
Tricuspid Valve
Copyright 2009
Definition
The Tricuspid Valve is the right atrioventricular valve, placed between the right atrium and the right ventricle. Structurally its components include a fibrous annular ring, leaflet tissue, chordae tendineae, and papillary muscles. Functionally it guards the inlet of the right ventricle and also directs flow toward the outflow segment during systole.
Diseases of the tricuspid valve may be primary (intrinsic valve disease- Ebstein anomaly, Infective endocarditis, carcinoid heart disease) or secondary (subsequent to left heart disease).
Diagnosis of primary tricuspid
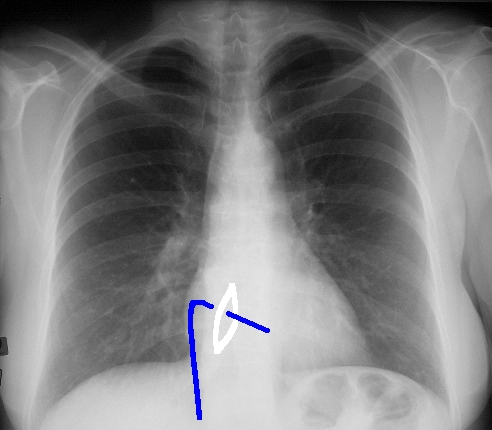
valve disease is rarely suspected, as these group of disorders receives less attention both clinically and in the literature because of their rarity. However an almost invariable consequence of tricuspid valve disease either stenosis or incompetence is elevated right atrial pressure (1) which promotes systemic venous congestion and may manifests clinically with engorged neck veins, elevated jugular venous pressures, hepatic congestion, abdominal edema and bilateral pitting pedal edema. Chest radiography may show RV enlargement in some cases but is not specific for tricuspid disease. EKG too is non specific and but may provide corroborative evidence in the form of right ventricular hypertrophy and ?strain? with right axis duration or right atrial enlargement with prominent tall P-waves (2). Two dimensional echocardiography with spectral and color flow Doppler evaluation provides anatomical and functional assessment of the tricuspid valve and is the most definitive modality for diagnosing tricuspid valve disease (2). Transesophageal echocardiography is indicated for better anatomic definitions of the valve lesions or precise measurement of the tricuspid annulus (2). Prior to the advent of diagnostic echocardiography, cardiac catheterization was used to confirm the presence and severity of tricuspid stenosis, but should rarely, if ever, be undertaken in this era (2).
Structural Considerations:
The tricuspid valve, so called because of its three triangular or trapezoidal leaflets , is the most apically (or caudally) placed valve (2)and with the largest orifice (11.0 cm circumference on average 1 )among the four valves of the heart . The tricuspid valve complex includes the fibrous annular ring, leaflet tissue, chordae tendineae, and papillary muscles.
Tricuspid annulus: The fibrous annulus, oval in shape expands in diastole when it becomes circular to provides for unimpeded inflow and constricts during mid systole to provide effective valve closure (2). It has an average major diameter on two-dimensional echocardiography of 3.0 to 3.5 cm in adults and an annular orifice area about 20% larger than that of the left sided mitral valve to provide for RV inflow to occur at a lower velocities (peak early velocities <1.0 m/s )and lower pressure drops (mean gradient across the tricuspid orifice in diastole being < 2 mm Hg) relative to those on the left side of the heart 2.
Leaflets: The tricuspid valve has three leaflets ? one each large, anterior and septal leaflets and a small functionally insignificant posterior one (2).
The septal leaflet unique to the tricuspid valve attaches to both membranous and muscular portions of the septum and is displaced toward the apex relative to the anterior mitral leaflet (1). The anterior leaflet is attached to the anterolateral margin.
Papillary muscles: There are three groups of papillary muscles (anterior, posterior and septal),. Septal papillary muscle ? as the name suggests arises from the septum, Anterior papillary muscle ? largest and most prominent arises from the anterior wall while the posterior papillary muscle which may consist of several parts arises from the inferior wall. The origin of papillary muscles from the septal surface is a unique feature of the right ventricle (3).
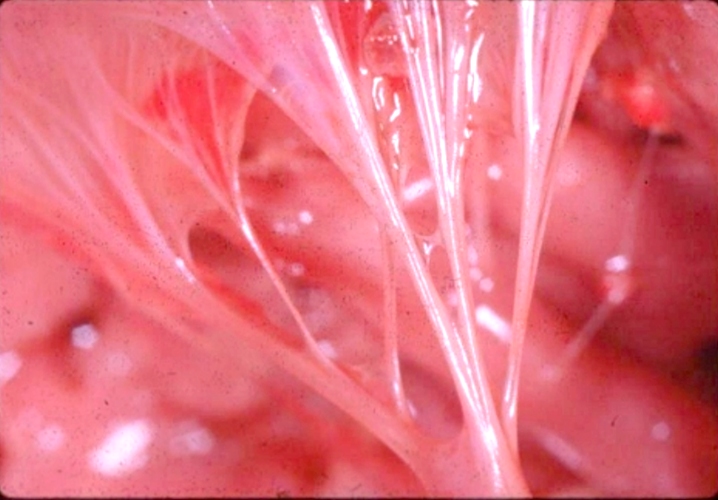
Chordae: The chordae arising from the papillary muscles inserted into two adjacent leaflet (2). Anterior papillary muscle chordae (anterior and posterior leaflets), Posterior papillary muscle chordate (posterior and septal) and Septal chordae (anterior and septal leaflet). This attachment of cords to adjacent leaflets , prevents their separation and inversion when tension is applied during ventricular systole.
One other unique feature of the tricuspid valve is the direct attachment of chords from the septal leaflet into the septum (3).Chordal attachments to the septal surface are never seen in the morphologically left ventricle except when the tricuspid valve straddles and inserts on to the left ventricular septal aspect (3).
Functional Considerations:
The valve by dilation of the annulus and relaxation of the chordate during diastole allows inflow into the right ventricle. The opposite accounts for systolic narrowing to prevent backward flow into the right atrium and to direct flow into the RVOT. More on functional aspects are discussed in the physiology section of the heart module.
Clinical Considerations:
50 to 60% of young adults exhibit mild tricuspid regurgitation on two-dimensional echocardiography (2).
Septal attachment of the tricuspid leaflet , in immediate proximity of the membranous ventricular septum provides a basis for spontaneous closure of perimembranous VSD (2).
References :
Blaustein A and Ramanathan A . TRICUSPID VALVE DISEASE Clinical Evaluation, Physiopathology, and Management. Cardiology Clinics 1998;16(3) :551-71
Shah PM and Raney AA. Tricuspid Valve Disease . Current problems in Cardiology 2008;33(2):47-84.
http://www.pediheart.org/practitioners/anatomy/ventricles.htm( last accessed on
Tricuspid Valve
Can you have the tricuspid valve in the left ventricle? The answer – no! What defines the name of the valve is the ventricle in which it lies. Hence the valve of the RV is the tricuspid, and the valve of the LV is the mitral (MV). The tricuspid valve is so named because it usually has 3 cusps, but this in fact is variable, and whether it has 3, 4, or 5, it is still named the tricuspid valve. The usual cusps are the anterior, septal and posterior cusps. The anterolateral papillary muscle of valve almost always originates from the moderator band which connects the free wall of the right ventricle with the septal wall. This papillary muscle can sometimes be used as an identifying feature of RV.
(Image courtesy of Ashley Davidoff M.D.) 06610 b trio

The anatomic specimen shows the appearance of a the inside of a normal right ventricle (RV) with its inflow and outflow (RVOT)
The inflow is identified by the large anterior leafllet of the tricuspid valve (TV) anchored to the septum by the anterolateral papillary muscle. The RVOT is superior to the TV is smooth walled and houses the base of the pulmonary valve note at the superior extent and middle of the RV.
Key words
cardiac heart right ventricle RVOT right ventricular outflow tract parietal band septal band conal septum papillary muscle of Lancisi conal papillary muscle anterolateral papillary muscle pulmonary valve pulmonary artery ventricular septum trabeculae carnii normal anatomy gross anatomy
Ashley Davidoff MD 2019
06409b01
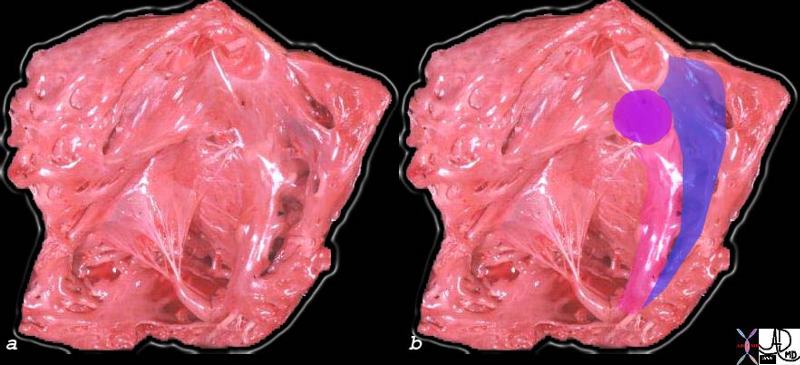
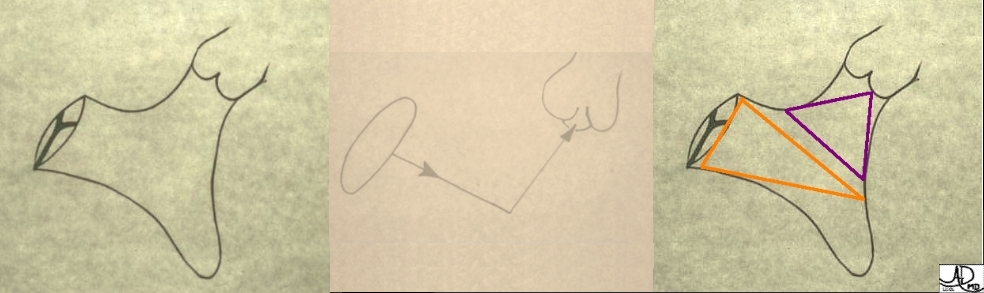
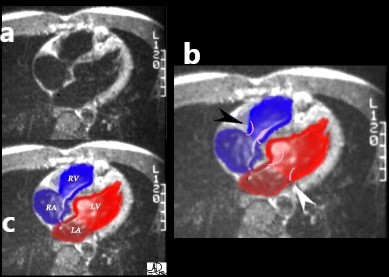
The superior aspect of the septal band (green in right image) has two limbs – the “Y” of the septal band. and the conal septum (lime green) embeds itself in the Y of the septal band. The (chordae) of the conal papillary muscle(aka papillary muscle of Lancisi- black arrow) also inserts in the “Y ” of the septal band. The anterolateral papillary muscle (purple )originates from the septal band) amd subtends the anterior leaflet of the tricuspid valve . The moderator band (not shown) connects the septum top the the free wall, and the parietal band (blue) completes the muscular ring that separates the inflow from the outflow tract. The pulmonary valve (white arrows) define the border between the RVOT and conus with the pulmonary artery.
Ashley Davidoff MD
06409c02
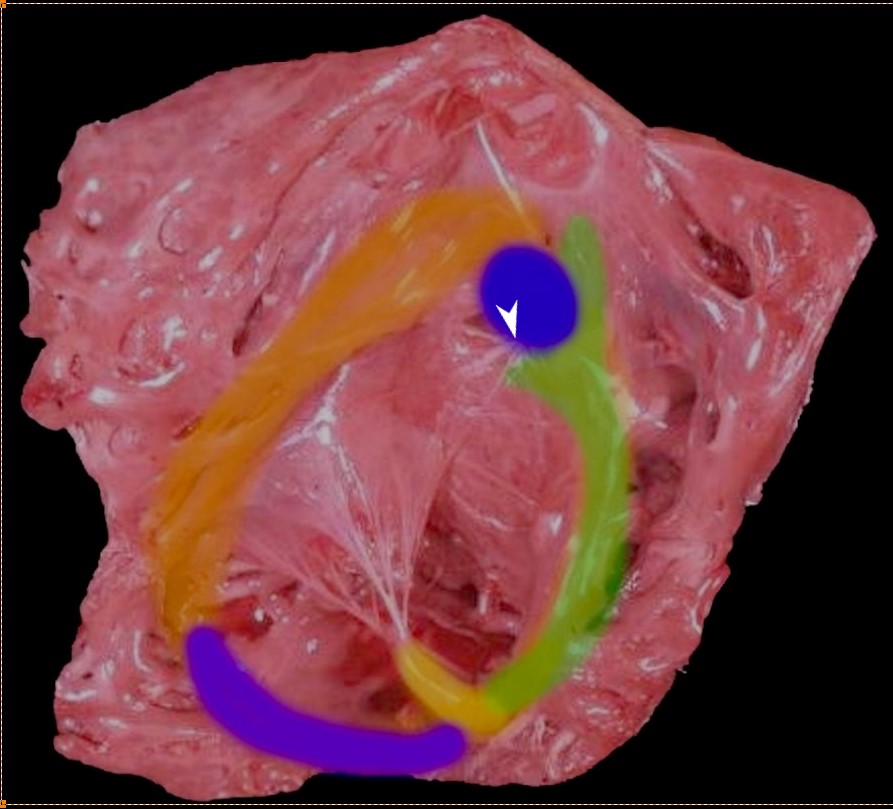
Thr superior aspect of the septal band (green) has two limbs – the “Y” of the septal band. and the conal septum (blue) embeds itself in the Y of the septal band. The (chordae) of the conal papillary muscle (aka papillary muscle of Lancisi- white arrow) also inserts in the “Y ” of the septal band. The anterolateral papillary muscle (yellow) )originates from the septal band) and subtends the anterior leaflet of the tricuspid valve . The moderator band (purple) connects the septum to the the free wall, and the parietal band (orange) completes the muscular ring that separates the inflow from the outflow tract. The pulmonary valve (above the parietal band and conal septum) defines the fborder between the RVOT and conus with the pulmonary artery.
Ashley Davidoff MD
06409 RV muscle bands b01.81

The tricuspid valve is overlaid in yellow showing the large anterior leaflet, and medially placed septal leaflet.
cardiac heart right ventricle RVOT right ventricular outflow tract parietal band septal band conal septum papillary muscle of Lancisi conal papillary muscle anterolateral papillary muscle pulmonary valve pulmonary artery ventricular septum trabeculae carneae normal anatomy gross anatomy Davidoff MD 06409c01

Ashley Davidoff MD
01592
(Image courtesy of Ashley Davidoff M.D.) 32099


In this four chamber echocardiogram the level is similar to the axial view that we have reviewed above. Note how much better we can see the tricuspid and mitral valves. Can you tell whether this image was taken in systole or diastole? It is a systolic frame, since the valves are closed, with a slight posterior bulge of the anterior leaflet of the mitral,and contracted ventricles.(Image courtesy of Philips Medical Systems, Ultrasound )
Current
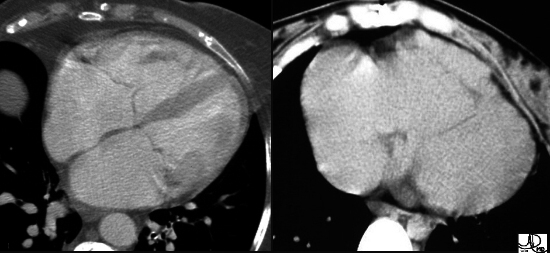
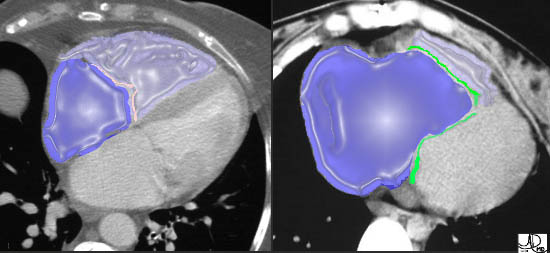
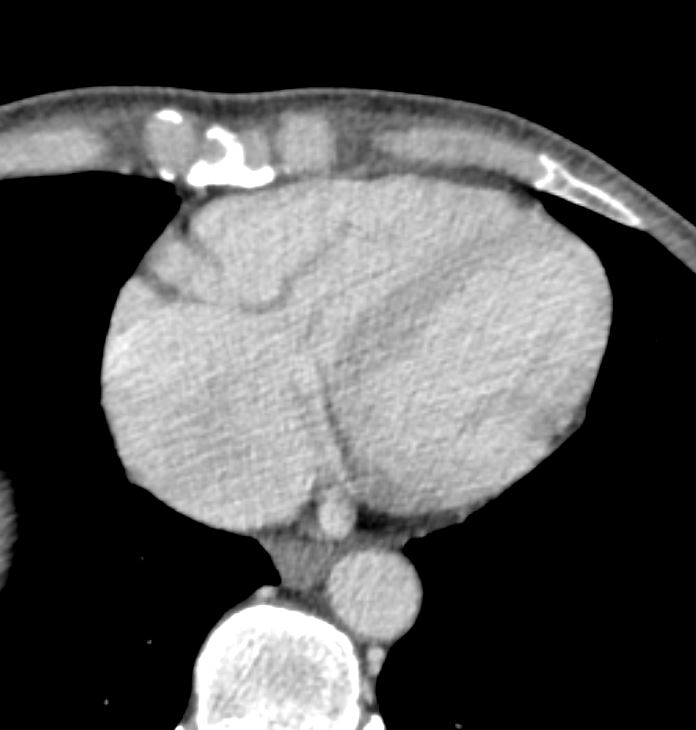
55-year-old male with carcinoid of unknown primary with extensive metastatic disease to liver. CT scan through the heart shows thickened tricuspid valve and enlarged right atrium indicating tricuspid stenosis
Ashley Davidoff TheCommonVein.net 124H 135905
Current
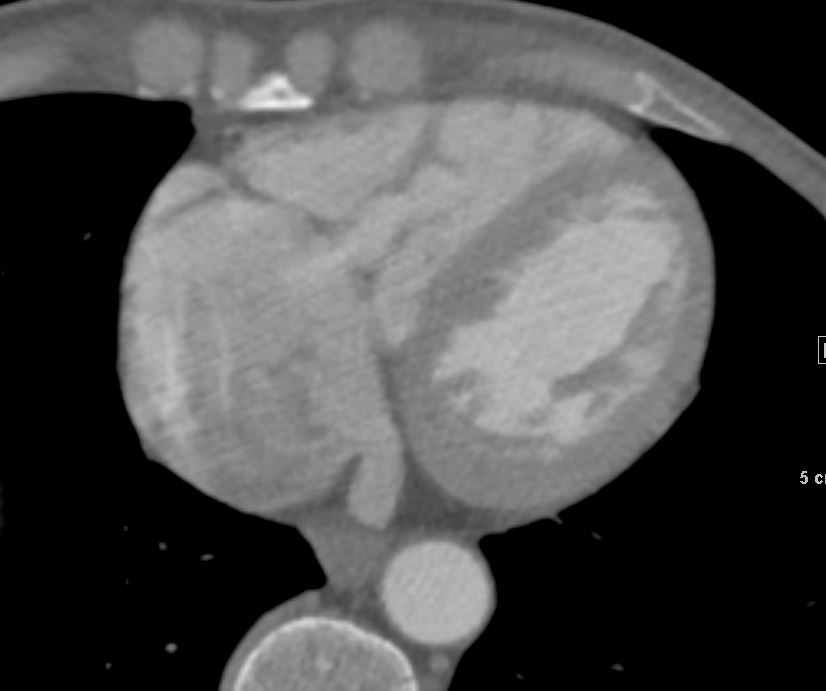
55-year-old male with carcinoid of unknown primary with extensive metastatic disease to liver. CT scan through the heart shows thickened tricuspid valve and enlarged right atrium indicating tricuspid stenosis
Ashley Davidoff TheCommonVein.net 124H 135906
Current
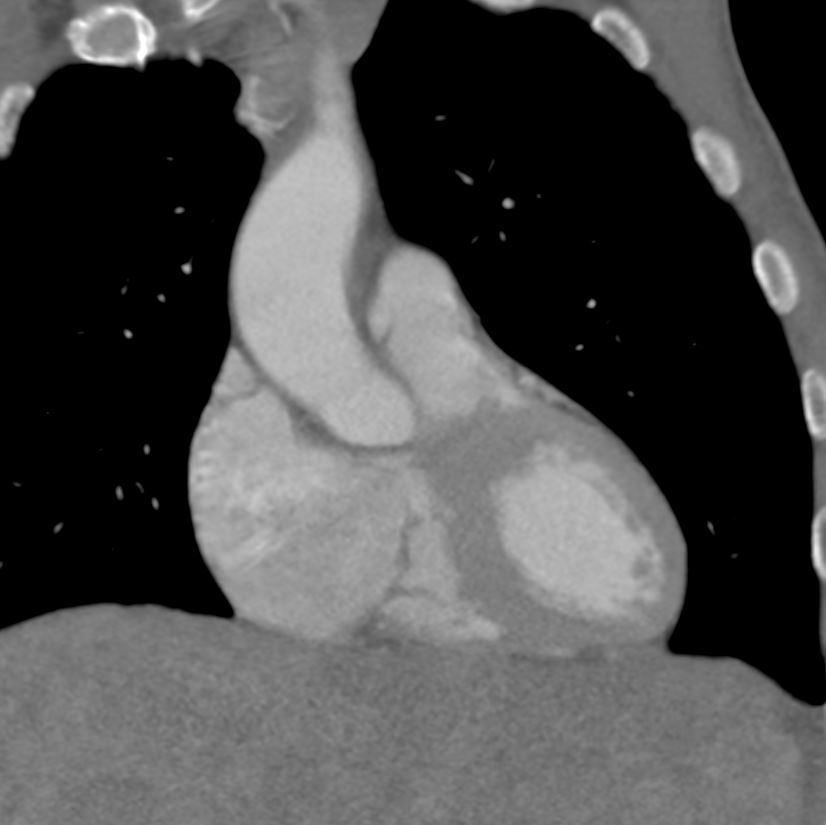
55-year-old male with carcinoid of unknown primary with extensive metastatic disease to liver. CT scan through the heart in the coronal plane shows thickened tricuspid valve and enlarged right atrium indicating tricuspid stenosis
The dome of the liver with metastases is noted
Ashley Davidoff TheCommonVein.net 124H 135908

Current
55-year-old male with carcinoid of unknown primary with extensive metastatic disease to liver. CT scan through the heart in the sagittal plane shows a thickened tricuspid valve and enlarged right atrium indicating tricuspid stenosis
The dome of the liver with metastases is noted
Ashley Davidoff TheCommonVein.net 124H 135909