
55-year-old male with no prior history became unresponsive during exercise. Required CPR and defibrillation, and subsequently required epinephrine drip
Echo showed EF 50-55%, and normal cardiac chambers.
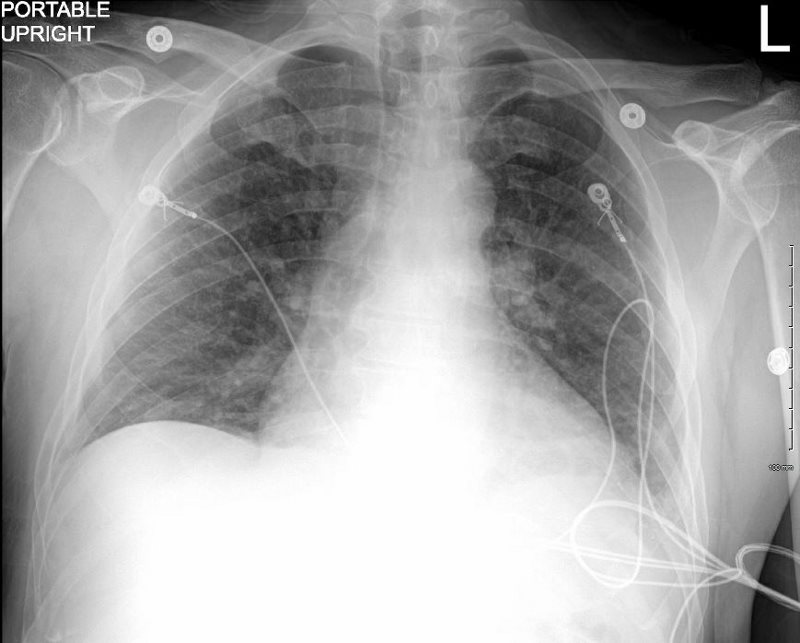
CXR showed CHF and LAE
Cardiac Cath showed normal coronaries, PCW 25 mm Hg
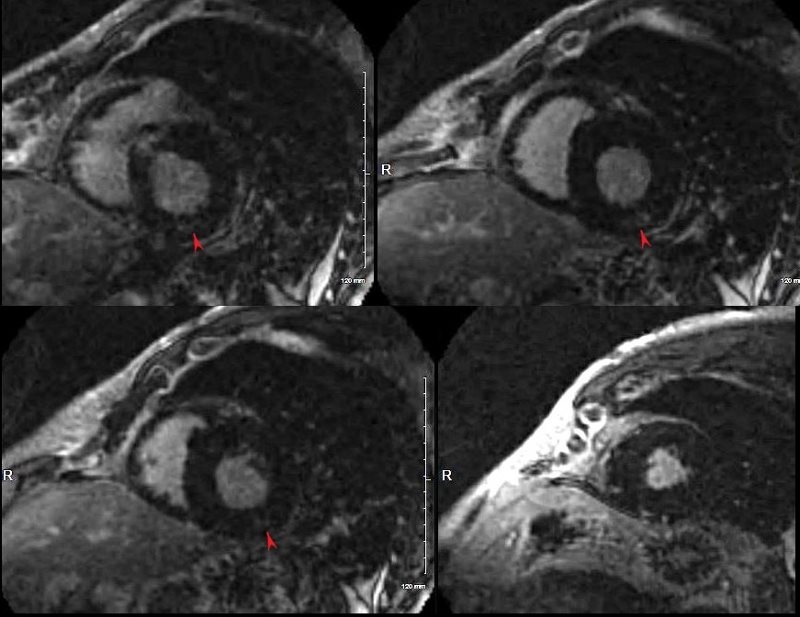
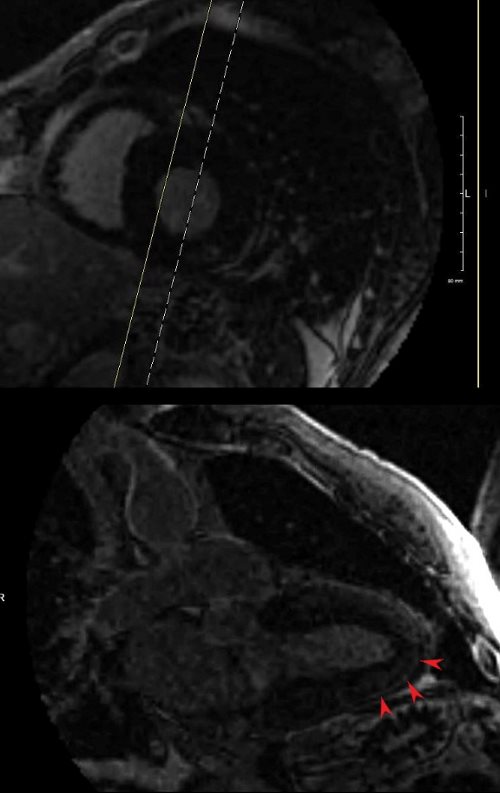
MRI showed mildly dilated LV and normal sized left atrium, right atrium and right ventricle. There was LGE in the mid myocardium in the apical anterior wall . Ejection fraction was 47% and myocardial mass was 61g/sqm. End diastolic volume was 160 ccs. Associated findings included bilateral pleural effusions. Finding were most consistent with a myocarditis, or sarcoidosis. Also included in the differential diagnosis was methamphetamine analogue use.
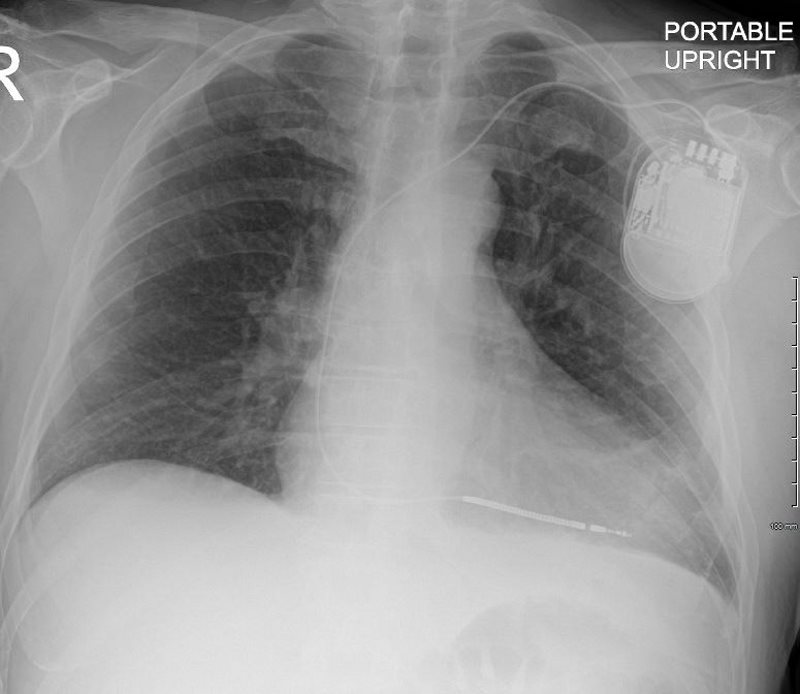
CXR following placement of a pacemaker/defibrillator showed improved CHF
Ashley Davidoff MD
Ashley Davidoff MD
Ashley Davidoff MD
Ashley Davidoff MD