
74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
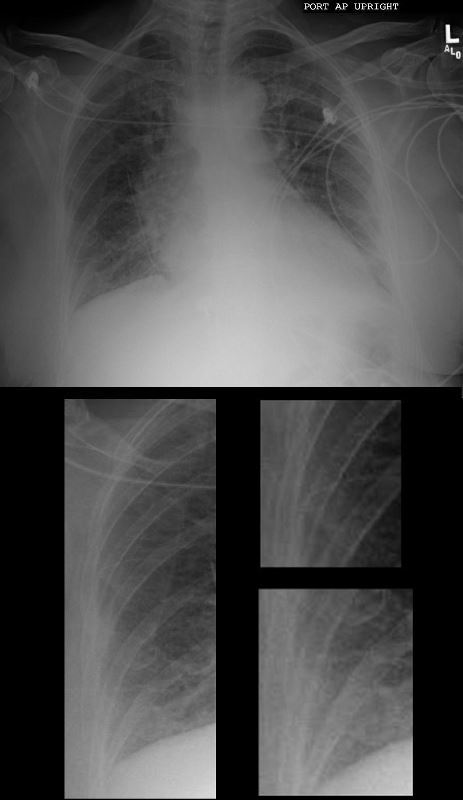
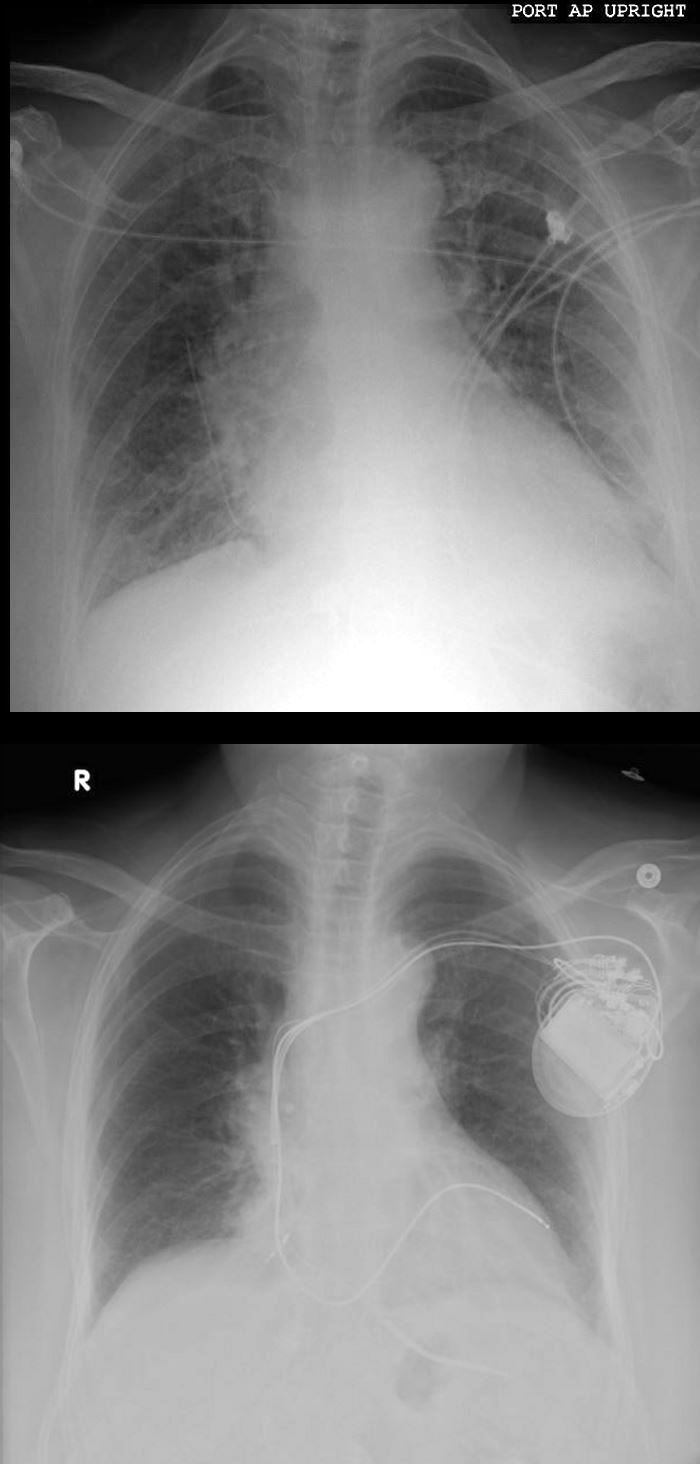
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Ashley Davidoff MD

74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Prior to implantation of a dual lead pacemaker she had a gated cardiac CT to define the venous anatomy.
The scout film shows an enlarged left atrium and suggestion of LV enlargement with right pleural effusion.
Ashley Davidoff MD

NON-COMPACTION AND CHF
Ashley Davidoff MD
74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Prior to implantation of a dual lead pacemaker she had a gated cardiac CT to define the venous anatomy.
The scout film shows an enlarged left atrium and suggestion of LV enlargement.
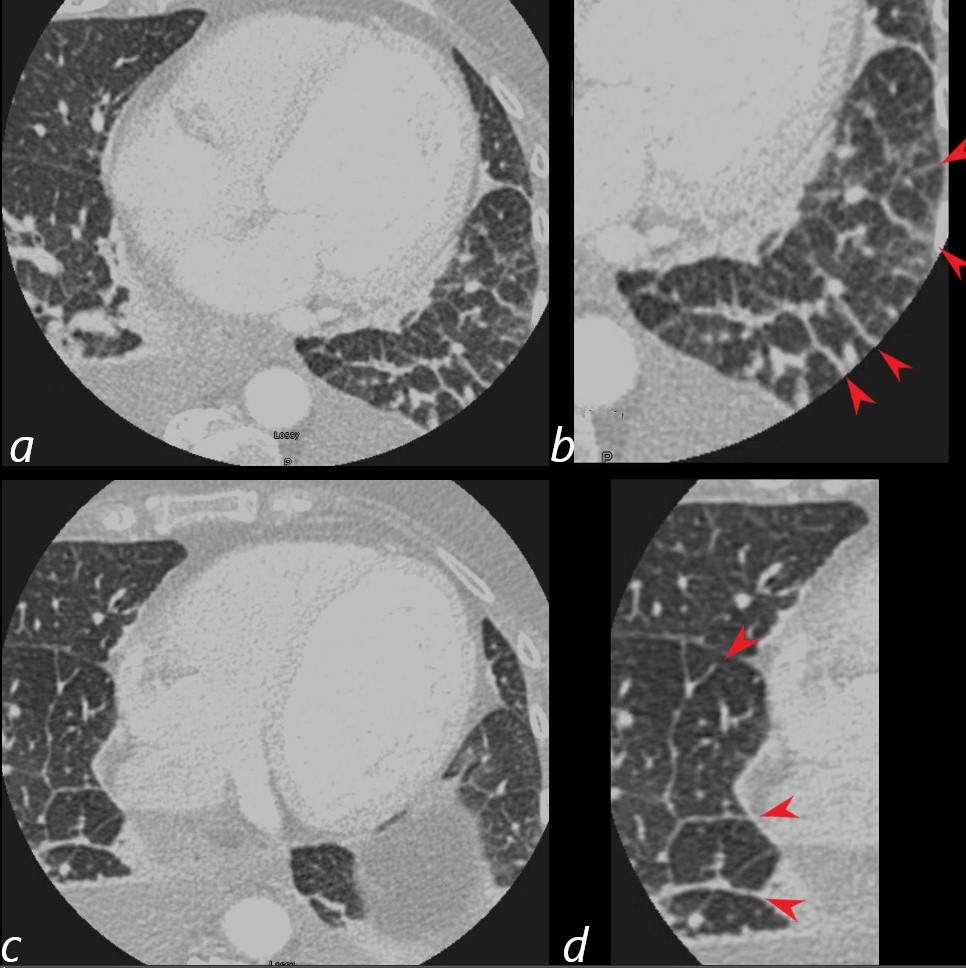
Lung windows confirmed the presence of prominent interlobular septa and LAE.
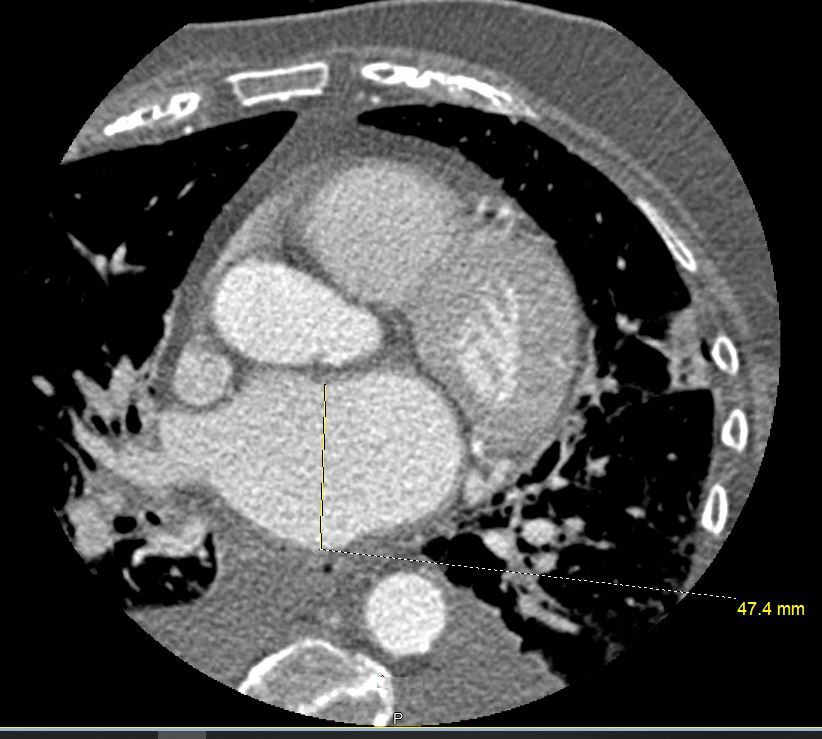
Axial soft tissue windows shows LAE with A_P dimension of 4.7cms (upper limits of normal is 4cms)
Ashley Davidoff MD
NON-COMPACTION AND CHF
74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Prior to implantation of a dual lead pacemaker she had a gated cardiac CT to define the venous anatomy.
The scout film shows an enlarged left atrium and suggestion of LV enlargement.
Lung windows confirmed the presence of prominent interlobular septa and LAE.
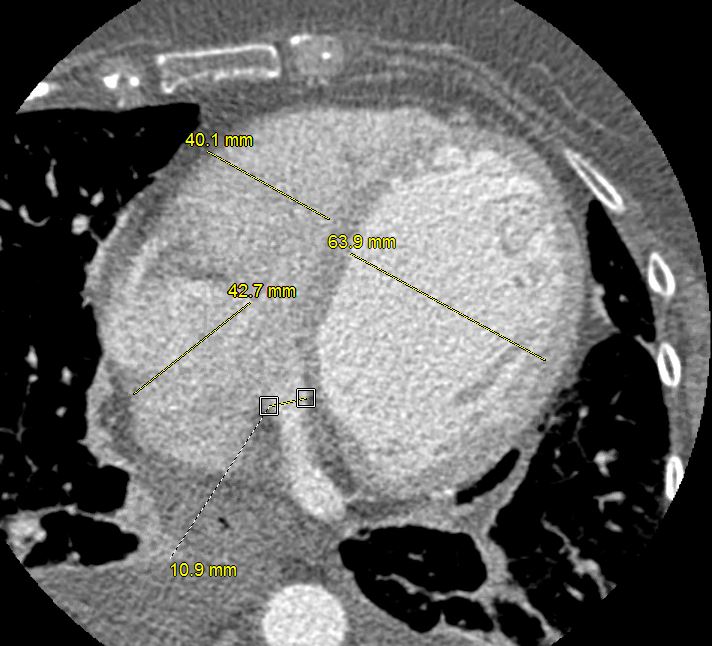
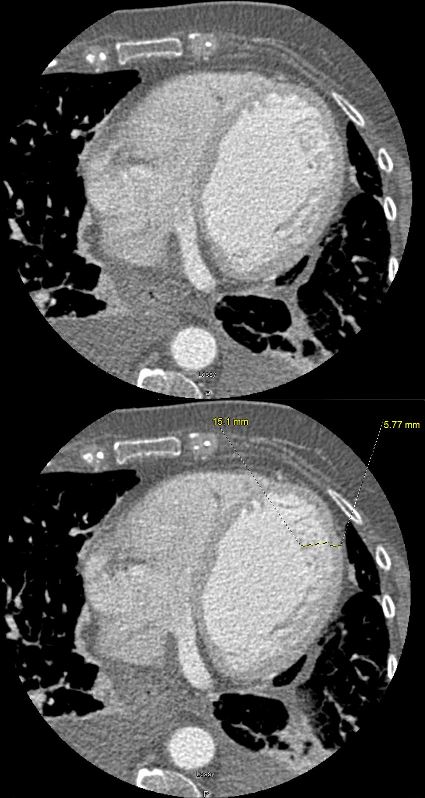
Axial soft tissue windows confirmed a diagnosis of non-compaction with non compaction thickness (NC) of 15mm and free wall thickness (C) of 6mm resulting in an abnormal NC:C ratio of 2.5 (upper limits normal NC:C ratio = 2.3)
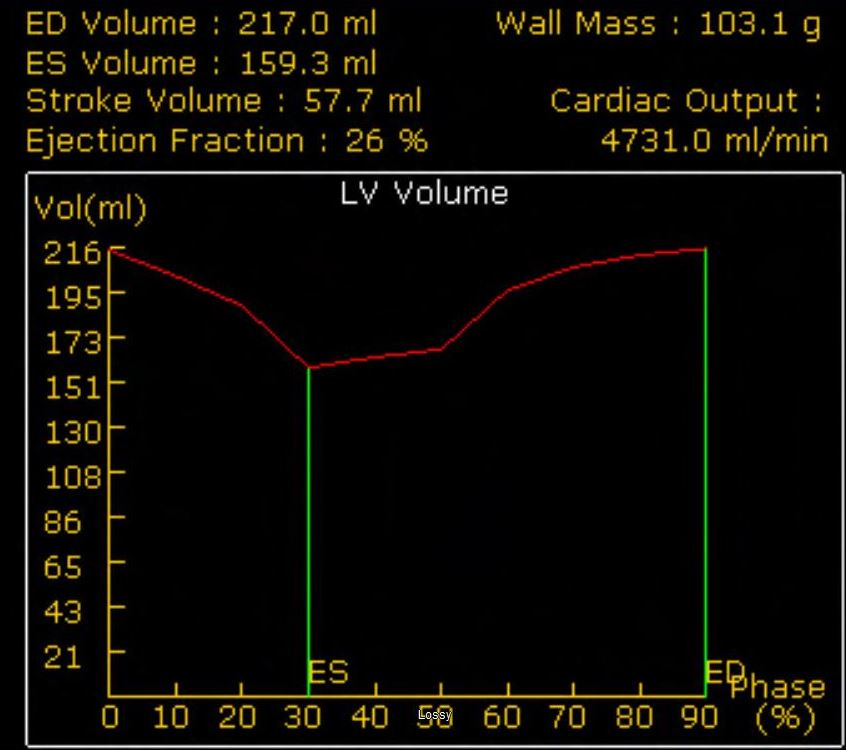
Volume measurements showed an end diastolic volume of 217 mls, an end systolic volume of 159ccs, a stroke volume of 58ccs with a resulting ejection fraction of 26%.
Ashley Davidoff MD
74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Prior to implantation of a dual lead pacemaker she had a gated cardiac CT to define the venous anatomy.
The scout film shows an enlarged left atrium and suggestion of LV enlargement.
Lung windows confirmed the presence of prominent interlobular septa and LAE.
Axial soft tissue windows confirmed a diagnosis of non-compaction with non compaction thickness (NC) of 15mm and free wall thickness (C) of 6mm resulting in an abnormal NC:C ratio of 2.5 (upper limits normal NC:C ratio = 2.3)
Volume measurements showed an end diastolic volume of 217 mls, an end systolic volume of 159ccs, a stroke volume of 58ccs with a resulting ejection fraction of 26%.
Ashley Davidoff MD

74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Prior to implantation of a dual lead pacemaker she had a gated cardiac CT to define the venous anatomy.
The scout film shows an enlarged left atrium and suggestion of LV enlargement.
Lung windows confirmed the presence of prominent interlobular septa and LAE.
Axial soft tissue windows confirmed a diagnosis of non-compaction with non compaction thickness (NC) of 15mm and free wall thickness (C) of 6mm resulting in an abnormal NC:C ratio of 2.5 (upper limits normal NC:C ratio = 2.3)
Volume measurements showed an end diastolic volume of 217 mls, an end systolic volume of 159ccs, a stroke volume of 58ccs with a resulting ejection fraction of 26%.
Ashley Davidoff MD
74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
Volume measurements based on the gated cardiac CT showed an end diastolic volume of 217 mls, an end systolic volume of 159ccs, a stroke volume of 58ccs with a resulting ejection fraction of 26%.
Ashley Davidoff MD (See LV volumes))
74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Prior to implantation of a dual lead pacemaker she had a gated cardiac CT to define the venous anatomy.
The scout film shows an enlarged left atrium and suggestion of LV enlargement.
Lung windows confirmed the presence of prominent interlobular septa and LAE with bilateral complex effusions.
Ashley Davidoff MD
74-year-old female presents in CHF and an echo showing reduced EF (35%) and non-compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Volume measurements showed an end diastolic volume of 217 mls, an end systolic volume of 159ccs, a stroke volume of 58ccs with a resulting ejection fraction of 26%.
Following placement of biventricular pacemaker CXR showed resolution of the heart failure, but persistence of the LAE.
Ashley Davidoff MD
References and Links
TCV References
- 003 Non Compaction Heart Failure and Pacemaker
- CXR Map
- CXR and CHF
- LA
- Left ventricle – LV
- Pacemakers
- CXR Map
Ebsteins Anomaly
ARVD
Non Compaction