
This page represents fat in the LV – All comers
There is a separate page for post MI fat
POST MI FAT
Lipomatous Metaplasia
- Post MI,
- myofibroblasts produce collagen as a repair mechanism
- Sometimes myofibroblasts
- differentiate into adipocytes,
- which is laid down in the scar
- Consequence of myocardial infarction.
- At autopsy
- Lipomatous Metaplasia
- was seen in about 70% of scars associated with
- chronic ischemic heart disease
- Lipomatous Metaplasia is also
- a significant predictor
- heart failure,
- all-cause mortality,
- sustained ventricular arrhythmia
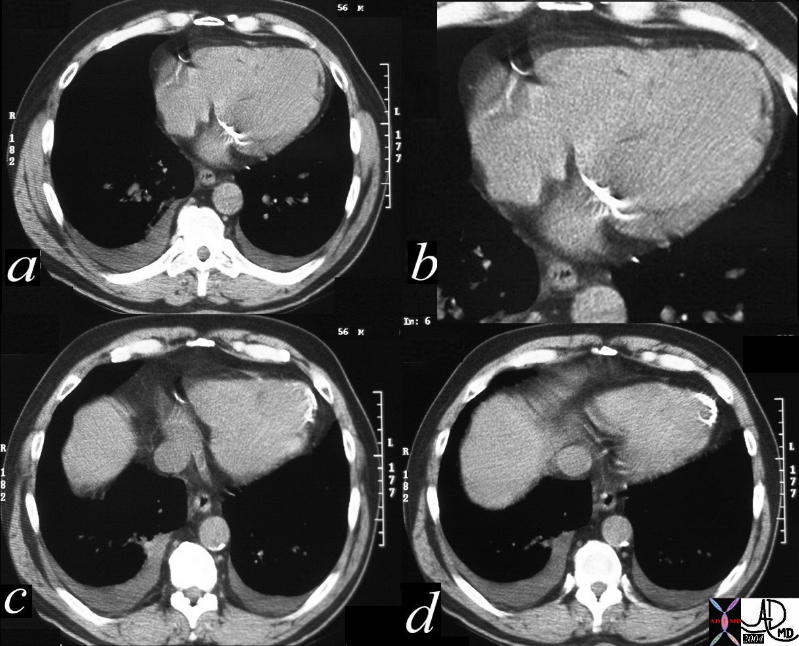
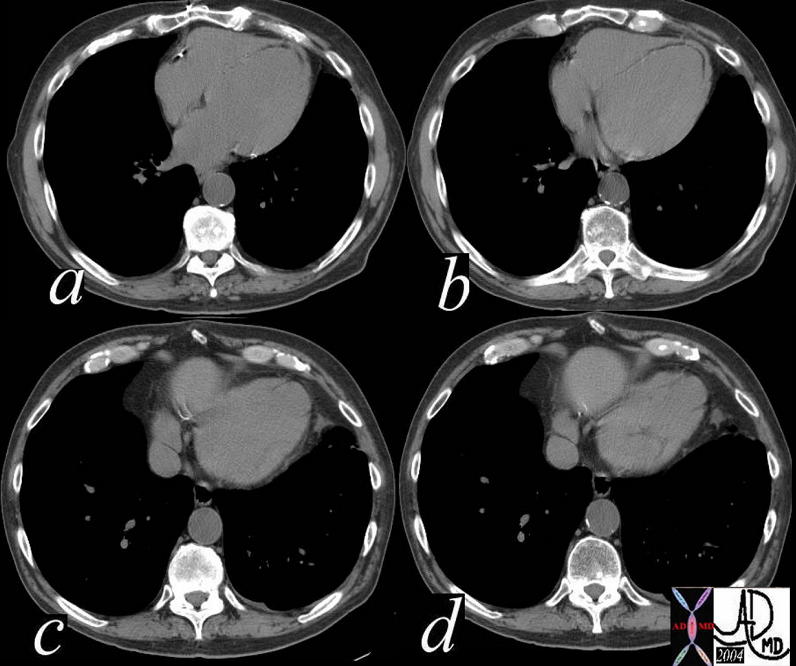
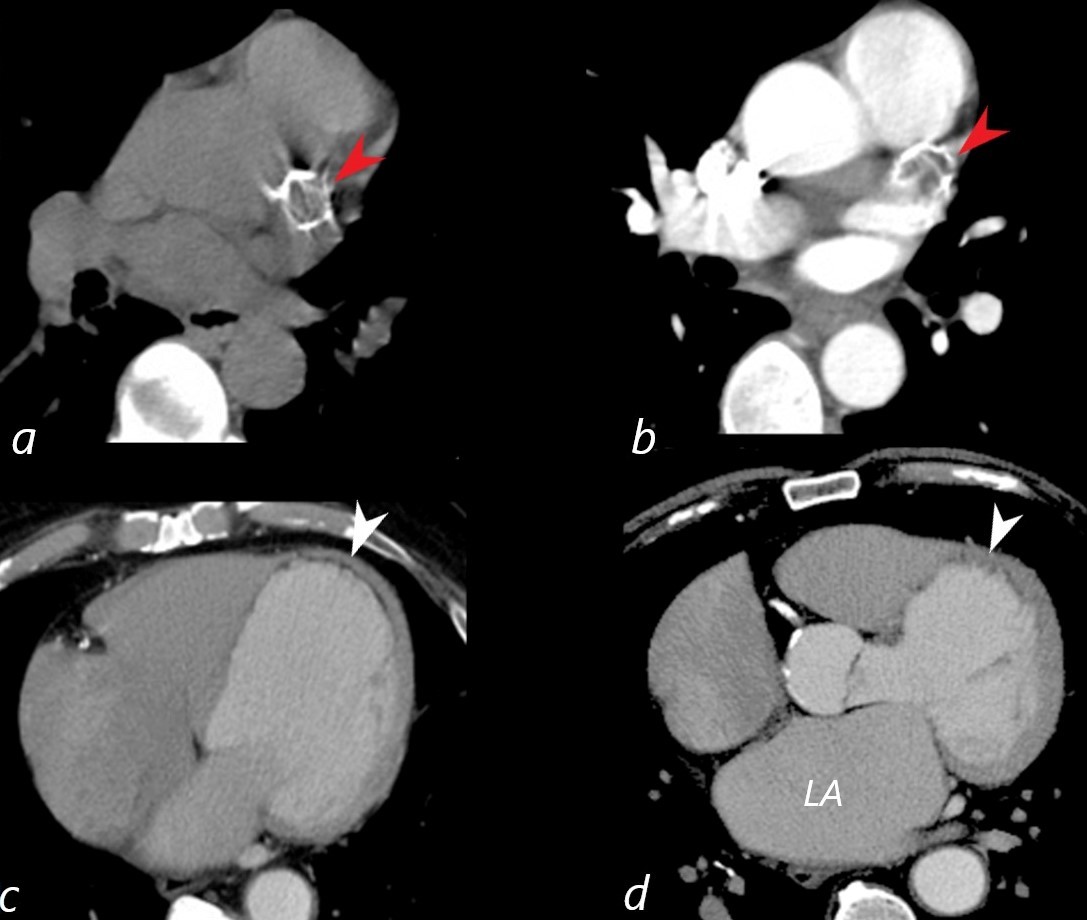
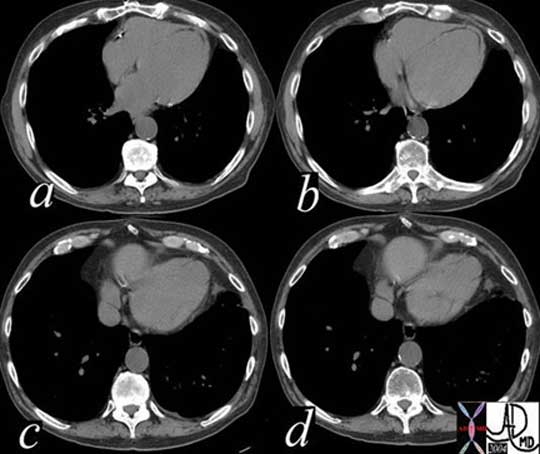
56 year old male with history of coronary artery disease. Axial CT through the heart shows apical curvilinear fat (yellow arrowheads, ( a and b) associated with apical myocardial dystrophic calcification (green arrowheads c and d) both indicating prior apical MI. In addition there mitral annular calcification (red arrowhead, b) and multifocal fatty deposits in the RV (white arrowheads, a and b) usually depicting age related degenerative changes,
Ashley Davidoff MD
The CommonVein.net

The CommonVein.net
The CommonVein.net
Ashley Davidoff
THECOMMONVEIN.net

Ashley Davidoff
THECOMMONVEIN.net
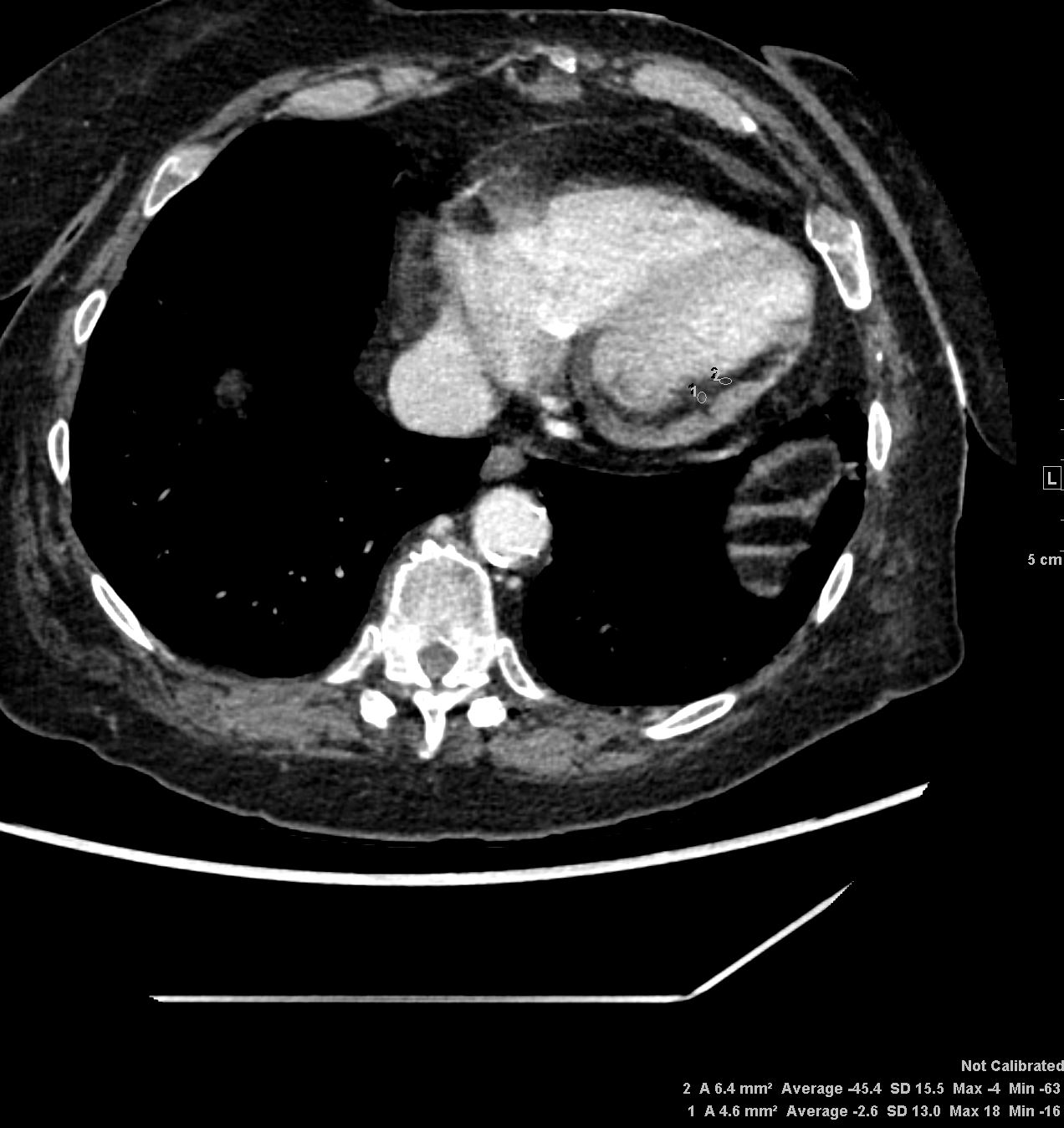
Note also a dissection in the descending aorta
Ashley Davidoff
THECOMMONVEIN.net

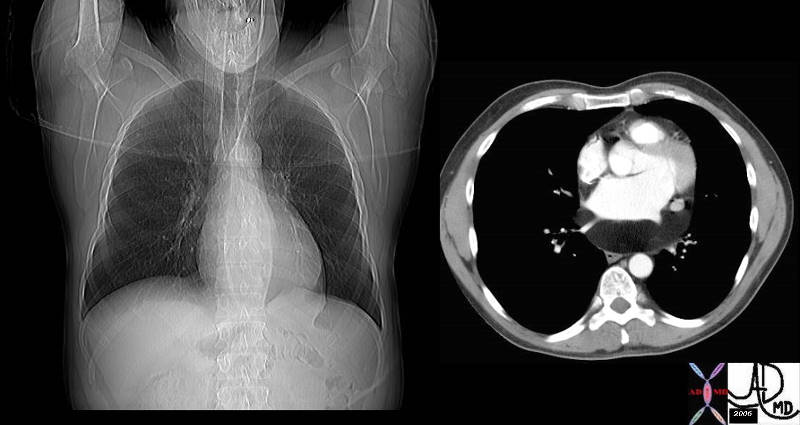
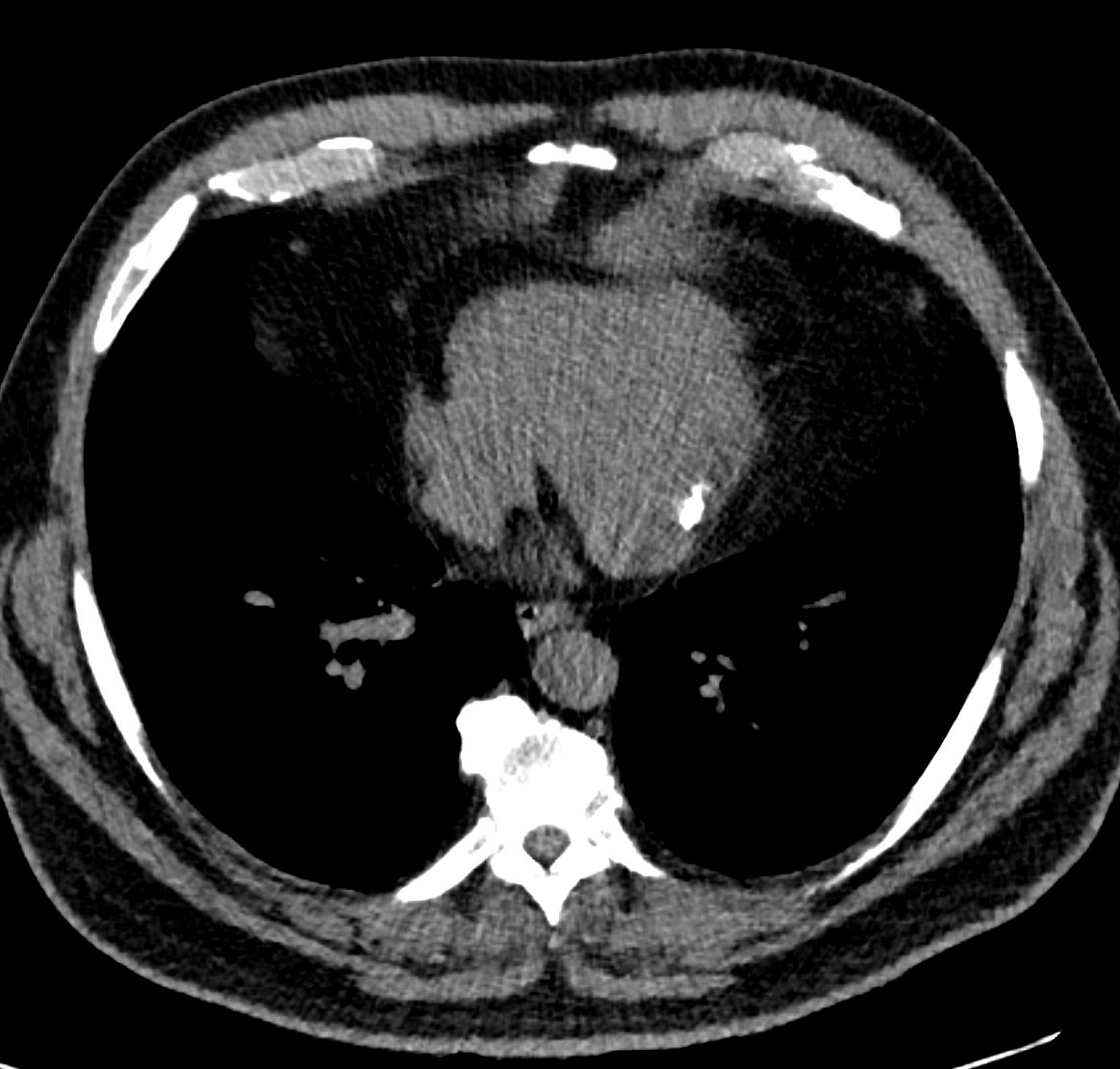
Dilated LV
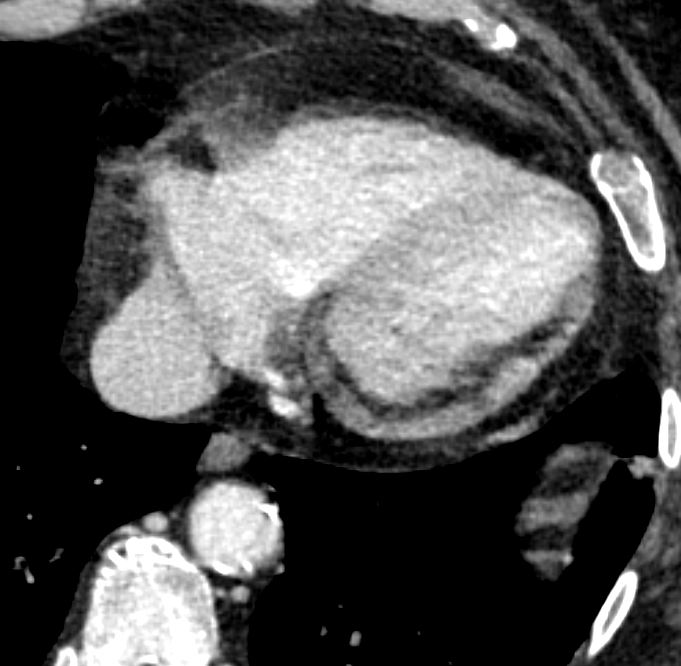
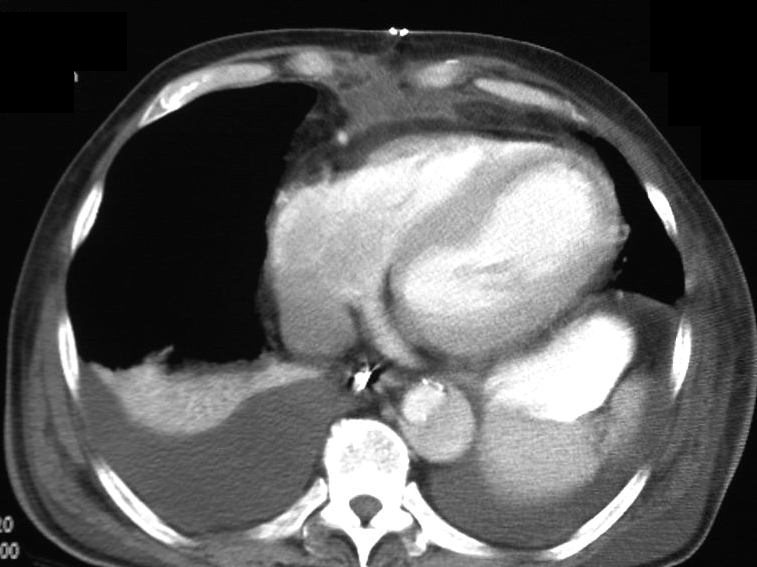
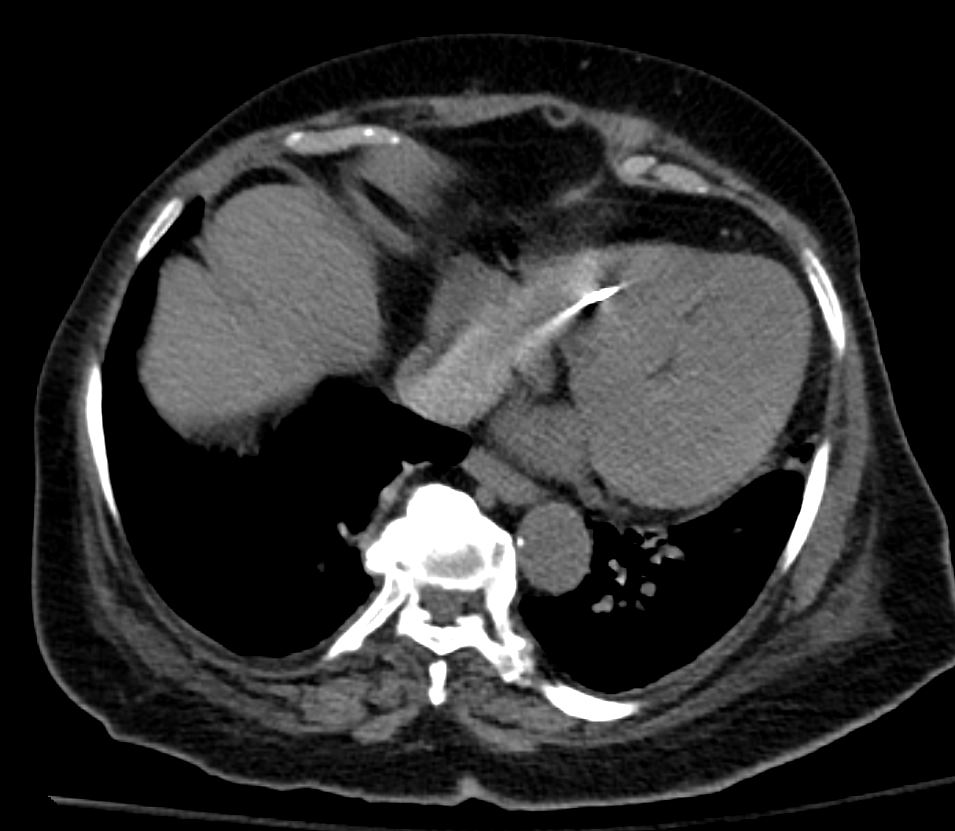
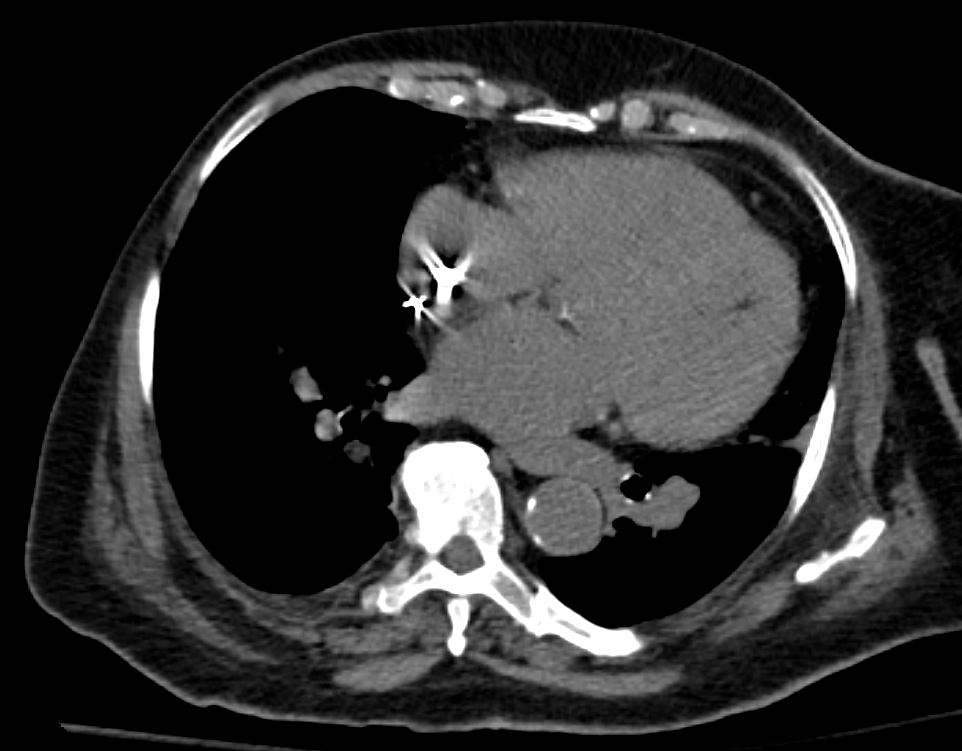
The CTscan is from a 76 year old man in whom the dominant finding is of left ventricular enlargement. The RA and RV are also enlarged based on this image, and LA was enlarged as well suggesting global cardiomegaly consistent with a cardiomyopathy. The clue to the cause of the enlargement is the segmental nature of the disease characterized by the asymmetry of the free wall and septum and the presence of fat (yellow overlay) in the thinned and probably scarred myocardium making ischemic cardiomyopathy the diagnosis. At the apex, there is there is a subtle calcification as well.
Courtesy Ashley Davidoff Copyright 2009 All rights reserved 86984c05.8s01
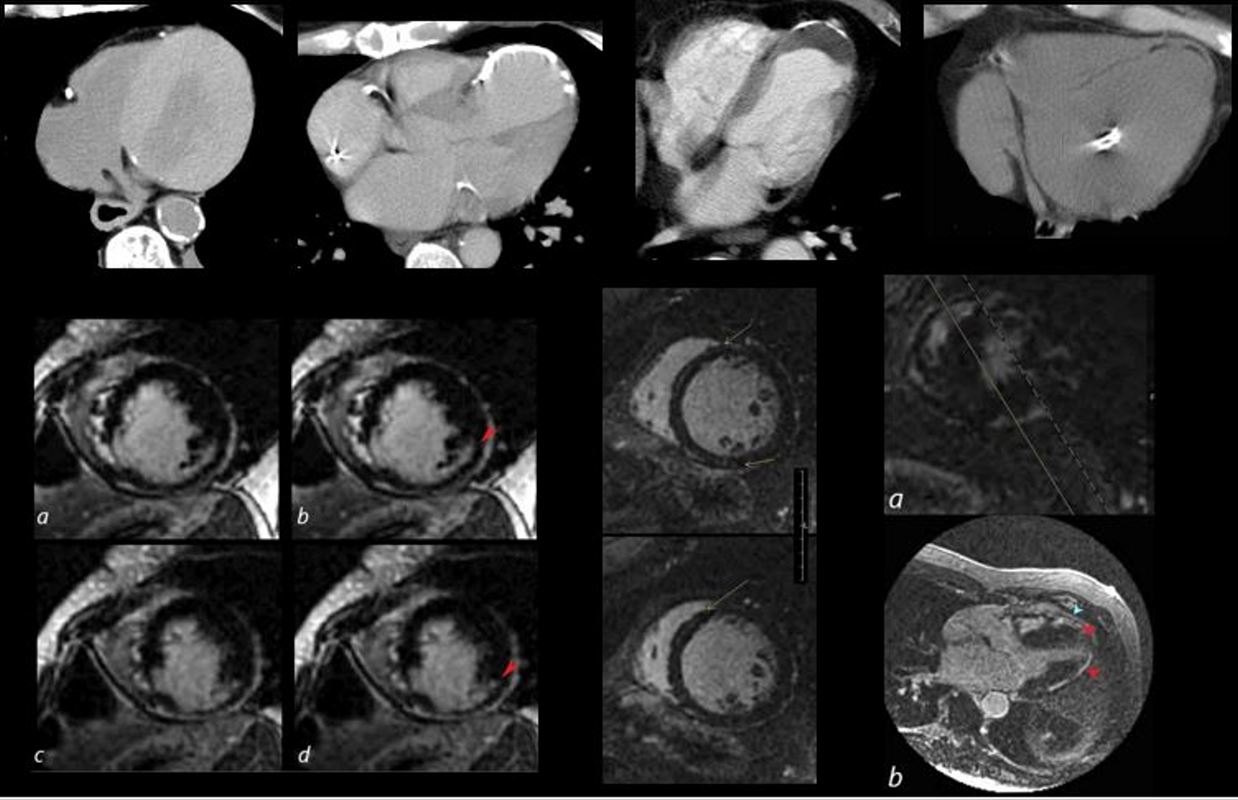
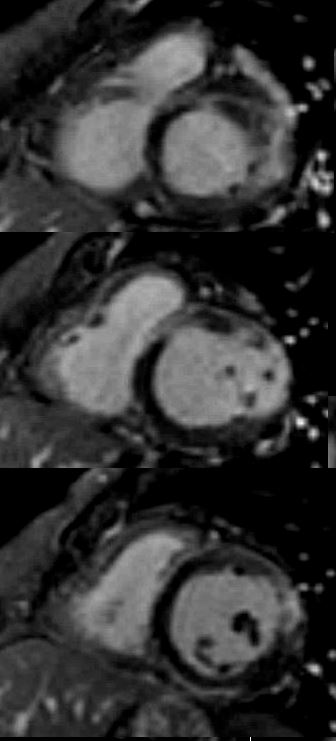
The collage reveals the variation in the tissue characterization of the LV in disease
Top row (from l to r) Patient with anemia showing low density of the blood and soft tissue density of the thickened myocardium. The 2nd image shows a calcified apical aneurysm. The 3rd image is a calcified aneurysm of the apex with thrombus in the lumen. The 4th image shows fat in the septum and the apex reflecting a previous MI in this region
2nd row 1st image is an MRI showing subendocardial delayed gadolinium enhancement (LGE) in a patient with a prior infarct of the inferolateral portion of the LV. The middle image shows a dilated LV with mid myocardial LGE in a patient with congestive cardiomyopathy. The last image shows multicentric linear and nodular LGE prominent in the subepicardial region and consistent with sarcoidosis.
heart 0086
Ashley Davidoff MD






FAT in PAPILLARY MUSCLES



INTERATRIAL LIPOMA (yellow arrow)
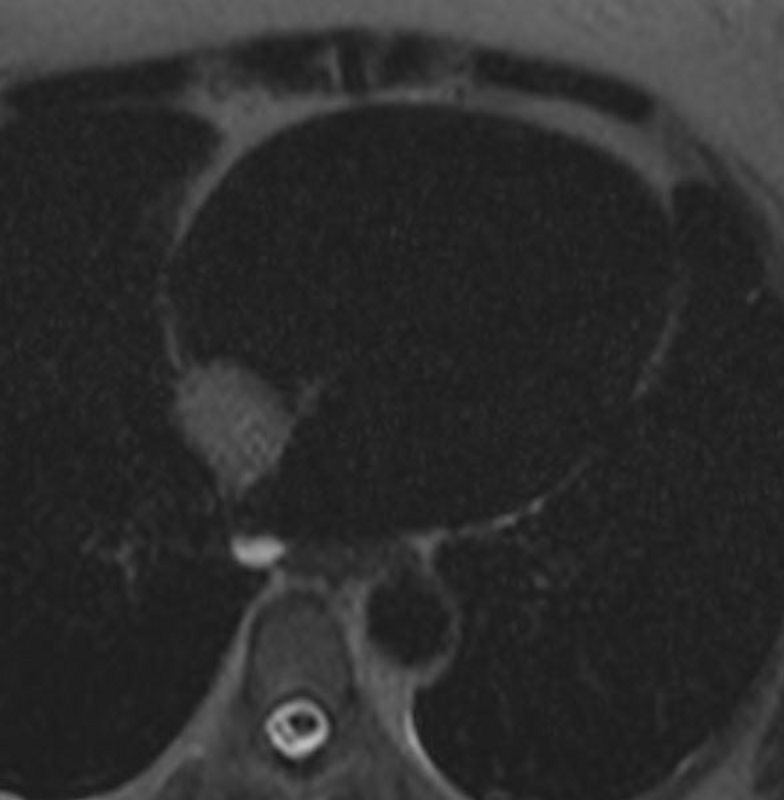
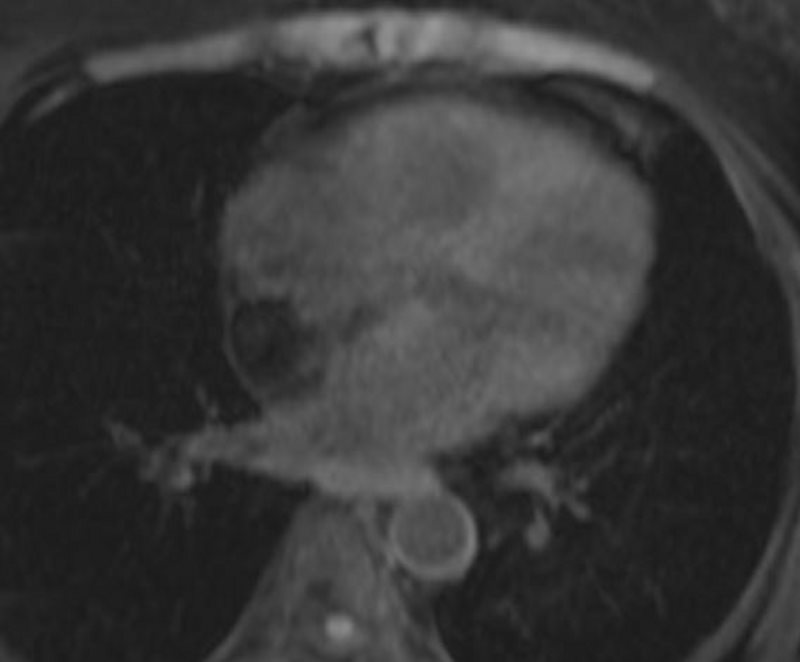
51-year-old female referred from echocardiography with diagnosis of a right atrial mass with suspected diagnosis of an atrial lipoma.
On a prior CT of the abdomen and pelvis, the inferior aspect of the heart showed lipomatous mass. An MRCP also confirmed a lipomatous cardiac mass bright on T1 in phase, losing signal on the out of phase and fat sat sequences.
The dedicated cardiac MRI confirms the presence of a lipoma of the interatrial septum. There is no evidence of enhancement of the mass.
These findings are all therefore consistent with lipoma of the interatrial septum
Ashley Davidoff MD

51-year-old female referred from echocardiography with diagnosis of a right atrial mass with suspected diagnosis of an atrial lipoma.
On a prior CT of the abdomen and pelvis, the inferior aspect of the heart showed lipomatous mass. An MRCP also confirmed a lipomatous cardiac mass bright on T1 in phase, losing signal on the out of phase and fat sat sequences.
The dedicated cardiac MRI confirms the presence of a lipoma of the interatrial septum. There is no evidence of enhancement of the mass.
These findings are all therefore consistent with lipoma of the interatrial septum
Ashley Davidoff MD
51-year-old female referred from echocardiography with diagnosis of a right atrial mass with suspected diagnosis of an atrial lipoma.
On a prior CT of the abdomen and pelvis, the inferior aspect of the heart showed lipomatous mass. An MRCP also confirmed a lipomatous cardiac mass bright on T1 in phase, losing signal on the out of phase and fat sat sequences.
The dedicated cardiac MRI confirms the presence of a lipoma of the interatrial septum. There is no evidence of enhancement of the mass.
These findings are all therefore consistent with lipoma of the interatrial septum
Ashley Davidoff MD
51-year-old female referred from echocardiography with diagnosis of a right atrial mass with suspected diagnosis of an atrial lipoma.
On a prior CT of the abdomen and pelvis, the inferior aspect of the heart showed lipomatous mass. An MRCP also confirmed a lipomatous cardiac mass bright on T1 in phase, losing signal on the out of phase and fat sat sequences.
The dedicated cardiac MRI confirms the presence of a lipoma of the interatrial septum. There is no evidence of enhancement of the mass.
These findings are all therefore consistent with lipoma of the interatrial septum
Ashley Davidoff MD
51-year-old female referred from echocardiography with diagnosis of a right atrial mass with suspected diagnosis of an atrial lipoma.
On a prior CT of the abdomen and pelvis, the inferior aspect of the heart showed lipomatous mass. An MRCP also confirmed a lipomatous cardiac mass bright on T1 in phase, losing signal on the out of phase and fat sat sequences.
The dedicated cardiac MRI confirms the presence of a lipoma of the interatrial septum. There is no evidence of enhancement of the mass.
These findings are all therefore consistent with lipoma of the interatrial septum
Ashley Davidoff MD

51-year-old female referred from echocardiography with diagnosis of a right atrial mass with suspected diagnosis of an atrial lipoma.
On a prior CT of the abdomen and pelvis, the inferior aspect of the heart showed lipomatous mass. An MRCP also confirmed a lipomatous cardiac mass bright on T1 in phase, losing signal on the out of phase and fat sat sequences.
The dedicated cardiac MRI confirms the presence of a lipoma of the interatrial septum. There is no evidence of enhancement of the mass.
These findings are all therefore consistent with lipoma of the interatrial septum
Ashley Davidoff MD
51-year-old female referred from echocardiography with diagnosis of a right atrial mass with suspected diagnosis of an atrial lipoma.
On a prior CT of the abdomen and pelvis, the inferior aspect of the heart showed lipomatous mass. An MRCP also confirmed a lipomatous cardiac mass bright on T1 in phase, losing signal on the out of phase and fat sat sequences.
The dedicated cardiac MRI confirms the presence of a lipoma of the interatrial septum. There is no evidence of enhancement of the mass.
These findings are all therefore consistent with lipoma of the interatrial septum
Ashley Davidoff MD
51-year-old female referred from echocardiography with diagnosis of a right atrial mass with suspected diagnosis of an atrial lipoma.
On a prior CT of the abdomen and pelvis, the inferior aspect of the heart showed lipomatous mass. An MRCP also confirmed a lipomatous cardiac mass bright on T1 in phase, losing signal on the out of phase and fat sat sequences.
The dedicated cardiac MRI confirms the presence of a lipoma of the interatrial septum. There is no evidence of enhancement of the mass.
These findings are all therefore consistent with lipoma of the interatrial septum
Ashley Davidoff MD
51-year-old female referred from echocardiography with diagnosis of a right atrial mass with suspected diagnosis of an atrial lipoma.
On a prior CT of the abdomen and pelvis, the inferior aspect of the heart showed lipomatous mass. An MRCP also confirmed a lipomatous cardiac mass bright on T1 in phase, losing signal on the out of phase and fat sat sequences.
The dedicated cardiac MRI confirms the presence of a lipoma of the interatrial septum. There is no evidence of enhancement of the mass.
These findings are all therefore consistent with lipoma of the interatrial septum
Ashley Davidoff MD
51-year-old female referred from echocardiography with diagnosis of a right atrial mass with suspected diagnosis of an atrial lipoma.
On a prior CT of the abdomen and pelvis, the inferior aspect of the heart showed lipomatous mass. An MRCP also confirmed a lipomatous cardiac mass bright on T1 in phase, losing signal on the out of phase and fat sat sequences.
The dedicated cardiac MRI confirms the presence of a lipoma of the interatrial septum. There is no evidence of enhancement of the mass.
These findings are all therefore consistent with lipoma of the interatrial septum
Ashley Davidoff MD
51-year-old female referred from echocardiography with diagnosis of a right atrial mass with suspected diagnosis of an atrial lipoma.
On a prior CT of the abdomen and pelvis, the inferior aspect of the heart showed lipomatous mass. An MRCP also confirmed a lipomatous cardiac mass bright on T1 in phase, losing signal on the out of phase and fat sat sequences.
The dedicated cardiac MRI confirms the presence of a lipoma of the interatrial septum. There is no evidence of enhancement of the mass.
These findings are all therefore consistent with lipoma of the interatrial septum
Ashley Davidoff MD
51-year-old female referred from echocardiography with diagnosis of a right atrial mass with suspected diagnosis of an atrial lipoma.
On a prior CT of the abdomen and pelvis, the inferior aspect of the heart showed lipomatous mass. An MRCP also confirmed a lipomatous cardiac mass bright on T1 in phase, losing signal on the out of phase and fat sat sequences.
The dedicated cardiac MRI confirms the presence of a lipoma of the interatrial septum. There is no evidence of enhancement of the mass.
These findings are all therefore consistent with lipoma of the interatrial septum
Ashley Davidoff MD

51-year-old female referred from echocardiography with diagnosis of a right atrial mass with suspected diagnosis of an atrial lipoma.
On a prior CT of the abdomen and pelvis, the inferior aspect of the heart showed lipomatous mass. An MRCP also confirmed a lipomatous cardiac mass bright on T1 in phase, losing signal on the out of phase and fat sat sequences.
The dedicated cardiac MRI confirms the presence of a lipoma of the interatrial septum. There is no evidence of enhancement of the mass.
These findings are all therefore consistent with lipoma of the interatrial septum
Ashley Davidoff MD

51-year-old female referred from echocardiography with diagnosis of a right atrial mass with suspected diagnosis of an atrial lipoma.
On a prior CT of the abdomen and pelvis, the inferior aspect of the heart showed lipomatous mass. An MRCP also confirmed a lipomatous cardiac mass bright on T1 in phase, losing signal on the out of phase and fat sat sequences.
The dedicated cardiac MRI confirms the presence of a lipoma of the interatrial septum. There is no evidence of enhancement of the mass.
These findings are all therefore consistent with lipoma of the interatrial septum
Ashley Davidoff MD



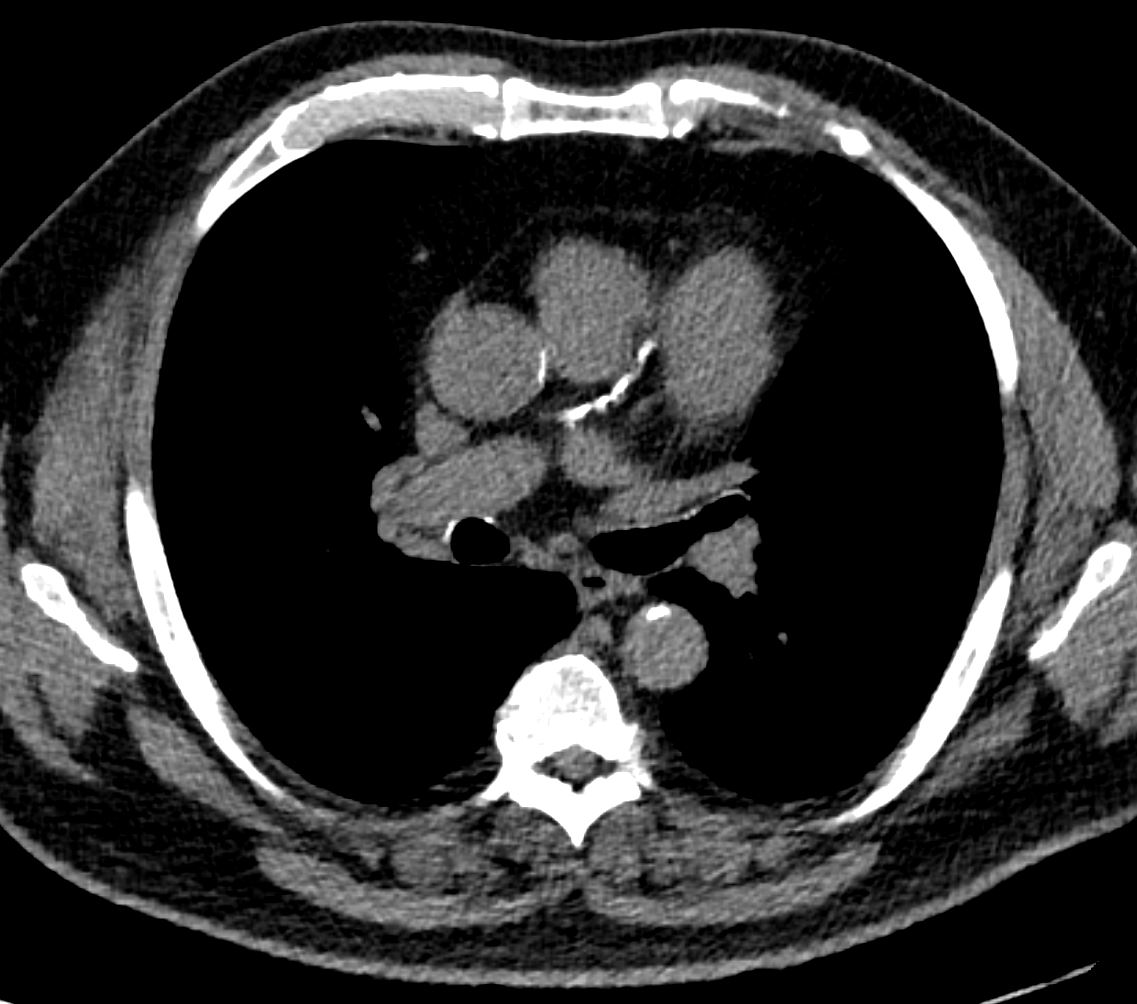
AMYLOIDOSIS TRACHEA BRONCHI BRONCHIOLES
56-year-old female with stable tracheobronchial amyloidosis.
The CXR shows in the AP projection shows a small tubular density which on CT reflect as a small bronchus which is thickened and contains calcification. The lateral exam shows bronchial wall thickening
The CT shows multicentric thickening of the trachea and bronchi.
The bronchi to the left lower lobe and a middle lobe bronchus are thickened and contain calcium
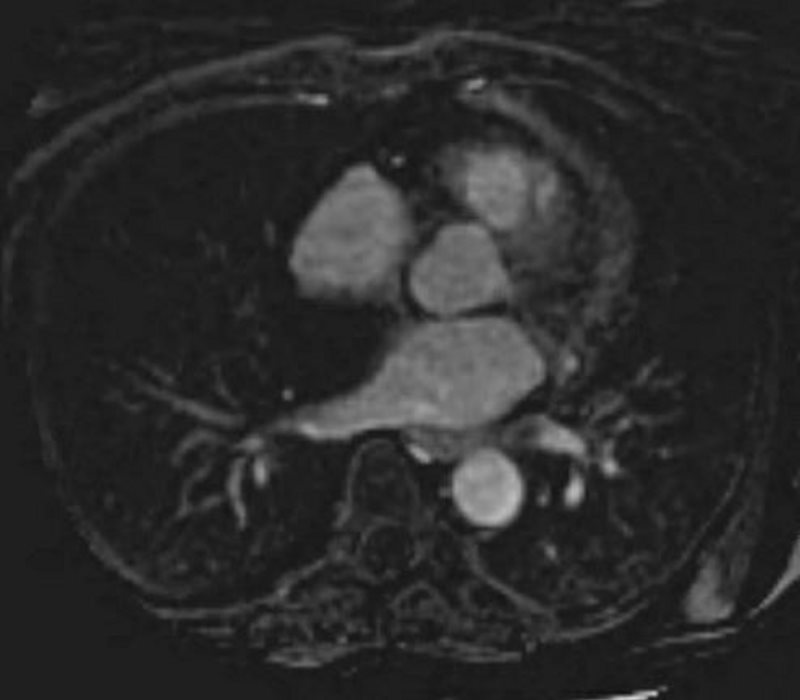
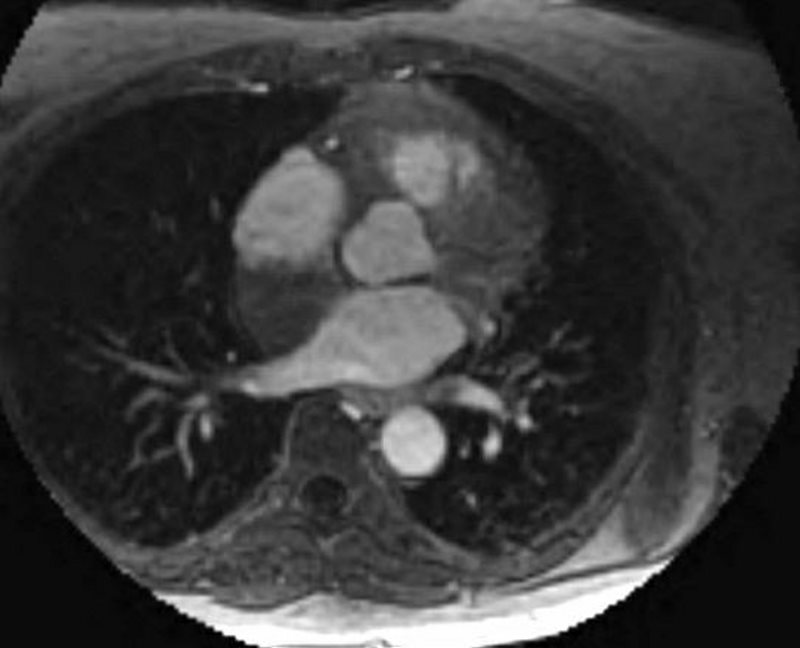
There is nodular fat accumulation along the lateral wall and apex of the LV and within the RV. There is also linear fat accumulation in the mid septal region and prominent pericardial fat around the anterior wall of the RV
Ashley Davidoff MD
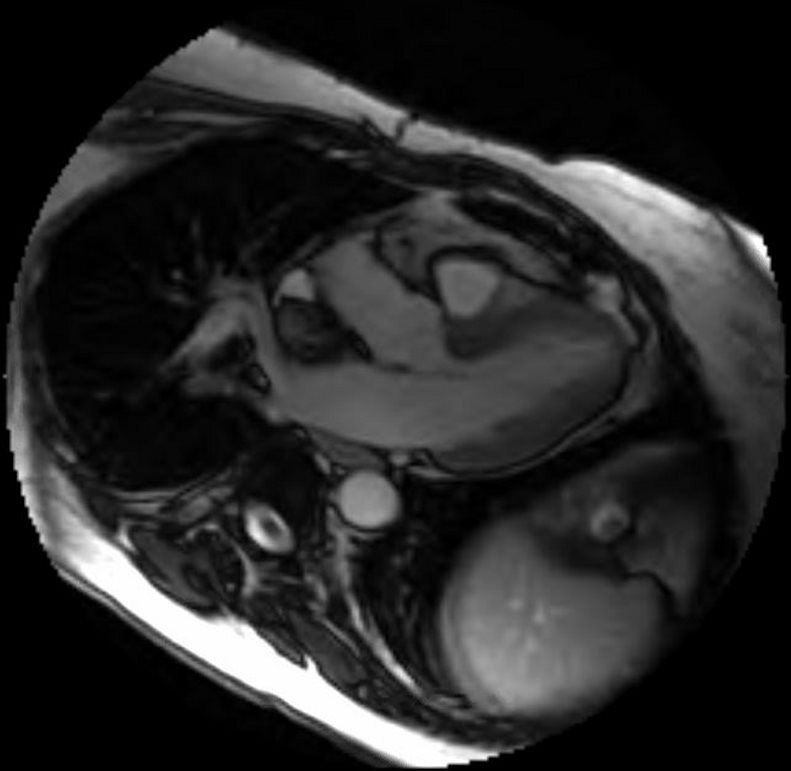
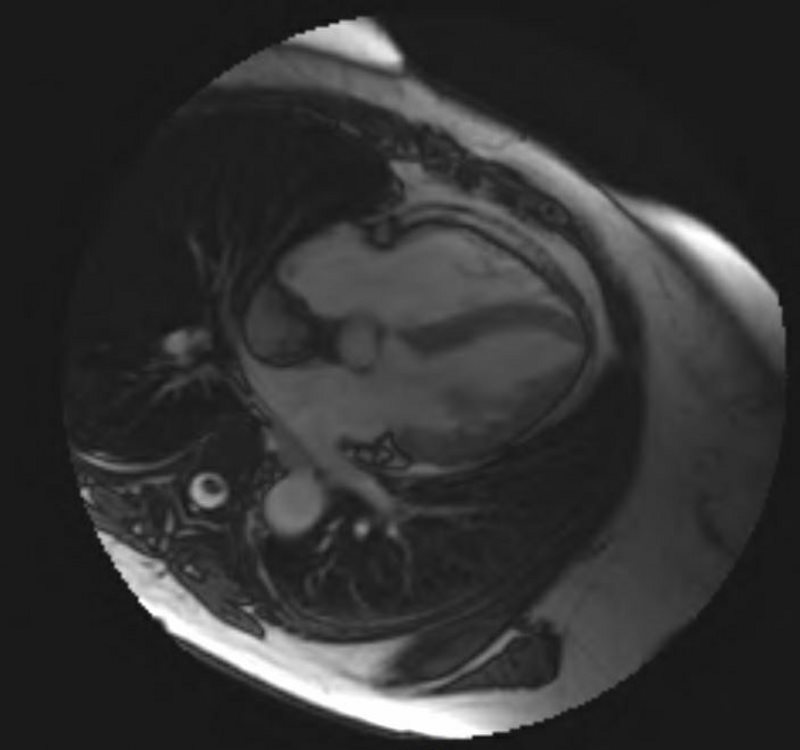
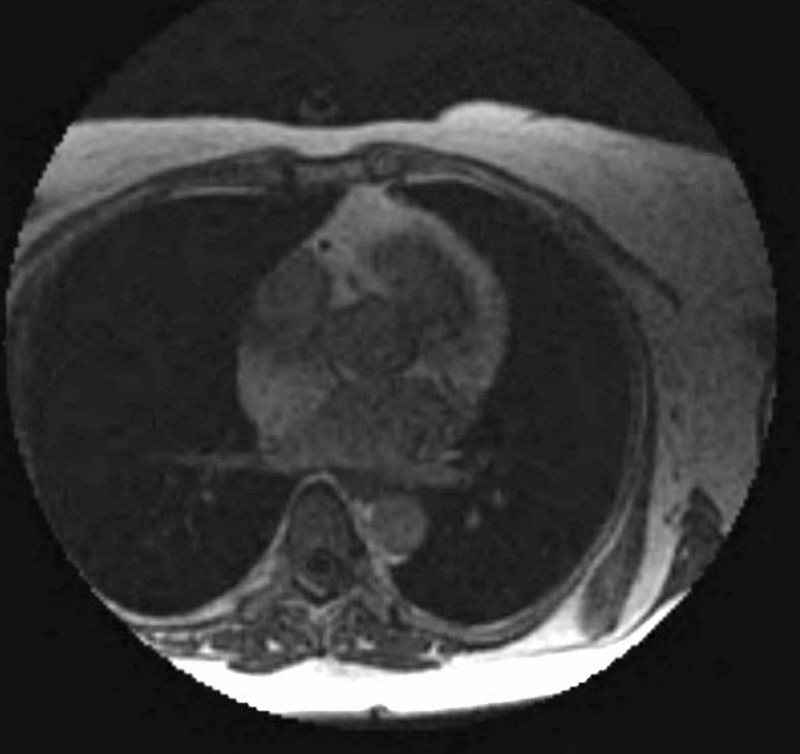
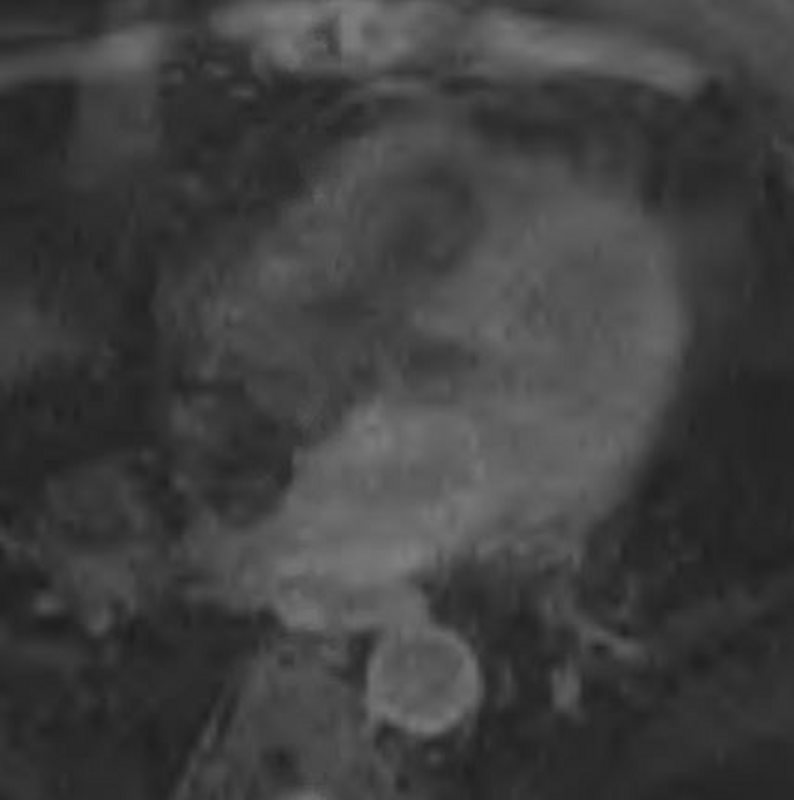
Long axis views using 2chamber view (upper left) shows diffuse mid myocardial LGE in the anterior wall and a short segment of subendocardial enhancement in the basal regions. The 3 chamber view (upper right shows LGE at the hinge point inferiorly, while the 4 chamber views show nodular mid myocardial nodular septal LGE and significant mid myocardial LGE at the base inferiorly.
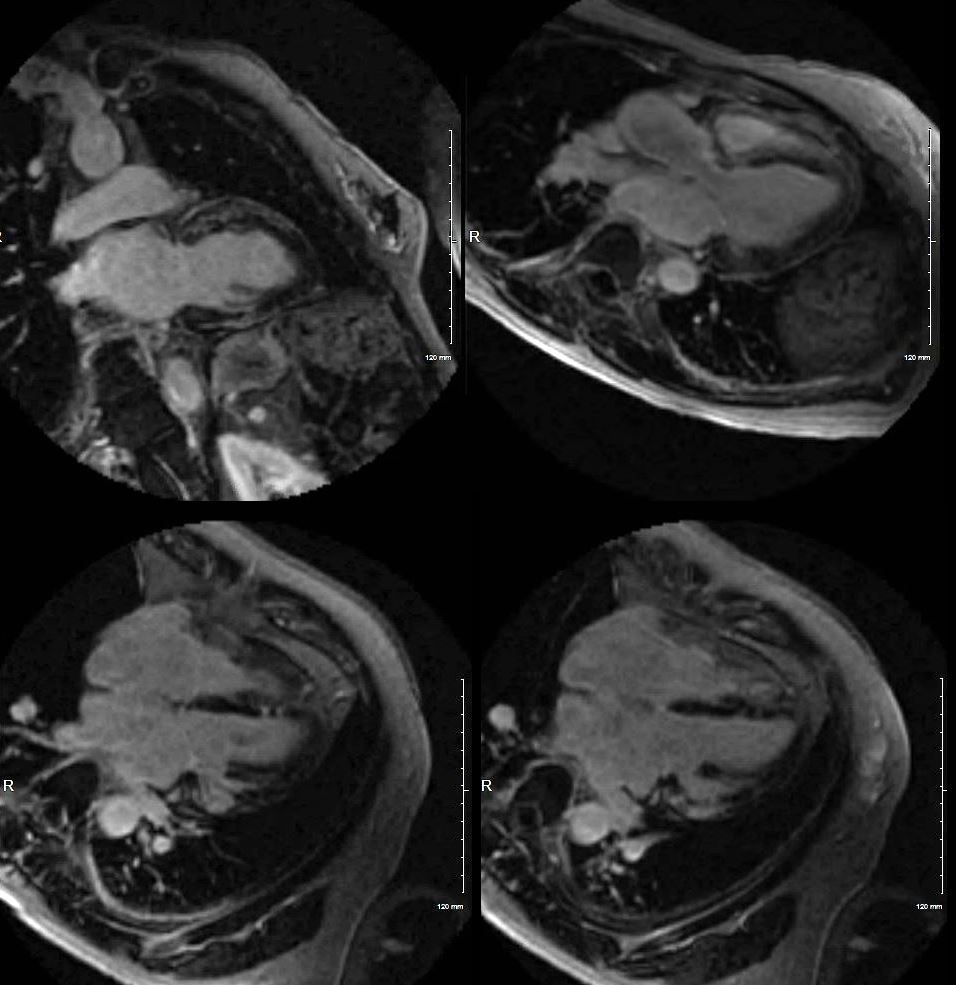
HX 50-year-old female with fatigue and palpitations
Initial echo showed mildly reduced ejection fraction of 49%, mildly enlarged LA, with normal sized LV cavity, and mild LVH, and mild diastolic dysfunction with regional wall abnormalities. There was no evidence of RV dysfunction.
The first MRI showed a normal ejection fraction of 38%, with basal hypokinesis and LGE in the lateral and basal region with subendocardial sparing. Additional LGE was noted along the basal septal region. Dilated cardiomyopathy was felt to be likely.
Subsequent MRI done 2 months later showed mildly enlarged left ventricle with an EF of 44% with LGE in the lateral and anterior , extending from the base to mid body with transmural involvement. Additionally intramural involvement of the inferior wall and patchy intramural enhancement of the septum and anterior wall .
Subsequent echo showed overall improvement but with dilated left and right atria and normal LV and RV, improved regional wall abnormalities, EF of 50-54%, and normal PA pressure (<36mmHg)
Ashley Davidoff MD.
LGE pattern shows anterospptal mid myocardial and linear pattern and transmural in the lateral wall.
HX 50-year-old female with fatigue and palpitations
Initial echo showed mildly reduced ejection fraction of 49%, mildly enlarged LA, with normal sized LV cavity, and mild LVH, and mild diastolic dysfunction with regional wall abnormalities. There was no evidence of RV dysfunction.
The first MRI showed a normal ejection fraction of 38%, with basal hypokinesis and LGE in the lateral and basal region with subendocardial sparing. Additional LGE was noted along the basal septal region. Dilated cardiomyopathy was felt to be likely.
Subsequent MRI done 2 months later showed mildly enlarged left ventricle with an EF of 44% with LGE in the lateral and anterior , extending from the base to mid body with transmural involvement. Additionally intramural involvement of the inferior wall and patchy intramural enhancement of the septum and anterior wall .
Subsequent echo showed overall improvement but with dilated left and right atria and normal LV and RV, improved regional wall abnormalities, EF of 50-54%, and normal PA pressure (<36mmHg)
Ashley Davidoff MD.
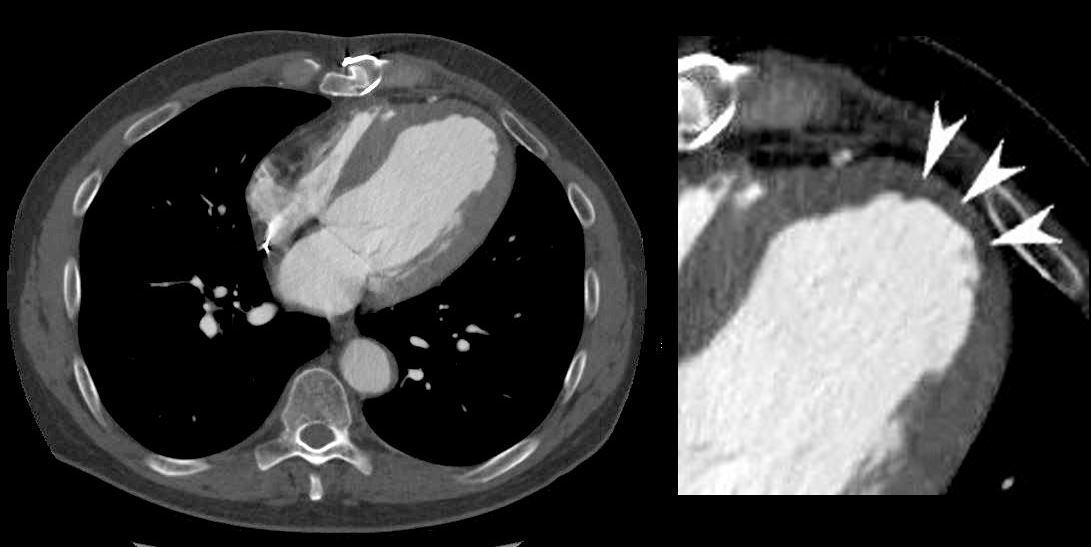
EPICARDIAL FAT NECROSIS
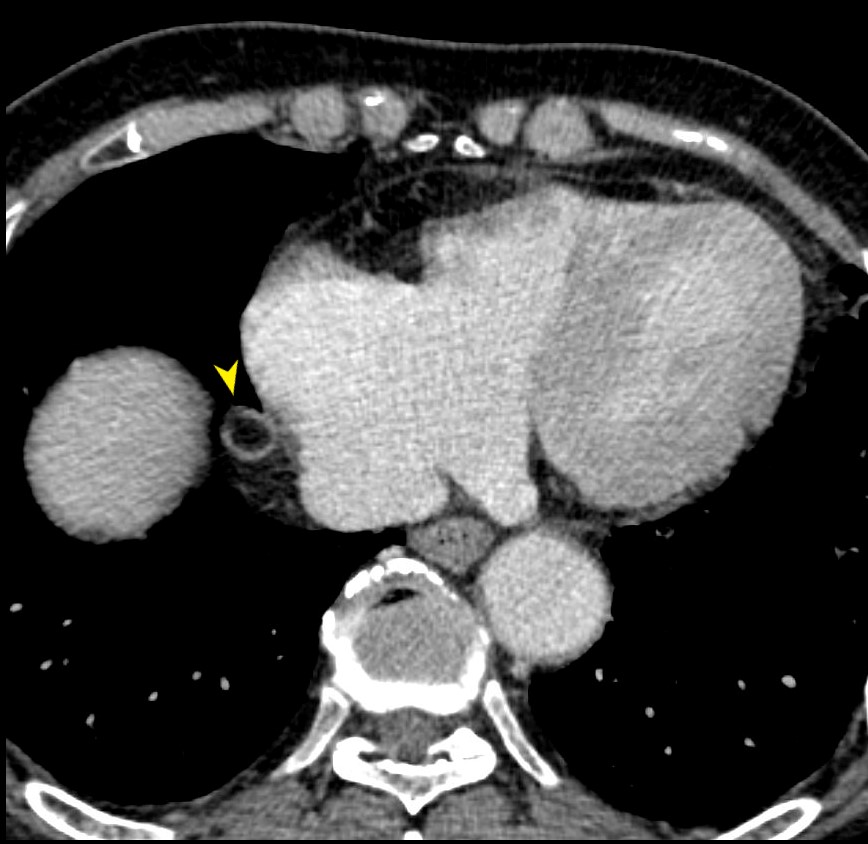
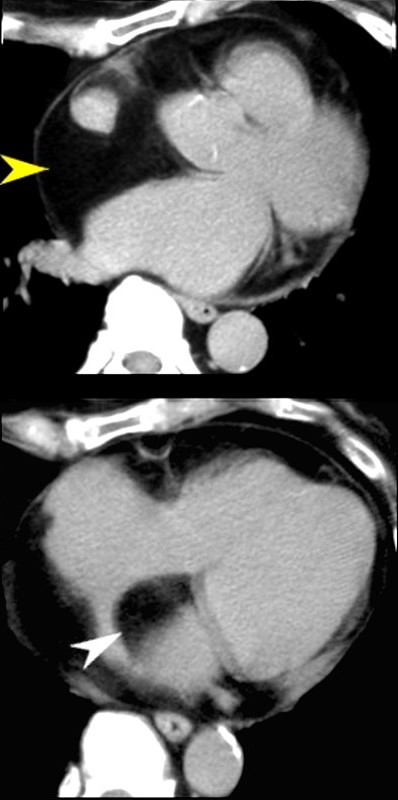
79-year male with asymptomatic finding on axial CT of a focal sclerotic ring surround the epicardial fat on the right side of the heart (yellow arrowhead). This most likely reflects chronic epicardial fat necrosis
Ashley Davidoff MD
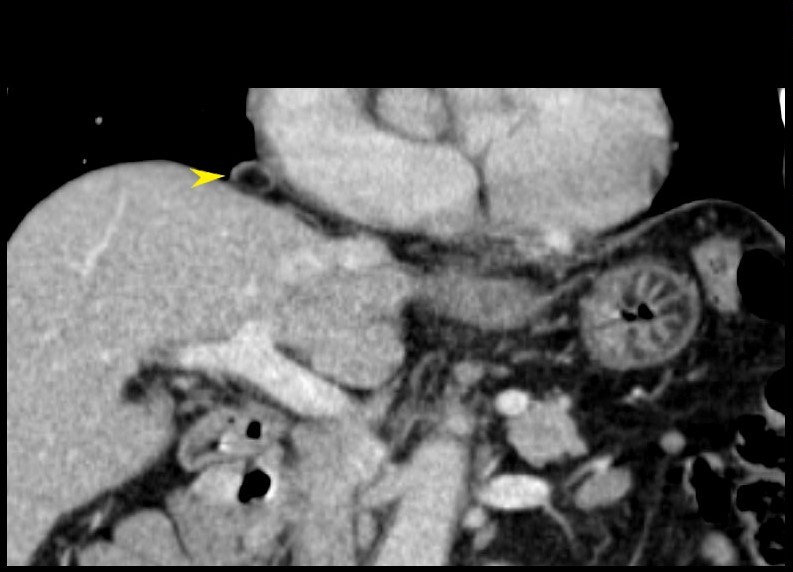
79-year male with asymptomatic finding on coronally reformatted CT of a focal sclerotic ring surround the epicardial fat on the right side of the heart (yellow arrowhead). This most likely reflects chronic epicardial fat necrosis
Ashley Davidoff MD
56 year old male with history of coronary artery disease. Axial CT through the heart shows apical curvilinear fat (yellow arrowheads, ( a and b) associated with apical myocardial dystrophic calcification (green arrowheads c and d) both indicating prior apical MI. In addition there mitral annular calcification (red arrowhead, b) and multifocal fatty deposits in the RV (white arrowheads, a and b) usually depicting age related degenerative changes,
Ashley Davidoff MD

37 year old male with no history of CAD with a fat containing nodule at the LV apex most likely representing a lipoma of the myocardium
Ashley Davidoff MD

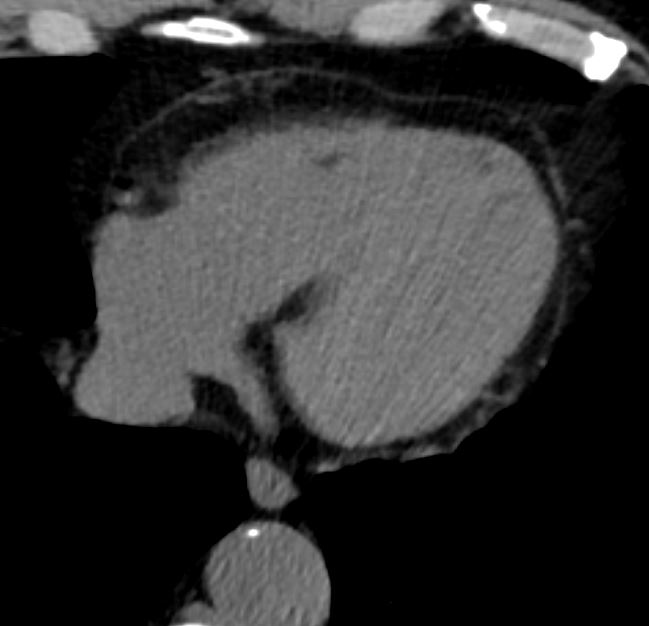
81 year old female presents 6 years earlier with non specific symptoms and abdominal CT without contrast was negative. Review of the inferior portions of the heart however show a pointed RV apex, an irregular contour of the anterior wall of the RV and small focal regions of fat.
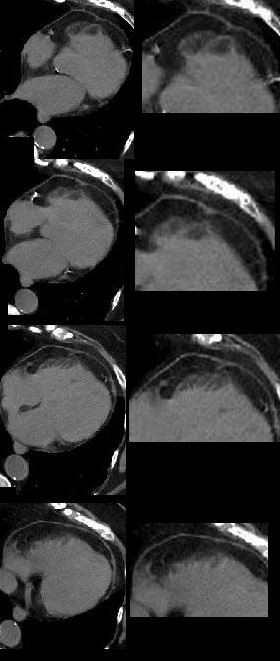
In the interim 2 years prior to the cardiac MRI she had a CT for rectal bleeding. The lower cuts demonstrate an unusual shape of the RV apex and a fairly large non enhancing RV apical filling defect reminiscent of thrombus.
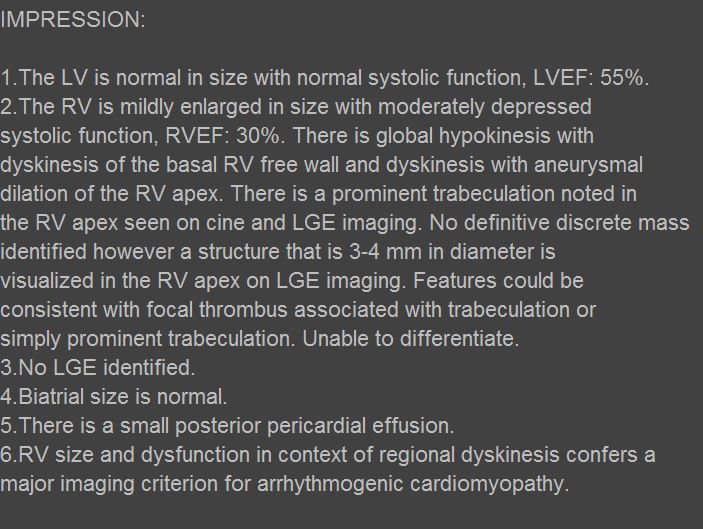
At the time of the cardiac MRI, she was having non sustained VT and echo raised the possibility of ARVD and an intracavitary mass.
The MRI shows a large abnormal appearing apex of the RV with accentuated trabeculations and cine images that show regions of dyskinesis. These finding are consistent with ARVD.
Ashley Davidoff MD Hristina Natcheva MD
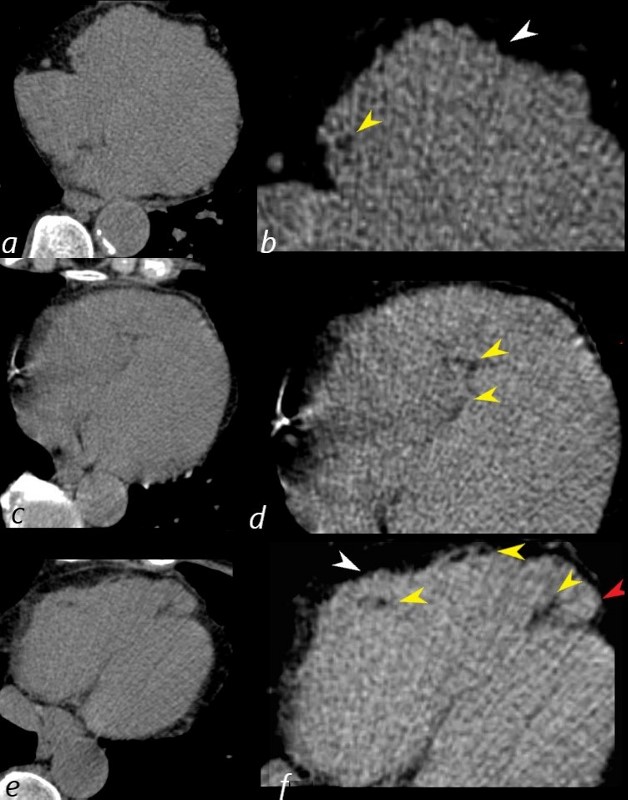
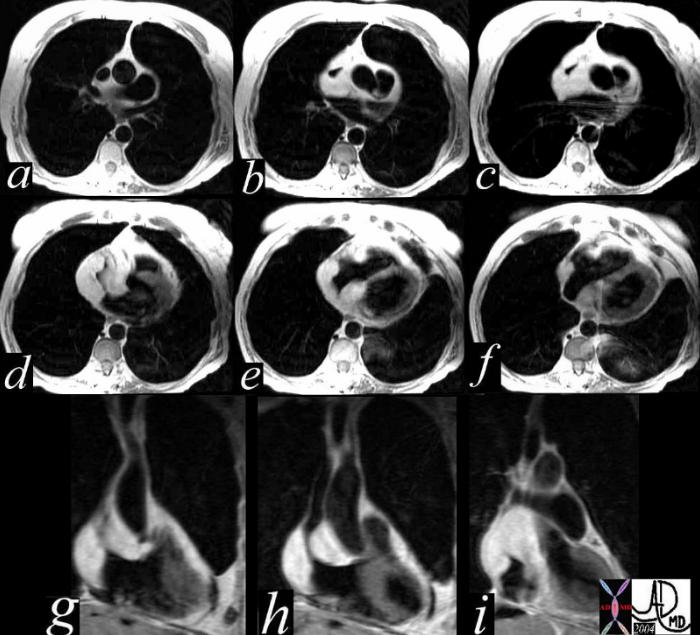
81 year old female presents 6 years earlier with non specific symptoms and abdominal CT without contrast was negative. Review of the inferior portions of the heart (images a,c,e are correspondingly magnified b,d,f) however show an unusually prominent and pointed RV apex (red arrowhead) , an irregular contour of the anterior wall of the RV (white arrowhead, f) and small focal regions of fat (yellow arrowheads b,d,f).
Ashley Davidoff MD Hristina Natcheva MD
75 year old female with findings consistent with cross fused ectopia. The left kidney is in intimate and inseparable contact with the right kidney and both lie in the right upper quadrantThey are both malrorated . The rightkidney is more superior and the pelvis points toward the right. The left kidney is lower and the pelvis points medially. There are 2 ureters. The right ureter enters the trigone on the right and the left on the left. 2 years later there is bilateral hydronephros as hydroureter of unknown etiology. Some mild reflux is noted to the right kidney on the cystogram
Ashley Davidoff MD

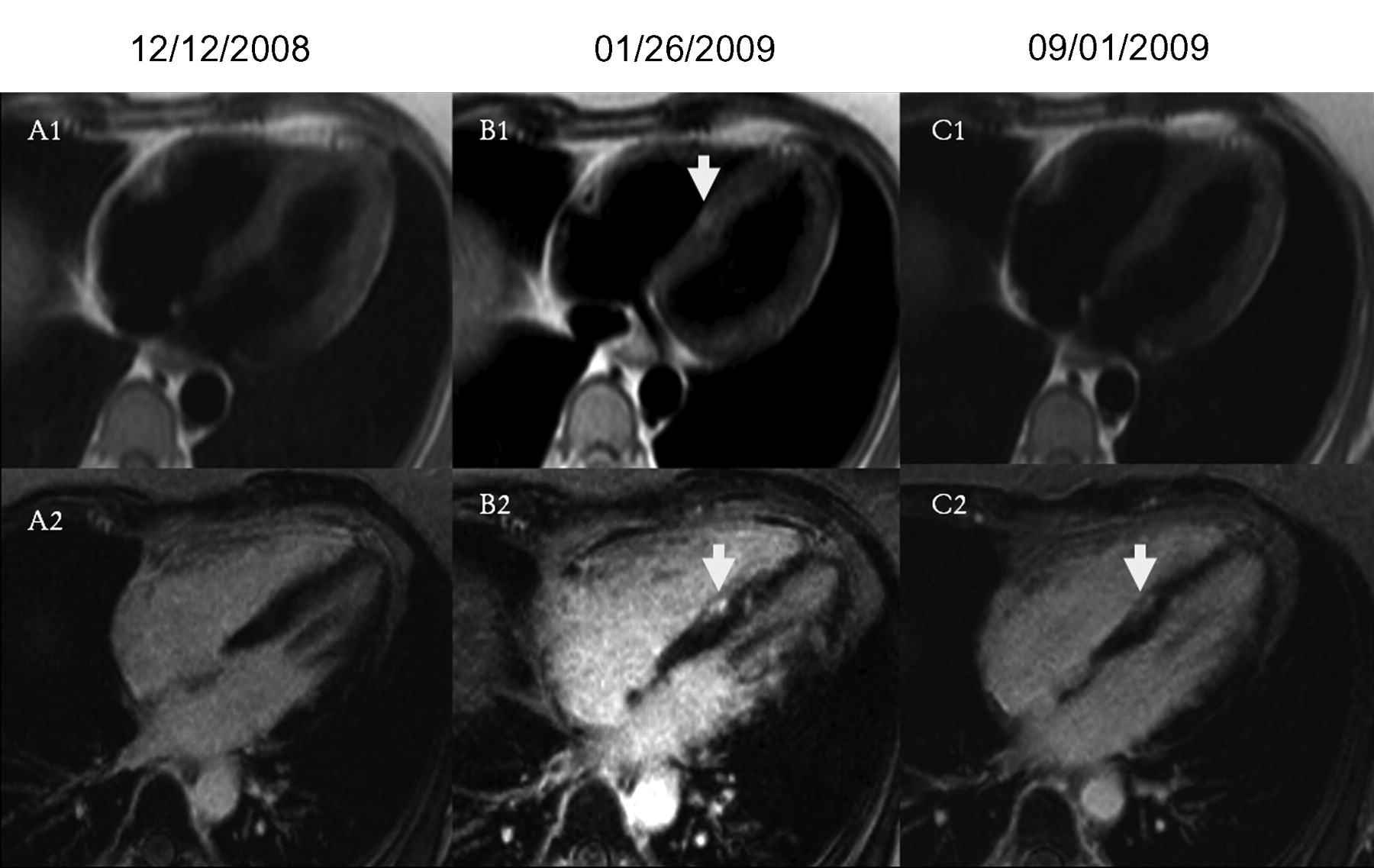
Delayed enhancement images, 4-chamber views. B2 demonstrates interventricular patchy enhancement (arrow) on cardiac MRI performed during an SLE flare and active chest pain. Appearance is typical for myocarditis and a new finding compared to the baseline scan A, with some residual involvement after resolution of the SLE flare and medical treatment (C2). The finding of myocarditis is supported by a patchy enhancement (arrow), consistent with myocardial edema and active inflammation on T2-weighted images without fat saturation. No active inflammation is noted on a followup scan (C1).
Goykman et al Subendocardial Ischemia and Myocarditis in Systemic Lupus Erythematosus Detected by Cardiac Magnetic Resonance Imaging
The Journal of Rheumatology February 2012, 39 (2) 448-450; DOI: https://doi.org/10.3899/jrheum.110812

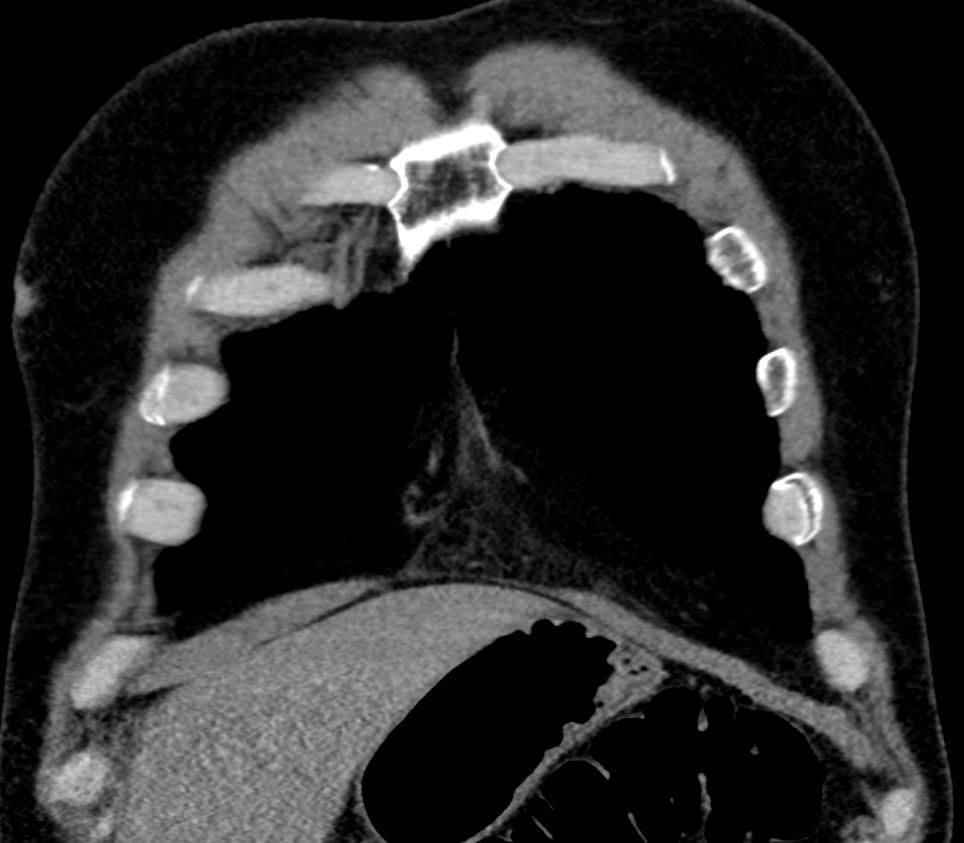
This series of axial T1 weighted MRI images of the heart show a high intensity mass surrounding the SVC (blue arrowhead) and the entrance to the right atrium (RA). There were no symptoms of SVC syndrome in this patient with known COPD. Note that the mass has the intensity of subcutaneous fat. An atrial lipoma is the most likely diagnosis.
Courtesy Jorge Medina
38449c
KEY WORDS
Cardiac, heart, vein, SVC , RA, mass, fat, lipoma, tumor, neoplasm, benign, imaging, radiology, MRI
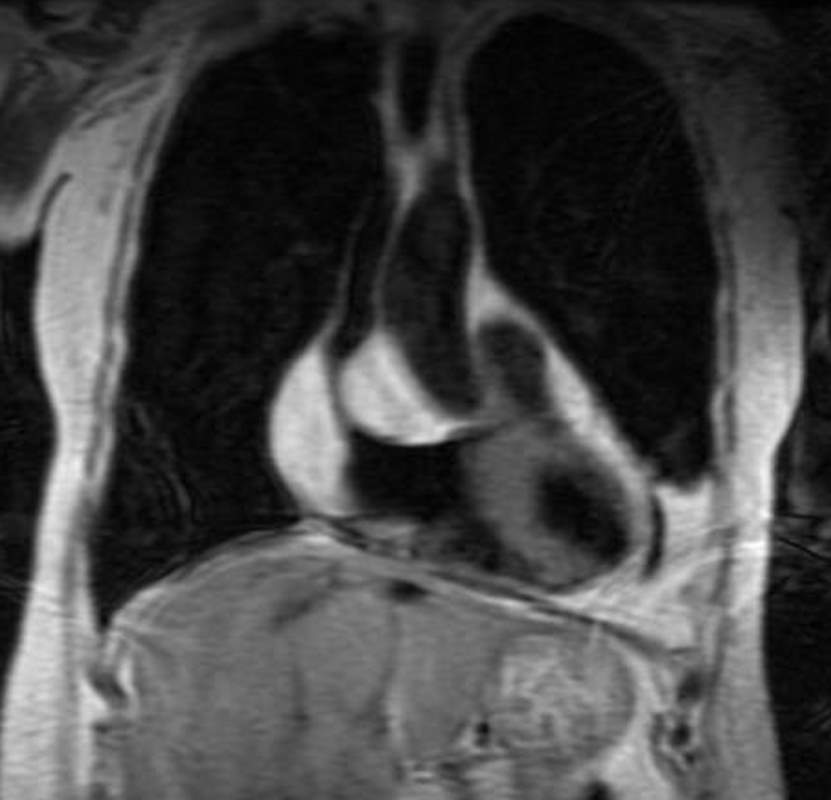
This image of a coronally acquired T1 weighted MRI image of the heart shows a high intensity mass surrounding the SVC and the entrance right atrium (RA) with narrowing of the SVC. There were no symptoms of SVC syndrome in this patient with known COPD. Note that the mass has the intensity of subcutaneous fat. An atrial lipoma is the most likely diagnosis.
Courtesy Jorge Medina
38449c
KEY WORDS
Cardiac, heart, vein, SVC , RA, mass, fat, lipoma, tumor, neoplasm, benign, imaging, radiology, MRI
This series of axial and coronal T1 weighted MRI images of the heart show a high intensity mass surrounding the SVC and the entrance to the right atrium. There were no symptoms of SVC syndrome in this patient with known COPD. Note that the mass has the intensity of the subcutaneous fat. An atrial lipoma is the most likely diagnosis.
Courtesy Jorge Medina
38449c
KEY WORDS
Cardiac, heart, vein, SVC , RA, mass, fat, lipoma, tumor, neoplasm, benign, imaging, radiology, MRI
Axial CT scan through the heart is from a 71year old female who is on steroid therapy. A large amount of fat is noted in the epicardium (yellow arrowhead) and also in the interatrial septum resulting in an atrial lipoma.
Keywords
Steroids, heart, interatrial septum, epicardial fat, fx large fat accumulation
dx interatrial lipoma
imaging
radiology CTscan
28386c03.8
34800c01 cardiac heart pericardium fx lucent subcarinal angle altered dx lipoma of pericardium fat CTscan plain film scout Davidoff MD
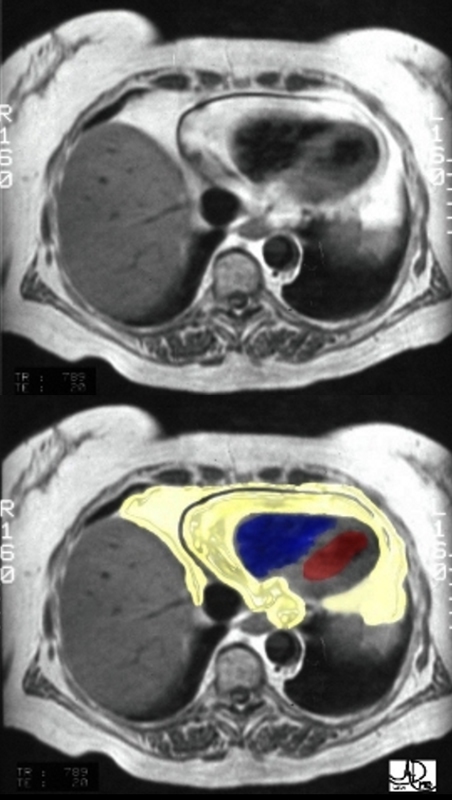
An axial T1 weighted MRI shows a large amount of fat (yellow overlay) around the heart. The epicardial fat is the inner layer and is intimately related to the heart and the pericardial fat is the outer layer. The normal pericardium is seen as a black line between the two layers of fat. Although the pericardium looks like a single layer, it actually consists of two structures – the epicardial serous component and the pericaricardial fibrous component. In pericardial effusion the two layers are separated.
The amount of fat is more than expected and this amount is often associated with Syndrome X.
Courtesy of Ashley Davidoff M.D. 32141.8 code normal heart epicardial fat pericardium anatomy cardiac imaging radiology MRI
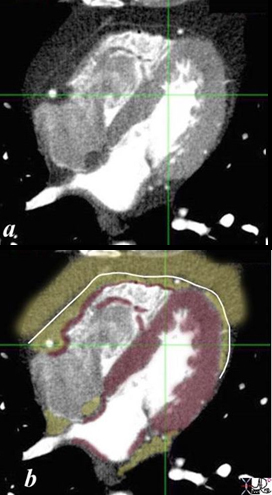
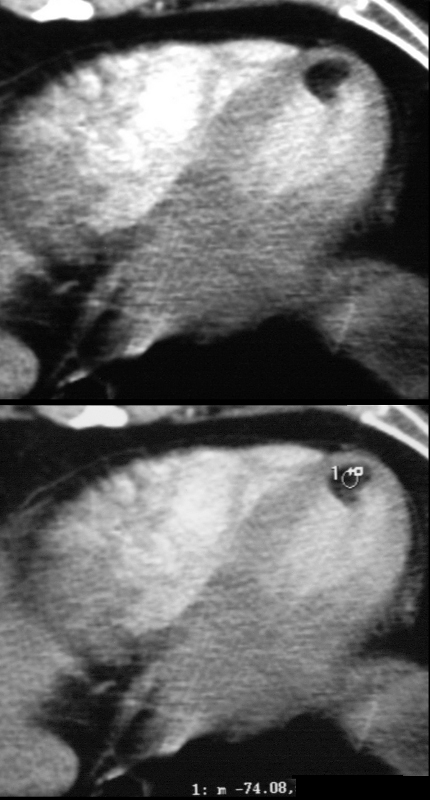
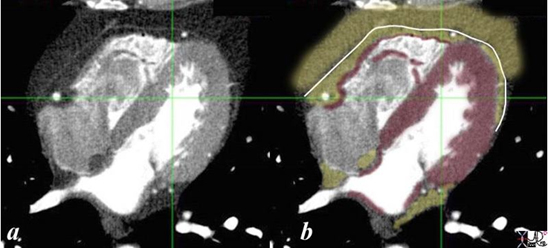
CT scanning is the digital form of X-ray evaluation characterizing tissue by revealing their densities. The myocardium is shown as a gray density in image a, and usually measures between 20 and 70 Hounsfield units, being on the low end before contrast and on the high end after contrast. In image b the myocardium is in maroon. The pericardial density is also soft tissue in nature and appears as a thin gray line in (a) and overlaid in white in b. Its CT density is also of a soft tissue nature. It is seen with exquisite detail in this image, despite it being submillimeter in thickness because it is surrounded by fat on either side. The epicardial and pericardial fat are lower density (light gray in a and overlaid in yellow in b). Contrast in the left side of the heart, coronary arteries and pulmonary veins is bright white because this study was timed to optimize the visualization of the coronary arteries. On the other side of the heart, unopacified blood (dark gray) is entering the right atrium at the tail end of the intravenous bolus injection, chasing the last portion of the bolus in the right ventricle which contains a combination of unopacified and opacified blood. A tiny dot of black air is seen in the anterior portion of the RV introduced during the injection. This small amount has no effect on the heart. Ashley Davidoff MD
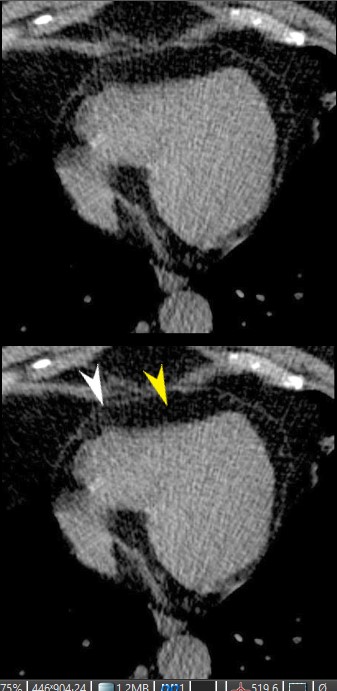
CT scan through the RV and LV shows epicardial fatty accumulation in the subendocardium of the right ventricle. The normal pericardium, (white arrowhead) and normal epicardial fat (yellow arrowhead) are shown in the lower images.
Ashley Davidoff MD
130641L
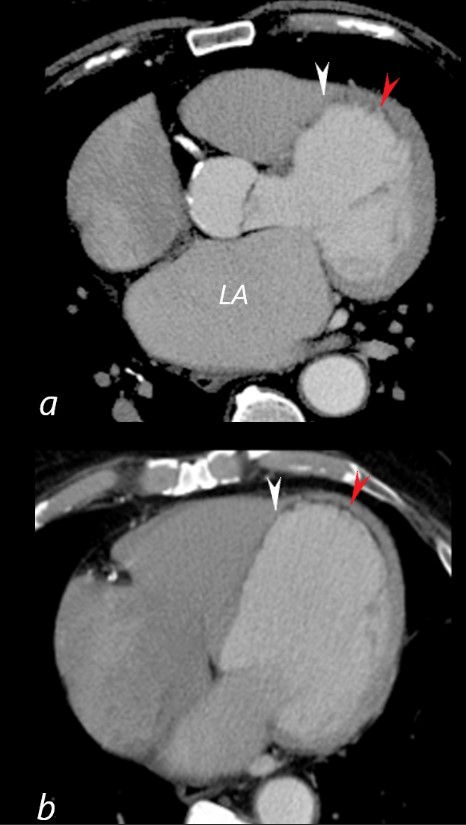
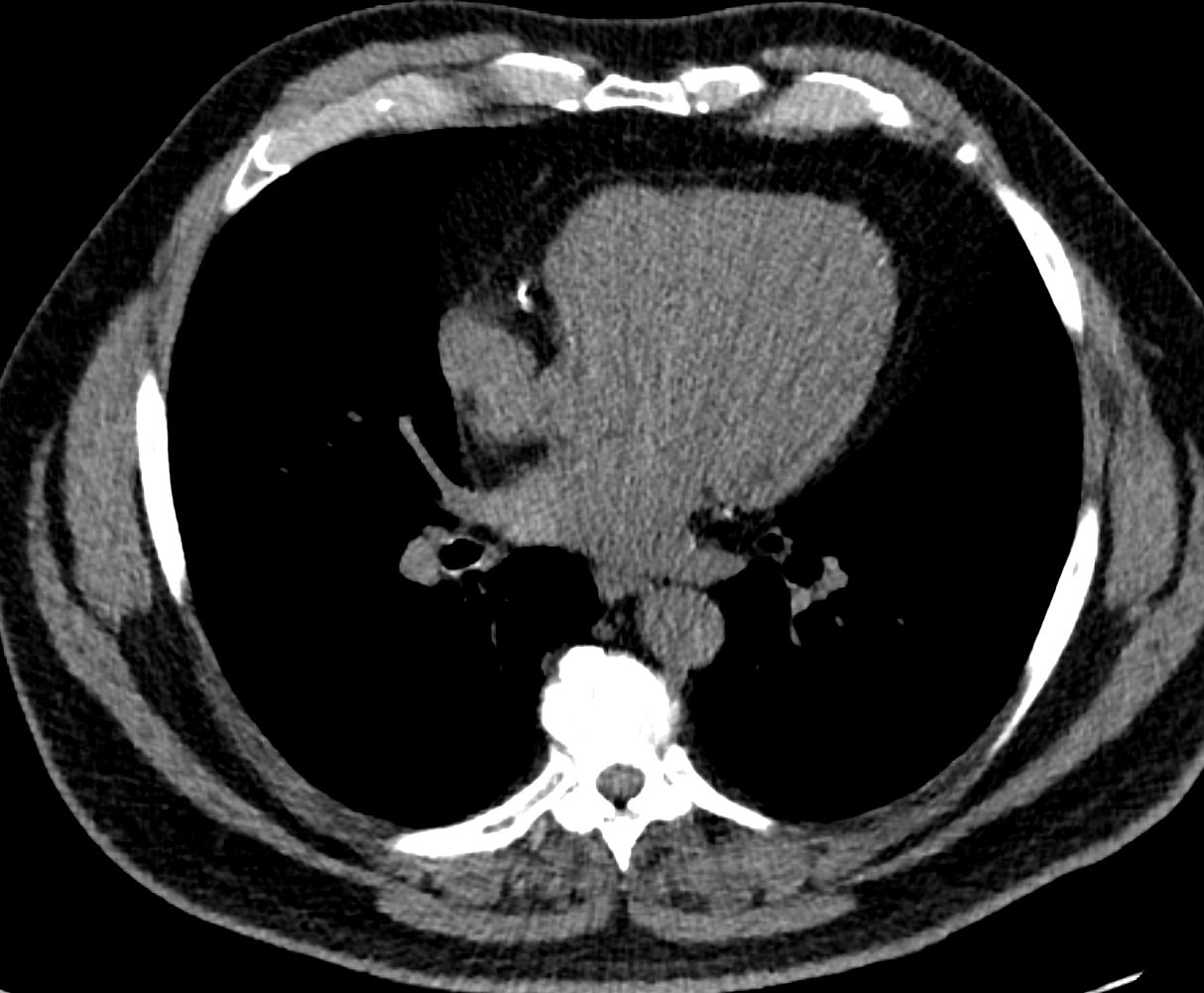
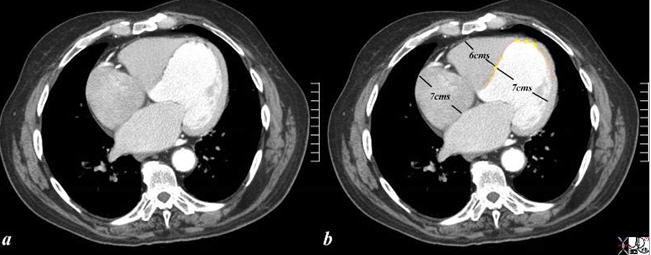
41 year old male presents with chest pain.
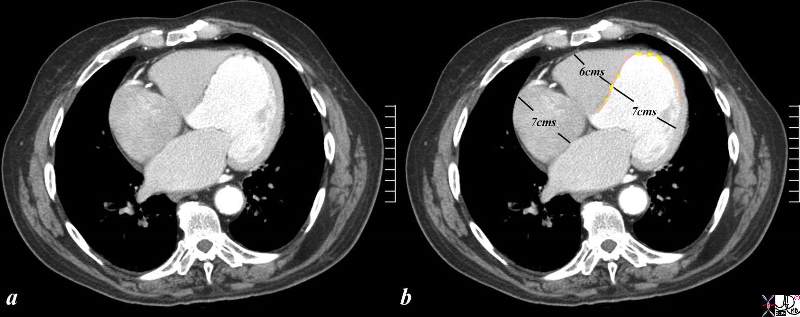
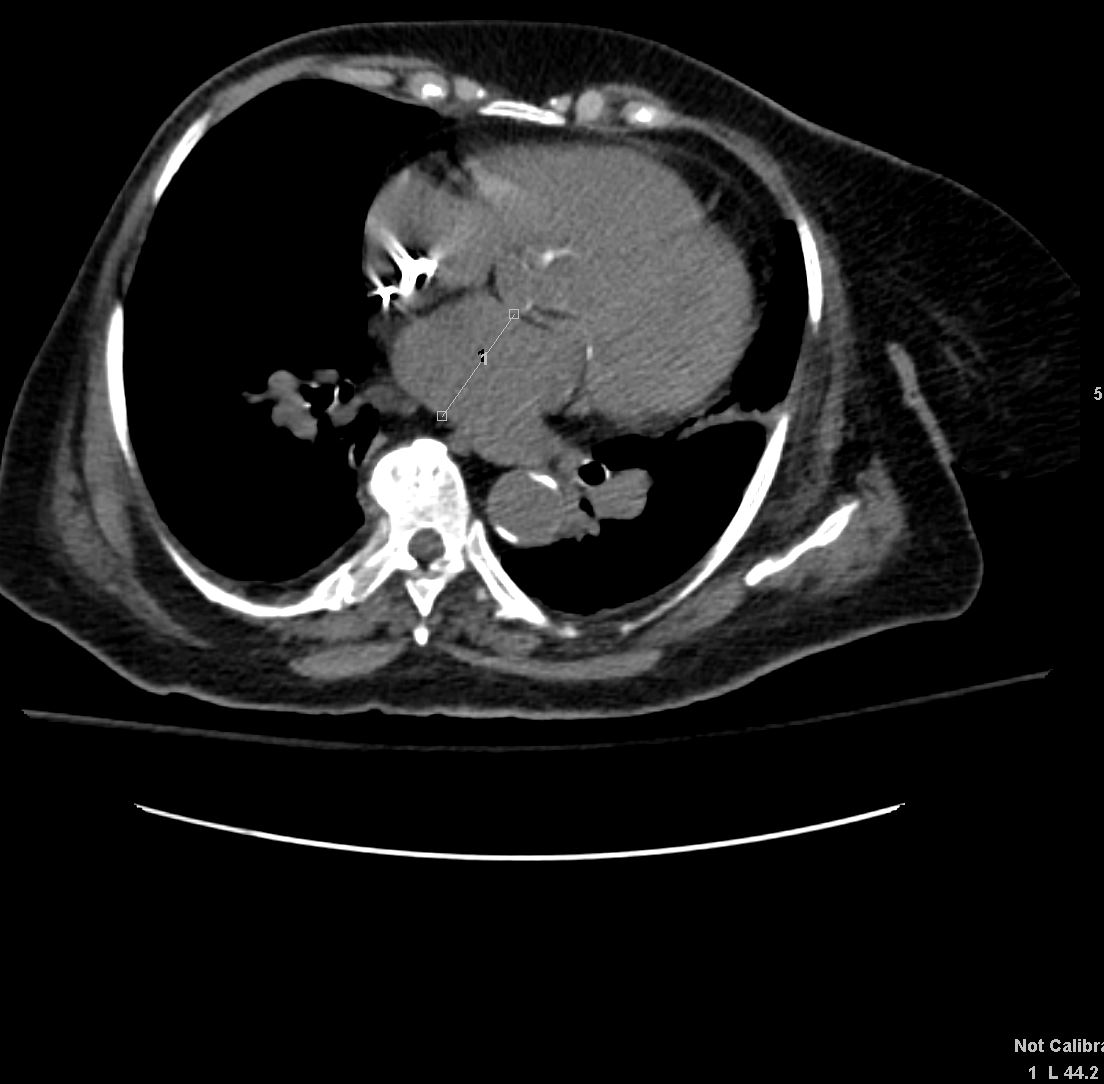
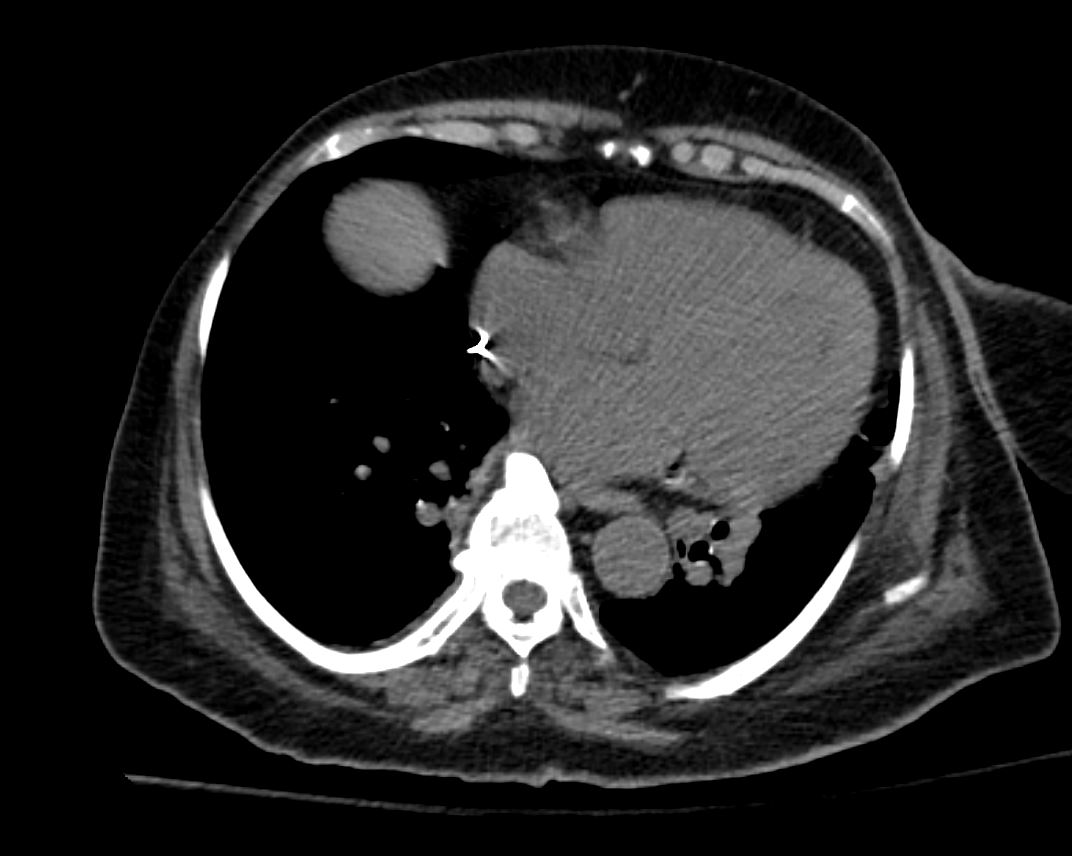
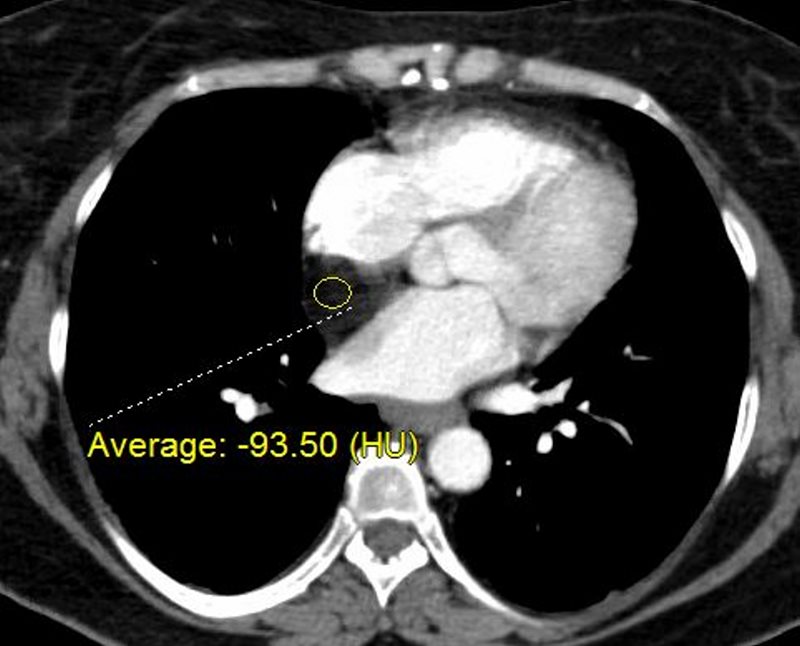
Axial CT with contrast at the level of the enlarged left atrium (LA) (a) reveals a dilated LV, with subendocardial fatty infiltration of the LV myocardium in the septum (white arrowhead), and apex red arrowhead). There is thinning of the myocardium in the septum and apex.
Image B is more inferior and taken at the level of the dilated RA and normal sized RV showing similar subendocardial fatty infiltration of the LV myocardium in the septum (white arrowhead), and apex red arrowhead). There is thinning of the myocardium in the septum and apex. The transverse dimension of the LV was 7.2 cms which is significantly dilated
These findings are consistent with myocardial infarction with and ischemic cardiomyopathy.
Ashley Davidoff MD
86943c03L
41 year old male presents with chest pain.
Axial CT without contrast (a) reveals aneurysmal calcification in the region of the proximal LAD,(red arrow). In image b is a similar image following contrast administration. The aneurysm is mostly thrombosed (red arrow). The calcification is approximately 2cms in size and represents a thrombosed aneurysm of the left coronary artery (LCA).
Imagesof the left ventricle ( c,d ) show a dilated LV, with subendocardial fatty infiltration of the LV myocardium in the septum, and apex (white arrowhead). There is thinning of the myocardium in the septum and apex.
These findings are consistent with myocardial infarction with and ischemic cardiomyopathy.
The left atrium (LA) is enlarged as noted in image d.
Ashley Davidoff MD
86943c01L01
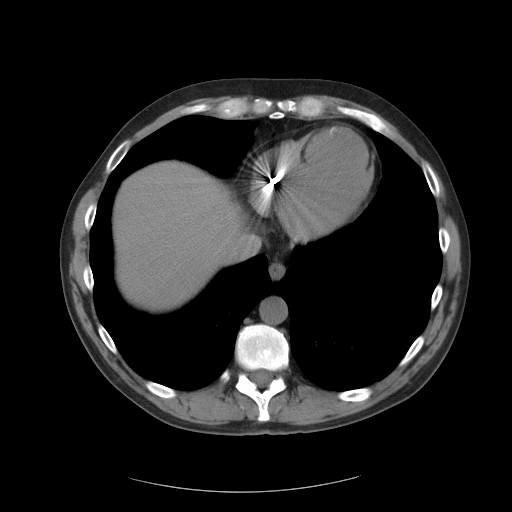
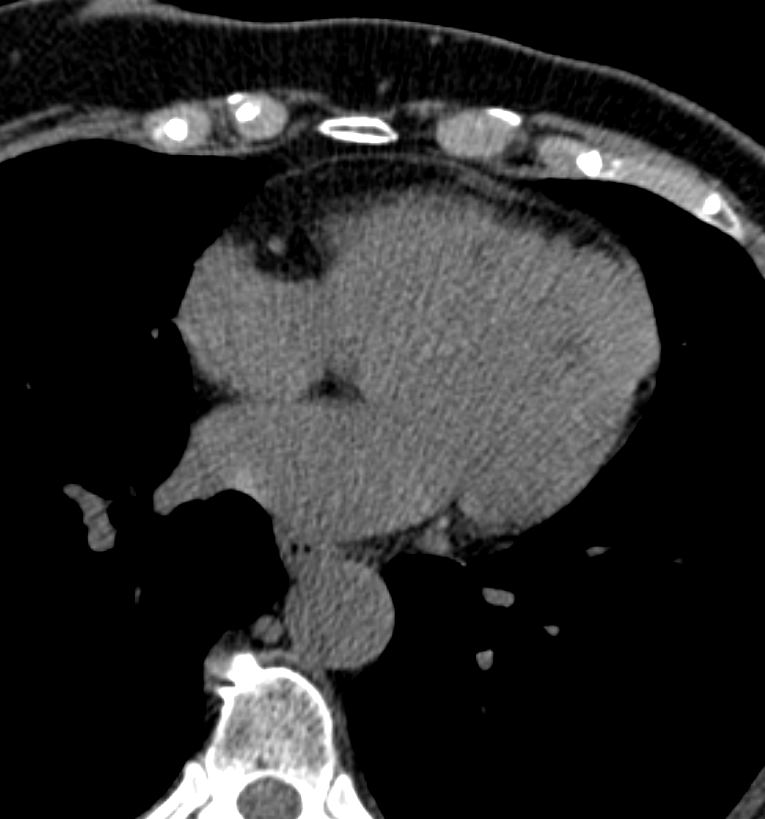
Axial CT through the left ventricle (LV) shows rounding of the apex and thinning of the overlying myocardium. This finding is consistent with an apical LV aneurysm most likely caused by LAD disease.
Note the fat dysplasia in the apical myocardium which conforms the prior infarct
Ashley Davidoff MD
0040 B heart 57 M aneurysm
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Courtesy of: Ashley Davidoff, M.D heart-anatomy-P-047