The Common Vein Copyright 2008
Definition
Barrett?s esophagus is an abnormal growth disorder of the gastroesophageal junction characterized by metaplastic change of the squamous epithelium into a glandular columnar epithelium caused by longstanding gastroesophageal reflux. With this change there may be resulting alteration in the DNA rendering the entity a premalignant condition.
The clinical presentation is non specific and include the dyspeptic symptoms of GERD . The diagnosis is made by endoscopy, where the extension of the gastric mucosa into the squamous territory is seen as cracks of salmon colored areas in the white esophageal mucosa. Biopsies need to be taken to evaluate for dysplasia. In the absence of dysplasia treatment includes ongoing surveillance, with aggressive medical treatment of the GERD. In the presence of dysplasia removal of the dysplastic abnormalities is indicated. A variety of endoscopic ablative therapies and surgical options are available.
Normal Regular “Z” line (left) and and Barrett’s Esophagus (right)
|
| 73474 squamocolumnar junction gastroesophageal junction squamous epithelium gastric epithelium columnar epithelium normal Z line anatomy histology endoscopy endoscope Courtesy Joshua Namias MD
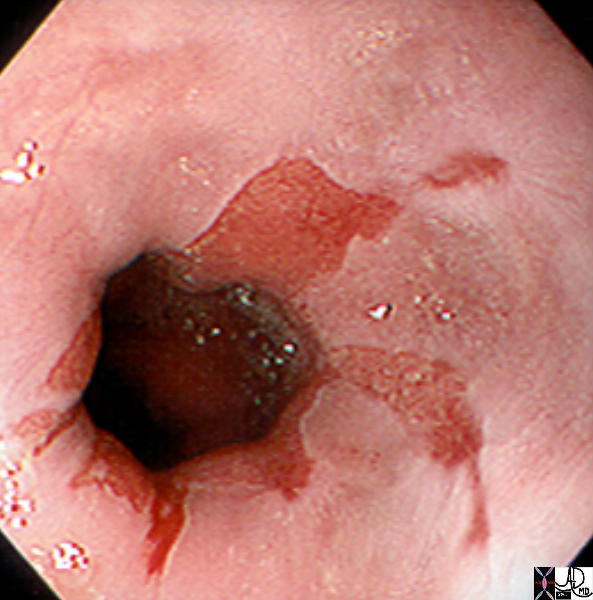
73475 squamocolumnar junction gastroesophageal junction squamous epithelium gastric epithelium columnar epithelium Extension of columnar epithelium toward the squamous epithelium space occupation Barrett’s esophagus endoscopy endoscope Courtesy Joshua Namias MD |

Barretts Esophagus
12254 Gross specimen showing Barrett’s mucosa. The lighter white portion is normal esophageal squamous epithelium, and the tan-brown area is abnormal. This is where the normal squamous epithelium has been replaced by metaplastic columnar epithelium, comprising Barrett’s esophagus. Courtesy Barbara Banner MD |
 Barretts Esophagus Barretts Esophagus |
|
12255 Microscopic section at low power showing Barrett’s mucosa. Note that a glandular type of mucosa is present overlying the cluster of esophageal glands. This tells us that where there ought to be squamous epithelium, there is now columnar metaplasia, and this is the definition of Barrett’s esophagus. histopathology Courtesy Barbara Banner MD |
Causes and Predisposing Factors
Barrett?s is a sequela of longstanding reflux. The mean age of diagnosis is 55, although can be seen earlier with rare cases reported in the pediatric population. The male to female ratio is 2 to 1 with a higher incidence in the white and Hispanic population. It is less frequently seen in the black and asian population.
With the continuous injury from acid, the esophagus attempts to protect itself by changing to the more acid resistant intestinal type mucosa. However, with this transformation, there is DNA alteration and malignant changes can occur.
Result
The specialized intestinal metaplasia is glandular mucosa with mucin-type cells and abundant goblet cells.
The risk of Barrett?s Esophagus is the conversion to carcinoma. This conversion can be thought of as a stepwise process.
GERD-à Erosive Esophagitisà Specialized Intestinal Metaplasiaà Low Grade Dysplasiaà High Grade Dysplasiaà Carcinoma
Esophageal carcinoma has increased 300% since the 1970s. There are many reasons for this but clearly detection by endoscopic procedure and routine surveillance for Barrett?s plays a large role.
Diagnosis
Barrett?s Esophagus is a endoscopic and histopathologic diagnosis. Upon endoscopic visualization of the GE junction, one can appreciate a regular appearing ?Z? line. Again, this is the area of change from squamous esophageal mucosa to gastric type mucosa.
With Barrett?s, however, there is an irregularity of this line with finger like projections starting at the transition point and traversing more proximally. This salmon colored tissue is the specialized intestinal metaplasia.
  Barrett’s Esophagus Barrett’s Esophagus |
| 01235c03 01235 by endoscopy Barret’s Courtesy Ashley Davidoff MD code esophagus epiphrenic ampulla hiatus hernia esophagitis barium swallow upper GI UGI imaging radiology contrast X-Ray |
This finding is not uncommonly seen and it has been estimated that 1/100 ?routine? EGDs will demonstrate Barrett?s, while those done for ?reflux? will show a incidence of approximately 1/10.
Barrett?s itself does not have associated symptoms. Instead, patients are often symptomatic from the underlying reflux. There are cases where the first presenting symptom is dysphagia or odynophagia and endoscopy reveals Barrett?s and esophageal carcinoma. Autopsy studies have shown Barrett?s to be present in 1/57-1/105 cases.
Biopsies should be taken at the initial finding of Barrett?s. The biopsies are taken from 4 quadrants and in 1cm intervals. It is extremely important to have patients with no evidence of dysplasia to undergo surveillance endoscopies. After Barrett?s is found endoscopy should be performed annually for 2 years and the every three if no dysplasia is found.
Those patients who have progressed to dysplasia must consider further therapies. Regardless of the modality chosen (described below) annual endoscopies are required.
 Barret’s Esophagus by Endoscopy No Specific Findings Barret’s Esophagus by Endoscopy No Specific Findings
Suspect in the Setting of Peptic Esohagitis and its Sequelae |
| This series of images of the esophagus from a double contrast barium swallow shows a focal irregular stricture at the GE junction (a) associated with a hiatus hernia. (d,e,f). The irregularity suggest ongoing esophagitis but Barrett’s esophagus has to be considered. The patient complained of cervical dysphagia. A 13mm barium pill was held up at the junction implying a significant narrowing. The stricture seen in d,e,f has a concentric ring like appearance reminiscent of a Schatki’s ring.
Courtesy Ashley Davidoff MD 38421c02 code esophagus stricture narrowing irregular HH Schatzki’s ring barium pill |
Treatment
Strict acid suppression is key, but it should be noted that regression of Barrett?s is not thought to be possible. Instead, the acid suppression is thought to reduce the ongoing acid exposure and damage to the wall.
There are four main therapeutic options in patients with Barrett?s.
Endscopic Ablative Therapies include Multipolar Electrocoagulation (MPEC) which is heat induced damage to the Barrett?s mucosa. It is reserved for non-dysplastic cases. It carries a risk of perforation, stricture formation, and residual Barrett?s can be found in upto 28% of cases.
Argon Plasma Coagulation is another endoscopic modality that uses ionized electronically charged gas, again to burn the mucosa. Strictures can form in upto 10%.
Photodynamic therapy involves giving systemic administration of a photo-sensitizing agent and the endoscopic to laser light that causes and oxidative damage to the mucosa.
Endoscopic Mucosal Resection consists of an upper endoscopy with the removal of the esophageal mucosa.
Surgical esophagectomy is a invasive approach but one that completely removes the Barrett?s and the possible conversion to cancer. However, clearly, complications and post-surgical morbidity is higher. Patients can develop dysphagia, weight loss, dumping syndrome, in addition to the surgical complications.
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Barret’s Esophagus by Endoscopy No Specific Findings
Suspect in the Setting of Peptic Esohagitis and its Sequelae
This series of images of the esophagus from a double contrast barium swallow shows a focal irregular stricture at the GE junction (a) associated with a hiatus hernia. (d,e,f). The irregularity suggest ongoing esophagitis but Barrett’s esophagus has to be considered. The patient complained of cervical dysphagia. A 13mm barium pill was held up at the junction implying a significant narrowing. The stricture seen in d,e,f has a concentric ring like appearance reminiscent of a Schatki’s ring.
Courtesy Ashley Davidoff MD 38421c02 code esophagus stricture narrowing irregular HH Schatzki’s ring barium pill
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Barret’s Esophagus by Endoscopy No Specific Findings
Suspect in the Setting of Peptic Esohagitis and its Sequelae
This series of images of the esophagus from a double contrast barium swallow shows a focal irregular stricture at the GE junction (a) associated with a hiatus hernia. (d,e,f). The irregularity suggest ongoing esophagitis but Barrett’s esophagus has to be considered. The patient complained of cervical dysphagia. A 13mm barium pill was held up at the junction implying a significant narrowing. The stricture seen in d,e,f has a concentric ring like appearance reminiscent of a Schatki’s ring.
Courtesy Ashley Davidoff MD 38421c02 code esophagus stricture narrowing irregular HH Schatzki’s ring barium pill
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This series of images of the esophagus from a double contrast barium swallow shows a focal irregular stricture at the GE junction (a) associated with a hiatus hernia. (d,e,f). The irregularity suggest ongoing esophagitis but Barrett’s esophagus has to be considered. The patient complained of cervical dysphagia. A 13mm barium pill was held up at the junction implying a significant narrowing. The stricture seen in d,e,f has a concentric ring like appearance reminiscent of a Schatki’s ring.
Courtesy Ashley Davidoff MD 38421c02 code esophagus stricture narrowing irregular HH Schatzki’s ring barium pill
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This series of images of the esophagus from a double contrast barium swallow shows a focal irregular stricture at the GE junction (a) associated with a hiatus hernia. (d,e,f). The irregularity suggest ongoing esophagitis but Barrett’s esophagus has to be considered. The patient complained of cervical dysphagia. A 13mm barium pill was held up at the junction implying a significant narrowing. The stricture seen in d,e,f has a concentric ring like appearance reminiscent of a Schatki’s ring.
Courtesy Ashley Davidoff MD 38421c02 code esophagus stricture narrowing irregular HH Schatzki’s ring barium pill
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Barret’s Esophagus by Endoscopy No Specific Findings
Suspect in the Setting of Peptic Esohagitis and its Sequelae
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Barret’s Esophagus by Endoscopy No Specific Findings
Suspect in the Setting of Peptic Esohagitis and its Sequelae
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Barrett’s Esophagus
01235c03 01235 by endoscopy Barret’s Courtesy Ashley Davidoff MD code esophagus epiphrenic ampulla hiatus hernia esophagitis barium swallow upper GI UGI imaging radiology contrast X-Ray
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Barrett’s Esophagus
01235c03 01235 by endoscopy Barret’s Courtesy Ashley Davidoff MD code esophagus epiphrenic ampulla hiatus hernia esophagitis barium swallow upper GI UGI imaging radiology contrast X-Ray
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 01235c03 01235 by endoscopy Barret’s Courtesy Ashley Davidoff MD code esophagus epiphrenic ampulla hiatus hernia esophagitis barium swallow upper GI UGI imaging radiology contrast X-Ray
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 01235c03 01235 by endoscopy Barret’s Courtesy Ashley Davidoff MD code esophagus epiphrenic ampulla hiatus hernia esophagitis barium swallow upper GI UGI imaging radiology contrast X-Ray
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Barrett’s Esophagus
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Barrett’s Esophagus
)
https://beta.thecommonvein.net/wp-content/uploads/2023/04/01235c03.jpg https://beta.thecommonvein.net/wp-content/uploads/2023/04/01235.jpg
http://thecommonvein.net/media/01235c03.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Barretts Esophagus
12255 Microscopic section at low power showing Barrett’s mucosa. Note that a glandular type of mucosa is present overlying the cluster of esophageal glands. This tells us that where there ought to be squamous epithelium, there is now columnar metaplasia, and this is the definition of Barrett’s esophagus. histopathology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Barretts Esophagus
12255 Microscopic section at low power showing Barrett’s mucosa. Note that a glandular type of mucosa is present overlying the cluster of esophageal glands. This tells us that where there ought to be squamous epithelium, there is now columnar metaplasia, and this is the definition of Barrett’s esophagus. histopathology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
12255 Microscopic section at low power showing Barrett’s mucosa. Note that a glandular type of mucosa is present overlying the cluster of esophageal glands. This tells us that where there ought to be squamous epithelium, there is now columnar metaplasia, and this is the definition of Barrett’s esophagus. histopathology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
12255 Microscopic section at low power showing Barrett’s mucosa. Note that a glandular type of mucosa is present overlying the cluster of esophageal glands. This tells us that where there ought to be squamous epithelium, there is now columnar metaplasia, and this is the definition of Barrett’s esophagus. histopathology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Barretts Esophagus
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Barretts Esophagus
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Barretts Esophagus
12254 Gross specimen showing Barrett’s mucosa. The lighter white portion is normal esophageal squamous epithelium, and the tan-brown area is abnormal. This is where the normal squamous epithelium has been replaced by metaplastic columnar epithelium, comprising Barrett’s esophagus. Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Barretts Esophagus
12254 Gross specimen showing Barrett’s mucosa. The lighter white portion is normal esophageal squamous epithelium, and the tan-brown area is abnormal. This is where the normal squamous epithelium has been replaced by metaplastic columnar epithelium, comprising Barrett’s esophagus. Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Barretts Esophagus
12254 Gross specimen showing Barrett’s mucosa. The lighter white portion is normal esophageal squamous epithelium, and the tan-brown area is abnormal. This is where the normal squamous epithelium has been replaced by metaplastic columnar epithelium, comprising Barrett’s esophagus. Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Barretts Esophagus
12254 Gross specimen showing Barrett’s mucosa. The lighter white portion is normal esophageal squamous epithelium, and the tan-brown area is abnormal. This is where the normal squamous epithelium has been replaced by metaplastic columnar epithelium, comprising Barrett’s esophagus. Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal Regular “Z” line (left) and and Barrett’s Esophagus (right)
73474 squamocolumnar junction gastroesophageal junction squamous epithelium gastric epithelium columnar epithelium normal Z line anatomy histology endoscopy endoscope Courtesy Joshua Namias MD
73475 squamocolumnar junction gastroesophageal junction squamous epithelium gastric epithelium columnar epithelium Extension of columnar epithelium toward the squamous epithelium space occupation Barrett’s esophagus endoscopy endoscope Courtesy Joshua Namias MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal Regular “Z” line (left) and and Barrett’s Esophagus (right)
73474 squamocolumnar junction gastroesophageal junction squamous epithelium gastric epithelium columnar epithelium normal Z line anatomy histology endoscopy endoscope Courtesy Joshua Namias MD
73475 squamocolumnar junction gastroesophageal junction squamous epithelium gastric epithelium columnar epithelium Extension of columnar epithelium toward the squamous epithelium space occupation Barrett’s esophagus endoscopy endoscope Courtesy Joshua Namias MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 73474 squamocolumnar junction gastroesophageal junction squamous epithelium gastric epithelium columnar epithelium normal Z line anatomy histology endoscopy endoscope Courtesy Joshua Namias MD
73475 squamocolumnar junction gastroesophageal junction squamous epithelium gastric epithelium columnar epithelium Extension of columnar epithelium toward the squamous epithelium space occupation Barrett’s esophagus endoscopy endoscope Courtesy Joshua Namias MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 73474 squamocolumnar junction gastroesophageal junction squamous epithelium gastric epithelium columnar epithelium normal Z line anatomy histology endoscopy endoscope Courtesy Joshua Namias MD
73475 squamocolumnar junction gastroesophageal junction squamous epithelium gastric epithelium columnar epithelium Extension of columnar epithelium toward the squamous epithelium space occupation Barrett’s esophagus endoscopy endoscope Courtesy Joshua Namias MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal Regular “Z” line (left) and and Barrett’s Esophagus (right)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal Regular “Z” line (left) and and Barrett’s Esophagus (right)
)
