
Pathogenesis – From renal Parenchymal Infection to the Submucosa to the Infundibulum to the Renal Pelvis and Down the Ureter
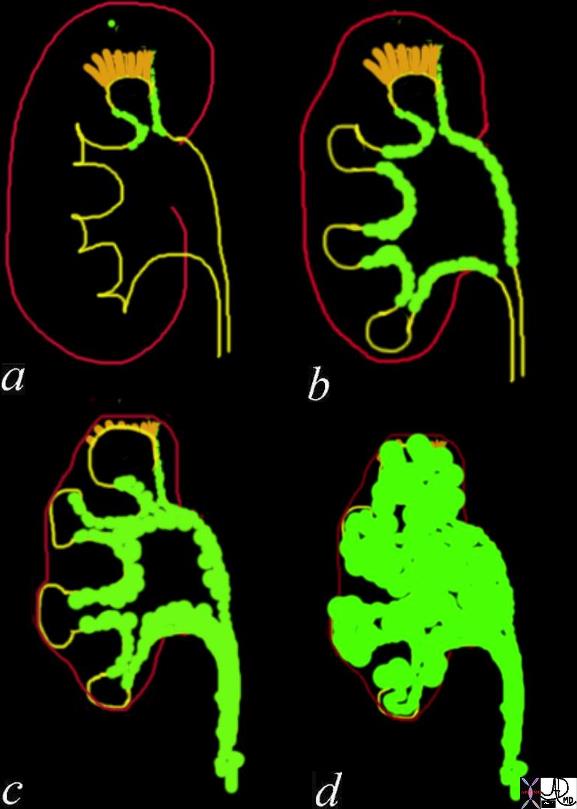
TB of the Kidney starts with a parenchymal infection that spreads to the lymphatics with a predisposition for the infundibulum of the calyx resulting in sclerosis of the infundibulum and infundibular stenosis (a). This may only affect 1 infundibulum in the early stages 9a)but eventually spreads throughout the submucosal lymphatics and causing contraction of the pelvis (b) and UPJ obstruction (c) Caseous necrosis ensues and the renal pelvis gets filled with caseous material (?putty kidney?) (d) with extensive calcification. Back pressure atrophy causes the kidney to shrink resulting in a non-functioning kidney (?autonephrectomy?). The infection continues to descend in the ureters and may eventually involve the bladder
Davidoff Art Davidoff Drawing Ashley Davidoff MD TheCommonVein.net 22419c01

58-year-old male with known history of tuberculosis. The CXR is normal with no active nor evidence of chronic granulomatous disease
The X ray of the lumbar spine shows a compression injury of the L1 vertebral body with compression of the superior endplate
CT of the kidney shows replacement of the upper pole of the right kidney with focal hydronephrosis caused by infundibular stenosis and atrophy of the remainder of the right kidney.
There is enlargement of the bilateral adrenal glands, with multiple nodular structures encompassing the left adrenal gland, which may also represent infectious process.
Examination of the lumbar spine on the CT scan shows findings consistent with TB osteomyelitis with destruction of T12 and L1 vertebral bodies with prevertebral and epidural collections extending into the spinal canal.
The left psoas muscle shows peripherally enhancing communicating retroperitoneal and epidural fluid collection as well as multiple peripherally enhancing left psoas fluid collections.
Aspiration of the psoas muscle was performed
The MRI confirms the presence of an osteomyelitis discitis associated with an epidural abscess with multiple collections in the left psoas muscle
Contributed by Christina LeBedis MD

58-year-old male with known history of tuberculosis. The CXR is normal with no active nor evidence of chronic granulomatous disease
The X ray of the lumbar spine shows a compression injury of the L1 vertebral body with compression of the superior endplate
CT of the kidney shows replacement of the upper pole of the right kidney with focal hydronephrosis caused by infundibular stenosis and atrophy of the remainder of the right kidney.
There is enlargement of the bilateral adrenal glands, with multiple nodular structures encompassing the left adrenal gland, which may also represent infectious process.
Examination of the lumbar spine on the CT scan shows findings consistent with TB osteomyelitis with destruction of T12 and L1 vertebral bodies with prevertebral and epidural collections extending into the spinal canal.
The left psoas muscle shows peripherally enhancing communicating retroperitoneal and epidural fluid collection as well as multiple peripherally enhancing left psoas fluid collections.
Aspiration of the psoas muscle was performed
The MRI confirms the presence of an osteomyelitis discitis associated with an epidural abscess with multiple collections in the left psoas muscle
Contributed by Christina LeBedis MD