| Suspect Acute Cholecystitis – Imaging Strategy
Author: Charles Allison, MB ChB
Editor Ashley Davidoff MD
copyright 2006
CLINICAL BACKGROUND –
The “classical ” presentation of acute cholecystitis is characterised by intermittant RUQ pain that lasts for 1-6 hours with intermittant colicky components when the intensity of the pain increases. Precipitaing factors include a recent ingestion of a meal.. The pain may radiate to the right scapula or shoulder. Associated symptoms include nausea and vomiting, fever and chills. While the wcc is usually elevated, a normal wcc does not exclude the diagnosis. The bilirubin and alakaline phosphatase are usually slightly elevated. Murphy’s sign is diagnostic.
WHAT STUDY?
Ultrasound is the investigation of choice in this patient with suspected acute cholecystitis. Findings of a probe tender, distended gallbladder, with fluid in the gallbladder fossa and gallstones are pathognomonic features. Plain abdominal film is not helpful in the diagnosis. In the equivocal case when ultrasound is not characteristic and the clinical suspicion is strong, an imaging alternative is a HIDA scan.
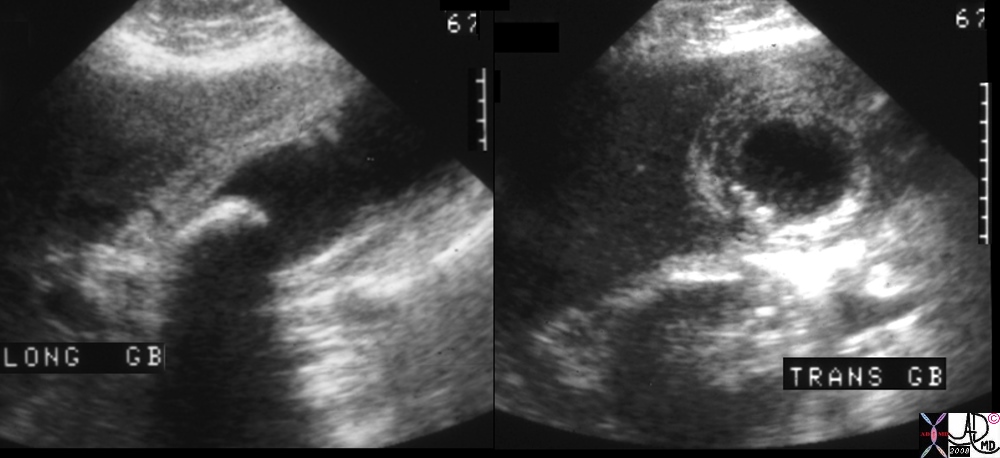 Acute Cholecystitis Acute Cholecystitis |
| 00401.1cs 67Male right upper quadrant pain RUQ pain positive Murphy’s sign gallbladder gallbladder fossa thickened linear lacy thickening gall stones calculi calculous large stone in the infundibulum shadowing multiple small stones cholelithiasis cholecystitis acute cholecystitis acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008 |
WHY?
Ultrasound provides a non-invasive method for establishing evidence of gallstones / gallbladder inflammation as a cause for the symptoms. Acute cholecystitis is an indication for cholecystectomy. If the symptoms are of less than 48 hours duration this can be performed immediately; alternatively, the gallbladder may be removed after the inflammation has settled in 4-6 weeks (interval cholecystectomy).
BACKGROUND TO THE DISEASE:
Gallstone disease affects 10-20% of the population, though the majority are asymptomatic incidental findings. Classically occur in fair, fat, fertile females in their forties ? fifties. Most gallstones are predominantly cholesterol (80%, often solitary if solely cholesterol), but may also be pigmented (formed from bile with less than 25% cholesterol content, usually multiple and irregular) or mixed (faceted appearance, calcium containing). 90% of patients who develop acute cholecystitis have gallstones. Symptoms typically follow impaction of a gallstone in the cystic duct. It is differentiated from biliary colic mainly by the presence of inflammation (fever, leucocytosis, local peritonism); also the pain is not necessarily associated with food.
WHEN?
Ultrasound should be performed at time of presentation, as the patient requires immediate management.
HOW TO ORDER?
The patient should be hospitalized; the investigation may be performed in the emergency room or as an inpatient as an urgent study.
When ordering an ultrasound for acute cholecystitis it is important to reference the symptom or the sign as the clinical indication and not the diagnosis.
ie Patient with “RUQ pain” is acceptable
Patient with R/O cholecystitis is not acceptable.
Patient with “RUQ pain, R/O cholecystitis” is optimal
The examination is called a “limited RUQ ultrasound”
PATIENT PREPARATION
The patient for US should be fasting for 4 hours and the study should take about thirty minutes.
CLINICAL RED FLAGS:
A triad of jaundice, fever and RUQ pain (Charcot?s triad) is indicative of cholangitis, which has a high mortality if not treated promptly with appropriate antimicrobials (to cover enterococcus and enteric organisms, typically 3rd generation cephalosporin and metronidazole). Acalculous cholecystitis, in which no gallstones are visualized, may be seen in the elderly, trauma, or ICU setting and also has a high mortality without treatment.
Web References
ACR
Acute Abdominal Pain and Fever
Acute Right Upper Quadrant Pain
Suspected Abdominal Abscess
American Society of Gastroenterology
Family Practice Notebook
For assistance with imaging strategies email radiologist@thecommonvein.net
|
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Cholecystitis
00401.1cs 67Male right upper quadrant pain RUQ pain positive Murphy’s sign gallbladder gallbladder fossa thickened linear lacy thickening gall stones calculi calculous large stone in the infundibulum shadowing multiple small stones cholelithiasis cholecystitis acute cholecystitis acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Cholecystitis
00401.1cs 67Male right upper quadrant pain RUQ pain positive Murphy’s sign gallbladder gallbladder fossa thickened linear lacy thickening gall stones calculi calculous large stone in the infundibulum shadowing multiple small stones cholelithiasis cholecystitis acute cholecystitis acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 00401.1cs 67Male right upper quadrant pain RUQ pain positive Murphy’s sign gallbladder gallbladder fossa thickened linear lacy thickening gall stones calculi calculous large stone in the infundibulum shadowing multiple small stones cholelithiasis cholecystitis acute cholecystitis acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 00401.1cs 67Male right upper quadrant pain RUQ pain positive Murphy’s sign gallbladder gallbladder fossa thickened linear lacy thickening gall stones calculi calculous large stone in the infundibulum shadowing multiple small stones cholelithiasis cholecystitis acute cholecystitis acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Acute Cholecystitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Acute Cholecystitis
)
https://beta.thecommonvein.net/wp-content/uploads/2023/04/00401.1cs.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
Suspect Acute Cholecystitis – Imaging Strategy
Author: Charles Allison, MB ChB
Editor Ashley Davidoff MD
copyright 2006
CLINICAL BACKGROUND –
The “classical ” presentation of acute cholecystitis is characterised by intermittant RUQ pain that lasts for 1-6 hours with intermittant colicky components when the intensity of the pain increases. Precipitaing factors include a recent ingestion of a meal.. The pain may radiate to the right scapula or shoulder. Associated symptoms include nausea and vomiting, fever and chills. While the wcc is usually elevated, a normal wcc does not exclude the diagnosis. The bilirubin and alakaline phosphatase are usually slightly elevated. Murphy’s sign is diagnostic.
WHAT STUDY?
Ultrasound is the investigation of choice in this patient with suspected acute cholecystitis. Findings of a probe tender, distended gallbladder, with fluid in the gallbladder fossa and gallstones are pathognomonic features. Plain abdominal film is not helpful in the diagnosis. In the equivocal case when ultrasound is not characteristic and the clinical suspicion is strong, an imaging alternative is a HIDA scan.
Acute Cholecystitis
00401.1cs 67Male right upper quadrant pain RUQ pain positive Murphy’s sign gallbladder gallbladder fossa thickened linear lacy thickening gall stones calculi calculous large stone in the infundibulum shadowing multiple small stones cholelithiasis cholecystitis acute cholecystitis acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008
WHY?
Ultrasound provides a non-invasive method for establishing evidence of gallstones / gallbladder inflammation as a cause for the symptoms. Acute cholecystitis is an indication for cholecystectomy. If the symptoms are of less than 48 hours duration this can be performed immediately; alternatively, the gallbladder may be removed after the inflammation has settled in 4-6 weeks (interval cholecystectomy).
BACKGROUND TO THE DISEASE:
Gallstone disease affects 10-20% of the population, though the majority are asymptomatic incidental findings. Classically occur in fair, fat, fertile females in their forties ? fifties. Most gallstones are predominantly cholesterol (80%, often solitary if solely cholesterol), but may also be pigmented (formed from bile with less than 25% cholesterol content, usually multiple and irregular) or mixed (faceted appearance, calcium containing). 90% of patients who develop acute cholecystitis have gallstones. Symptoms typically follow impaction of a gallstone in the cystic duct. It is differentiated from biliary colic mainly by the presence of inflammation (fever, leucocytosis, local peritonism); also the pain is not necessarily associated with food.
WHEN?
Ultrasound should be performed at time of presentation, as the patient requires immediate management.
HOW TO ORDER?
The patient should be hospitalized; the investigation may be performed in the emergency room or as an inpatient as an urgent study.
When ordering an ultrasound for acute cholecystitis it is important to reference the symptom or the sign as the clinical indication and not the diagnosis.
ie Patient with “RUQ pain” is acceptable
Patient with R/O cholecystitis is not acceptable.
Patient with “RUQ pain, R/O cholecystitis” is optimal
The examination is called a “limited RUQ ultrasound”
PATIENT PREPARATION
The patient for US should be fasting for 4 hours and the study should take about thirty minutes.
CLINICAL RED FLAGS:
A triad of jaundice, fever and RUQ pain (Charcot?s triad) is indicative of cholangitis, which has a high mortality if not treated promptly with appropriate antimicrobials (to cover enterococcus and enteric organisms, typically 3rd generation cephalosporin and metronidazole). Acalculous cholecystitis, in which no gallstones are visualized, may be seen in the elderly, trauma, or ICU setting and also has a high mortality without treatment.
Web References
ACR
Acute Abdominal Pain and Fever
Acute Right Upper Quadrant Pain
Suspected Abdominal Abscess
American Society of Gastroenterology
Family Practice Notebook
For assistance with imaging strategies email radiologist@thecommonvein.net
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] =>
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Suspect Acute Cholecystitis – Imaging Strategy
Author: Charles Allison, MB ChB
Editor Ashley Davidoff MD
copyright 2006
CLINICAL BACKGROUND –
The “classical ” presentation of acute cholecystitis is characterised by intermittant RUQ pain that lasts for 1-6 hours with intermittant colicky components when the intensity of the pain increases. Precipitaing factors include a recent ingestion of a meal.. The pain may radiate to the right scapula or shoulder. Associated symptoms include nausea and vomiting, fever and chills. While the wcc is usually elevated, a normal wcc does not exclude the diagnosis. The bilirubin and alakaline phosphatase are usually slightly elevated. Murphy’s sign is diagnostic.
WHAT STUDY?
Ultrasound is the investigation of choice in this patient with suspected acute cholecystitis. Findings of a probe tender, distended gallbladder, with fluid in the gallbladder fossa and gallstones are pathognomonic features. Plain abdominal film is not helpful in the diagnosis. In the equivocal case when ultrasound is not characteristic and the clinical suspicion is strong, an imaging alternative is a HIDA scan.
Acute Cholecystitis
00401.1cs 67Male right upper quadrant pain RUQ pain positive Murphy’s sign gallbladder gallbladder fossa thickened linear lacy thickening gall stones calculi calculous large stone in the infundibulum shadowing multiple small stones cholelithiasis cholecystitis acute cholecystitis acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008
WHY?
Ultrasound provides a non-invasive method for establishing evidence of gallstones / gallbladder inflammation as a cause for the symptoms. Acute cholecystitis is an indication for cholecystectomy. If the symptoms are of less than 48 hours duration this can be performed immediately; alternatively, the gallbladder may be removed after the inflammation has settled in 4-6 weeks (interval cholecystectomy).
BACKGROUND TO THE DISEASE:
Gallstone disease affects 10-20% of the population, though the majority are asymptomatic incidental findings. Classically occur in fair, fat, fertile females in their forties ? fifties. Most gallstones are predominantly cholesterol (80%, often solitary if solely cholesterol), but may also be pigmented (formed from bile with less than 25% cholesterol content, usually multiple and irregular) or mixed (faceted appearance, calcium containing). 90% of patients who develop acute cholecystitis have gallstones. Symptoms typically follow impaction of a gallstone in the cystic duct. It is differentiated from biliary colic mainly by the presence of inflammation (fever, leucocytosis, local peritonism); also the pain is not necessarily associated with food.
WHEN?
Ultrasound should be performed at time of presentation, as the patient requires immediate management.
HOW TO ORDER?
The patient should be hospitalized; the investigation may be performed in the emergency room or as an inpatient as an urgent study.
When ordering an ultrasound for acute cholecystitis it is important to reference the symptom or the sign as the clinical indication and not the diagnosis.
ie Patient with “RUQ pain” is acceptable
Patient with R/O cholecystitis is not acceptable.
Patient with “RUQ pain, R/O cholecystitis” is optimal
The examination is called a “limited RUQ ultrasound”
PATIENT PREPARATION
The patient for US should be fasting for 4 hours and the study should take about thirty minutes.
CLINICAL RED FLAGS:
A triad of jaundice, fever and RUQ pain (Charcot?s triad) is indicative of cholangitis, which has a high mortality if not treated promptly with appropriate antimicrobials (to cover enterococcus and enteric organisms, typically 3rd generation cephalosporin and metronidazole). Acalculous cholecystitis, in which no gallstones are visualized, may be seen in the elderly, trauma, or ICU setting and also has a high mortality without treatment.
Web References
ACR
Acute Abdominal Pain and Fever
Acute Right Upper Quadrant Pain
Suspected Abdominal Abscess
American Society of Gastroenterology
Family Practice Notebook
For assistance with imaging strategies email radiologist@thecommonvein.net
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 00401.1cs 67Male right upper quadrant pain RUQ pain positive Murphy’s sign gallbladder gallbladder fossa thickened linear lacy thickening gall stones calculi calculous large stone in the infundibulum shadowing multiple small stones cholelithiasis cholecystitis acute cholecystitis acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 00401.1cs 67Male right upper quadrant pain RUQ pain positive Murphy’s sign gallbladder gallbladder fossa thickened linear lacy thickening gall stones calculi calculous large stone in the infundibulum shadowing multiple small stones cholelithiasis cholecystitis acute cholecystitis acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Acute Cholecystitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Acute Cholecystitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 42
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Suspect Acute Cholecystitis – Imaging Strategy
Author: Charles Allison, MB ChB
Editor Ashley Davidoff MD
copyright 2006
CLINICAL BACKGROUND –
The “classical ” presentation of acute cholecystitis is characterised by intermittant RUQ pain that lasts for 1-6 hours with intermittant colicky components when the intensity of the pain increases. Precipitaing factors include a recent ingestion of a meal.. The pain may radiate to the right scapula or shoulder. Associated symptoms include nausea and vomiting, fever and chills. While the wcc is usually elevated, a normal wcc does not exclude the diagnosis. The bilirubin and alakaline phosphatase are usually slightly elevated. Murphy’s sign is diagnostic.
WHAT STUDY?
Ultrasound is the investigation of choice in this patient with suspected acute cholecystitis. Findings of a probe tender, distended gallbladder, with fluid in the gallbladder fossa and gallstones are pathognomonic features. Plain abdominal film is not helpful in the diagnosis. In the equivocal case when ultrasound is not characteristic and the clinical suspicion is strong, an imaging alternative is a HIDA scan.
Acute Cholecystitis
00401.1cs 67Male right upper quadrant pain RUQ pain positive Murphy’s sign gallbladder gallbladder fossa thickened linear lacy thickening gall stones calculi calculous large stone in the infundibulum shadowing multiple small stones cholelithiasis cholecystitis acute cholecystitis acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008
WHY?
Ultrasound provides a non-invasive method for establishing evidence of gallstones / gallbladder inflammation as a cause for the symptoms. Acute cholecystitis is an indication for cholecystectomy. If the symptoms are of less than 48 hours duration this can be performed immediately; alternatively, the gallbladder may be removed after the inflammation has settled in 4-6 weeks (interval cholecystectomy).
BACKGROUND TO THE DISEASE:
Gallstone disease affects 10-20% of the population, though the majority are asymptomatic incidental findings. Classically occur in fair, fat, fertile females in their forties ? fifties. Most gallstones are predominantly cholesterol (80%, often solitary if solely cholesterol), but may also be pigmented (formed from bile with less than 25% cholesterol content, usually multiple and irregular) or mixed (faceted appearance, calcium containing). 90% of patients who develop acute cholecystitis have gallstones. Symptoms typically follow impaction of a gallstone in the cystic duct. It is differentiated from biliary colic mainly by the presence of inflammation (fever, leucocytosis, local peritonism); also the pain is not necessarily associated with food.
WHEN?
Ultrasound should be performed at time of presentation, as the patient requires immediate management.
HOW TO ORDER?
The patient should be hospitalized; the investigation may be performed in the emergency room or as an inpatient as an urgent study.
When ordering an ultrasound for acute cholecystitis it is important to reference the symptom or the sign as the clinical indication and not the diagnosis.
ie Patient with “RUQ pain” is acceptable
Patient with R/O cholecystitis is not acceptable.
Patient with “RUQ pain, R/O cholecystitis” is optimal
The examination is called a “limited RUQ ultrasound”
PATIENT PREPARATION
The patient for US should be fasting for 4 hours and the study should take about thirty minutes.
CLINICAL RED FLAGS:
A triad of jaundice, fever and RUQ pain (Charcot?s triad) is indicative of cholangitis, which has a high mortality if not treated promptly with appropriate antimicrobials (to cover enterococcus and enteric organisms, typically 3rd generation cephalosporin and metronidazole). Acalculous cholecystitis, in which no gallstones are visualized, may be seen in the elderly, trauma, or ICU setting and also has a high mortality without treatment.
Web References
ACR
Acute Abdominal Pain and Fever
Acute Right Upper Quadrant Pain
Suspected Abdominal Abscess
American Society of Gastroenterology
Family Practice Notebook
For assistance with imaging strategies email radiologist@thecommonvein.net
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Suspect Acute Cholecystitis – Imaging Strategy
Author: Charles Allison, MB ChB
Editor Ashley Davidoff MD
copyright 2006
CLINICAL BACKGROUND –
The “classical ” presentation of acute cholecystitis is characterised by intermittant RUQ pain that lasts for 1-6 hours with intermittant colicky components when the intensity of the pain increases. Precipitaing factors include a recent ingestion of a meal.. The pain may radiate to the right scapula or shoulder. Associated symptoms include nausea and vomiting, fever and chills. While the wcc is usually elevated, a normal wcc does not exclude the diagnosis. The bilirubin and alakaline phosphatase are usually slightly elevated. Murphy’s sign is diagnostic.
WHAT STUDY?
Ultrasound is the investigation of choice in this patient with suspected acute cholecystitis. Findings of a probe tender, distended gallbladder, with fluid in the gallbladder fossa and gallstones are pathognomonic features. Plain abdominal film is not helpful in the diagnosis. In the equivocal case when ultrasound is not characteristic and the clinical suspicion is strong, an imaging alternative is a HIDA scan.
Acute Cholecystitis
00401.1cs 67Male right upper quadrant pain RUQ pain positive Murphy’s sign gallbladder gallbladder fossa thickened linear lacy thickening gall stones calculi calculous large stone in the infundibulum shadowing multiple small stones cholelithiasis cholecystitis acute cholecystitis acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008
WHY?
Ultrasound provides a non-invasive method for establishing evidence of gallstones / gallbladder inflammation as a cause for the symptoms. Acute cholecystitis is an indication for cholecystectomy. If the symptoms are of less than 48 hours duration this can be performed immediately; alternatively, the gallbladder may be removed after the inflammation has settled in 4-6 weeks (interval cholecystectomy).
BACKGROUND TO THE DISEASE:
Gallstone disease affects 10-20% of the population, though the majority are asymptomatic incidental findings. Classically occur in fair, fat, fertile females in their forties ? fifties. Most gallstones are predominantly cholesterol (80%, often solitary if solely cholesterol), but may also be pigmented (formed from bile with less than 25% cholesterol content, usually multiple and irregular) or mixed (faceted appearance, calcium containing). 90% of patients who develop acute cholecystitis have gallstones. Symptoms typically follow impaction of a gallstone in the cystic duct. It is differentiated from biliary colic mainly by the presence of inflammation (fever, leucocytosis, local peritonism); also the pain is not necessarily associated with food.
WHEN?
Ultrasound should be performed at time of presentation, as the patient requires immediate management.
HOW TO ORDER?
The patient should be hospitalized; the investigation may be performed in the emergency room or as an inpatient as an urgent study.
When ordering an ultrasound for acute cholecystitis it is important to reference the symptom or the sign as the clinical indication and not the diagnosis.
ie Patient with “RUQ pain” is acceptable
Patient with R/O cholecystitis is not acceptable.
Patient with “RUQ pain, R/O cholecystitis” is optimal
The examination is called a “limited RUQ ultrasound”
PATIENT PREPARATION
The patient for US should be fasting for 4 hours and the study should take about thirty minutes.
CLINICAL RED FLAGS:
A triad of jaundice, fever and RUQ pain (Charcot?s triad) is indicative of cholangitis, which has a high mortality if not treated promptly with appropriate antimicrobials (to cover enterococcus and enteric organisms, typically 3rd generation cephalosporin and metronidazole). Acalculous cholecystitis, in which no gallstones are visualized, may be seen in the elderly, trauma, or ICU setting and also has a high mortality without treatment.
Web References
ACR
Acute Abdominal Pain and Fever
Acute Right Upper Quadrant Pain
Suspected Abdominal Abscess
American Society of Gastroenterology
Family Practice Notebook
For assistance with imaging strategies email radiologist@thecommonvein.net
)
