
Introduction

The colon has not captured the imagination of poets, artists, and historians to the extent that other organs such as the heart, liver, and the brain have. The colon on the other hand is usually a subject that is avoided in cultured circles and is commonly the brunt of coarse jocularity in casual circles. Its contents are usually compared and used as expressions and expletives of disgust and disagreement, while reference to its tail end is used in reference to the last and the least. However, when one explores this organ in the objective world of science and biology, one can only look upon its importance in water balance, and its beauty of form and function with admiration. Rather than looking down on the organ we should look up to it (like the endoscopist does) and express our gratitude that it not only has taken on the dirtiest job of the body, but also that it performs its job with aplomb and humility. To understand the importance of the intact and functioning colon, one only has to review the ravaging results of the untreated or poorly treated effects of cholera. Unreplaced water and electrolyte loss leads to a mortality ranging from 50-90%. The in humility suffered by the incontinent elderly also reminds one of the importance of this organ in the maintenance of physical and psychological health. Almost 50 years after the event, I can still remember the embarrassment and fear of a child who had been incontinent of feces as he stood frozen at the front entrance of the classroom during recess.
Overview
In health the colon serves to:
- Concentrate fecal effluent by absorbing water and electrolytes
- Store and control evacuation of fecal material
- Digest and absorb undigested carbohydrates as a lesser function
However, the colon is not essential for survival but its functions contribute significantly to the overall well-being of humans. Patients who have had total colectomies for ulcerative colitis, Crohn?s disease, or ischemic colitis can survive since the small bowel will assume the functional void left by the absent colon.
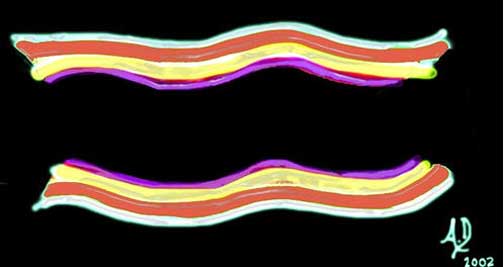
There are three outstanding morphological features that are unique to the colon.
- Three longitudinal muscles called taenia coli that run almost the entire length of the colon.
- Sacculations or haustra that result from the ?pleating ? of the colon caused by the taenia coli
- Odd looking fatty growth excrescences called appendices epiploica that arise from the pericolonic fat
While the structure of the taenia and haustra seem to have functional relevance, the structure and function of the appendices epiploica remains a mystery.

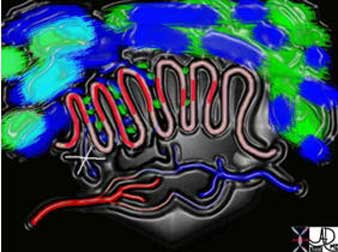
This overlay of the transverse colon reveals the three outstanding morphological features of the colon including the bright yellow appendices epiploica, one of the three longitudinal muscles called the taenia coli in maroon and the sacculations called haustra caused by pleating of the colon by the taenia.
Courtesy Ashley Davidoff, M.D.
Principles
The colon is a muscular and tubular organ and is specifically designed for water and electrolyte reabsorption and the storage, transport and evacuation of feces. In general the body is made up of tubes and factories. The factories process and produce and the tubes transport. As in any functioning system, whether it is biological or otherwise, there are controlling influences that govern supply and demand, and in the case of the body these controlling systems are executed through the nerves and hormones of the body.

Examples of tubes include the gastrointestinal system, tracheobronchial tree, the biliary system, circulatory system, and urinary system. Even the brain needs a tubular system to allow for the transport of CSF. The colon is the downstream end of the gastrointestinal system. In the diagram you can identify some of the aforementioned tubular systems.
Courtesy Ashley Davidoff, M.D.
As a tube the colon is subject to the laws, principles, and physics of tubes. Relevant factors relating to rate and velocity of tubular flow include radius, length, pressure differences, type of content being moved, and resistance within the tubular system. The function of the colon is to mix the chyme and absorb the remaining water in the right colon, while slowly moving the product onward to the left colon where storage is the major function. Finally, evacuation requires rapid movement and expulsion of a relatively bulky product.
The colon needs to have a large surface area to increase its absorptive powers, which it accomplishes by folding its mucosa inward to form crypts, the so-called crypts of Lieberkuhn. The small bowel also uses a similar structural trick of increasing its functional surface area by its villous microstructure, while the lung bulges its surface area by forming grape-like sacculations called alveoli around its ductal system.
Histology
Let us examine the histological makeup of the colon first in the context of other tubular systems and then review its makeup with a focus on how it functions.
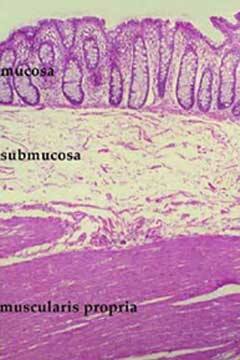
Like many other tubes in the body its wall has four layers. The inner layer that lines the lumen is called the mucosa which rests on its basement membrane. The mucosa consists of a single layer of rectangular cells and the layer is called an epithelium. Because of the rectangular shape of the cells they are called columnar cells and so the layer is called a columnar epithelium. The second layer is the submucosa which contains blood vessels, lymphatics, nerves and loose connective tissue. The third layer is the muscular layer called the muscularis and the fourth layer is called the serosa or adventitia which acts as a protective outer ?skin? for the colon. This layer is called a serosa when it is surrounded by peritoneum (transverse colon and sigmoid colon) and called an adventitia when it is retroperitoneal (ascending colon, descending colon and part of the rectum).
This diagram illustrates the 4 basic layers of the colon. The inner pink layer is the mucosa, the yellow layer beneath the mucosa is called the submucosa, while the red layer is the muscular layer (muscularis) and the 4th layer is called the serosa or adventitia.
Courtesy Ashley Davidoff, M.D.
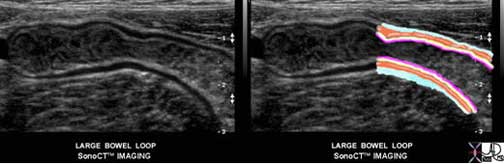
This ultrasound image of the colon demonstrates the 4 layers of the large bowel quite beautifully. The luminal contents are heterogeneous and are bordered by an echogenic line that is the combination of the mucosa and submucosa. The lucent line we see is the muscular layer while the outer echogenic line represents the serosa or adventitia
Courtesy Philips Medical Systems

The mucosa consists of a simple columnar epithelium which means it is a single layer of epithelial cells that are each shaped like a column – similar to a tall rectangular block of apartments.
Courtesy Ashley Davidoff, M.D.
Histology: Submucosa and Crypts
The submucosa contains the vital lifelines including the terminal branches of the arteries, the capillary network, the smallest and earliest venous branches and the lymphatics. There are nerve endings in the submucosa as well as the muscular layer. Circulating white cells that perform the vital local defense functions police the submucosa for potentially harmful organisms and substances. The muscularis contains spindle shaped smooth muscle cells while the serosa and adventitia consist of relatively strong connective tissue, and in the case of the serosa a layer of epithelial cells derived from the peritoneal lining.

The lifelines together with the small rounded lymphoid cells are illustrated in submucosa. A capillary network between arteries and veins forms creating the end of one part of the circulation and the beginning of the next. The spindle shaped smooth muscle cells are illustrated in the red muscular layer and the outer layer in white is made of connective tissue and in the case of the serosa a layer of flat epithelial cells derived from the peritoneum.
Courtesy Ashley Davidoff, M.D.
In order to optimize water absorption the mucosa of the large bowel is thrown into innumerable folds creating the crypts of Lieberkuhn which look like epithelial lined test tubes. Unlike the small bowel the mucosa does not contain villous projections, but rather these mucosal infolds called crypts which contain mucus secreting and water absorbing cells.
By creating tightly packed infoldings, the surface of the colon is increased significantly. Macroscopically the mucosal surface of the colon is mostly smooth except for folds called the plicae circulares which are formed by the pleating effect of the taenia coli.
Courtesy Barbara Banner, M.D.

Courtesy Barbara Banner, M.D.
Histology: The Wall
The wall of the colon requires a very substantial vascular supply and effective nerve and lymphatic system in order to coordinate its function with other physiological events occurring within the gastrointestinal system specifically and within the body at large. The neural, lymphatic, and vascular channels enter through supporting mesentery and penetrate the wall (just like the cable systems, water systems, electrical and sewerage enter and leave our homes). These penetrations produce weakening of the wall and remain the potential site for diverticuli to develop. The vessels terminate in the submucosa.

Courtesy Ashley Davidoff MD

Courtesy Ashley Davidoff, M.D.
The mucosa and wall of the bowel are not isolated structures. Each is connected and dependent on the other organs and the colon and its substructures are no different. It is not surprising therefore that disease of the colon, for example, is associated with disease in other parts of the body. The association of ulcerative colitis and sclerosing cholangitis is a prime example. The psyche and the bowel are also intimately related. Acute anxiety is notorious for inducing diarrhea.
The proximal large bowel is presented with the sludge-like byproducts of small bowel digestion consisting of mostly water, and undigested complex carbohydrates. Colonic mucosa absorbs most of the water and together with churning action and bacterial digestion, the nature of the sludgy semiliquid stool is transformed into a more solid and compacted stool.

In the above image the fluid filled chyme represented in the left part of image (light green), is transformed into the gas filled compacted solid stool (dark green) seen on the right side of image.
Courtesy Ashley Davidoff, M.D.
Physiology: Transport Function
The contents of the colon move in a slow and steady fashion. If the colon were to be an instrument in a band or an orchestra I would imagine it would be in the bass or double bass section. Its nature is quiet, efficient, deep, slow, and essential. It gets the job done without drama and fanfare. Occasionally it does have to let off some steam in which case it brings in the wind instruments and changes its pitch, but most of the day and night it is droning away, working slowly and efficiently in the background. It may take several days for stool to move from the cecum to the rectum. Movement of the colon is complex in the variety of contraction patterns which are executed by an inner circular and outer longitudinal muscle.
The contractions result in two basic patterns:
- one optimized for mixing
- the other for propulsion
Tonic contractions of these muscles result in a mixing pattern of the stool while rhythmic contractions serve to propel the stool. Borborygmi is the fancy name given to the gurgling or rumbling sound made by the gastrointestinal tract as it moves water and gas over each other. These sounds are not specific to the colon and originate in the stomach, small intestine and colon. They usually start at low pitch and end after about 30 seconds at a higher pitch. In patients with intestinal obstruction these sounds become exaggerated in intensity and frequency as a result of the attempt of the bowel to push its contents along. As the muscle tires late in the process the sounds may become ominously quiet in bowel obstruction.
Physiology: Muscles of the Colon
The location of the smooth muscle of the large bowel is consistent with other tubular systems of the body since it is found in the muscularis layer between the submucosa and the outer serosa or adventitia. The inner circular muscle has classical arrangement in that it is found in almost uniform thickness surrounding the entire large bowel. The longitudinal muscle concentrates and thickens in three longitudinal muscle bands as noted previously called taenia coli, each about 6mm to 8mm in width. They run almost the entire length of the colon, only becoming more uniform and forming a continuous, complete, circumferential layer at the level of the rectum. They are unique to the colon and are located at equal distances from each other around the circumference of the colon.
The presence of the longitudinal muscles along three fixed points of the colon creates a pleating effect and creates the haustra or sacs which facilitate storage and to some extent increase the surface area of the colon. (a haustrum is the singular form of haustra) On the luminal side the pleating effects causes folds in the mucosa called plica circulares or semilunar folds. When the contraction of the taenia is strong the haustral pattern is marked and when they relax the haustral pattern may be absent. If the taenia were to be removed from the colon it would be a longer and straighter organ without its haustrations.
Sometimes when the ascending colon is cut perfectly transversely on a CT scan, and because the taenia are equidistant and the degree of contraction is perfect, the haustra produce a perfect clover leaf formation.
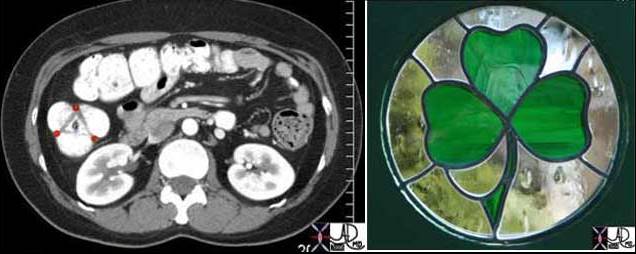
When the ascending colon is cut perfectly transversely, the three equidistant haustra produce a shape that looks like a clover leaf. The taenia are positioned at each point of the infolding. These muscle bands are relatively flat and so are not usually seen radiologically. The anterior taenia of the ascending colon is the taenia libera, while the medial muscle is the taenia mesocolica, and the lateral bundle is called the taenia omentalis. The triangle that is seen in this image represents the plica circulares which are the mucosal folds seen on the luminal side caused by the pleating effect discussed above.
Courtesy Ashley Davidoff, M.D.
These images reflect a contraction band (burgandy) in the rectosigmoid region. The colon upstream of the contraction is relaxed as is the colon that is distal to the contraction.
Courtesy Ashley Davidoff, M.D.
The non propulsive movements described above are intermittently combined with propulsive movements including slow irregular contractions that are more rhythmic in their nature. There is one type of propulsive movement which serves to slowly edge the stool forward caused by a contraction wave that starts proximally, is short lived, and involves a relatively short segment of colon. The second type of propulsive movement is stronger, occurs a few times in the day, and results in a mass movement where the product is aggressively moved onward and forward and when the colon shows off its muscular strength and power. This function is also called mass peristalsis, and most commonly occurs after a meal induced by the gastrocolic and duodenocolic reflexes.
This type of propulsive movement is also stimulated when a person wakes in the morning. Propulsive movements allow emptying of the upstream bowel of relatively large amounts of stool. The stool is moved a relatively long distance, and provides room for incoming contents. As stool moves downstream, the function of the colon evolves from churning and mixing to one of storage. There is also a pattern of muscular function called receptive relaxation which enables the receiving part of the bowel to accommodate new volume of chyme or stool. The movement of the stool is almost factory like with the product on a conveyer belt being worked on, refined and produced in the initial stages and when ready, signaled to move on where it is stored until it can be mailed out to its final destination.
Thus the smooth muscle of the gastrointestinal tract is designed to allow a coordinated and connected contractile movement. The individual cells are connected through their cell membranes in an intimate fashion to each other, allowing the cells to behave as a syncytium. This means that muscle activity in one muscle fiber is easily transmitted and propagated to other muscle fibers. This close connection allows for transmission of electrical activity through the muscle ? usually a function restricted to the nerves. In the colon therefore, muscle movement is controlled through both the usual autonomic innervation, hormonal control, as well as through muscle activity itself.
Physiology: Evacuation or Defecation
The mechanisms involved with defecation are even more complex since they involve somatic and visceral nerves, voluntary and involuntary muscles, and cerebral and an autonomic nervous system control. When the rectum fills, the person becomes conscious of a need to evacuate. The sensory path is so beautifully adapted enabling exquisite differentiation by pressure sensors to be made between air, watery stool, and solid stool. Even our second set of eyes (our hands) cannot easily ?feel? air. Have you ever been able to hold a volume of air in your hand and sense its presence? Of course if the air is moving or under pressure you will, but the sensory powers of the rectum and stomach in particular, and the gastrointestinal tract in general, are quite outstanding in their ability to sense gaseous content.
Once rectal fullness is sensed it is left up to cerebral decisions as to when emptying will take place. Normally the rectum should be empty since the function of the rectum is really to sense the presence of contents, discriminate the type of content, and then in the best of worlds to evacuate contents as soon as possible. The rectum is a type of post office ? once the letters and parcels come in they should be transported to their destinations as soon as possible ? do not allow backup! Since there is such a strong cerebral component to evacuation and since it is often not convenient, we often postpone the inevitable, and override the urge in our busy lives. Sometimes this may cause retroperistalsis which empties the rectum back to the sigmoid and quells the urge. If we postpone evacuation too frequently and for too long, the rectum becomes stretched and or the sensory fibers adapt, and our sensors sour and become less effective. The full rectum and the impacted rectum (rectum fa-shtoptum – a Yiddish phrase from the old country) is an entity seen in the pediatric population and even more so in the aging, the aged, the infirm, and the mentally handicapped.
There are two sphincters surrounding the rectum and the anal canal and a group of muscles called the levator ani muscles which are all functionally related to enable defecation. The internal sphincter is controlled by the autonomic nervous system and the external sphincter and levator ani by voluntary mechanisms. Once the decision to evacuate is made, the person will open the external sphincter and the internal sphincter will open in sympathy resulting in strong propulsive peristaltic wave, usually aided by a Valsalva maneuver allowing contents to move into the free world. This can occur normally from as frequently as several times in a day to as infrequently as once every few days.
Post evacuation CT image on the right shows an ascending colon with semisolid stool characterized by an air fluid level, and a descending colon that is empty. The colon frames the abdomen so that the ascending colon is the most rightward structure while on the left it is posterolateral. The sigmoid colon and rectum are also empty as seen in the second image. The patient defecated just before the scan was performed.
Courtesy Ashley Davidoff, M.D.
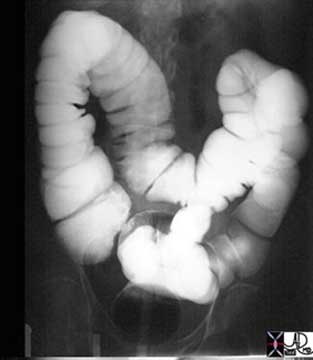
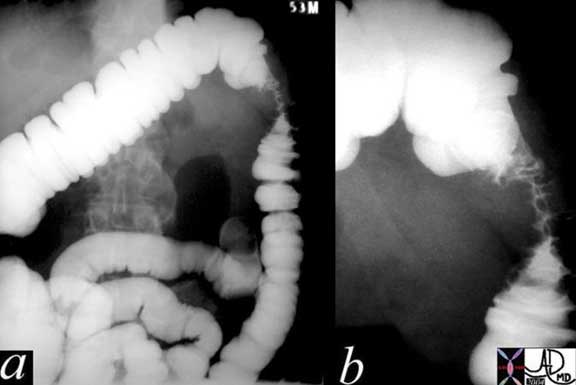
This series of two images shows the efficiency of the evacuation process. The above image is from a single contrast barium enema and shows a colon distended with contrast.
Courtesy Ashley Davidoff, M.D.

This X-ray of the abdomen shows about 80 percent of barium has been evacuated. Note that a small amount of barium refluxed into the terminal ileum on the ?post evacuation?, that the cecum, ascending transverse and part of descending colon are decompressed, and that the distal descending, and sigmoid colon are entirely empty while the rectum has a small residual within it. Now that is what you call a bowel movement! Some people would die for this kind of result.
Courtesy Ashley Davidoff, M.D.
Physiology: Absorptive Function
On the average about 1.5 liters of fluid enter the colon and only about 100-200ccs is excreted in the stool so that 90-95% of the water is reabsorbed. The maximum absorptive power of the colon is about 4.5 liters per day. In disease states where more than 4.5 liters is presented, diarrhea will result.
Most of the absorption takes place in the ascending colon with the descending colon acting in storage capacity. Electrolytes and particularly sodium are absorbed by the creation of a gradient by the sodium pump, which also helps in the absorption of water. There is active secretion of bicarbonate which helps neutralize the acid produced by the bacteria.

Courtesy Ashley Davidoff, M.D.
Physiology: Digestion and Absorption of Undigested Food Products
The colon is filled with an abundant zoo of anaerobic and aerobic bacteria which for the health of the body have to be caged in the ?safe? environment of the colon since if let loose into the rest of the body can be lethal foes. There are over 400 species of organisms that live in the colon including bacteria yeasts and some parasites. Most of these are helpful, some are just there for the ride providing no significant contribution, while others have the potential to be harmful. Other than functioning to ferment complex carbohydrates, they also synthesize vitamins like B12, biotin, thiamin, riboflavin and vitamin K. Vitamin K is especially important. Lactobacillus Acidophilus provides an antibacterial activity against many potentially harmful gram-negative and gram-positive pathogens.
The anaerobic bacteria dominate in the large bowel and together with the aerobic bacteria help break down and ferment products that were either missed by the small bowel or that were incapable of digestion by the small bowel such as cellulose and other complex carbohydrates found in fiber. Small amounts of fat, starch and proteins are also digested by these colonic mechanisms. E Coli can for example help split triglycerides. A small amount of complex carbohydrates are thus broken down into short chain fatty acids which are easily absorbed by colonic mucosa. The amount of energy provided by this process however is very small.
The human body lacks the enzyme called alpha-galactosidase that is required for the digestion of the complex carbohydrates found in vegetables such as beans, cabbage, soybeans, broccoli peas and onions. Beans contain particularly large amounts of complex carbohydrates and hence their notoriety as gas producers. Complex sugars are fermented by the bacteria, forming the short-chain fatty acids, butyrate, propionate and acetate. The fermentation process produces gas that contains hydrogen, carbon dioxide, and methane which are found both within the stool and in the lumen of the colon. Some people are unable to digest simpler sugars in the small bowel such as lactose which is found in milk and other dairy products. These simpler sugars are therefore presented to the large bowel where the fermenters turn the sugars into gas. When excessive gas is produced in these patients, symptoms include abdominal pain, discomfort bloating and flatulence.
The gas produced by the fermentation process can be found either within the stool or within the lumen of the bowel. If there is excessive gas within the stool it floats because the specific gravity is less than water. It is the gas that is in the lumen that causes distension of the bowel, which in turn stimulates the pressure sensing nerves in the wall of the bowel and in turn the sensation of flatulence. If the gas is upstream in the colon it may cause discomfort and pain and if it is downstream near the sigmoid colon and rectum a stimulus is created and interpreted as ?gas waiting to be passed? and it can be passed on a voluntary basis.
Courtesy Ashley Davidoff, M.D.
Courtesy Ashley Davidoff, M.D.
Physiology: Mucus Secretion
In the depths of the crypts of Lieberkuhn, mucus secreting cells called goblet cells are abundant. There are no enzyme secreting cells in these pits of the large bowel. Mucus is a normal secretion that is an excellent lubricant and protectant. It is spread on the surface of the bowel as a thin film preventing direct contact of the feces on the mucosa and thus protecting the mucosa from mechanical injury. It also adheres to the feces which enables the fecal nuggets to adhere to each other forming a stool mass which in turn facilitates transport. The mucus on the surface results in reduced friction of the feces and additionally helps transport of the stool. The mucus acts as a mechanical barrier to the zoo of bacteria that are housed in the colon and with an alkaline PH of about 8 it neutralizes acids in the stool. When the colonic wall becomes irritated, colitis ? an inflammation of the wall results, causing the mucosa to exude and secrete water, electrolytes and mucus. In addition, mucosal dysfunction in colitis will also prevent water that is arriving from the small bowel not to be optimally absorbed. The clinical consequence is a watery diarrhea, often with mucus. If severe enough and left untreated dehydration can ensue, which in the young and elderly can be fatal.
Principles of Disease: Diarrhea
Diarrhea is caused by mucosal malfunction most commonly called colitis or enteritis as stated above. There are many causes of diarrhea. Infections caused by salmonella, shigella and cholera cause diarrhea by affecting the mucosa while others such as amebiasis and Schistosomiasis affect the deeper layers as well. Ulcerative colitis another well known cause of chronic diarrhea is a non infectious mucosal disease while Crohn?s disease, ischemic colitis, and pseudomembranous colitis are transmural diseases, which mean they affect the entire wall of the bowel. When a disease is isolated to the mucosa, a CT scan may show bowel thickening but will not show induration of the pericolonic fat. In transmural disease the CT findings include wall thickening as well as changes in the pericolonic fat.
From a clinical standpoint diarrhea is defined as an increased frequency (more than 3 times per day) of liquid like stools. It can also be defined as a daily stool weight of greater than 200 grams. The usual weight of stools is 100-200 grams. The classifications of diarrhea are based on duration of the illness (acute vs chronic), based on the pathophysiological causes (osmotic vs secretory) or based on the cause (infectious, ischemic, inflammatory). (Sanaka and Soffer)

Courtesy Ashley Davidoff, M.D.
Courtesy Ashley Davidoff, M.D.
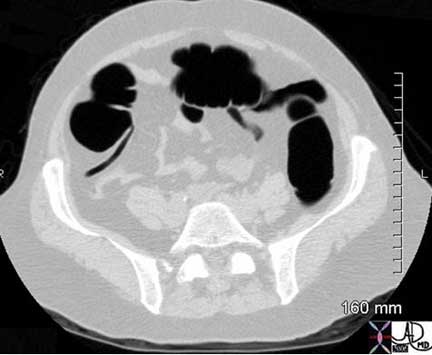
Diarrhea on CT

Note that in this patient the colon is mildly distended and the contents are fluid in nature, unlike the feces seen in the CT scans above. This 71-year-old male patient has diarrhea caused by ulcerative colitis which is a disease of the mucosa.
Courtesy Ashley Davidoff, M.D.
Crohn?s disease
In this patient with Crohn?s disease the ascending colon is empty, thick walled with changes noted in the pericolonic fat.
Courtesy Ashley Davidoff, M.D.

The transverse colon in this patient is thick walled with mild transmural changes in the pericolonic fat in the right and left upper quadrants. Transmural changes occurred as a result of ischemia. Note the calcific atherosclerotic changes in the aorta.
Courtesy Ashley Davidoff MD
Principles of Disease: Constipation
There is no single universal definition of constipation because of the wide variability of the bowel habits. The parameters that are considered for the diagnosis include the frequency and nature of the stool, the need and degree of effort to evacuate, and the sensation of incomplete evacuation. There are two basic causes of constipation. The first is called primary or idiopathic constipation which implies that there is no known cause, and the second is called secondary constipation, implying that there is a known cause for the entity. There are 3 types in the idiopathic group including: normal-transit constipation, slow-transit constipation, and dyssynergic defecation. In the normal-transit constipation the time that it takes to form and transport the stool is normal but the patient has a perception of difficulty in passing the stool. In the slow transit constipation, transit time as implied is slow and urge to defecate is also reduced. In the dyssynergic defecation the coordination required to process the action of defecation is lost.
The secondary causes of constipation include a long list of drugs, metabolic, psychogenic, endocrinologic, and gastrointestinal disorders.
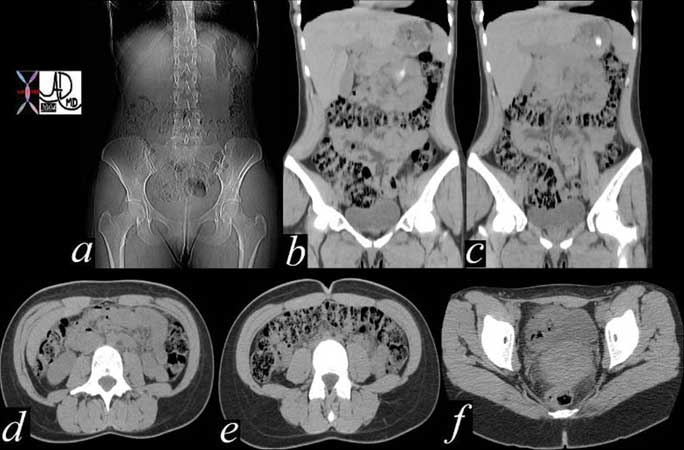
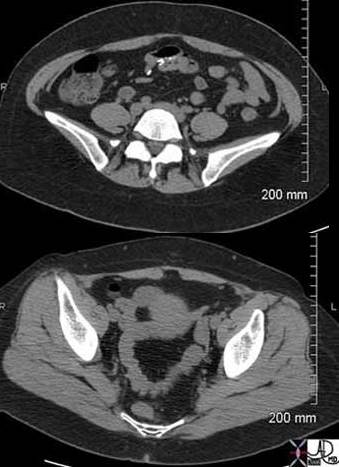
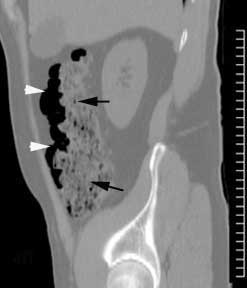
The series of images shows the radiological equivalent of constipation in this 28-year-old female patient who complained of bloating. The entire colon is distended with feces (a, b, c, d, e) though the rectum is empty (f).
Courtesy Ashley Davidoff, M.D.

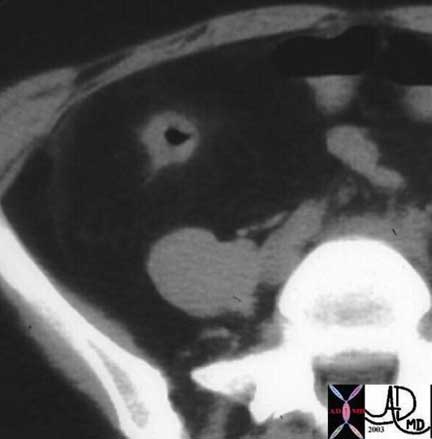
This CT scan reflects a very uncomfortable looking scan which unfortunately is not uncommon in the elderly. The rectum is truly impacted with feces. Since this is a slow process of accumulation the mucosa muscularis and blood supply can usually accommodate the large volume, but at some point the wall can become compromised with ensuing obstruction, ischemia and perforation.
Courtesy Ashley Davidoff, M.D.
Principles of Disease: Tumors
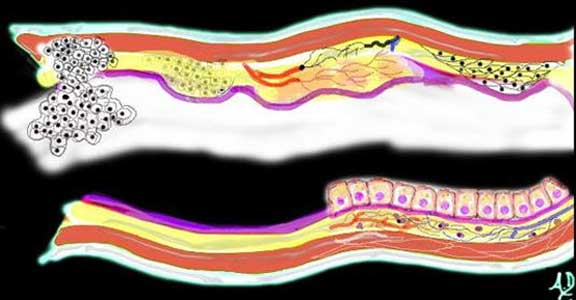
The most common site for tumor development is the mucosa. The mucosa is a highly active structure and cell turnover is rapid, with the reproduction of new cells and death of old cells occurring about every four days.

beginning of a neoplasm
The diagram shows a single columnar cell on the top side of the lumen that for whatever reason has been programmed to become ?different? and instead of growing with characteristic columnar shape with pink nucleus and ?peaches and cream? cytoplasm in this case has become round with white cytoplasm and black nucleus. It is a neoplasm ? i.e. a new growth.
Courtesy Ashley Davidoff, M.D.

Over time this neoplasm will continue to grow. If it grows slowly with monotony and uniformity in the morphology of cells, minding its own business and not disturbing its neighbors it is considered a benign neoplasm. It would be called a benign polyp and since it arises from the mucosa, it would be called an adenomatous polyp.
Courtesy Ashley Davidoff, M.D.
Tumors: Benign Polyps

This 5mm polyp is a common finding on colonic evaluation and at this size is a benign abnormality. Left intact it can grow into a monster. Hence it is usually removed by the endoscopist.
Courtesy Ashley Davidoff, M.D.

This series of images from a virtual colonoscopy shows an 8 mm polyp seen on the surface rendering images (salmon colored images, cross marks the polyp) referenced to the sigmoid colon (bottom left) and with conventional CT imaging (bottom middle). At this size the polyp is almost certainly benign and can be removed through the colonoscope safely.
Courtesy Scott Tsai, M.D.
Tumors: Malignant Tumors
The diagram illustrates the transformation from benign to malignant as the neoplasm starts to reveal an aggressive nature and invades and destroys surrounding tissue. In this instance it has advanced into the submucosa and muscularis as well as expanded into the lumen.
Courtesy Ashley Davidoff, M.D.
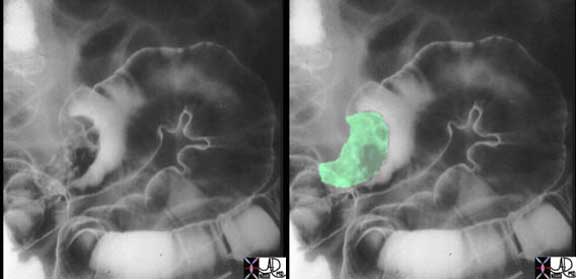
The double contrast barium enema shows a large irregularly shaped mass in the sigmoid colon outlined by air and contrast. The mass seen in green in the second image is greater than 2cm in size, so that the risk of malignancy is substantially increased.
Courtesy Ashley Davidoff, M.D.

Left undiagnosed and untreated the malignant cells continue to grow without regard to the neighboring structures. It encircles the colon in ?napkin-ring? fashion (as shown above) eventually blocking off the lumen and causing a bowel obstruction. It may grow through the wall and cause a bowel perforation and or grow into regional lymph nodes and portal venous radicles after which it will metastasize to the liver and other organs.
Courtesy Ashley Davidoff, M.D.
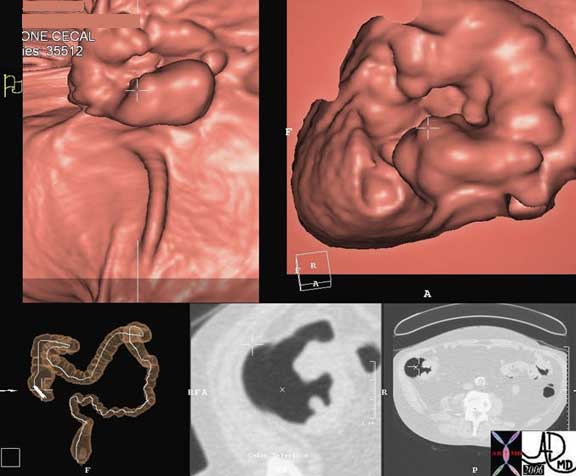
This series of images from a virtual colonoscopy shows a 5 cm ulcerated mass (cross marks the mass) seen on the surface rendering images (salmon colored images) referenced to the cecum (bottom left) and with conventional CT imaging (bottom middle). At this size and shape the mass is almost certainly malignant and cannot be removed through the colonoscope safely. Note how similar the morphology of this tumor is to the pathology of the specimen above (different patient).
Courtesy Scott Tsai, M.D.
Courtesy Scott Tsai, M.D.
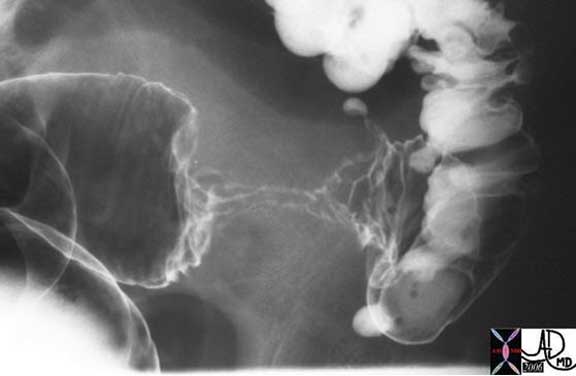
The double contrast barium enema shows an apple core lesion caused by circumferential growth of a malignant tumor of the colon in ?napkin-ring? fashion. The lumen is compromised. Note how the distal colon which is receiving air and barium via the enema tip is relatively dilated when compared to the descending colon which is relatively decompressed suggesting an obstructive process. Note also the presence of contrast filled diverticuli at the rectosigmoid junction. The two entities of carcinoma and diverticulosis often coexist since diverticulosis is very common in Westernized nations.
Courtesy Ashley Davidoff, M.D.
Parts of the Colon
In general it is practical to divide the colon into two parts split in the middle of the transverse colon. The right side consists of the cecum, ascending and hepatic flexure while the left consists of the splenic flexure, descending, sigmoid and rectum. This broad division is a functional division with the right side of the large bowel being responsible for absorption of water and electrolytes and the left side for storage.
The anatomic division into the better known parts of cecum, appendix, ascending colon, hepatic flexures, transverse colon, splenic flexure descending colon sigmoid and rectum follows.

These two diagrams give an approximate sense of the parts of the colon with no consistent divisions marking the transitions from one part into the next. The cecum (green) is well demarcated by the entrance of the ileum, with the ascending colon (light blue) transitioning into the hepatic flexure (royal blue) just before the turn below the liver. The transverse colon (pink) is of variable length and then makes a turn at the splenic flexure (yellow) just under the spleen. The descending colon (orange) extends along the left side of the abdomen after which it escapes from the retroperitoneum and becomes the sigmoid colon (gold). The proximal part of the rectum (brown) becomes bound by peritoneum and transitions into the anal canal a few centimeters shy of the anus which is the last part of the colon.
Courtesy Ashley Davidoff, M.D.
Parts of the Colon: Ileocecal Valve

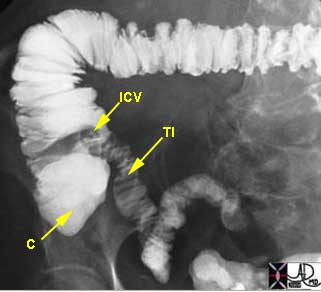
Courtesy Ashley Davidoff, M.D
The volume of chyme that passes through the ileocecal valve is relatively small and amounts to between 450 and 1000cc per day.

Courtesy Ashley Davidoff, M.D.
Parts of the Colon: Cecum
The cecum marks the beginning of the colon and is a blind ending sac whose upper border is defined by the ileocecal valve. It is one of the widest portions of the colon. The word cecum comes from the Latin word ?blind? since the proximal and inferior portion is blind ending. In herbivores it is fairly large since it is important in the digestion and fermentation of complex carbohydrates while it is small in carnivores that have little or no fiber in their diet.
It measures about 6 cm in length and about 7.5 cm in breadth and is situated in the right iliac fossa, usually above the inguinal ligament.
Rapid cecal distention is a warning sign of an impending perforation. A cecal diameter >10 -12 cm is an ominous sign and may indicate impending perforation. However, slow and chronic distension allows the cecum to adapt and hypertrophy its muscle so that larger diameters can be tolerated. It is therefore imperative to review old films before sending a patient off to the OR with a diagnosis of impending rupture.
Because of the large capacity of the cecum, malignancy in the cecum rarely presents with obstruction. Thus, patients who develop cecal carcinomas present relatively late in the disease usually presenting with a less dramatic anemia or occult blood in the stool. The importance of colonoscopic screening cannot be overemphasized. The U.S. Preventive Services Task Force strongly recommends that all men and women of 50 years of age or older be screened for colorectal cancer using one of the following techniques: fecal occult blood testing each year, flexible sigmoidoscopy every five years, fecal occult blood testing every year combined with flexible sigmoidoscopy every five years, double-contrast barium enema every five to 10 years or colonoscopy every 10 years.

This X-ray (left image) and CT scan (right image) of a patient with an enlarged cecum (yellow arrows) in the right iliac fossa measuring close to 12 cms. The size is a sign of impending rupture.
Courtesy Ashley Davidoff, M.D.
The cecum is usually covered by peritoneum on less than two thirds of its circumference making it a fixed retroperitoneal structure, but in about 5-10 % of people it is devoid of peritoneal fixation and is associated with an elongated mesentery making the cecum and proximal part of the ascending colon unusually mobile.
The cecum is supplied by the ileocolic artery which is a branch of the SMA and its venous drainage is into the SMV.
Cecum: Applied Anatomy
The floppy cecum and ascending colon are given the freedom to rotate which predisposes the structure to two types of important mechanical diseases. When it flops and kinks anteriorly and upward the resulting entity is called cecal bascule ? usually a reversible kink. In cecal bascule the fixed point is in the ascending colon while the floppy cecum moves on the hinge, flips upward to the right upper quadrant and kinks the bowel. This flip often reverses itself. The clinical presentation is one of intermittent obstruction and pain which commonly subsides as the kink spontaneously reverses itself. The radiographic appearance is one of a dilated cecum that is located in the RUQ in a subhepatic location.
When the bowel twists around itself, torsion or volvulus occurs along the longitudinal axis of the ascending colon. With a twist of 180-360 degrees it usually cannot untwist itself easily and the resulting volvulus is complicated by vascular compromise, infarction of the bowel wall and perforation ? a condition with high mortality. The radiographic image is usually characteristic with the dilated loop, sometimes described as an omega shape, presenting as dilated loop in the left upper quadrant with a twisted or whirl like appearance. A barium enema would give a beak shaped appearance at the site of the twisting in the right lower quadrant. Either way, when the colon reaches 12cm it implies impending rupture. A 9cm cecum in the appropriate clinical setting, particularly if rapid distension is the presentation, should raise concern for rupture.

In the image on the left the cecum is dilated and found in the RUQ characteristic of a cecal bascule, while in the image on the right it is found in the LUQ which is characteristic of a cecal bascule. In both cases the cecum has a risk of rupture due to the size of the cecum, but in the case of volvulus, vascular compromise adds to the risk of rupture.
Courtesy Ashley Davidoff, M.D.

This 69-year-old male presented with abdominal pain and distension. The CT coronal reformat shows a very large cecum in the right upper quadrant while the axial image shows an air fluid level in the cecum. The third image is from a barium enema and shows a beaking effect in the RLQ and a large air-filled cecum in the LUQ. These findings are consistent with a cecal volvulus.
Courtesy Ashley Davidoff, M.D.
An inverted cone best describes the normal shape of the cecum with the point of the cone pointing down, while the slit like ileocecal junction situated medially further defines its characteristic shape. The three longitudinal taenia originate near the base of the appendix and further define the shape of the cecum and depending on their positioning as well as their state of contraction the cecal shape will be defined at any given time. There are a number of conditions that cause the cecum to become narrowed, spastic, or coned caused by intrinsic disease of the cecum, muscle spasm within the cecum, or mass effect on the cecum by extrinsic disease. These diseases include infections such as amebiasis, tuberculosis (TB), actinomycosis, typhoid fever, typhlitis, and appendicitis and inflammatory diseases such as Crohn?s disease, and ulcerative colitis. Carcinoma and mucocele of the appendix are other entities that can deform the cecum.

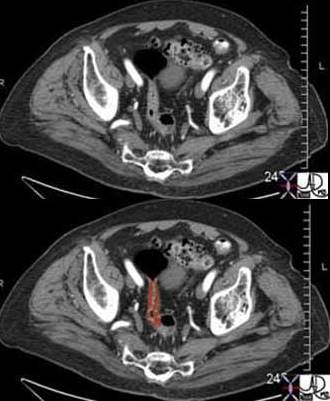
The CT scan is of a 32-year-old female who presents with RLQ pain. The enlarged appendix (overlaid in orange) causes mass effect on the rightward positioned contrast filled cecum resulting in a change in shape and size of the cecum that is reminiscent of an arrowhead.
Courtesy Ashley Davidoff, M.D.
Courtesy Ashley Davidoff, M.D.
Cecum: Intussusception
Another condition commonly seen in the cecum is intussusception (eMedicine). In children it is usually a benign entity that can often be treated with a gentle barium enema, while in adults it is usually associated with a tumor acting as the leading edge and has the additional risk of ischemic or obstructive complications. In the adult, surgery is indicated once the diagnosis is made. The findings are characterized by the finding of bowel within bowel, so that in the center one should see a narrow column of contrast in the inner lumen of the intussusceptum, surrounded by some mesenteric fat that has been dragged into the receiving loop, and then a hint of coiled springs of mucosa that has been telescoped by the process, and lastly the loop of receiving bowel called the intussuscipiens. Ischemic or obstructive changes may be associated.

Note in this instance the central lumen contains a dot of contrast surrounded by a thickened wall with no definite fat seen. A hint of coiled springs is seen at 7 and 11 o?clock reflecting the telescoped bowel that has been inverted and drawn in. The receiving loop is obvious as the outer layer contains air and contrast. No obstruction is present in this patient.
Courtesy Ashley Davidoff, M.D.
Parts of the Colon: Appendix
The appendix is a long narrow, blind ended tube that is also called the vermiform appendix because it has a worm-like appearance (vermiform means worm-like in Latin). Its overall diameter is between 3-6mm when empty and its length ranges from 2-10cm, but can be up to 20cm. In the human appendix, the submucosa does contain lymphoid tissue and therefore the appendix is assumed to have a minor function within the immune system, though it has no role in digestion. It has a very narrow lumen and if this lumen becomes blocked from fecal material or due to lymphoid hyperplasia in the wall, secondary obstruction, dilatation, ischemia and infection results in the clinical entity of appendicitis. Weakening of the wall can be complicated by rupture with consequences of abscess formation or generalized peritonitis.
The position of the appendix is variable and it can sometimes be very difficult to identify by CT, particularly when the normal appendix is not surrounded by fat and is instead surrounded by other loops of small and large bowel, or when the cecum itself is in an abnormal position. When the appendix is not obvious on initial perusal it is worthwhile using the more easily identified ileocecal valve with its fat laden lips as a guide, and then looking posteromedially and inferiorly for the appendix which usually lies within 2.5cm of the ileocecal valve. If the tenia coli were easy to see on the CT scan, finding the appendix in any situation would be a cinch since these longitudinal muscles all arise from around the appendix. These muscles are difficult to see on the CT scan.

This image reflects a large vermiform appendix filled from a single contrast barium enema. Its inferomedial origin is characteristic while the body and tip have an unpredictable course as seen in this image.
Courtesy Ashley Davidoff, M.D.
Appendix: Applied Anatomy
CT scanning is highly sensitive and specific for the entity of appendicitis. Periappendiceal stranding is the most specific sign occurring in 100% of patients with the disease, while thickening of greater than 6mm is also sensitive (93%) and specific (100%) (Rao). The finding of appendicoliths on the other hand does not necessarily imply acute appendicitis, but is often associated with the acute condition. A stone stuck in the distal right ureter can sometimes masquerade as an appendicolith (Lane ).
In humans the appendix is a vestigial structure, while in obligate herbivores the appendix is large, allowing it to participate in the fermentation process of cellulose.

Courtesy Ashley Davidoff, M.D.
Parts of the Colon: Ascending Colon
The origin of the ascending colon is well-defined as it starts just cranial to the ileocecal valve and it continues to the hepatic flexure where there is no definite defining border between the two. It is retroperitoneal in its location and is slightly narrower in diameter than the cecum and measures up to 20-25 cm long.
The ascending colon is supplied by the right colic artery which is a branch of the superior mesenteric artery (SMA) and it is drained by the right colic vein which drains into the superior mesenteric vein (SMV).

The ascending colon (aqua blue) in this patient is relatively short in this projection. It starts just above the ileocecal valve and ends in an ill-defined region under the liver at the hepatic flexure.
Courtesy Ashley Davidoff, M.D.
Ascending Colon: Applied Anatomy
Angiodysplasia of the colon is an acquired arteriovenous malformation, which occurs most commonly in the cecum and ascending colon. It is not an uncommon cause of lower GI bleeding. When diverticuli bleed, they usually bleed from right sided diverticulosis even though in Western cultures the sigmoid colon is far more frequently involved with diverticulosis. Tuberculosis (TB) of the colon usually affects the right side of the colon. The radiological distinction between Crohn?s disease, carcinoma and TB may be difficult to differentiate. While carcinoma is described as having an apple core shape, TB is said to have a shape that is more reminiscent of a hourglass.
Other diseases that occur on the right side of the colon are relatively universal to the colon as a whole and include diverticulitis, ischemia and carcinoma
Barium enema of a 29-year-old male from India who presented with intermittent small bowel obstruction. TB was thought to be more likely but carcinoma and Crohn?s disease was in the differential diagnosis. The shape of the lesion seemed to be more like an hourglass than a apple core and so we favored TB. At surgery, colon carcinoma was diagnosed ? go figure. A classical apple core lesion is demonstrated in the sigmoid colon section below.
Courtesy Ashley Davidoff, M.D
.
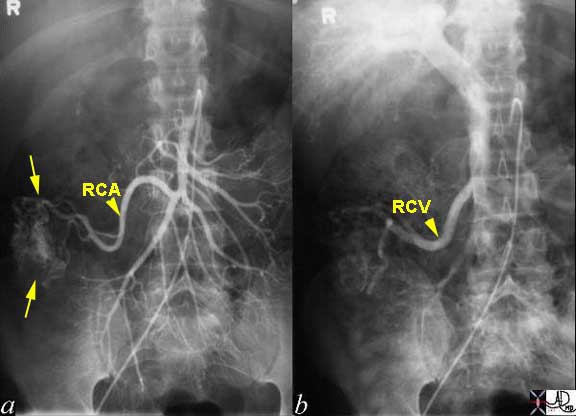
The angiogram from a 45-year-old man shows a hypervascular lesion (yellow arrows) in the mid portion of the ascending colon. The right colic artery (RCA) supplies the lesion and is enlarged as seen in Image A and a large right colic draining vein (RCV) is seen in Image B draining into the portal vein and into the liver.
Courtesy Laura Feldman, M.D.
Parts of the Colon: Hepatic Flexure
The hepatic flexure is the junction between the transverse colon and the ascending colon. There are no defining structural changes, other than for the endoscopist trying to navigate the colon who may be able to see the dark extrinsic impression of the liver on the colon, thus marking the distinction between the end of the ascending and beginning of transverse colon. The hepatic flexure receives its blood supply in part from the right colic vessels and in part from the middle colic vessels.

The beginning and end of the hepatic flexure (blue) are ill-defined, but it connects the ascending colon with the transverse colon.
Courtesy Ashley Davidoff, M.D.

Hepatic Flexure: Applied Anatomy
The close relationship of this part of the colon with the liver and gallbladder is sometimes relevant in disease. Occasionally an aggressive carcinoma may spread directly from the colon to the liver or gallbladder, making surgical resection difficult.

The coronal reformat from a frail and elderly woman shows a thick walled hepatic flexure with transmural extension toward the liver. Note the fluid filled colon caused by a mucin secreting adenocarcinoma.
Courtesy Ashley Davidoff, M.D.
Parts of the Colon: Transverse Colon
The transverse colon is the longest and most mobile part of the large bowel. It extends from the right upper quadrant to the LUQ usually dipping down in its mid portion, sometimes as far as the pelvis and then ascending to its highest position of the colon in the abdomen in the LUQ at the level of the splenic flexure.

In this patient the transverse colon (purple) is relatively short and only dips down a short distance before it ascends to the splenic flexure. The haustra are well demonstrated in this image. The right colon sigmoid and rectum are relatively empty suggesting recent evacuation. Note also that when the descending colon is empty it approximates the size of the small bowel. It has the smallest diameter of the colon.
Courtesy Ashley Davidoff, M.D.
Courtesy Ashley Davidoff, M.D.
The transverse colon ranges from 30-60cm in length and has a diameter that should measure less than 5cm.
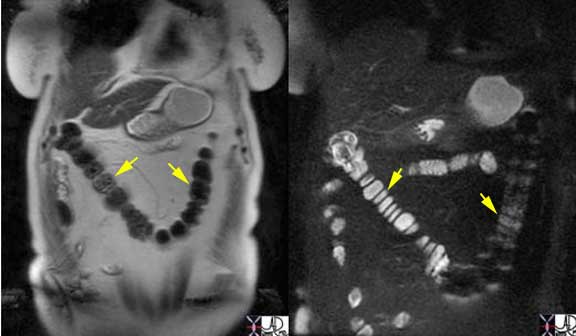
Coronal MR images of the normal and relatively decompressed images of the transverse colon (yellow arrows) demonstrating its location and shape. The low intensity of content on the T2-weighted image (left image) combined with high intensity seen on the T2-weighted image with fat suppression (right image) reflects fluid in the colon. In this case the transverse colon dips down deep into the pelvis.
Courtesy Ashley Davidoff, M.D.
The transverse colon is the most anterior portion of the large bowel, which is an important fact to remember and apply in the execution of a double contrast barium enema.
The first phase of the enema is to get the contrast into the cecum. The radiologist does not want to overfill the bowel with barium since for the double contrast study the barium is just needed to coat the wall and not to fill the lumen. It is the objective of the air to fill the lumen and for the barium to outline the mucosa. Less barium is better in the performance and optimization of the barium enema examination. Therefore, once the barium column reaches the splenic flexure the radiologist really wants to just roll the barium down the transverse colon up to the hepatic flexure, and then down the ascending colon ? a slow roller coaster ride. As the barium column reaches the splenic flexure, the patient is placed in the prone position so that the barium will be aided by gravity as it moves anteriorly in the transverse colon. In this position the barium should traverse most of the transverse colon after which a right decubitus should take the barium to the hepatic flexure. Getting it over the hepatic flexure hump is sometimes difficult but once accomplished it is downhill for the barium. The patient is placed supine as the technologist uncoils the enema tubes from the patients legs and the table tipped up in the grand hope of bringing the barium home safely into the cecum. Not always so easy. Once it is reached ? huge relief for the radiologist. Double contrast enemas are one of the most challenging examinations for the radiologist and knowledge of the position of the parts of the colon is essential to enlist gravity as an aide to move the barium and air.
The sagittal multiplanar reformat (MPR) of this abdominal CT scan shows the anterior position of the transverse colon (purple).
Courtesy Ashley Davidoff, M.D.
Parts of the Colon: Ligaments of the Transverse Colon
The transverse colon is suspended by two ligaments and acts as a support for a third. The two supporting ligaments are the gastrocolic ligament and the transverse mesocolon. The transverse mesocolon (tm) runs between the pancreas and the posterior and superior aspect of the colon (c). The gastrocolic ligament (gcl) also known as the lesser omentum runs between the inferior aspect of the stomach and the antero-superior aspect of the transverse colon. The greater omentum (go) is a thin apron of fat that hangs off the inferior aspect of the transverse colon.
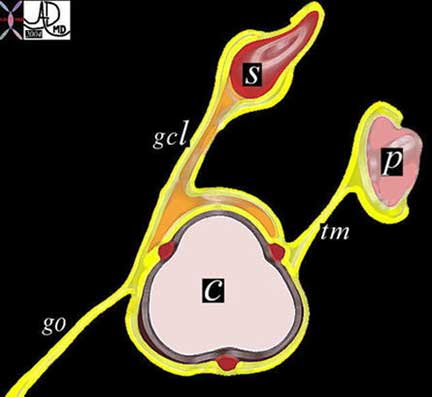
The transverse colon is suspended by two ligaments and acts as a support for a third. The gastrocolic ligament (gcl) extends from the stomach (S) to the anterosuperior aspect of the transverse colon (C), while the transverse mesocolon (tm) extends from the pancreas (P) to the posterosuperior aspect. The greater omentum extends as an apron of fat from the anterior aspect of the transverse colon for a variable distance sometimes reaching all the way to the pelvis.
Courtesy Ashley Davidoff, M.D.
The transverse colon receives blood mainly from the middle colic artery, but has crossover supply from both the right and left colic arteries. Venous drainage is via the corresponding veins and into the SMV and portal vein
Ligaments of the Transverse Colon: Applied Anatomy
Disease can spread along these ligaments so that in the case of diseases of the stomach, they can spread along the gastrocolic ligament to the superior aspect of the colon, while diseases such as pancreatitis can spread to the posterior and sometimes superior aspect of the colon. The greater omentum is notorious for collecting ovarian cancer deposits and when identified, the complex of the fat of the omentum and the soft tissue elements of the cancer has been described as ?omental cake?. It is therefore very important for the radiologist to examine the superior, posterior and inferior borders of the transverse colon which may hold clues to important diseases in the abdomen.

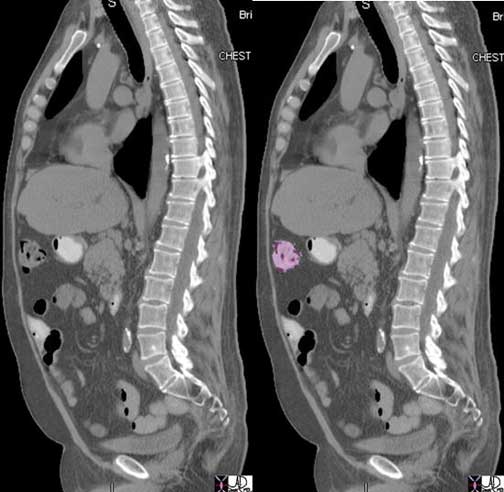
This patient has pancreatitis. Note the irregular and nodular changes of the superior border of the distal transverse colon just prior to the splenic flexure. These findings are caused by spread of the inflammatory process from the pancreas via the transverse mesocolon to the posterosuperior border of the colon.
Courtesy Ashley Davidoff, M.D.
Since the transverse colon is anterior and the greater omentum forms an apron of protection just below the anterior abdominal wall, they are both subject to traumatic injury. The following case represents the abdominal CT scan of a football player.

This CT coronal reformat is from a young college football player who presented with RUQ pain and fever. There is a region of homogeneous increase in attenuation of the greater omentum in the right upper quadrant (bright orange) which was shown to be hemorrhage in the omentum. The patient subsequently recalled that he had previously been hit in the abdomen ? an event which he had forgotten when questioned prior to the surgery. Note also the gastrocolic ligament (in light yellow aka lesser omentum) which connects the stomach above with the transverse colon below.
Courtesy Ashley Davidoff, M.D.
As stated above the greater omentum is a thin double layer of mesentery consisting of fat and connective tissue, that hangs off the transverse colon and seems to collect metastases particularly from the ovary, but also from gastric, pancreatic and colonic carcinoma as well. The nodules on the omentum are described as omental cake.
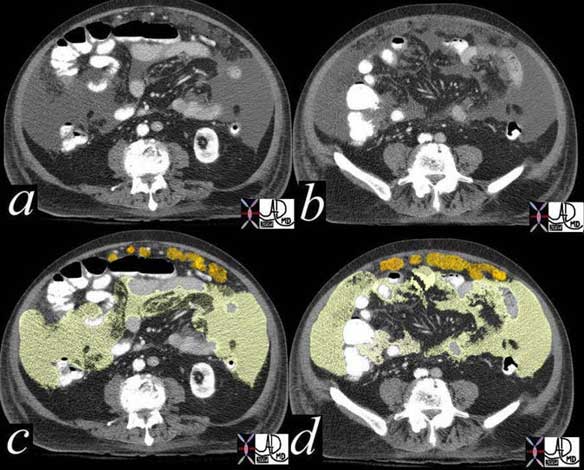
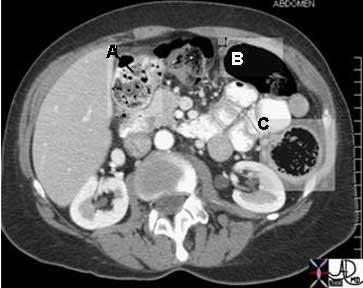
The CT is from an 81-year-old patient with metastatic pancreatic carcinoma which spread to the peritoneal cavity causing ascites (light yellow). In this instance the metastases can be identified as nodules on the greater omentum (orange) described by radiologists as omental cake. Image c is the overlay for a. Image d is the overlay for b.
Courtesy Ashley Davidoff, M.D.
Parts of the Colon: Transverse Colon Herniation
The transverse colon due to its anterior position as well as its redundancy is sometimes trapped in abdominal wall defects resulting in herniation. When the defect is large the colon can be reduced either spontaneously or manually. However, if the orifice is small strangulation and incarceration of the colon can occur, resulting in a surgical emergency.

Courtesy Ashley Davidoff, M.D.
When the hernial orifice, the hole through which the bowel protrudes is small, and the structural components in the hernia become more bulky for one of many reasons, the bowel in the hernial sac gets stuck, and cannot be reduced. This entity may be complicated by venous and then arterial compromise with resulting ischemia and infarction ? an entity known as an incarcerated hernia.

The CT images from a coronal reformat just off the anterior abdominal wall show a loop of transverse colon (overlaid in red) associated with surrounding edema of the subcutaneous fat. At surgery this was shown to be incarcerated. The pathology specimen is not from the same case but shows hemorrhagic infarction of small bowel.
Courtesy Ashley Davidoff, M.D., Grosspathology
Courtesy Barbara Banner, M.D.
Parts of the Colon: Toxic Megacolon
Toxic megacolon (eMedicine) is a life threatening condition where an underlying colonic disease suddenly accelerates and the patient presents with a severe clinical syndrome. The colon is not always dilated in this syndrome and hence a better term is toxic colitis. The dilatation, when it occurs is caused by an ileus thought to originate as a result of damage to the nerves in the submucosa by the disease. In the absence of normal function of these nerves, motility of the bowel is limited and hence an ileus results.
When toxic colitis presents with megacolon it is usually the transverse colon that is affected and the theory for its involvement relates to the position of the transverse colon. The ill patient usually being confined to bed lies predominantly in the supine position. Air in any part of the colon will rise to the most anterior part of the colon and therefore accumulates in the transverse colon. The transverse colon is therefore stretched and since the air cannot be transported due to the ileus, there is progressive dilatation of the transverse colon and hence progressive ischemia and worsening of the clinical situation.
There are multiple causes of the toxic colitis or toxic megacolon including ulcerative colitis, ischemic colitis, and pseudomembranous colitis.

The plain film of the abdomen shows a transverse colon that is greater than 6cms in a patient who has known ulcerative colitis with sudden clinical deterioration and marked systemic changes. Note that the distal descending colon has evidence of pinky printing (fine undulations of the air column) suggesting associated involvement with the colitis.
Courtesy Ashley Davidoff, M.D.
Parts of the Colon: Splenic Flexure
The splenic flexure is the junction between the transverse colon and the descending colon and is usually the most cranial portion of the colon. It is the embryological junction point between the midgut and hindgut, and is the watershed of two circulations so that it is the border where the circulations of the superior mesenteric artery (SMA) and inferior mesenteric artery (IMA) meet. Its drainage is via the corresponding mesenteric veins into the superior mesenteric vein (SMV) and then portal circulation. It is attached to the diaphragm by the phrenicocolic ligament. Like the hepatic flexure it can also vary in length and at its longest can be quite redundant with similar radiological difficulties to uncoil it during a barium enema.

The splenic flexure (yellow) in this single contrast barium enema is relatively short and almost a 90 degree turn. Note its cranial position ? it is the highest point of the colon in the abdominal cavity.
Courtesy Ashley Davidoff, M.D.

In this normal double contrast study, the splenic flexure has a steep climb to its mountain top position and then an almost 180 degree turn as it begins its steep descent.
Courtesy Ashley Davidoff, M.D.
Splenic Flexure: Applied Anatomy
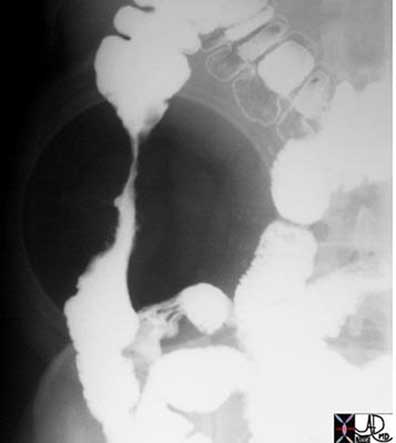
The colon cutoff sign (Pickhardt) is a characteristic finding in patients with pancreatitis where the inflammatory process extends along the tail of the pancreas to the left side where it comes into contact with a triangular ligament that connects the left colon to the diaphragm, just to the left of the lateral aspect of the transverse mesocolon. This ligament is called the phrenicocolic ligament because it is connected to the diaphragm (phrenic) on the one end and the colon on the other. As the inflammatory process spreads along this ligament it comes into contact and spreads the inflammatory process to the splenic flexure and proximal descending colon resulting in a reversible stricture caused by a combination of swelling and spasm.

The colon cutoff sign (yellow arrow) in the splenic flexure is obvious in this patient with acute pancreatitis. The cutoff in this instance is quite straight, but in most patients there is usually a sharp transition from dilated transverse to decompressed descending colon.
Courtesy Ashley Davidoff, M.D.
This is a beautiful example of the colon cutoff sign demonstrated by a single contrast barium enema in a patient with acute pancreatitis.
Courtesy Ashley Davidoff, M.D.
Parts of the Colon: Descending Colon
The descending colon originates after the splenic flexure and ends at the origin of the sigmoid colon in the pelvis. By the time the stool reaches this region most of the water and retrievable products have been absorbed and the descending colon acts as a storage station. The length of the descending colon is between 10 and about 25 cm and is between 3 and 4cm in diameter. When empty it may have the same dimensions as the small bowel. The peritoneum covers the front and the sides and binds it to the posterior abdominal wall giving it very little mobility. It takes a straight and narrow path and is given no freedom to move about the abdomen. In this location it lies in the retroperitoneum and therefore is relatively protected from intraperitoneal processes but open to the spread of retroperitoneal disease, the most common being acute pancreatitis.
It receives its blood supply from the left colic artery and drains into the left colic vein.

Two images from a double contrast barium enema show the proximal descending colon in the first image and the distal descending colon in the second. Note that the folds do not traverse the entire diameter of the colon.
Courtesy Ashley Davidoff, M.D.
The following cases reflect diseases that can occur anywhere in the colon, but in these instances affected the descending colon.
Descending Colon: Crohn?s disease
Crohn?s disease is usually thought of as an inflammatory disease of the small bowel but it can affect any part of the gastrointestinal tract, and not uncommonly affects the large bowel. In the large bowel it is referred to as Crohn?s colitis or granulomatous colitis. It is called ?granulomatous? because the most specific feature of Crohn?s disease for the pathologist, whether it occurs in the large or small bowel, is the finding of a granuloma or chronic inflammatory nodule in the submucosa.
It is important to remember that Crohn?s disease is a disease that affects all layers of the bowel wall so that in the acute stage the finding of pericolic fat involvement would be an important differentiating feature from ulcerative colitis which is a disease that usually only affects the mucosa. In the acute phases of Crohn?s there may be extensive ulceration of the mucosa so that only islands of tissue remain between the extensive ulceration. This appearance has reminded pathologists and radiologists of a cobblestone street and hence the descriptive term for this entity.

This pathological specimen reflects cobblestone changes in the terminal ileum in a patient with Crohn?s disease. The ?nodules? that you see are islands of normal mucosa between areas of extensive ulceration.
Courtesy Ted Gulkin, M.D.
In the chronic phase of Crohn?s disease, fibrosis results causing shortening, loss of pliability, thickening of the wall and narrowing of the lumen. This leads to the rubber hose or lead pipe appearance.

The transverse colon, splenic flexure and descending colon from this single contrast barium enema show a nodular mucosa which radiologists and pathologists have called cobblestone appearance.
Courtesy Ashley Davidoff, M.D.

Longstanding Crohn?s disease in this 59-year-old female patient has resulted in fibrosis with wall thickening, rigidity, luminal narrowing, and shortening of the bowel. These findings are demonstrated in the distal descending colon in this coronal reformat. ?Rubber hose? and ?lead pipe? have been descriptive phrases used by pathologists and radiologists for this appearance which can occur in ulcerative colitis as well.
Courtesy Ashley Davidoff, M.D.
Descending Colon: Lymphoma
Lymphoma is a disease that can present with involvement of the lymph nodes in a regional manner, so that it may present for example with involvement of the nodes of the neck as the presenting site. As the disease becomes more advanced, lymph nodes in other parts of the body such as mediastinum and then nodes on the other side of the diaphragm become involved. The involvement of regional nodes is the classical form of lymphoma. Sometimes, however, the lymphoid tissue in the submucosa is the site of origin of the disease and this may therefore occur anywhere where lymphoid tissue resides. In the gastrointestinal system the submucosa is the site where lymphoid tissue resides and its function is to protect the body from bacteria and other potentially harmful substances that may enter from the food or fluids we ingest. These lymphocytes can become neoplastic and develop into a localized form of lymphoma. Generally lymphoma does not incite much inflammatory reaction and since it is usually a soft mass, it only occludes structures when it is extremely bulky. Thus, when we identify a large mass in the intestinal system that does not obstruct and is not associated with significant pericolic changes in the fat, lymphoma is a prime consideration.

The descending colon (yellow arrows) in this image shows severe thickening of the wall with the lumen still fairly well maintained and very little pericoloc stranding. The usual expected donut appearance of the colon is not present in this case telling us we are dealing with a different animal. This animal normally lives in the submucosa and when it runs amuck it is called lymphoma.
Courtesy Ashley Davidoff, M.D.
Descending Colon: Posterior Abdominal Wall Hernias
Since the descending colon is fixed in the retroperitoneum it is not usually a part of the colon that herniates, nor does it usually undergo neither volvulus nor torsion. Occasionally it may protrude into a lumbar hernia or through a surgical defect of the posterior abdominal wall such as might occur in patients who have had a nephrectomy.

The surgery for nephrectomy is via the retroperitoneum and thus the approach is through the flank. The nephrectomy in this patient has resulted in weakness of the flank muscles, and herniation of the descending colon. The small bowel has not only taken up residence in the previous bed of the left kidney but has assumed its structural identity. Is it not remarkable how closely the loop of small bowel resembles the kidney and its vessels?
Courtesy Ashley Davidoff, M.D.
Courtesy Ashley Davidoff, M.D.
Parts of the Colon: Sigmoid Colon
The sigmoid colon pounces out of the retroperitoneum like a horse out of the barn, as it gains its freedom from the confines of the retroperitoneum. It acquires a cloak of long mesentery ? the sigmoid mesocolon that fans out from the base to the apex of the sigmoid colon. The freedom does come with a price and it is at risk for torsion or volvulus in the same way as the cecum is predisposed, though sigmoid volvulus is far more common than cecal volvulus. In the perfect world the sigmoid colon holds on to the feces it receives from the straight and narrow descending colon. Its shape and mobility allows it to store fairly large volumes feces. Although it usually resides in the pelvis it has the freedom to move up into the abdomen because of its mobility. When opportunity knocks it passes its product onto the rectum which signals to its owner the need to move on and out. If this message is received at an inconvenient time, the stool is forced back into the sigmoid, which holds onto the feces in storage until a more convenient time to evacuate is found.

The normal sigmoid colon (gold) is demonstrated in this double contrast barium enema. The shape and length as well as the diameter of the sigmoid colon are variable.
Courtesy Ashley Davidoff, M.D.
The sigmoid is ?s? or sigmoid shaped and hence its name. It is very different in shape to its predecessor in the chain ? the descending colon which is straight and the rectum which comes after it which is also relatively straight. It measures about 40 cm in length but can sometimes assume immense proportions both in diameter and length. (Bhatnagar) It is large in patients and cultures that have larger volumes of fiber in their diet and thus in Africa for example where dietary fiber is high the sigmoid colon is much larger. The incidence of sigmoid volvulus in these cultures is also much higher.
The sigmoid colon transitions to the rectum at about the level of the 3rd sacral vertebra. At the transition point the longitudinal muscles ? taenia coli, spread and incorporate the entire rectum. The pleating effect therefore disappears and consequently the rectum does not have haustra.

The CT scan shows the morphological differences between the normal sigmoid which is ?S? shaped and the rectum below which is straight. The sigmoid colon has taenia coli muscle and so it also has haustra whereas the rectum lacks taenia and therefore lacks a haustral pattern. The difference is typified in this image.
Courtesy Ashley Davidoff, M.D.
The sigmoid colon is supplied by branches of the inferior mesenteric artery and the venous drainage is into the inferior mesenteric vein.
Sigmoid Colon: Applied Anatomy
This entity describes an enlarged colon that is not related to mechanical obstruction and is characterized by a cecum that is larger than 12cm, an ascending colon larger than 8cms, or a rectosigmoid that is greater than 6.5cm.
It has three forms. We have discussed toxic megacolon and the other two are acute megacolon (Ogilvie?s syndrome) and chronic megacolon. In the cases shown below the megacolon and megarectum are of the chronic form.

This plain film is from an asymptomatic institutionalized patient. Talking about an organ that jumps out at you from the film ? diagnosis ? chronic megacolon. Previous films over a few years had shown similar appearance in this asymptomatic patient (aside from chronic abdominal distension) and hence sigmoid volvulus was not a clinical consideration.
Courtesy Ashley Davidoff, M.D.

A CT performed shows that the sigmoid measured 8.3cms in diameter and was filled with air.
Courtesy Ashley Davidoff, M.D.

In this case there is impaction of feces in the sigmoid colon and rectum but there is no evidence of obstruction because the rest of the colon is not dilated. These findings were of a chronic nature and unchanged. A diagnosis of chronic megacolon is likely.
Courtesy Ashley Davidoff, M.D.
Although it is rather surprising that the patient above was not obstructed other complications such as stercoral ulcers due to chronic irritation of the feces on the mucosa, and bowel ischemia from vascular compromise must be considered in the appropriate clinical setting.
Sigmoid Colon: Diverticulosis
Diverticulosis is a very common entity in Western civilizations and is thought to be due to the lack of fiber bulk in our diets. In the USA approximately 50-60% of the elderly have evidence of diverticulosis and it is found predominantly on the left side of the colon and most commonly in the sigmoid colon. In the Asian population interestingly, diverticulosis occurs predominantly on the right side. The rectum is not affected presumably because of the extra layer of longitudinal muscle that completely encompasses the circumference. The pathogenesis of the entity is thought to relate to excessive pressure build up in the colon due to strong peristaltic action on the low bulk content, causing excessive intraluminal pressure, muscular hypertrophy, mucosal thickening, bowel shortening, and to some degree luminal narrowing. The increased luminal pressure is transferred to the walls of the bowel and blow out predominantly of the mucosa through weak regions in the bowel wall occurs.
The diverticuli are easily identified on any of the diagnostic studies performed including endoscopy barium enema and CT scan.
Feces and debris may get trapped in the narrow necked diverticulum and result in an inflammatory response. Mucus secretion and swelling of the mucosa result, which in turn cause further pressure to build up in the diverticulum. The pressure on the walls may cause ischemia with microperforation with extension of the inflammatory process and infection to the surrounding fat. Complications include abscess formation, peritonitis, and fistulization to the bladder or skin. CT is the study of choice, and the diagnosis is made by finding inflammatory changes in the pericolic fat or of changes within the sigmoid mesocolon.
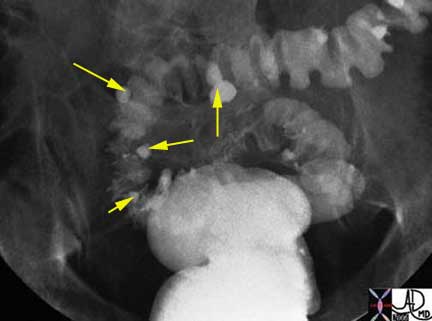
This patient demonstrates barium accumulations in diverticuli (yellow arrows) of the sigmoid colon associated with prominent circumferential muscle bands and minor degree of luminal narrowing. Note the absence of diverticulosis in the rectum.
Courtesy Ashley Davidoff, M.D.

In this CT scan of the pelvis the diverticular disease is seen as small outpouchings of gas (black circular areas) that extend beyond the expected confines of the wall of the bowel.
Courtesy Ashley Davidoff, M.D.
Parts of the Colon: Rectum
The rectum is a remarkable organ with its ability to detect the nature of its contents enabled by a rich supply of nerves and blood vessels. It can for example distinguish between solid stool, liquid stool, and air. It is far more complex in form, sensitivity, and muscular function than any other part of the colon.
The rectum is formed at about the 3rd sacral segment. As the sigmoid loses its freedom and dives back into the retroperitoneum to form the rectum, the three taenia coli expand to form a complete circumferential layer of longitudinal muscle rather than the three distinct bands. The rectum ends at the anorectal junction where it turns at an angle of about ninety degrees posteriorly at the perineal flexure into the anus.
Since there is no taenia coli in the rectum there are no haustra. Its walls are therefore relatively smooth but for three mucosal folds or valves that cross about one third of the diameter of the rectum ? two to the left side and one to its right. They are named according to their position as superior, middle and inferior rectal folds. The crescentic mucosal folds are also called Houston?s valves, and their function may be to partially support the stool so that all the feces do not drop in as one mass into the most dependent part of the rectum.

The rectum has 3 crescentic folds with the superior and inferior on the left and the middle rectal fold on the right. The superior fold marks the border between the first inlet part of the rectum above and the ampulla below. The inlet portion is narrow, widening at the ampulla and then narrowing again at the anorectal junction. The outlet portion contains the rectal columns and the pectinate line which is the anorectal junction.
Courtesy Ashley Davidoff, M.D.
The middle fold is an important clinical landmark since it is the approximate position of the peritoneal reflection. A perforation above the fold would result in stool contents leaking into the peritoneal space with widespread and potentially devastating clinical consequence, while a perforation below the middle fold results in a more confined leak into the retroperitoneal or extraperitoneal space. It also so happens that the distance from the anus to the middle fold is about 7cm, which is about the length of the examining finger. Thus, theoretically if one suspects a perforation and it can be felt by rectal examination then one is able to place it below the middle fold and therefore predict an extraperitoneal or retroperitoneal extension.
The upper part of the rectum above the middle fold may contain feces, but in healthy normal individuals the rectum should be devoid of stool. The finding of stool in the ampulla suggests a diagnosis of chronic constipation.
The upper portion of the rectum, above the superior fold is about the diameter of the sigmoid colon above. The middle portion, below the superior fold called the ampulla, is more capacious and distensible. At its inferior aspect the rectum again narrows at the level of the rectal columns just above the pectinate line also marking the position of the internal sphincter muscle.
Near the anorectal junction, the mucosa and some smooth muscle become heaped up to form the rectal columns between which are the rectal sinuses, and just below the columns is the pectinate line ? the border between the rectum and anus. Pectinate derives from the Latin word for comb since the shape of the line is reminiscent of a comb. It is also known as the dentate line because it also looks like a row of teeth.
The anorectal junction is the most distinct and obvious junction of the entire colon. It has embryological significance since the rectum derives from endoderm (an embryologic tissue responsible for bowel development) and the anus which derives from ectoderm (an embryologic tissue responsible for skin and brain development). The epithelium changes from the rectal columnar epithelium described above to a squamous epithelium. The lymphatic drainage changes from the internal iliac nodes and mesenteric nodes for the rectum, to the inguinal nodes for the anus, and it also marks the area of blood supply for the middle rectal artery above the line to the inferior rectal artery below the line. The pectinate line which is found about 2-3 cm from the anal opening, also marks the upper portion of the internal sphincter and the level of the internal hemorrhoids.
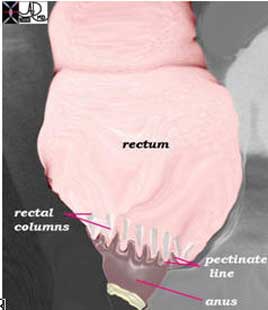
Courtesy Ashley Davidoff, M.D.

Courtesy Ashley Davidoff, M.D.
Although the word rectum means straight, when viewed from the lateral projection it is far from straight. The rectum conforms to the arch of the sacrum and coccyx, and when looked at from the lateral projection is seen to fit snugly into the gentle curve of the sacrum. At the anorectal junction the anus turns backward so that the anal axis from anal opening to anorectal junction is from posterior to anterior directed toward the umbilicus. This anatomic point is very important for all professionals who insert tubes, drains or scopes into the rectum. From the anal verge the catheter must be directed to an imaginary point that coincides with the umbilicus.
The rectum is about 12cm in length, and should be about 4cms in diameter. A rectum that is larger than 6.5cm is abnormal and considered a megarectum. As stated above, the rectum is a retroperitoneal organ. The sigmoid on its long mesentery is intraperitoneal. When the transition to rectum occurs the peritoneum initially covers the anterior and lateral walls of the rectum, then more distally only the anterior wall is covered while the lower third has no peritoneal covering.
The rectum has a dual blood supply. It receives supply from the IMA and the internal iliac arteries. The superior rectal arises from the IMA while the middle rectal and inferior rectal arise from the internal iliacs. The internal submucosal venous plexus situated in the upper portion of the rectum drains into the inferior mesenteric vein while the lower portion of the rectum and external hemorrhoidal plexus drains into the iliac veins. Carcinomas of the upper and middle rectal region will metastasize to the liver via the portal vein, while a tumor in the lower rectum will spread to the systemic venous system and will travel via the IVC and heart ending up as a metastasis in the lung.
In the female, one of the anterior relations of the rectum is the vagina and hence disease from the one can spread to the second. The result is a fistula between the two ? rectovaginal fistula.

Courtesy Ashley Davidoff, M.D.
Ulcerative Colitis (UC)
Ulcerative colitis is an inflammatory condition of the mucosa of the large bowel which characteristically starts distally in the colon involving the rectum progressing in a retrograde manner to the right side of the colon via the left side. As a rule the rectum is almost always involved. Backwash ileitis can occur when the cecum is involved. In severe cases the disease can spread to the deeper layers, and in long standing cases carcinoma can develop. The involvement of the deeper layers and the ileum creates difficulty for the radiologist and pathologist sometimes to distinguish Crohn?s disease and UC. The finding of granulomas as noted in the section on Crohn?s disease, distinguishes the two entities pathologically (eMedicine).
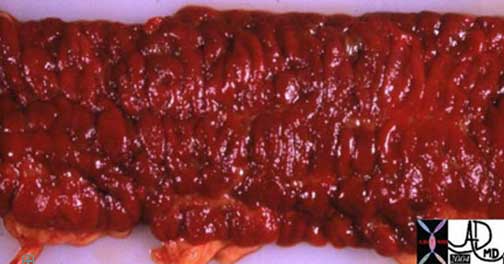
The pathology specimen reveals a hyperemic (swollen with blood) mucosa from a patient with severe acute hemorrhagic ulcerative colitis. The appearance is reminiscent of raw meat.
The radiology of acute ulcerative colitis was discussed in the section on diarrhea and is represented below again to correlate with the pathology image above.
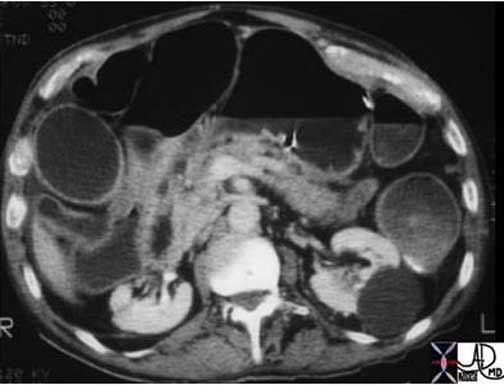
Note that in this patient the colon is mildly distended and the contents are fluid in nature. This 71-year-old male patient has diarrhea caused by ulcerative colitis which is a disease of the mucosa.
Courtesy Ashley Davidoff, M.D.
Chronic ulcerative colitis shows thickening, shortening rigidity sometimes becoming stiff and straight like a lead pipe. There is also accumulation of fat in the submucosa as well as in the pericolonic region.

Three distinct lines are noted in the wall of the rectosigmoid colon. There is the inner bright line that represents the mucosa and submucosa, the black line that represents fat infiltration in the submucosa and the outer white line that represents the muscularis and the serosa. The fatty infiltration reflects chronicty and is not specific for UC and can be seen in Crohn?s disease.
Courtesy Ashley Davidoff, M.D.
Parts of the Colon: Anus

There is a distinct anatomic border defining the junction which is not easily appreciated radiologically. In this cross section of the region as seen by MRI none of the mucosal landmarks are apparent. The luminal contents in this case are well-characterized as water, dark on T1-weighted (yellow arrow in the first image) and bright on T2-weighted in the second (yellow arrowhead) and one can almost make out the 4 components of the wall in the second T2-weighted image. As for the rectal columns and pectinate line ? they are currently not within the viewing range of our technology.
Courtesy Ashley Davidoff, M.D.
The anus is the last part of the colon. It consists of the anal canal which ends in the anal opening on the outside of the body. Anus means ring in Latin and it describes the shape of the organ.
There are two sphincters that extend across the anal length which is about 3 cm. The internal sphincter is the involuntary smooth muscle that is found in close association with the pectinate line and is situated more proximally. The external sphincter is a voluntary skeletal muscle and it is found along the anal canal and in close association with the external opening and therefore situated more distally. These muscles in the basal state are both contracted until the act of defecation. Thus the anal canal is closed by muscle contraction in its ?resting? state.
The anorectal angle is the angle of the axis of the rectum with the axis of the anus which is produced by yet another group of muscles that affect anorectal function. At rest the normal angle is between 90 and 110 degrees. This angle is kept in position by the puborectalis muscle which acts as a sling around the anorectal junction. The puborectalis is attached anteriorly to the pubic bones and posteriorly it forms its sling around the anorectal junction. It is contracted under basal conditions so the anorectal junction is pulled forward creating the described 90-110 degree flexure. This angulation helps maintain continence. During defecation the puborectalis relaxes, the angle is reduced and the passage is straightened and opened. This function occurs in concert with the relaxation of both the internal and external sphincters causing the canal to open gaining a passage for the feces to enter the free world?. but that is yet another story.
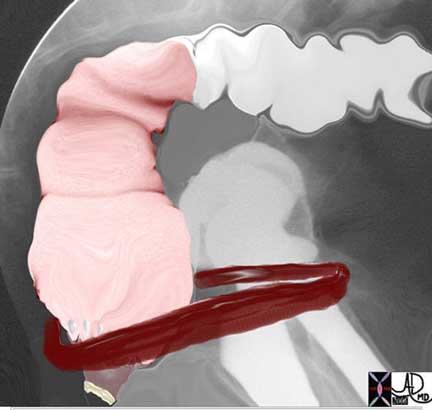
The puborectalis muscle (burgendy band) acts as a sling around the anorectal junction. It is normally contracted so that it pulls the anorectal junction toward the pubis resulting in a kink in the junction which helps to maintain continence. In this image the muscle is relaxed and the anorectal angle is thus reduced allowing the act of defecation.
Courtesy Ashley Davidoff, M.D.
The pelvic diaphragm is a hammock of skeletal muscle through which the pelvic viscera including the rectum pass. It is made of three muscles including the pubococcygeus, the ileococcygeus and the coccygeus muscle. The pubococcygeus is the anterior member, the ileococcygeus is in the middle and the coccygeus is posterior. The puborectalis described above is part of the inner portion of the pubococcygeus. The pubococcygeus and the ileococcygeus together form the levator ani muscles.
When feces enter the rectum the urge to defecate is initiated. The rectal distension results in relaxation of the involuntary smooth muscle of the internal sphincter. If the time is opportune the squatting or sitting position helps increase the intraabdominal pressure which pushes the pelvic diaphragm downward causing straightening of the anorectal angle. The voluntary signal to go forward and onward results in relaxation of the external sphincter and puborectalis and the anorectal angle is further straightened. Valsalva maneuver causes increased abdominal pressure which serves to flatten the levator ani and pelvic diaphragm even more, further providing a straight shot. Manually pushing on the abdomen also helps increase the abdominal pressure aiding in the pushing down of the pelvic diaphragm. Signals about the activities in the smooth and skeletal muscles get transmitted to the autonomic nervous system and mass peristalsis occurs allowing rectosigmoid to empty as well as the distal transverse and descending colon.
Nerve Supply
Control of the colonic function is a beautifully coordinated process. It is truly like a factory pipeline with activities of intake, processing, packaging, storage and transport an efficient and coordinated process. Events that are happening upstream in the stomach for example are sent by a messenger hormone gastrin, to get things going downstream by causing the ileocecal valve to open and allow emptying of the small bowel into the large in order to provide space for the new load of food. Peristaltic movements result in contraction in one palace in the bowel with receptive relaxation in another.
The nervous system with some help from the hormonal system, are the machines that are working quietly in the background connecting and controlling the processes. There are local control systems as well as systemic control systems. In the systemic systems the basic mechanism consists of a sensory system which senses and perceives the milieu in the bowel, and then sends signals via the afferent nerves to the spinal cord and the brain. The efferent nerves bring the signals back to the bowel of what has to be done, and neuromuscular endings carry out the orders by causing contraction or relaxation of muscles.
The sensors in the bowel wall are receptive to both chemical and mechanical stimuli. They are not able to sense temperature and pain from a pin prick for example, though excessive pressure does induce a painful sensation. The sensors that are responsible for identifying the local chemical milieu are thought to be located in the submucosa and are otherwise known as Meissner?s plexus, while those that sense pressure and other mechanical stimuli are found in the smooth muscle, and are known as Auerbach?s plexus (Sykes) (Kamm).
The autonomic nervous system is an involuntary system which is responsible for the minute to minute as well as the day to day functions of the colon. It consists of a parasympathetic system and a sympathetic system. In general the parasympathetic system in the gastrointestinal tract gets things moving by increasing peristalsis and opening valves and sphincters, and increasing blood flow to the digestive organs. In essence it promotes digestion and absorption, which is best done while the person is resting. The sympathetic system is the ?fight or flight? component, and directs energy and blood to skeletal muscle and other organs that need energy when a person is active, and in turn directs energies away from the gastrointestinal tract. Thus, in the digestive system, it slows things down by slowing peristalsis, closing valves and sphincters, and decreasing blood flow to the digestive tract. The nerves for the colon run with the arteries for the colon so that they travel with the superior mesenteric artery, inferior mesenteric artery, and internal iliac arteries. The plexuses and ganglia are halfway houses that receive afferent nerves from the bowel and efferent nerves from the spinal cord. They are located around the blood vessels and are named celiac, superior mesenteric, and inferior mesenteric ganglia, and superior and inferior hypogastric plexuses.
The controlling central organs for the autonomic nervous system are in the brain and are within the medulla, pons and hypothalamus. The afferent system carries the signals from the colon to the spinal cord and brain, while the efferent nerves carry the signals from the brain and spinal cord back to the colon. The afferent system for the sympathetic and parasympathetic nerves lies within the splanchnic nerves that run with the arteries of the bowel. The parasympathetic efferent system runs in the vagus nerve along the SMA controlling the right side of the colon and along the iliac arteries in the pelvic splanchnic nerves for the left side of the colon. The nerves that carry efferent sympathetic function run with the splanchnic nerves alongside the SMA (thoracic splanchnic nerve), IMA (lumbar splanchnic nerve) and internal iliac artery, as nerves derived from sacral segments 2, 3 and 4 are called the pelvic splanchnic nerves.
The voluntary nervous system that controls the external sphincter and levator ani muscles consists of the pudendal and inferior hemorrhoidal nerve that enable relaxation of these muscles.
Blood Supply
The superior mesenteric artery (SMA), inferior mesenteric artery (IMA), and internal iliac arteries are the vessels that supply the colon. The SMA is the artery of the midgut while the IMA is the artery of the hindgut. The distal and terminal portion of the hindgut is supplied by the rectal branches of the internal iliac arteries.
Blood Supply: Superior Mesenteric Artery (SMA)
The superior mesenteric artery (SMA), as the midgut artery supplies the right side of the colon from the ileocecal valve to the region of the distal transverse colon and splenic flexure. The SMA shares the supply of the splenic flexure with the IMA, and therefore does theoretically help supply the proximal hindgut.
The SMA arises from the aorta between T12 and L2. The usual branches of the SMA to the colon include the ileocolic artery, the right colic artery and the middle colic artery, supplying in general the cecum ascending colon and transverse colon respectively. The ileocolic artery almost always arises directly from the SMA. The right colic may arise from the SMA, but sometimes arises from one of its branches ? the ileocolic or the middle colic artery. The middle colic artery strangely arises from the SMA from a more proximal position in the SMA than the ileocolic even though it supplies the colon that is more distal in location. Its origin is at the first part of the SMA close to the origins of the jejunal branches.
The branches course in the mesentery and extend to the medial and mesenteric edge of the ascending colon, and then branch so that they course and connect along the inner margin of the colon forming the marginal artery allowing the branches to connect with each other. In the transverse colon the mesenteric edge is posterior and hence the marginal artery is posterior. The vasa recta (recta = straight) branch from the marginal artery and course over the colon finally penetrating the wall of the colon to form a capillary network in the submucosa. Once the vessels proceed beyond the marginal artery and into the bowel wall, there are not usually collateral pathways so that any occlusion beyond the marginal artery will result in ischemia.
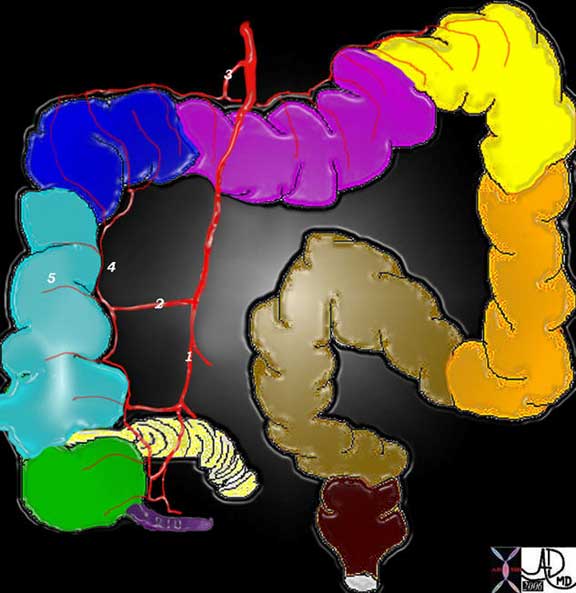
The diagram shows the branches of the SMA including the ileocolic (1), right colic (2) and the middle colic (3). These vessels connect through the marginal artery (4) which runs along the inner or mesenteric border of the colon (5) and gives rise to the vasa recta that run over the colon before branching into the wall of the colon to finally enter the submucosa.
Courtesy Ashley Davidoff, M.D.
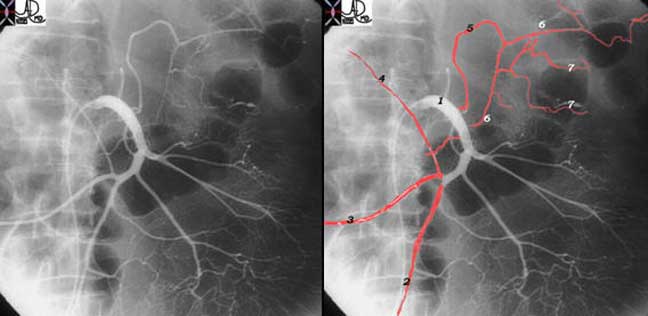
The three major branches to the right colon are demonstrated arising from the SMA (1). The ileocolic (2) right colic (3) and the middle colic (5) arise in usual fashion. A hepatic flexural artery is occasionally present, and is shown in this patient (4). Note that the middle colic (5) arises as the first colic artery even though it supplies a distal portion of the right colon. It divides in two, with one part of the marginal artery going to the right and the other to the left (6). The right sided branch will finally connect with the marginal vessels created by the ileocolic and right colic arteries. The left part of the marginal branch courses to the splenic flexure where it will connect with the marginal component of the left colic artery created by the sigmoid and left colic arteries. The marginal artery gives rise to the vasa recta (7) which course over the colon before penetrating the wall of the colon.
Courtesy Ashley Davidoff, M.D.
The SMA and celiac axis connect through the pancreaticoduodenal arcade that runs through the head of the pancreas and also connect to some extent through the transverse pancreatic artery that runs through the body and tail of the pancreas. The arc of Buehler is an embryologic connection between the SMA and celiac axis that is seen uncommonly as a persistent communication. The SMA also connects to the IMA via the marginal artery on the left side of the colon. Thus the three major arteries and circulations do have important connections that become life saving when one becomes narrowed or blocked.
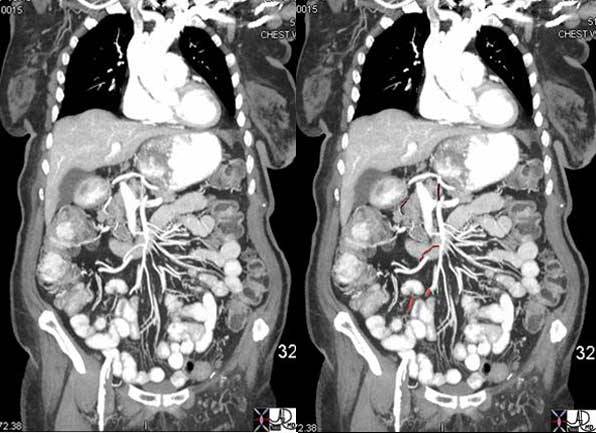
CTA of the abdomen can easily identify the proximal portions of the mesenteric vessels and is able to depict the first order of branches reasonably and accurately as well. In this image one is able to see remnants of the ileocolic, (bright red) right colic (light maroon) and parts of the middle colic (dark maroon) at 7, 9, and 12 o?clock respectively. The thinner arteries are seen coursing with slightly plumper veins to the jejunal branches to the left side.
Courtesy Ashley Davidoff, M.D.
Blood Supply: Applied Anatomy
Disorders of the SMA arterial circulation are relatively common including bowel ischemia from thrombosis, embolization, dissection, and hypotension. Disorders that lead to lower GI bleeding include angiodysplasia and diverticular disease.
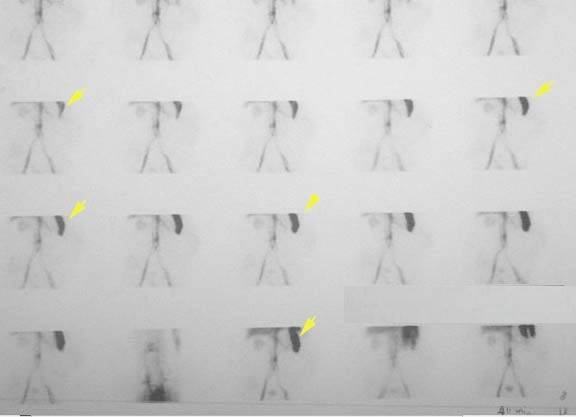
Courtesy Ashley Davidoff, M.D.

The angiogram of the SMA shows a worm like accumulation of contrast (bright red) appearing at the bottom of a puddle of blood (pink blob) noted to be arising from the left side of the middle colic artery. In the course of the angiogram, one first sees the spillage of contrast as the bright red worm like accumulation and as the contrast continues to spill into the bowel lumen it becomes a puddle of less dense contrast as it mixes with colonic content and spreads.
Courtesy Ashley Davidoff, M.D.

The ability to achieve subselection of the vasa recta allowed us to embolize the bleeding vessel with metallic ?coils?. An X-ray of the specimen shown in figure 2 reveals the metallic coil within the resected splenic flexure. The cause of the bleed was a hemorrhaging diverticulum.
Courtesy Ashley Davidoff, M.D.

These magnified views of an aortic dissection (a) (arrowhead) show extension of the dissection noted as a fine line in the aorta in (a), into the SMA characterized by a linear lucency in the SMA (b) (arrow) . There is a collar of increased density around the SMA in (c) and (d) (arrowheads) , representing periadventitial rupture, meaning a contained rupture in the last layer of the blood vessel.
Courtesy Ashley Davidoff, M.D.
Blood Supply: Inferior Mesenteric Artery (IMA)
The inferior mesenteric artery (IMA) originates from the aorta around L3 and is a fairly small vessel arising at an acute angle. One therefore has to choose a catheter that has an acute angle in order to engage this vessel for selective catheterization.
In its proximal portion the vessels parallel the aorta for about 3-4 cm. Its branches include the left colic, sigmoid branches and superior rectal artery. As stated above, it connects with the SMA via the marginal artery with a watershed region created in the splenic flexure. Since this region is an end arterial circulation for the SMA and IMA it is potentially a weak link in the circulation predisposing it to ischemia.
There are three major branches of the IMA including the left colic artery, sigmoid arteries (usually about 2-3 vessels) and the superior rectal artery (aka superior hemorrhoidal artery).
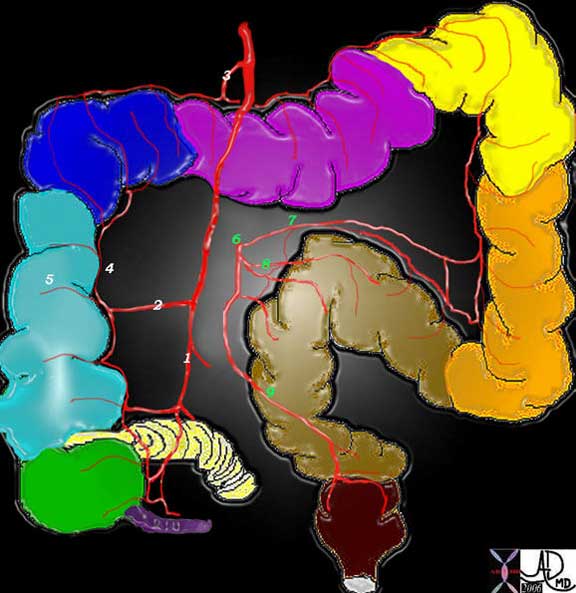
The IMA (6) gives rise to the left colic artery (7), 3 sigmoid branches (8) and the superior rectal artery also known as the superior hemorrhoidal artery (9).
To review: The diagram shows the branches of the SMA including the ileocolic (1), right colic (2) and the middle colic (3). These vessels connect through the marginal artery (4) which runs along the inner or mesenteric border of the colon (5) and gives rise to the vasa recta that run over the colon before branching into the wall of the colon to finally enter the submucosa.
Courtesy Ashley Davidoff, M.D.
Blood Supply: Internal Iliac Arteries
The iliac arteries supply includes mid to distal rectum and anal regions. They provide an important collateral pathway between the systemic circulation at large with the mesenteric circulation. The middle and inferior rectal branches supply the distal rectum and anal regions.
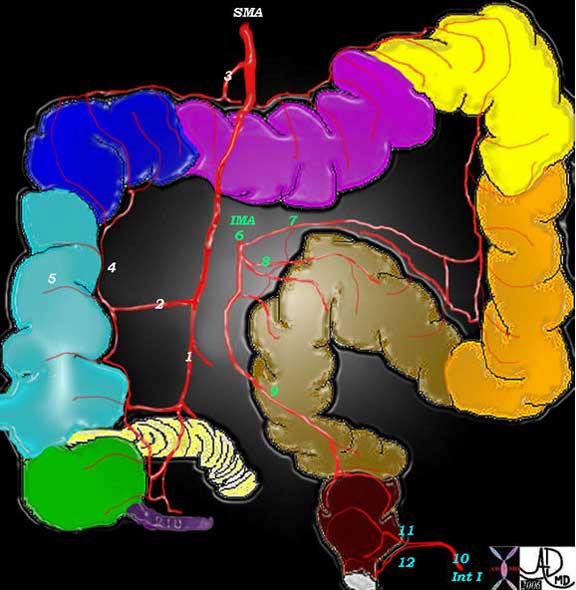
The internal iliac artery (10) supplies the distal part of the rectum and gives rise to the middle rectal artery (11), and inferior rectal (12) arteries. These are paired arteries arising from the left and right iliacs and they are connected through collaterals with the superior rectal artery.
Courtesy Ashley Davidoff, M.D.
The single superior rectal artery arises from the terminal portion of the IMA, and divides initially into two main branches, one supplying the left side and one the right of the upper portion of the rectum. The middle and inferior rectal branches on the other hand, have paired origins, one arising from the left internal iliac and the other from the right internal iliac artery.
Venous Drainage
The final common pathway of colonic venous drainage is dominantly via the portal system but also via the systemic venous system using the internal iliac veins to gain access to the IVC. The veins in general follow the course of the arteries and are similarly named. Thus, there is a superior mesenteric vein (SMV), inferior mesenteric vein (IMV) and rectal or hemorrhoidal veins. The SMV usually drains with the splenic vein into the portal vein and in fact their confluence gives rise to the portal vein. The IMV usually drains into splenic vein. The middle rectal vein and inferior rectal vein drain into the internal iliac veins and then into the IVC as stated previously.

This MPR of the abdomen shows middle colic venules and arterioles in the transverse mesocolon becoming confluent to form the right and left branches of the middle colic vessels.
Courtesy Ashley Davidoff, M.D.

A
Coronal CT scan shows the normal appearance of the superior mesenteric artery and superior mesenteric vein. The artery is to the left, smaller in diameter, and in this instance slightly brighter. The SMV is to the right, larger, and becomes confluent with the splenic vein to form the portal vein which courses to the liver.
Courtesy Ashley Davidoff, M.D.

This image shows jejunal veins to the left of the patient’s body and ileocolic vein draining the proximal ascending colon. The SMV, splenic vein and portal vein are again demonstrated. Note how close this image correlates with the venographic phase in the next image.
Courtesy Ashley Davidoff, M.D.
There are two venous plexuses in the anorectal region. The superior hemorrhoidal venous plexus lies above the pectinate line and is covered with mucosa. The inferior hemorrhoidal venous plexus lies below the pectinate line, and is covered by anoderm and perianal skin. The superior plexus drains into the superior rectal vein while the inferior drains into the middle and inferior rectal veins.
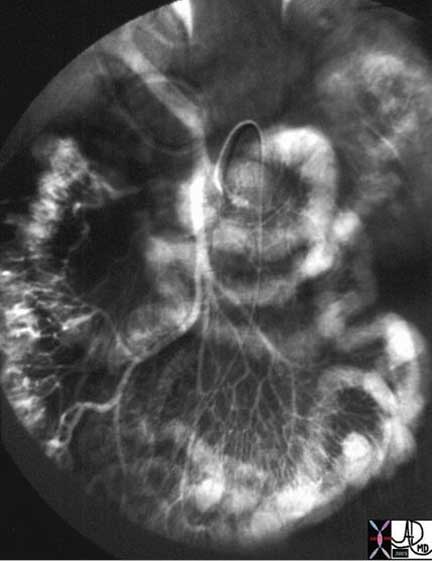
This venous phase of a SMA injection shows jejunal veins to the left, ileocolic and right colic veins to the right, entering into a common SMV which at the porta hepatis joins with the splenic (not opacified) to form the portal vein.
Courtesy Ashley Davidoff, M.D.
Venous Drainage : Applied Anatomy
There are two types of hemorrhoids ? internal and external. The internal hemorrhoids are caused by varicosity and distension of the internal plexus while external hemorrhoids are caused by similar changes in the external plexus. Both are caused by increased intraabdominal pressure that may be caused by chronic constipation, obesity, pregnancy. They can also be caused by venous hypertension as might be related to portal hypertension.
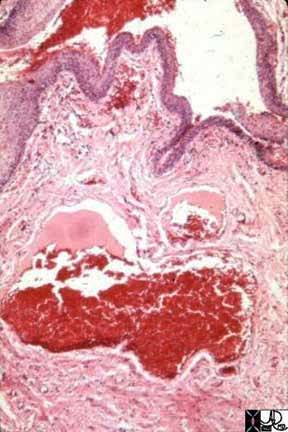
This microscopic section shows dilated veins in the submucosa characterized by the large venous channels filled with blood (red). This finding is characteristic of internal hemorrhoids.
Courtesy Barbara Banner, M.D.
Lymphatic Drainage
The lymph nodes are named mostly according to the vessels along which they travel. Thus the names include the ileocolic, right colic, middle colic, left colic, sigmoid, superior rectal, middle rectal, and inferior rectal lymph nodes. These in turn drain to the appropriate group of nodes situated at the origin of main mesenteric vessels including the SMA, IMA and iliac nodal stations. The nodes that are along the mesenteric border where the marginal artery is located are called the paracolic nodes. In addition there are two special groups of nodes around the cecum. One group is called prececal and the second is called retrocecal ? both named according to their position with respect to the cecum.
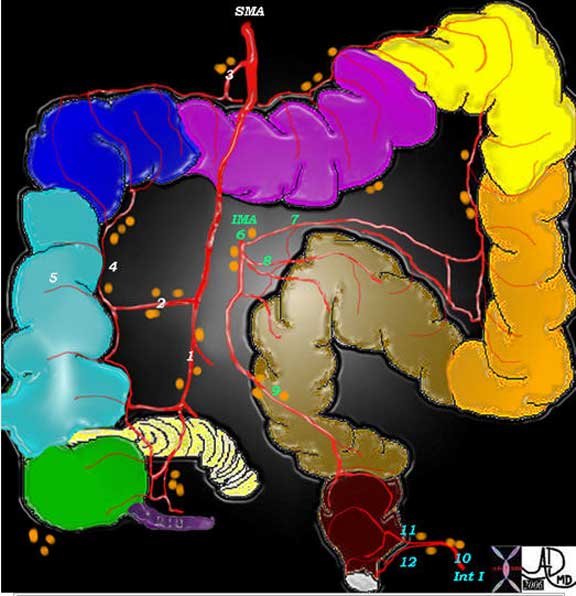
The lymph nodes are named according to the blood vessels with which they travel. Thus there is the ileocolic group (1) right colic (2), middle colic (3) left colic (7), sigmoid (8), superior rectal (9), middle rectal (11), and inferior rectal (12). These nodes drain into the regional halfway houses for the nodes including the SMA, IMA and iliac groups. The paracolic groups are located along the marginal artery (4) and the prececal and retrocecal are seen in relation to the cecum.
Courtesy Ashley Davidoff, M.D.
The solitary lymphatic nodules of submucosal lymphoid tissue in the large intestine are most abundant in the cecum and appendix, but are also found throughout the rest of the colon.
Lymphatic Drainage: Applied Anatomy

The paracolic lymph nodes (orange overlay) travel with the marginal artery along the mesenteric border of the colon, and are seen as sub centimeter soft tissue densities along the upper border of the decompressed colon. They are situated in this case within the transverse mesocolon along the middle colic territory. These are not usually as large as this but were prominent in this patient who had bulky lymphomatous nodes along the superior mesenteric vessels.
Courtesy Ashley Davidoff, M.D.
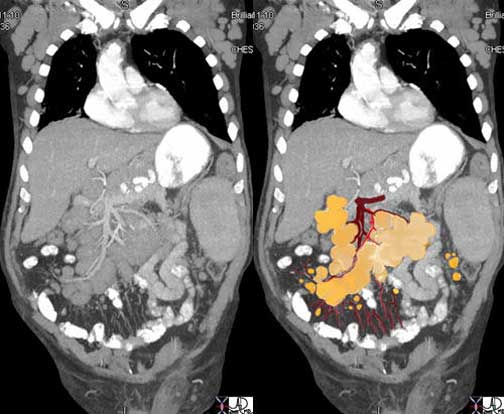
This elderly man has lymphoma and the enlarged lymph nodes are clustered around the SMV (maroon) and SMA (red) like a bunch of grapes. Smaller nodes are also seen in the small bowel mesentery and along the left colic and left paracolic region.
Courtesy Ashley Davidoff, M.D.
Imaging the Colon
The plain film of the abdomen was the initial study that enabled physicians to study the colon after Roentgen discovered X-rays in 1895, while barium sulphate as a contrast agent in the intestinal tract was first used by Krause in 1910 (Schott). The plain film still remains the study of choice for patients suspected of having acute colonic disease in the emergency room, particularly when bowel obstruction, volvulus, ischemia, or bowel perforation is suspected. Prior to colonoscopy, use of the single contrast barium enema, followed by double contrast barium, were the only methods available for the diagnosis of mucosal disease. With the development and refinement of colonoscopy starting in the 1950?s, it is now the procedure of choice to study the mucosa since it not only allows direct visualization, but also provides an opportunity to intervene if necessary. The concept of ?point of care? is an important evolving concept in medicine and relates to the timely relationship between diagnosis and treatment. The closer in time that accurate diagnosis, and successful treatment can come, the more valuable the care. In the case of colonoscopy, the ability to first diagnose an abnormality and then move forward with either a biopsy for definitive diagnosis, or definitively treat a small polyp or bleeder at the same sitting for example, makes this a valuable ?point of care? tool. It is, however, a procedure that usually requires sedation, carries a small risk of perforation ( 0.2-0.4% with diagnostic colonoscopy and 0.3-1.0% with polypectomy) (eMEdicine).
Full visualization of the colon is not always accomplished by colonoscopy due to redundancies or severe obstruction. Colonoscopy requires insufflation of air so that in patients with severe inflammation or a weakened wall the risk of rupture or translocation of organisms into the circulation is limiting, and therefore the procedure is relatively contraindicated in these conditions. Lastly, colonoscopy is a technique that is focused to the mucosa of the bowel and is not able to evaluate the deeper layers. Conventional CT on the other hand is able to evaluate the wall of the colon and also allows a global view of the abdomen. Identifying small polyps and sometimes even large mucosal masses is not consistently within the realm of conventional CT for a few reasons, but mostly due to the presence of feces, and the variable degrees of distension and non distension of the bowel which can mask soft tissue changes like a mass. CT colonoscopy is a study of the clean colon with the use of air to distend the colon. This allows the radiologist to evaluate the mucosa, and polyps as small as 5mms can be identified. In patients who have had a failed colonoscopy it is the study of choice. It is not uncommon to have a patient transported to CT from the endoscopy suite, to complete a colonoscopic study because the endoscopist had failed to traverse a redundant colon or a severe obstruction. Despite its strength to evaluate the wall it cannot differentiate the layers of the wall as well as ultrasound or MRI. These studies are limited at this time to the rectal wall only, but their ability to define the layers is exquisite and they play a very important role in the staging of rectal cancer by defining the extent of tumor penetration into, and sometimes through the wall. The depth of tumor penetration has bearing on how a tumor will be treated. In order for the US or MRI to obtain the necessary resolution the probes have to be in close contact with the mucosa, limiting the techniques at this time to the evaluation of the rectal wall.
PET-CT has been an extremely valuable addition in the management of cancer in general, but in the colon has found specific applicability in staging the disease and for detecting recurrence.
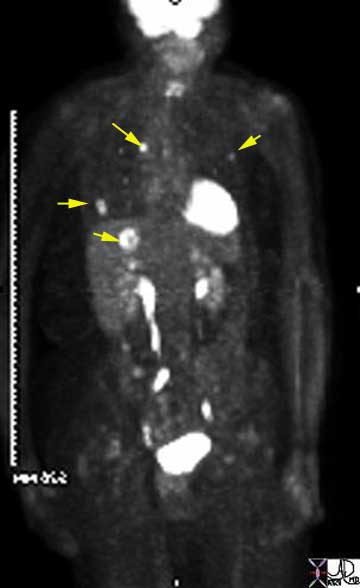
In this elderly female with known sigmoid colon carcinoma, the PET CT is positive for metastatic disease in the liver, lungs, and mediastinum. The findings include high FDG uptake in a single focus in the dome of the right lobe of the hepatic parenchyma, as well as in multiple small foci in both lungs, and a single very bright focus in the mediastinum. These findings reflect stage IV disease.
Courtesy Ashley Davidoff, M.D.
Conclusion
The colon as you have now learned is a remarkable and interesting organ. Its basic structure is universal to the intestinal tract and to some extent universal to other tubular organs of the body, but it has some unique features. The appendices epiploica are the oddest. The taenia and haustra are not only elegant but also quite pleasing in their appearance and unique and important in their function. Each part of the colon also has unique features that relate to function. The ileocecal valve with its fatty lips, the rotund cecum with its blind bottom end,, the straight and fixed ascending and descending colon and the swingers of the family in the transverse colon and sigmoid, are all quite remarkable. The swingers because of their mobility have a higher likelihood of getting into trouble with the law of physics, since if they swing too much they can get into a twist. Apart from the mechanical diseases, the inflammatory diseases with particular reference to Crohn?s disease and ulcerative colitis are the common ailments that affect the colon. Pseudomembranous colitis is another common disease that is seen frequently in the hospital based population. Imaging and endoscopy play an important role in tumor detection and treatment with the result of a declining incidence of colon cancer in the culture.
Knowledge of the blood supply is at first glance complicated but once mastered is applicable to the venous system and lymphatics. The repetition of the concepts is intentional in the module with the aim of enhancing memorization and understanding.
The future is interesting with virtual CT evolving into a mature technique, CTA and MRA taking over the function of diagnostic angiography. Accurate evaluation of perfusion and consistent diagnosis of ischemia still eludes us, and PET CT has become an invaluable tool in detection, staging, and management of colon cancer.
References
Books
Gray’s Anatomy of the Human Body
Henry Gray ?
30th Edition 1984
Lippincott Williams & Wilkins
Histology: A Textbook and Atlas
Ross MH, Romrell LJ, Kaye G.
3rd ed. 1994.
Lippincott Williams & Wilkins
Textbook of Medical Physiology
Guyton, AC, Hall JE.
10th Edition 2000
Elsevier Science
The Ciba Collection of Medical Illustrations
Vol 3 The Digstive System Part II
Lower Digestive Tract
Netter FH
2nd edition 1980
Ciba Pharmaceutical Division
Journals
Balthazar, EJ , Birnbaum, BA., Yee, J., et al Acute appendicitis: CT and US correlation in 100 patients. Radiology, Vol 190, 31-35
Bhatnagar BN, et al Study on the anatomical dimensions of the human sigmoid colon. Clin Anat. 2004 Apr;17(3):236-43
Benjaminov et al Frequency of Visualization and Thickness of Normal Appendix at Nonenhanced Helical CT Radiology 2002;225:400-406)
Horton et al CT Evaluation of the Colon: Inflammatory Disease Radiographics. 2000;20:399-418. excellent
Kamm M A Why the enteric nervous system is important to clinicians Gut 2000;47(Suppl 4):iv8-iv9
Kunzellman et al Electrolyte transport in the mammalian colon: mechanisms and implications for disease. Physiol Rev. 2002 Jan;82(1):245-89.
Lane et al Suspected Acute Appendicitis: Nonenhanced Helical CT in 300 Consecutive Patients
Rao et al Primary epiploic appendagitis: evolutionary changes in CT appearance. Radiology 1997; 204:713-717.
Rao et al. Appendicitis: use of arrowhead sign for diagnosis at CT. Radiology 1997; 202:363-366.
Phillips et al Functions of the large bowel: an overview. Scand J Gastroenterol Suppl. 1984;93:1-12.
Pickhardt et al The Colon Cutoff Sign Radiology. 2000;215:387-389.)
Schott Some Observations On The History Of The Use Of Barium Salts In Medicine Med Hist. 1974 January; 18(1): 9?21.
Simon et al Isolated Infarction of the Cecum: CT Findings in Two Patients Radiology. 2000;214:513-516.)
Electronic References and Interesting Links
ACR Appropriateness Criteria
Colorectal Screening Cancer (Update in Progress)
Pre-Treatment Staging of Colorectal Cancer (Update in Progress)
Cleveland Clinic Colonic Diverticular Disease Aydin, et al
Cleveland Clinic Acute Diarrhea Sanaka, et al
CTisUS CT Of Cecal Volvulus – Unraveling The Image:
eMedicine 5*
Atresia, Stenosis, and Other Obstruction of the Colon
Cecal Volvulus Khan.
Colon, Adenocarcinoma Radiology
Colonoscopy Bonheur
Diverticulitis Kooperman
Intussesception Child Wood
Polyposis Familial Adenomatous
Polyposis Syndromes Radiology
Polyps Medicine
Polyps Radiology
Toxic Megacolon Rossi
Tumors Pediatrics
Typhlitis Stoehr
Ulcerative Colitis Khan
First Principles of Gastroenterology
Physiology of the Colon Vanner 5*
Lapsurgery.com Laparascopic Treatment of Cecal Volvulus Armstrong et al
Merck Pathology.com
Radresources and Radquiz links to Organizations and Journals 5*
Report of a Joint FAO/WHO Expert Consultation 1997 Physiological Effects of Dietary Fibre
Supportive Oncology Pathogenesis of Constipation Sykes
University of Washington On Line Syllabus on the Colon
First Principles of Gastroenterology ? Turnbull et al
Links
(5* = excellent, 4* very good, 3* good)
Dictionary
Etymology Univ. of Penn.
Myth Terminology
Databases
Anatomy
Grays 5*
Physiology
First Principles of Gastroenterology
Physiology of the Colon Vanner 5*
Histology
Pathology
Clinical Medicine
eMedicine 5*
Imaging
ACR Appropriateness Criteria
Colorectal Screening Cancer (Update in Progress)
Pre-Treatment Staging of Colorectal Cancer (Update in Progress)
Rennes Atlas 4*
RSNA 2005
On Line Education Exhibit 2005 5*
Acute and Chronic Portal Vein Thrombosis: A Pictorial Review
Normal and Pathologic Anterior Abdominal Wall: MDCT Findings
Pelvic MR Imaging in post Surgical -Anorectal Disease
Pitfalls in MDCT Colonography: A Systematic Approach
Pictorial Review of Common and Uncommon Abdominal Hernias
Role of Biphasic CT and Mesenteric CT Angiography in the Evaluation of …