Gregory Waryasz MD, Ashley Davidoff MD
The Common Vein Copyright 2011
Definition
Fractures of the tibia are usually caused by by direct trauma, twisting, avulsion, or rotational forces and are often characterized by associated injuries with the fibula because of the interosseus membrane which forces the two bones to move as a unit.
Tibial fractures can be either open or closed injuries. The location of the fracture on the tibia varies.
Tibial plateau fractures can be open or closed injuries. The Schatzker Classification System is used to describe the six types of patterns. A type I is a lateral plateau, split fracture. A type II is a lateral plateau, split depression fracture. Type III fractures are depression fractures of the lateral plateau. The type IV fracture involves the medial plateau. A type V fracture is a bicondylar fracture. The type IV fracture is a plateau fracture with metaphyseal separation from the diaphysis. Typically types I to III are low energy injuries, while IV to VI are high energy injuries.
Tibial shaft fractures often occur in conjunction with fractures of the fibular shaft. These fractures can be open or closed. Fractures are described based on the pattern, location, and level of comminution. Spiral, transverse, and oblique fractures are simple. Wedge fractures include spiral wedge, bending wedge, and fragmented wedge. Complex fractures include spiral, segmented, and irregular.
Ankle fractures can contain a tibial and/or fibular component. The Lauge-Hansen Classification system describes the injuries that result from four different mechanisms; supination-adduction (SA), supination-external rotation (SER), pronation-abduction (PA), and pronation-external rotation (PER).
Tibial plafond fractures are classified by the Rueid and Allgower Classification system. Type 1 injuries are nondisplaced. Type 2 are displaced with minimal impaction or comminution. Type 3 are displaced with significant intraarticular involvement and metaphyseal impaction.
The fracture may be complicated in the acute phase by neurovascular injury, or in the subacute or chronic phases by nonunion, malunion, infection, osteonecrosis, and osteoarthritis. Specific complications pertaining to fractures of the tibia include loss of knee or ankle motion, compartment syndrome, peroneal nerve injury, vascular injury, reflex sympathetic dystrophy, fat embolism, and claw toe deformity.
The diagnosis of this injury is usually made by a combination of physical examination and x-ray imaging.
Imaging includes the use of plain x-rays, and if indicated CT-scan, or MRI.
Treatment depends on the specific type of fracture and how acutely sick the patient is.
Tibial plateau fractures can be treated nonoperatively if there is no displacement or if there is minimal displacement. These patients are treated with protected weight bearing, early physical therapy, and a hinged-brace.
Tibial plateau fractures with articular depression, compartment syndrome, vascular injury, or open fractures are treated surgically. The surgery usually consists of placement of screws and a lateral plate.
Tibial shaft fractures can be treated nonoperatively if there is minimal displacement. Tibial shaft fractures with displacement or comminution can be treated with intramedullary nailing, flexible nails, external fixation devices, or plates and screws. Intramedullary nailing is typically performed.
Ankle fractures are typically given an attempt at closed reduction to try to regain anatomic alignment. Often a reduction can reduce the need for surgery. Unstable fractures, open fractures, and failure to achieve anatomic alignment by closed reduction requires open reduction and internal fixation (ORIF) surgery.
Tibial plafond fractures are treated nonoperatively for nondisplaced injuries. Displaced fractures are treated with ORIF surgery or external fixation.
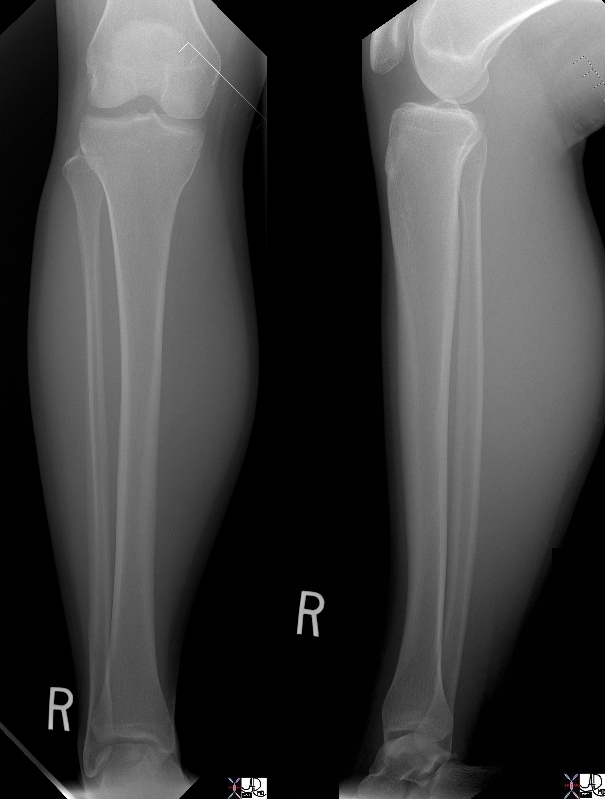
Normal Tibia and Fibula
|
|
Courtesy Ashley Davidoff MD 46711c01
|

The Distal Tibia |
|
The 3D reconstructed CT scan of the forefoot exemplifies the normal anatomy of the distal tibia, fibula, tibio-talar joint, talo navicular joint, and navicular cuboid. The cuneiforms are also well visualized. This patient does have an avulsion fracture off the navicular but it is not obvious on this view.
Courtesy Ashley Davidoff MD 72585
|
86255c.8s
|
|
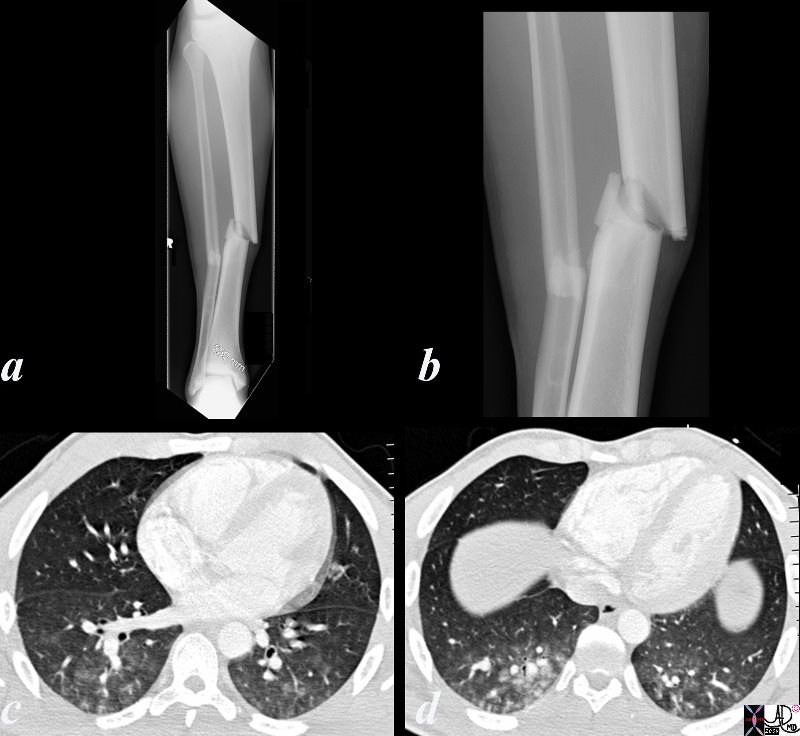
21 year old college student and football player who sustained a compound fracture of his right tibia and fibula. While awaiting surgeryhe became short of breasth, tachpneic and tachycardicand his saturations dropped to 70’s from 90’son room air. he hasd a fever to 103 heart rate of 100 respiratory rate of 30 and a systolic pressure of 140.. He required intubation for 5 days
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 86255c.8s
|

Avulsion fracture of the Disatal Anterior Tibia and Incomplete Hairline Fracture of the Distal Fibula
|
|
The X-ray of the ankle in a 15 year old male in the anteroposterior projection (A-P) shows a simple incomplete complex hairline fracture of the distal fibula (b, e green overlay) magnified in c and f, and an avulsion fracture of the anterior portion of the distal tibia (green arrow h). The close relationship of the two bones in the ankle region and the presence of an interosseus membrane that binds the two bones into a single unit, makes combination fractures common. .
Courtesy Ashley Davidoff Copyright 2011 99940c03.8s
|
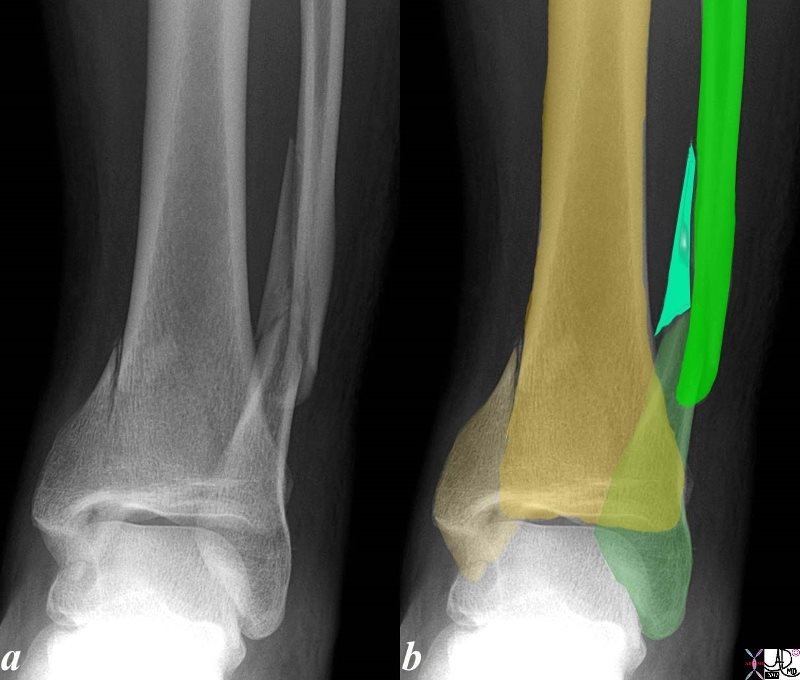
Fracture of the Tibia and Fibula
|
|
The X-ray of the right ankle in the anteroposterior projection (A-P) shows a simple appearing vertical fracture of the tibia with near anatomical alignment and a comminuted spiral fracture of the distal shaft of the fibula with a butterfly fragment (overlaid in turquoise in b) The close relationship of the two bones in the ankle region an the presence of an interosseus membrane that binds the two bones into a single unit makes combination fractures common. . COD
Courtesy Ashley Davidoff Copyright 2011 101075b04L.8
|
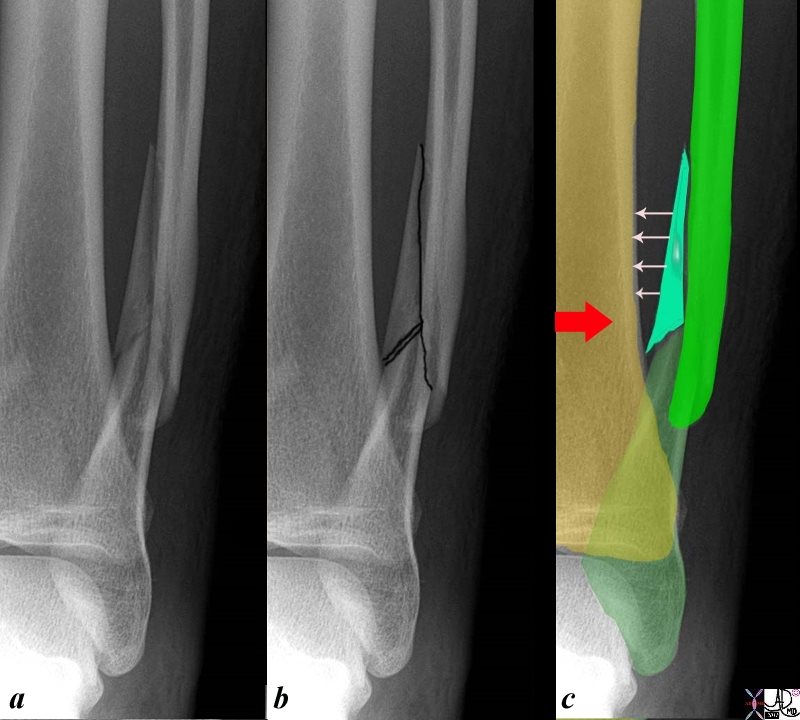
Role of the Interosseus Membrane Causes the Tibia and Fibula to Move Together
In the Case of Trauma this often Results in a Fracture of Both
|
|
This X-ray on the antero-posterior (A-P) projection shows a comminuted spiral fracture of the distal shaft of the fibula in a 26 year old male. Image b shows the fracture as best depicted in a single projection with black overlay, while image c reveals three fragments with the lightest turquoise green overlaying the triangular or butterfly fragment. The mechanism of this injury is usually a twisting or torsional injury. The interosseus membrane also acts as a resisting force and may account for the butterfly fragment
Courtesy Ashley Davidoff Copyright 2011 101075b06L.81c
|
Davis MF, Davis PF, Ross DS. Expert Guide to Sports Medicine. ACP Series, 2005.
Elstrom J, Virkus W, Pankovich (eds), Handbook of Fractures (3rd edition), McGraw Hill, New York, NY, 2006.
Koval K, Zuckerman J (eds), Handbook of Fractures (3rd edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Lieberman J (ed), AAOS Comprehensive Orthopaedic Review, American Academy of Orthopaedic Surgeons, 2008.
Moore K, Dalley A (eds), Clinically Oriented Anatomy (5th edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Wheeless?s Textbook of Orthopaedics: Tibia Fracture Menu (http://www.wheelessonline.com/ortho/menu_for_the_tibia_tibia_frx)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Role of the Interosseus Membrane Causes the Tibia and Fibula to Move Together
In the Case of Trauma this often Results in a Fracture of Both
This X-ray on the antero-posterior (A-P) projection shows a comminuted spiral fracture of the distal shaft of the fibula in a 26 year old male. Image b shows the fracture as best depicted in a single projection with black overlay, while image c reveals three fragments with the lightest turquoise green overlaying the triangular or butterfly fragment. The mechanism of this injury is usually a twisting or torsional injury. The interosseus membrane also acts as a resisting force and may account for the butterfly fragment
Courtesy Ashley Davidoff Copyright 2011 101075b06L.81c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Role of the Interosseus Membrane Causes the Tibia and Fibula to Move Together
In the Case of Trauma this often Results in a Fracture of Both
This X-ray on the antero-posterior (A-P) projection shows a comminuted spiral fracture of the distal shaft of the fibula in a 26 year old male. Image b shows the fracture as best depicted in a single projection with black overlay, while image c reveals three fragments with the lightest turquoise green overlaying the triangular or butterfly fragment. The mechanism of this injury is usually a twisting or torsional injury. The interosseus membrane also acts as a resisting force and may account for the butterfly fragment
Courtesy Ashley Davidoff Copyright 2011 101075b06L.81c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This X-ray on the antero-posterior (A-P) projection shows a comminuted spiral fracture of the distal shaft of the fibula in a 26 year old male. Image b shows the fracture as best depicted in a single projection with black overlay, while image c reveals three fragments with the lightest turquoise green overlaying the triangular or butterfly fragment. The mechanism of this injury is usually a twisting or torsional injury. The interosseus membrane also acts as a resisting force and may account for the butterfly fragment
Courtesy Ashley Davidoff Copyright 2011 101075b06L.81c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This X-ray on the antero-posterior (A-P) projection shows a comminuted spiral fracture of the distal shaft of the fibula in a 26 year old male. Image b shows the fracture as best depicted in a single projection with black overlay, while image c reveals three fragments with the lightest turquoise green overlaying the triangular or butterfly fragment. The mechanism of this injury is usually a twisting or torsional injury. The interosseus membrane also acts as a resisting force and may account for the butterfly fragment
Courtesy Ashley Davidoff Copyright 2011 101075b06L.81c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Role of the Interosseus Membrane Causes the Tibia and Fibula to Move Together
In the Case of Trauma this often Results in a Fracture of Both
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Role of the Interosseus Membrane Causes the Tibia and Fibula to Move Together
In the Case of Trauma this often Results in a Fracture of Both
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Fracture of the Tibia and Fibula
The X-ray of the right ankle in the anteroposterior projection (A-P) shows a simple appearing vertical fracture of the tibia with near anatomical alignment and a comminuted spiral fracture of the distal shaft of the fibula with a butterfly fragment (overlaid in turquoise in b) The close relationship of the two bones in the ankle region an the presence of an interosseus membrane that binds the two bones into a single unit makes combination fractures common. . COD
Courtesy Ashley Davidoff Copyright 2011 101075b04L.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Fracture of the Tibia and Fibula
The X-ray of the right ankle in the anteroposterior projection (A-P) shows a simple appearing vertical fracture of the tibia with near anatomical alignment and a comminuted spiral fracture of the distal shaft of the fibula with a butterfly fragment (overlaid in turquoise in b) The close relationship of the two bones in the ankle region an the presence of an interosseus membrane that binds the two bones into a single unit makes combination fractures common. . COD
Courtesy Ashley Davidoff Copyright 2011 101075b04L.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The X-ray of the right ankle in the anteroposterior projection (A-P) shows a simple appearing vertical fracture of the tibia with near anatomical alignment and a comminuted spiral fracture of the distal shaft of the fibula with a butterfly fragment (overlaid in turquoise in b) The close relationship of the two bones in the ankle region an the presence of an interosseus membrane that binds the two bones into a single unit makes combination fractures common. . COD
Courtesy Ashley Davidoff Copyright 2011 101075b04L.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The X-ray of the right ankle in the anteroposterior projection (A-P) shows a simple appearing vertical fracture of the tibia with near anatomical alignment and a comminuted spiral fracture of the distal shaft of the fibula with a butterfly fragment (overlaid in turquoise in b) The close relationship of the two bones in the ankle region an the presence of an interosseus membrane that binds the two bones into a single unit makes combination fractures common. . COD
Courtesy Ashley Davidoff Copyright 2011 101075b04L.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Fracture of the Tibia and Fibula
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Fracture of the Tibia and Fibula
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Avulsion fracture of the Disatal Anterior Tibia and Incomplete Hairline Fracture of the Distal Fibula
The X-ray of the ankle in a 15 year old male in the anteroposterior projection (A-P) shows a simple incomplete complex hairline fracture of the distal fibula (b, e green overlay) magnified in c and f, and an avulsion fracture of the anterior portion of the distal tibia (green arrow h). The close relationship of the two bones in the ankle region and the presence of an interosseus membrane that binds the two bones into a single unit, makes combination fractures common. .
Courtesy Ashley Davidoff Copyright 2011 99940c03.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Avulsion fracture of the Disatal Anterior Tibia and Incomplete Hairline Fracture of the Distal Fibula
The X-ray of the ankle in a 15 year old male in the anteroposterior projection (A-P) shows a simple incomplete complex hairline fracture of the distal fibula (b, e green overlay) magnified in c and f, and an avulsion fracture of the anterior portion of the distal tibia (green arrow h). The close relationship of the two bones in the ankle region and the presence of an interosseus membrane that binds the two bones into a single unit, makes combination fractures common. .
Courtesy Ashley Davidoff Copyright 2011 99940c03.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The X-ray of the ankle in a 15 year old male in the anteroposterior projection (A-P) shows a simple incomplete complex hairline fracture of the distal fibula (b, e green overlay) magnified in c and f, and an avulsion fracture of the anterior portion of the distal tibia (green arrow h). The close relationship of the two bones in the ankle region and the presence of an interosseus membrane that binds the two bones into a single unit, makes combination fractures common. .
Courtesy Ashley Davidoff Copyright 2011 99940c03.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The X-ray of the ankle in a 15 year old male in the anteroposterior projection (A-P) shows a simple incomplete complex hairline fracture of the distal fibula (b, e green overlay) magnified in c and f, and an avulsion fracture of the anterior portion of the distal tibia (green arrow h). The close relationship of the two bones in the ankle region and the presence of an interosseus membrane that binds the two bones into a single unit, makes combination fractures common. .
Courtesy Ashley Davidoff Copyright 2011 99940c03.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Avulsion fracture of the Disatal Anterior Tibia and Incomplete Hairline Fracture of the Distal Fibula
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Avulsion fracture of the Disatal Anterior Tibia and Incomplete Hairline Fracture of the Distal Fibula
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
86255c.8s
21 year old college student and football player who sustained a compound fracture of his right tibia and fibula. While awaiting surgeryhe became short of breasth, tachpneic and tachycardicand his saturations dropped to 70’s from 90’son room air. he hasd a fever to 103 heart rate of 100 respiratory rate of 30 and a systolic pressure of 140.. He required intubation for 5 days
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 86255c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
86255c.8s
21 year old college student and football player who sustained a compound fracture of his right tibia and fibula. While awaiting surgeryhe became short of breasth, tachpneic and tachycardicand his saturations dropped to 70’s from 90’son room air. he hasd a fever to 103 heart rate of 100 respiratory rate of 30 and a systolic pressure of 140.. He required intubation for 5 days
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 86255c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
21 year old college student and football player who sustained a compound fracture of his right tibia and fibula. While awaiting surgeryhe became short of breasth, tachpneic and tachycardicand his saturations dropped to 70’s from 90’son room air. he hasd a fever to 103 heart rate of 100 respiratory rate of 30 and a systolic pressure of 140.. He required intubation for 5 days
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 86255c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
21 year old college student and football player who sustained a compound fracture of his right tibia and fibula. While awaiting surgeryhe became short of breasth, tachpneic and tachycardicand his saturations dropped to 70’s from 90’son room air. he hasd a fever to 103 heart rate of 100 respiratory rate of 30 and a systolic pressure of 140.. He required intubation for 5 days
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 86255c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
86255c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
86255c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
The Distal Tibia
The 3D reconstructed CT scan of the forefoot exemplifies the normal anatomy of the distal tibia, fibula, tibio-talar joint, talo navicular joint, and navicular cuboid. The cuneiforms are also well visualized. This patient does have an avulsion fracture off the navicular but it is not obvious on this view.
Courtesy Ashley Davidoff MD 72585
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
The Distal Tibia
The 3D reconstructed CT scan of the forefoot exemplifies the normal anatomy of the distal tibia, fibula, tibio-talar joint, talo navicular joint, and navicular cuboid. The cuneiforms are also well visualized. This patient does have an avulsion fracture off the navicular but it is not obvious on this view.
Courtesy Ashley Davidoff MD 72585
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The 3D reconstructed CT scan of the forefoot exemplifies the normal anatomy of the distal tibia, fibula, tibio-talar joint, talo navicular joint, and navicular cuboid. The cuneiforms are also well visualized. This patient does have an avulsion fracture off the navicular but it is not obvious on this view.
Courtesy Ashley Davidoff MD 72585
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The 3D reconstructed CT scan of the forefoot exemplifies the normal anatomy of the distal tibia, fibula, tibio-talar joint, talo navicular joint, and navicular cuboid. The cuneiforms are also well visualized. This patient does have an avulsion fracture off the navicular but it is not obvious on this view.
Courtesy Ashley Davidoff MD 72585
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The Distal Tibia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The Distal Tibia
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal Tibia and Fibula
Courtesy Ashley Davidoff MD 46711c01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal Tibia and Fibula
Courtesy Ashley Davidoff MD 46711c01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Courtesy Ashley Davidoff MD 46711c01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Courtesy Ashley Davidoff MD 46711c01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal Tibia and Fibula
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal Tibia and Fibula
)
