
Ischemia
PRIOR INFARCTION
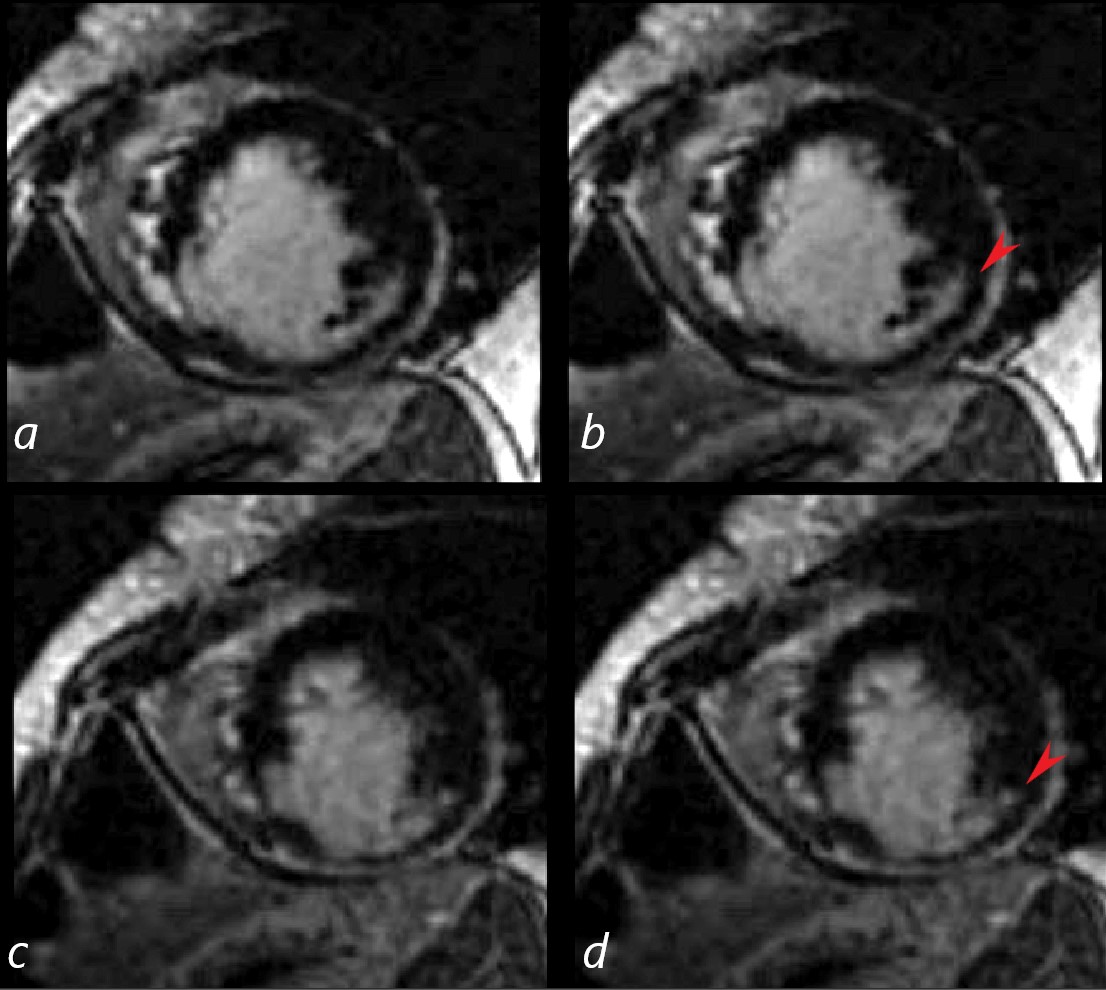
62 year old female with acute chest pain atrial fibrillation, hypotension admitted to ICU. Clinical evaluation was considered to be non-ischemic cardiomyopathy with EF by echo of about 20%. She was hypotensive and, in the ICU, and CXR showed acute CHF with cardiomegaly. The TEE was more in keeping with segmental dyssynergy, Cardiac cath showed occluded RCA bot good collateralization from the LAD. MRI showed subendocardial LGE in the inferior and inferolateral portions of the LV as shown in images b and d (red arrowheads) consistent with a prior infarction. EF of the LV was of 20%
Ashley Davidoff MD
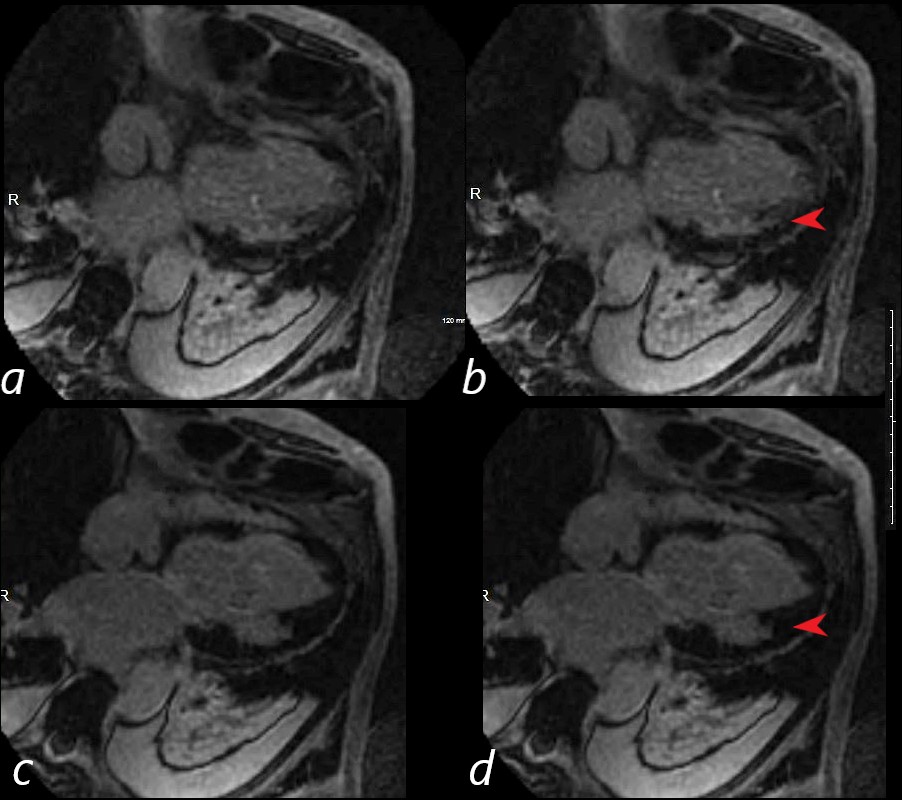
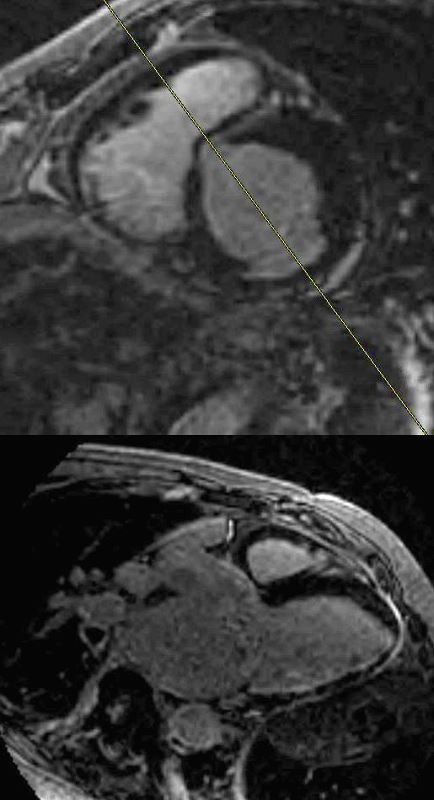
62 year old female with acute chest pain atrial fibrillation, hypotension admitted to ICU. Clinical evaluation was considered to be non-ischemic cardiomyopathy with EF by echo of about 20%. She was hypotensive and, in the ICU, and CXR showed acute CHF with cardiomegaly. The TEE was more in keeping with segmental dyssynergy, Cardiac cath showed occluded RCA bot good collateralization from the LAD. MRI showed subendocardial LGE in the inferior and inferolateral portions of the LV as shown in images b and d (red arrowheads) consistent with a prior infarction. The LGE occupies more than 50% of the myocardium. EF of the LV was of 20%
Ashley Davidoff MD
Prior Infarction
 SUBENDOCARDIAL LGE ? ISCHEMIA
SUBENDOCARDIAL LGE ? ISCHEMIA
76 year old male with history of ischemic heart disease . Delayed gadolinium enhancement shows intense subendocardial delayed gadolinium enhancement in the infero basal region of the left ventricle consistent with coronary artery ischemic disease
{kind=link}
Non Ischemic Cardiomyopathy
Amyloidosis
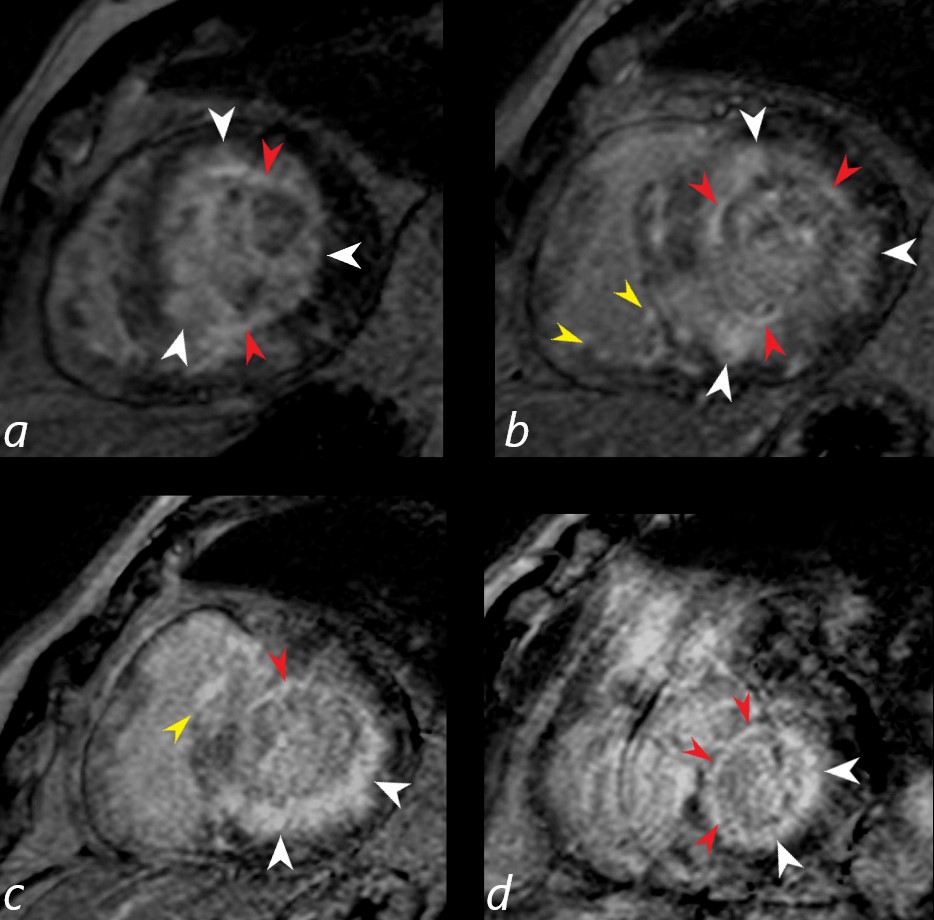
Gated short axis delayed gadolinium sequence through the base LV during diastole and shows subendocardial LGE (red arrowheads in a,b,c, and d, diffuse mid myocardial LGE (white arrowheads) (a,b,c,d) and subepicardial LGE in the RV (yellow arrowheads (b,c)
Ashley Davidoff MD Case 006
Dilated Cardiomyopathy
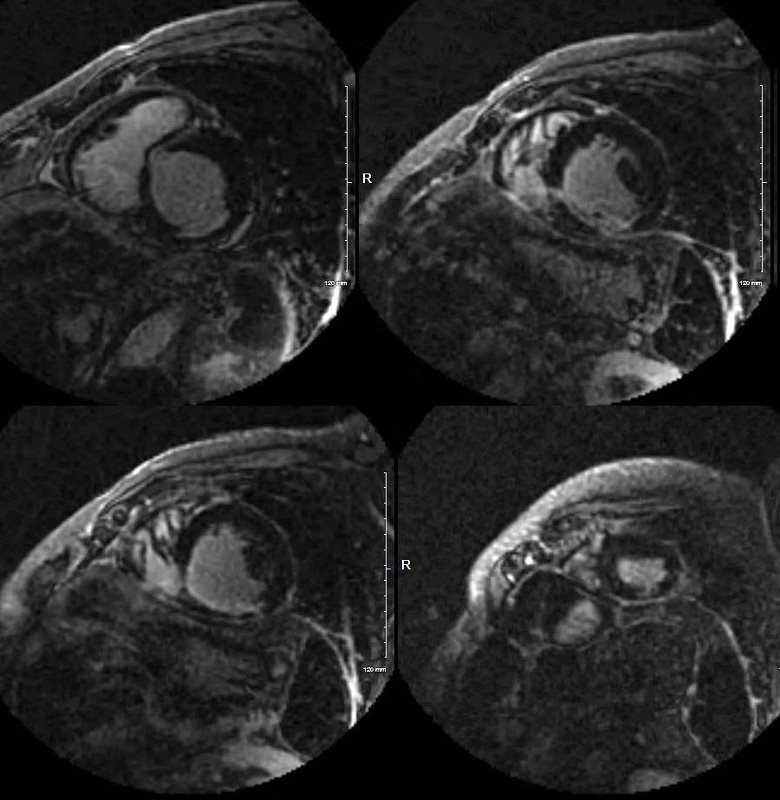
MRI showed LV mass of 113g/m sq and extensive subendocardial LGE involving apex, and inferior wall with minor mid myocardial nodular LGE at inferior septal region and linear in the anterior wall
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD Case 013
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD Case 013
References and Links