
31 year old female with history of Polyareteritis Nodosa biopsy proven PAN (c/b mesenteric, renal, splenic artery, intracranial, extracranial aneurysms), chronic pain disorder on oxycodone, HTN, GERDHTN, CAD, GERD, depression, chronic pain ,
Biopsy proven PAN in 14 years ago involving mesenteric and renal arteries with numerous aneurysms of celiac trunk, SMA, R renal artery, splenic artery, intracranial and extracranial vessels, as well as history of jejunal ulcer.
10 years ago














CT barain 7 years ago








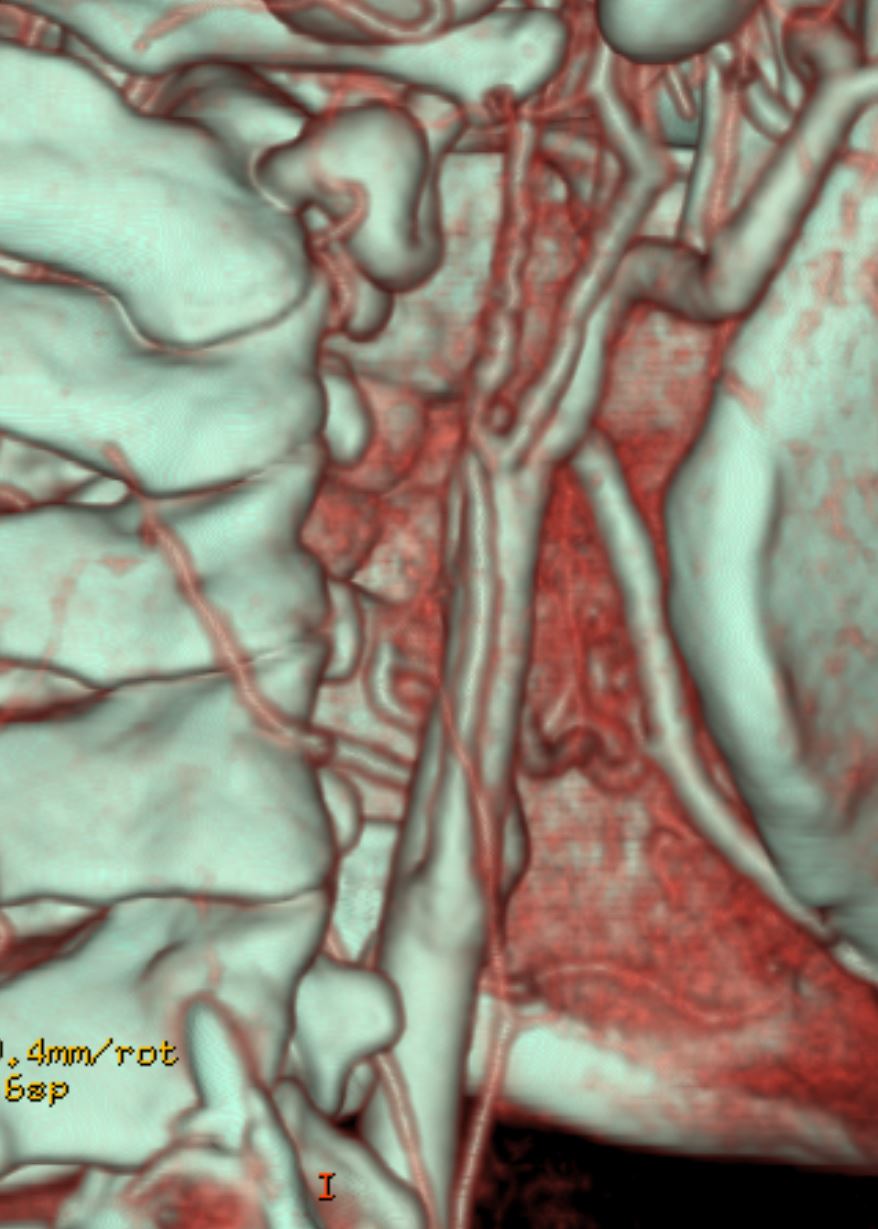


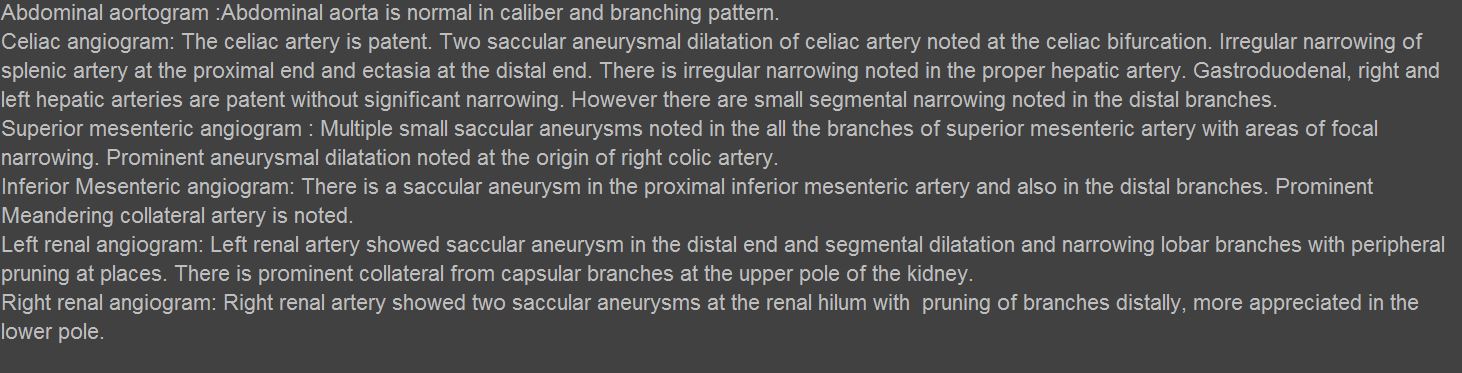
CTA head and neck:
The visualized portions of the arch as well as innominate, right
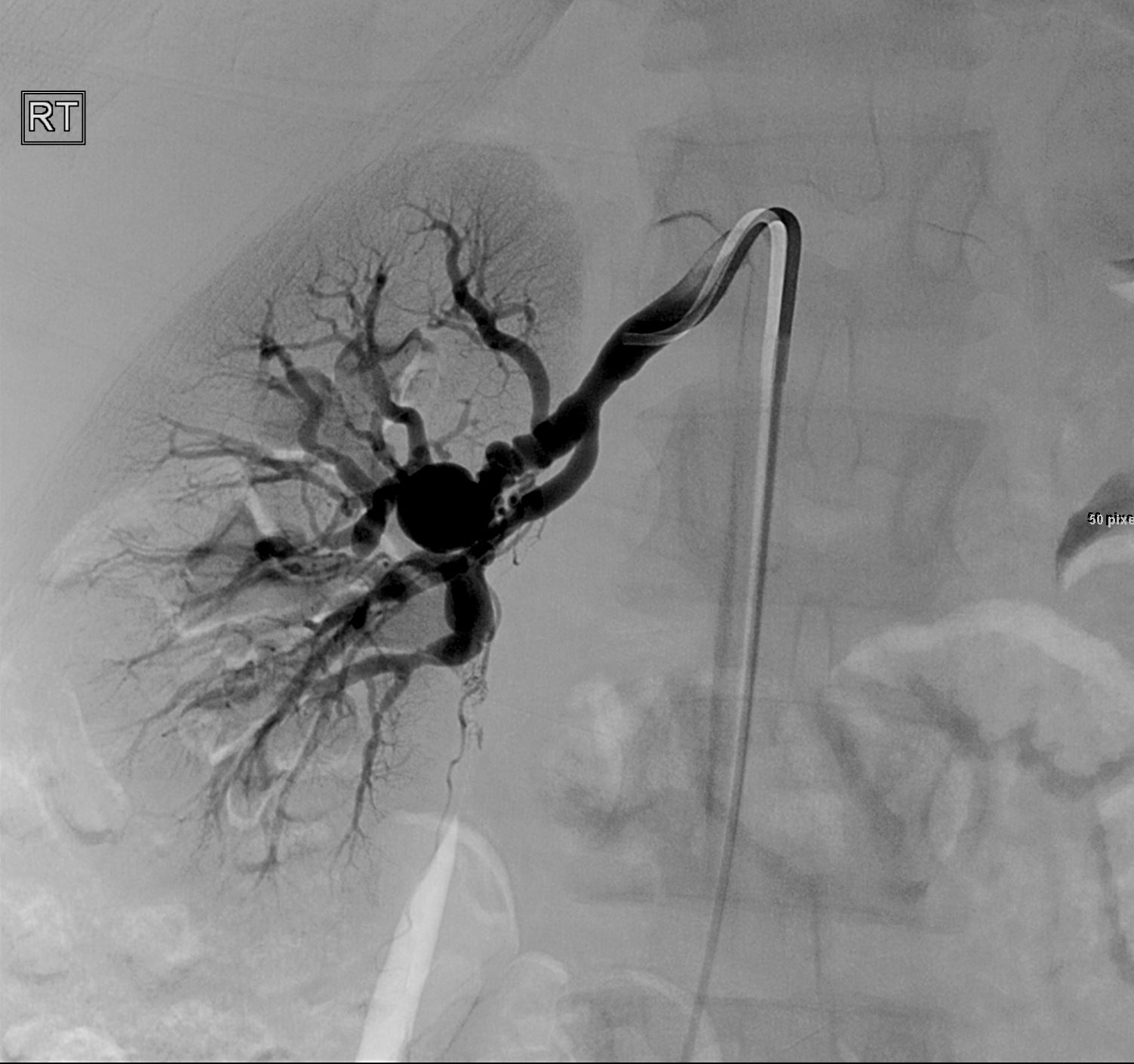
common carotid, right subclavian, left common carotid and left
subclavian arteries are unremarkable.
The common carotid arteries are unremarkable to the bifurcations.
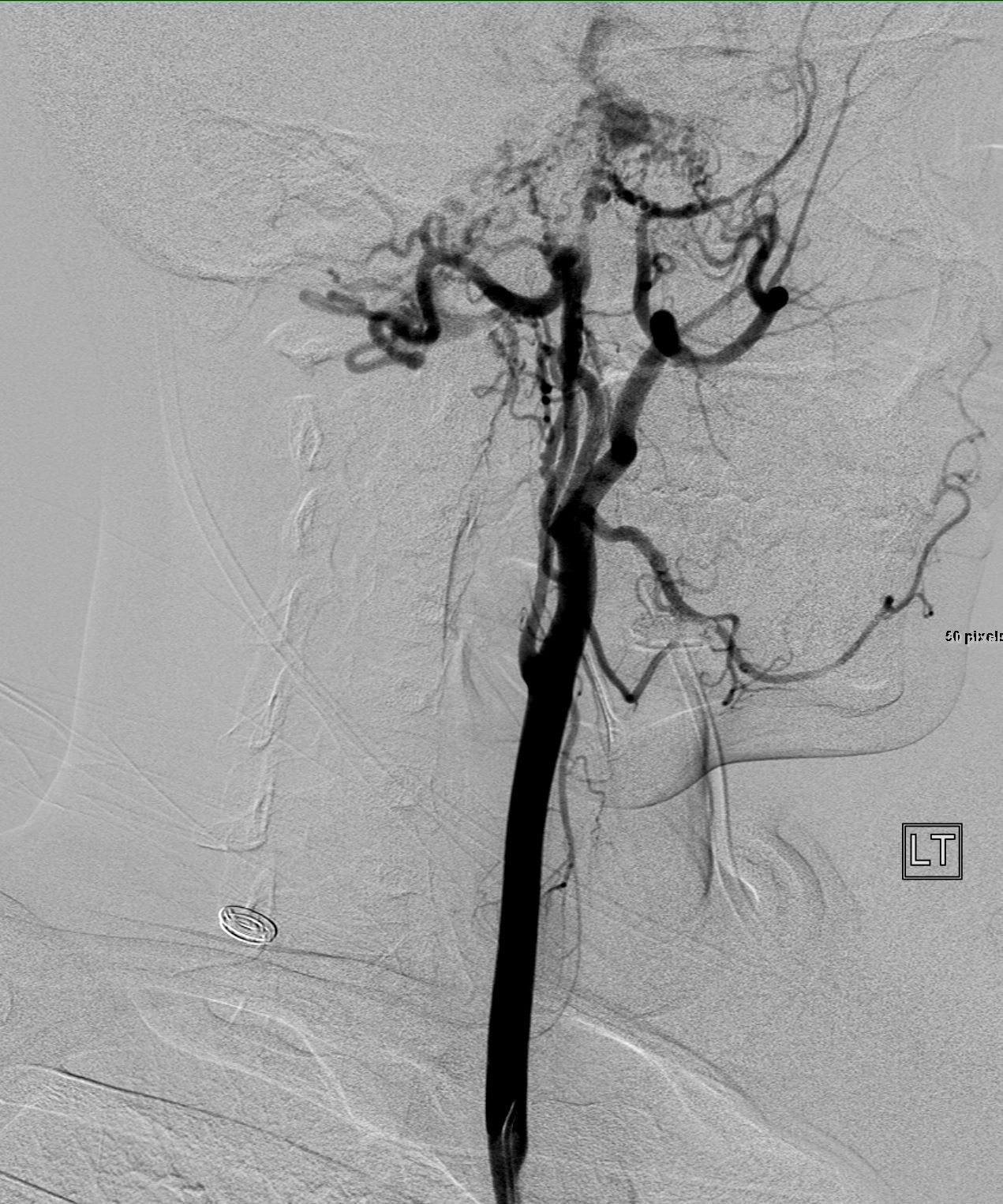
Bilateral extracranial ICAs are diffusely stenotic.
The right internal carotid artery narrows to approximately 1 mm or
less at the level of C2-C3 with an extremely
thready and beaded appearance throughout the distal course.
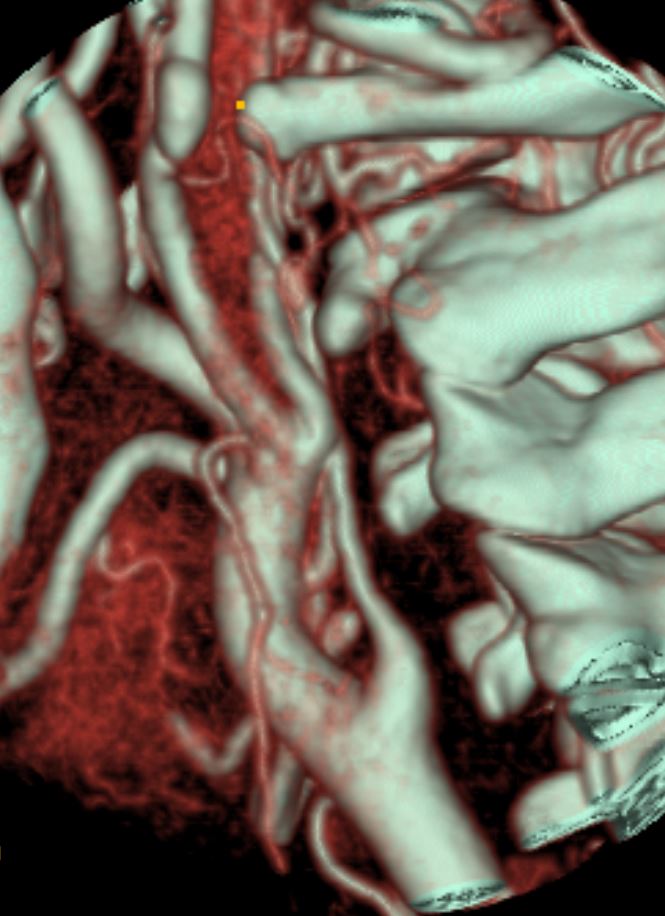
There is virtual occlusion of the left ICA again noted (less than 1
mm diameter suggested) approximately 1 cm below the skullbase, . Left ascending pharyngeal artery is larger
caliber than the left ICA throughout its course.
The external carotid systems provide extensive collaterals to the
petrous and cavernous segments of the ICAs and ophthalmic segment of left ICA as previously noted.
Extracranial internal carotid artery stenosis estimates are not based
on the use of distal ICA as the denominator since the distal ICAs are
diffusely abnormal. Severe stenosis is based on absolute diameters.
The right vertebral artery is dominant and smooth in caliber
(approximately 4 mm diameter) until the C2 level where there is
fusiform and multilobulated aneurysmal dilatation of the vessel measuring up to 9 mm. Another fusiform aneurysm
at C1 level measures up to 12 mm diameter (series 6, image 281).
These findings are unchanged from the prior exam.
The left vertebral artery is small caliber from its origin
(approximately 2 mm) and there is focal severe stenosis -virtual
occlusion -at the C2 level. The LV is reconstituted at the C1 level
by collaterals that appear to be primarily from the left occipital
artery and there is a junctional aneurysm of the left vertebral at
the confluence (extradural, approximately 5 mm diameter, 1 cm long –
This is unchanged fromprior exam.
Again seen is a 1-1.5 mm artery traveling anterior to the cervical
spinal cord the which joins the distal left vertebral artery just
proximal to the vertebrobasilar junction and may be an extremely
dilated anterior spinal artery.
No aneurysmal dilatation or focal stenosis of the bilateral
superficial temporal, facial or internal maxillary arteries.
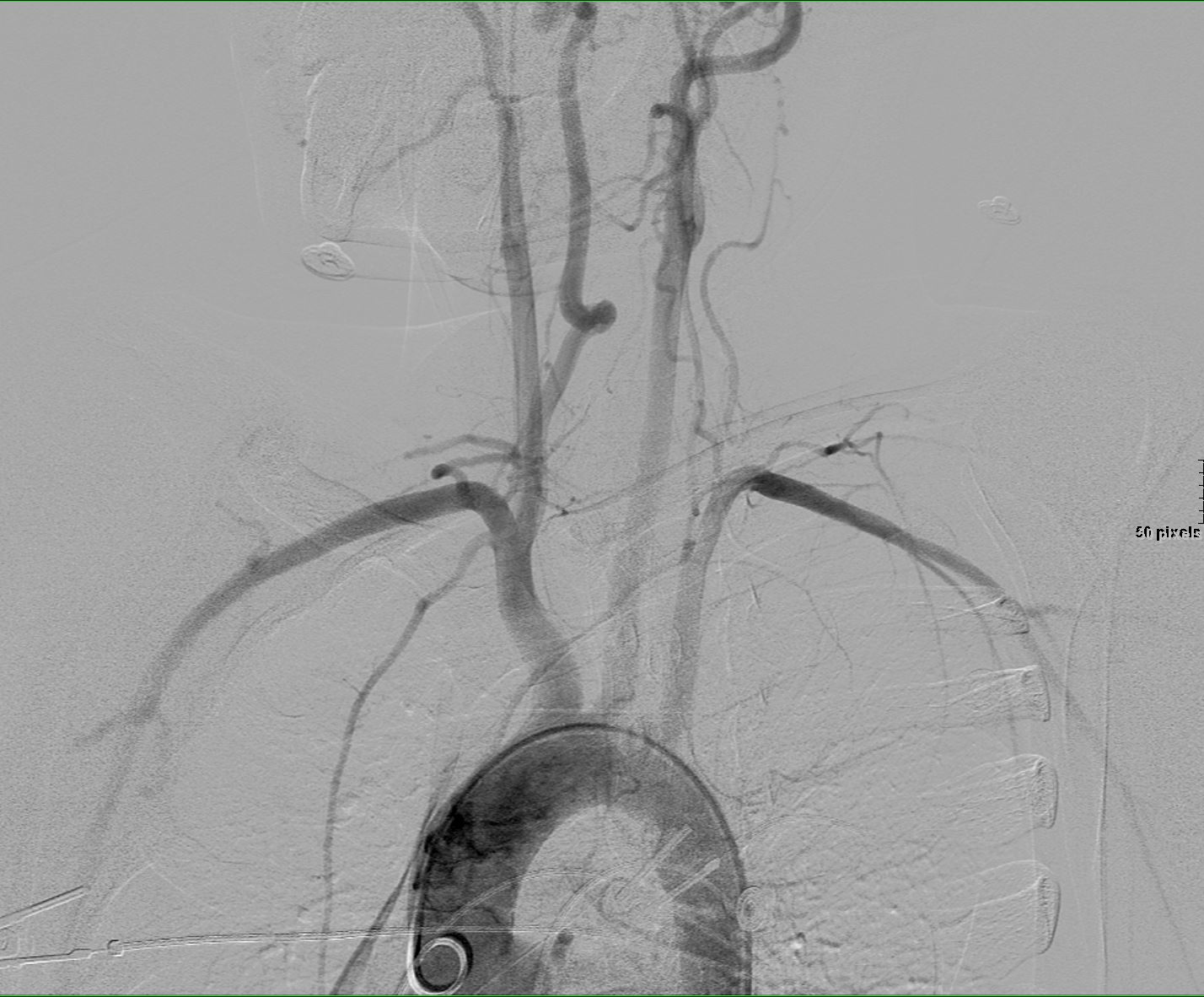
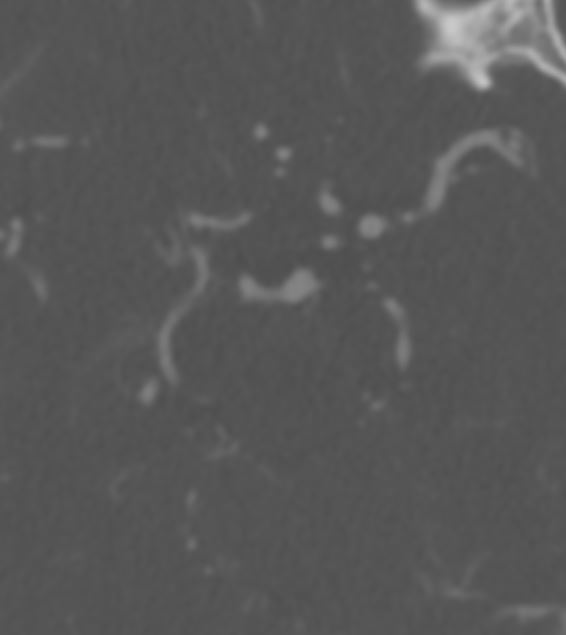
Intracranial internal carotid arteries are narrow proximally and
increase in caliber distally due to extensive collaterals as noted
above.
Lateral projecting 6 mm aneurysm arising from the cavernous portion of the left ICA is unchanged
Bilateral posterior communicating arteries are large, without
aneurysm in these locations.
There is an unchanged irregular contour of the proximal left MCA with
apparent fenestration (coronal views series 601b, image 53). The more distal segments of the left MCA, right MCA and ACAs are unchanged and relatively unremarkable. There is a fetal-type right PCA with a robust left posterior communicating artery. No significant stenosis or aneurysmal dilatation of the PCAs.
Intracranial vertebral and basilar arteries are unremarkable.
IMPRESSION:
No significant interval change in the findings consistent with
polyarteritis nodosa including:
1. Severe stenosis of the extracranial internal carotid arteries with
extensive external carotid collaterals.
2. Severe stenosis of the left vertebral artery with collaterals.
3. Multiple aneurysms, both extracranial and intracranial. There are
2 aneurysms of the extracranial right vertebral artery, 1 of the
extracranial left vertebral artery, and 1 arising from the
intracranial left internal carotid artery, as described above.
1 year ago




- There are several aetiologies for CAV; with
- Kawasaki?s disease,
- Takayasu’s arteritis,
- Polyarteritis Nodosa, and
- Giant-Cell Arteritis
- PAN
- PAN can also be associated with
- stenosis
- aneurysm
- occlusion
- dissection and
- rupture
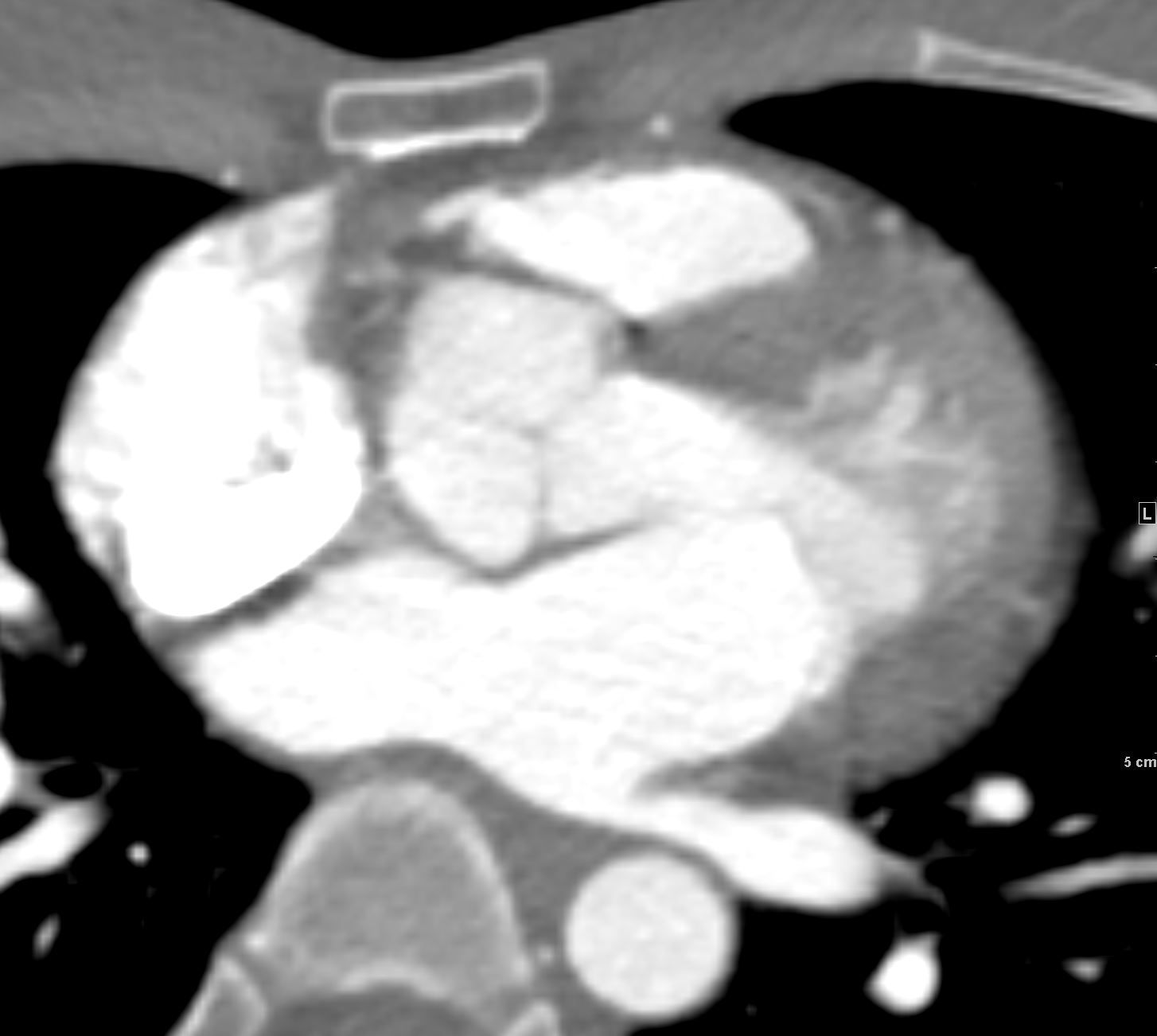
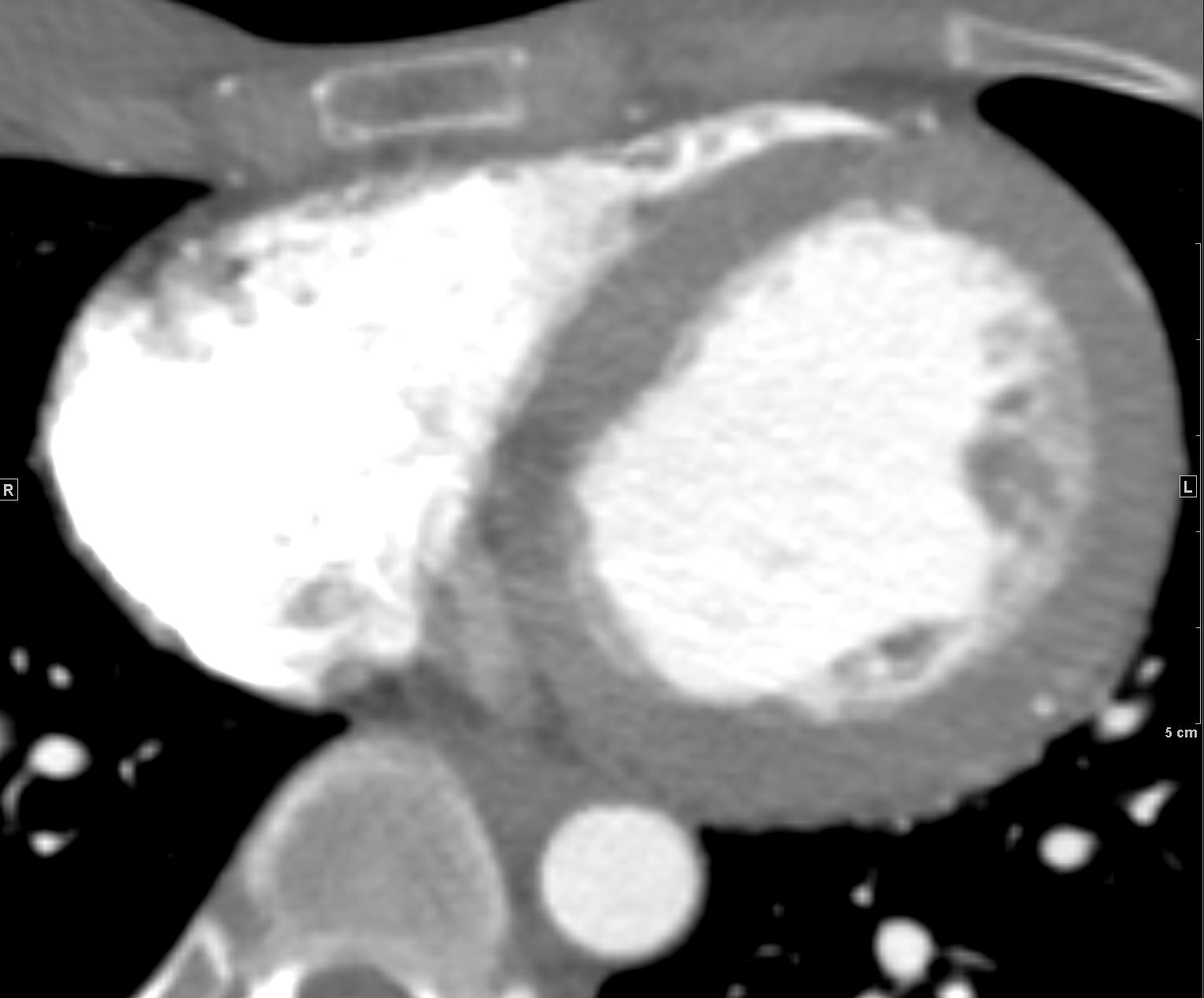
- premature
- atherosclerotic coronary disease
- usually asymptomatic
- most common cardiac clinical manifestation
- congestive heart failure
- caused by a combination of
- hypertension and
- silent myocardial ischemia
- most common cardiac clinical manifestation
- PAN can also be associated with





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
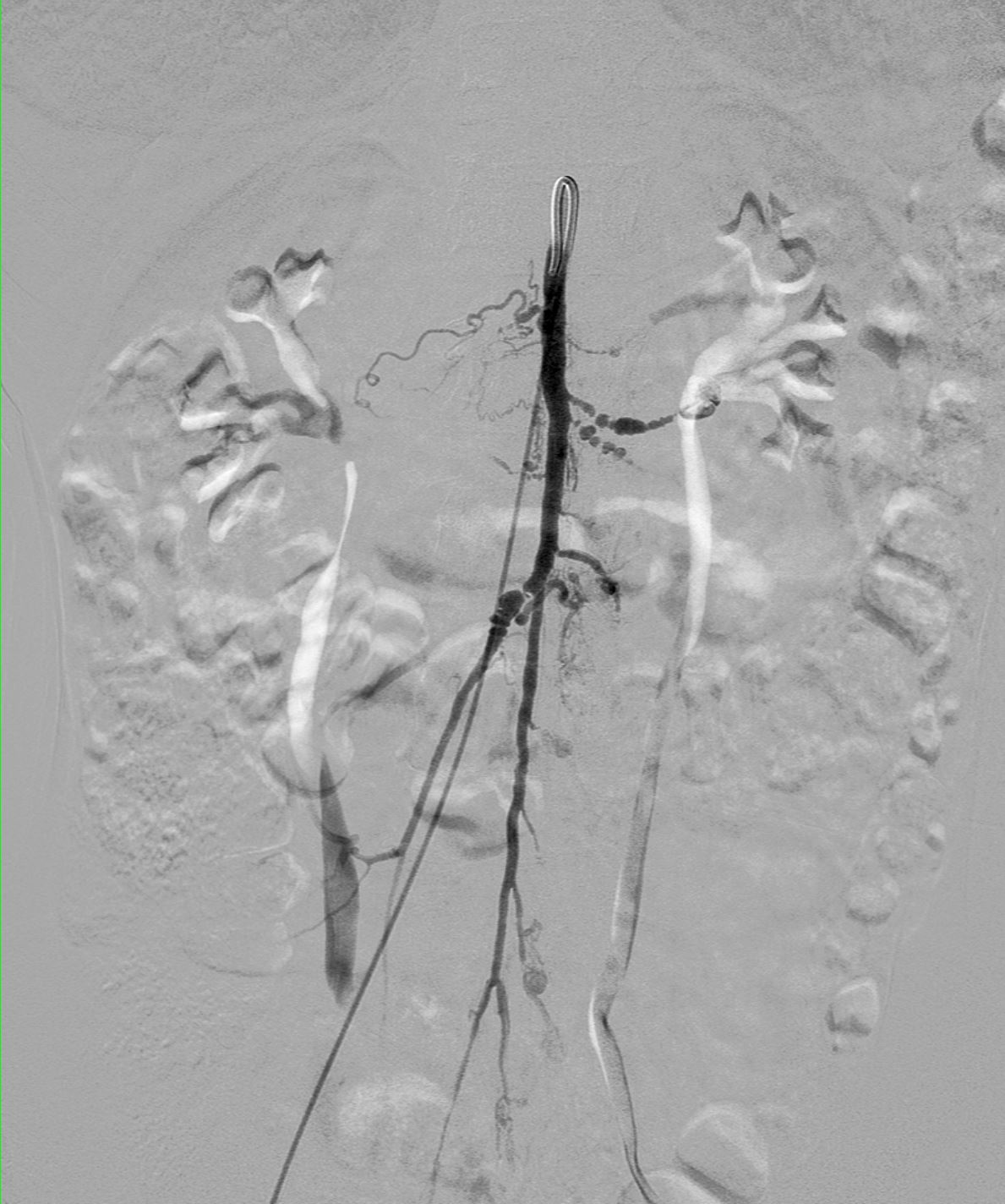
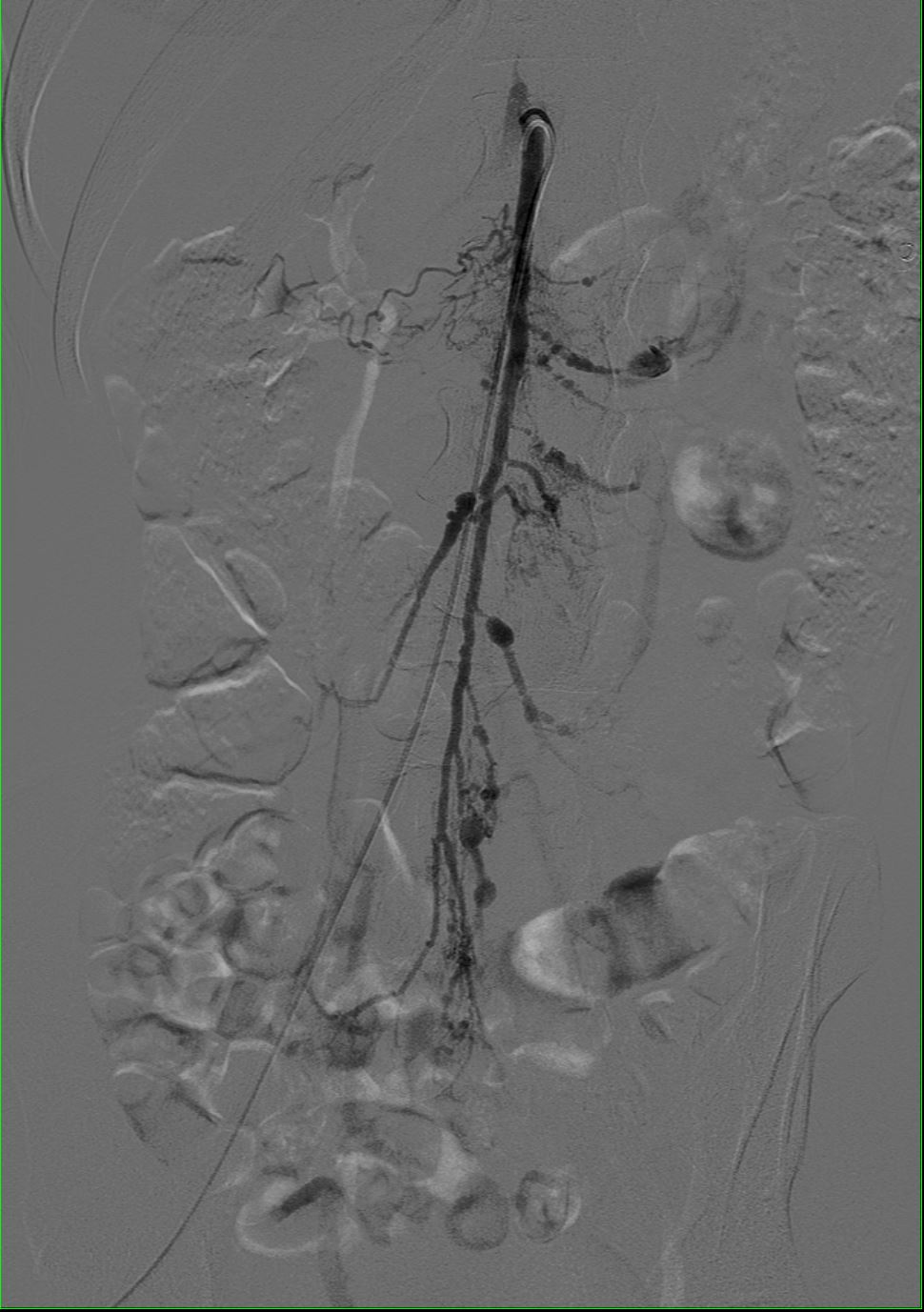
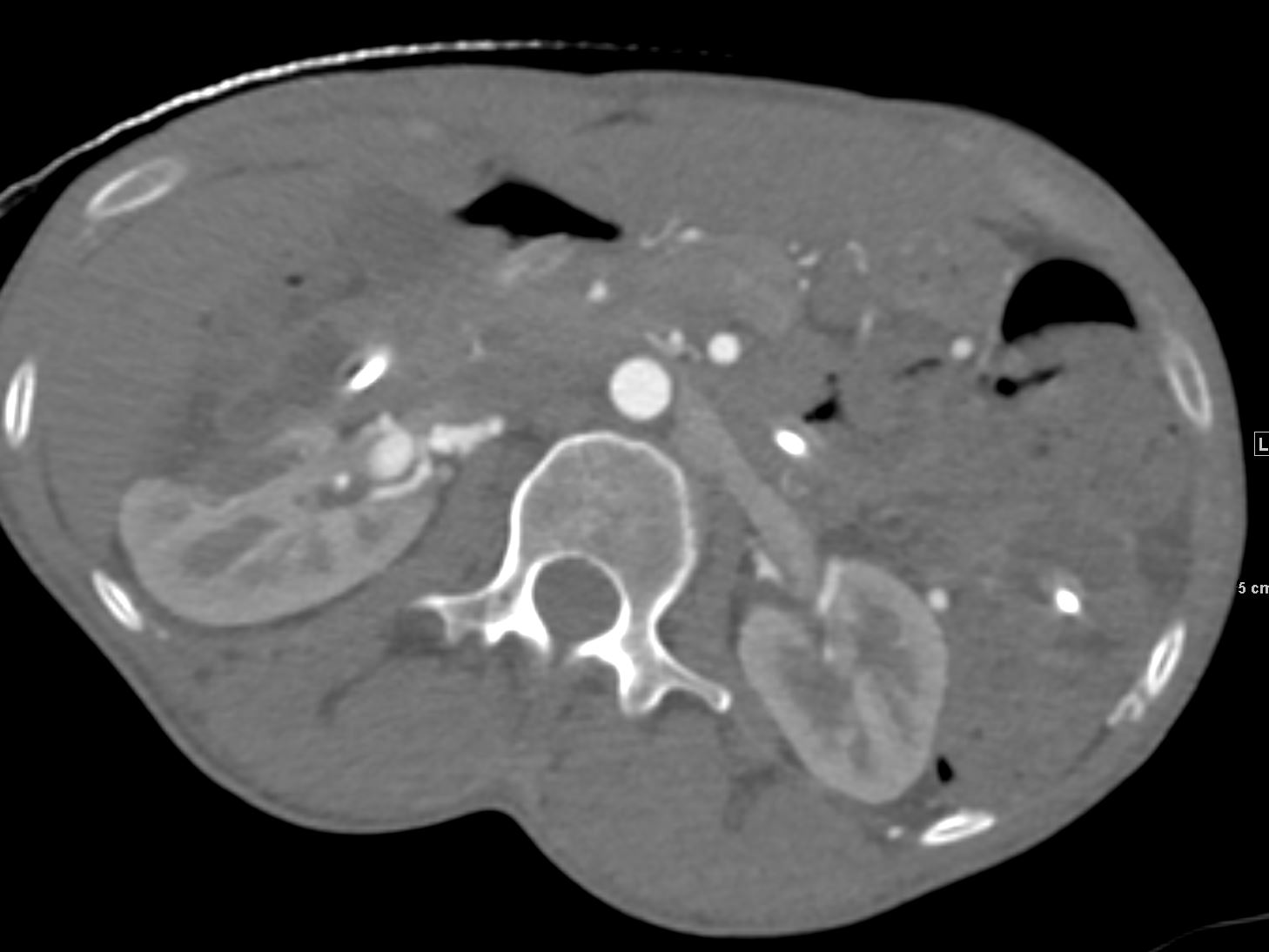
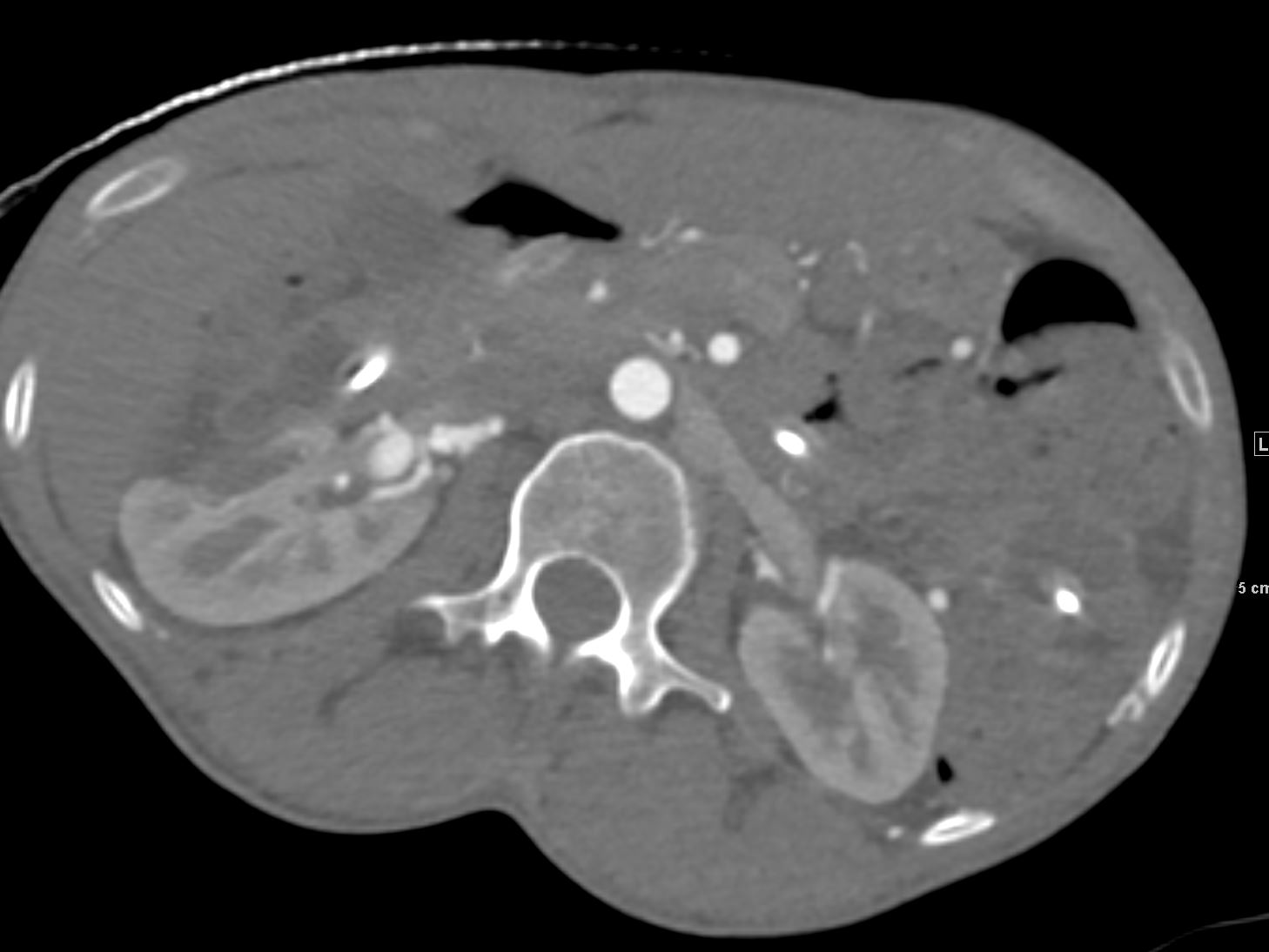
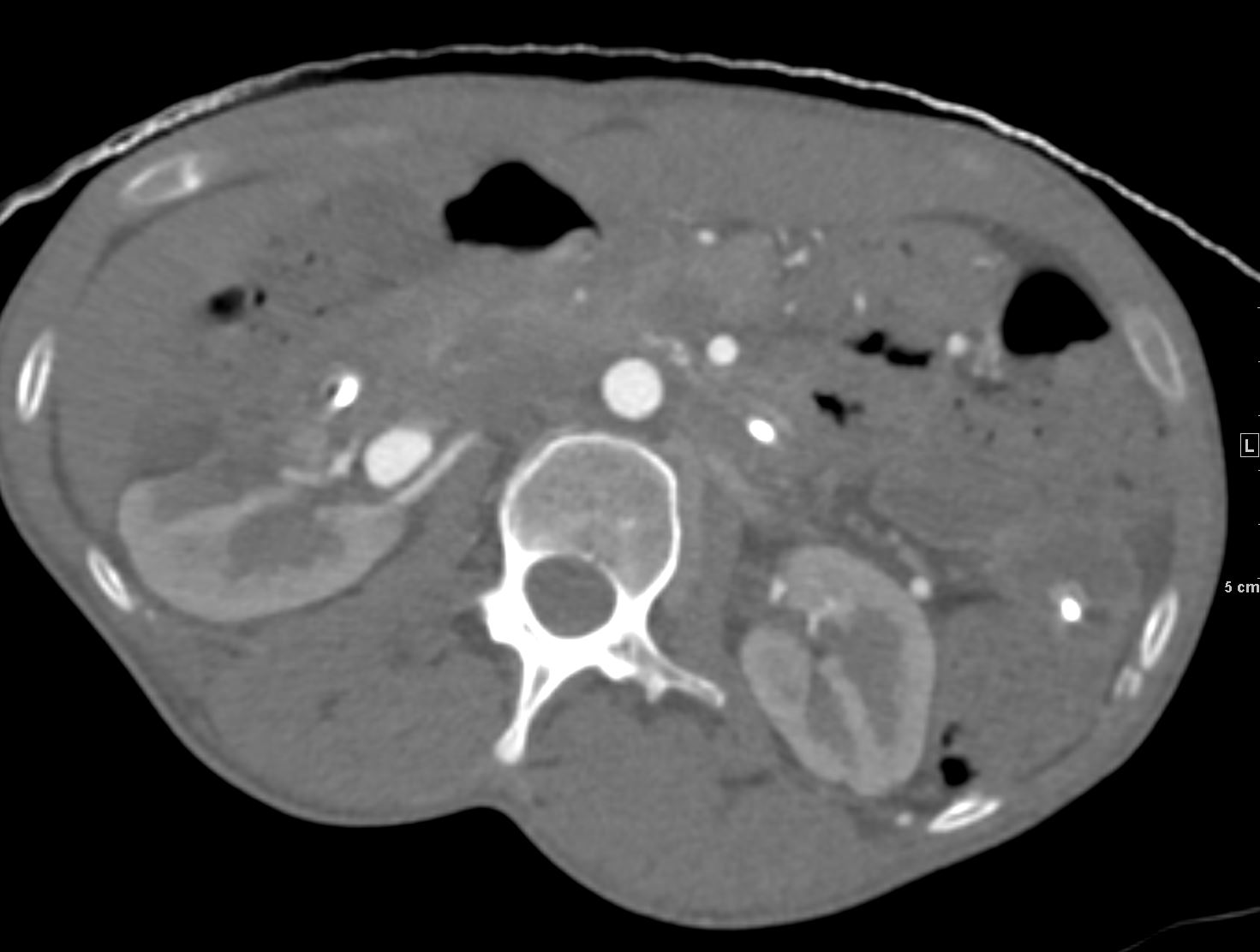
Vessels: No dissection. Again seen are numerous visceral artery aneurysms
which are unchanged in size
Some of the larger aneurysms included a celiac artery measuring 9 mm, splenic artery measuring 9 mm, the right renal artery measuring 10 mm. Additional smaller scattered aneurysms in the hepatic artery, the distal superior mesenteric
artery, the inferior mesenteric artery and its branches.