
27-year-old female presents with dyspnea and a past history of SLE, Raynaud?s disease, and Lupus nephritis.
Chest X-ray shows cardiomegaly with right ventricular configuration on the PA and an enlarged main and probably left pulmonary and an enlarged descending RPA. The lateral confirms the enlarged RV and raises the possibility of LV enlargement.
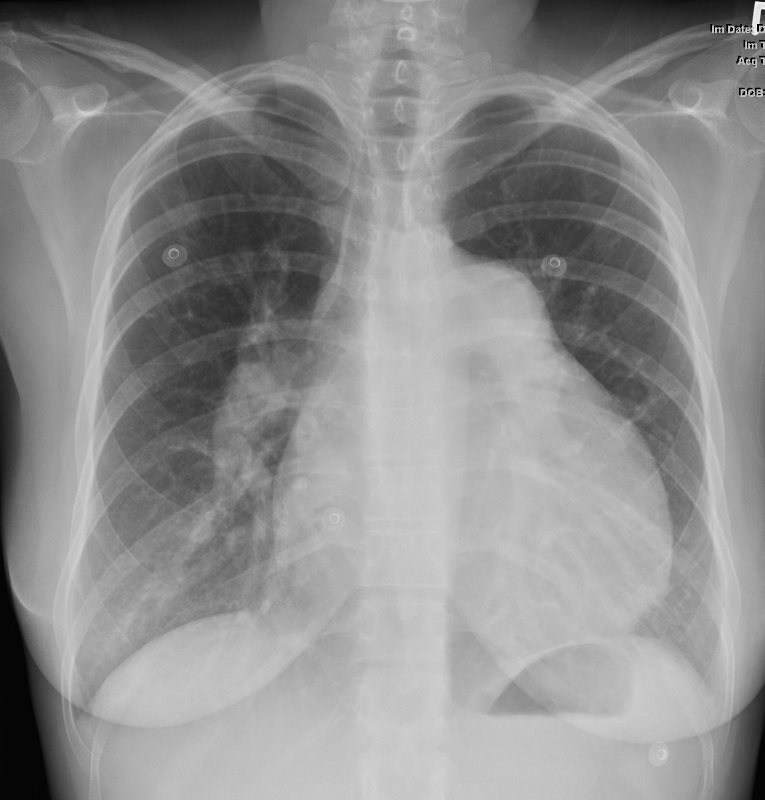 CARDIOMEGALY WITH RVE and LARGE PA Ashley Davidoff MD
CARDIOMEGALY WITH RVE and LARGE PA Ashley Davidoff MD
{kind=link}

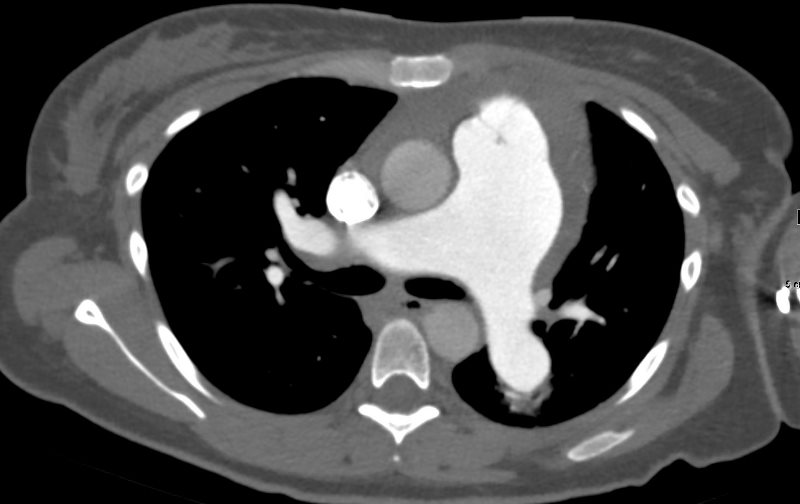
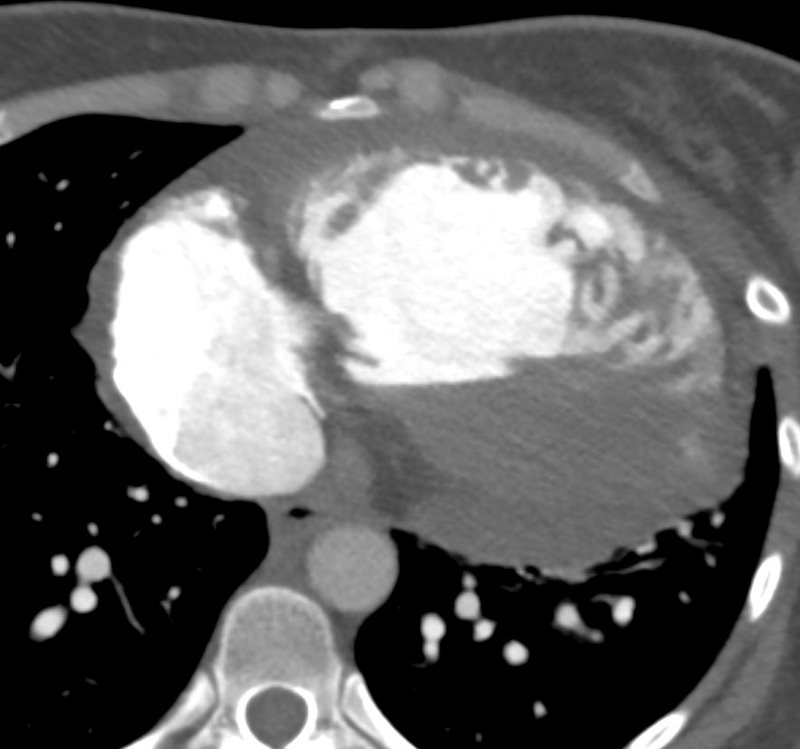
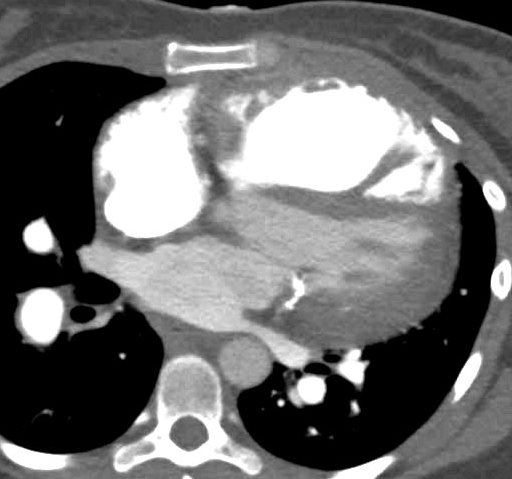
SLE and PULMONARY HYPERTENSION without ILD
Ashley Davidoff MD
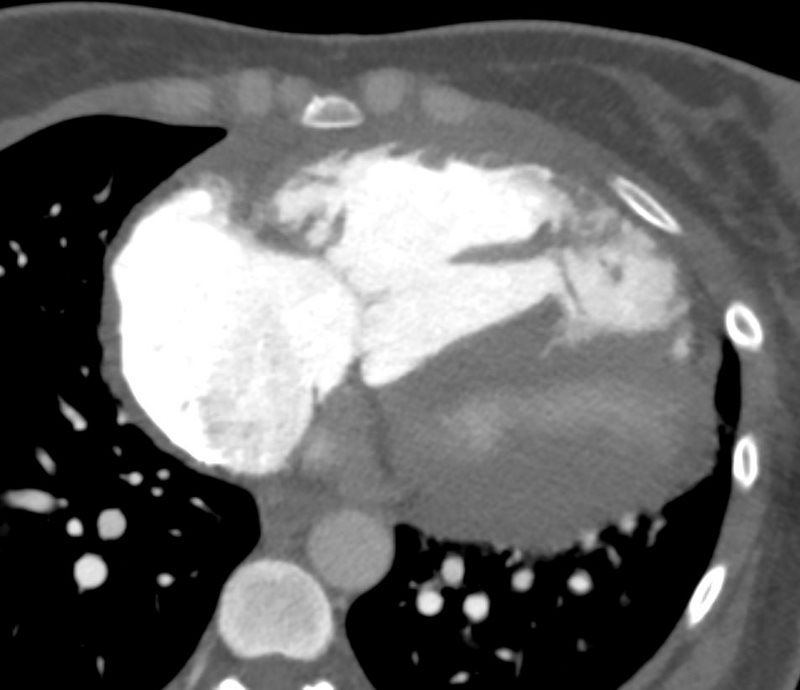
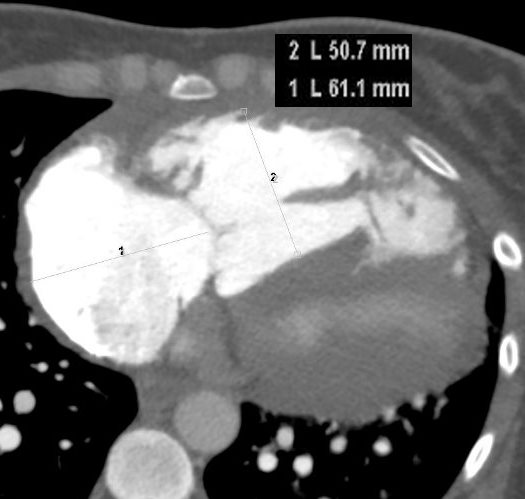
The CT scan confirms an enlarged MPA, RPA, RA and RV, and shows calcification on the posterior leaflet of the mitral valve consistent with Libman Sacks vegetation. There is mild ground glass opacity at the lung bases but no sign of ILD.
Ashley Davidoff MD
Ashley Davidoff MD
Ashley Davidoff MD
Ashley Davidoff MD

Ashley Davidoff MD
- murantic or verrucous endocarditis, is a form of

Ashley Davidoff MD
Ashley Davidoff MD

Ashley Davidoff MD

Ashley Davidoff MD

Ashley Davidoff MD
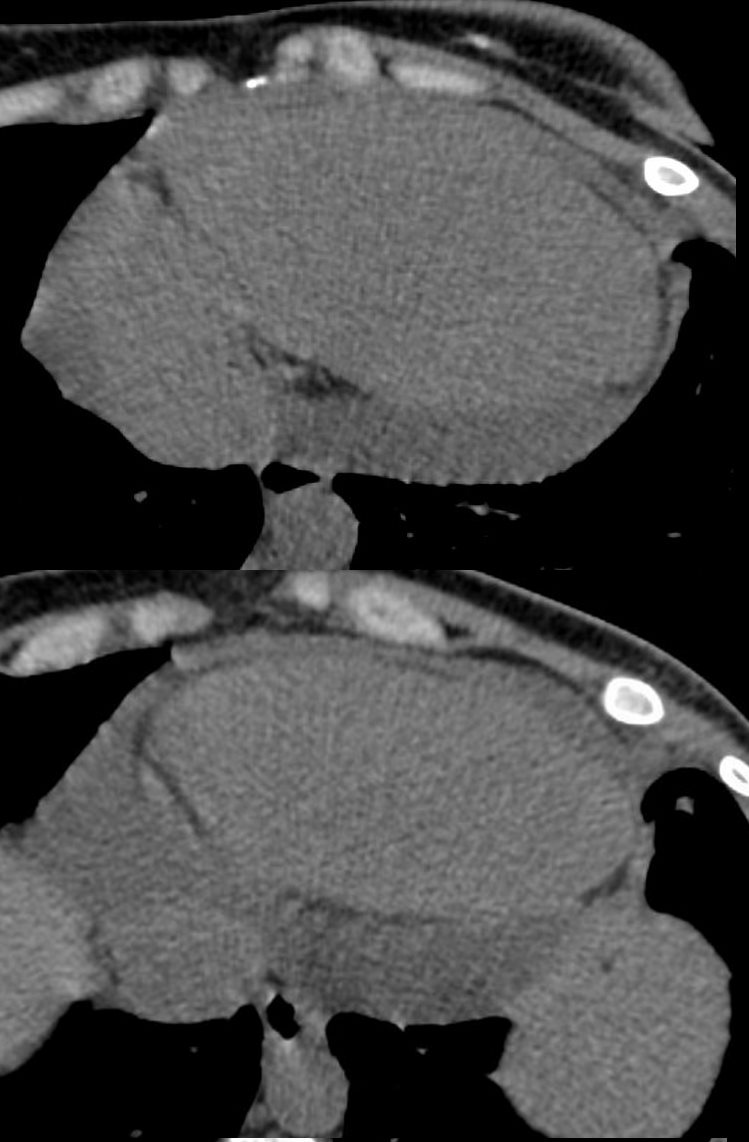
A current non contrast abdominal CT shows a pericardial effusion
Ashley Davidoff MD