
Assessment of pulmonary hypertension (PH) on a chest X-ray is limited, as this imaging modality is not very sensitive for detecting changes in the pulmonary vasculature. However, certain features on a chest X-ray may suggest the presence of PH, and further imaging studies and clinical evaluation may be necessary to confirm the diagnosis.
Here are some features on a chest X-ray that may suggest the presence of PH:
Enlargement of the main pulmonary artery: The main pulmonary artery may appear enlarged on a chest X-ray in cases of PH.
The Main Pulmonary Artery
Normal

When a line is drawn from the aortic knob to the left edge of the heart, (red line) the pulmonary artery should lie medial to that line (ie along the line drawn to 1.5cms medial to the line)
Ashley Davidoff MD TheCommonVein.net
Pulmonary Hypertension
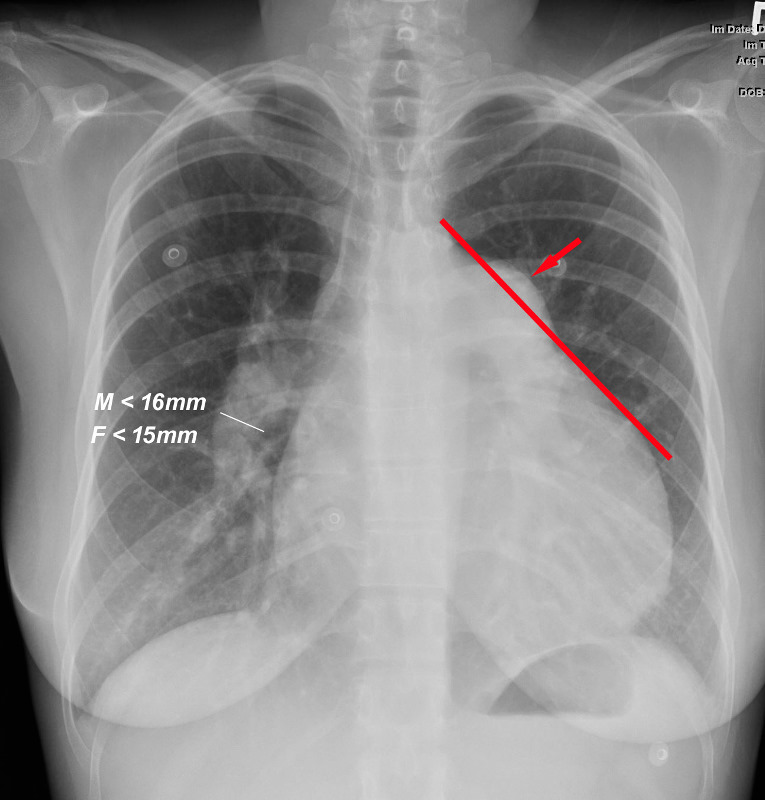
When a line is drawn from the aortic knob to the left edge of the heart, (red line) the pulmonary artery lies lateral to that line indicating an enlarged pulmonary artery most commonly caused by hypertension . In this instance the size of the descending right pulmonary artery is greater than 15 mms confirming the presence of pulmonary hypertension
Ashley Davidoff MD TheCommonVein.net
27-year-old female presents with dyspnea and a past history of SLE, Raynaud?s disease, and Lupus nephritis.
Chest X-ray shows cardiomegaly with right ventricular configuration on the PA and an enlarged main and probably left pulmonary and an enlarged descending RPA. The lateral confirms the enlarged RV and raises the possibility of LV enlargement.
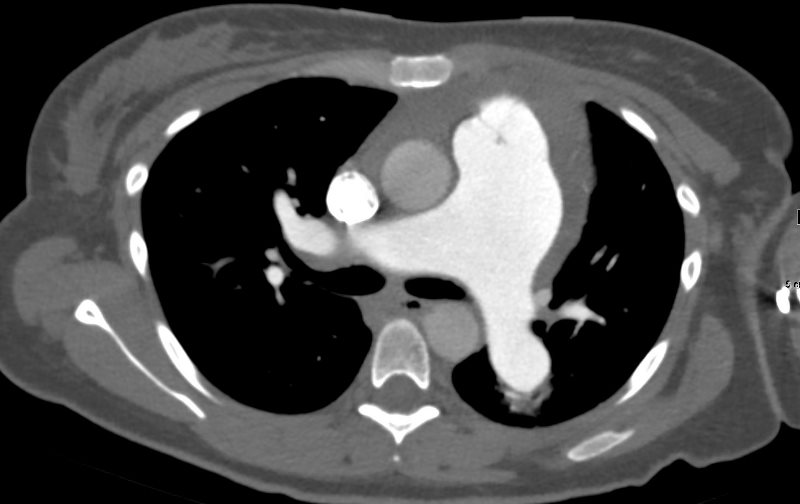
The CT scan confirms an enlarged MPA, RPA, RA and RV, and shows calcification on the posterior leaflet of the mitral valve consistent with Libman Sacks vegetation. There is mild ground glass opacity at the lung bases but no sign of ILD.
-
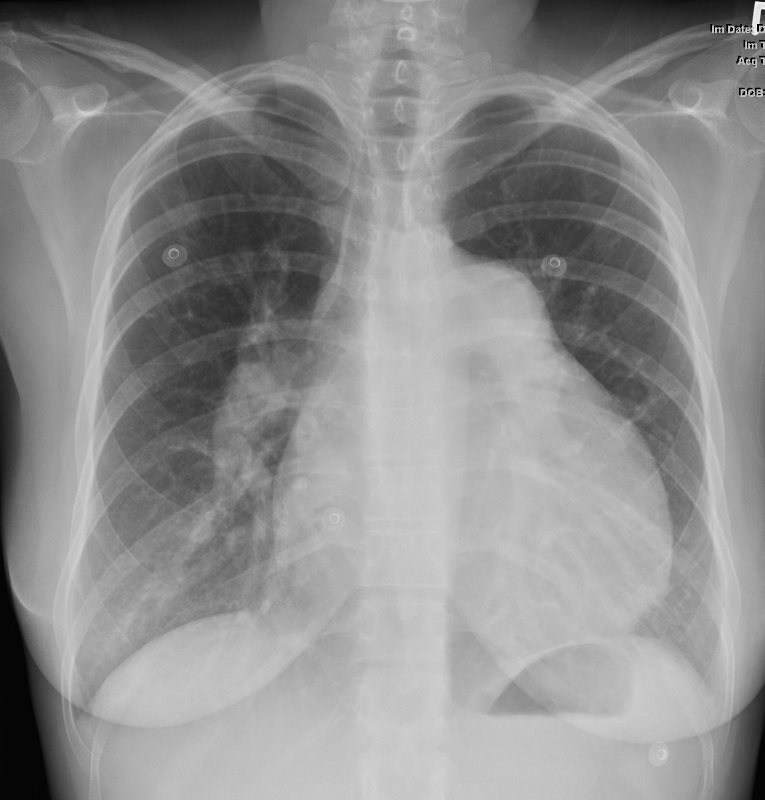
CARDIOMEGALY WITH RVE and LARGE PA
SLE and PULMONARY HYPERTENSION without ILDA current non contrast abdominal CT shows a pericardial effusion and normal sized kidneys
Ashley Davidoff MD -
LARGE PA SLE and PULMONARY HYPERTENSION without ILD
27-year-old female presents with dyspnea and a past history of SLE, Raynaud?s disease, and Lupus nephritis.
Chest X-ray shows cardiomegaly with right ventricular configuration on the PA and an enlarged main and probably left pulmonary and an enlarged descending RPA. The lateral confirms the enlarged RV and raises the possibility of LV enlargement.
The CT scan confirms an enlarged MPA, RPA, RA and RV, and shows calcification on the posterior leaflet of the mitral valve consistent with Libman Sacks vegetation. There is mild ground glass opacity at the lung bases but no sign of ILD.
A current non contrast abdominal CT shows a pericardial effusion and normal sized kidneys
Ashley Davidoff MD -

SLE and PULMONARY HYPERTENSION without ILD
Ashley Davidoff MD -

RVE AND RVH, LIBMAN SACKS
SLE and PULMONARY HYPERTENSION without ILD
Ashley Davidoff MD - References and Links