
- 75M
- PMH HTN, HLD, previous tobacco use COPD (previous exacerbations have required intubations), and chronic bronchiectasis, COVID-19 infection
- witnessed collapse with complaints of SOB,
- became unresponsive o
- found to be in VF arrest 2/2 inferior STEMI.
- 7 rounds epi, shocks; also given amio and lidocaine. Post-arrest ECG w/ STE in inferior leads, RBBB, and LAFB.
- cath lab,
- complete occlusion of the RCA, and stents were placed to proximal RCA.
- Right Dominant
Left Main: Normal
Left Anterior Descending: Appeared to be flush occluded at takeoff, no visible stump, not filling via collaterals.
Left Circ: Mild Luminal Irregularities less than 30%
RCA: Large ectatic vessel, difficult to enagage secondary to anterior and inferior take off. Extremely tortuous mid vessel. 70% proximal lesion. Totally occluded mid vessel.PROCEDURAL COMMENTS:
Pt had incessant VF in the ER requiring multiple shocks. EKG showed inferior ST elevations with IVCD. - TTE showed EF 60% with
- mild inferolateral wall hypokinesis and
- moderate inferior wall hypokinesis;
- RV systolic dysfunction was mildly reduced. T
Ashley DAvidoff
TheCommonVein.net
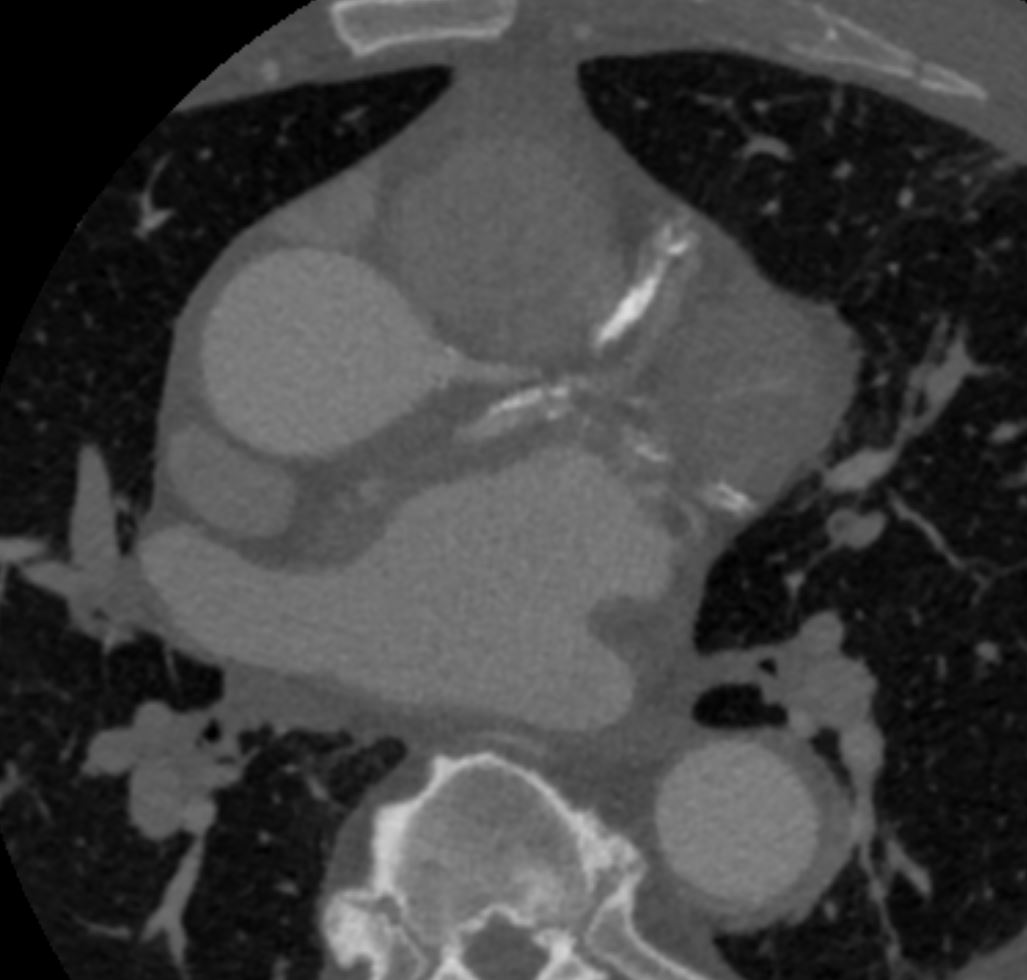
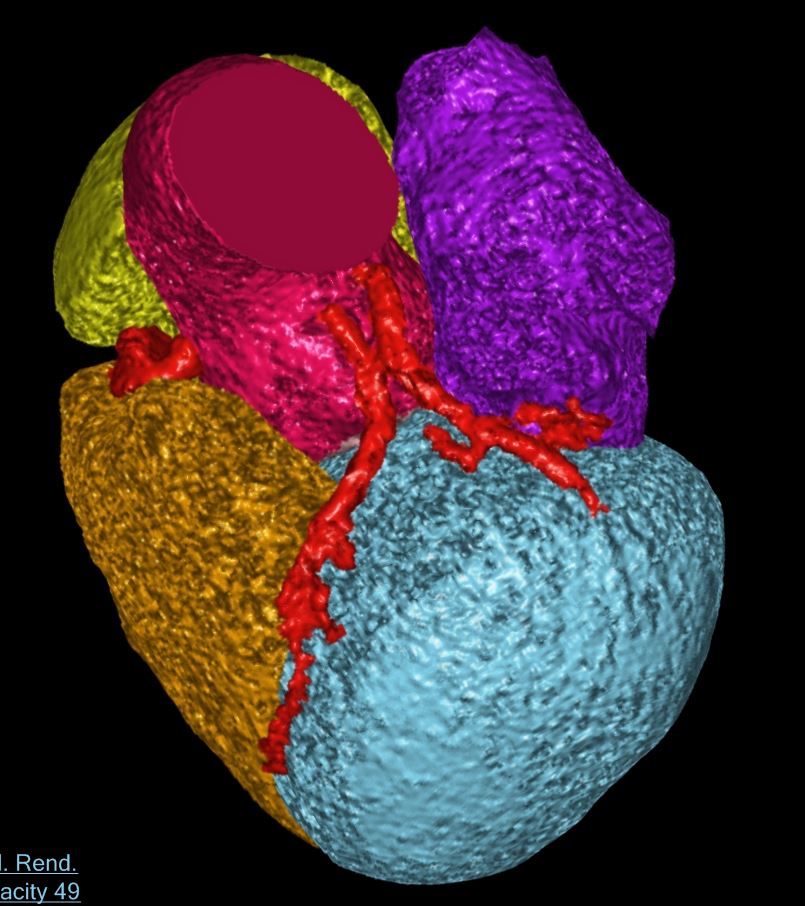
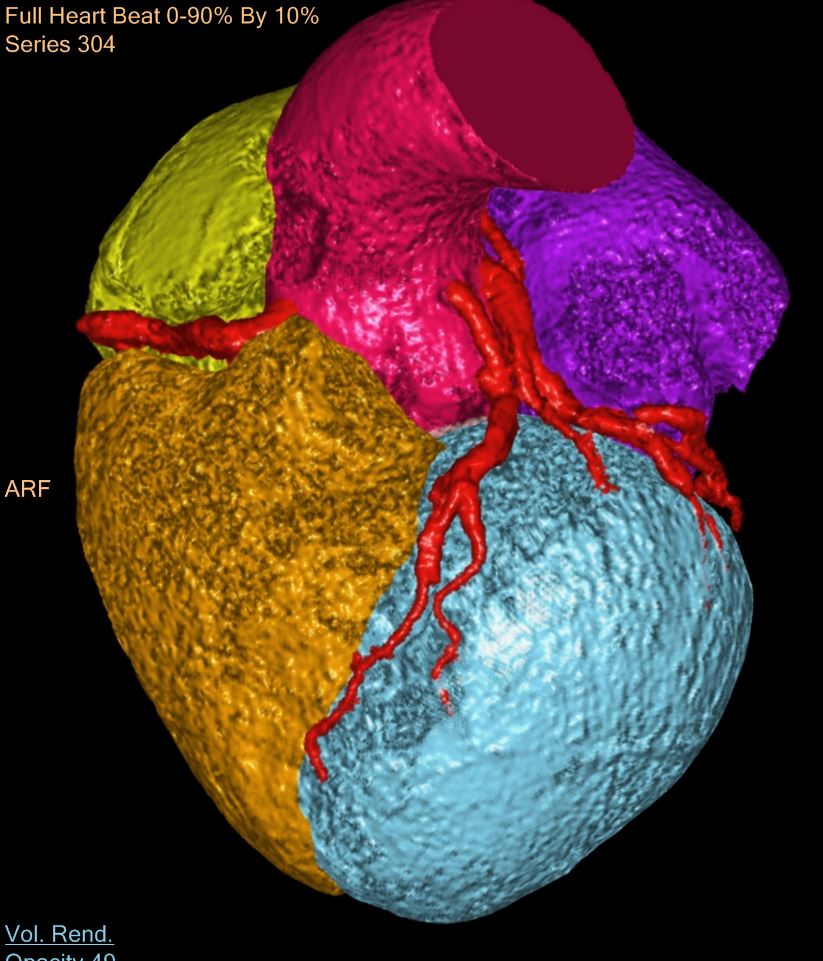
CTA coronaries
Ashley DAvidoff
TheCommonVein.net
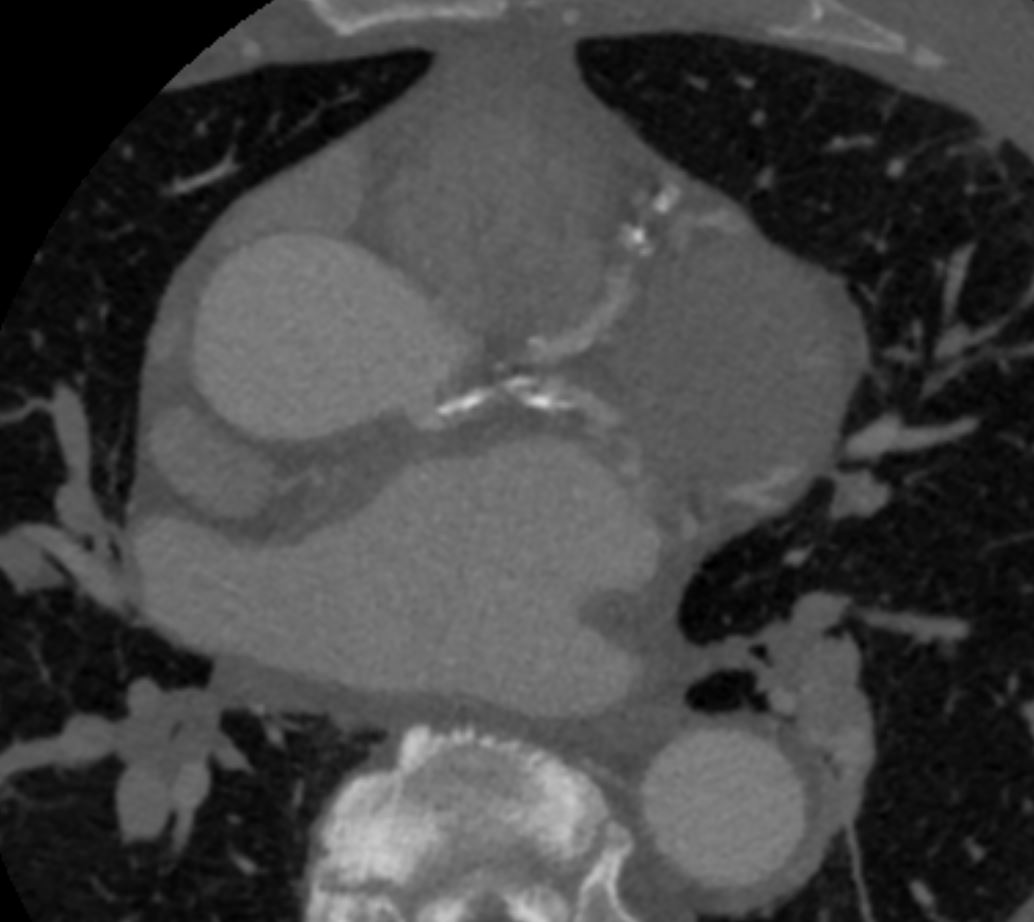
CTA coronaries
Ashley DAvidoff
TheCommonVein.net
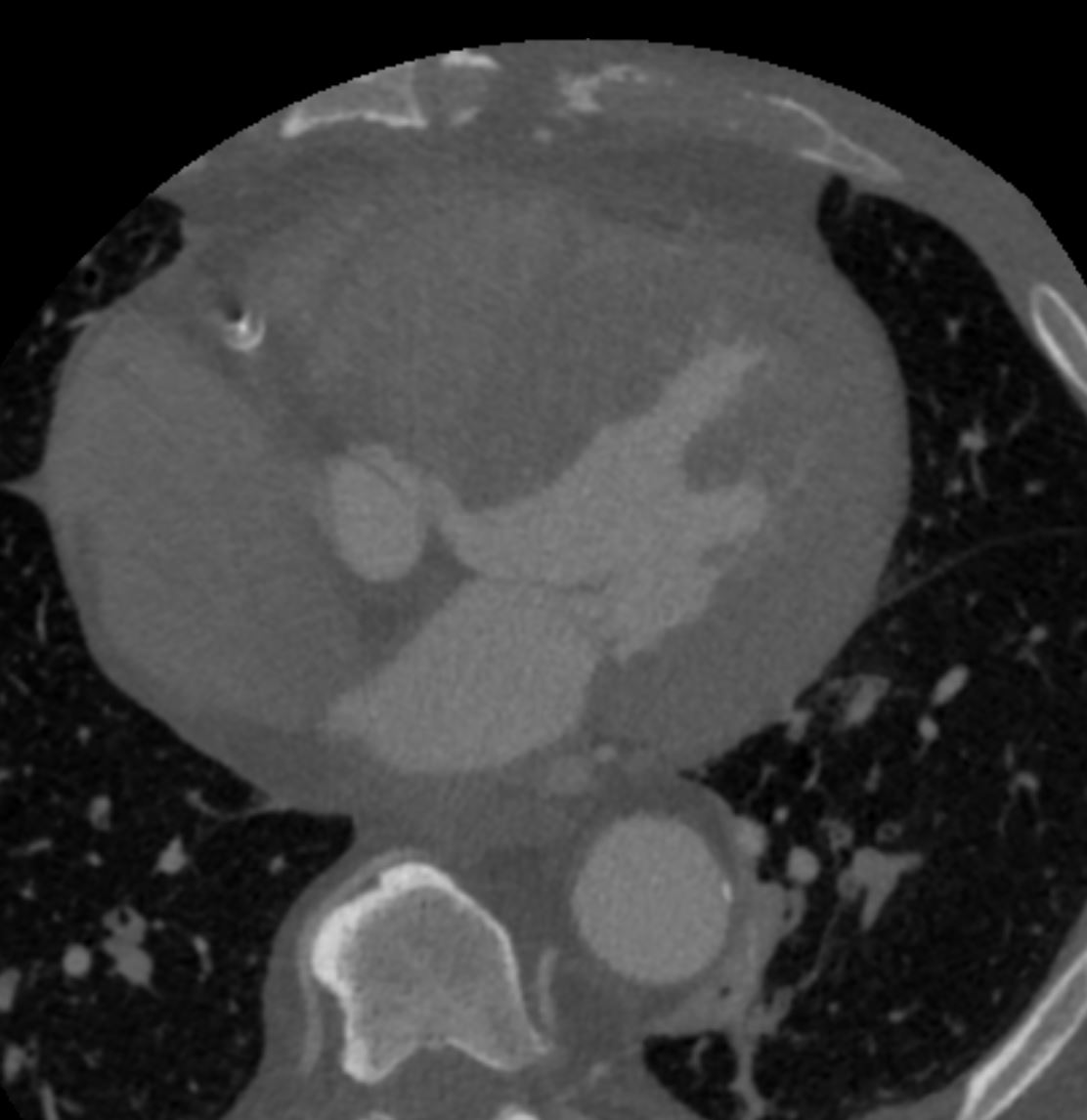
CTA coronaries
Ashley DAvidoff
TheCommonVein.net
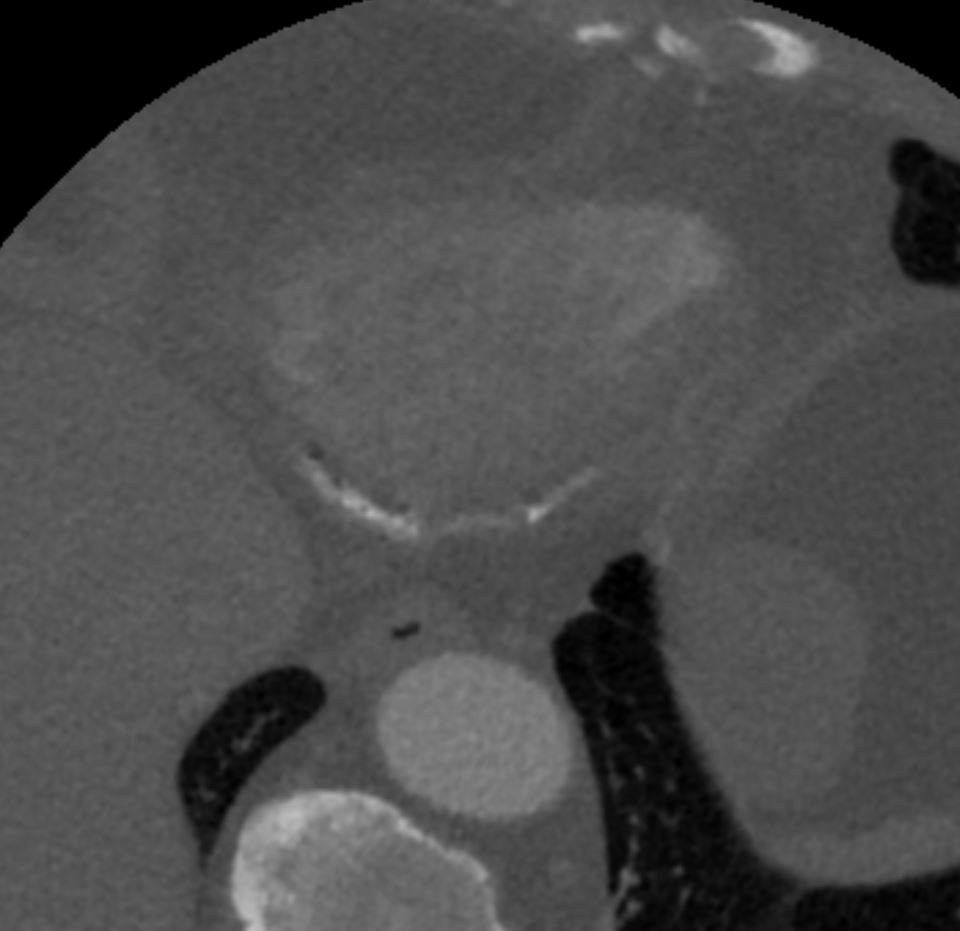
CTA coronaries
Ashley DAvidoff
TheCommonVein.net
CTA coronaries
Ashley DAvidoff
TheCommonVein.net
CTA coronaries
{kind=link}
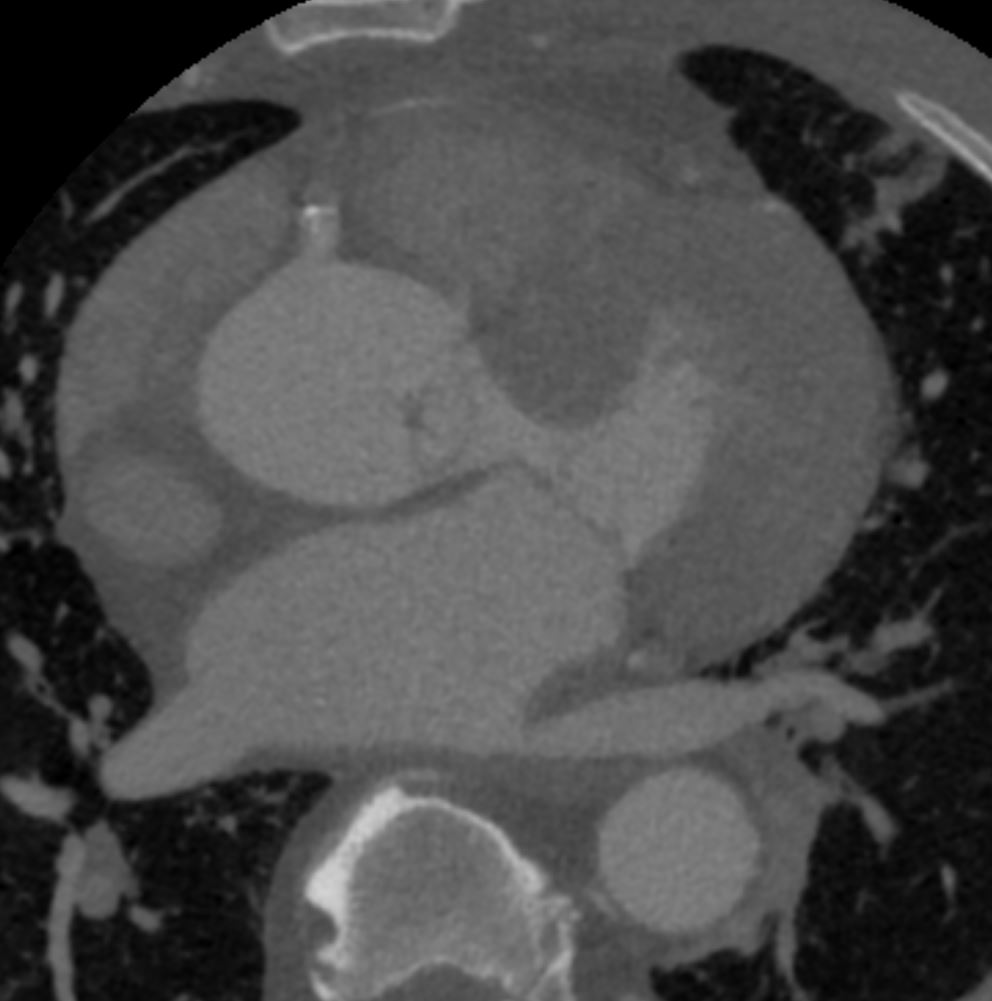
His LAD appeared to be ostially occluded on angiography; however, the anterior wall appeared to move well on echo. He underwent coronary CT angiogram to further evaluate, revealing “extensive calcified plaque in the LAD, RCA and left circumflex coronary arteries. I
-
-
- study extremely limited for evaluation of stenosis/luminal narrowing…
- LAD arises directly from the aortic root just above the sinus of Valsalva and has a sharp acute course at the origin between the aorta and main pulmonary artery.”
- Lcx arises separately from the left coronary cusp
- EF 50%
- study extremely limited for evaluation of stenosis/luminal narrowing…
-
DB136