
Clinical
?Sinus tachycardia
?Elevated jugular venous pressure
?Pulsus paradoxus
- Echo
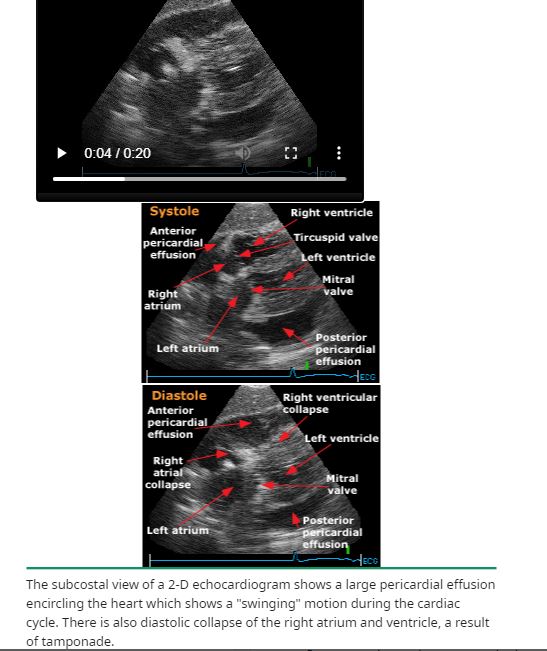
- Collapse of the right atrium at end-diastole
- At end-diastole (during atrial relaxation), the RA volume is minimal, but pericardial pressure is maximal, causing the RA to buckle
- Collapse of the right ventricle in early diastole
- less sensitive for the presence of cardiac tamponade than RA
- occurs in early diastole when the RV volume is still low.
- may not be present when the RV is hypertrophied diastolic pressure is significantly elevated
- collapse of any cardiac chamber, but usually the right sided chambers, oes are only slightly exceeded by those in the pericardium
- may not be present when the RV is hypertrophied diastolic pressure is significantly elevated
-
From Up to Date
Collapse of the right atrium and right ventricle in diastole
From Up to Date
Slit like of right ventricle in diastole
- Reciprocal changes in left and right ventricular volumes with respiration, which are important in the pathogenesis of pulsus paradoxus
- IVC
- IVC >20mm
- On inspiration stays the same – Should decrease with inspiration by about 50%
- Collapse of the right atrium at end-diastole
- CT
- distention of the
- venae cavae and hepatic veins,
- deformity cardiac chambers,
- bowing of the interventricular septum, and
- reflux of contrast into the azygos vein and inferior vena cava
- ? coronary sinus compression on CT is an early specific indicator
- ?right ventricular wall flattening