Gregory Waryasz MD, Ashley Davidoff MD
The Common Vein Copyright 2011
Definition
Fractures of the are usually caused by high energy blunt trauma.
Indirect injury occurs when there is axial loading of an outstretched arm to cause glenoid, scapular neck, and intraarticular fractures. Dislocation of a shoulder can cause a glenoid fracture. Avulsion fractures can occur due to muscles and ligaments.
Fractures of the scapula can be anatomically classified as scapular body, glenoid, scapular neck, acromion, scapular spine, and coracoids.
Intraarticular glenoid fractures are classified by the Ideberg Classification. Type I is an avulsion fracture of the anterior margin. Type IIa is a transverse fracture through the glenoid fossa with an exit inferiorly. Type IIb is an oblique fracture through the glenoid fossa with an exit anteriorly. Type III is an oblique fracture through the glenoid with a superior exit and is associated with an AC joint injury. Type IV fractures are a transverse fracture that exits though the medial border of the scapula. Type V is a type II and a type IV combination pattern. Type VI is a comminuted fracture.
Acromial fractures are subdivided into three types. Type I is non-displaced or minimally displaced. Type II is displaced without compromising the subacromial space. Type III is a displaced fracture with subacromial space being narrowed.
There are two types of coracoid fractures; type I and II. Type I is a fracture proximal to the coracoclavicular ligament. Type II is a fracture distal to the coracoclavicular ligament.
The fracture may be complicated in the acute phase by neurovascular injury, or in the subacute or chronic phases by nonunion, malunion, infection, osteonecrosis, or osteoarthritis. More specific to scapular fractures is the potential to injure the suprascapular nerve. There are associated injuries in 80-90% of patients including pneumothorax, pulmonary contusion, clavicle fractures, shoulder dislocation, brachial plexus injury, axillary artery injury, and rib fractures.
The diagnosis of this injury is usually made by a combination of physical examination and x-ray imaging.
Imaging includes the use of plain x-rays, and if indicated CT-scan, or MRI.
Most scapula fractures are treated non-operatively if there is no or minimal displacement. Severely comminuted glenoid fractures are often treated best non-operatively. Non-operative management includes the use of a sling for comfort.
Surgical indications include displaced fractures of the glenoid, acromion, and scapular neck. Scapular body fractures can be treated operatively if there is neurovascular compromise. Acromial fractures must have os acromiale ruled out and any possible rotator cuff injury prior to surgery. Acromial fractures can be tension banded.
CT reconstruction of a Normal Scapula
|
| Courtesy Ashley Davidoff MD 49640 |

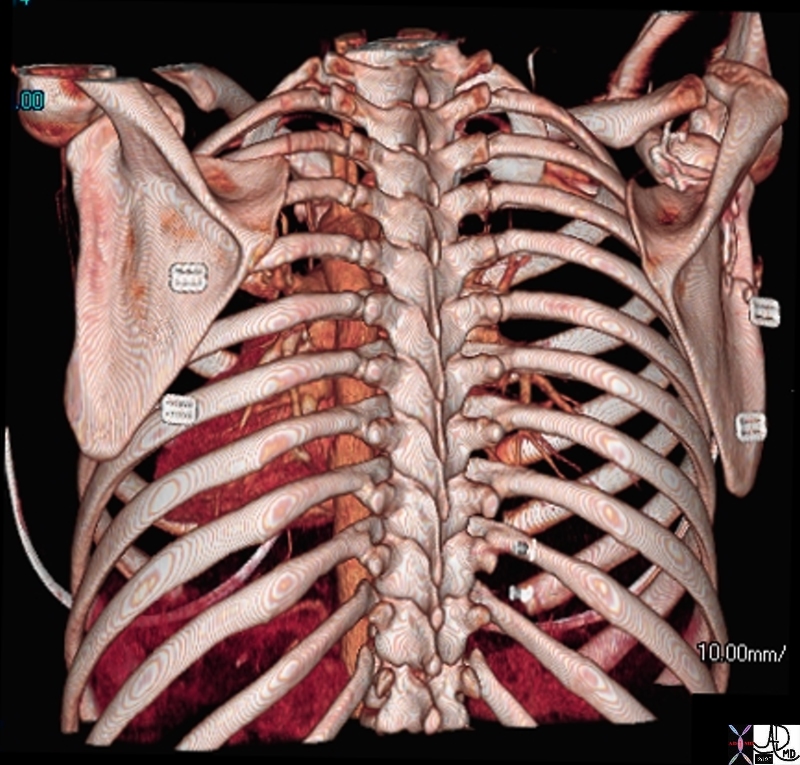
3D Reconstruction in the Lateral Projection of the Scapula
|
| Courtesy Ashley DAvidoff MD 73601 |
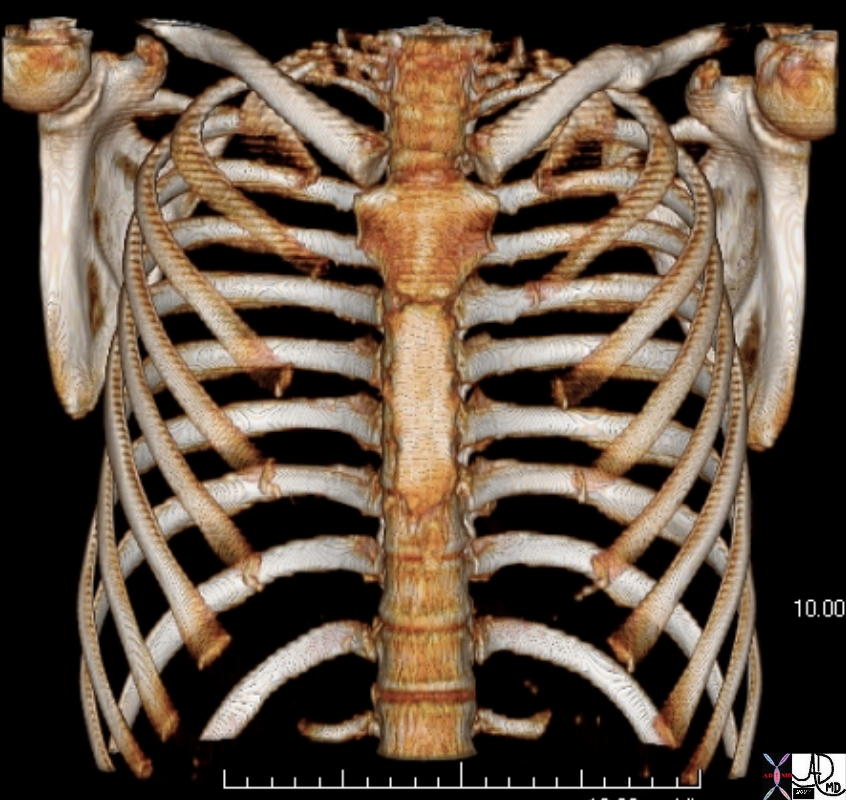
3D Reconstruction in the A-P Projection of the Scapula |
| Courtesy Ashley DAvidoff MD 73602 |

88652.8
|
|
Young patient following trauma showing a fracture within the left rib and scapula
Courtesy Ashley Davidoff MD 88652.8
|
References
Davis MF, Davis PF, Ross DS. Expert Guide to Sports Medicine. ACP Series, 2005.
Elstrom J, Virkus W, Pankovich (eds), Handbook of Fractures (3rd edition), McGraw Hill, New York, NY, 2006.
Koval K, Zuckerman J (eds), Handbook of Fractures (3rd edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Lieberman J (ed), AAOS Comprehensive Orthopaedic Review, American Academy of Orthopaedic Surgeons, 2008.
Moore K, Dalley A (eds), Clinically Oriented Anatomy (5th edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Wheeless?s Textbook of Orthopaedics: Scapula Fractures (http://www.wheelessonline.com/ortho/scapular_fractures)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
88652.8
Young patient following trauma showing a fracture within the left rib and scapula
Courtesy Ashley Davidoff MD 88652.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
88652.8
Young patient following trauma showing a fracture within the left rib and scapula
Courtesy Ashley Davidoff MD 88652.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Young patient following trauma showing a fracture within the left rib and scapula
Courtesy Ashley Davidoff MD 88652.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Young patient following trauma showing a fracture within the left rib and scapula
Courtesy Ashley Davidoff MD 88652.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
88652.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
88652.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
3D Reconstruction in the A-P Projection of the Scapula
Courtesy Ashley DAvidoff MD 73602
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
3D Reconstruction in the A-P Projection of the Scapula
Courtesy Ashley DAvidoff MD 73602
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Courtesy Ashley DAvidoff MD 73602
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Courtesy Ashley DAvidoff MD 73602
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
3D Reconstruction in the A-P Projection of the Scapula
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
3D Reconstruction in the A-P Projection of the Scapula
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
3D Reconstruction in the Lateral Projection of the Scapula
Courtesy Ashley DAvidoff MD 73601
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
3D Reconstruction in the Lateral Projection of the Scapula
Courtesy Ashley DAvidoff MD 73601
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Courtesy Ashley DAvidoff MD 73601
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Courtesy Ashley DAvidoff MD 73601
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
3D Reconstruction in the Lateral Projection of the Scapula
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
3D Reconstruction in the Lateral Projection of the Scapula
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
CT reconstruction of a Normal Scapula
Courtesy Ashley Davidoff MD 49640
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
CT reconstruction of a Normal Scapula
Courtesy Ashley Davidoff MD 49640
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Courtesy Ashley Davidoff MD 49640
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Courtesy Ashley Davidoff MD 49640
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
CT reconstruction of a Normal Scapula
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT reconstruction of a Normal Scapula
)
