). The septal perforators (unlabeled) are shown as multiple small vertical branches off the PDA that supply the lower 1/3 of the septum. Note in this patient the PDA curves around to supply the apex – This is uncommon since the LAD usually assumes this function.
Courtesy: Ashley Davidoff, M.D.
The Right Coronary Artery: The Conal Artery
The conal artery is the first branch of the right coronary artery and it supplies the right ventricular outflow tract. It collateralizes with its counterpart, the first branch of the LCA. The collateral pathway plays a significant role in patients with evolving, hemodynamically significant stenoses in the left main, proximal LAD and proximal RCA lesions.
The normal coronary arteries of the post mortem specimen have been injected with barium. The heart is projected in AP (a, b) and lateral projection (c, d). The conal artery is the first branch of the RCA and it supplies the right ventricular outflow tract. It collateralizes with the smaller counterpart which is a branch of the left coronary artery. It is magnified and displayed with red overlay in (b) and (d). The white arrow shows a branch of the smaller conal artery arising from the LCA.
Courtesy: Ashley Davidoff, M.D.
The Right Coronary Artery: SA Nodal Artery
In the past it was thought that a single SA nodal artery was present. It is now felt that there often two sources of SA nodal artery supply, and that there are multiple potential routes for the artery to find its way to the SA node. Infarction of the SA node is rare possibly for the reasons stated above. (Kawashima)
The right coronary artery has been injected into the right coronary artery and displayed in the right anterior oblique projection and it shows a prominent SA nodal artery arising as the first vessel off the RCA. The vessel also supplies the right atrium itself.
Courtesy: Ashley Davidoff, M.D.
The Right Coronary Artery: Acute Marginal Artery
The marginal branch of the right coronary artery, follows the right acute margin of the right ventricle and supplies branches to both the anterior and posterior surfaces of the right ventricle. In angiography it helps define the anterior from the posterior aspects of the AV groove.

The right coronary artery has been injected and displayed in the right anterior oblique projection The acute marginal artery is the largest of the anterior right ventricular branches and it marks the border between the anterior and posterior wall of the right ventricle.
Courtesy: Ashley Davidoff, M.D.
The Right Coronary Artery: Posterior Descending Coronary Artery
The posterior descending artery marks the posterior border of the interventricular septum and originates by taking a typical 90 degree turn down toward the interventricular septum. It is smaller than the LAD, usually falls short of the apex but anastomoses with the distal LAD which usually supplies the apex. The PDA sometimes has an early takeoff from the right coronary artery before it reaches the crux of the heart. It occasionally supplies the apex. It usually supplies the posterior fascicle of the left bundle conduction system. It often branches off the posterior RCA before it reaches the apex, and rarely it duplicated. It is distinguished from the posterior left ventricular branches by the septal arteries which originate at 90 degrees from the PDA.
Both coronary arteries have been injected with barium in this post mortem angiogram taken in shallow left anterior oblique projection. The PDA is shown in red as it takes a 90 degree turn off the right coronary artery. Note the acute marginal artery (AM) reflects the edge of the right side of the heart, and the obtuse marginal off the LCA and circumflex reflects the left edge of the heart. The PDA reflects the inferior border of the heart. The septal perforators supply the posterior and inferior 1/3 of the ventricular septum and arise at right angles off the PDA.
Courtesy: Ashley Davidoff, M.D.
Septal branches of the posterior descending artery
The posterior descending artery supplies vasculature to the lower 1/3 to 1/4 of the interventricular septum, which anastomoses with the branches arising from the LAD. They arise at right angles off the PDA. They supply the post fascicle of the left bundle branch.
The Right Coronary Artery: AV Nodal Artery
The AV nodal artery is a branch of the posterior and distal portion of the right coronary artery in 90% of patients and arises at the posterior crux of the heart, formed by the distal RCA, that often continues to the left side to branch into posterior left ventricular branches, the AV nodal artery that proceeds cranially, and the posterior descending artery that proceeds inferiorly. In 10% of patients the AV node is supplied by the left coronary system. The AV node is situated just anterior to the coronary sinus at the entrance of the IVC.
AV block is associated with acute myocardial infarctions involving the right coronary artery.

The coronary arteries of the normal heart specimen have been injected with barium and the posterior aspect of the heart in the region of the crux is exposed. The distal circulation of the RCA is overlaid in red in (b) revealing the distal right coronary artery (RCA), the origin of the AV nodal artery, posterior descending artery (PDA) and the posterior left ventricular branches. In images (c) and (d) the posterior wall of the right atrium has been lifted and the extent of the AV nodal artery magnified and exposed. The opening of the IVC is ringed in blue.
Courtesy: Ashley Davidoff, M.D.
The Right Coronary Artery: Posterior LV Branches
The posterior left ventricular branches are also known as the posterolateral arteries. The supply of the posterior aspect of the left ventricle is variable and may arise from the left coronary or right coronary system, or from a combination.
The coronary angiogram of the RCA has been shown above but is shown again relevant to this discussion. It is taken in the left anterior oblique projection showing the posterior left ventricular branches taking origin just after the AV nodal artery (AVn). There are two large posterior LV branches that course inferiorly on the posterior aspect of the left ventricle.
Courtesy: Ashley Davidoff, M.D.
Applied Anatomy
Atherosclerosis is a degenerative disorder of the vascular wall characterised by a fibrofatty deposition (plaque) in the inner lining of the artery.
It is the most common disorder of the coronary arteries and a challenging disease to Western cultures particularly because of the high prevalence of the disease and the associated high morbidity and mortality that attends the disease. Atherosclerosis is a normal aging phenomenon but is accelerated in genetically predisposed individuals and is associated with common diseases such as diabetes and hypertension.
The accumulation of plaque in the wall causes narrowing of the lumen of the arteries progressively restricting flow. In addition, the normal smooth and glistening lining of the arteries are replaced by a rough irregular inner wall that is a factor that predisposes to thrombosis, sometimes an acute life threatening event if the arteries of the heart or brain are affected.
The clinical presentation depends on the organ involved and the degree of narrowing. In the heart for example simple narrowing results in chest pain called angina. When total acute obstruction occurs with thrombosis of the artery, severe unremitting chest pain occurs, and myocardial infarction ensues.
The coronary arteries are essentially end arteries and their branching pattern is tree like so that a specific area of the myocardium is essentially only supplied by one mother vessel. As implied in the text, the presence of collaterals, best defined in the conal arteries and septum are available. These however usually require time to mature these collaterals in order that they can compensate for physiological demands at rest and excercise. In an acute coronary thrombosis in a young patient with little atherosclerosis, the collateral system often fails because the collateral system is innately ill equipped to respond to this situation.
Cause: It occurs as a normal course of aging, but it is accelerated by genetic, dietary and behavioral factors.
Result/Diagnosis: The clinical presentation depends on the organ involved and the degree of narrowing. In the heart for example simple narrowing results in chest pain called angina. When total acute obstruction occurs with thrombosis of the artery, severe unremitting chest pain occurs, and myocardial infarction ensues.Each organ has varied manifestations of clinical presentation, all relating to reduced perfusion of the end organ due to narrowing. Imaging plays an essential role in diagnosis. Ultrasound can directly view the lumen and wall of accesible vessels, while CTscan and MRI are advancing to be the mainstay of diagnosis for the deeper arteries. Angiography was the gold standard of the past, is still used and is invaluable in selected circumstances, particulalrly if therapeutic intervention is needed.
Atherosclerosis of the Aorta
Courtesy: Henri Cuenoid, M.D.
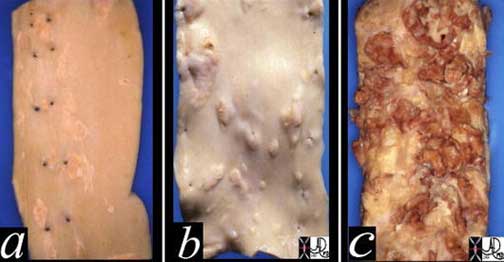
The proximal RCA is the most common site of symptomatic atherosclerosis.

The normal right coronary artery of a pediatric patient has been opened and the lumen and wall have been exposed. The section has been magnified in (b) and (c) and shows a widely patent lumen (red) and a thick muscular wall. (light pink) exemplified in (c).
Courtesy: Ashley Davidoff, M.D.

Courtesy: Henri Cuenod, M.D.
Coronary Stenosis
Coronary stenosis is caused by progressive accumulation of atherosclerotic burden in the wall of the vessels resulting in progressive stenosis. Stenosis of greater than 70% is hemodynamically significant. In the left main, a 50% stenosis is clinically relevant. The plaque is variably composed of acute inflammatory changes, fatty cholesterol deposits, fibrous capsules and calcium.
Angiography and more recently CT and MRI are able to define the stenotic lesions.
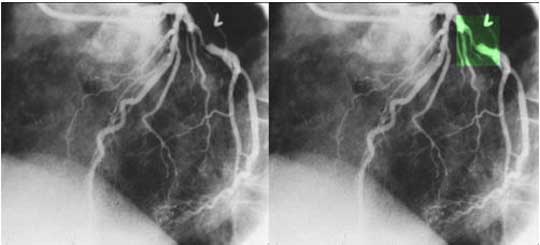
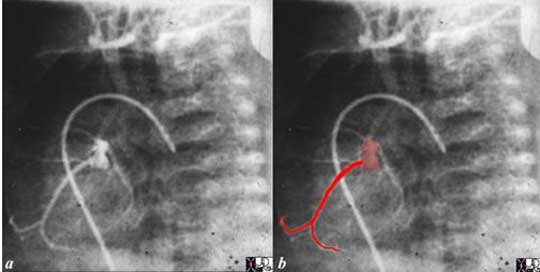
The coronary angiogram in the LAO projection shows a severe proximal stenosis (> 70%) of the circumflex with some post stenotic dilatation. The second image has a green overlay indicating the region of disease with the post stenotic dilatation. This lesion is considered hemodynamically significant.
Courtesy: Ashley Davidoff, M.D.

Filet view of the right coronary artery using CT technology and curved reformatting revealing calcific plaque disease (bright white densities). CT is the study of choice for the evaluation for calcific atherosclerotic disease.
Courtesy: Ashley Davidoff, M.D.
Coronary Thrombosis
Coronary thrombosis is an acute occlusive process of the coronary artery, almost universally in the presence of atherosclerotic disease resulting in a variety of syndromes commonly presenting with acute chest pain.

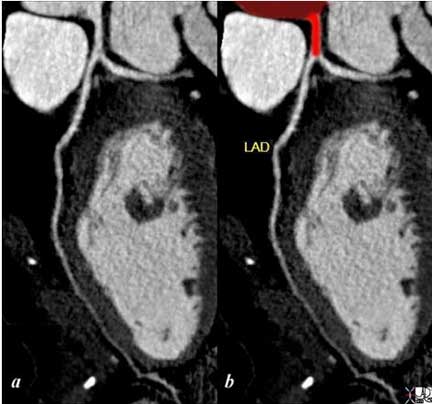
The first image shows a coned down LAO projection of the in a patient with acute thrombosis of the left anterior descending artery. In the second image the thrombus in the artery is overlaid in maroon. Following thrombolysis *third image minimal irregularity of the endothelium is seen. This may be residual thrombus or reflect the soft tissues of a plaque rupture.
Courtesy: Ashley Davidoff, M.D.
Conclusion
Knowledge of the anatomy and variation of the anatomy of the coronary circulation is the key to the understanding and evaluation of disease in the vessels on imaging studies. The framework of the coronary vessels is one of a cross which corresponds to the interatrial septum and interventricular septum in the vertical plane, and the atrioventricular groove in the horizontal plane.
The right and left coronary arteries, although distinctly separate, act in unison via collaterals which are essential when stenosis or occlusions occur.
The most important role of coronary CTA is in the patients with atypical chest pain.
Coronary arteriography remains the gold standard for the evaluation of the coronary arteries.
References
Anderson KR, Ho SY, Anderson RH: The location and vascular supply of the sinus node in the human heart. Br Heart J 1979; 41:28.[Abstract/Free Full Text]
Anderson H, Webb S, Brown NA. Clinical anatomy of the Atrial septum with references to its developmental components. Clinical Anatomy 1999;12:362-74.
Anderson H, Brown NA, Webb S. Development and structure of the Atrial Septum. Heart 2002;88:104-10.
Arnsdorf M F The SA node Up to Date
Barash PG, Cullen BF, Stoelting RK, Cahalan M, Stock CM Clinical Anesthesia 6th Edition Wolters Kluwer Lippincott Williamsand Wilkins
Cohn LH, Edmunds LH Jr, eds. Cardiac Surgery in the Adult. New York: McGraw-Hill, 2003:791-810.
Condado JA and Gimon MV., Catheter-Based Approach to Mitral Regurgitation. (J Interven Cardiol 2003;16:523?534.
Boon, NA, Colledge NR., , Davidson S, Walker B.R., Davidson’s Principles & Practice of Medicine, Churchill Livingstone Elsevier 20th Edition
Duytschaever M, Ho SY, Devos D and Tavernier R., The left hand as a model for the right atrium: a simple teaching tool. Europace 2006 8(4):245-250.
Duerinckx A.J MD, Phd., Coronary Magnetic Angiography Newark, NJ: Springer-Verlag, 2002
Ed’s Histology Notes
Gertsch, Marc MD, The ECG: A Two-step Approach to Diagnosis, Springer VerlagNnewYork 2004
Ho SY. Anatomy of mitral valve. Heart 2002;88(Suppl IV):iv5?iv10.
Ho SY, Anderson RH and Quintana DS. Atrial structures and fibers: morphological basis of atrial conduction. Cardiovascular Research 54 (2002) 325 ?336.
Kahle Werner Leonhardt Platzer Werner Color Atlas text of Human Anatomy Vol 2 4th Revised Edition Thieme Stuttgart Germany 1992
Kawashima T; Sasaki H The morphological significance of the human sinuatrial nodal branch (artery). Heart Vessels 2003 Sep;18(4):213-9.
Kitzman D, Edwards WD., Minireview: Age-related changes in the anatomy of the normal human heart. J Gerontol Med Sci. 1990;45:M33
Krause William, The Art of Interpreting Histologic preparations: A laboratory MAnual and Study Guide for histology Universal Publishers Florida 2004
Larry R. Kaiser, Irving L. Kron, Thomas L. Spray., Mastery Of Cardiothoracic Surgery. 2006: 525-530.
Lazarova D Gjorgov NJ., Dimensions of the triangle of Koch. Bratisl Lek Listy 2006;107 (4):107-9.
Libby. Braunwald, Heart Disease. A text book of cardiovascular Medicine 8th edition.
Mihaljevic T i, Paul S i , Cohn L Hi , Wechsler A i., Pathophysiology of Aortic Valve Disease.
Mill, MR Wilcox, B.R., Anderson R Surgical Anatomy of the Heart from Cohn Lh, ed. Cardiac Surgery in the Adult. New York: McGraw-Hill, 2008:3-28.
Netter FH., The Ciba collection of medical illustrations Vol 5 Heart. Summit, NJ: Ciba Pharmaceutical, 1969
Oudkerk Matthijs editor, Coronary Radiology, Springer Verlag
Schuenke, M Schulte E, Schumacher, U., Ross, L.M., Lamperti, E.D.,
Atlas of Anatomy: Neck and Internal Organs V2 2006 Thieme
University of Arkansas Department of Neurobiology and Developmental Sciences. Nerves of the Thoracic Region
Walmsley T. The Heart. In: Sharpey-Schafer E, Symington J,Bryce TH, eds. Quain?s Elements of Anatomy, 11th ed. Vol 4,part 3. London: Longmans, Greens & Co, 1929, p. 42.