
A 69 year old woman with hypertension and a smoking history was brought in by EMS for a syncopal episode. She was tachycardic to the 130s-160s, alert and oriented x 2, and had blood pressures of 99/73 in left arm, 130/79 in right on arrival. She was resuscitated

Ashley Davidoff MD
133882
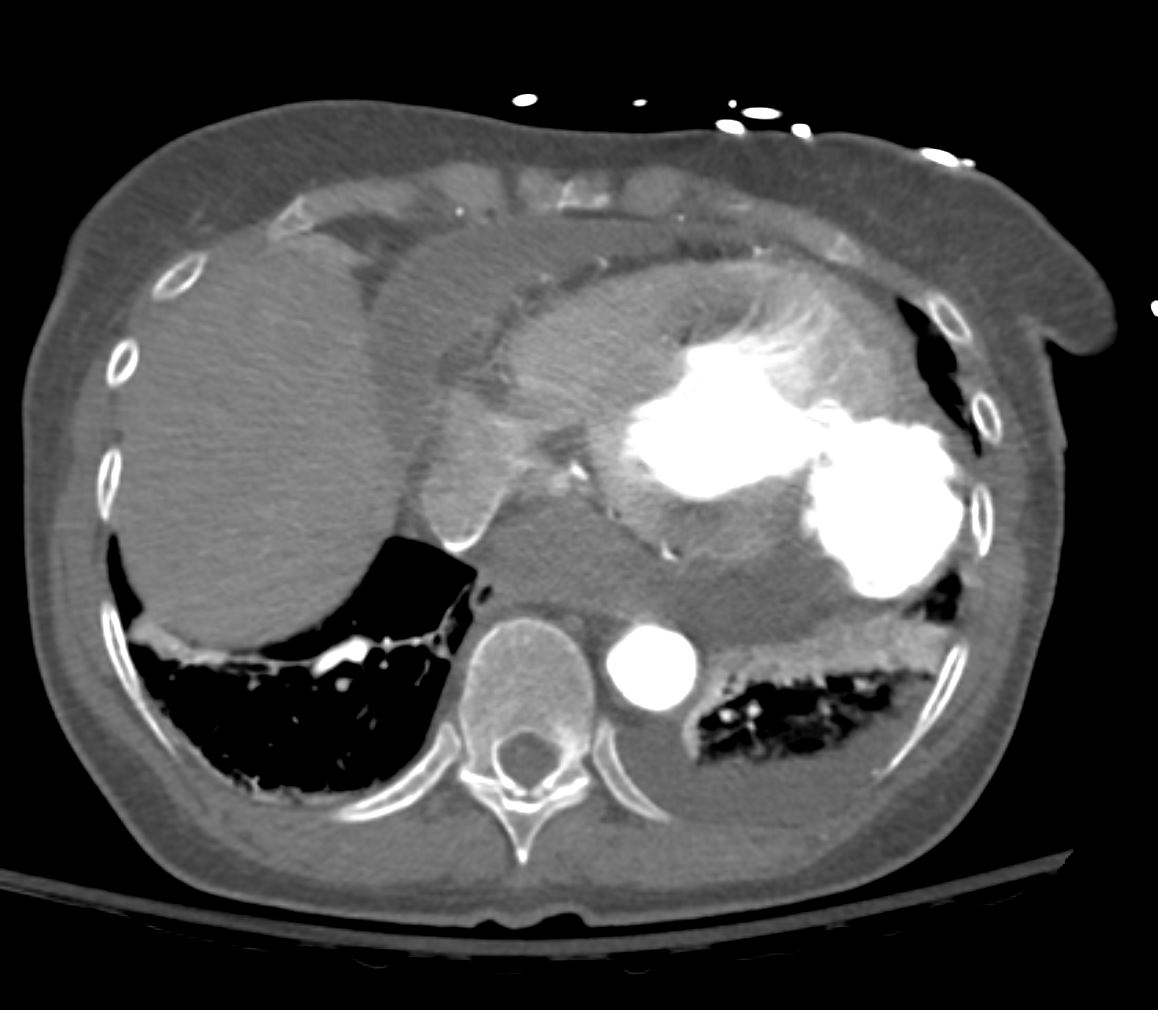
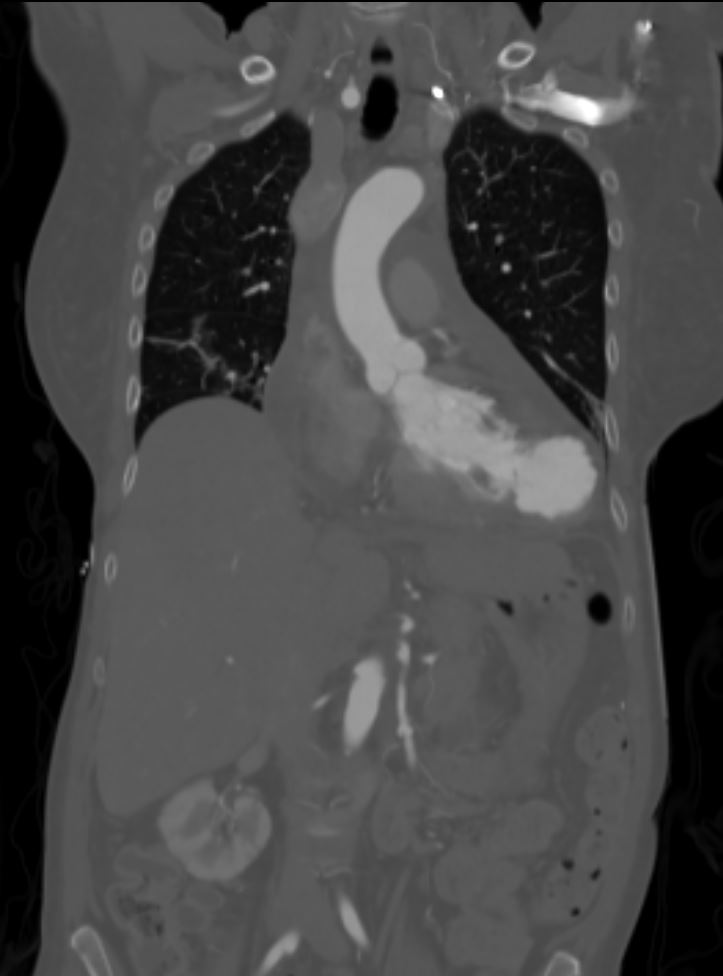
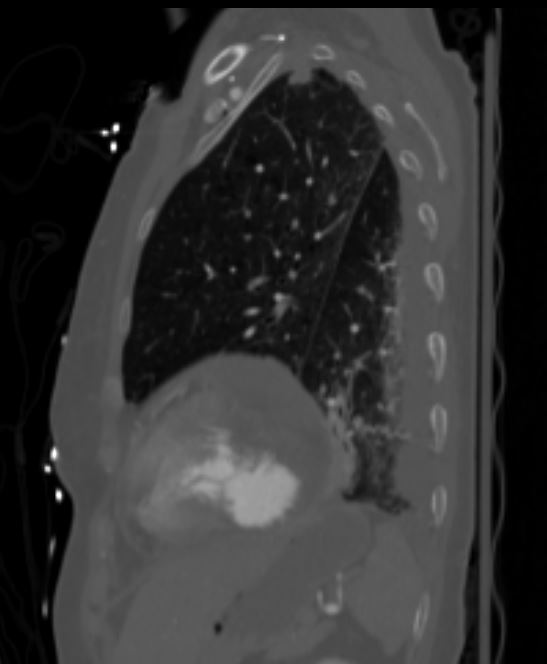
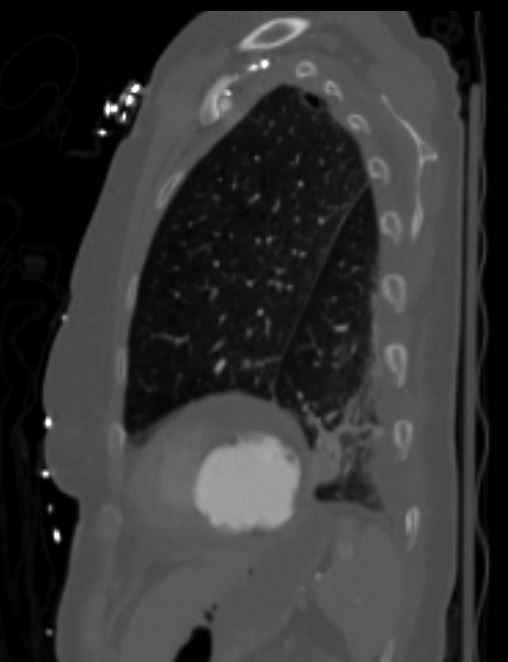
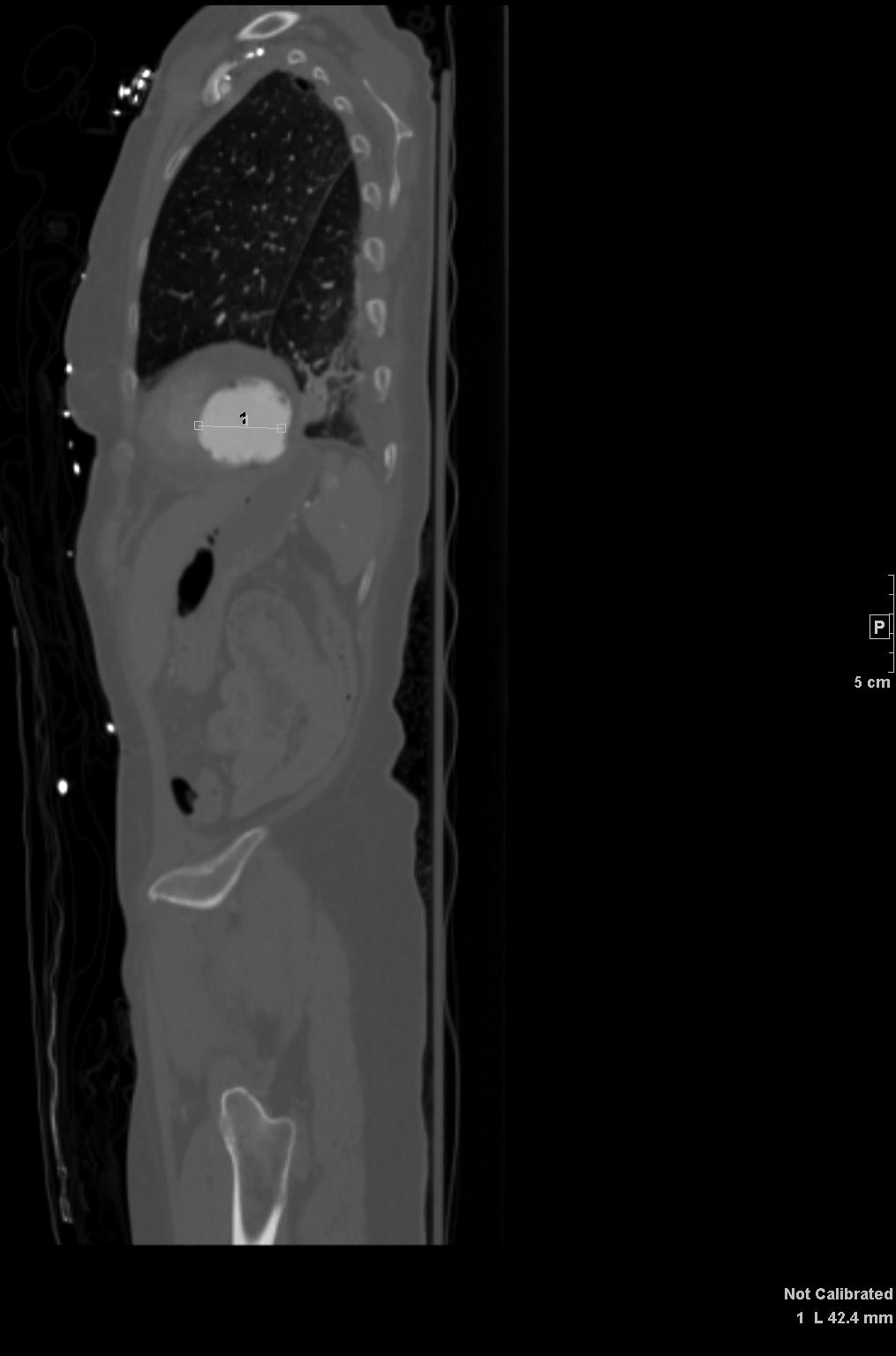
EKG findings included RBBB, left atrial enlargement, and a lateral infarct. Given her infarct on EKG, neck pain, blood pressure differential in her arms, and back pain, a CTA CAP was performed with an aortic dissection protocol for suspicion of aortic dissection. She also received a bedside echocardiogram.
EchoThe lateral wall of the left ventricle is akinetic with a large pseudoaneurysm/contained left ventricular wall rupture of the distal lateral wall?-?There is systolic flow into the contained rupture cavity size that measures at least 3 cm, through a narrow neck measuring ~1 cm connecting the LV cavity and pseudoaneurysm space?.-?Other regions of the LV are compensatorilyhyperkinetic with LVEF ~40-45%. LV cavityand RV are relatively small and may be underfilled.?-?There is a moderate sized circumferential pericardial effusion that is hyperechoic and suggestive of hemorrhage/ partly clotted blood in the pericardial space surrounding the heart?-?There is a focal large accumulation of dense pericardial effusion (likely clotted blood) measuring 2.1 cm that is compressing the RV free wall and impairing RV expansion.?-?IVC is dilated with reduced respirophasicvariation, the findings overall are suggestive of lateral wall cardiac rupture and impending tamponade physiology?























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Features of pseudoaneurysms?
- Ventricular pseudoaneurysms are
- ruptures that are contained within the pericardium,
- walled off by pericardium, and
- adhesions
- involve rupture of all 3 layers of the heart
- risk of rupture, up to 45% (1)?
- , they require immediate intervention
- most common artery f
- left circumflex artery.
- ruptures that are contained within the pericardium,