
The Common vein Copyright 2011
Fractures
Description and thus classification of a fracture provides the key to understanding the complexity of the injury and provides a basis for treatment planning. In the foregoing discussion, classification based on the mechanism of injury (blunt vs penetrating), vectors of the forces (horizontal compressive, rotational) and age of the patient (young vs old), were the focus. In the following discussion specific descriptors are used to direct clinical decisions. Therefore accurate description and appropriate use of terminology is important. The frequent “bottom line” is whether the fracture is going to require manipulation or not. The background to the bottom line is whether the fracture is stable, and whether it will heal without intervention. The most important element is relative position of the components of the fracture.
However the first priority is to establish whether the fracture is open to the external environment or whether it is closed.
Open (Compound) or Closed Fractures – An early important clinical action point
This distinction between an open and closed fracture is easily made at the bedside. It is an extremely important decision, since an open or compound fracture infers that the bony components of the fracture have been exposed to the outside and by definition the bone is infected precluding placement of hardware until the infection is cleared. By default these fractures require intraoperative debridement and attention to complete decontamination before decisions are made about further surgical management. Most fractures are closed, so once clinically confirmed, radiological assessment is the next step.
The Appearance of the Fracture on X-Ray
The X-ray is used to assess stability of the fracture and determine the amount of bone on bone contact which is relevant for future stability and healing.
Basic Descriptive Algorithm
A descriptive approach to fractures is no different from adjectives used to describe other structures in these modules. Defining the component parts is the first step. A fracture consists of at least two fragments as well as the fracture line itself. Thereafter the elements that relate to the size, shape position and character of the fracture follow. Associated findings completes the basic elements of description.
Parts Size, Shape, Position, and Associated Findings
The algorithm starts with defining the parts, then fracture line itself and then defining how the fracture fragments relate to each other . If the fracture contains two parts it is considered a simple fracture, and once it contains 3 or more it is defined as a comminuted fracture. Counting the parts in this instance also describes the size of the fracture. Next, the fracture line is addressed. Is the fracture partial or complete? Does it extend through both sides of the bone (complete), or only part (incomplete). This evaluation is also part of assessing the size of the fracture. Next is the shape of the fracture line. The fracture for example may be transverse, oblique or spiral. Lastly the positional elements of the fragments of the fracture, which includes the general geographic location of the fracture such as which bone , which side of the body, and location in the bone, eg right tibial shaft. More importantly is the position of the parts in relation to each other. The question is whether the fracture fragments are displaced and if so, the detail of the displacement. Fractures may be described as being anatomically aligned, displaced, angulated, foreshortened or lengthened.
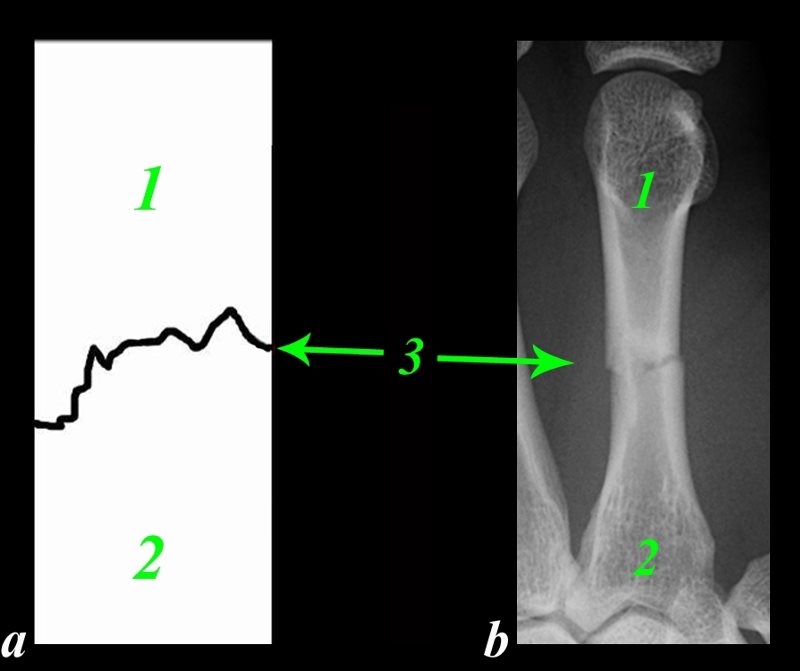
The drawing (a) in conjunction with a fracture of a long bone (b) shows the simplest form of a fracture consisting of three basic parts. The proximal fragment (1) the distal fragment (2) and the fracture itself (3) In this instance the size shape and position would be described as a simple (size- two parts), complete, involving both sides of the cortex (size), transverse fracture (shape of 3) of the shaft of the 3rd right metacarpal (position).
The positional relationship of the components of the fracture defines whether the fracture needs manipulation. In this case the component parts are anatomically aligned and no manipulation is required since the fracture is stable. Splinting will be required to maintain the alignment while it is healing.
Courtesy Ashley Davidoff Copyright 2011 103498fg02.8

Image a, is the X-ray in the lateral projection of the right femur of a 93 year old female and image b is the same image overlaid in green with the fracture highlighted in black and white.
Applying the algorithm to this fracture would result in the following description. There is a simple (two parts -size), complete (size), transverse (shape) fracture of the mid shaft of the right femur (position). The distal part is displaced posteriorly and superiorly resulting in foreshortening (position).
There is no ?bone on bone? contact and hence healing would be near to impossible and open reduction therefore necessary This is an example of a transverse pathological fracture caused by metastatic malignant disease.
Courtesy Ashley Davidoff Copyright 2011 101121c.8s
The descriptors will be discussed in more detail in the following paragraphs.
The Convention of Describing the Distal Fragment in Relation to the Proximal Fragment
When the fragments are displaced then it is the convention to describe the distal fragment in relation to the proximal fragment. Thus if the distal fragment is medially positioned then the fracture is described with “medial displacement of the distal fracture in relation to the proximal fragment”.

The A-P projection of the left humerus is from a 76year old female who fell. Step 1 (b)of the assessment of her X-Ray reveals a simple (size = 2 fragments) oblique (shape = green line 3) fracture through mid shaft of the left humerus (position).
This fracture is more complex because of the aberrant position of the fragments and the next step requires an evaluation of the fragments to determine the need for intervention. The elements that create concern are shortening (size), angulation (shape), displacement or rotation (position). In this case (c) there is no foreshortening, but there is angulation (yellow lines in c), displacement, but no rotation. In addition the fragments are distracted and bone on bone contact is limited. The intersection of the two yellow lines describes the angulation of the apex and it is pointing laterally. The need to intervene to improve bone on bone contact and improve alignment is necessary in this case. External manipulation was utilized with success.
Courtesy Ashley Davidoff Copyright 2011 103519cd08.8

A closed reduction was performed, resulting in excellent anatomical alignment of the fracture fragments with significant bone on bone contact. As long as this contact is maintained (and confirmed in the lateral projection), excellent healing should proceed.
Courtesy Ashley Davidoff 103519cL.8
Complete Fractures
Simple or Comminuted – Counting the Fragments
With X-ray in hand the decision points relates to the amount of bone on bone contact, and the stability of the fracture . This decision is not a straightforward one and is multifaceted.
A descriptive approach to fractures follows an algorithm of the structural descriptions used in these modules which includes the parts that make up the structure and the the size, shape position and character of the component parts. Thereafter follows a description of the associated findings.
Sometimes the decision is black and white when there is obvious distraction and malalignment and the components will not come together by closed reduction. The importance of bone on bone contact are relevant for healing and stability .

This A-P examination of the proximal left femur of a 91 year old female shows a comminuted transverse fracture of the intertrochanteric region of the right femur with mild varus deformity. A fragment of the lesser trochanter is seen medially
Courtesy Ashley Davidoff Copyright 2011 101640b01.8

The artistic rendering of fractures of the skeletal system are typified by a dramatic comminuted fracture of the skull that dominates the centre of the image. The pain of the patient is palpable. Surrounding the depressed comminuted skull fractures are other examples of comminuted fractures including 2 examples of a Colle?s fracture in the row above the skull, comminuted fractures of the phalanges at 3 and 9 oclock, and complex comminuted iliac crest fractures on either side of the lower row.
Courtesy Philips medical Systems (skull X-ray) Artistic Rendering Courtesy Ashley Davidoff MD copyright 2011 all rights reserved 88361c03.32k.85s
Position of the Fracture

Two views of the proximal radius of a 38 year female following blunt trauma in oblique and lateral projection show a comminuted fracture of the head of the radius with involvement of the joint surface (white arrow). A transverse fracture at the junction of the diaphysis with the metaphysic is better seen on the lateral examination An avulsed fragment is shown by the green arrow, easily seen in b, but barely visible in d.
Courtesy Ashley Davidoff MD 103258c02.8s
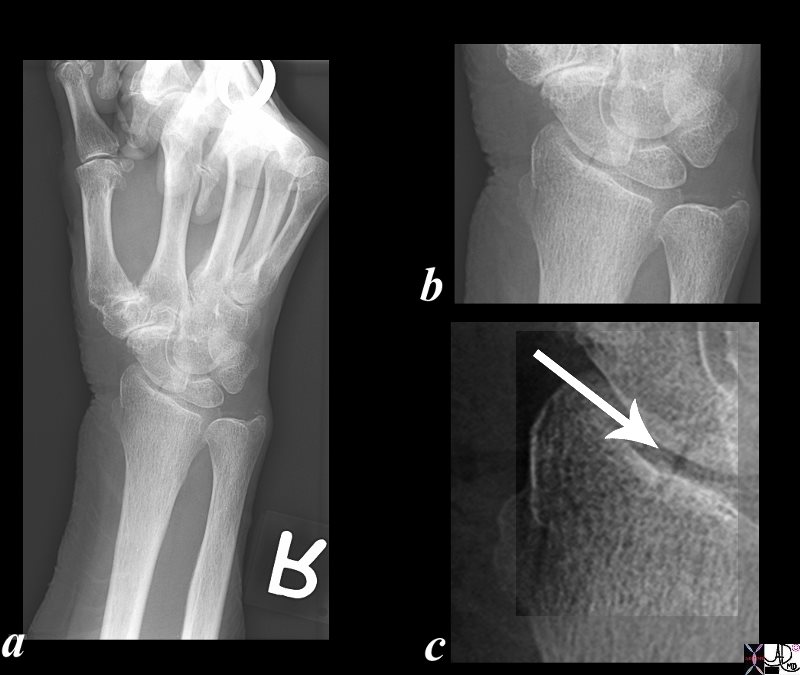
Single oblique view of the distal radius in oblique and lateral projection shows a simple fracture of the distal radius with involvement of the joint surface (white arrow c). Anatomic alignment is well maintained. The main issue of this minor fracture is the associated joint involvement
Courtesy Ashley Davidoff MD 103271c03.81s
Position of the Component Parts of the Fracture
Alignment
Alignment of the component fracture fragments is a key component in the evaluation of fractures. Alignment describes the relationship of the longitudinal axis of one fragment to another.
When a fracture has anatomical alignment it means that almost 100% of the surface of the two components of the fracture are appropriately aligned in the longitudinal axis. Anatomical alignment means that continuity of the fragments is maintained. Since the fracture needs bone on bone contact for the reparative process it is most important that optimal contact is achieved.
Partial continuity implies that there is some contact between the components.
Fractures that have some continuity of osseous fragments may, in general, be treated by closed reduction, while fractures that have lost continuity usually require open reduction.
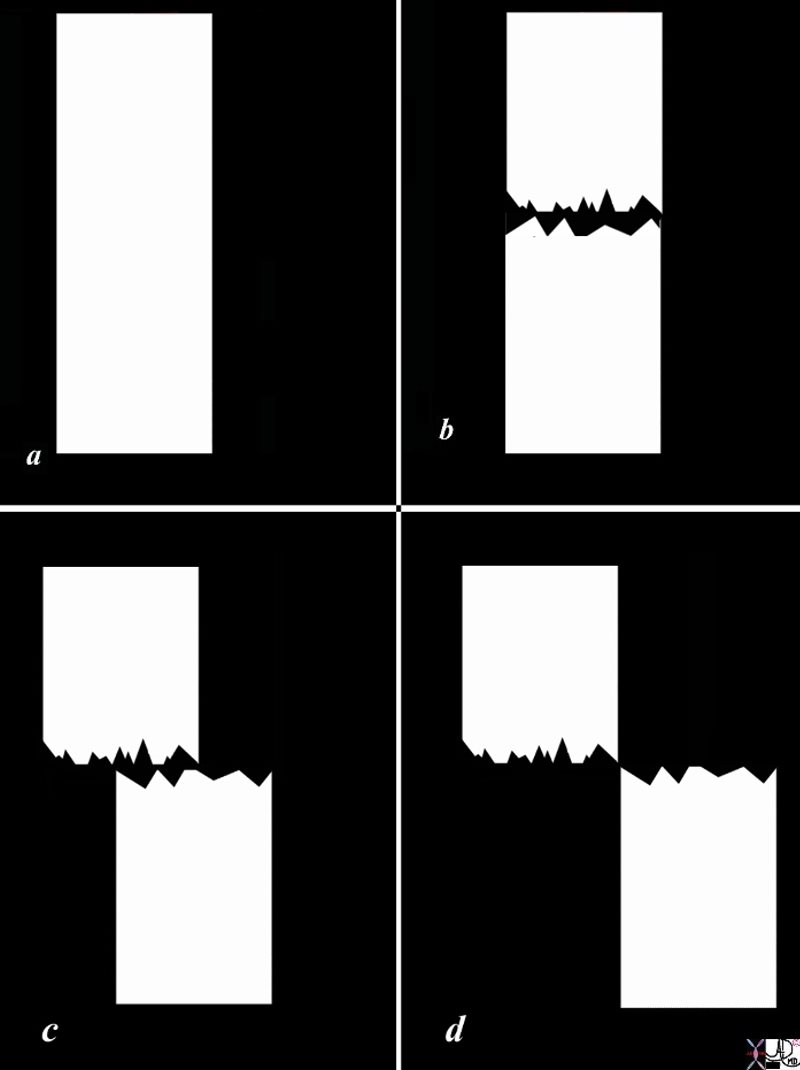
The diagram shows a diagram of a bone without fracture (a), an example of an anatomically aligned fracture with no length change, a fracture that is displaced by about 50% (c), and a fracture in which the component parts are totally displaced (d) without any bone on bone contact. As long as the finding on the A-P examination is in agreement with the lateral examination regarding alignment, the fracture exemplified in b, will likely not require reduction, the fracture in d probably require reduction and the fracture in c, may or may not require reduction.
Courtesy Ashley Davidoff Copyright 2011 103498l01bc02.8s
100% “bone on bone”
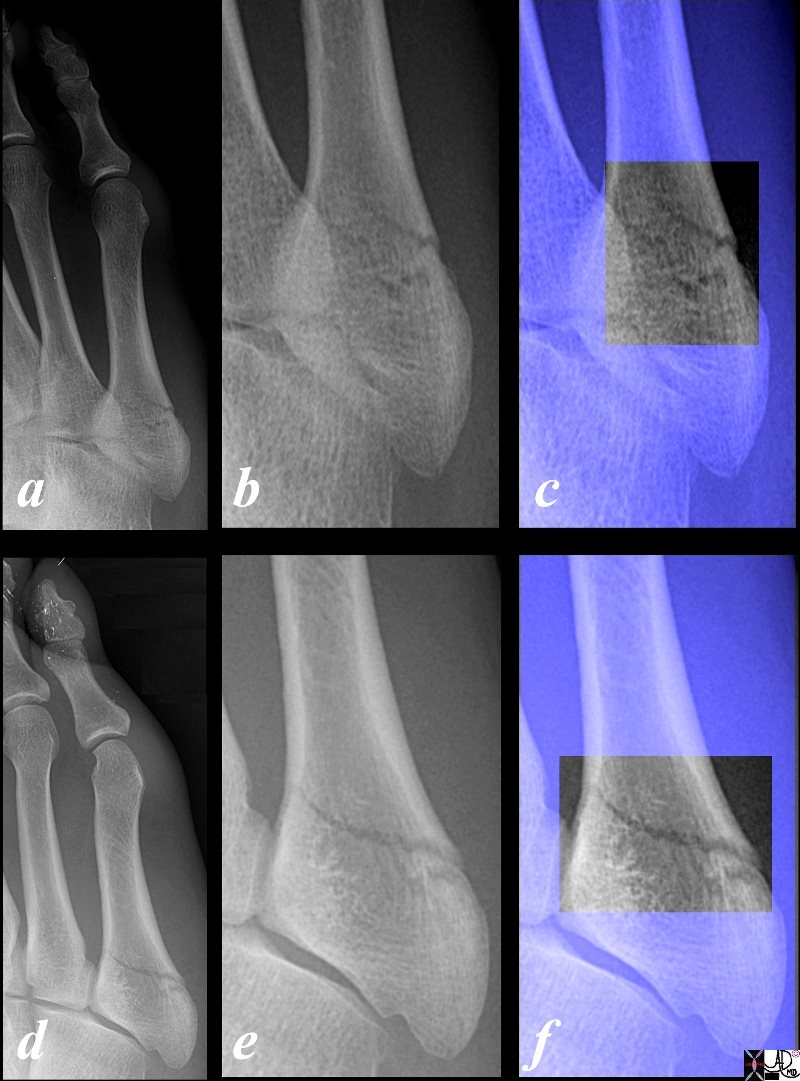
This X-ray of the right foot of a 31 year old male who sustained a traumatic episode is taken in the A-P (a) projection. The base of the right 5th metatarsal is magnified in image b and overlaid and highlighted in image c, and shows a simple transverse fracture of the base of the fifth metatarsal with anatomical alignment. Image d is an X-ray in the oblique projection again showing a simple non- displaced transverse fracture of the base of the fifth metatarsal. Image e represents the magnified view and image f shows the fracture highlighted and overlaid. The fracture was not visualized on the lateral projection. This series of images exemplify a complete bone on bone fracture with perfect anatomical alignment. As long this alignment remains intact healing without reduction should proceed effectively and normally.
Courtesy Ashley Davidoff Copyright 2011. 99718cb03L.01.8s
Displacement
Displacement is the term used to describe the malalignment of two fracture fragments where there is loss of cortical continuity. There are many adjectives used to describe the displacement, since the fracture fragments can be displaced anteriorly posteriorly medially, laterally, superiorly inferiorly or any combination of these.
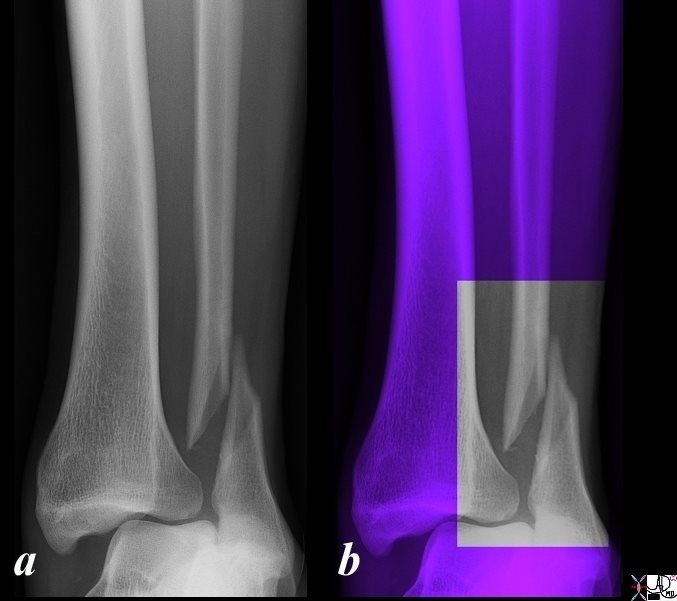
No “Bone on Bone” Alignment
The X-ray is taken in the antero-posterior (A-P) projection and shows a simple displaced oblique fracture of the distal shaft of the fibula in a 36 year old male following blunt trauma. In image b the ankle is overlaid in purple and the area of interest is highlighted in black and white. There is significant, medial displacement of the proximal fragment so there is virtually no bone on bone alignment. This morphology is not conducive to satisfactory healing and likely would require open reduction. In addition to the fracture there has been significant damage to soft tissues and the mortise is not intact with medial displacement and dislocation of the tibia in relation to the talus suggesting rupture of at least the deltoid ligament. The mechanism of this injury is likely due to a direct hit on the lateral aspect of the fibula causing the oblique fracture and dislocation of the tibia off the talus.
Courtesy Ashley Davidoff Copyright 2011 99854.6b01c001
There are three major aspects that encompass displacement including length discrepancy, angulation, and rotation.
This diagnosis of displacement requires two views on an X -ray since a foreshortened appearance may for example also be due to the one component being pushed down and posterior and the other being pushed up and anteriorly.
Displacement – Length Discrepancy
Length discrepancy occurs when the the two major fragments become overlapped or distracted.
Overlap occurs as a result of the downward movement of the one component and or the upward movement of the second fragment. This is also called apposition (or bayonet apposition) which infers fragment overlap. As a result there is shortening of the bone.
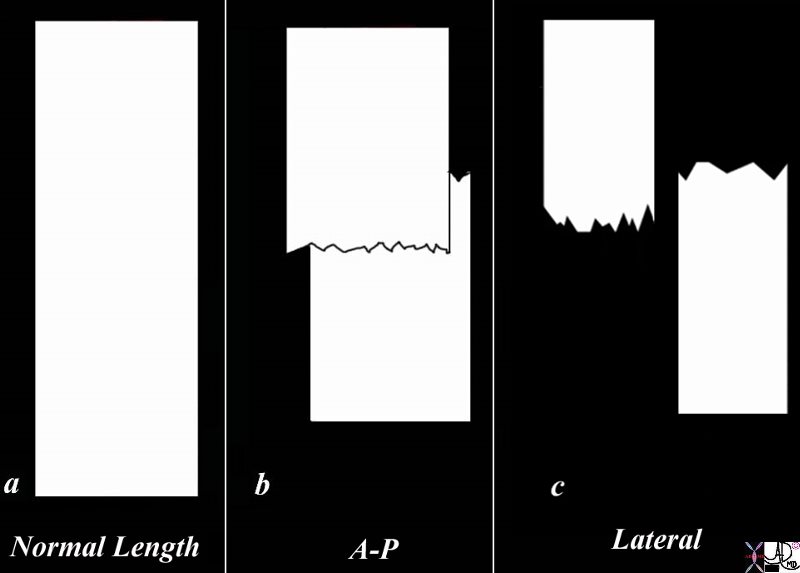
The diagram shows a normal length bone represented by a white rectangle without fracture (a), and (b) an example of overlap fracture in the A-P projection with overall shortening of the bone, while the lateral examination (c) shows posterior and superior displacement of the distal fragment accounting for the foreshortening. Sometimes this fracture in the one projection may look anatomically aligned but in the orthogonal projection, no bone on bone contact is seen. Two views are essential in the evaluation of all fractures.
Courtesy Ashley Davidoff Copyright 2011 103498k04.8s
Impaction fractures occur when one component of a fracture is driven into, or telescoped into the second part causing foreshortening of the bone.

Three views of the distal radius and ulna in the anteroposterior (a), oblique (b), and lateral (c), projection show an acute simple transverse and impacted (arrow) fracture of the shaft of the distal ulna with near anatomic alignment.
Courtesy Ashley Davidoff MD 76722c.81L
Distraction infers the longitudinal separation of the fragments, and overall lengthening of the bone.
Displacement – Angulation
Angulation infers an angular relationship of the longitudinal axis of the fracture fragments, and usually describes the distal fragment. Angulation may be due to medial lateral anterior or posterior displacement of the distal fragment.
Certain alternate terms have been used that are synonyms sometimes specifically related to the part of the body being described and sometimes as a matter of preference. Anterior and posterior are sometimes described as ventral, and dorsal, palmar when in reference to the hand, plantar when in reference to the foot, volar, varus and valgus angulation as a matter of preference.
Anterior angulation (ventral angulation, palmar angulation)
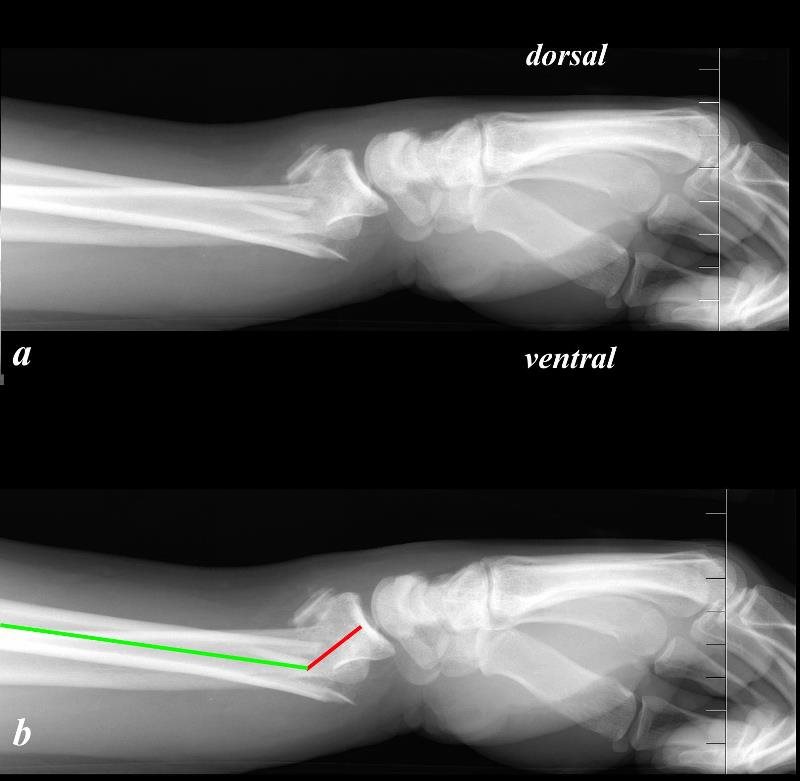
aka Distal Displacement
The image demonstrates the lateral projection of an X-ray from a 40 year old man who fell on an outstretched hand and sustained a fracture of the distal radius. This fracture is called a Colle?s fracture and is characterized by its location being about 1.5 inches from the distal end of the radius, at the weak portion of the distal radius where the diaphysis meets the metaphysis called the at the cortico-cancellous junction. Additionally it is characterized by dorsal displacement of the distal fracture fragment but with ventral angulation of the fracture. The shape of the combined appearance of the proximal fragment, distal fragment and the carpals and metacarpals on clinical and lateral radiological examination is reminiscent of a dinner fork and hence the deformity is called “dinner fork deformity”.
The anatomical position of the forearm is by convention with the palm of the hand facing forward (anteriorly), and so the palm of the hand is the ventral surface. The back of the hand is called the dorsal or posterior surface.
The direction of the forces and weight pushes on the wrist so that the radius gets pushed to the anatomically named ventral portion of the forearm and the distal fragment attached to the wrist gets pushed dorsally.
Courtesy Ashley Davidoff Copyright 2011 101288c02.8
Posterior angulation (dorsal angulation, volar angulation, plantar angulation)

This X-ray shows a simple transverse fracture of the middle of the shaft of the left second metacarpal with the hand held in the antero-posterior (A-P) projection. Image b shows the fracture overlaid in black and the green line is almost straight suggesting near anatomical alignment. The presence of minimal foreshortening suggests angulation which is better appreciated on the oblique projection, (c and d). In this view there is dorsal or posterior angulation and some impaction accounting for the foreshortening seen on the A-P projection.
Courtesy Ashley Davidoff Copyright 2011. 101198.8cL03
Medial angulation (valgus)
Lateral angulation (varus)
Some of these terms we have already used such as impaction fractures
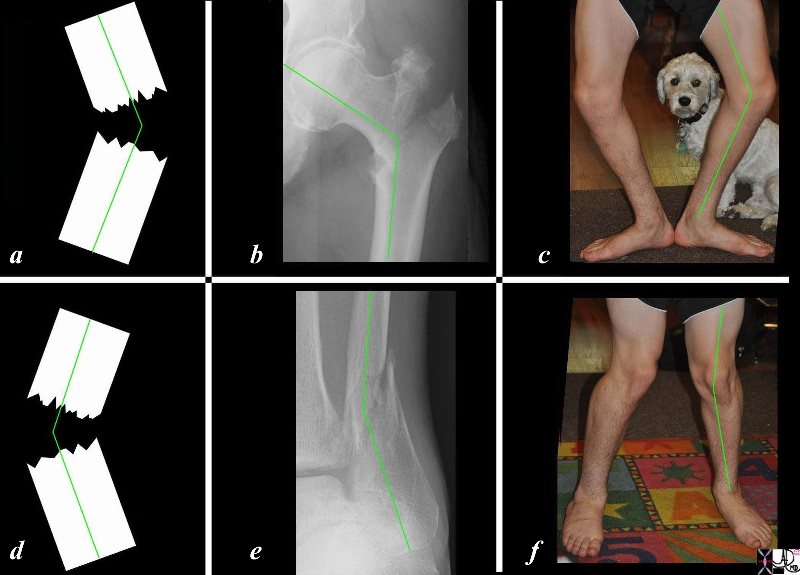
The diagram labeled a, shows representation of a fracture that is angulated toward the lateral aspect. Image b shows a intertrochanteric fracture of the proximal left femur, with similar lateral angulation (b). This type of angulation is also known as varus angulation. Varus is a Latin word which means bow legged. A bowlegged stance is shown in image c. The diagram labeled c, shows representation of a fracture that is angulated toward the medial aspect. Image d shows a distal fibula fracture, with similar lateral angulation. This type of angulation is also known as valgus angulation. Valgus is a Latin word which means ?bandy legged or knock kneed. A knock kneed stance is shown in image c.
Courtesy Ashley Davidoff Copyright 2011 103498l02c06L.8s
The terms varus and valgus are very similar and a variety of mnemonics have been used to try and remember which one is which. The best mnemonic relates to the story of a Russian woman walking down the street when a loose pig runs between her legs. As it does so, she looks down opens her legs and shouts “Varus the pig?” This scene is so comical and unforgettable that it has stuck in my mind for 30 years and I have never forgotten the difference between the two types of angulation.

The descriptions of a ?valgus? and ?varus? deformity are orthopedic terms referring to the direction of the distal fragment. Varus deformity is the term used for the inward deformity of the distal fragment and valgus the outward deformity. Varus means ?bow legged?, and valgus ?knock-kneed? That the words sound so much alike and because they are not only used to describe knee deformity but also deformity in other areas in orthopedics, there is often confusion in the terminology. Thus one of the mnemonics is to describe an old woman walking down the street who is surprised by a pig that runs through her legs. She looks down between her legs and exclaims ?Varus is the pig?? Because this is so ridiculous it is memorable. Another way of remembering the varus deformity is to recall the ?air? of ?v-air- us? describing the large amount of ?air? between the legs.
Courtesy Ashley Davidoff Copyright 2011 96172pd06.83
This A-P examination of the right humerus of a 76 year old female following blunt trauma shows an acute almost transverse simple fracture of the middle of the shaft of the left humerus. The component parts are not touching at all in this projection with mild varus angulation (a). The lack of bone on bone after the initial injury required reduction. In this instance, following closed reduction the component parts were well aligned with significant bone on bone contact and near anatomic alignment.
Courtesy Ashley Davidoff 103519cL.8
Nature of the Fracture
This category is closely linked to the mechanism of injury.
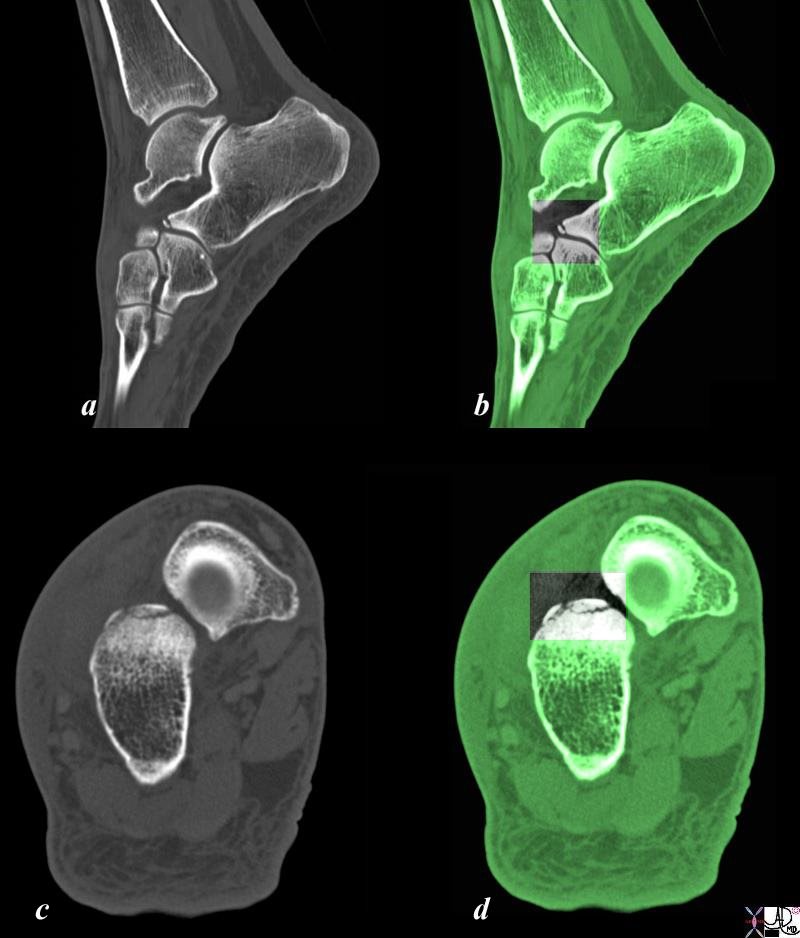
The sagittal reconstruction of the CT scan of an adult female following trauma shows an avulsion fracture of the anterior tip of the calcaneus, accentuated in black and white over the green overlay (b).
Images c and d are axial sections through the anterior aspect of the calcaneus and they show a fragmented comminuted avulsion fracture. In image d the section is overlaid in green and the area of interest is highlighted in black and white. The avulsion fracture is a result of the pull of a ligament or tendon that inserts onto the calcaneus.
Courtesy Ashley Davidoff Copyright 2011 99844c.81s
The blunt injury forces have been described but high velocity and penetrating injuries bring a different perspective since the bony injury by its nature is more complex and the soft tissue injury often more pronounced.
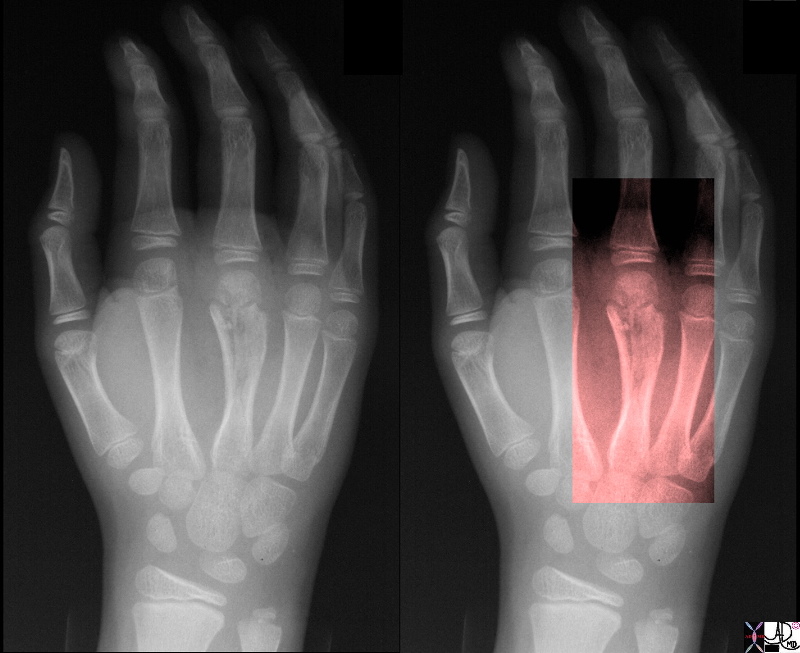
The A-P examination of the hand of a young patient with unfused epiphyses reveal a gunshot injury to the hand resulting in a shattered third metacarpal of the right hand. The distal shaft of the bone is flared with a horizontal fracture through the growth plate and fractures along the long axis of the shaft. The soft tissues are swollen and some air is noted around the fracture site . This is a example of a high velocity penetration injury
Courtesy Ashley Davidoff Copyright 2011 32754c01.8s
Power Tool Injury High Velocity Saws
Injuries to the hand among power tool operators are not uncommon and often result in soft tissue injury, but the power of the tool easily overcomes the strength of bone and a combination of soft tissue injury and bone injury in the hand is commonly seen as well.

The series of X-ray are from a 29 year old man who amputated the tip of his right middle finger with a sharp power tool. Image a is an A-P view, magnified in image b and overlaid with the fracture line (black) in c. The green arrow points to the bone edge of the distal tuft, which is reduced in size and has lost its outer cortex, exposing a fragmented and trabeculated border. The red arrow points to the difficult to see skin edge. Image d is a lateral projection of the middle finger, magnified in image e, and overlaid with the photograph of the soft tissues of the finger and nail bed. This projection reveals the well defined and relatively straight skin and bone injury as a result of the sharpness of the instrument. The black line reveals the inverted ?T? shaped fracture.
Courtesy Ashley Davidoff Copyright 2011 102105bc07L.8s

This is one of the most painful X-rays of my career and it is older than 30 years. The exact history eludes me but there has been obvious traumatic injury to the hand with multiple fractures (black arrows) a transverse skin incision that contains a broad band of air (white arrow), probable debridement of the severely injured metacarpal row, and extensive pinning and wiring of the thumb following surgical trauma. The combination of the large somatic sensory nociceptor supply to the hand, together with the extensive skin, bone,and tissue damage, is difficult to perceive the extent of the pain that this poor patient went through. The remarkable feature is the maintenance of blood supply to the hand.
Courtesy Ashley Davidoff MD copyright 2008 17496c02.8s
Aside from the high velocity fractures there are fractures that are considered crush injuries where compressive forces fragment the bone into many pieces. These may take the benign form of a crush injury of the distal phalanx, or may be more severe in the spine where impingement on the cord or nerves predisposes to a dangerous complication of nerve or devastating spinal cord damage.
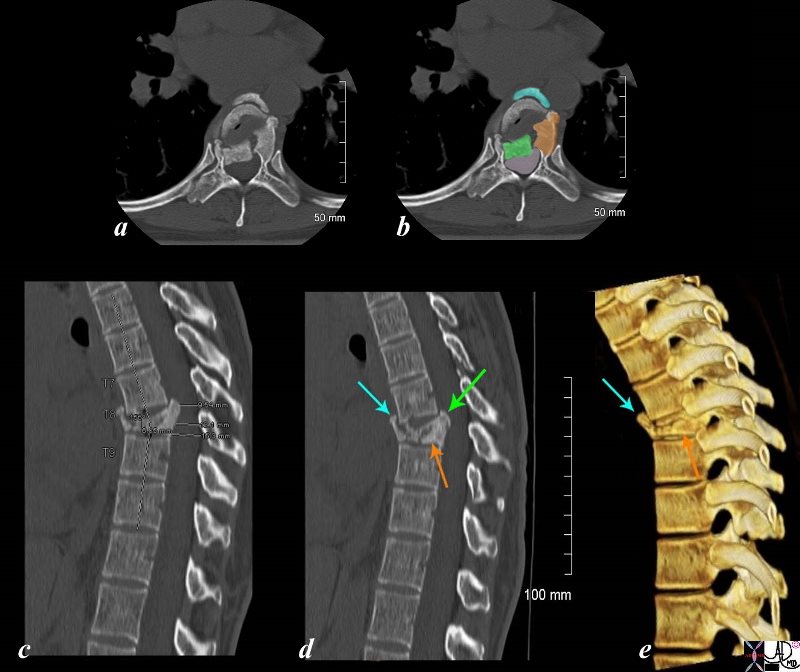
The panel of images using CT technology revealing a compression fracture of T8 in a 43 year old female who sustained compressive trauma to the thoracic spine resulting in a kyphosis at that level. Images a and b are transverse images showing a right sided retropulsed fragment (green) impinging on the thecal sac (light pink in b) The fragment that has ruptured anteriorly is overlaid in teal blue. The middle portion of the fracture is overlaid in orange. Image c is a mid sagittal reconstruction of the thoracic spine and shows the compression fracture with a 9.5mm retropulsed fragment with reduction of the thecal sac diameter to 11mm. The overall bony density of the fracture is increased suggesting a non pathological compression fracture. Image d is also a midsagittal reconstruction showing the retropulsed fragment (green arrow), the anteriorly displaced fragment (teal arrow) and the fragment in the middle indicated by the orange arrow. Image e is a 3D reconstruction of the T8 fracture enabling the visualization of the anterior fragment (teal arrow) and the middle portion of the fracture (orange arrow).
Courtesy Ashley Davidoff Copyright 2011 102190c05L.8s
References
Herring, William recognizing Fractures and Describing Them On Line Powerpoint Show