The right ventricle (RV) is the right sided pump of the heart receives deoxygenated blood from the right atrium (RA) via the tricuspid valve and transmits the blood to the lung for oxygenation.
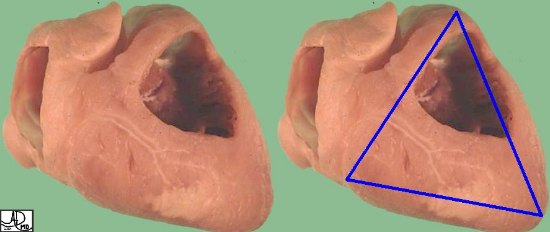
Structurally it is characterized by its position, triangular shape, trabeculated nature, with muscular walls thinner than those on the left . Functionally the RV serves as a pump to transmit blood to the lung.
Sir William Harvey in his De Motu Cordis: described this as “Thus the right ventricle may be said to be made for the sake of transmitting blood through the lungs, not for nourishing them?
Diseases of the right ventricle are usually secondary to LV dysfunction or secondary to lung disease, but may be primary as a result of coronary artery disease, valvular disease, and to less common and rare diseases such as arrhythmogenic right ventricular dysplasia.
The diagnosis of RV dysfunction is suspected clinically by the presence of peripheral dependant edema, ascites, hepatomegaly, an increased jugular venous pressure, which can be increased further by the hepatojugular reflux, a parasternal heave, loud S2(second heart sound) in the pulmonic area and a pan systolic murmur of tricuspid regurgitation .
Imaging includes the use of echocardiography which can reveal enlargement and hypertrophy, usually associated with right atrial enlargement and often accompanied by tricuspid regurgitation.
Medical therapy is used for congestive heart failure or infective endocarditis, and minimally invasive techniques and surgical options are available mostly for intractable tricuspid regurgitation.
The artistic rendition of the heart attempts to reveal the ambivalence in the shape of the heart as either a triangular structure or an oval on its side, and it seems to satisfy both shapes in this view. the right ventricle dominates the anterior view and the left ventricle peeks around the left border of the heart holding its power as its trump card behind the right ventricle. davidoff art copyright 2009 Courtesy Ashley Davidoff MD aka 87180b11.8s aka heart0001
Structural considerations:
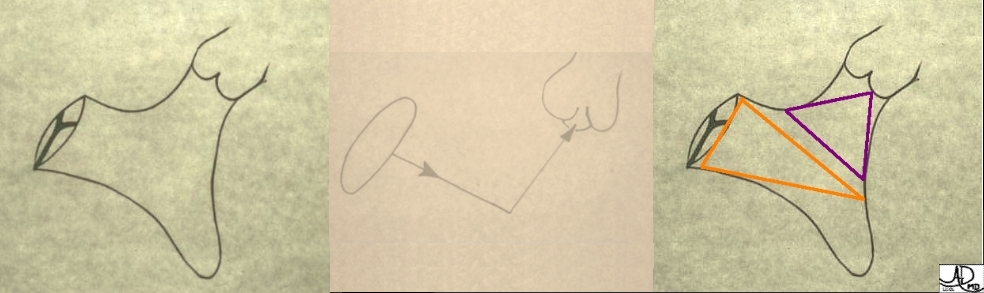
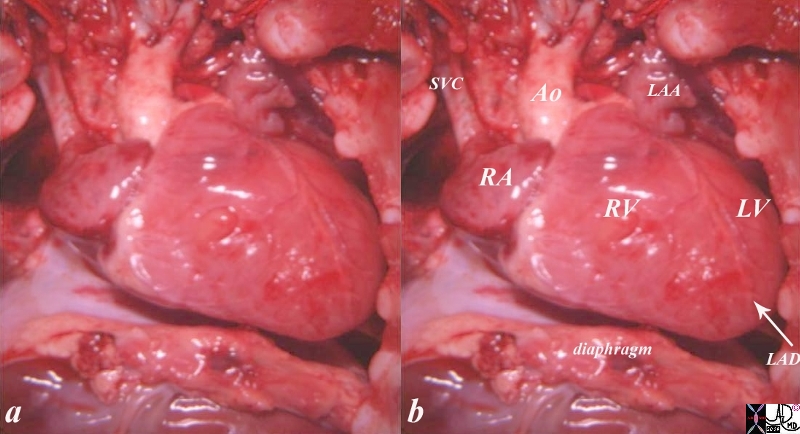
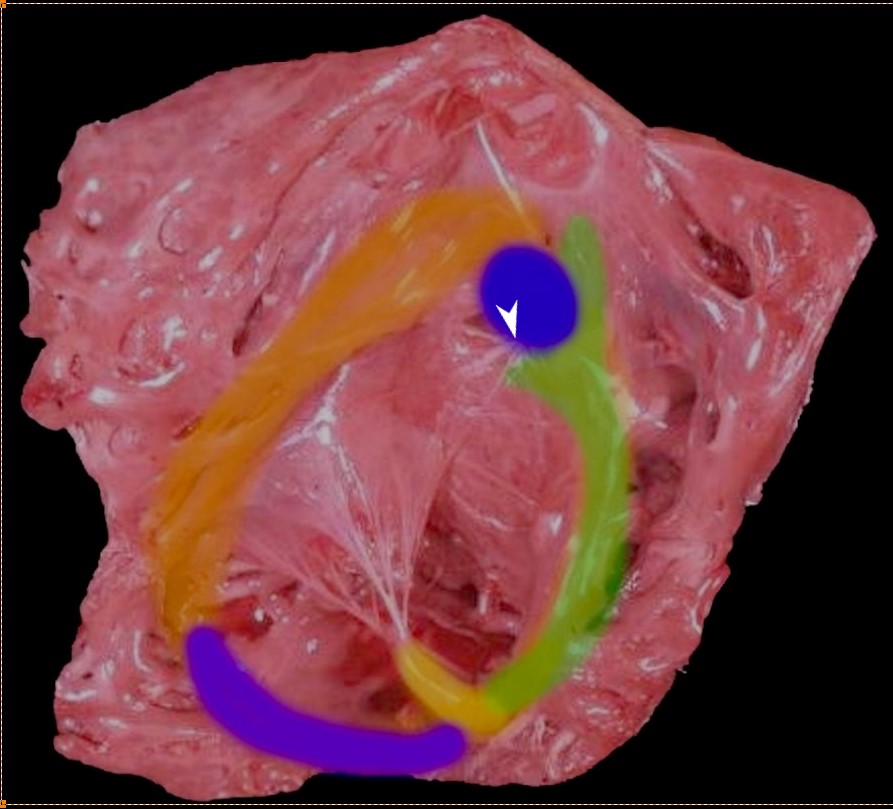
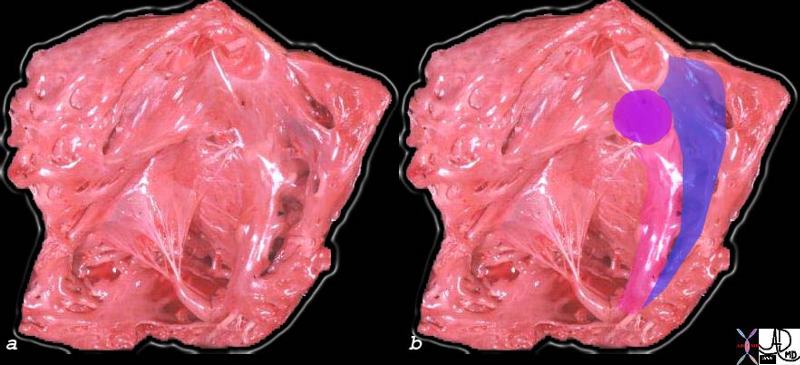
The Inflow and Outflow of the Right Ventricle Tricuspid Valve and Pulmonary Valve The first diagram is a simple drawing of the right ventricle as seen in a frontal projection. The tricuspid valve is to the right (patient position)and inferior and the pulmonary valve to the left and superior. The arrows of the second diagram show the inflow portion of the right ventricle and the outflow portion. The third and last diagram shows the two chambers that make up the right ventricle. The right ventricular inflow chamber also called the RV sinus is triangular and in orange while the outflow chamber is more tubular or cylindrical and has been called many names – but somehow it does not seem to care. Right ventricular outflow tract (RVOT), and infundibulum seem to be the most popular. Courtesy of Ashley Davidoff M.D. 32087 06610 b trioThe post mortem view of the heart in the chest cavity shows a horizontal orientation of the heart, since the lungs are deflated and the heart has an almost rectangular shape. The anterior view is dominated by the right ventricle. The inferior border of the heart is flattened, while the right ward, superior and left ward border are rounded. Courtesy Ashley Davidoff MD copyright 2019 06925c02.8sThe Right Ventricle The anatomic specimen shows the appearance of a the inside of a normal right ventricle (RV) with its inflow and outflow (RVOT) The inflow is identified by the large anterior leafllet of the tricuspid valve (TV) anchored to the septum by the anterolateral papillary muscle. The RVOT is superior to the TV is smooth walled and houses the base of the pulmonary valve note at the superior extent and middle of the RV. Key words cardiac heart right ventricle RVOT right ventricular outflow tract parietal band septal band conal septum papillary muscle of Lancisi conal papillary muscle anterolateral papillary muscle pulmonary valve pulmonary artery ventricular septum trabeculae carnii normal anatomy gross anatomy Ashley Davidoff MD 2019 06409b01 The tricuspid valve is overlaid in yellow showing the large anterior leaflet, and medially placed septal leaflet enabling the identification of the inflow tract and the outflow tract which is overlaid in dark red, The pulmonary valve is overlaid in pink at the superior extent and middle of the RVOT . cardiac heart right ventricle RVOT right ventricular outflow tract parietal band septal band conal septum papillary muscle of Lancisi conal papillary muscle anterolateral papillary muscle pulmonary valve pulmonary artery ventricular septum trabeculae carneae normal anatomy gross anatomy Ashley Davidoff MD 06409c01 MusclesBands Between the Inflow and Outflow Tract of the Right Ventricle (RV Thr superior aspect of the septal band (green) has two limbs – the “Y” of the septal band. and the conal septum (blue) embeds itself in the Y of the septal band. The (chordae) of the conal papillary muscle (aka papillary muscle of Lancisi- white arrow) also inserts in the “Y ” of the septal band. The anterolateral papillary muscle (yellow) )originates from the septal band) and subtends the anterior leaflet of the tricuspid valve . The moderator band (purple) connects the septum to the the free wall, and the parietal band (orange) completes the muscular ring that separates the inflow from the outflow tract. The pulmonary valve (above the parietal band and conal septum) defines the fborder between the RVOT and conus with the pulmonary artery. Ashley Davidoff MD 06409 RV muscle bands b01.81
The RV is an asymmetric chamber that appears crescent shaped
Short axis of an anatomic specimen showing the tricuspid valve within the right ventricle and the mitral valve within the left ventricle. the anterior leaflet of the mitral valve is in fibrous continuity with the aortic valve Ashley Davidoff MD 01592
Size
The walls of the RV are muscular with maximum thickness at the base and thinning toward the apex. The free wall thickness of the RV is less than that of the LV with the proportion between them being 1:3, consequent to a low resistance in the pulmonary circulation.
In the mature child and adult, the volume of the RV is larger than the volume of the LV, whereas RV mass is approximately one sixth that of the LV.
Fetal heart on Ultrasound This image is a 3D reconstruction of a fetal heart in sagittal view, showing the aorta with brachiocephalic vessels, the left atrium abutting the descending aorta posteriorly, and the right ventricle situated anteriorly. No other technology has such an exquisite ability to image the fetal heart. keyt words code heart normal fetus imaging cardiac echo overlay Courtesy of Philips Medical Systems, Ultrasound 32143
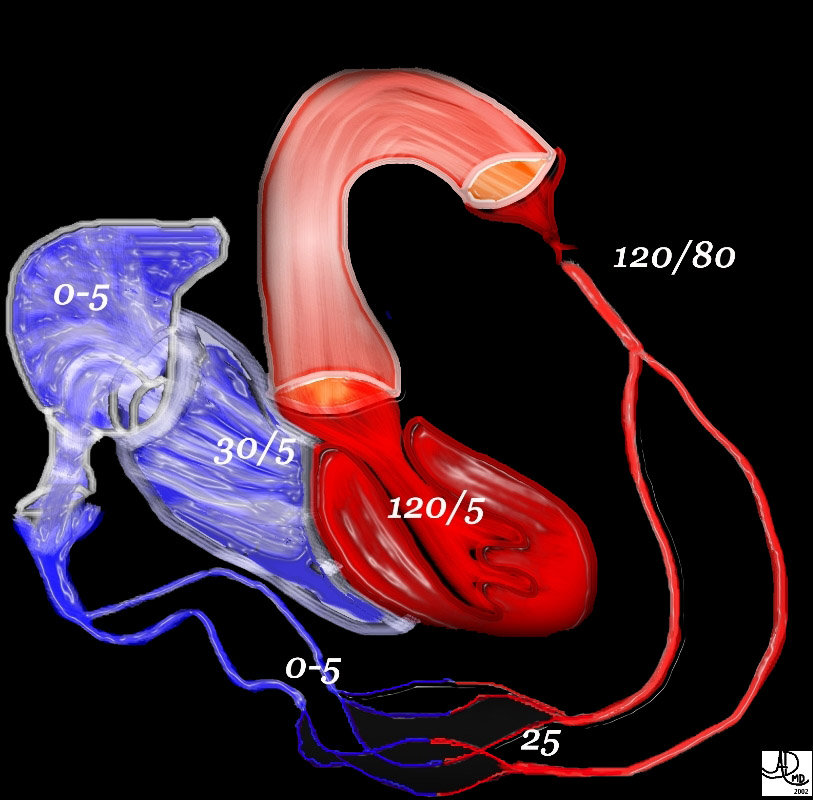
Pressures on the Systemic Side of the Circulation Note the difference in the pressures between the left side of the circulation and the right. The left ventricular pressure reaches a systolic of 120 mmHg, while the right atrial pressure is close to zero. This large difference allows blood to flow through the circulation. pressure principles 49483b01 Davidoff MD Davidoff art
Applied Anatomy
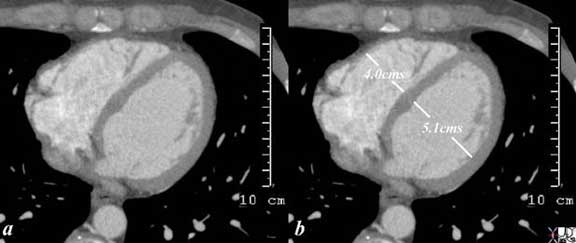
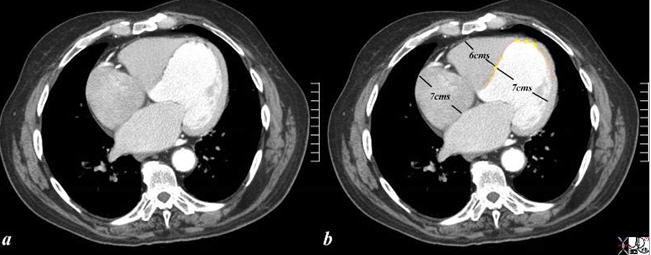
Normal Size of the Right Ventricle and Left Ventricle in the Axial projection During Diastole The axial gated CT scan through the right and left ventricle at end diastole shows the normal size and shape of the right ventricular inflow tract and left ventricle. The right ventricular inflow (underlying the RV measurement) looks smaller than the LV in volume, in this view, since essentially it makes up for the volume in its second “floor” which sits more cranially as the right ventricular outflow tract. The left ventricle only has a single level or floor. Thus in this view the RV looks and measures smaller then the LV. Note also that the apex of the left ventricle protrudes slightly more anteriorly than the RV even though it is the posterior ventricle, because it is the chamber that forms the apex of the heart. The septum also bulges toward the right ventricle due to the higher pressure in the left ventricle. Courtesy of: Ashley Davidoff, MD aka 37758b01c01.8s aka heart anatomy P 040Enlarged Left Ventricle What is the cause of the cardiomegaly? The CT scan is from a 76 year old man in whom the dominant finding is of left ventricular enlargement, characterized by the rotund shape of the ventricle and the increased dimension. The RA and RV are also enlarged based on this image, and LA was enlarged as well suggesting global cardiomegaly consistent with a cardiomyopathy. The clue to the cause of the enlargement is the segmental nature of the disease, characterized by the asymmetry thickness when the free wall thickness is compared to that of the thinning of the septum. In addition, the presence of fat (yellow overlay) in the thinned and probably scarred myocardium, makes ischemic cardiomyopathy the likely diagnosis. Courtesy of: Ashley Davidoff, M.D heart-anatomy-P-047Enlarged Right Atrium (RA) and Right Ventricle (RV) The axial CT scan through the right side of the heart shows an enlarged right atrium and right ventricle in this 88 year old patient with right heart failure with known tricuspid regurgitation The round capaciousness of both chambers provides the subjective impression of RAE and RVE. key words cardiac heart CVS RA large enlarged imaging radiology CTscan Courtesy Ashley Davidoff MD 2019 70344a
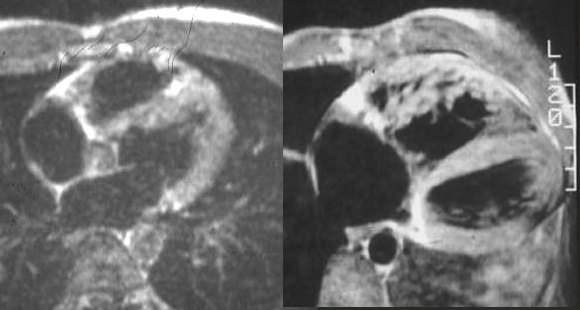
Normal and Abnormal RV Axial images through the heart using black blood imaging shows a normal MRI on the left, alongside an hypertrophied right ventricle (right). Note the thickening and heavy trabeculation of the anterior wall of the right ventricle in the second image . Note also the ovoid shape of the normal LV and the triangular shape of the RV. Courtesy of Ashley Davidoff M.D. 2019 32076
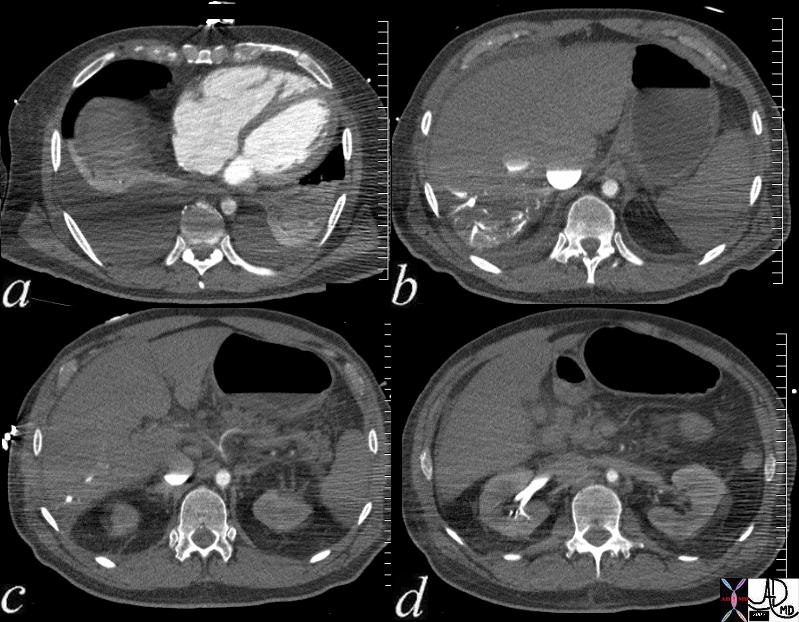
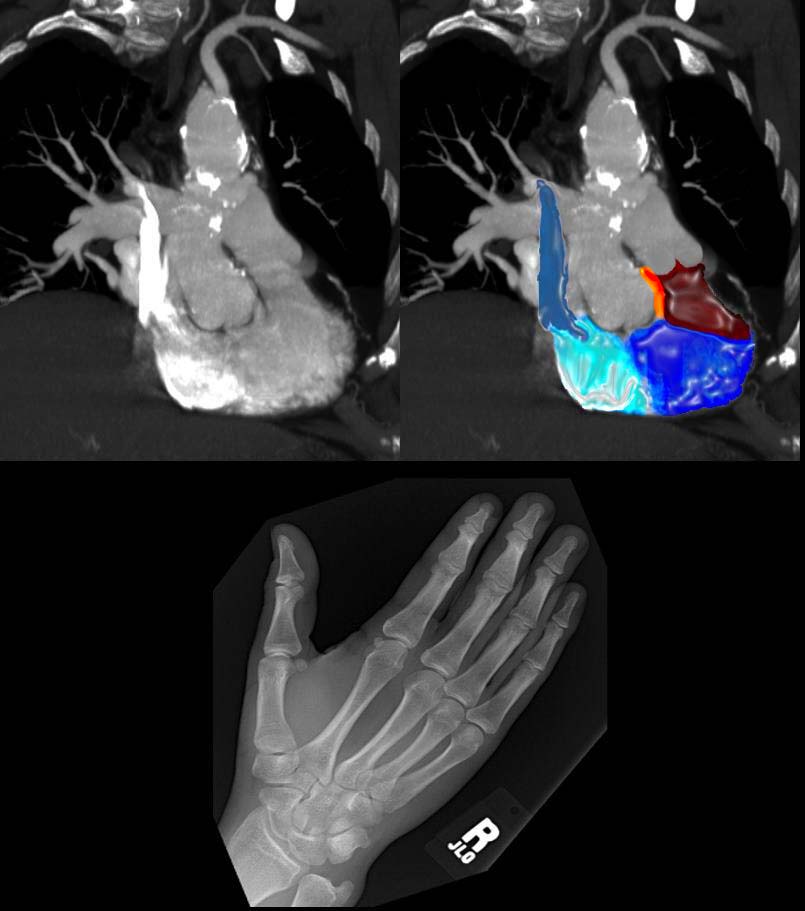
Cardiogenic Shock Multiple axial images through the lower chest and upper abdomen in a patient with cardiogenic shock reveals the consequences on the right side of the circulation. In image (a), the right ventricle and right atrium are enlarged and there are bilateral pleural effusions. Image (b) shows stasis of contrast into the IVC with a blood contrast level. The column is relatively static due to peripheral constriction and slow return. There is reflux into the hepatic veins due to tricuspid regurgitation and the reflux extends all the way to the periphery indicating poor forward flow in the hepatic circulation again due to peripheral constriction. Note how small the aorta is due to contraction of the muscular media in this life threatening situation. In image c the celiac axis with branches hepatic artery and splenic artery show severe vasoconstriction. In d the reflux of contrast low pressure extends deep into the renal parenchyma for the reasons outlined above. key words heart circulation kidney hepatic vein reflux artery celiac axis spasm aorta small shock CTscan Courtesy Ashley Davidoff MD 73796c01
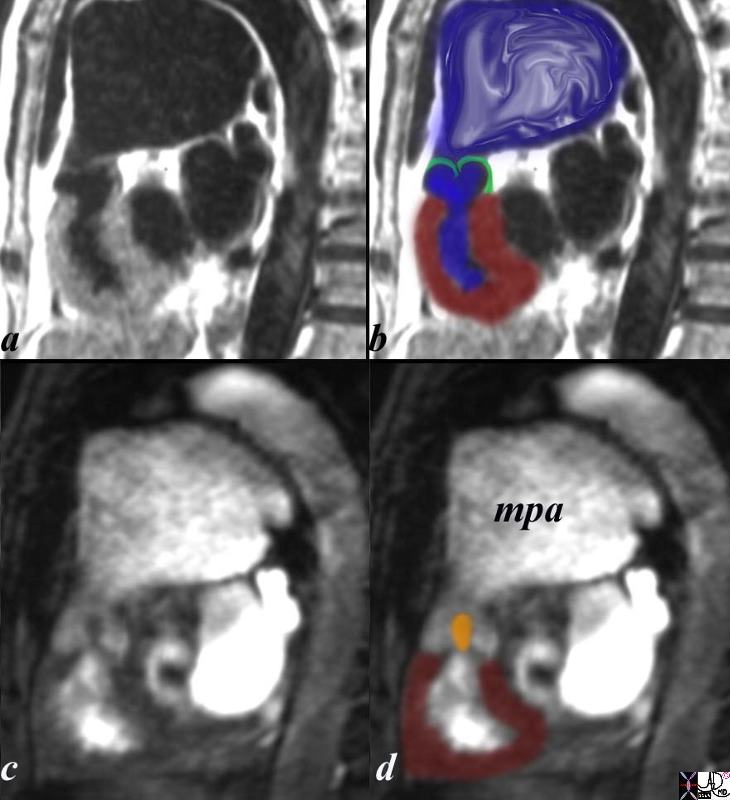
Congenital Pulmonary Stenosis The sagittal view using MRI with black blood (a,b) and white blood(c,d) imaging is from a patient with pulmonary stenosis. The RV (maroon overlay) is hypertrophied, the domed stenotic pulmonary valve (green overlay)is best seen in a and b, and the turbulence through the valve is seen in c, overlaid in orange in d. there is significant post stenotic dilatation of the main pulmonary artery (mpa) inferred by the turbulence in b (blue overlay). code heart cardiac pulmonary valve right ventricle pulmonary artery size enlarged doming stenosis thickened turbulence turbulent flow MRI post stenotic dilatation congenital Courtesy Ashley Davidoff copyright 2019 15437c03.8s
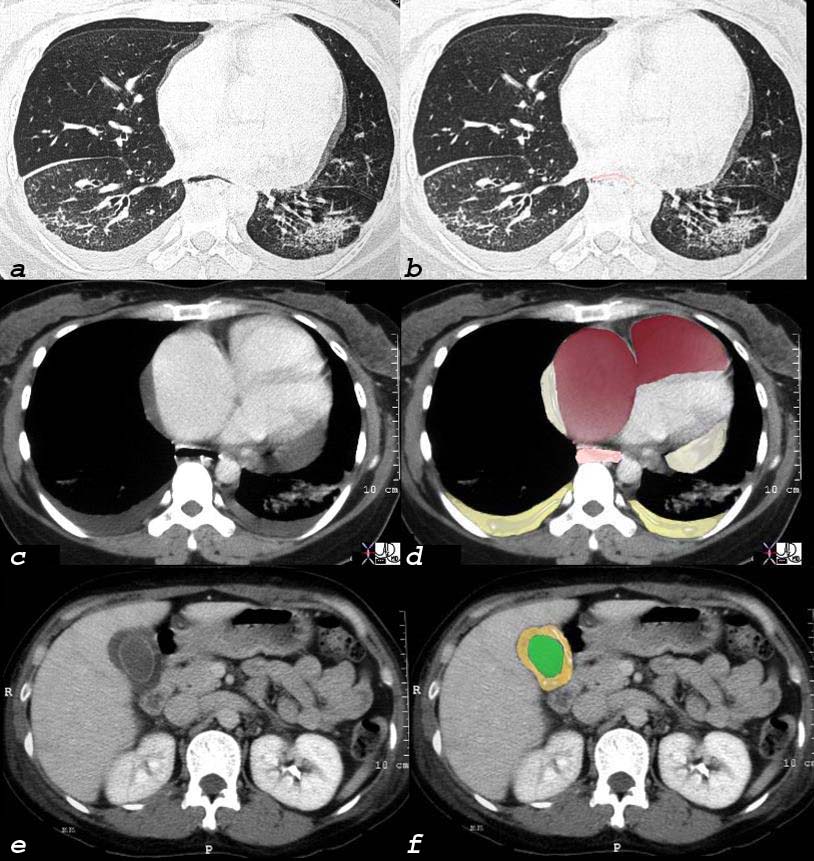
Scleroderma, Interstitial Lung Disease, and Cor Pulmonale 40 year old female with known interstitial lung disease (a and b) shows enlarged right atrium and right ventricle and small pericardial effusion (c and overlaid in maroon in d) and enlarged esophagus (overlay in pink in d) and an edematous gallbladder wall from chronic right heart failure. key words lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD 2019 30464c08
Dilated Left and Right Ventricle Complex Size Changes with Disease Atrophy Caused by Old Infarction, Swelling with New Infarction, Compensatory Hypertrophy and Normal This pathological specimen shows a short axis through the heart with the left ventricle (right of image) and the right ventricle (left of the image). The free wall of the left ventricle contains the papillary muscles and is slightly thickened either as compensation to the remaining diseased myocardium or due to other comorbid diseases such as hypertension or aortic stenosis. There is a fresh infarction (black) posteriorly in the left ventricle extending to the posterior wall of the RV as well. The septum is thinned and fibrotic from an old infarction. The anterior wall of the right ventricle is hypertrophied. Ashley Davidoff MD 15365b01b aka heart-anatomy-P-031.
Shape
It is is triangular in shape, that in cross section is crescentic
Shape of the RV and LV This is an external and frontal view of the heart. The vessel that you see coursing straight down the center of the heart is the left anterior descending artery, (LAD) that runs anterior to the ventricular septum (vertical limb of the cross) separating the right and left ventricles. Conceptualize the triangular shape of the right ventricle, and the ovoid almost football shape of the left ventricle. Courtesy of Ashley Davidoff M.D. 32078
RV shape The right ventricle is less sporty in its shape. It is triangular. (Images courtesy of Ashley Davidoff M.D.32080The drawing of the right side of the heart in sagittal view shows the two parts of the right ventricle (RV). The triangular inflow portionstarts at the tricuspid valve at the base of the heart, extends toward the pointed apex and then proceeds cranially toward the smooth and tubular right ventricular outflow tract (RVOT) (overlaid in maroon). The RVOT terminates at the pulmonary valve, Note that the valve and RVOT point toward the patients toes. The aorta on the other hand (not shown) points toward the patient’s heels because the subaortic conus has undergone resorption which brings it into fibrous continuity with the mitral valve. key words heart cardiac pulmonary artery growth of the subpulmonary conus pulmonary valve infundibulum RV right ventricle RA right atrium IVC inferior vena cava tricuspid valve anatomy embryology position shape of pulmonary artery Courtesy Ashley Davidoff Davidoff drawing 06376b04A lateral view of a right ventricular (RV) angiogram in a patient with severe pulmonary stenosis shows a catheter in the hypoplastic RV inflow tract, (purple) hypercontractile infundibulum (blue)a doming and highly stenotic pulmonary valve and post stenotic dilatation of the pulmonary artery due to a turbulent jet. The intravasation of contrast into the coronary veins seen anterior to the RV inflow (sinus) indicates suprasystemic pressure in the RV key words lung pulmonary artery heart cardiac hypoplastic right ventricular syndrome hypoplastic right ventricle small right ventricle small RV PS pulmonary valve pulmonary stenosis post stenotic dilatation doming pulmonary valve intravasation into coronary arteries suprasystemic RV pressure congenital heart disease size shape RV angiogram angiography Ashley Davidoff MD 15036c01Shape of the RV and LV in Coronal Projection The CT scan of the heart has been reconstructed in the coronal view with image (a) being slightly anterior to image b. In image a, the triangular nature of the RV is noted and in image b the ovoid nature of the LV is noted. All images courtesy of: Ashley Davidoff, M.D. 31235c.81s aka heart anatomy P 060
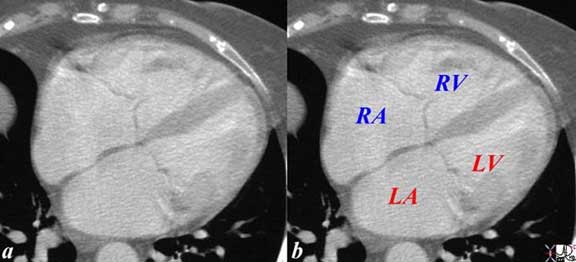
Position of the Chambers and the Atrioventricular Valves of the Heart The cross-sectional images from a CT scan through all 4 chambers reveals the relative position of the chambers and A-V valves. In general “blue” chambers are both anterior to and superior to the “red” chambers so that both the right atrium (RA) and right ventricle (RV) are anterior to the LA and LV. The tricuspid valve (blue valve) follows the rule and is slightly anterior to the mitral valve as well. Not shown here is that the fact that the right sided structures are slightly superiorly positioned. Ashley Davidoff, M.D. 27531cd01.8s aka heart-anatomy-P-070
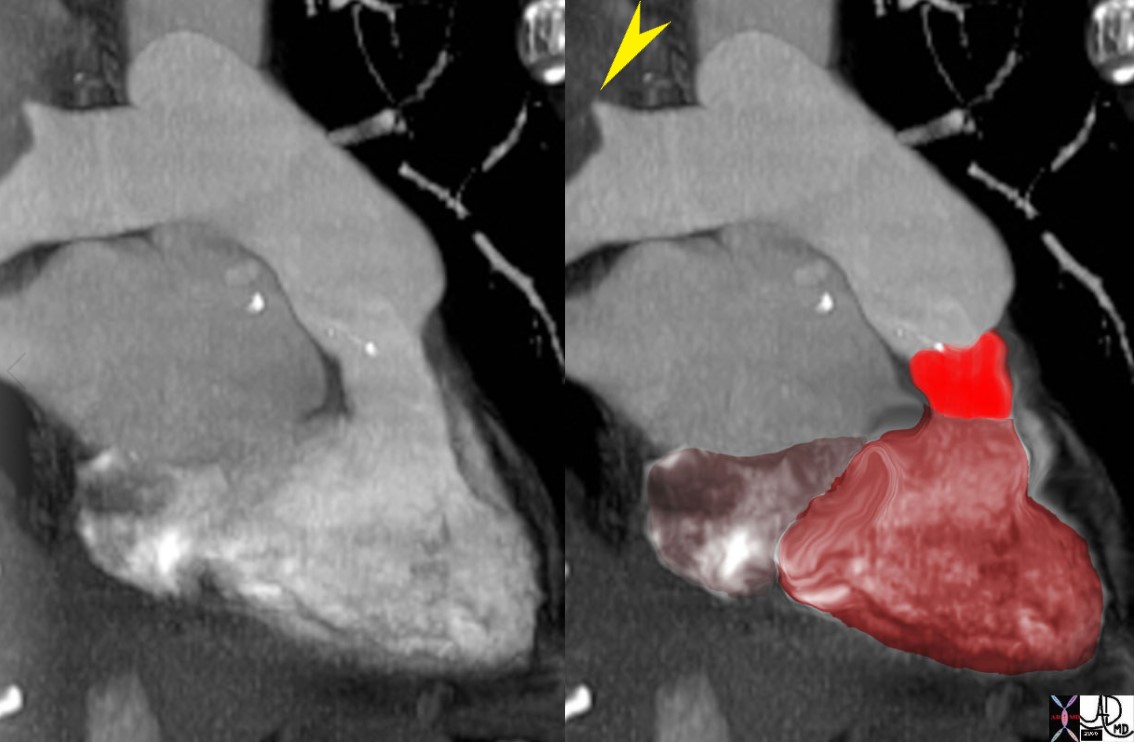
Right Ventricular Enlargement and Hypertrophy CT scan reconstructed in the sagittal plane shows right ventricular enlargement with hypertrophy of the trabeculated inflow portion and smooth walled outflow (RVOT) portion. The RVOT points anteriorly. The MPA also appears dilated. The left atrium is enlarged and is compressing on a dilated esophagus. The anterior leaflet of the mitral valve is in fibrous continuity with the aortic valve. key words infundibulum right ventricle RVOT right ventricular outflow tract aortic valve aortic sclerosis calcification enlarged left atrium heart normal conotruncal relationship cardiac Courtesy Ashley Davidoff MD 2019 31149b.8s
Position
The right ventricle forms the largest part of the anterior surface of the heart , a small part of the diaphragmatic surface and almost entire inferior border of the heart.
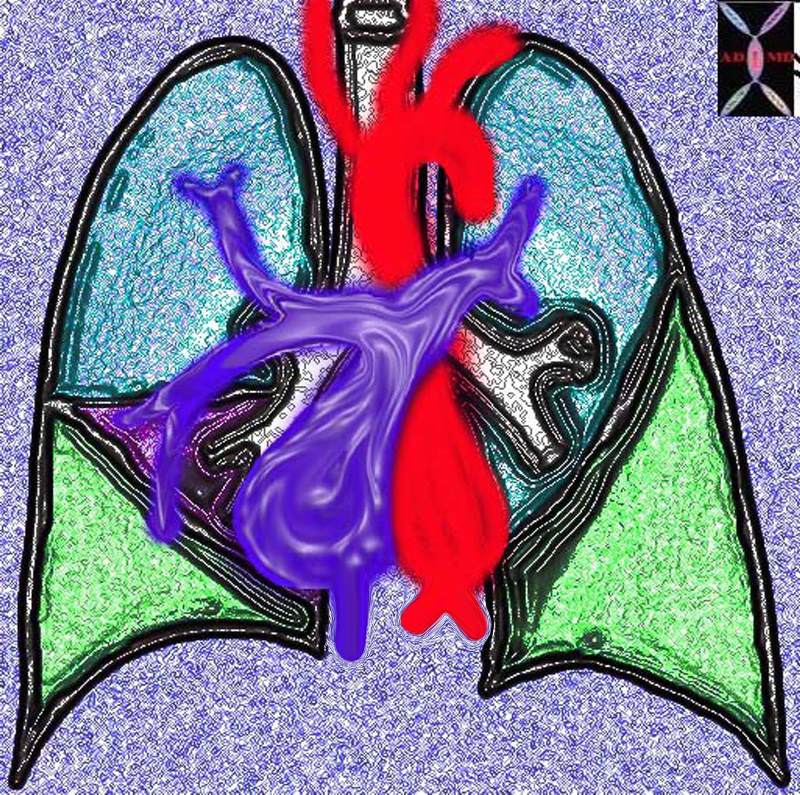
Two Pumps in Series Systemic Circulation and Pulmonary Circulation This diagram shows the right ventricle and lobar pulmonary arteries in blue and the left ventricle and aorta in red. The right sided component of the pump (blue) receives blood from the systemic circulation via the SVC and IVC, pumps it to the lungs. The left sided circulation (red) receives oxygenated blood and pumps it to the systemic circulation. Note that the lobar pulmonary arteries have the same irregular dichotomous branching pattern as the lobar bronchi and give 3 major branches to the right lung (RUL, RML and RLL arteries) and two to the left (LUL and LLL pulmonary arteries). As you will see and learn later, even the position and direction of the main pulmonary arteries in relation to the main stem bronchi are asymmetrical. Courtesy Ashley Davidoff MD 32687b02.15k.8s Davidoff art
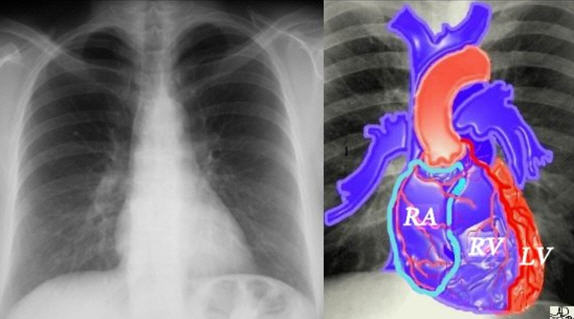
The Anterior Right Ventricle If we were to “crack open” the chest of the chest X-ray, the structures that would dominate this bloody, black and white scene, would be the right sided chambers. The right ventricle (RV) would be the dominant anterior chamber, and would form the dominant interface with the diaphragm. The right atrium (RA) would form the border with the right lung. The RA would of course be slightly posterior to the RV. The left border would be formed by the left ventricle. Most the left ventricle is hidden posteriorly in this view. The left anterior descending artery would be visible from this anterior view. It marks the position of the interventricular septum. Ashley Davidoff MD 32064 aka heart-anatomy-P-035
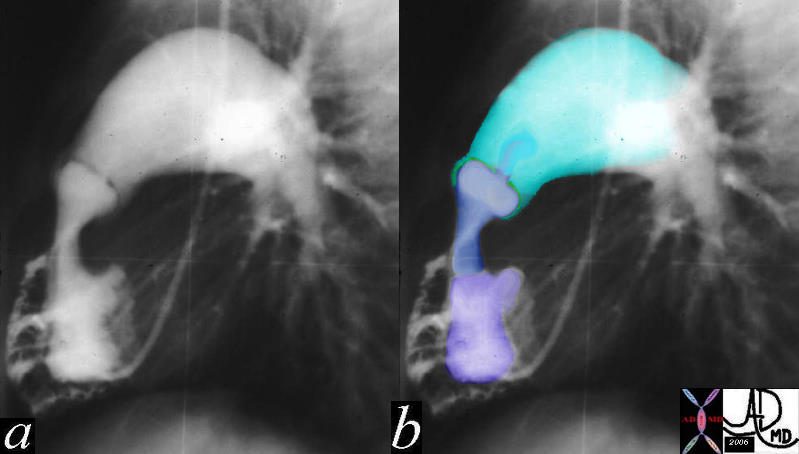
Lateral Examination of the Heart The lateral chest examination reveals an overlay of the structures that are visible, with the right ventricle (triangular blue structure) being anterior giving rise to the pulmonary outflow tract. The heart occupies 1/3 of the length of the sternum, with the upper 2/3 being occupied by lung (black tissue) The left ventricle is posterior and inferior most (2/3) of the posterior border of the heart and occupying the most inferior portion. The left atrium forms the upper 1/3 of the posterior border. Ashley Davidoff MD aka 15416C02W.8s aka heart anatomy P 068
Orientation and Positions of the Right Atrium, (RA), Right Ventricle (RV) Right ventricular Outflow Tract (RVOT) If one places one’s right hand in the air then the thumb points to the RA, and the fingers to the RVOT, pointing in direction toward the left shoulder. keywords cardiac heart SVC right atrium right ventricle right ventricular inflow RV sinus RVOT infundibulum conal septum D loop aorta subpulmonary conus conal septum embryology anatomy Ashley Davidoff MD 47777c04b
Mesocardia This is a CT scan through the chest in which the apex of the heart points forward. The left ventricle (LV) is left sided and the right ventricle is right sided. There is situs solitus of the atria. This is a case of mesocardia ie neither right nor leftward pointing apex. key words heart mesocardia cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD. 19689
Character
Parts
The RV is really composed of two chambers – an inflow or sinus portion and an outflow or infundibular portion. Aristotle had suggested that the heart consisted of 3 chambers. Stella van Praagh a wonderful teacher and friend has translated the original Greek version of Aristotle’s work and firmly believes in her published work that Aristotle had the insight to recognize the right ventricular outflow chamber as the 3rd chamber, with the left and right ventricle each being the other two chambers. It can be divided into basal, mid and apical portions for descriptive reasons. The RV medial wall is shared with the LV and is formed by the interventricular septum, which normally bulges into the RV.
The Inflow and Outflow of the Right Ventricle Tricuspid Valve and Pulmonary Valve The first diagram is a simple drawing of the right ventricle as seen in a frontal projection. The tricuspid valve is to the right (patient position)and inferior and the pulmonary valve to the left and superior. The arrows of the second diagram show the inflow portion of the right ventricle and the outflow portion. The third and last diagram shows the two chambers that make up the right ventricle. The right ventricular inflow chamber also called the RV sinus is triangular and in orange while the outflow chamber is more tubular or cylindrical and has been called many names – but somehow it does not seem to care. Right ventricular outflow tract (RVOT), and infundibulum seem to be the most popular. Courtesy of Ashley Davidoff M.D. 32087 06610 b trio
Muscles Bands Between the Inflow and Outflow Tract of the Right Ventricle (RV) The superior aspect of the septal band (green in right image) has two limbs – the “Y” of the septal band. and the conal septum (lime green) embeds itself in the Y of the septal band. The (chordae) of the conal papillary muscle(aka papillary muscle of Lancisi- black arrow) also inserts in the “Y ” of the septal band. The anterolateral papillary muscle (purple )originates from the septal band) and subtends the anterior leaflet of the tricuspid valve . The moderator band (not shown) connects the septum top the the free wall, and the parietal band (blue) completes the muscular ring that separates the inflow from the outflow tract. The pulmonary valve (white arrows) define the border between the RVOT and conus with the pulmonary artery. Ashley Davidoff MD 06409c02
It is is triangular in shape, relatively thin walled, but heavily trabeculated, and built to adapt to volume changes rather than pressure changes. The interior of the right ventricle can be described in terms of 3 components: (1)inlet ? tricuspid valve , chordae tendineae and papillary muscles, (2) trabeculated apical myocardium (3) smooth outflow tract forming the conus or infundibulum.
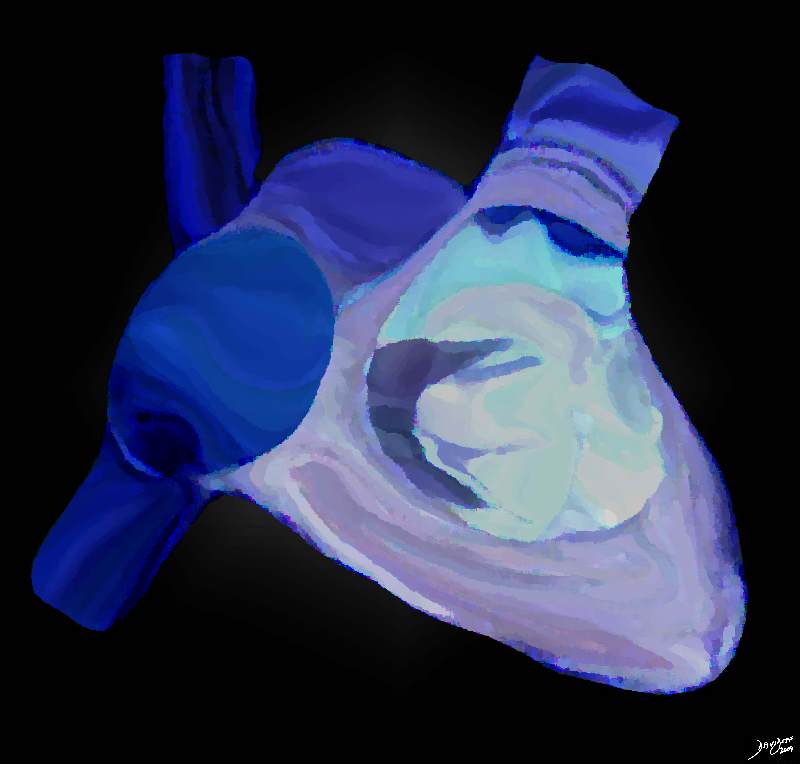
A Peek inside the Right Ventricle The artistic rendition of the right atrium and right ventricle. The spatial relationship is best viewed conceptually by tacking the thumb of your right hand and placing it in the middle of the right atrium, and your palm will be aligned with the RVOT Davidoff art Courtesy Ashley Davidoff copyright 2019 06566b12b13.4kb05i.8s
Normal Right Ventricle Coronal reconstruction of a CT scan shows the normal trabeculated appearance of the right ventricular inflow tract (maroon) and the smooth walled tubular right ventricular outflow tract (bright red). The patient has a right hilar carcinoma that is encasing the upper lobe pulmonary artery (yellow arrow) key words heart artery pulmonary trunk encasement right ventricle RV infundibulum dx carcinoma of the lung CTscan Ashley Davidoff MD 46645c01.801
Inlet portion of the RV extends from the tricuspid valve to the chordal insertions. The papillary muscles are three in number ( anterior , posterior and septal)
Trabeculated muscular portion is identified by prominent muscle bundles that traverse the chamber from the septum to the free wall. It is this region that, trans-venous pacemaker leads are lodged and biopsy tissues are obtained from.
The right ventricular outflow tract is formed by a smooth collar of myocardium know as the conus or infundibulum.
A C shaped ring of muscle known as the supraventricular crest formed by the parietal band , outlet septum , septal band and moderator band forms the non obstructive opening into the RVOT. The parietal band which separates the tricuspid and pulmonary valves is a free wall structure. The outlet septum separates the two outflow tracts and lies between the left and right commissures of the pulmonary and aortic valve respectively. The septal band is a Y shaped structure with a long broad stem and small inferior and anterior limbs. The two limbs give rise to the septal tricuspid papillary muscle. Apically the septal band merges with the apical trabeculations and gives rise to the to the moderator band that inserts at the base of the anterior papillary muscle.
The membranous septum lies midway between the pulmonary valve annulus and inferior aspect of the tricuspid annulus.
Echocardiography:
A line drawn from the apical to the membranous septum divides the interventricular septum into anterior and inferior portions which in turn can be divided into basal mid and apical portions ? giving rise to a total of 6 segments.
The inferior basal and mid segments correspond to the inlet septum.
The apical inferior and anterior along with the mid anterior segments correspond to the muscular septum
The rest of the segments correspond to the outlet septum.
Clinical Considerations:
Differentiation of LV and RV :The RV is defined by its morphology and not by its connections and position. the more apical displacement of the septal leaflet of the tricuspid valve relative to the anterior leaflet of the mitral valve; (2) the presence of a moderator band; (3) the presence of more than 3 papillary muscles; (4)septal papillary attachment of the tricuspid leaflet (5) coarse thicker trabeculations (6) variable locations of the papillary muscles .
The right bundle branch traverses across the septal and moderator bands.
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal Right VentricleCoronal reconstruction of a CT scan shows the normal trabeculated appearance of the right ventricular inflow tract (maroon) and the smooth walled tubular right ventricular outflow tract (bright red). The patient has a right hilar carcinoma that is encasing the upper lobe pulmonary artery (yellow arrow)key wordsheart artery pulmonary trunk encasement right ventricle RV infundibulum dx carcinoma of the lung CTscanAshley Davidoff MD46645c01.801
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal Right VentricleCoronal reconstruction of a CT scan shows the normal trabeculated appearance of the right ventricular inflow tract (maroon) and the smooth walled tubular right ventricular outflow tract (bright red). The patient has a right hilar carcinoma that is encasing the upper lobe pulmonary artery (yellow arrow)key wordsheart artery pulmonary trunk encasement right ventricle RV infundibulum dx carcinoma of the lung CTscanAshley Davidoff MD46645c01.801
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal Right VentricleCoronal reconstruction of a CT scan shows the normal trabeculated appearance of the right ventricular inflow tract (maroon) and the smooth walled tubular right ventricular outflow tract (bright red). The patient has a right hilar carcinoma that is encasing the upper lobe pulmonary artery (yellow arrow)key wordsheart artery pulmonary trunk encasement right ventricle RV infundibulum dx carcinoma of the lung CTscanAshley Davidoff MD46645c01.801
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal Right VentricleCoronal reconstruction of a CT scan shows the normal trabeculated appearance of the right ventricular inflow tract (maroon) and the smooth walled tubular right ventricular outflow tract (bright red). The patient has a right hilar carcinoma that is encasing the upper lobe pulmonary artery (yellow arrow)key wordsheart artery pulmonary trunk encasement right ventricle RV infundibulum dx carcinoma of the lung CTscanAshley Davidoff MD46645c01.801
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
A Peek inside the Right VentricleThe artistic rendition of the right atrium and right ventricle. The spatial relationship is best viewed conceptually by tacking the thumb of your right hand and placing it in the middle of the right atrium, and your palm will be aligned with the RVOTDavidoff art Courtesy Ashley Davidoff copyright 2019 06566b12b13.4kb05i.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
A Peek inside the Right VentricleThe artistic rendition of the right atrium and right ventricle. The spatial relationship is best viewed conceptually by tacking the thumb of your right hand and placing it in the middle of the right atrium, and your palm will be aligned with the RVOTDavidoff art Courtesy Ashley Davidoff copyright 2019 06566b12b13.4kb05i.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
A Peek inside the Right VentricleThe artistic rendition of the right atrium and right ventricle. The spatial relationship is best viewed conceptually by tacking the thumb of your right hand and placing it in the middle of the right atrium, and your palm will be aligned with the RVOTDavidoff art Courtesy Ashley Davidoff copyright 2019 06566b12b13.4kb05i.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
A Peek inside the Right VentricleThe artistic rendition of the right atrium and right ventricle. The spatial relationship is best viewed conceptually by tacking the thumb of your right hand and placing it in the middle of the right atrium, and your palm will be aligned with the RVOTDavidoff art Courtesy Ashley Davidoff copyright 2019 06566b12b13.4kb05i.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Muscles Bands Between the Inflow and Outflow Tract of the Right Ventricle (RV)The superior aspect of the septal band (green in right image) has two limbs – the “Y” of the septal band. and the conal septum (lime green) embeds itself in the Y of the septal band. The (chordae) of the conal papillary muscle(aka papillary muscle of Lancisi- black arrow) also inserts in the “Y ” of the septal band. The anterolateral papillary muscle (purple )originates from the septal band) and subtends the anterior leaflet of the tricuspid valve . The moderator band (not shown) connects the septum top the the free wall, and the parietal band (blue) completes the muscular ring that separates the inflow from the outflow tract. The pulmonary valve (white arrows) define the border between the RVOT and conus with the pulmonary artery.Ashley Davidoff MD06409c02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Muscles Bands Between the Inflow and Outflow Tract of the Right Ventricle (RV)The superior aspect of the septal band (green in right image) has two limbs – the “Y” of the septal band. and the conal septum (lime green) embeds itself in the Y of the septal band. The (chordae) of the conal papillary muscle(aka papillary muscle of Lancisi- black arrow) also inserts in the “Y ” of the septal band. The anterolateral papillary muscle (purple )originates from the septal band) and subtends the anterior leaflet of the tricuspid valve . The moderator band (not shown) connects the septum top the the free wall, and the parietal band (blue) completes the muscular ring that separates the inflow from the outflow tract. The pulmonary valve (white arrows) define the border between the RVOT and conus with the pulmonary artery.Ashley Davidoff MD06409c02
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Muscles Bands Between the Inflow and Outflow Tract of the Right Ventricle (RV)The superior aspect of the septal band (green in right image) has two limbs – the “Y” of the septal band. and the conal septum (lime green) embeds itself in the Y of the septal band. The (chordae) of the conal papillary muscle(aka papillary muscle of Lancisi- black arrow) also inserts in the “Y ” of the septal band. The anterolateral papillary muscle (purple )originates from the septal band) and subtends the anterior leaflet of the tricuspid valve . The moderator band (not shown) connects the septum top the the free wall, and the parietal band (blue) completes the muscular ring that separates the inflow from the outflow tract. The pulmonary valve (white arrows) define the border between the RVOT and conus with the pulmonary artery.Ashley Davidoff MD06409c02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Muscles Bands Between the Inflow and Outflow Tract of the Right Ventricle (RV)The superior aspect of the septal band (green in right image) has two limbs – the “Y” of the septal band. and the conal septum (lime green) embeds itself in the Y of the septal band. The (chordae) of the conal papillary muscle(aka papillary muscle of Lancisi- black arrow) also inserts in the “Y ” of the septal band. The anterolateral papillary muscle (purple )originates from the septal band) and subtends the anterior leaflet of the tricuspid valve . The moderator band (not shown) connects the septum top the the free wall, and the parietal band (blue) completes the muscular ring that separates the inflow from the outflow tract. The pulmonary valve (white arrows) define the border between the RVOT and conus with the pulmonary artery.Ashley Davidoff MD06409c02
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
The Inflow and Outflow of the Right VentricleTricuspid Valve and Pulmonary ValveThe first diagram is a simple drawing of the right ventricle as seen in a frontal projection. The tricuspid valve is to the right (patient position)and inferior and the pulmonary valve to the left and superior. The arrows of the second diagram show the inflow portion of the right ventricle and the outflow portion. The third and last diagram shows the two chambers that make up the right ventricle. The right ventricular inflow chamber also called the RV sinus is triangular and in orange while the outflow chamber is more tubular or cylindrical and has been called many names – but somehow it does not seem to care. Right ventricular outflow tract (RVOT), and infundibulum seem to be the most popular. Courtesy of Ashley Davidoff M.D. 32087 06610 b trio
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
The Inflow and Outflow of the Right VentricleTricuspid Valve and Pulmonary ValveThe first diagram is a simple drawing of the right ventricle as seen in a frontal projection. The tricuspid valve is to the right (patient position)and inferior and the pulmonary valve to the left and superior. The arrows of the second diagram show the inflow portion of the right ventricle and the outflow portion. The third and last diagram shows the two chambers that make up the right ventricle. The right ventricular inflow chamber also called the RV sinus is triangular and in orange while the outflow chamber is more tubular or cylindrical and has been called many names – but somehow it does not seem to care. Right ventricular outflow tract (RVOT), and infundibulum seem to be the most popular. Courtesy of Ashley Davidoff M.D. 32087 06610 b trio
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The Inflow and Outflow of the Right VentricleTricuspid Valve and Pulmonary ValveThe first diagram is a simple drawing of the right ventricle as seen in a frontal projection. The tricuspid valve is to the right (patient position)and inferior and the pulmonary valve to the left and superior. The arrows of the second diagram show the inflow portion of the right ventricle and the outflow portion. The third and last diagram shows the two chambers that make up the right ventricle. The right ventricular inflow chamber also called the RV sinus is triangular and in orange while the outflow chamber is more tubular or cylindrical and has been called many names – but somehow it does not seem to care. Right ventricular outflow tract (RVOT), and infundibulum seem to be the most popular. Courtesy of Ashley Davidoff M.D. 32087 06610 b trio
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The Inflow and Outflow of the Right VentricleTricuspid Valve and Pulmonary ValveThe first diagram is a simple drawing of the right ventricle as seen in a frontal projection. The tricuspid valve is to the right (patient position)and inferior and the pulmonary valve to the left and superior. The arrows of the second diagram show the inflow portion of the right ventricle and the outflow portion. The third and last diagram shows the two chambers that make up the right ventricle. The right ventricular inflow chamber also called the RV sinus is triangular and in orange while the outflow chamber is more tubular or cylindrical and has been called many names – but somehow it does not seem to care. Right ventricular outflow tract (RVOT), and infundibulum seem to be the most popular. Courtesy of Ashley Davidoff M.D. 32087 06610 b trio
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
MesocardiaThis is a CT scan through the chest in which the apex of the heart points forward. The left ventricle (LV) is left sided and the right ventricle is right sided. There is situs solitus of the atria. This is a case of mesocardia ie neither right nor leftward pointing apex.key words heart mesocardia cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD.19689
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
MesocardiaThis is a CT scan through the chest in which the apex of the heart points forward. The left ventricle (LV) is left sided and the right ventricle is right sided. There is situs solitus of the atria. This is a case of mesocardia ie neither right nor leftward pointing apex.key words heart mesocardia cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD.19689
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
MesocardiaThis is a CT scan through the chest in which the apex of the heart points forward. The left ventricle (LV) is left sided and the right ventricle is right sided. There is situs solitus of the atria. This is a case of mesocardia ie neither right nor leftward pointing apex.key words heart mesocardia cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD.19689
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
MesocardiaThis is a CT scan through the chest in which the apex of the heart points forward. The left ventricle (LV) is left sided and the right ventricle is right sided. There is situs solitus of the atria. This is a case of mesocardia ie neither right nor leftward pointing apex.key words heart mesocardia cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD.19689
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Orientation and Positions of the Right Atrium, (RA), Right Ventricle (RV) Right ventricular Outflow Tract (RVOT)If one places one’s right hand in the air then the thumb points to the RA, and the fingers to the RVOT, pointing in direction toward the left shoulder.keywordscardiac heart SVC right atrium right ventricle right ventricular inflow RV sinus RVOT infundibulum conal septum D loop aorta subpulmonary conus conal septum embryology anatomyAshley Davidoff MD47777c04b
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Orientation and Positions of the Right Atrium, (RA), Right Ventricle (RV) Right ventricular Outflow Tract (RVOT)If one places one’s right hand in the air then the thumb points to the RA, and the fingers to the RVOT, pointing in direction toward the left shoulder.keywordscardiac heart SVC right atrium right ventricle right ventricular inflow RV sinus RVOT infundibulum conal septum D loop aorta subpulmonary conus conal septum embryology anatomyAshley Davidoff MD47777c04b
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Orientation and Positions of the Right Atrium, (RA), Right Ventricle (RV) Right ventricular Outflow Tract (RVOT)If one places one’s right hand in the air then the thumb points to the RA, and the fingers to the RVOT, pointing in direction toward the left shoulder.keywordscardiac heart SVC right atrium right ventricle right ventricular inflow RV sinus RVOT infundibulum conal septum D loop aorta subpulmonary conus conal septum embryology anatomyAshley Davidoff MD47777c04b
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Orientation and Positions of the Right Atrium, (RA), Right Ventricle (RV) Right ventricular Outflow Tract (RVOT)If one places one’s right hand in the air then the thumb points to the RA, and the fingers to the RVOT, pointing in direction toward the left shoulder.keywordscardiac heart SVC right atrium right ventricle right ventricular inflow RV sinus RVOT infundibulum conal septum D loop aorta subpulmonary conus conal septum embryology anatomyAshley Davidoff MD47777c04b
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Lateral Examination of the HeartThe lateral chest examination reveals an overlay of the structures that are visible, with the right ventricle (triangular blue structure) being anterior giving rise to the pulmonary outflow tract. The heart occupies 1/3 of the length of the sternum, with the upper 2/3 being occupied by lung (black tissue) The left ventricle is posterior and inferior most (2/3) of the posterior border of the heart and occupying the most inferior portion. The left atrium forms the upper 1/3 of the posterior border.Ashley Davidoff MDaka 15416C02W.8saka heart anatomy P 068
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Lateral Examination of the HeartThe lateral chest examination reveals an overlay of the structures that are visible, with the right ventricle (triangular blue structure) being anterior giving rise to the pulmonary outflow tract. The heart occupies 1/3 of the length of the sternum, with the upper 2/3 being occupied by lung (black tissue) The left ventricle is posterior and inferior most (2/3) of the posterior border of the heart and occupying the most inferior portion. The left atrium forms the upper 1/3 of the posterior border.Ashley Davidoff MDaka 15416C02W.8saka heart anatomy P 068
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Lateral Examination of the HeartThe lateral chest examination reveals an overlay of the structures that are visible, with the right ventricle (triangular blue structure) being anterior giving rise to the pulmonary outflow tract. The heart occupies 1/3 of the length of the sternum, with the upper 2/3 being occupied by lung (black tissue) The left ventricle is posterior and inferior most (2/3) of the posterior border of the heart and occupying the most inferior portion. The left atrium forms the upper 1/3 of the posterior border.Ashley Davidoff MDaka 15416C02W.8saka heart anatomy P 068
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Lateral Examination of the HeartThe lateral chest examination reveals an overlay of the structures that are visible, with the right ventricle (triangular blue structure) being anterior giving rise to the pulmonary outflow tract. The heart occupies 1/3 of the length of the sternum, with the upper 2/3 being occupied by lung (black tissue) The left ventricle is posterior and inferior most (2/3) of the posterior border of the heart and occupying the most inferior portion. The left atrium forms the upper 1/3 of the posterior border.Ashley Davidoff MDaka 15416C02W.8saka heart anatomy P 068
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
The Anterior Right Ventricle If we were to “crack open” the chest of the chest X-ray, the structures that would dominate this bloody, black and white scene, would be the right sided chambers. The right ventricle (RV) would be the dominant anterior chamber, and would form the dominant interface with the diaphragm. The right atrium (RA) would form the border with the right lung. The RA would of course be slightly posterior to the RV. The left border would be formed by the left ventricle. Most the left ventricle is hidden posteriorly in this view. The left anterior descending artery would be visible from this anterior view. It marks the position of the interventricular septum.Ashley Davidoff MD 32064 aka heart-anatomy-P-035
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
The Anterior Right Ventricle If we were to “crack open” the chest of the chest X-ray, the structures that would dominate this bloody, black and white scene, would be the right sided chambers. The right ventricle (RV) would be the dominant anterior chamber, and would form the dominant interface with the diaphragm. The right atrium (RA) would form the border with the right lung. The RA would of course be slightly posterior to the RV. The left border would be formed by the left ventricle. Most the left ventricle is hidden posteriorly in this view. The left anterior descending artery would be visible from this anterior view. It marks the position of the interventricular septum.Ashley Davidoff MD 32064 aka heart-anatomy-P-035
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The Anterior Right Ventricle If we were to “crack open” the chest of the chest X-ray, the structures that would dominate this bloody, black and white scene, would be the right sided chambers. The right ventricle (RV) would be the dominant anterior chamber, and would form the dominant interface with the diaphragm. The right atrium (RA) would form the border with the right lung. The RA would of course be slightly posterior to the RV. The left border would be formed by the left ventricle. Most the left ventricle is hidden posteriorly in this view. The left anterior descending artery would be visible from this anterior view. It marks the position of the interventricular septum.Ashley Davidoff MD 32064 aka heart-anatomy-P-035
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The Anterior Right Ventricle If we were to “crack open” the chest of the chest X-ray, the structures that would dominate this bloody, black and white scene, would be the right sided chambers. The right ventricle (RV) would be the dominant anterior chamber, and would form the dominant interface with the diaphragm. The right atrium (RA) would form the border with the right lung. The RA would of course be slightly posterior to the RV. The left border would be formed by the left ventricle. Most the left ventricle is hidden posteriorly in this view. The left anterior descending artery would be visible from this anterior view. It marks the position of the interventricular septum.Ashley Davidoff MD 32064 aka heart-anatomy-P-035
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Two Pumps in SeriesSystemic Circulation and Pulmonary CirculationThis diagram shows the right ventricle and lobar pulmonary arteries in blue and the left ventricle and aorta in red. The right sided component of the pump (blue) receives blood from the systemic circulation via the SVC and IVC, pumps it to the lungs. The left sided circulation (red) receives oxygenated blood and pumps it to the systemic circulation.Note that the lobar pulmonary arteries have the same irregular dichotomous branching pattern as the lobar bronchi and give 3 major branches to the right lung (RUL, RML and RLL arteries) and two to the left (LUL and LLL pulmonary arteries). As you will see and learn later, even the position and direction of the main pulmonary arteries in relation to the main stem bronchi are asymmetrical.Courtesy Ashley Davidoff MD 32687b02.15k.8s Davidoff art
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Two Pumps in SeriesSystemic Circulation and Pulmonary CirculationThis diagram shows the right ventricle and lobar pulmonary arteries in blue and the left ventricle and aorta in red. The right sided component of the pump (blue) receives blood from the systemic circulation via the SVC and IVC, pumps it to the lungs. The left sided circulation (red) receives oxygenated blood and pumps it to the systemic circulation.Note that the lobar pulmonary arteries have the same irregular dichotomous branching pattern as the lobar bronchi and give 3 major branches to the right lung (RUL, RML and RLL arteries) and two to the left (LUL and LLL pulmonary arteries). As you will see and learn later, even the position and direction of the main pulmonary arteries in relation to the main stem bronchi are asymmetrical.Courtesy Ashley Davidoff MD 32687b02.15k.8s Davidoff art
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Two Pumps in SeriesSystemic Circulation and Pulmonary CirculationThis diagram shows the right ventricle and lobar pulmonary arteries in blue and the left ventricle and aorta in red. The right sided component of the pump (blue) receives blood from the systemic circulation via the SVC and IVC, pumps it to the lungs. The left sided circulation (red) receives oxygenated blood and pumps it to the systemic circulation.Note that the lobar pulmonary arteries have the same irregular dichotomous branching pattern as the lobar bronchi and give 3 major branches to the right lung (RUL, RML and RLL arteries) and two to the left (LUL and LLL pulmonary arteries). As you will see and learn later, even the position and direction of the main pulmonary arteries in relation to the main stem bronchi are asymmetrical.Courtesy Ashley Davidoff MD 32687b02.15k.8s Davidoff art
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Two Pumps in SeriesSystemic Circulation and Pulmonary CirculationThis diagram shows the right ventricle and lobar pulmonary arteries in blue and the left ventricle and aorta in red. The right sided component of the pump (blue) receives blood from the systemic circulation via the SVC and IVC, pumps it to the lungs. The left sided circulation (red) receives oxygenated blood and pumps it to the systemic circulation.Note that the lobar pulmonary arteries have the same irregular dichotomous branching pattern as the lobar bronchi and give 3 major branches to the right lung (RUL, RML and RLL arteries) and two to the left (LUL and LLL pulmonary arteries). As you will see and learn later, even the position and direction of the main pulmonary arteries in relation to the main stem bronchi are asymmetrical.Courtesy Ashley Davidoff MD 32687b02.15k.8s Davidoff art
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Right Ventricular Enlargement and HypertrophyCT scan reconstructed in the sagittal plane shows right ventricular enlargement with hypertrophy of the trabeculated inflow portion and smooth walled outflow (RVOT) portion. The RVOT points anteriorly. The MPA also appears dilated. The left atrium is enlarged and is compressing on a dilated esophagus. The anterior leaflet of the mitral valve is in fibrous continuity with the aortic valve.key wordsinfundibulum right ventricle RVOT right ventricular outflow tract aortic valve aortic sclerosis calcification enlarged left atrium heart normal conotruncal relationship cardiacCourtesy Ashley Davidoff MD 201931149b.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Right Ventricular Enlargement and HypertrophyCT scan reconstructed in the sagittal plane shows right ventricular enlargement with hypertrophy of the trabeculated inflow portion and smooth walled outflow (RVOT) portion. The RVOT points anteriorly. The MPA also appears dilated. The left atrium is enlarged and is compressing on a dilated esophagus. The anterior leaflet of the mitral valve is in fibrous continuity with the aortic valve.key wordsinfundibulum right ventricle RVOT right ventricular outflow tract aortic valve aortic sclerosis calcification enlarged left atrium heart normal conotruncal relationship cardiacCourtesy Ashley Davidoff MD 201931149b.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Right Ventricular Enlargement and HypertrophyCT scan reconstructed in the sagittal plane shows right ventricular enlargement with hypertrophy of the trabeculated inflow portion and smooth walled outflow (RVOT) portion. The RVOT points anteriorly. The MPA also appears dilated. The left atrium is enlarged and is compressing on a dilated esophagus. The anterior leaflet of the mitral valve is in fibrous continuity with the aortic valve.key wordsinfundibulum right ventricle RVOT right ventricular outflow tract aortic valve aortic sclerosis calcification enlarged left atrium heart normal conotruncal relationship cardiacCourtesy Ashley Davidoff MD 201931149b.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Right Ventricular Enlargement and HypertrophyCT scan reconstructed in the sagittal plane shows right ventricular enlargement with hypertrophy of the trabeculated inflow portion and smooth walled outflow (RVOT) portion. The RVOT points anteriorly. The MPA also appears dilated. The left atrium is enlarged and is compressing on a dilated esophagus. The anterior leaflet of the mitral valve is in fibrous continuity with the aortic valve.key wordsinfundibulum right ventricle RVOT right ventricular outflow tract aortic valve aortic sclerosis calcification enlarged left atrium heart normal conotruncal relationship cardiacCourtesy Ashley Davidoff MD 201931149b.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Position of the Chambers and the Atrioventricular Valves of the HeartThe cross-sectional images from a CT scan through all 4 chambers reveals the relative position of the chambers and A-V valves. In general “blue” chambers are both anterior to and superior to the “red” chambers so that both the right atrium (RA) and right ventricle (RV) are anterior to the LA and LV. The tricuspid valve (blue valve) follows the rule and is slightly anterior to the mitral valve as well. Not shown here is that the fact that the right sided structures are slightly superiorly positioned.Ashley Davidoff, M.D.27531cd01.8s aka heart-anatomy-P-070
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Position of the Chambers and the Atrioventricular Valves of the HeartThe cross-sectional images from a CT scan through all 4 chambers reveals the relative position of the chambers and A-V valves. In general “blue” chambers are both anterior to and superior to the “red” chambers so that both the right atrium (RA) and right ventricle (RV) are anterior to the LA and LV. The tricuspid valve (blue valve) follows the rule and is slightly anterior to the mitral valve as well. Not shown here is that the fact that the right sided structures are slightly superiorly positioned.Ashley Davidoff, M.D.27531cd01.8s aka heart-anatomy-P-070
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Position of the Chambers and the Atrioventricular Valves of the HeartThe cross-sectional images from a CT scan through all 4 chambers reveals the relative position of the chambers and A-V valves. In general “blue” chambers are both anterior to and superior to the “red” chambers so that both the right atrium (RA) and right ventricle (RV) are anterior to the LA and LV. The tricuspid valve (blue valve) follows the rule and is slightly anterior to the mitral valve as well. Not shown here is that the fact that the right sided structures are slightly superiorly positioned.Ashley Davidoff, M.D.27531cd01.8s aka heart-anatomy-P-070
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Position of the Chambers and the Atrioventricular Valves of the HeartThe cross-sectional images from a CT scan through all 4 chambers reveals the relative position of the chambers and A-V valves. In general “blue” chambers are both anterior to and superior to the “red” chambers so that both the right atrium (RA) and right ventricle (RV) are anterior to the LA and LV. The tricuspid valve (blue valve) follows the rule and is slightly anterior to the mitral valve as well. Not shown here is that the fact that the right sided structures are slightly superiorly positioned.Ashley Davidoff, M.D.27531cd01.8s aka heart-anatomy-P-070
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Scleroderma, Interstitial Lung Disease, and Cor Pulmonale40 year old female with known interstitial lung disease (a and b) shows enlarged right atrium and right ventricle and small pericardial effusion (c and overlaid in maroon in d) and enlarged esophagus (overlay in pink in d) and an edematous gallbladder wall from chronic right heart failure.key wordslungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx sclerodermaCourtesy Ashley Davidoff MD 2019 30464c08
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Scleroderma, Interstitial Lung Disease, and Cor Pulmonale40 year old female with known interstitial lung disease (a and b) shows enlarged right atrium and right ventricle and small pericardial effusion (c and overlaid in maroon in d) and enlarged esophagus (overlay in pink in d) and an edematous gallbladder wall from chronic right heart failure.key wordslungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx sclerodermaCourtesy Ashley Davidoff MD 2019 30464c08
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Scleroderma, Interstitial Lung Disease, and Cor Pulmonale40 year old female with known interstitial lung disease (a and b) shows enlarged right atrium and right ventricle and small pericardial effusion (c and overlaid in maroon in d) and enlarged esophagus (overlay in pink in d) and an edematous gallbladder wall from chronic right heart failure.key wordslungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx sclerodermaCourtesy Ashley Davidoff MD 2019 30464c08
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Scleroderma, Interstitial Lung Disease, and Cor Pulmonale40 year old female with known interstitial lung disease (a and b) shows enlarged right atrium and right ventricle and small pericardial effusion (c and overlaid in maroon in d) and enlarged esophagus (overlay in pink in d) and an edematous gallbladder wall from chronic right heart failure.key wordslungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx sclerodermaCourtesy Ashley Davidoff MD 2019 30464c08
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Fetal heart on UltrasoundThis image is a 3D reconstruction of a fetal heart in sagittal view, showing the aorta with brachiocephalic vessels, the left atrium abutting the descending aorta posteriorly, and the right ventricle situated anteriorly. No other technology has such an exquisite ability to image the fetal heart.keyt wordscode heart normal fetus imaging cardiac echo overlayCourtesy of Philips Medical Systems, Ultrasound 32143
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Fetal heart on UltrasoundThis image is a 3D reconstruction of a fetal heart in sagittal view, showing the aorta with brachiocephalic vessels, the left atrium abutting the descending aorta posteriorly, and the right ventricle situated anteriorly. No other technology has such an exquisite ability to image the fetal heart.keyt wordscode heart normal fetus imaging cardiac echo overlayCourtesy of Philips Medical Systems, Ultrasound 32143
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Fetal heart on UltrasoundThis image is a 3D reconstruction of a fetal heart in sagittal view, showing the aorta with brachiocephalic vessels, the left atrium abutting the descending aorta posteriorly, and the right ventricle situated anteriorly. No other technology has such an exquisite ability to image the fetal heart.keyt wordscode heart normal fetus imaging cardiac echo overlayCourtesy of Philips Medical Systems, Ultrasound 32143
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Fetal heart on UltrasoundThis image is a 3D reconstruction of a fetal heart in sagittal view, showing the aorta with brachiocephalic vessels, the left atrium abutting the descending aorta posteriorly, and the right ventricle situated anteriorly. No other technology has such an exquisite ability to image the fetal heart.keyt wordscode heart normal fetus imaging cardiac echo overlayCourtesy of Philips Medical Systems, Ultrasound 32143
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Short axis of an anatomic specimen showing the tricuspid valve within the right ventricle and the mitral valve within the left ventricle. the anterior leaflet of the mitral valve is in fibrous continuity with the aortic valveAshley Davidoff MD01592
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Short axis of an anatomic specimen showing the tricuspid valve within the right ventricle and the mitral valve within the left ventricle. the anterior leaflet of the mitral valve is in fibrous continuity with the aortic valveAshley Davidoff MD01592
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Short axis of an anatomic specimen showing the tricuspid valve within the right ventricle and the mitral valve within the left ventricle. the anterior leaflet of the mitral valve is in fibrous continuity with the aortic valveAshley Davidoff MD01592
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Short axis of an anatomic specimen showing the tricuspid valve within the right ventricle and the mitral valve within the left ventricle. the anterior leaflet of the mitral valve is in fibrous continuity with the aortic valveAshley Davidoff MD01592
)