
The Common Vein Copyright 2011
Definition
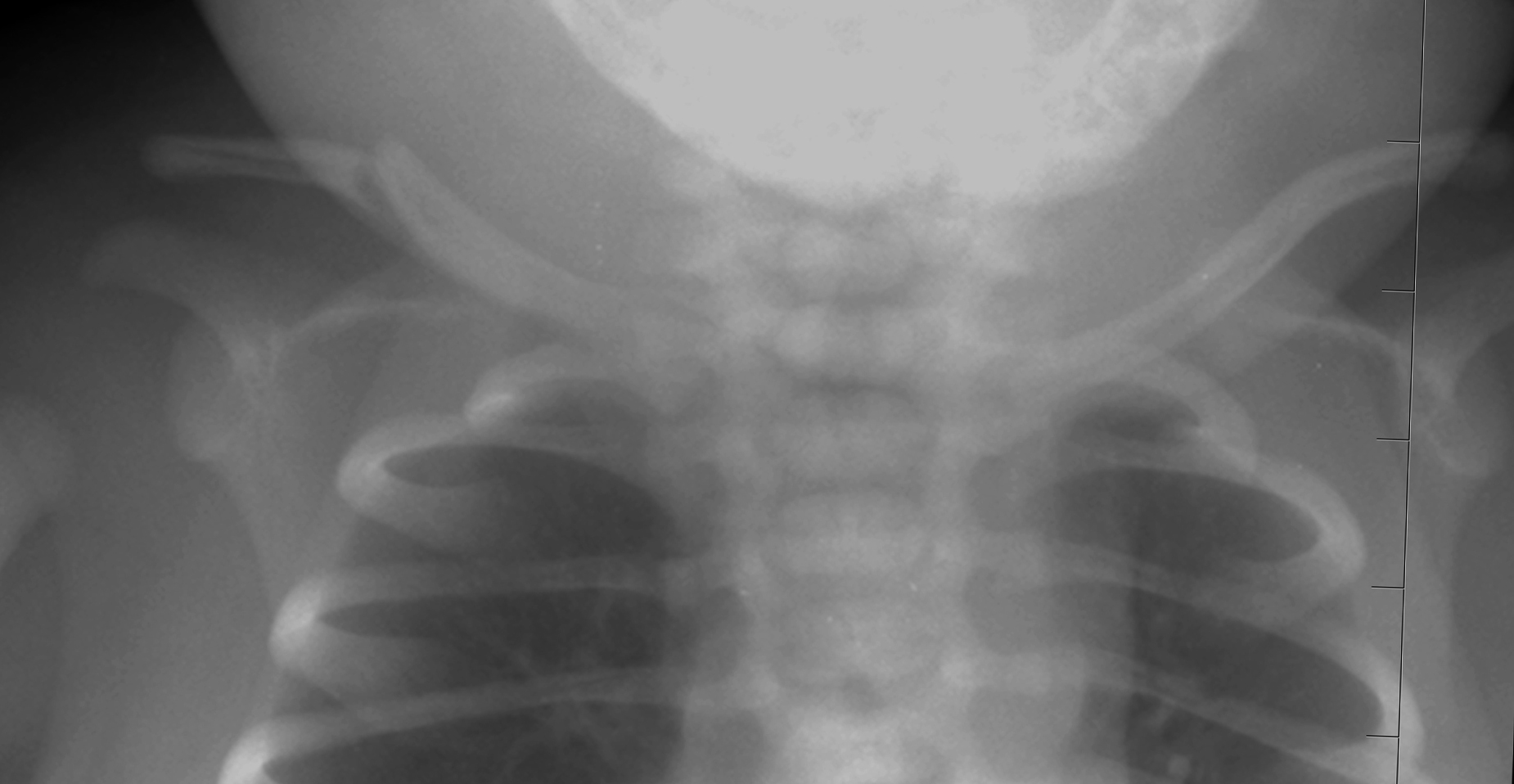
Fractures of the clavicle are usually caused by a fall or a crush injury but other causes include direct blow or gunshot wound and birth injury. Muscle contraction is a rare cause of clavicular fracture. The clavicle can be fractured in infants during the birth process. It results in damage to the bone cortex and disruption of other soft tissue structures. Fractures characteristically occur in the middle third of the bone with approximately 80% of all clavicle fractures occurring in this position.
The Allman classification system divides the fractures by location, displacement, and level of comminution. A Group 1 fracture is of the middle third of the clavicle with the ends still secured by the ligaments.
A Group 2 fracture is of the distal third. There are three major types of Group 2 fractures. Type I is minimal displacement of the fragments. Type II is a displacement due to injury to the coracoclavicular ligaments. A Type IIA has the conoid and trapezoid ligaments still attached to the distal fragment. A Type IIB has the trapezoid still attached, but the conoid is torn. A Type III is an intra-articular fracture with no ligament injury, it appears clinically like a 1st degree AC joint separation.
Group 3 fractures are of the proximal third of the clavicle. Type I is minimal displacement. Type II is displaced. Type III is intra-articular. Type IV has epiphyseal separation. Type V is comminuted.
The fracture may be complicated in the acute phase by neurovascular injury, or in the subacute or chronic phases by nonunion, malunion, infection, osteonecrosis, or osteoarthritis.
The diagnosis of this injury is usually made by a combination of physical examination and x-ray imaging.
Imaging includes the use of plain x-rays, and if indicated CT-scan, or MRI.
Most clavicle fractures can be treated nonoperatively with a sling and potentially a swathe for comfort. Immobilization should occur for 4 to 6 weeks, but there should be exercises for the elbow, wrist, and hand.
The accepted indications for clavicle fracture repair are open fractures, neurovascular compromise/injury, and skin tenting/risk for open fracture. Repair can be performed with a plate and screw fixation or intramedullary pin.
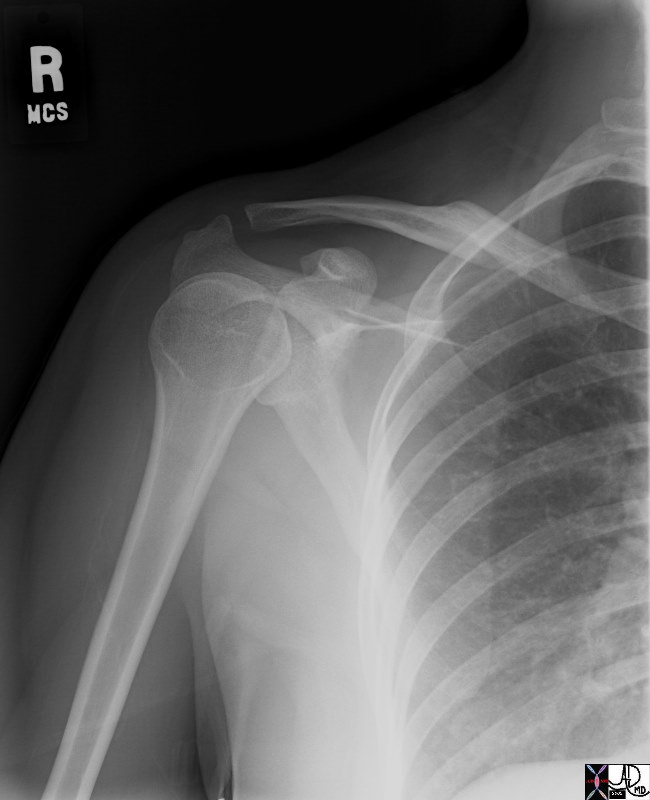
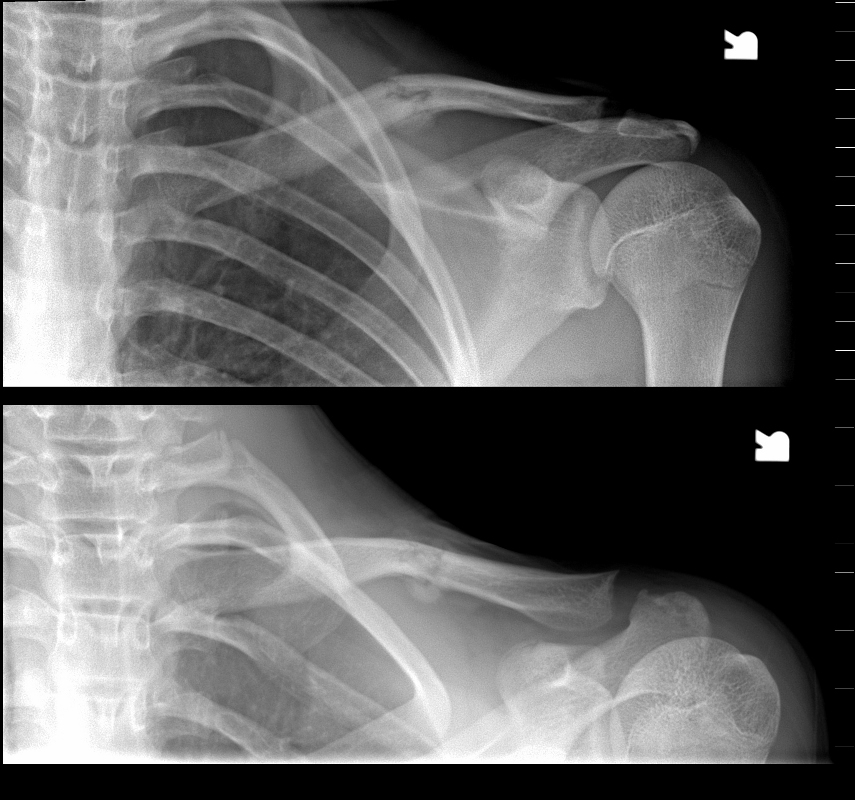
This A-P examination of the right shoulder of a young adult shows a healed fracture of the middle of the right clavicle with reasonable anatomical alignment. The patient can probably feel a fullness overlying the area.
Courtesy Ashley Davidoff 39177.800
Ashley Davidoff MD
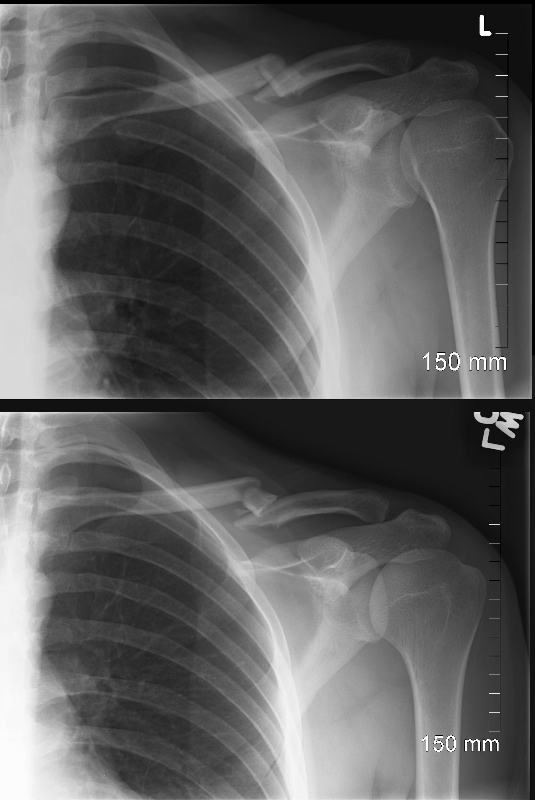
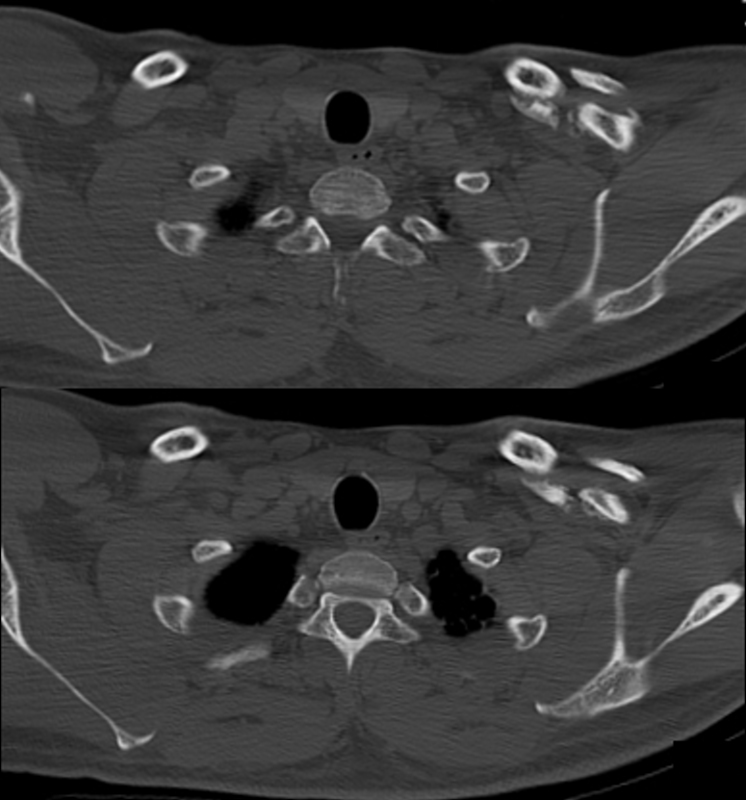
Acute Fracture
Ashley Davidoff MD

Ashley Davidoff MD
Ashley Davidoff MD
Healing Clavicular Fracture
Ashley Davidoff MD
References
Davis MF, Davis PF, Ross DS. Expert Guide to Sports Medicine. ACP Series, 2005.
Elstrom J, Virkus W, Pankovich (eds), Handbook of Fractures (3rd edition), McGraw Hill, New York, NY, 2006.
Koval K, Zuckerman J (eds), Handbook of Fractures (3rd edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Lieberman J (ed), AAOS Comprehensive Orthopaedic Review, American Academy of Orthopaedic Surgeons, 2008.
Moore K, Dalley A (eds), Clinically Oriented Anatomy (5th edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Wheeless?s Textbook of Orthopaedics: Clavicle Fractures (http://www.wheelessonline.com/ortho/clavicle_fractures)