
78 year old male with PMH CAD MI x3 s/p PCI X3 in 18 years ago, dementia, p/w SOB cardiogenic shock Intubated for hypoxemic respiratory failure new MI suspected, new q waves elevated troponins Echo in the ER showed EF of 30-40%- septal and apical hypokinesis Cath showed LM occlusion by thrombus. There was complete occlusion of mid LAD stent.
PCI and then IABP for 24 hours with improvement
Repeated episodes of VT and Rxed for infection
Negative COVID
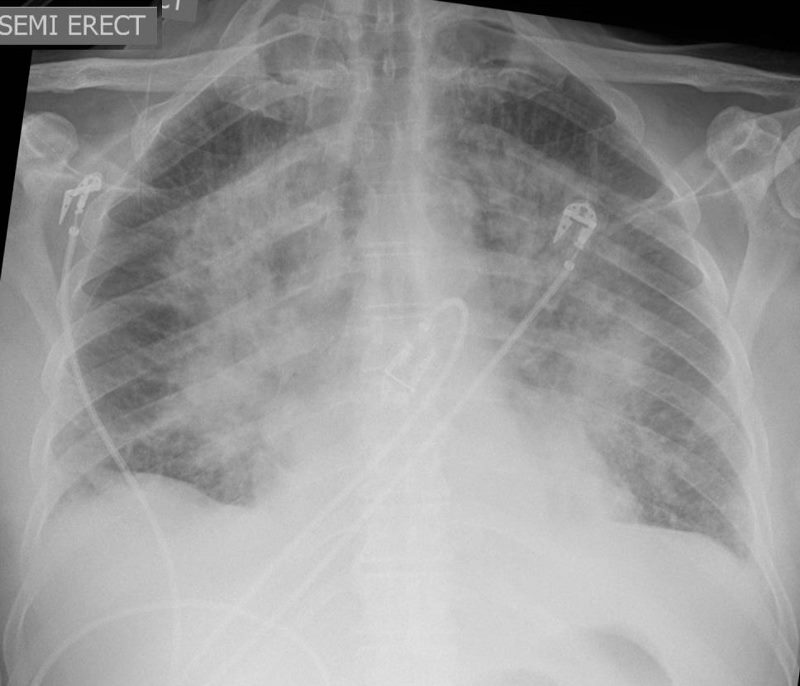
CXR performed on shows perihilar infiltrates with air bronchograms consistent with alveolar edema. The left atrium is enlarged. The peripheral lung is relatively spared. These findings are consistent with acute severe CHF with PCW pressure that is in the 30 mmHg range.
Ashley Davidoff MD
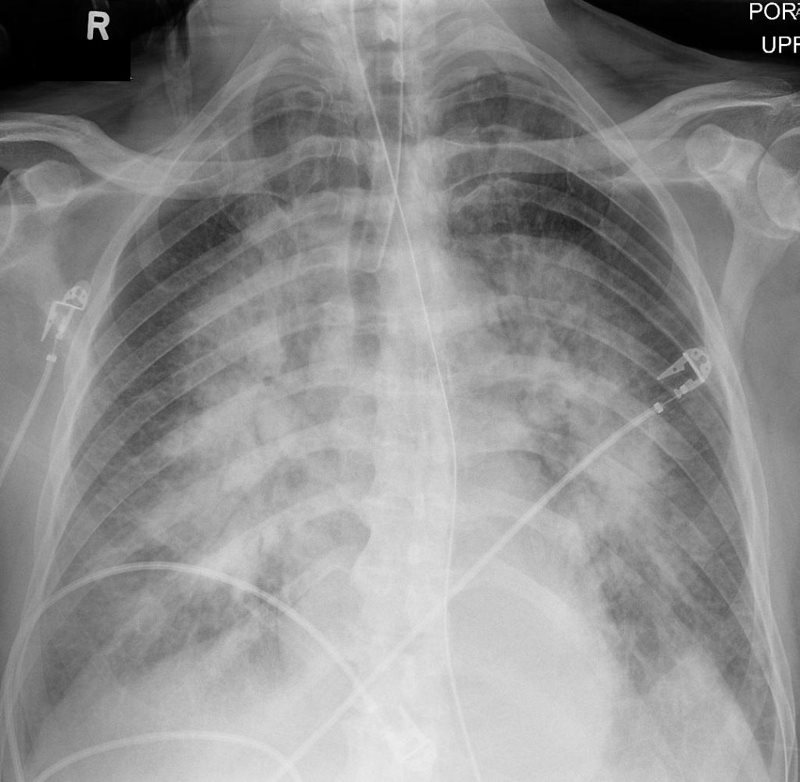
CXR performed 1 hour later following intubation shows persistent but improving perihilar infiltrate with air bronchograms consistent with alveolar edema
Ashley Davidoff MD
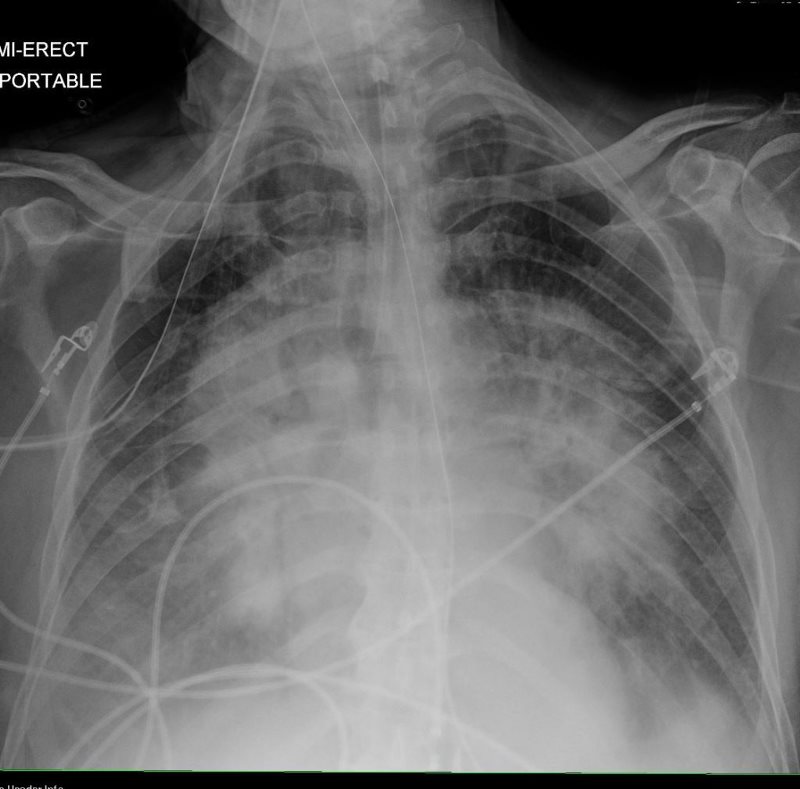
CXR performed 5 hours later shows persistent perihilar infiltrate (batwing pattern) with air bronchograms interstitial edema, Kerley B lines and bilateral pleural effusions, consistent with alveolar/pulmonary edema
Ashley Davidoff MD

CXR performed 2 days later shows persistent but improving perihilar infiltrate (batwing pattern) with air bronchograms, improving interstitial edema, bilateral pleural effusions, consistent with improving alveolar/pulmonary edema. Note is made of Swan Ganz line and IABP (Intra-aortic Balloon Pump)
Ashley Davidoff
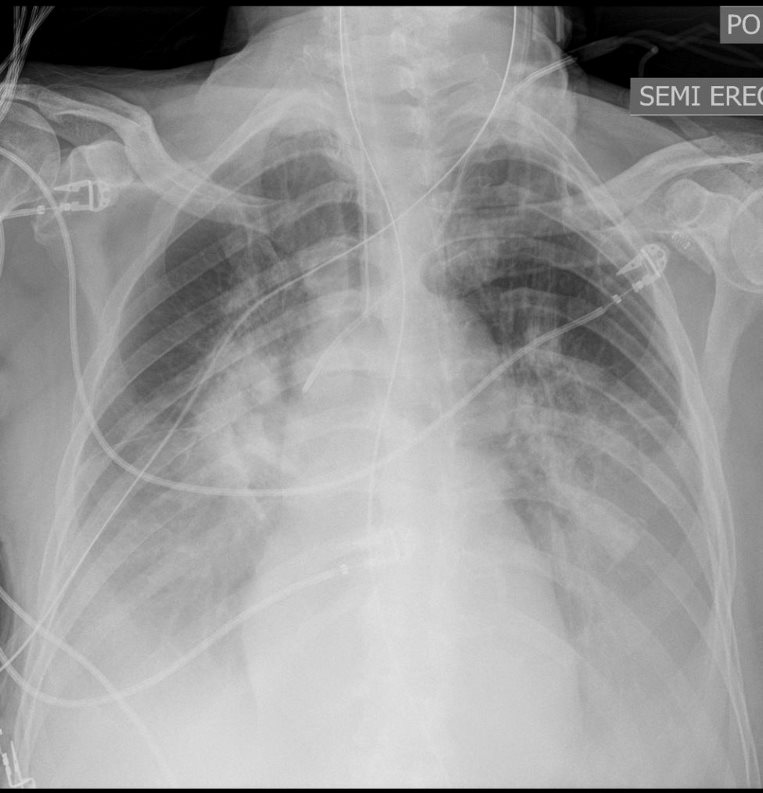
CXR performed on day 10 shows persistent but improving perihilar infiltrate but increasing bilateral pleural effusions. The Swan Ganz line and IABP (Intra-aortic Balloon Pump) have been discontinued
Ashley Davidoff MD