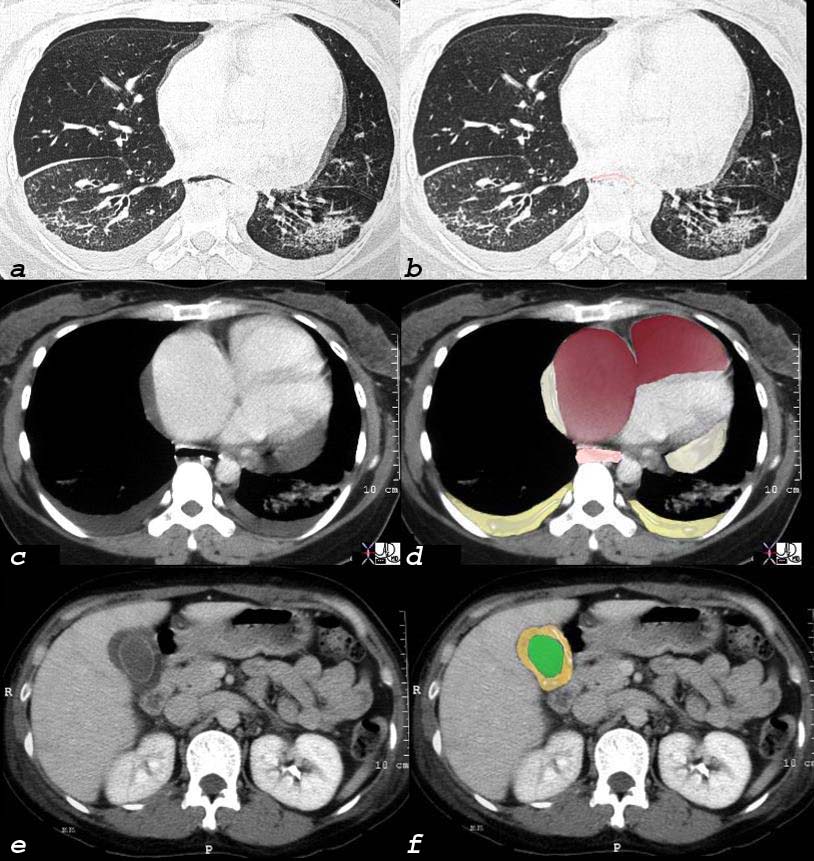
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
Scleroderma – Involvement of Lung and Esophagus
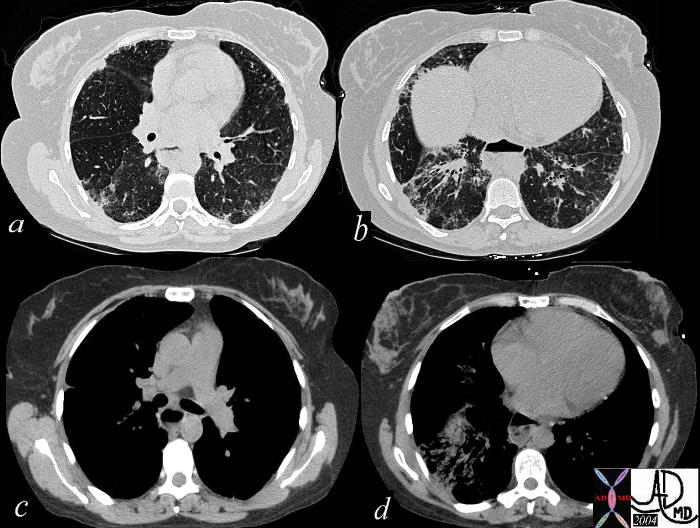
This series of axial CT scans in a 75 year old patient through the chest show coarsened interstitial markings with a a reticular pattern, dominant in the lower lobes and to some extent peripheral. In the right lower lobe there is evidence of alveolar type change with mild traction bronchiectasis. Note also the dilated esophagus in c and d. This patient has scleroderma.
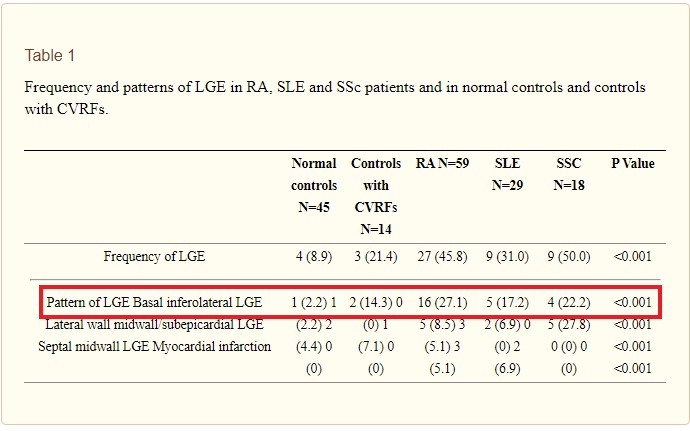
PATTERN OF LGE IN RA, SLE and SCLERODERMA Ntusi et al Myocardial tissue characterisation with late gadolinium enhancement in rheumatoid arthritis, systemic lupus erythematosus and systemic sclerosis J Cardiovasc Magn Reson. 2013; 15(Suppl 1): O47.
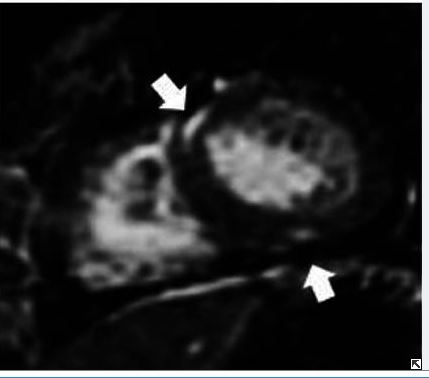
SCLERODERMA RVH and PERICARDIAL EFFUSION Short-axis SSFP image in systole (A) demonstrates RV hypertrophy secondary to pulmonary hypertension in this patient with scleroderma. PF = pericardial fluid. Straightening of the inter-ventricular septum suggests increased RV pressure. Anirudh (Ani) Mirakhur Beyond the Common Ground: The Unusual Suspects in Late Gadolinium Enhancement Conference Paper · January 2013 European Congress of Radiology SCLERODERMA LGE Long-axis image demonstrateS focal mid-wall LGE (arrows) in basal and mid-cavity inferoseptal LV wall and inferior RV wall. Mirakhur Beyond the Common Ground: The Unusual Suspects in Late Gadolinium Enhancement Conference Paper · January 2013 European Congress of Radiology
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Scleroderma – Involvement of Lung and Esophagus
This series of axial CT scans in a 75 year old patient through the chest show coarsened interstitial markings with a a reticular pattern, dominant in the lower lobes and to some extent peripheral. In the right lower lobe there is evidence of alveolar type change with mild traction bronchiectasis. Note also the dilated esophagus in c and d. This patient has scleroderma.
Courtesy Ashley Davidoff MD 39081c code lung pulmonary interstitium interstitial lung disease lower lobes ILD bronchiectasis esophagus dilated air fluid level scleroderma systemic sclerosis CREST CRST caoolagen vascular disease imaging radiology CTscan radiologists and detectives
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Scleroderma – Involvement of Lung and Esophagus
This series of axial CT scans in a 75 year old patient through the chest show coarsened interstitial markings with a a reticular pattern, dominant in the lower lobes and to some extent peripheral. In the right lower lobe there is evidence of alveolar type change with mild traction bronchiectasis. Note also the dilated esophagus in c and d. This patient has scleroderma.
Courtesy Ashley Davidoff MD 39081c code lung pulmonary interstitium interstitial lung disease lower lobes ILD bronchiectasis esophagus dilated air fluid level scleroderma systemic sclerosis CREST CRST caoolagen vascular disease imaging radiology CTscan radiologists and detectives
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This series of axial CT scans in a 75 year old patient through the chest show coarsened interstitial markings with a a reticular pattern, dominant in the lower lobes and to some extent peripheral. In the right lower lobe there is evidence of alveolar type change with mild traction bronchiectasis. Note also the dilated esophagus in c and d. This patient has scleroderma.
Courtesy Ashley Davidoff MD 39081c code lung pulmonary interstitium interstitial lung disease lower lobes ILD bronchiectasis esophagus dilated air fluid level scleroderma systemic sclerosis CREST CRST caoolagen vascular disease imaging radiology CTscan radiologists and detectives
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This series of axial CT scans in a 75 year old patient through the chest show coarsened interstitial markings with a a reticular pattern, dominant in the lower lobes and to some extent peripheral. In the right lower lobe there is evidence of alveolar type change with mild traction bronchiectasis. Note also the dilated esophagus in c and d. This patient has scleroderma.
Courtesy Ashley Davidoff MD 39081c code lung pulmonary interstitium interstitial lung disease lower lobes ILD bronchiectasis esophagus dilated air fluid level scleroderma systemic sclerosis CREST CRST caoolagen vascular disease imaging radiology CTscan radiologists and detectives
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Scleroderma – Involvement of Lung and Esophagus
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Scleroderma – Involvement of Lung and Esophagus
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Pulmonary Hypertension – Scleroderma
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Pulmonary Hypertension – Scleroderma
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Pulmonary Hypertension – Scleroderma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Pulmonary Hypertension – Scleroderma
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Scleroderma – Involvement of Lungs Pleura Pericardium Heart and Esophagus
30464c07 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Scleroderma – Involvement of Lungs Pleura Pericardium Heart and Esophagus
30464c07 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
)